")
Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 15
Physicians’ Examination and Referral Practices on Orthodontic Problems Among 6–12-Year-Old Children in Saudi Arabia
Authors Alrejaye NS , Alnasser LA, Alsuliman AF, Alomran DK , Alshehri HH, Almalki MM, Alenazi SS, Bushnak IA, Abolfotouh MA
Received 11 September 2023
Accepted for publication 11 October 2023
Published 20 October 2023 Volume 2023:15 Pages 225—236
DOI https://doi.org/10.2147/CCIDE.S438306
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Christopher E. Okunseri
Najla S Alrejaye,1– 3 Lubna A Alnasser,2 Abdalaziz F Alsuliman,4 Dema Khalid Alomran,4 Hanan H Alshehri,3 Maram M Almalki,3 Suha S Alenazi,3 Ibraheem A Bushnak,2 Mostafa A Abolfotouh2
1Dental Health Services, King Abdulaziz Medical City/Ministry of National Guard Health Affairs, Riyadh, 11426, Saudi Arabia; 2King Abdullah International Medical Research Center/ King Saud bin Abdulaziz University for Health Sciences/ Ministry of National Guard Health Affairs, Riyadh, 14611, Saudi Arabia; 3College of Dentistry/ King Saud bin Abdulaziz University for Health Sciences/ Ministry of National Guard Health Affairs, Riyadh, 11426, Saudi Arabia; 4College of Dentistry/ King Saud University, Riyadh, 11451, Saudi Arabia
Correspondence: Mostafa A Abolfotouh, King Abdullah International Medical Research Center/King Saud bin Abdulaziz University for Health Sciences/Ministry of National Guard Health Affairs, POB 22490, Riyadh, 11426, Saudi Arabia, Email [email protected]
Background: Physicians are more likely to examine children than dentists; thus, they may have a significant role in detecting oral and dentofacial problems. This study aimed to determine the rate and comprehensiveness of examinations, the rate and quality of referral practices, and the predictors of referral practice of physicians regarding orthodontic problems among children.
Methods: In a multi-center cross-sectional study, a total of 518 physicians in Saudi Arabia were subjected to an e-questionnaire of four sections: (1) Physicians’ demographic and work-related characteristics; (2) Physicians’ comprehensiveness of oral and orthodontic examinations; (3) Physicians’ referral practices to orthodontists and reasons considered for referral; and (4) Physicians’ sources of orthodontic education. Logistic regression analysis was applied to identify the significant predictors of referral practice. The significance was set at p < 0.05.
Results: Most physicians reported partial oral (78.5%) and orthodontic (72.2%) examinations, while the full examination was reported by only 12% and 2.5% of physicians, respectively. Referral to orthodontists was practiced by most of the physicians (83.8%), yet for the majority of them, the quality of referral was poor (40.3%) or fair (46.1%), with only 13.6% who practiced quality referral. Dental development issues (53.3%) and functional issues (51.5%) were reported as the main reasons for referral, followed by family/patient request (42.9%), dental alignment (42.5%), oral respiratory issues (32.4%), and finally jaw relation (26.1%). Referral practice was predicted by the comprehensive oral (OR = 2.37, p = 0.007) and orthodontic (OR = 4.26, p < 0.001) examinations, number of patients seen by the physician (OR = 1.58, p = 0.007), and level of training (OR = 1.88, p = 0.03).
Conclusion: Although most physicians reported high rates of examination and referral practices on orthodontic problems among children in Saudi Arabia, only a small portion showed comprehensive examinations and quality referral practice. Including dental courses in medical curricula and improving oral and orthodontic examination guidelines for physicians are recommended.
Keywords: dentofacial, dental development, malocclusion, pediatrics, orthodontists, multidisciplinary
Introduction
Oral health is an integral part of a child’s overall health and may have significant effects on the general physical and/or mental health status. However, it has been shown that physicians’ awareness on oral and dental health is insufficient, and medical curricula have not dedicated the needed attention to oral health education.1 Physicians are usually more likely to examine children in early life; thus, they may have a significant role in detecting oral and dentofacial problems.2,3
Orthodontic problems are among the significant oral issues which could result from genetic and/or environmental factors. These problems may vary from affecting only the teeth (dental) to more severe conditions involving the face and/or jaws (skeletal). Oral habits such as non-nutritive sucking on a thumb, digit, or pacifier, and tongue thrusting may cause malocclusion such as protrusion of the maxillary incisors, increase in overjet, lip incompetence, and anterior open bite. Such maxillary incisors protrusion and overjet increase may increase the risk of dental trauma and thus infection besides affecting facial appearance and self-esteem.4 Orthodontic problems may impact the child’s quality of life, mental health, and psychosocial well-being.5–7 Such problems may significantly increase bullying among children.8
Orthodontic referral and timely treatment may favorably change a child’s life. Early or interceptive orthodontics may eliminate factors that impede the normal development of dental arches and/or jaws.9 In certain cases, management for dentofacial and/or orthodontic problems should begin early to reduce the case complexity later in life, increase treatment efficiency, and improve function (chewing and speech), esthetics, and psychosocial wellbeing.5,9 Orthodontic treatment does not only manage dental alignment but also improves oral function, esthetics, and overall dental health by enhancing jaw relations and facial orthopedics.3,10 Pediatric patients make up a significant portion of orthodontic patients. Therefore, interdisciplinary collaboration between pediatricians and orthodontists is essential.11
Several studies reported that pediatricians showed inadequate knowledge and referral practice regarding orthodontic problems in children.7,12–14 A recent study showed that although family physicians in Turkey had adequate orthodontic knowledge, their oral and maxillofacial evaluations were suboptimal during routine examinations.15
There is a scientific gap in the literature in Saudi Arabia regarding the physicians’ examination and referral practices on orthodontic problems in children. Thus, the aims of this study were; (1) to determine the rate and comprehensiveness of oral and orthodontic examinations, (2) to determine the rate and quality of referral practices, and (3) to identify the predictors of referral practice of physicians regarding orthodontic problems among children in Saudi Arabia.
Methods
Study Design
This is a national, multi-center, cross-sectional study.
Study Population and Sampling Technique
This study targeted primary care physicians (general practitioners, family physicians, and internists), pediatricians, and Ear, Nose, and Throat (ENT) specialists working in primary, secondary, or tertiary healthcare centers in Saudi Arabia. This study used convenience sampling and invited eligible participants through social media to participate in the survey. The sample of this study included internists because some healthcare facilities in Saudi Arabia have pediatric patients evaluated by internists too. Nonetheless, participants were eligible to participate only if they gave an affirmative answer to a screening question, “Do you examine pediatric patients (Age = 6–12 Years)?”. In other words, physicians who reported not examining pediatric patients with this specified age range were excluded.
As no previous data exist in Saudi Arabia, a prevalence of 50% of physicians performing oral clinical examination and referral practice on their pediatric patients was assumed, and a 95% confidence interval and 5% margin of error, the minimum sample size required was 378 participants. A non-probability convenience sampling technique was used. However, it was considered that all regions of the Kingdom were represented with all targeted specialties of physicians in such regions. Those who responded with valid completed questionnaires were 518 physicians (out of a total of 625 physicians).
Data Collection
An electronic, self-administered questionnaire was structured with inspiration from the survey developed by Koufatzidou et al.12 The questionnaire was composed of four main sections as follows: the first section included questions about physicians’ demographic characteristics and clinical experience. The second section was about oral examination protocol and the type of orthodontic conditions routinely screened; in this s ection, participants were asked if they examine the oral cavity (yes/no) of pediatric patients and if a participant gave an affirmative answer to this question, he/she was asked follow-up questions on which elements of the oral cavity (six elements) were examined and which orthodontic conditions (eight elements) they screen during their oral clinical examination.
Participants were instructed to choose all answers that apply. The levels of examination were categorized as; none, partial, and full examination. A brief description was included for the dental terminologies used and a photograph of the clinical presentation of orthodontic conditions to ensure that physicians did not misclassify conditions that they screened for because of their dental terminology. For example, the term crossbite was defined as “narrow upper jaw” and a clinical photograph of a crossbite was added. The third section inquired about reasons the physicians had considered for referral to an orthodontist. The quality of referral to orthodontics was assessed based on the number of reasons each physician considered for referral as follows: poor (1–2 reasons), fair (3–6 reasons), and good quality (7 or more reasons). The fourth section was about physicians’ sources of education about orthodontics and the role of orthodontists in treating malocclusion in children.
The data was collected between the 6th and 13th of August 2022 after receiving ethical approval from the Institutional Review Board (IRB) of the Ministry of National Guard Health Affairs (MNGHA), Riyadh, Saudi Arabia (Ref#. RSS22R/021/07). An electronic questionnaire was distributed to the targeted physicians. Participation was voluntary with informed written consent. The participants’ information was anonymously treated for their privacy and confidentiality, no identifiers were collected, and all data were kept in a secure place within Ministry of National Guard Health Affairs (MNGHA) premises. A pilot study was conducted on fifteen subjects to test the reliability and feasibility of the questionnaire. The questionnaire was assessed in terms of internal consistency. Cronbach’s alpha was computed, and a coefficient alpha of 0.81 was considered adequate. Test–retest reliability was also assessed using Cronbach’s alpha and Pearson’s correlation coefficient (r). Construct validity of the checklist was assessed using expert opinion, and the final version was approved after making the necessary modifications.
Statistical Analysis
SPSS software Ver. 27 was used for data entry and analysis. Descriptive analysis summarized the categorical variables using frequency and percentage distribution. The distribution of demographic and clinical characteristics of participants across the clinical specialties was compared, and the elements of the oral cavity and the orthodontic conditions that were examined by participants were summarized. To summarize the comprehensive list of reasons for referral to an orthodontist, the reasons were categorized into six broad categories based on the reason’s type and/or impact.
Pearson chi-square test and chi-square test for linear trend were used to test the association between referral practice and each possible independent variable. Odds ratios and corresponding 95% confidence intervals were calculated to assess the association between the practice of referral (yes or no) and each demographic and clinical characteristic of physicians. Logistic regression analysis was applied to identify the significant predictors of referral practice, with the following independent variables; sex, age in years, level of training (ordinal), specialty, years of experience, work sector (public versus others), working hours/week, number of patients/week, comprehensiveness of oral examination (ordinal), and comprehensiveness of orthodontic examination (ordinal). Significance was set at p < 0.05.
Results
A total of 518 (out of 625) physicians gave an affirmative answer about seeing pediatric patients, within the age range of 6 to 12 years, in their practices and thus were considered eligible to be included in the current study. Demographic and work-related characteristics are shown in Table 1. More than one-half of the participants (287, 55.4%) were males, and most of the sample were; between 26 and 35 years of age (399, 77%), general practitioners (224, 43.2%), working in public (governmental) healthcare facilities (435, 83.9%), and working between 26 and 50 hours per week (275, 53.1%).
 |
Table 1 Demographic and Clinical Characteristics of 518 Physicians |
Table 2 shows the responses of 518 physicians in relation to examination of the oral cavity elements and orthodontic conditions in pediatric patients. Regarding examination of oral cavity elements, most physicians (407, 78.5%) reported partial comprehensive examination (1–5 oral cavity elements), while only 12% (62) reported full comprehensive examination of the six oral cavity elements listed. Physicians more often reported examining the oral hygiene (74.9%) and oral soft tissues including the mucosa (68.5%) and tongue (67.0%) compared to teeth (27.6%) and jaws (24.7%) positions, which were less frequently examined. Looking at the examination of orthodontic conditions, most physicians (374, 72.2%) reported partial comprehensive examination (1–7 orthodontic conditions), while only 13 physicians (2.5%) reported full comprehensive examination of the eight orthodontic conditions listed. The two orthodontic conditions examined the most were missing teeth and oral habits (40.5% each).
 |
Table 2 Responses of 518 Physicians About Examination of the Oral Cavity Elements and Orthodontic Conditions in Pediatric Patients |
Physicians’ responses regarding reasons considered for referral to orthodontists showed remarkable variations (Table 3 and Figure 1). Dental development issues, which included early tooth loss, delayed teeth eruption or change, and missing teeth, were reported by 53.3% of the physicians as the main reason for referral. Similarly, functional issues, which included jaw deviation, temporomandibular joint (TMJ) sounds, biting difficulty, and sleep grinding, were considered as the second most frequent reason for referral by almost half of the physicians (267, 51.5%). However, jaw relation issues which included prognathism, retrognathism, and facial asymmetry were considered for referral by only 135 (26%) of the physicians. Mouth breathing, snoring, and obstructive sleep apnea were categorized as respiratory issues and were considered by about one-third (32%, 168) of the physicians. Regarding the issues related to dental alignment: crowding, spacing, open bite, deep bite, and crossbite, 42.5% (220) of the participants considered it as a reason for referral to an orthodontist; referral upon patient or family request showed a similar frequency (42.9%, 222). Referral to orthodontists was practiced by most of the physicians (83.8%), yet for the majority of them, the quality of referral was poor (40.3%) or fair (46.1%), with only 13.6% practicing good quality referral.
 |
Table 3 Reasons Considered for Orthodontic Referral by 518 Physicians |
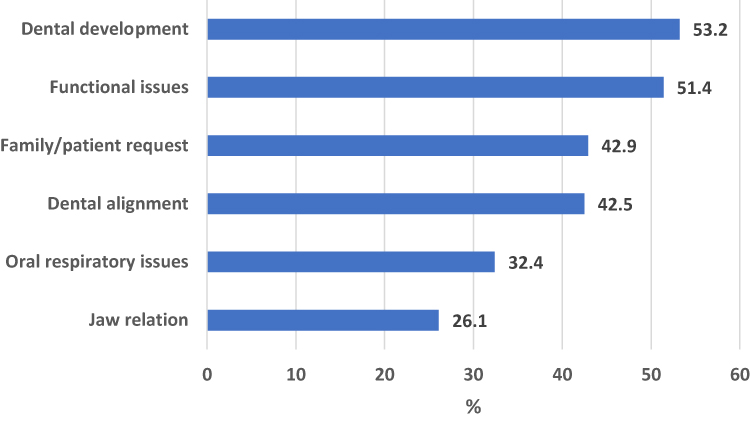 |
Figure 1 Reasons to consider for orthodontic referral as reported by the physicians. |
Table 4 shows the rate of orthodontic referral practice by physicians according to some demographic and work-related characteristics. The bivariate analyses showed a statistically significant association between referral practice and level of training, work sector, and number of patients seen per week (P < 0.05 each). More specifically, specialists had significantly higher odds of considering referral compared to general practitioners (OR = 2.17, p = 0.015). Moreover, physicians working in the private sector besides their work in public institutions were more than four times more likely to consider orthodontic referral compared to those working in public institutions only (OR = 4.48, p = 0.026). Also, more than a two-fold increase was detected in the odds for considering referral for those who see more than 20 patients per week (OR = 2.44, p = 0.025) and more than 30 patients (OR = 2.84, p = 0.048) compared to those who see only 1–10 patients weekly.
 |
Table 4 Prevalence of Orthodontic Referral by Physicians According to Some Characteristics |
Figure 2 shows the association between the levels of oral and orthodontic examinations and the practice of referral to orthodontists by physicians. As the levels of comprehensiveness of oral examination rise, there is a significant rise in the rate of referral (Chi-square for linear trend = 26.84, p < 0.001). Likewise, physicians who carry out a more comprehensive orthodontic examination showed a significantly higher rate of referral to an orthodontist (Chi-square for linear trend = 45.27, p < 001). After adjusting for all possible confounders using logistic regression analysis in Table 5, this association between the levels of comprehensiveness of oral (OR = 2.37, p = 0.007) and orthodontic (OR = 4.26, p < 0.001) examinations remained significant. Other significant predictors of referral practice to orthodontists were the number of patients seen by the physician (OR = 1.59, p = 0.006), and the level of training (OR = 1.88, p = 0.030).
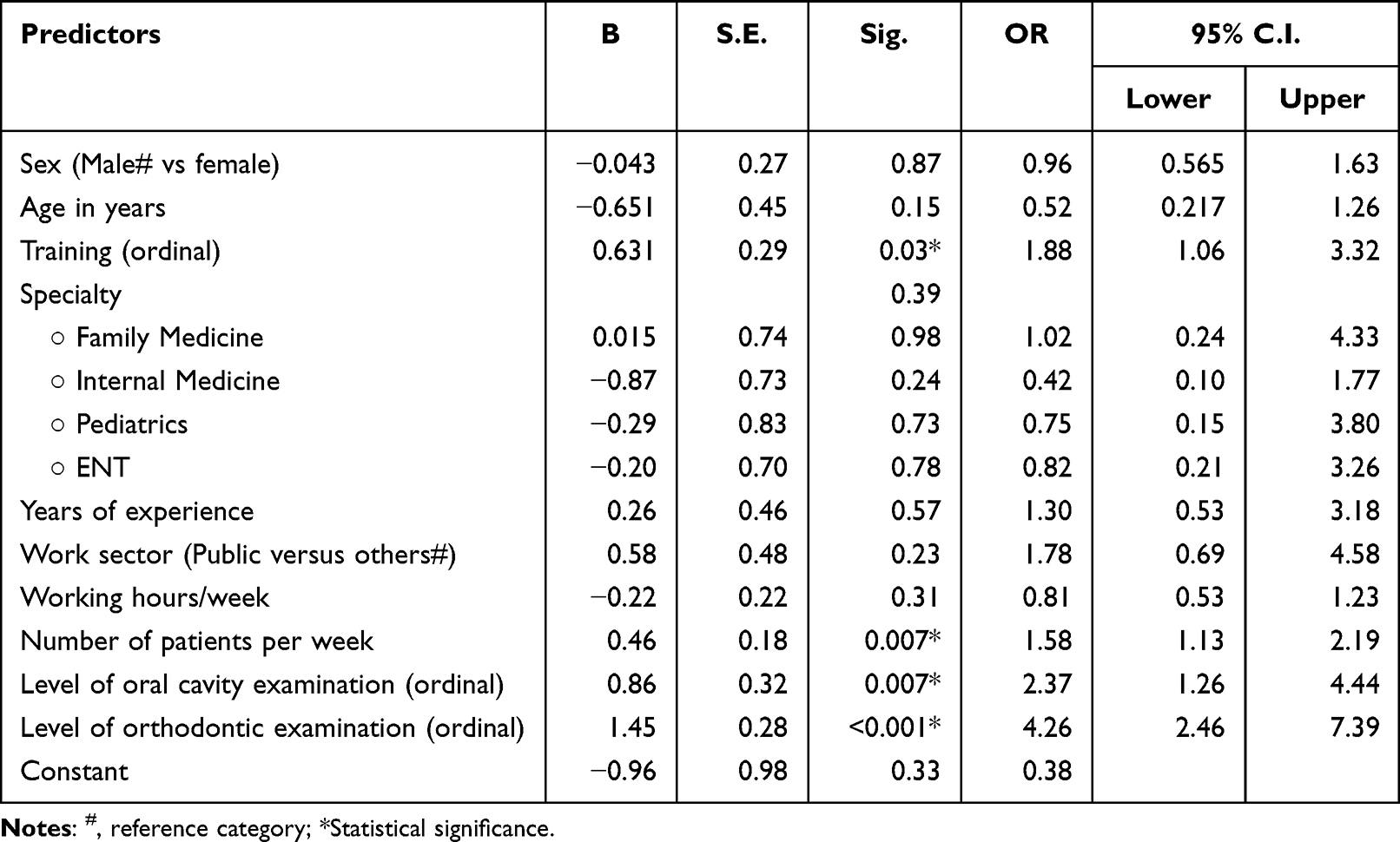 |
Table 5 Predictors of Orthodontic Referral by Physicians |
 |
Figure 2 Association between the comprehensiveness of oral /orthodontic examinations and the rate of referral. |
Figure 3 shows the main source of orthodontic education reported by 518 physicians. Less than half (47%) of physicians reported that the general medical degree was a main source for their orthodontic background.
 |
Figure 3 The main source of orthodontic education reported by 518 physicians. |
Discussion
The results of this study indicate that there was a great variability among physicians regarding the examination and referral practices on orthodontic problems among children in Saudi Arabia, with an overall lack of comprehensive examinations, and low quality of referral practice. Although previous studies reported that pediatricians showed inadequate knowledge and referral practice regarding orthodontic problems in children,7,12–14 there is a scientific gap in the literature in the region of Saudi Arabia regarding this issue. The results of a significant variability in oral and orthodontic examinations considered by physicians are in agreement with previous similar studies.12,14 It was more meaningful to look at the result more critically in this study rather than withdrawing generalized conclusions. Therefore, the level of comprehensiveness of examination was determined for each: oral cavity elements and orthodontic conditions (none, partial, or full) as shown in Table 2. A significant proportion of the physicians reported that they do not perform an examination of the oral cavity or orthodontic conditions on a usual basis, 9.5% and 25.3%; respectively. These findings are similar to those reported by Maden and Eker who found that 28.9% of pediatricians in Turkey did not perform an oral examination for malocclusion.7 Also, 17% of pediatricians in Gujarat, India, reported that they do not examine the oral cavity in another study.14 Maden and Eker7 reported that although a majority of the pediatricians did not have the pertinent knowledge and practice to perform complete oral and orthodontic examinations, they were aware that pediatricians have an important role in the prevention of parafunctional oral habits and orthodontic problems. This is in accordance with the present finding of the low percentage of physicians who reported full examination of oral or orthodontic conditions, 12% and 2.5%, respectively.
Looking at oral cavity element examination, physicians more often reported examining the oral hygiene and oral soft tissues including the mucosa and tongue compared to teeth and jaw positions, which were less frequently examined. Similar findings were reported in the previous surveys done in India and Greece.12,14 Also, Buyuk et al15 showed that family physicians in Turkey reported higher rate of oral cavity evaluation during routine examination (59.25%) compared to teeth (36.75%) and jaw (30.75%) positions.
Less than one-half of the physicians in this study (40.5%) reported that they conduct examination for parafunctional oral habits on a usual basis such as finger sucking, pen biting, lip trap, tongue thrust, and so on. Similarly, 43.4% of pediatricians in Turkey reported they evaluate their patients for oral habits, while 88% of pediatricians in India and 95% of pediatricians in Greece reported they actually do.7,12,14 It is worth mentioning that the design of these previous studies targeted pediatricians only and had smaller sample sizes compared to the present study.
The interesting finding after analyzing the referral reasons was that the high rate of referral to an orthodontist was 83.8% considering at least one reason for referral, yet less than 2% of physicians reported referral to an orthodontist for 7 or more reasons (quality referral) and 16.2% reported no referral at all for any of the listed reasons (poor quality). This may enlighten the fact that a significant percentage of physicians underestimates the importance of orthodontics to help with obtaining optimal oral and general health in children. The literature presented the significant role of dentists especially orthodontists dealing with the consequences of respiratory issues such as mouth breathing, snoring, and obstructive sleep apnea;16 however, only 32.4% of physicians reported considering respiratory issues for orthodontic referral in the present study and only 24% of pediatricians in Greece reported referral for mouth breathing or snoring.12 Jaw relation issues which included prognathism, retrognathism, and facial asymmetry as reasons for referral to an orthodontist were considered by only 26% of the physicians in the present study; however, it was more frequently reported (>50%) in the previous surveys done in India and Greece.12,14
A remarkable finding was the significant positive association between the level of comprehensiveness of oral and orthodontic examinations and the rate of referral practice (Figure 2). As the level of comprehensiveness of examination increases, the rate of pediatric patient referral to an orthodontist increases significantly, meaning that, physicians who carry out a more comprehensive examination showed significantly higher quality of referral to an orthodontist, which may help with more effective interdisciplinary management. Other significant predictors of referral practice to orthodontists were the number of patients seen by the physician (OR = 1.58, p = 0.007) and the level of training (OR = 1.88, p = 0.03). These predictors imply that higher training and experience may enhance orthodontic referral and interdisciplinary care. Therefore, shedding light on the importance of improving physicians’ knowledge and awareness. Buyuk et al15 also reported in a recent study that family physicians with an experience of more than five years had an increase in referral rate to orthodontists by 17%.
It was interesting that “family members” was selected as the second main source of physicians’ orthodontic knowledge (16%) following the general medical degree, which was selected by 47% of physicians. This may illuminate the fact of lack of adequate education in this area during medical training. Maxey et al17 showed that providing adequate training to primary care physicians helped to expand their roles in integrated healthcare delivery models through better identification of oral health issues.
Limitations
The results of this study are credible and new for this geographic area, showed relatively reasonable and significant results, and provide advances in this field. However, it has some limitations. Since the study relied upon a self-reported questionnaire, its results are liable to recall bias, as some of the physicians may have responded more favorably regarding their examination and referral practices to appear more comprehensive than their actual practice. Also, the study is subjected to non-responder’s bias, as some of the non-responders might have had different answers than those of the responders and this might have had an implication for the generalizability of the study findings. The cause-and-effect relationship between the predictors of orthodontic referral (as an exposure) and the levels of oral cavity and orthodontic conditions (as an outcome), because of its cross-sectional design. Moreover, study results may not truly represent the entire population of the study region, and its generalization may suffer from reporting bias. Lastly, since the survey was conducted via the internet, it could result in selection bias, especially that the sample was over-representative of well-educated people and those who have internet access.
Conclusion
- The results of this study indicate that there was a great variability among physicians regarding the examination and referral practices on orthodontic problems among children in Saudi Arabia, with an overall lack of comprehensive examinations.
- Although most physicians reported high rates of examination and referral practices on orthodontic problems among children in Saudi Arabia, only a small portion showed comprehensive examinations and quality referral practice.
- Physicians with more comprehensive oral and orthodontic examination showed significantly higher quality of referral.
- The inclusion of dental courses in medical curricula and an improvement of oral and orthodontic examination guidelines for physicians are recommended to establish more effective and holistic management of pediatric patients.
Abbreviations
KAMC King Abdulaziz Medical city; MNGHA Ministry of National Guard-Health Affairs; KAIMRC King Abdullah International Medical Research Center; IRB Institutional Review Board.
Data Sharing Statement
Most of the data supporting our findings is contained within the manuscript, and all others, excluding identifying/confidential data, will be shared upon request from the corresponding author [[email protected]].
Ethics Approval and Consent to Participate
Participation in this study was voluntary. Participants were assured in a written informed consent that their responses would remain anonymous. They were asked to respond to the survey if they agreed to the informed consent. The study protocol was approved by the Institutional Review Board (IRB) of the Ministry of National Guard-Health Affairs (MNGHA), Riyadh, Saudi Arabia (Ref. # RSS22R/021/07). This study was conducted in accordance with the Declaration of Helsinki.
Acknowledgment
This study was initiated by King Abdullah International Medical Research Center, and King Saud bin-Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia. The study was one of the research projects of the 13th Research Summer School program conducted during July–August 2022, under the full supervision of the KAIMRC staff. All individuals included in this section have consented to the acknowledgement. The abstract of this paper was presented at the 7th Health Professions Conference, King Saud bin Abdulaziz University for Health Sciences, as a poster presentation with interim findings on December 25, 2022.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Krol DM. Children’s oral health and the role of the pediatrician. Curr Opin Pediatr. 2010;22(6):804.
2. Nirschl RF, Kronmiller JE. Evaluating oral health needs in preschool children. Clin Pediatr (Phila). 1986;25(7):358–362. doi:10.1177/000992288602500705
3. Quinonez RB, Kranz AM, Lewis CW, et al. Oral health opinions and practices of pediatricians: updated results from a national survey. Acad Pediatr. 2014;14(6):616–623. doi:10.1016/j.acap.2014.07.001
4. Wagner Y, Heinrich-Weltzien R. Occlusal characteristics in 3-year-old children--results of a birth cohort study. BMC Oral Health. 2015;15(1):94. doi:10.1186/s12903-015-0080-0
5. Roberts-Harry D, Sandy J. Orthodontics. Part 1: who needs orthodontics? Br Dent J. 2003;195(8):433. doi:10.1038/sj.bdj.4810592
6. Abanto J, Carvalho TS, Mendes FM, Wanderley MT, Bönecker M, Raggio DP. Impact of oral diseases and disorders on oral health-related quality of life of preschool children. Community Dent Oral Epidemiol. 2011;39(2):105–114. doi:10.1111/j.1600-0528.2010.00580.x
7. Arat Maden E, Eker I. Pediatricians’ Knowledges, Attitudes, and Practices on Parafunctional Oral Habits and Orthodontic Problems in Children. Clin Exp Health Sci. 2021;11(4):834–841. doi:10.33808/clinexphealthsci.971473
8. Shaw WC, Meek SC, Jones DS. Nicknames, teasing, harassment and the salience of dental features among school children. Br J Orthod. 1980;7(2):75–80. doi:10.1179/bjo.7.2.75
9. Tausche E, Luck O, Harzer W. Prevalence of malocclusions in the early mixed dentition and orthodontic treatment need. Eur J Orthod. 2004;26(3):237–244. doi:10.1093/ejo/26.3.237
10. Adegbite K, Ogunbanjo B, Ajisafe O, Adeniyi A. Knowledge of Orthodontics as a Dental Specialty: a Preliminary Survey among LASUCOM Students. Ann Med Health Sci Res. 2012;2(1):14–18. doi:10.4103/2141-9248.96930
11. Moorrees CF, Sisson WR, Peckos PS, Christie RG, Baldwin DC. Need for collaboration of pediatrician and orthodontist. Pediatrics. 1962;29(1):142–147. doi:10.1542/peds.29.1.142
12. Koufatzidou M, Koletsi D, Basdeki EI, Pandis N, Polychronopoulou A. Pediatricians’ awareness on orthodontic problems and related conditions-a national survey. Prog Orthod. 2019;20(1):33. doi:10.1186/s40510-019-0285-x
13. Sharma R, Kumar S, Singla A, Kumar D, Chowdhary S. Knowledge, attitude and practices of pediatricians regarding malocclusion in Haryana, India. J Indian Assoc Public Health Dent. 2016;14(2):197. doi:10.4103/2319-5932.183803
14. Thakkar D, Kubavat A, Bachwani R. Awareness on Orthodontic Problems and Referral among Pediatricians in Gujarat, India. Glob J Res Anal. 2020;9(8):54–56.
15. Kutalmış Buyuk S, Abay F, Yıldırım OU, Enginyurt O. Analysis of family physicians’ awareness and knowledge about orthodontic treatment. Iran J Orthod. 2023;18(1):1–7. doi:10.22034/IJO.2023.1989021.1102
16. Behrents RG, Shelgikar AV, Conley RS, et al. Obstructive sleep apnea and orthodontics: an American Association of Orthodontists White Paper. Am J Orthod Dentofac Orthop off Publ Am Assoc Orthod Its Const Soc Am Board Orthod. 2019;156(1):13–28.e1. doi:10.1016/j.ajodo.2019.04.009
17. Maxey HL, Norwood CW, Weaver DL. Primary Care Physician Roles in Health Centers with Oral Health Care Units. J Am Board Fam Med JABFM. 2017;30(4):491–504. doi:10.3122/jabfm.2017.04.170106
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.