")
Back to Journals » OncoTargets and Therapy » Volume 16
Post-HSCT Maintenance Treatment Using Entrectinib for an AML Patient Accompanied with ETV6::NTRK3: A Case Report
Authors Zhao X, Hao M, Zhang X, Wei J, Feng S, He Y, Jiang E, Han M
Received 9 August 2023
Accepted for publication 4 December 2023
Published 18 December 2023 Volume 2023:16 Pages 1055—1059
DOI https://doi.org/10.2147/OTT.S434590
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Geoffrey Pietersz
Xiaoli Zhao,1,2 Mengze Hao,1,2 Xiaoyu Zhang,1,2 Jialin Wei,1,2 Sizhou Feng,1,2 Yi He,1,2 Erlie Jiang,1,2 Mingzhe Han1,2
1State Key Laboratory of Experimental Hematology, National Clinical Research Center for Blood Diseases, Haihe Laboratory of Cell Ecosystem, Institute of Hematology and Blood Diseases Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Tianjin, 300020, People’s Republic of China; 2Tianjin Institutes of Health Science, Tianjin, 301600, People’s Republic of China
Correspondence: Yi He, State Key Laboratory of Experimental Hematology, National Clinical Research Center for Blood Diseases, Haihe Laboratory of Cell Ecosystem, Institute of Hematology and Blood Diseases Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Tianjin, 300020, People’s Republic of China, Tel +86022-23909492, Email [email protected]
Abstract: The neurotrophic receptor tyrosine kinase (NTRK) gene fusions occur in a large number of solid tumors and tropomyosin receptor kinase (TRK) inhibitors exhibit attractive antitumor activity. However, the occurrence of NTRK fusions is rare in hematological malignancies, and just a few cases or pre-clinical researches have been reported. This case report presents a refractory acute myeloid leukemia (AML) patient, accompanied with ETV6::NTRK3, was failed by traditional chemotherapy, then entered long-term remission after hematopoietic stem cell transplantation (HSCT) and maintenance therapy with entrectinib. It was the first successful use of the TRK inhibitor in an AML patient after HSCT.
Keywords: entrectinib, acute myeloid leukemia, ETV6::NTRK3, allogeneic hematopoietic stem cell transplantation
Introduction
The neurotrophic receptor tyrosine kinase (NTRK) genes include NTRK1, NTRK2, and NTRK3, which encode the tropomyosin receptor kinase (TRK) family, including TRKA, TRKB, and TRKC respectively. The ligand binding initiates the process of homodimerization, which is followed by the specific tyrosine residue's phosphorylation in the kinase domain. This step results in the activation of several downstream pathways including JAK/STAT, PI3K/AKT, and RAS/MAPK to promote proliferation, differentiation, and survival.1 TRK proteins can be activated by a variety of mechanisms, including NTRK gene mutations, splice variants, overexpression, and NTRK gene fusion, of which, fusions involving NTRK1, NTRK2, or NTRK3 are the most common mechanisms of oncogenic TRK activation.2 NTRK gene fusions occur in many types of solid tumors.3 The frequency of NTRK fusions was detected in only 0.1% of patients (8 of 7311) with hematologic malignancies.4 In our hospital, only one patient carrying ETV6::NTRK3 (0.08%, 1/1200) has been detected since the implementation of RNA sequencing for the detection of fusion gene technology. The ETV6, mapping to chromosome 12p13 in humans, translocates to several partner genes in diverse cancers.5 Numerous hematological diseases have the fusions between ETV6 and phosphotyrosine kinases (PTKs),5 however, ETV6::NTRK3 frequencies in AML are rare.
Larotrectinib and entrectinib are TRK inhibitors approved by the Food and Drug Administration (FDA) for the treatment of adult and pediatric patients with solid tumors harboring an NTRK fusion gene, regardless of the histological types.6,7 TRK inhibitors have attracted considerable attention over the past few years due to their remarkable efficacy in solid tumor patients harboring NTRK fusions. Although, the occurrence of NTRK fusions are rare in hematological malignancies, some clinical cases or pre-clinical researches have been reported. In mouse models of acute lymphoid leukemia with ETV6::NTRK3, larotrectinib showed encouraging results in vivo and in vitro.8 Could TRK inhibitors be a choice for patients with hematologic malignancies accompanied by NTRK fusions? Here we report, for the first time, on one acute myeloid leukemia (AML) patient who was treated with entrectinib as maintenance therapy after hematopoietic stem cell transplantation (HSCT).
Case Presentation
The patient, a 46-year-old male, was admitted due to “intermittent fever and fatigue for over 2 months” in January 2021. The details of his blood cell analysis results after admission were: WBC 61.4×109/L, RBC 2.29×1012/L, HGB 70g/L, PLT 137×109/L, RET% 0.3%. Bone marrow aspiration was completed and morphology showed AML (FAB-M5b). Bone marrow trephine biopsy revealed acute leukemia with myelofibrosis (MF-3). Flow cytometry analysis demonstrated one population of immature cells accounted for 23.4%, expressing CD34, CD33, HLA-DR, CD13, CD123, CD117, CD11b, CD56, but MPO, cCD3, TDT and another myeloid lymphoid marker were negative. Chromosome fluorescence in-situ hybridization using CEP7/D7S486 found −7. The chromosome karyotype was complex which was 47, XY, t(2;15;3) (p23;q24;q26.2), +16 [7]/48, idem, +8[6]/46, idem, −7[3]/48, idem, +21[2]/46, XY[2]. No hotspot mutations were detected by next generation sequencing technology. RNA sequencing detected the ETV6::NTRK3 fusion gene due to t (12; 15) (p13.2; q25.3) (Table 1). According to morphology, immunology, cytogenetic and molecular criteria, the patient was diagnosed as AML (poor-risk, with ETV6-NTRK3, complex karyotype). The patient received the first induction therapy with cytarabine and daunorubicine but did not achieve remission. Then the patient received the second induction regimen with cytarabine, idarubicine and cyclophosphamide, however they had no response. The further salvage therapy with cladribine, homoharringtonine and cytarabine still did not obtain a reaction. A haploid match was detected between the HLA genotype of the patient and his son, and donor specific antibodies (DSA) were negative. Conditioning therapy was initiated on 18th May, 2021, specifically: melphalan (Mel) 60 mg/kg from days −9 to −8; cladribine (2-CdA) 5 mg/m2/d from days −7 to −5; busulfan (BU) 3.2 mg/kg/d from days −5 to −3; cyclophosphamide (CTX) 40 mg/kg/d from days −2 to −1; anti-thymocyte globulin (ATG, rabbit) 2.5 mg/kg/d from days −5 to −2. Tacrolimus, methotrexate and mycophenolate mofetil were used for prophylaxis of graft versus host disease (GVHD). Posaconazole was used for prophylaxis of fungal infection after transplantation. Haploidentical hematopoietic stem cells from donor (MNC 8.47×108/kg, and CD34+cell count 7.62×106/kg) were infused on 27th May, 2021. Granulocyte engraftment on day +11 and platelet engraftment on day +12. Minimal residual disease (MRD) monitoring was negative on days +28, +42, and +60. Maintenance therapy with entrectinib (400 mg once daily) has been initiated since day +60. After treatment for 3 weeks, due to decreased blood pressure (the lowest: 76/61mmHg) and fatigue, considered to be drug-related, entrectinib was discontinued. Then the blood pressure was gradually recovered and the symptoms were relieved. The patient received treatment with entrectinib (200mg once daily) again after 20 days of discontinuation. After one-week treatment, the drug was discontinued again due to unendurable muscle pain. Which was relieved after 3 weeks of discontinuation. The dosage of entrectinib was adjusted to 200 mg once every other day. Then the patient experienced edema and hyperuricemia, which were tolerable. Entrectinib was discontinued after one year treatment. Unfortunately, ETV6::NTRK3 became positive once again after 8 months discontinuation, 22 months post-transplantion. At the same time, the patient initialed preemptive therapy with entrectinib (200 mg once every other day). After 4 months treatment, the ETV6::NTRK3 became negative again. Currently, the patient has survived 27 months after the transplantation. The treatment strategy and evaluation are shown in Figure 1a and b.
 |
Table 1 The details of ETV6::NTRK3 fusion gene, with RNA sequencing, in the patient |
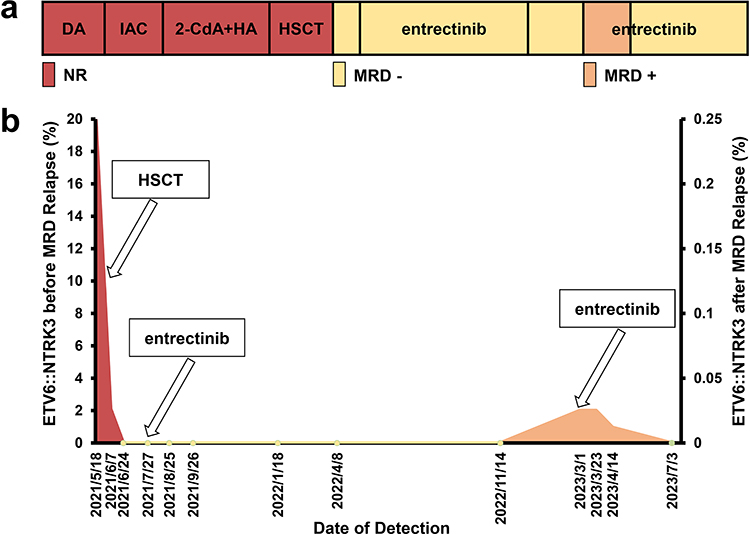 |
Figure 1 The treatment strategy and evaluation of this patient: (a) The patient received no response after three cycles of traditional treatments. The patient obtained the first complete response to HSCT, then survived with ETV6::NTRK3 negative after entrectinib maintenance treatment; (b) RNA sequencing regularly monitored quantification of ETV6::NTRK3. |
Discussion
The patient was diagnosed with AML, accompanied with ETV6::NTRK3 and complex karyotype at onset. Depressingly, it did not receive a response after multiple traditional treatments. Considering efficacy and safety of modified melphalan and busulfan-based regimen for refractory AML patients, we chose a regimen of HSCT to achieve a first remission.9 Although the patient received complete response after HSCT there was a high risk of relapse. Reasonable maintenance therapy after transplantation was necessary, which could reduce the chances of a relapse.10 Current options for maintenance therapy include: demethylating drugs, HDAC inhibitors, FLT3 inhibitors, IDH inhibitors, and so on.11 For this patient, carrying the ETV6::NTRK3 fusion gene, should TRK be selected as a target for maintenance therapy after transplantation?
In 1998, a 59-year-old woman diagnosed with AML FAB-M2 with ETV6::NTRK3 was first reported.12 The bone marrow of this patient was accompanied with severe fibrosis at the time of diagnosis, and the karyotype was complex, including +8. The patient had no response to three cycles of chemotherapy and died of multiple organ failure. Another patient diagnosed with AML FAB-M0 with ETV6::NTRK3 was a 55-year-old man in 2011, who had no response to traditional chemotherapy and gemtuzumab ozogamicine, and the patient died after a short period of supportive care.13 Our patient was a 46-year-old man, accompanied with severe fibrosis and +8, which was the same as the first woman patient, and the three patients did not achieve a response to traditional chemotherapy. Maybe ETV6::NTRK3 fusion in AML is related to a poor prognosis. Could TRK inhibitors be picked up to treat patients with hematologic malignancies with NTRK fusions, as TKI inhibitors treat patients with BCR/ABL fusions? At present, a small number of trials have reported the use of TRK inhibitors in hematological malignancies. In the AML cell line with ETV6::NTRK3 fusion, entrectinib blocked cell proliferation and induced apoptotic cell death in vitro and resulted in tumor regression in an animal model.14 A patient with AML who harbored an ETV6::NTRK2 fusion received 100 mg larotrectinib twice daily and receive a partial response.4 Based on these studies, TRK inhibitors might show clinical efficacy in hematologic malignancies.
Considering our patient with ETV6::NTRK3 and with a high risk of relapse, including with their central nervous system, we selected entrectinib as the maintenance therapy for them, after two months of transplantation. Given that the patient was required to take posaconazole for the prevention of fungal infections, the dose of entrectinib was adjusted to 400 mg, once daily. However, the drug was temporarily discontinued due to hypotension after 3 weeks of entrectinib therapy. Two weeks later, the drug dose was adjusted to 200 mg once daily for continued treatment but significant generalized muscle soreness occurred during treatment and it was discontinued again, 1 week after the treatment. Entrectinib is mainly metabolized by cytochrome P3A4 enzyme. When taken with CYP3A inhibitors, such as itraconazole, the plasma concentration of entrectinib is significantly increased (6-fold increase).15 Therefore, after the symptoms were relieved, the drug dose was adjusted to 200 mg once every other day for treatment. After adjustment, the patient experienced edema and hyperuricemia, which were tolerable. Unfortunately, ETV6::NTRK3 became positive once again after 8 months discontinuation. Fortunately, ETV6::NTRK3 became negative again after 4 months treatment with entrectinib alone. The patient has survived 27 months after transplantation and is the only AML patient who has survived with ETV6::NTRK3.
Conclusion
In conclusion, this study is a case of risk-taking but successful treatment of refractory leukemia and is the first time that a TRK inhibitor has been used for post-transplant maintenance therapy. Because of the low incidence of ETV6::NTRK3 in hematological malignancies, it is difficult to perform a large number of clinical studies to evaluate the efficacy and safety of TRK inhibitors. At present it can only be explored step by step through special cases.
Data Sharing Statement
All data related to the study are included in the paper.
Ethics Approval
This study was approved by the ethical committee of the Institute of Hematology and Blood Diseases Hospital, Chinese Academy of Medical Sciences.
Informed Consent Statement
Written informed consent has been obtained from the patient to publish this paper.
Acknowledgments
The authors are grateful to the patient for his participation.
Author Contributions
All authors contributed to proposing the treatment strategy, data analysis, drafting or revising the manuscript. All authors reviewed and agreed on the version of the article to be published, the journal to which the manuscript has been submitted, and agreed to be accountable for the contents of the article.
Funding
The authors received no specific funding for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Vaishnavi A, Le AT, Doebele RC. TRKing down an old oncogene in a new era of targeted therapy. Cancer Discovery. 2015;5(1):25–34. doi:10.1158/2159-8290.CD-14-0765
2. Joshi SK, Davare MA, Druker BJ, Tognon CE. Revisiting NTRKs as an emerging oncogene in hematological malignancies. Leukemia. 2019;33(11):2563–2574. doi:10.1038/s41375-019-0576-8
3. Cocco E, Scaltriti M, Drilon A. NTRK fusion-positive cancers and TRK inhibitor therapy. Nat Rev Clin Oncol. 2018;15(12):731–747. doi:10.1038/s41571-018-0113-0
4. Taylor J, Pavlick D, Yoshimi A, et al. Oncogenic TRK fusions are amenable to inhibition in hematologic malignancies. J Clin Investigation. 2018;128(9):3819–3825. doi:10.1172/JCI120787
5. Zhou F, Chen B. Acute myeloid leukemia carrying ETV6 mutations: biologic and clinical features. Hematology. 2018;23(9):608–612. doi:10.1080/10245332.2018.1482051
6. Drilon A, Laetsch TW, Kummar S, et al. Efficacy of Larotrectinib in TRK Fusion-Positive Cancers in Adults and Children. N Eng j Med. 2018;378(8):731–739. doi:10.1056/NEJMoa1714448
7. Doebele RC, Drilon A, Paz-Ares L, et al. Entrectinib in patients with advanced or metastatic NTRK fusion-positive solid tumours: integrated analysis of three Phase 1-2 trials. Lancet Oncol. 2020;21(2):271–282. doi:10.1016/S1470-2045(19)30691-6
8. Roberts KG, Janke LJ, Zhao Y, et al. ETV6-NTRK3 induces aggressive acute lymphoblastic leukemia highly sensitive to selective TRK inhibition. Blood. 2018;132(8):861–865. doi:10.1182/blood-2018-05-849554
9. Chen S, Zhang X, Zhai W, et al. P1390: the efficacy and safety of modified melphalan and busulfan-based regimen for allogeneic transplantation in refractory/relapsed AML patients. HemaSphere. 2022;6:1274–1275. doi:10.1097/01.HS9.0000848420.57492.c3
10. Pasvolsky O, Shimony S, Yeshurun M, et al. Maintenance therapy after allogeneic hematopoietic transplant for acute myeloid leukemia: a systematic review and meta-analysis. Acta oncologica. 2021;60(10):1335–1341. doi:10.1080/0284186X.2021.1955969
11. Rautenberg C, Germing U, Haas R, Kobbe G, Schroeder T. Relapse of Acute Myeloid Leukemia after Allogeneic Stem Cell Transplantation: prevention, Detection, and Treatment. Int J Mol Sci. 2019;20(1):228. doi:10.3390/ijms20010228
12. Setoyama M, Tojo A, Nagamura F, et al. A unique translocation of the TEL gene in a case of acute myelogenous leukemia with inv(12)(p13q15). Blood. 1998;92(4):1454–1455. doi:10.1182/blood.V92.4.1454
13. Kralik JM, Kranewitter W, Boesmueller H, et al. Characterization of a newly identified ETV6-NTRK3 fusion transcript in acute myeloid leukemia. Diagn. Pathol. 2011;6(1):19. doi:10.1186/1746-1596-6-19
14. Smith KM, Fagan PC, Pomari E, et al. Antitumor Activity of Entrectinib, a Pan-TRK, ROS1, and ALK Inhibitor, in ETV6-NTRK3-Positive Acute Myeloid Leukemia. Mol Cancer Therapeutics. 2018;17(2):455–463. doi:10.1158/1535-7163.MCT-17-0419
15. Frampton JE. Entrectinib: a Review in NTRK+ Solid Tumours and ROS1+ NSCLC. Drugs. 2021;81(6):697–708. doi:10.1007/s40265-021-01503-3
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.