")
Back to Journals » Journal of Healthcare Leadership » Volume 16
Physician Leadership and Burnout: The Need for Agency; a Qualitative Study of an Academic Institution
Authors Hu JS , Pangaro LN, Gloria Andrada BM, Ceasar RC, Phillips JL
Received 16 November 2023
Accepted for publication 18 February 2024
Published 1 March 2024 Volume 2024:16 Pages 121—130
DOI https://doi.org/10.2147/JHL.S419203
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Zhanming Liang
James S Hu,1 Louis N Pangaro,2 Bami M Gloria Andrada,3 Rachel C Ceasar,4 Jennifer L Phillips5
1Department of Medicine – MD, EdD, Keck School of Medicine of USC, Los Angeles, CA, USA; 2Department of Medicine – MD, F. Edward Hébert School of Medicine of the Uniformed Services University of the Health Sciences, Bethesda, MD, USA; 3Department of Medicine – MS, Keck School of Medicine of USC, Los Angeles, CA, USA; 4Department of Population and Public Health Sciences, University of Southern California, Los Angeles, CA, USA; 5USC Rossier School of Education – DLS, University of Southern California, Los Angeles, CA, USA
Correspondence: James S Hu, Department of Medicine, University of Southern California, 1441 Eastlake Ave, NTT 3440, Los Angeles, CA, USA, Email [email protected]
Purpose: Organizational approaches to physician burnout are limited. Training physician leaders to influence the organizational environment is a growing area of study. This study explored perceived physician leadership behaviors in response to burnout from the viewpoint of faculty physicians not in formal leadership positions. Understanding physician leadership behaviors from the viewpoint of those faculty being led can inform organizational strategy and leadership training to address physician burnout.
Subjects and Methods: Interview requests were sent to 70 randomly identified faculty physicians from a roster containing all 1145 physician faculty that excluded the Pediatric Department, at an academic health care institution in Southern California. The first ten respondents were asked to participate in a 30-to-40-minute semi-structured virtual interview via Zoom. The interviewees were asked two questions pertaining to burnout and their perception of how leadership responded. The two questions were “What has leadership done to address burnout?” and “If you had five minutes to advise your leaders on burnout, what would you say?” The recorded interviews were transcribed, redacted, and then sent to two reviewers. Thematic analysis through iterative coding was completed, and categories were constructed that aligned with the two interview questions.
Results: Overall, five themes were identified. These themes were organized according to the interview questions and broadly categorized as physician leadership behaviors observed that corresponded to the interview question of what leadership had done to address burnout and physician leadership behaviors desired corresponding to the second interview question of what advice should be given. Leadership behaviors observed in the context of burnout included three themes; referral to individual wellness programs, increased number of meetings and events, and a lack of agency in addressing wellness issues. The two themes of leadership behaviors desired were the obtainment of more resources and the granting of greater appreciation and recognition for work done through enhanced communication.
Conclusion: This small study of faculty physician perceptions of leadership behaviors identified several themes that had been identified in previous studies of leadership and burnout; need for relationship building through communication, need for resources to address work issues, and referral to wellness programs. However, the identification of a lack of agency in addressing factors in the wellness environment has not been identified in the previous burnout and physician leadership literature. Further study into the causes of this perceived lack of agency should be explored. Understanding the root causes of physician leaders’ lack of agency can further inform physician leadership education as an organizational approach to burnout.
Keywords: physician, leadership, qualitative, health care, burnout
Introduction
A general review of reported factors and sources of physician burnout reveals a complex mix of issues that range from problems with patient care delivery and resources, relationships with colleagues and leaders, and individual resiliency.1,2 Burnout can be viewed as a diminished state of wellness that is characterized by emotional exhaustion, depersonalization, and lack of accomplishment.3 Burnout is considered an emotional state that develops chronically over time in response to work-related issues and is distinguishable from depression, as the latter can also result from non-work-related factors, such as a poor home life. Job dissatisfaction, similarly, though correlated with burnout, may not have the components of emotional exhaustion, depersonalization, or lack of accomplishment.4 Therefore, burnout can be viewed as a distinct work-related condition that is a component of wellness but is distinct from other measures of wellness including job dissatisfaction, depression, and disengagement. Admittedly, the conceptual and operational understanding of wellness is not well delineated and can often include elements of mental, social, physical, and integrated aspects such as meaning in work in its understanding.5 Despite this ambiguity, measurements of burnout predominate in the physician wellness literature and are often a significant component of many health care wellness studies.
The consequences of physician burnout include increased physician turnover, poor patient care, diminished personal health, higher medical error rates, compromised patient safety, and increased cost to organizations and the general health care system.6,7 Therefore, effective interventions into burnout and wellness have been sought and are divided into individual-based approaches (ie, wellness programs) and organizational approaches (ie, work hour limitations).8 Extant organizational approaches toward improving physician wellness that include support for individual wellness programs, enhancing feelings of belonging in the workplace through values alignment and social events, and procuring needed resources to allow for efficient and effective health care delivery, may not be adequate to optimally address the physician burnout epidemic.8–10 Adaptive solutions to complex problems such as physician burnout will require a combination of these approaches from physician leadership including change initiatives aimed at the wellness environment. Physician leadership influence on the work environment, therefore, is a vital component of organizational strategies geared toward improving physician burnout and wellness.
Physician leadership behaviors demonstrate a strong correlation with wellness and burnout in those physicians being led9,11,12 Most of the literature on effective physician leadership behaviors that lead to improved wellness focus on the leadership category of relationship building.10 Relationship building may not be the only category of leadership behavior that is important for wellness; leadership change behaviors in obtaining resources or optimizing processes and task accomplishment may also be important.13,14 Relationship-based behaviors that attend to the growth and concerns of individuals, individual and organizational values alignment, and engagement of faculty in decision-making have been extensively studied and represent the predominant components of the relational category of physician leadership that correlate with wellness. However, non-relational leadership behaviors, including task accomplishment or change management, have neither been extensively studied nor identified in the context of burnout or wellness.
The current study aimed to delve deeper into perceived physician leadership behaviors by faculty physicians using in-depth interviews. Since many previous studies were quantitative in nature, the goal of these interviews was to gain a deeper understanding of physician faculty’s perception of physician leadership behaviors so that meaningful interventions by leaders to reduce burnout among their physician faculty could be better informed. Since an abundance of studies has already shown that leadership behaviors centered mostly around relationship building correlate with burnout in those being led, our study sought to explore how faculty understood other leadership behaviors in the context of burnout at an academic institution.
Methods
Between April 2021 and May 2021, all faculty physician names at this Southern California institution who practiced within the University hospital system were placed on a numbered spread sheet. The Pediatric Department was excluded as the Pediatric faculty primarily practiced at institutions outside of this Southern California institution but do have appointments within the school of medicine. Seventy faculty members from this list of the remaining 1145 names of physicians working in the hospital system were randomly identified and sent an email invitation. The numbers that corresponded to the names on the consecutively numbered list were randomly produced from an online number generator. An email request was sent to these 70 faculty members, who were given the email address of the independent interviewer. The first ten faculty respondents who were not formal physician leaders at the Chief or Chair levels of authority were offered the opportunity to participate in a 30–40-minute interview. Experiencing burnout, either self-reported or assessed through an instrument, was not a criterion for interviewee participation.
The identities of the ten participants who accepted the invitation to participate were not revealed to the transcript reviewers. The interviews were captured on Zoom videoconferencing platform (Zoom Video Communications Inc., 2020), and the recordings were stored separately in a secure platform space that was not accessible to the reviewers.
The research question: “How do faculty physicians understand and perceive their physician leader’s response to burnout?” was explored using semi-structured interviews. The two interview questions that corresponded to the research question and follow-up questions were designed to help elucidate how faculty understand their physician leader’s response to burnout. Therefore, the following interview questions were designed to explore faculty’s understanding of what leadership behaviors were observed by faculty physicians and what behaviors were desired by faculty physicians in the context of burnout. The specific interview questions were as follows:
• “What has leadership done to address burnout?”
• “If you had five minutes to advise your leaders on burnout, what would you say?”
These interview questions were delivered and conducted by an independent interviewer trained in qualitative research who was not affiliated with the institution being studied. The follow-up questions to the interview questions were left to the interviewer’s discretion with clarification that the immediate supervising physician leader was the subject of the interview questions. The interviewer was instructed to redact the transcript for any identifying information and to deliver the redacted transcript to two reviewers for thematic analysis.
Thematic analysis was used in this study. Analyzing qualitative data typically involves coding the data and identifying themes that help to answer research questions. An “in vivo” coding approach, which is an inductive process that draws emergent or open coding from within the data or literature, was used in this study.15 The transcripts were reviewed independently by two researchers using the Atlas TI coding scheme following an inductive iterative method within the context of the research question.16 After codes were identified, these codes were categorized within the context of the research question, and themes were developed. Frequency of themes was reported only after coding and themes were generated (Tables 1 and 2). This study was approved by the Institutional Review Board at the University of Southern California and the participants provided written informed consent for publication of their responses (Study # UP-20-01358).
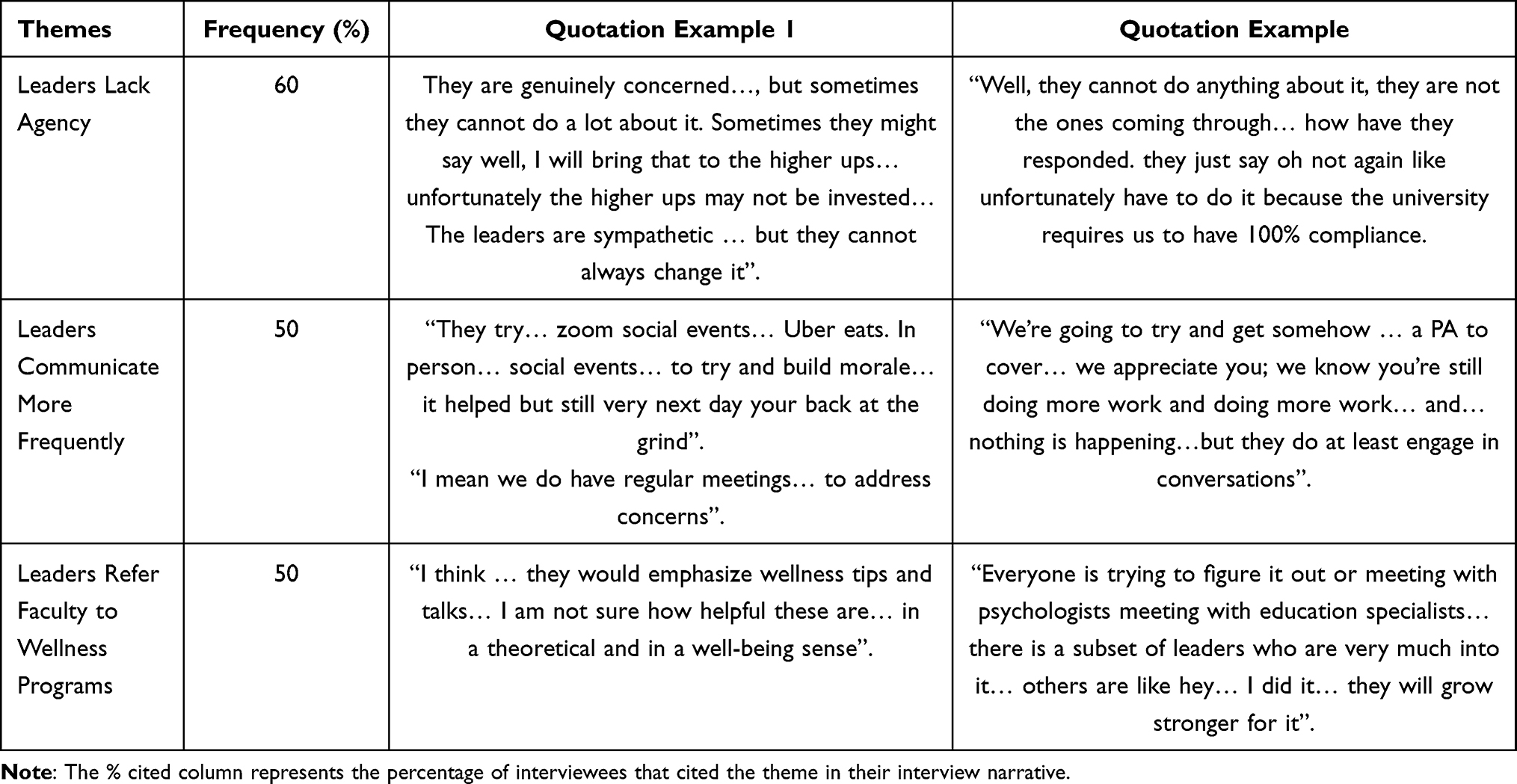 |
Table 1 Perceived Leadership Behaviors Observed in Response to Faculty Burnout (N = 10) |
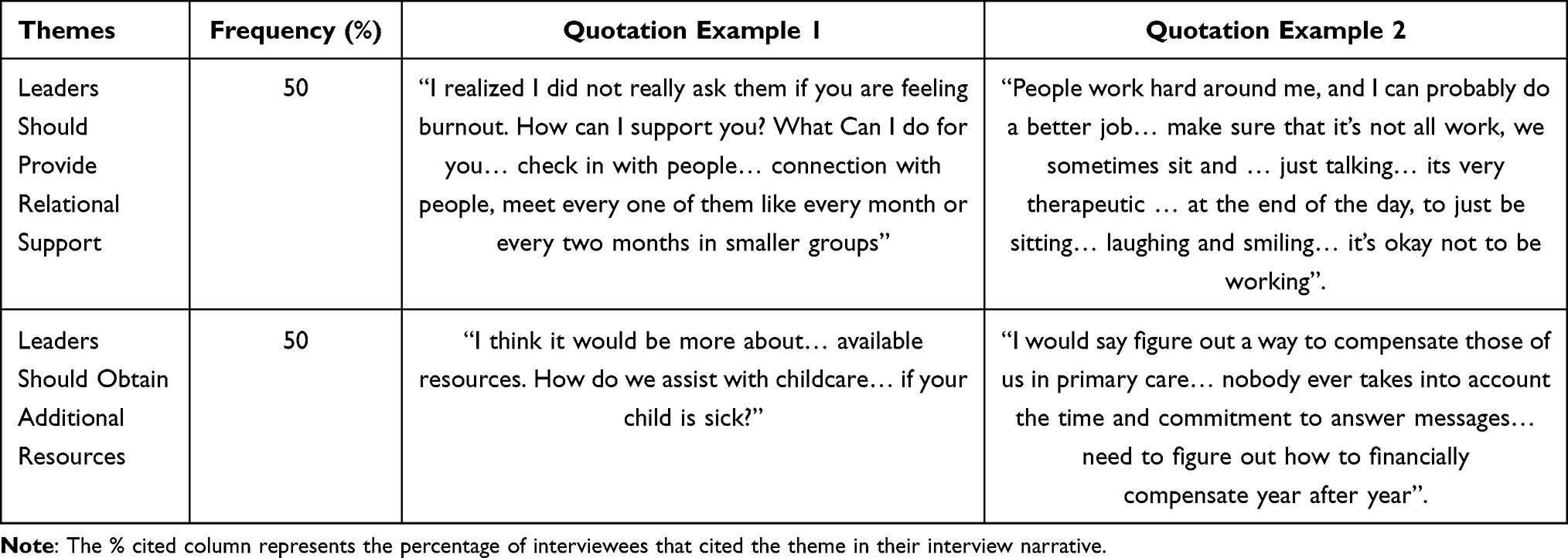 |
Table 2 Leadership Goals and Behaviors Desired by Faculty in Response to Burnout (N = 10) |
Results
Five themes were generated from the interview transcripts that addressed the research question and aligned with the two interview questions. Codes were organized around the interview questions, and themes were generated from these codes (Appendix 1). Three themes aligned with interview question number one, and two themes aligned with interview question number two and were labeled as leadership behaviors observed and leadership behaviors desired, respectively. Each theme was presented with representative quotations with narrative context.
Leadership Behaviors Observed
Our faculty’s understanding of their physician leaders’ behavior in the context of faculty burnout converged on themes directed at attempts to enhance communication, referral to existing wellness programs, or a complete lack of agency in affecting the work environment.
Leaders Lack Agency
One description of physician leadership behaviors identified in response to burnout reflected the idea that leaders lack agency, described also as an inability or unwillingness, to address the pressing factors that led to burnout. Interviewee number 4, for example, in discussing items such as patient scheduling flexibility described how leaders demonstrate genuine concern, but “sometimes they can’t do a lot about it” (Table 1). Similarly, interviewee number 7 cited an instance when additional on-line compliance training was required in addition to greater administrative work activities and lamented “well they can’t do anything about it, they are not the ones coming through” (Table 1). These two examples demonstrate a perception of a lack of agency as a leadership behavior in dealing with common burnout factors, including flexibility in scheduling and extraneous work, implying that either their physician leaders do not have the decision-making authority (power) to make decisions or, if they do, are unwilling to address these factors leading to burnout. Interviewee number 3 discussed how leadership “engages in meetings and conversations” and “might say well I will bring that up to the higher up’s and we’ll see what we can do”, however “they can’t always change it”. This latter interviewee appreciated the advocacy in addressing burnout that was related to altering the clinic schedule but did not perceive any appreciable effects of change.
Leaders Communicate More Frequently
Communication, both through individual and group meetings, emerged as a common leadership behavior demonstrated by physician leaders. Several participants indicated their leaders would host regular meetings where they would try to address concerns raised by faculty. Some of the participants acknowledged that though their leaders seem to care or have empathy, there are issues that “are going to be impossible to address” (Interviewee number 2) and that leaders see an issue “but they can’t always change it” (Interviewee number 3). Communication was also demonstrated by leaders through the hosting of more social events according to interviewee number 8 “I think they try… zoom social events… Uber eats” (Table 1).
Overall, most of the faculty acknowledged an appreciation of gestures to conduct more group and individual meetings. These leadership behaviors were felt to inspire motivation among the participants due to their respective leader’s genuine concern for their welfare. These behaviors were welcomed by the participants who identified them as “present”. Additionally, these behaviors are distinguishable from the lack of agency discussed by other participants, where most of the reactions were negative when a lack of agency was described.
Leaders Refer Faculty to Wellness Programs
When describing other leadership behaviors demonstrated by physician leaders in response to burnout, the interviewees described referrals or suggestions for participation in wellness programs. Many of the interviewees identified that their leadership would either individually or collectively encourage participation in wellness programs both as a prevention or therapeutic intervention.
Others describe referrals to wellness programs in a more general sense where the upper leadership made wellness programs available to the faculty. In a comment about the usefulness and availability of these programs, interviewee number 9 discussed how on a group and organizational level, communications with regard to wellness were readily available when they mentioned how “overall as an institution I do see our institution trying to create a better environment for people to prevent burnout”. They continued to state that these resources were useful. Others were more skeptical of the value of wellness programs, “I think … they would emphasize wellness tips and talks … I am not sure how helpful these are … in a theoretical and in a well-being sense” (Table 1).
The interview data suggests that leaders respond to burnout by referring to institutional wellness programs. This action by physician leaders led to mixed reviews from the participants in terms of effectiveness. The overall sentiment from the participants seems to view this leadership behavior as helpful but not significantly impactful on burnout. Many of the interviewees seemed to view wellness programs in a very abstract sense in that they were sponsored by the institution but not necessarily by their immediate leadership.
Leadership Behaviors Desired
The leadership behaviors desired centered on two themes: Relational Support and Resource Obtainment. Relational Support included communication, moral support, and increasing efforts to include faculty in the decision-making process. Resource obtainment alluded to greater compensation for extra work done, more labor resources, and more time or resources to aid in childcare.
Leaders Should Provide Relational Support
Leadership behaviors or actions recommended or desired by participants reiterated many of the leadership behaviors observed by faculty in this sample. These categorical themes centered on communication, moral support, and community.
An associated group of leadership behaviors that were expressed as desired among the participants addressed the idea of leaders making them feel included and involved in the decision-making process. Interviewee number 10, referring to the feeling that leadership is not being transparent, recommended that listening, communicating, and being transparent are needed of leaders. Interviewee number 10 went on to say that people need to “feel like they are being heard and included in the decisions and being talked to instead of being talked at”. Interview number 1, expressing a feeling of being ignored, also described frustrations in immediate communication in stating that leaders should know “what is really going on”. Finally, interviewee number 6 discussed how giving constructive feedback to trainees should start by building trust through mentorship, so that those mentees understand that “honest feedback” is for their benefit and growth.
In conclusion, relationships that were built through communication, feeling heard, acceptance into the group, and inclusion in non-work activities represent a group of leadership behaviors that were desired of physician leaders (Table 2). These noted behaviors occurred in several contexts including individual meetings, group meetings, and social events. These behaviors that attempted to build relationships were identified as desirable by the interviewees.
Leaders Should Obtain Additional Resources
Obtaining additional resources was a common theme for many of the faculty participants. Physicians referred to compensation in many forms, especially monetary compensation for work done, but also through providing clerical help to drive efficiency. Interviewee number 3, in the context of expectations for physicians to answer emails from both patients and administrators, stated, “I would say figure out a way to compensate, those of us in primary care … because remember we asked for raises”.
Interviewee number 9 emphasized the need for proactive compensatory assessments when it is related that a researcher on the team is working extra hard and is deserving of some compensation in the form of not just monetary compensation but by giving a title to grant more empowerment: “you know you can’t get bonuses in these types of positions, so you can change your job title so without telling her I am looking into changing their job title to a different category” (Table 2).
Technical or clerical support was also mentioned by two other interviewees as something they desired leaders to provide. In dealing with the high clinical workload and lack of support in clinic, interviewee number 7 described how nurse practitioners, physician assistants, and scribes could help the clinic move much easier and could take the writing load off physicians “so that it is no longer on your own back to do all these patient notes yourself”. Finally, interviewee number 8 described how leadership could provide more resources and assistance in the form of “childcare (for) sick kids, and work that is satisfying”. Interviewee number 4 similarly alluded to a theme where more time resources could be allocated like a “wellness day like Kaiser” for the faculty to account for the unexpected time demands of clinical work.
These allusions to leadership behaviors desired in the form of providing resources were a commonly cited theme by our faculty interviewees. From the perspective of the participants, the provision of additional resources could be time, additional labor, or compensation for additional work activities performed. Overall, these additional resources were felt to add not only to the effectiveness and efficiency of clinics but also to the well-being of physicians in helping to reduce their burnout.
Discussion
Expected leadership behaviors by physicians are not limited to relationship building activities, but also task accomplishment and change behaviors.17–19 Yukl’s useful categorization of leadership behaviors has been used in several health care studies to describe health care leadership behaviors and is helpful in interpreting the findings of our study.20–22 The categories of relationship building, task accomplishment, and change behaviors can be used to frame the thematic responses of our faculty (Table 3). In answer to the question of leadership behaviors that were desired, our faculty identified additional resources in the form of clerical help, job crafting, and provider help as important expectations that leaders should provide. In addition, those leadership behaviors desired also centered on the theme of enhanced communication to build morale. When queried about what leadership behaviors were observed, our faculty identified reactive behaviors such as referral to wellness courses or relationship-based behavior that included social events and more frequent meetings as a response to burnout. None of the interviewees witnessed behaviors that procured additional resources that could lead to change to prevent future burnout. The absence of these additional favorable leadership response behaviors has not been adequately described in the health care literature in the context of burnout or wellness. Instead, task accomplishment and change behaviors have been discussed mostly in the context of performance and outcome studies.23,24 Since many of the needed organizational changes identified that lead to physician wellness (ie, compensation for clerical tasks related to the electronic health record and additional needed resources such as scribes) require organizational attainment of additional resources that often rely on systems or organizational reprioritization, change behaviors by physician leaders are of growing importance in convincingly advocating or implementing change objectives related to a culture of wellness.13,25,26 Therefore, physician leadership agency in accomplishing wellness objectives may require more than just relationship skills.
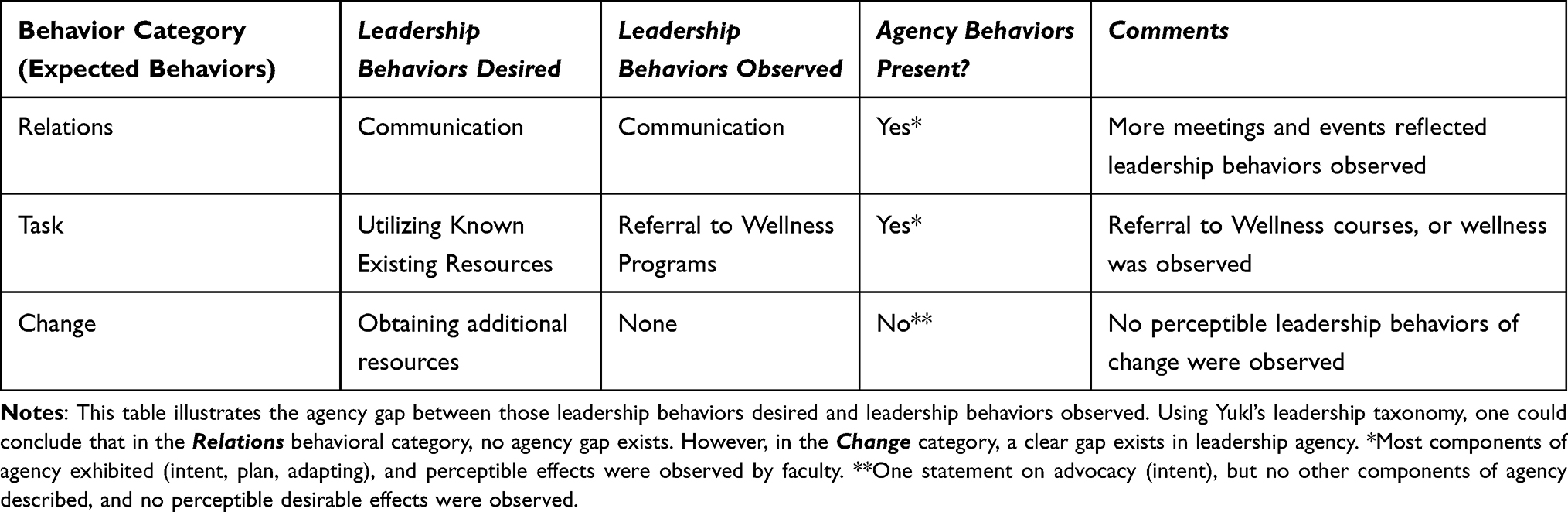 |
Table 3 Interpretation of Expected, Desired, and Observed Leadership Behaviors and Agency |
Before discussing agency, it is useful to define the role expectations of physician leadership in the health care system. Since perceived physician leadership performance is related to the expectations of those physicians being led; it is important to understand those elements of good physician leadership that is expected. In one qualitative international study, 50 physicians from various ranks including residents, specializing physicians, department chairs, and division chiefs granted interviews.19 Physician leaders were expected to display relational skills that include empathy, social skills, two-way communication skills, collegial respect, and medical expertise. In addition, good physician leadership included an understanding of and influence on the working conditions that allowed other physicians to practice optimally including obtaining and maintaining the resources needed for operations to run smoothly.27 Other studies extend expectations of a physician leader’s scope of responsibility to include organizational clinical performance goals (ie, safety and cardiac mortality rates) and traditional business performance goals (ie, financial goals or hospital rankings).23,28 Although reference to business performance and hospital rankings were not contained in the narratives of our study in the context of burnout, many of the relational behaviors such as more meetings and events, were identified (Table 3). The relational aspect of leadership in response to burnout therefore seems to be prevalent in our faculty’s understanding of their physician leaders’ behaviors and appears to meet the desired expectations of faculty.
Task accomplishment in addition to relation behaviors, however, is also expected of leaders. A recent systematic review of physician role responsibilities using the Theory of Expert Leadership framework demonstrated that expected physician leadership behaviors extended to strategic decision-making in guiding the direction of hospital policy in both clinical measures such as safety as well as business measures in terms of financial performance.18 Like previous studies, these physician leadership behaviors that should be displayed in the context of these extended roles were categorized as task-oriented and relationship-oriented behaviors. Thus, the behavioral range of physician leaders as defined in this systematic review included task-related behaviors focused on organizational goals and relational behaviors aimed at addressing the needs of physicians being led. Change-related behaviors by physician leaders were alluded to as an additional theme but were not clearly delineated as an expected behavior in this review. In our study, our faculty physicians expect their physician leaders to show not only relational behaviors but also task accomplishment behaviors in the form of utilizing existing resources to help with burnout (ie, wellness programs) and change behaviors in the form of implementing additional systems and resources that account for extraneous workloads resulting from a new electronic documentation system. Therefore, faculty from this Southern California institution expected all three categories of leadership behaviors. In terms of task accomplishment, one can interpret referrals to wellness programs as a behavior that at least partially met the desired expectations of faculty (Table 3).
In contrast, desired leadership change behaviors of procuring additional resources were not only absent from the narratives of our interviews but the perceptions of physician leaders lack of agency in addressing these needs was a prevalent theme in the faculty’s understanding. Agency is defined as the intentional exercise by humans of behaviors that can influence the course of events and the shaping of their lives.29 The perceived lack of agency of physician leaders can be viewed as not only ineffectual efforts in affecting change but also absence of efforts or motivation to affect change. Agency as opposed to empowerment is a more accurate description of perceived leadership behaviors since behaviors of agency are observable, unlike a leader’s psychological empowerment which has been defined as an intrinsic motivational vehicle that is less observable. As one interviewee stated, the lack of effective leadership action in addressing the wellness environment was perceived to be related to a lack of motivation when they mention how leaders’ lack of transparency in dealing with wellness issues is intentional (Appendix 1). Therefore, one can conclude that this interviewee views the leaders’ empowerment to be adequate, but the intent to change or the agency to change is absent.30 A better description of those perceived leadership behaviors that were lacking, is better explained by behaviors of agency that include four major elements: intentionality, forethought (planning), self-reactiveness (adaptation) and self-reflection (Appendix 2).31
By extension, agency can be viewed as a cognitive and motivational construct that possesses each of these four components in affecting “the course of events” in the environment.29,31 This concept, when applied to leadership, can be used as a descriptive and analytical term for leadership behaviors that impact the work environment in producing change and task accomplishment. The concept of agency differs from the term performance because the former not only relates to the successful attainment of a defined goal but also the process and plans used to attain full or partial accomplishment of a performance goal. In our study, perceptible effects of relational behavior from physician leaders were noted, but perceptible effects in change behaviors were not (Table 3). In other words, an agency gap was less apparent in relational behaviors, but a clear gap existed in change agency both in terms of obtaining resources and engaging in the process of agency.
Studies of leadership agency in the health care environment are limited. A few studies are available in the fields of health care business and nursing leadership. Such health care business studies assessed a manager’s agency in adaptive change in response to external policy or market pressures.32 Studies in nurse leadership have researched the role of leadership empowerment of nurses being led and found that through greater empowerment of nurses; autonomy and agency resulted.33 However, no studies have examined the concept of agency in relation to physician leadership in the context of wellness, and few have even examined how physician leaders adapt to changes in the health care environment.
The one study examining how physician leaders respond (ie, demonstration of agency) to changing environments was limited to a case study of a clinical outcome in the context of a quality improvement initiative. This case study examined the collective agency of various physician and non-physician stakeholders in the establishment of a new integrative clinical program in a Canadian Health region. This longitudinal study over four years described not only the successful outcome of change but alluded to physicians changing their attitudes toward working more collaboratively with non-physician stakeholders. Although specific adaptive and reflective behaviors were not described, intent and planning could be discerned from the descriptions.34 Therefore, although this case study examined a few agentic responses by physicians that resulted in the successful accomplishment of a change initiative, it did not fully describe change through the full spectrum of agency. One useful model of agency and its effects on the environment was proposed by Yoon and can form the basis of understanding how physician leadership agency interacts with the environment to accomplish change.35
Perhaps, the dearth of studies identifying agency behaviors in relation to change in physician leaders is not surprising since physician leadership challenges are many and include conflicts and constraints such as identity issues related to the optimal balance between clinical and business goals, feelings of exclusion from the decision-making process, personal sacrifice of relationships with colleagues for taking on managerial roles, relational problems with non-physicians, lack of adequate leadership training, and barriers to boundary crossing to accomplish objectives.36,37 The physician leader faced with the daunting challenges of change-related behaviors inherent in improving the wellness environment may not be inspired or motivated to lead these initiatives due to their lack of agency or a closely related sense of a lack of self-efficacy (Appendix 2).31
In conclusion, our study on leadership and burnout at an academic medical center demonstrated findings consistent with those in the literature, but additionally revealed the key concept of a lack of agency or an agency gap in change behaviors in accomplishing goals. Many studies have shown that effective relationships between leaders and followers are important in ameliorating burnout; however, this study showed that other leadership behaviors are important as well. In this rapidly changing health care environment, physician leadership that is adaptive and demonstrates individual and collective leadership in achieving the needed change requirements for wellness (ie, demonstrating agency for change) is sorely needed.25 More research into identifying and evaluating agency gaps and their associated factors in physician leaders is needed to better improve the health care environment of wellness for those frontline physicians. As a part of our institution’s professional development initiative, developing physician leadership agency using systems approaches is currently being taught and evaluated.
Limitations
Generalization of these findings to other institutions should be made with caution. The small number of interviewees limits its generalizability to other institutions as the first ten interviewees were set as the cutoff. It is not known if more interviews would have affected the results discovered. In addition, although burnout conditions seem similar today compared to the period of collection for this study, it is not known if the burnout environment or the physician leadership environment has changed significantly to affect the results. Although the feasibility and acceptability of conducting interviews via Zoom has been documented, potential technical difficulties may have arisen that would not have been encountered in a face-to-face context.38 The interviewer, however, did not report any technical problems. Furthermore, because of the anonymized and confidential nature of the study, one could not determine the demographic factors of the interviewees. Therefore, there may have been unforeseen selection bias of participants despite the random selection process.
The meaning and definitions of agency used in our study may not be the same as those described in the literature.22,39,40 For example, our use of agency considers the four elements of agency which have not been consistently used in studies of agency in the health care literature. In several studies assessing distributive leadership, the understanding of Bandura’s framework was limited to intent and initiation of action to address a clinical change initiative.34 The extent of assessing adaptation of a plan to the environment and reflection on the results were not evident. Therefore, our definition of agency may differ from other definitions. Uniformity of understanding of this concept is needed to better compare studies of agency between institutions and environments.
Finally, the activities of our physician population include caring for patients at a safety net hospital. Extrapolation of these findings to non-safety net organizations may not be appropriate as the needs and challenges faced in these environments may be different and therefore the interviewees’ answers may not apply to other academic medical centers not affiliated with safety net health care systems.
Acknowledgement
This study was supported by several groups and individuals. We would like to acknowledge the assistance provided by the following: the ten participants in this study, Cohort 1 of our physician leadership course, Kimberly Jen, and Janene Batten.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Dillon EC, Tai-Seale M, Meehan A, et al. Frontline perspectives on physician burnout and strategies to improve well-being: interviews with physicians and health system leaders. J Gen Intern Med. 2020;35(1):261–267. doi:10.1007/s11606-019-05381-0
2. Sibeoni J, Bellon-Champel L, Mousty A, et al. Physicians’ perspectives about burnout: a systematic review and metasynthesis. J Gen Intern Med. 2019;34(8):1578–1590. doi:10.1007/s11606-019-05062-y
3. Maslach C, Jackson SE, Leiter MP, Schaufeli WB, Schwab RL. Maslach Burnout Inventory Manual. Menlo Park, CA: Mind Garden; 2018.
4. West CP, Dyrbye LN, Shanafelt TD. Physician burnout: contributors, consequences and solutions. J Intern Med. 2018;283(6):516–529. doi:10.1111/joim.12752
5. Brady KJS, Trockel MT, Khan CT, et al. What do we mean by physician wellness? A systematic review of its definition and measurement. Acad Psychiatry. 2018;42(1):94–108. doi:10.1007/s40596-017-0781-6
6. Fred HL, Scheid MS. Physician burnout: causes, consequences, and (?) cures. Tex Heart Inst J. 2018;45(4):198–202. doi:10.14503/THIJ-18-6842
7. Bayes A, Tavella G, Parker G. The biology of burnout: causes and consequences. World J Biol Psychiatry. 2021;22(9):686–698. doi:10.1080/15622975.2021.1907713
8. West CP, Dyrbye LN, Erwin PJ, et al. Interventions to prevent and reduce physician burnout: a systematic review and meta-analysis. Lancet. 2016;388(10057):2272–2281. doi:10.1016/S0140-6736(16)31279-X
9. Dyrbye LN, Major-Elechi B, Hays JT, et al. Relationship between organizational leadership and health care employee burnout and Satisfaction. Mayo Clin Proc. 2020;95(4):698–708. doi:10.1016/j.mayocp.2019.10.041
10. Olson K, Marchalik D, Farley H, et al. Organizational strategies to reduce physician burnout and improve professional fulfillment. Curr Probl Pediatr Adolesc Health Care. 2019;49(12):100664. doi:10.1016/j.cppeds.2019.100664
11. Shanafelt TD, Gorringe G, Menaker R, et al. Impact of organizational leadership on physician burnout and satisfaction. Mayo Clin Proc. 2015;90(4):432–440. doi:10.1016/j.mayocp.2015.01.012
12. Mete M, Goldman C, Shanafelt T, et al. Impact of leadership behaviour on physician well-being, burnout, professional fulfilment and intent to leave: a multicentre cross-sectional survey study. BMJ Open. 2022;12(6):e057554. doi:10.1136/bmjopen-2021-057554
13. Shanafelt TD, Schein E, Minor LB, et al. Healing the professional culture of medicine. Mayo Clin Proc. 2019;94(8):1556–1566. doi:10.1016/j.mayocp.2019.03.026
14. Stoller JK. Change: leadership essentials for chest medicine professionals. Chest. 2021;159(4):1559–1566. doi:10.1016/j.chest.2020.09.094
15. Corbin JS. Basics of Qualitative Research: Techniques of Procedures for Developing Grounded Theory. Thousand Oaks, CA: Sage Publications Inc; 2015.
16. Creswell JWC. Research Design: Qualitative, Quantitative, and Mixed Methods Approaches. Thousand Oaks, CA: Sage Publishing Inc; 2018.
17. Schwartz RW, Pogge C. Physician leadership: essential skills in a changing environment. Am J Surg. 2000;180(3):187–192. doi:10.1016/S0002-9610(00)00481-5
18. Thoebes GP, Porter TH, Peck JA. Physicians as leaders: a systematic review through the lens of expert leadership. Leadersh Health Serv. 2024;37(1):95–111. doi:10.1108/LHS-02-2023-0008
19. Huikko-Tarvainen S. Elements of perceived good physician leadership and their relation to leadership theory. Leadersh Health Serv. 2022;35(1):14–29. doi:10.1108/LHS-01-2021-0002
20. Yukl G, Gordon A, Taber T. A hierarchical taxonomy of leadership behavior: integrating a half century of behavior research. J Leader Org Stud. 2002;9(1):15–32. doi:10.1177/107179190200900102
21. Barattucci M, Lo Presti A, Bufalino G, et al. Distributed leadership agency and work outcomes: validation of the Italian DLA and its relations with commitment, trust, and satisfaction. Front Psychol. 2020;11:512. doi:10.3389/fpsyg.2020.00512
22. Jonsson T, Unterrainer C, Jeppesen H-J, et al. Measuring distributed leadership agency in a hospital context. J Health Organ Manag. 2016;30(6):908–926. doi:10.1108/JHOM-05-2015-0068
23. Tasi MC, Keswani A, Bozic KJ. Does physician leadership affect hospital quality, operational efficiency, and financial performance? Health Care Manage Rev. 2019;44(3):256–262. doi:10.1097/HMR.0000000000000173
24. Kaiser F, Schmid A, Schluchtermann J. Physician-leaders and hospital performance revisited. Soc Sci Med. 2020;249:112831. doi:10.1016/j.socscimed.2020.112831
25. Jha AK, Iliff AR, Chaoui AA, Defossez S, Bombaugh MC, Miller YR. A crisis in health care: a call to action on physician burnout. Harvard TH Chan School of Public Health Harvard. 2019;2019:1–10.
26. Lustig A, Ogden M, Brenner RW, et al. The central role of physician leadership for driving change in value-based care environments. J Manag Care Spec Pharm. 2016;22(10):1116–1122. doi:10.18553/jmcp.2016.22.10.1116
27. Pihlainen V, Kivinen T, Lammintakanen J. Management and leadership competence in hospitals: a systematic literature review. Leadersh Health Serv. 2016;29(1):95–110. doi:10.1108/LHS-11-2014-0072
28. Savage M, Savage C, Brommels M, et al. Medical leadership: boon or barrier to organisational performance? A thematic synthesis of the literature. BMJ Open. 2020;10(7):e035542. doi:10.1136/bmjopen-2019-035542
29. Bandura A. Exercise of human agency through collective efficacy. Curr Direct Psych Sci. 2000;9(3):75–78. doi:10.1111/1467-8721.00064
30. Spence Laschinger HK, Finegan JE, Shamian J, Wilk P. A longitudinal analysis of the impact of workplace empowerment on work satisfaction. J Organizational Behav. 2004;25(4):527–545. doi:10.1002/job.256
31. Bandura A. Social cognitive theory: an agentic perspective. Annu Rev Psychol. 2001;52:1–26. doi:10.1146/annurev.psych.52.1.1
32. Payne J, Leiter J. Structuring agency: examining healthcare management in the USA and Australia using organizational theory. J Health Organ Manag. 2013;27(1):106–126. doi:10.1108/14777261311311825
33. Gottlieb LN, Gottlieb B, Bitzas V. Creating empowering conditions for nurses with workplace autonomy and agency: how healthcare leaders could be guided by strengths-based nursing and healthcare leadership (SBNH-L). J Healthc Leadersh. 2021;13:169–181. doi:10.2147/JHL.S221141
34. Chreim S, Williams BE (Bernie), Janz L, et al. Change agency in a primary health care context: the case of distributed leadership. Health Care Manage Rev. 2010;35(2):187–199. doi:10.1097/HMR.0b013e3181c8b1f8
35. Yoon JH. Toward agentic HRD: a translational model of Albert Bandura’s human agency theory. Adv Dev Human Res. 2019;21(3):335–351. doi:10.1177/1523422319851437
36. Onyura B, Crann S, Freeman R, et al. The state-of-play in physician health systems leadership research. Leadersh Health Serv. 2019;32(4):620–643. doi:10.1108/LHS-03-2019-0017
37. Stoller JK. Developing physician leaders: a perspective on rationale, current experience, and needs. Chest. 2018;154(1):16–20. doi:10.1016/j.chest.2017.12.014
38. Archibald MM, Ambagtsheer RC, Casey MG, et al. Using zoom videoconferencing for qualitative data collection: perceptions and experiences of researchers and participants. Int J Qual Methods. 2019;18:1609406919874596.
39. Vizheh M, Zurynski Y, Braithwaite J, et al. Determinants of women’s agency in accessing and utilising reproductive healthcare services; a systematic review. Cult Health Sex. 2023;2023:1–17.
40. Waitzberg R, Quentin W, Busse R, et al. Dual agency: a fresh perspective to identify dilemma mitigation strategies - A response to the recent commentaries. Int J Health Policy Manag. 2023;12:7758. doi:10.34172/ijhpm.2022.7758
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.