")
Back to Journals » Journal of Inflammation Research » Volume 14
Prealbumin and Retinol-Binding Protein 4: The Promising Inflammatory Biomarkers for Identifying Endoscopic Remission in Crohn’s Disease
Authors Chen R, Li L, Li C , Su Y , Zhang Y, Pang X, Zheng J, Zeng Z, Chen MH, Zhang S
Received 12 October 2021
Accepted for publication 9 December 2021
Published 25 December 2021 Volume 2021:14 Pages 7371—7379
DOI https://doi.org/10.2147/JIR.S343125
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Rirong Chen,1,* Li Li,1,* Chao Li,2 Yuhan Su,2 Yingfan Zhang,1 Xiaobai Pang,2 Jieqi Zheng,2 Zhirong Zeng,1 Min-Hu Chen,1 Shenghong Zhang1
1Division of Gastroenterology, The First Affiliated Hospital, Sun Yat-Sen University, Guangzhou, People’s Republic of China; 2Department of Clinical Medicine, Zhongshan School of Medicine, Sun Yat-Sen University, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shenghong Zhang
Division of Gastroenterology, The First Affiliated Hospital, Sun Yat-Sen University, No. 58 Zhongshan Road 2, Guangzhou, 510080, People’s Republic of China
Tel +86 20-87755766
Fax +86 20-87332916
Email [email protected]
Objective: Endoscopic remission is the primary therapeutic target and associated with clinical outcome in Crohn’s disease (CD). Non-invasive and accurate biomarkers are important in monitoring endoscopic remission frequently. Our study aimed at investigating the predictive capacity of prealbumin and retinol-binding protein 4 (RBP4) for identifying endoscopic remission.
Methods: From June 2018 to December 2020, 515 endoscopy procedures (332 in the training cohort and 183 in the validation cohort) were enrolled in this multicentre retrospective cohort study. Blood samples were collected for prealbumin or RBP4 testing with 7 days before the endoscopy. A simple Endoscopic Score for CD (SES-CD) was performed to evaluate endoscopic activity and defined endoscopic remission. The area under receiver operating characteristic curve (AUROC), sensitivity, specificity, positive predictive value and negative predictive value were performed to assess the predictive capacity of the biomarkers.
Results: Serum concentration of prealbumin and RBP4 was demonstrated to be higher in patients with endoscopic remission and significantly negatively correlated with SES-CD in the training cohort. The AUROC of prealbumin and specificity of prealbumin and RBP4 were larger than that of C-reactive protein in the training cohort and the validation cohort. The model combining prealbumin and faecal calprotectin had the largest AUROC (0.842 [95% CI: 0.775– 0.908]). Furthermore, in both cohorts, prealbumin had a larger AUROC than C-reactive protein for identifying endoscopic remission in patients with anti-tumour necrosis factor therapy.
Conclusion: Prealbumin and RBP4 were promising biomarkers for identifying endoscopic remission, especially in patients with anti-tumour necrosis factor therapy.
Keywords: Crohn’s disease, endoscopic remission, prealbumin, retinol-binding protein 4
Introduction
Crohn’s disease (CD) is a disabling condition characterized by chronic inflammation all around the gastrointestinal tract with a destructive course.1 With the development of treat-to-target strategy and advanced therapies, the therapeutic target of CD has been converted from clinical remission to endoscopic remission, which is associated with improved outcome in patients with CD.2 However, endoscopy, the optimal approach to assess endoscopic remission, is invasive, costly and lacks the accessibility to popularize under current health care landscapes. Therefore, heterogeneous group of surrogate assessing tools, such as serological and faecal biomarkers, are in an acute requirement for monitoring the disease activity.3
Presently, faecal calprotectin (FC) and C-reactive protein (CRP) are two reliable biomarkers in the assessment of endoscopic activity.4 FC is a promising biomarker in CD with high accuracy to evaluate the inflammatory process.5 Nevertheless, invalided optimal cut-off values and low utilization of FC would limit its ability in clinical practice.6 Compared with FC, CRP has been utilized more widely in clinical practice. However, since the serum concentration of CRP is affected by gene polymorphism and lacks clear correlation with mucosal activity, it still requires further research to seek novel serum biomarkers with high predictive capacity and convenience in identifying endoscopic remission.7,8
Prealbumin and retinol-binding protein 4 (RBP4) are traditionally considered as nutritional biomarkers, and they combine together to play an important role in the transportation of vitamin A.9 In the past decades, prealbumin and RBP4 were demonstrated to be acute-phase reactants, and their concentration would alter during acute or chronic inflammatory states, such as sepsis, coronary artery disease and rheumatoid arthritis.10–12 Furthermore, some pro-inflammatory cytokines including interleukin (IL)-6 and tumour necrosis factor (TNF)-α can affect serum level of prealbumin.13,14 The above studies suggested that prealbumin and RBP4 may be potential biomarkers for reflecting inflammation conditions. Our study is aimed at investigating the predictive capacity of prealbumin and RBP4 in distinguishing endoscopic remission from endoscopic activity in CD.
Materials and Methods
Patients and Study Design
Patients undergoing endoscopy procedures at the First Affiliated Hospital of Sun Yat-Sen University from June 2018 to December 2020 or at the Six Affiliated Hospital of Sun Yat-Sen University from June 2020 to December 2020 were recruited in this multicentre retrospective cohort study. Other inclusion criteria included: (1) a confirmed diagnosis of CD based on clinical symptoms, imaging presentations and histological data; (2) available blood samples for prealbumin or RBP4 testing within 7 days before the endoscopy procedures. Patients, who rejected to the recruitment, suffered infection within 3 months before the endoscopy procedure or had a diagnosis of upper gastrointestinal CD were excluded from this study.
Four hundred and thirty-seven samples from the First Affiliated Hospital of Sun Yat-Sen University and 78 samples from the Six Affiliated Hospital of Sun Yat-Sen University were eligible in the study and divided into two independent cohorts. The training cohort included samples obtained from the First Affiliated Hospital of Sun Yat-Sen University between June 2018 and May 2020. The validation cohort recruited samples obtained from the First Affiliated Hospital of Sun Yat-Sen University and the Six Affiliated Hospital of Sun Yat-Sen University between June 2020 and December 2020.
Demographic and Clinical Variables
Demographic and clinical variables, including gender, age at endoscopy procedures, age at diagnosis, disease location, disease behaviour, history of CD-related surgery, body mass index, medication use and endoscopy activity situation, were reported in this study. Age at diagnosis, disease location, and disease behaviour was described following the Montreal Classifications.15 Medication use referred to more than 3 months continuous use of 5-aminosalicylic acid, thiopurine, thalidomide, corticosteroids or anti-TNF agents.
Biomarker Testing
Blood samples and faecal samples were collected within 7 days before endoscopy procedures. Blood prealbumin concentrations were measured using the latex immune turbidimetry assay with a kit from beckman coulter (CA 92821, USA, OSR6175). The RBP4 concentrations were measured using a latex immune turbidimetry assay with a kit from Labco (Co-Health (Beijing) Laboratories Co., Beijing, China, GG21B2). Serum CRP levels were detected through scattering rate turbidimetry method (Siemens, Marburg, Germany, OQIY21). The FC levels were tested using immunofluorescence chromatography (Guangzhou Forreal Biotechnology Co., Guangzhou, China).
Definition of Endoscopic Remission and Activity
Simple Endoscopic Score for Crohn’s Disease (SES-CD) was used to describe the endoscopic activity situation.16 Two surgeons, blinded to the biomarker testing result, performed SES-CD for all endoscopies in the study, respectively. Endoscopic remission was defined as SES-CD≤2. Endoscopic activity was defined as SES-CD≥3. Furthermore, endoscopic activity was divided into three degrees based on SES-CD: mild activity (3–6), moderate activity (7–15) and severe activity (≥16).
Ethical Considerations
This study was conducted in accordance with the Declaration of Helsinki and approved by the Research Ethics Committee of the First Affiliated Hospital of Sun Yat-Sen University [No. IIT-2021-130]. All patients participated in this study had written informed consent.
Statistics Analysis
Continuous and categorical variables were presented as median (interquartile range, IQR) and n (%), respectively. The Mann–Whitney test and χ2 test were performed to evaluate the difference for continuous and categorical variables, respectively. Spearman’s regression was used for correlation analysis. A p-value less than 0.05 was considered to be statistically significant. The receiver operating characteristic (ROC) analysis was performed to calculate the area under ROC curve (AUROC). The cut-off value was determined by the Youden index in the training cohort and acted as a threshold for the biomarkers in the validation cohort. AUROC, sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) were used to assess the predictive capacity of the biomarkers for identifying endoscopic remission. We performed Pearson’s χ2 test to assess the difference in sensitivity and specificity of the biomarkers for identifying endoscopic remission. Logistic regression analysis was performed to build the model combined with prealbumin and FC. All statistical analysis was performed through R version 4.0.0 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Patients Characteristics
From June 2018 to December 2020, 515 endoscopy procedures (332 samples in the training cohort and 183 samples in the validation cohort) were enrolled in this cohort study (Table 1). In the training cohort, 242 (72.9%) patients were male, and the median age at endoscopic procedures was 28.0 years (IQR: 21.9–36.0). According to disease location, 68 (20.5%), 38 (11.4%), 226 (68.1) were ileal, colonic and ileocolonic, respectively. Fifty-nine (17.8%) patients received continuous anti-tumour necrosis factor (TNF) therapy more than 3 months before the endoscopy and 61 (18.4%) of samples were in endoscopic remission. In the validation cohort, only a percentage of patients with history of CD-related surgery (15.3% vs 22.9%; p = 0.040) and prior use of thiopurine (26.2% vs 17.5%; p = 0.019) differed significantly from that in the training cohort. Other demographic and clinical characteristics are showed in Table 1.
 |
Table 1 Demographic and Clinical Characteristics of Patients in the Study |
Relationship Between Biomarkers and Endoscopy Activity in the Training Cohort
First, we performed Mann–Whitney test to investigate the discrepant concentration of potential biomarkers including prealbumin, RBP4, vitamin D, albumin, globulin, CRP and FC, between endoscopic remission and endoscopic activity (Figure 1 and Supplement Table 1). Significantly higher concentration of prealbumin (remission vs activity: 254.0 [IQR 216.2.-292.0] mg/l vs 184.0 [IQR 147.0–225.0] mg/L, p < 0.001; Figure 1A), RBP4 (remission vs activity: 27.9 [IQR 22.8–32.1] mg/l vs 20.7 [IQR 16.3–25.8] mg/L, p < 0.001; Figure 1B), vitamin D (p = 0.018; Supplement Table 1) and albumin (p<0.001; Supplement Table 1) was shown in endoscopic remission compared with endoscopic activity, while CRP (p < 0.001; Figure 1C), FC (p < 0.001; Figure 1D) and globulin (p < 0.001; Supplement Table 1) concentrations were significantly lower in patients with endoscopic remission. Furthermore, prealbumin (0.773 [95% CI: 0.705–0.841]), RBP4 (0.728 [95% CI: 0.646–0.809]) and CRP (0.759 [95% CI: 0.692–0.826]) had larger AUROC than other serum biomarkers in distinguishing endoscopic remission from endoscopic activity (Supplement Table 2).
 |
Figure 1 Discrepant concentration of prealbumin (A), retinol-binding protein 4 (B), C-reactive protein (C) and faecal calprotectin (D) between endoscopic remission and endoscopic activity in the training cohort. The box plots present median and interquartile range of the data, and the whiskers show the maximum and minimum values. |
We next assessed the strength of the association between prealbumin, RBP4, CRP and endoscopy activity using Spearman correlation analysis. As shown in Table 2, prealbumin (r=−0.588, p < 0.01) was strongly correlated with SES-CD and RBP4 (r=−0.485, p < 0.01) was moderately correlated with SES-CD negatively. In addition to SES-CD, prealbumin (r=−0.761, p < 0.01) and RBP4 (r=−0.626, p < 0.01) also had negative correlation with CRP.
 |
Table 2 Spearman Correlation Analysis Between Prealbumin, RBP4, CRP and SES-CD in the Training Cohort |
Prealbumin and RBP4 Could Identify Endoscopic Remission
In order to assess the predictive capacity of prealbumin and RBP4 for distinguishing endoscopic remission from endoscopic activity, ROC analysis was performed in both training cohort (Table 3) and validation cohort (Table 4). In the training cohort, the result showed that the AUROC of prealbumin (0.773 [95% CI 0.705–0.841]) in identifying endoscopic remission was larger than that of RBP4 (0.728 [95% CI 0.646–0.809]) and CRP (0.759 [95% CI 0.692–0.826]), but smaller than FC’s (0.815 [95% CI 0.727–0.904]). The model combining FC and prealbumin had the largest AUROC (0.842 [95% CI: 0.775–0.908]). Moreover, the sensitivity of prealbumin at a cut-off value 215.5 mg/L was 0.770 (95% CI 0.642–0.865) and 0.697 (95% CI 0.638–0.751), respectively. RBP4 at a cut-off value of 24.8 mg/L had a sensitivity of 0.723 (95% CI 0.571–0.839) and a specificity of 0.702 (95% CI 0.639–0.759). We also observed that both prealbumin and RBP4 had higher specificity than CRP (0.587 [95% CI 0.525–0.646]; p = 0.007 for prealbumin vs CRP; p = 0.007 for RBP4 vs CRP; Table 3). The sensitivity of FC (0.704 95% CI [0.497–0.855]) was marginal lower than that of prealbumin and RBP4, but the differences were not significant (p = 0.505 for prealbumin vs FC; p = 0.865 for RBP4 vs FC) (Table 3). Although there was lack of head-to-head comparison among prealbumin, RBP4 and FC in the entire training cohort, we performed a ROC analysis in a smaller cohort (n [total] = 143; n [endoscopic remission] = 22) containing participants with all the data of prealbumin, RBP4 and FC, and found that prealbumin (0.832 [95% CI: 0.764–0.901]) and RBP4 (0.803 [95% CI: 0.726–0.880]) had similar AUROCs with FC (0.816 [95% CI: 0.718–0.915]) (Supplement Figure 1). Due to the limited sample sizes of endoscopic remission in this cohort, more research was necessary to validate the result.
 |
Table 3 The Predictive Capacity of Prealbumin, Retinol-Binding Protein 4, CRP and FC for Identifying Endoscopic Remission in the Training Cohort |
 |
Table 4 The Predictive Capacity of Prealbumin, Retinol-Binding Protein 4 and CRP and for Identifying Endoscopic Remission in the Validation Cohort |
In the validation cohort, prealbumin also had a larger AUROC (0.817 [95% CI 0.754–0.880]) than that of RBP4 (0.764 [95% CI 0.686–0.842]) and CRP (0.804 [95% CI 0.732–0.876]; Table 4). At a threshold of 215.5 mg/L, prealbumin had a sensitivity and specificity of 0.875 (95% CI 0.701–0.959) and 0.702 (95% CI 0.621–0.772). The specificity of prealbumin was superior to that of CRP (specificity: 0.556 [95% CI 0.473–0.663]; p = 0.009) and the sensitivity of prealbumin is not inferior to that of CRP (sensitivity: 0.844 [95% CI 0.665–0.941]; p = 0.719). Furthermore, sensitivity (0.862 [95% CI: 0.674–0.955]) and specificity (0.572 [95% CI: 0.485–0.655]) of RBP4 at a threshold of 24.8 mg/L were similar with that of CRP (p = 0.522 for sensitivity; p = 0.782 for specificity).
Prealbumin Was Superior to CRP in Patients with Anti-TNF Therapy
To investigate the predictive capacity of prealbumin for identifying endoscopic remission in different CD patients, we developed further subgroup analysis. As the result showed in Figure 2, prealbumin had a larger AUROC for identifying endoscopic remission than CRP in both training cohort (0.808 [95% CI:0.678–0.973] vs 0.716 [95% CI: 0.559–0.873]) and validation cohort (0.807 [95% CI:0.670–0.974] vs 0.753 [95% CI: 0.549–0.958]). Regarding patients with ileal disease, we found that prealbumin had a better predictive capacity than CRP in the validation cohort (0.726 [95% CI:0.589–0.684] vs 0.569 [95% CI: 0.422–0.716]), while both prealbumin and CRP were poor in predicting endoscopic remission in the validation cohort (Supplement Figure 2).
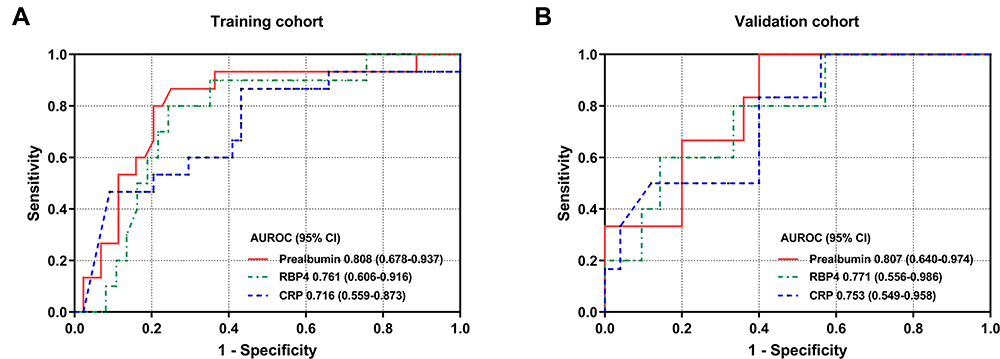 |
Figure 2 Receiver operating characteristic (ROC) curve of prealbumin, retinol-binding protein 4 (RBP4) and C-reactive protein (CRP) for identifying endoscopic remission in patients with anti-tumour necrosis factor agents use in the training cohort (A) or the validation cohort (B). |
Discussion
Endoscopic remission is now the primary therapeutic target in CD. Although endoscopy is the gold standard in assessing endoscopic activity, it is invasive, costly and unfavourable for CD patients. Therefore, identification of non-invasive and widely used biomarkers is important in monitoring endoscopic activity frequently. In this study, we demonstrated that prealbumin as well as RBP4 concentration was significantly higher in endoscopic remission than endoscopic activity and had a negative correlation with SES-CD. Further ROC analysis showed that prealbumin had a larger AUROC in identifying endoscopic remission when compared with CRP, especially in patients with anti-TNF therapy. The results of our study indicated the potential role of prealbumin and RBP4 in monitoring endoscopic remission in patients with CD.
Prealbumin, namely transthyretin, is synthesized in the liver and serves as a transporter of thyroid hormone and vitamin A.17 In addition to its function of transport, prealbumin also acts as a significant indicator in reflecting nutritional status, or even predicting the effect of nutritional therapy in some diseases, such as CD.18 For instance, Xu et al illustrated that the change of prealbumin concentration from baseline to the first week of exclusive enteral nutrition treatment could predict the following clinical remission in colonic CD patients.19 Moreover, previous studies have found that the concentration of prealbumin is associated with the disease activity of inflammatory states such as rheumatoid arthritis and tuberculosis infection.20,21 Similar to these studies, we firstly demonstrated that serum prealbumin level was strongly correlated with endoscopic disease severity and had a good capacity in distinguishing endoscopic remission from endoscopic activity. The malnutritional state, as well as the high concentration of IL-6, which could reduce serum prealbumin concentration, in CD patients with endoscopic activity, may explain the findings of our research, while further basic study needs to be performed to attest to this hypothesis.22
In this study, we determined the ability of RBP4, another nutritional-inflammatory biomarker, in identifying endoscopic remission. We discovered that RBP4 was similar but slightly inferior to prealbumin in its correlation with CRP and SES-CD and its predictive ability in identifying endoscopic activity. The close relationship between RBP4 and prealbumin seems to explain this result in our study. Previous studies have demonstrated that RBP4 also exhibited an important function in transporting vitamin A and could be combined with prealbumin to compose a retinol circulating complex, which stabilized the structure of prealbumin and prevented RBP4 from filtration through glomerulus.18,23 Therefore, the alteration of RBP4 or prealbumin concentration may exert an implication on the other one’s concentration. Because prealbumin had a stronger correlation with endoscopic activity than RBP4, we hypothesised that the intestinal inflammation and circulating pro-inflammatory cytokine in CD patients mainly reduced the serum prealbumin concentration, which then affected the serum level of RBP4.
Besides prealbumin and RBP4, other nutritional indicators such as vitamin D, albumin, uric acid-to-creatine ratio are considered to be associated with the disease or endoscopic activity in CD.24–26 Among these indicators, vitamin D is one of the most widely studied biomarkers in CD and is effective in the assessment of disease activity, prediction of clinical outcome and response to biologics therapy.27 Similar to vitamin D, prealbumin and RBP4 are demonstrated to play an important role in the activity assessment and prognosis prediction of some inflammatory diseases.17,28,29 Furthermore, previous study and our study indicated that the predictive capacity of prealbumin and RBP4 was likely superior to vitamin D in identifying endoscopic remission.30 This suggests that prealbumin or RBP4 may be promising biomarkers with broad application in CD, and more research needs to be carried out.
It is important to mention that, in this study, prealbumin was demonstrated to be more accurate in predicting endoscopic remission than CRP, one of the most widely utilized biomarkers in clinical practice. In particular, the AUROC of prealbumin in patients with anti-TNF therapy was obviously superior to that of CRP. Anti-TNF agents are one of the most significant and effective therapy in inducing and maintaining remission in CD. And frequent monitoring of disease or endoscopic activity during anti-TNF therapy was momentous for assessing therapeutic response and selecting optimal approach.31 Therefore, based on the result of this study, we suggested the routine utilization of prealbumin in monitoring disease activity during anti-TNF therapy in CD. In addition to the better predictive capacity, prealbumin has an advantage over CRP in identifying endoscopic remission since the serum concentration of prealbumin was not found to be affected by ethnic differences or gene polymorphisms.7,17 Thus, we believe prealbumin would become a reliable and universal biomarker for monitoring endoscopic remission and benefit more patients with CD.
There are some limitations in our study. First, this study was a retrospective cohort study, recruiting patients who underwent prealbumin or RBP4 testing within 7 days before endoscopy, which may cause selection bias. Second, we lacked a head-to-head comparison in the entire cohort between prealbumin, RBP4 and FC, which was currently considered the most effective biomarker in disease activity assessment. In order to address this problem to some extent, we performed an ROC analysis on participants that had all data of prealbumin, RBP4 and FC and found similar capacities for these biomarkers to identify endoscopic remission. Nevertheless, only a small number of participants with endoscopic remission were included in this analysis, thus confirming the result necessitated more research with large sample sizes. Moreover, there was only a small cohort of patients with colonic disease in this study, so the predictive capacity of prealbumin and RBP4 in colonic CD patients required further validations.
In conclusion, prealbumin and RBP4 are promising biomarkers for assessing endoscopic activity and identifying endoscopic remission in patients with CD. The application of prealbumin and RBP4 for frequent monitoring of endoscopic activity may be significant for the treat-to-target approaches and benefit CD patients.
Data Availability
The data supporting the result in this study are available from the corresponding author (Shenghong Zhang, China) on request.
Acknowledgments
This project was supported by grants from the National Natural Science Foundation of China (#81670498, #81870374, #81870384, #81630018, #82000520), Guangzhou Science and Technology Department (#202002030041), Guangdong Science and Technology (#2017A030306021, #2020A1515010249), China Postdoctoral Science Foundation (#2019M653228) and Science and Technology Innovation Young Talents of Guangdong Special Support Plan (#2016TQ03R296). The abstract for this manuscript was presented at a conference named the 21st Congress of Gastroenterology China, 2021 (https://onlinelibrary.wiley.com/doi/10.1111/1751-2980.13053).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The Authors declare that there is no conflict of interest.
References
1. Roda G, Ng SC, Kotze PG, et al. Author Correction: Crohn’s disease. Nat Rev Dis Primers. 2020;6(1). doi:10.1038/s41572-020-0193-x
2. Shah SC, Colombel JF, Sands BE, Narula N. Systematic review with meta-analysis: mucosal healing is associated with improved long-term outcomes in Crohn’s disease. Aliment Pharm Ther. 2016;43(3):317–333. doi:10.1111/apt.13475
3. Buisson A, Gonzalez F, Poullenot F, et al. Comparative acceptability and perceived clinical utility of monitoring tools: a nationwide survey of patients with inflammatory bowel disease. Inflamm Bowel Dis. 2017;23(8):1425–1433. doi:10.1097/MIB.0000000000001140
4. Mosli MH, Zou GY, Garg SK, et al. C-reactive protein, fecal calprotectin, and stool lactoferrin for detection of endoscopic activity in symptomatic inflammatory bowel disease patients: a systematic review and meta-analysis. Am J Gastroenterol. 2015;110(6):802–819. doi:10.1038/ajg.2015.120
5. Lin JF, Chen JM, Zuo JH, et al. Meta-analysis: fecal calprotectin for assessment of inflammatory bowel disease activity. Inflamm Bowel Dis. 2014;20(8):1407–1415. doi:10.1097/MIB.0000000000000057
6. Limketkai BN, Singh S, Jairath V, Sandborn WJ, Dulai PS. US practice patterns and impact of monitoring for mucosal inflammation after biologic initiation in inflammatory bowel disease. Inflamm Bowel Dis. 2019;25(11):1828–1837. doi:10.1093/ibd/izz081
7. Carlson CS, Aldred SF, Lee PK, et al. Polymorphisms within the C-reactive protein (CRP) promoter region are associated with plasma CRP levels. Am J Hum Genet. 2005;77(1):64–77.
8. Saverymuttu SH, Hodgson HJ, Chadwick VS, Pepys MB. Differing acute phase responses in Crohn’s disease and ulcerative colitis. Gut. 1986;27(7):809–813. doi:10.1136/gut.27.7.809
9. Blaner WS. Retinol-binding protein: the serum transport protein for vitamin A. Endocr Rev. 1989;10(3):308–316.
10. Biolo G, Toigo G, Ciocchi B, et al. Metabolic response to injury and sepsis: changes in protein metabolism. Nutrition. 1997;13(9 Suppl):52S–57S. doi:10.1016/S0899-9007(97)00206-2
11. Lambadiari V, Kadoglou NP, Stasinos V, et al. Serum levels of retinol-binding protein-4 are associated with the presence and severity of coronary artery disease. Cardiovasc Diabetol. 2014;13:121. doi:10.1186/s12933-014-0121-z
12. Ni M, Wei W, Feng Q, et al. Transthyretin as a potential serological marker for the diagnosis of patients with early rheumatoid arthritis. Clin Exp Rheumatol. 2013;31(3):394–399.
13. Banks RE, Forbes MA, Storr M, et al. The acute phase protein response in patients receiving subcutaneous IL-6. Clin Exp Immunol. 1995;102(1):217–223. doi:10.1111/j.1365-2249.1995.tb06659.x
14. Aguilera A, Codoceo R, Selgas R, et al. Anorexigen (TNF-alpha, cholecystokinin) and orexigen (neuropeptide Y) plasma levels in peritoneal dialysis (PD) patients: their relationship with nutritional parameters. Nephrol Dial Transplant. 1998;13(6):1476–1483. doi:10.1093/ndt/13.6.1476
15. Silverberg MS, Satsangi J, Ahmad T, et al. Toward an integrated clinical, molecular and serological classification of inflammatory bowel disease: report of a Working Party of the 2005 Montreal World Congress of Gastroenterology. Can J Gastroenterol. 2005;19(19 Suppl A):5A–36A. doi:10.1155/2005/269076
16. Daperno M, D’Haens G, Van Assche G, et al. Development and validation of a new, simplified endoscopic activity score for Crohn’s disease: the SES-CD. Gastrointest Endosc. 2004;60(4):505–512. doi:10.1016/S0016-5107(04)01878-4
17. Ingenbleek Y, Bernstein LH. Plasma transthyretin as a biomarker of lean body mass and catabolic states. Adv Nutr. 2015;6(5):572–580. doi:10.3945/an.115.008508
18. Ingenbleek Y, Van Den Schrieck HG, De Nayer P, De Visscher M. The role of retinol-binding protein in protein-calorie malnutrition. Metabolism. 1975;24(5):633–641. doi:10.1016/0026-0495(75)90143-2
19. Xu YH, Guo Z, Huang LY, et al. A nomogram for predicting the response to exclusive enteral nutrition in adult patients with isolated colonic Crohn’s disease. Ther Adv Gastroenter. 2019;12:175628481988130. doi:10.1177/1756284819881301
20. Wang JH, Xi HY, Zhang K, et al. Circulating C-reactive protein to prealbumin ratio and prealbumin to fibrinogen ratio are two promising inflammatory markers associated with disease activity in rheumatoid arthritis. Clin Lab. 2020;66(5):757–762. doi:10.7754/Clin.Lab.2019.190833
21. Luo Y, Xue Y, Yuan X, et al. Combination of prealbumin and tuberculosis-specific antigen/phytohemagglutinin ratio for discriminating active tuberculosis from latent tuberculosis infection. Int J Clin Pract. 2020;75(4):e13831. doi:10.1111/ijcp.13831
22. Jones J, Loftus EV, Panaccione R, et al. Relationships between disease activity and serum and fecal biomarkers in patients with Crohn’s disease. Clin Gastroenterol H. 2008;6(11):1218–1224. doi:10.1016/j.cgh.2008.06.010
23. Hyung SJ, Deroo S, Robinson CV. Retinol and retinol-binding protein stabilize transthyretin via formation of retinol transport complex. Acs Chem Biol. 2010;5(12):1137–1146. doi:10.1021/cb100144v
24. Gubatan J, Chou ND, Nielsen OH, Moss AC. Systematic review with meta-analysis: association of vitamin D status with clinical outcomes in adult patients with inflammatory bowel disease. Aliment Pharmacol Ther. 2019;50(11–12):1146–1158. doi:10.1111/apt.15506
25. Kaplan M, Yuksel M, Ates I, et al. Is ischemia modified albumin a disease activity marker for inflammatory bowel diseases? J Gastroen Hepatol. 2016;31(6):1120–1125.
26. Zhu F, Feng D, Zhang T, et al. Altered uric acid metabolism in isolated colonic Crohn’s disease but not ulcerative colitis. J Gastroenterol Hepatol. 2019;34(1):154–161. doi:10.1111/jgh.14356
27. Nielsen OH, Rejnmark L, Moss AC. Role of vitamin D in the natural history of inflammatory bowel disease. J Crohns Colitis. 2018;12(6):742–752. doi:10.1093/ecco-jcc/jjy025
28. Zabetian-Targhi F, Mahmoudi MJ, Rezaei N, Mahmoudi M. Retinol binding protein 4 in relation to diet, inflammation, immunity, and cardiovascular diseases. Adv Nutr. 2015;6(6):748–762. doi:10.3945/an.115.008292
29. Nguyen MVC, Baillet A, Romand X, et al. Prealbumin, platelet factor 4 and S100A12 combination at baseline predicts good response to TNF alpha inhibitors in rheumatoid arthritis. Joint Bone Spine. 2019;86(2):195–201. doi:10.1016/j.jbspin.2018.05.006
30. Ye LN, Lin ZW, Liu J, Cao CQ. Vitamin D deficiency is associated with endoscopic severity in patients with Crohn’s disease. Gastroent Res Pract. 2017;2017:1–5. doi:10.1155/2017/4869718
31. Cohen BL, Sachar DB. Update on anti-tumor necrosis factor agents and other new drugs for inflammatory bowel disease. Brit Med J. 2017;357:j2505.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.