")
Back to Journals » Journal of Healthcare Leadership » Volume 15
Physician-Chef-Dietitian Partnerships for Evidence-Based Dietary Approaches to Tackling Chronic Disease: The Case for Culinary Medicine in Teaching Kitchens
Authors Wood NI , Stone TA, Siler M, Goldstein M, Albin JL
Received 1 March 2023
Accepted for publication 12 July 2023
Published 24 July 2023 Volume 2023:15 Pages 129—137
DOI https://doi.org/10.2147/JHL.S389429
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Pavani Rangachari
Nathan I Wood,1 Theresa A Stone,2 Milette Siler,3 Max Goldstein,4 Jaclyn Lewis Albin5
1Department of Internal Medicine, Yale School of Medicine, New Haven, CT, USA; 2Department of Internal Medicine, MedStar Health, Washington, DC, USA; 3Moncrief Cancer Institute, University of Texas Southwestern Medical Center, Fort Worth, TX, USA; 4Digestive Health Center, Yale New Haven Health, New Haven, CT, USA; 5Departments of Internal Medicine and Pediatrics, University of Texas Southwestern Medical Center, Dallas, TX, USA
Correspondence: Jaclyn Lewis Albin, Department of Pediatrics, University of Texas Southwestern, Medical Center, 5323 Harry Hines Blvd, Dallas, TX, 75390, USA, Tel +1 214 648 9498, Email [email protected]
Abstract: Since the middle of the 20th century, the American food environment has become increasingly ultra-processed. As a result, the prevalence of chronic, diet-related disease in the United States has skyrocketed. Meanwhile, physicians are still poorly trained in nutrition. A recent innovation that aims to address this is “culinary medicine” programming taught by teams of physicians, chefs, and registered dietitian nutritionists. Culinary medicine is an evidence-based, interprofessional field of medicine that combines culinary arts, nutrition science, and medical education to prevent and treat diet-related disease. It employs hands-on learning through healthy cooking and is typically taught in a teaching kitchen, either in-person or virtually. It can be dosed either as a patient care intervention or as experiential nutrition education for students, medical trainees, and healthcare professionals. Culinary medicine programs are effective, financially feasible, and well-received. As a result, healthcare systems and medical education programs are increasingly incorporating culinary medicine, teaching kitchens, and interprofessional nutrition education into their patient care and training models.
Keywords: nutrition, interprofessional, innovation, education
Introduction
The prevalence of chronic, diet-related disease has risen dramatically since the middle of the 20th century, both in the United States and worldwide, and is a leading cause of death and disability.1,2 Cardiovascular disease has been the top killer of Americans every year since 1921.3 Today, 34.2 million US adults have type 2 diabetes,4 a more than 20-fold increase since the 1950s.5 One in two Americans is expected to have obesity by 2030,6 and the thirteen types of cancer associated with obesity are responsible for 40% of all cancer diagnoses every year in the United States.7
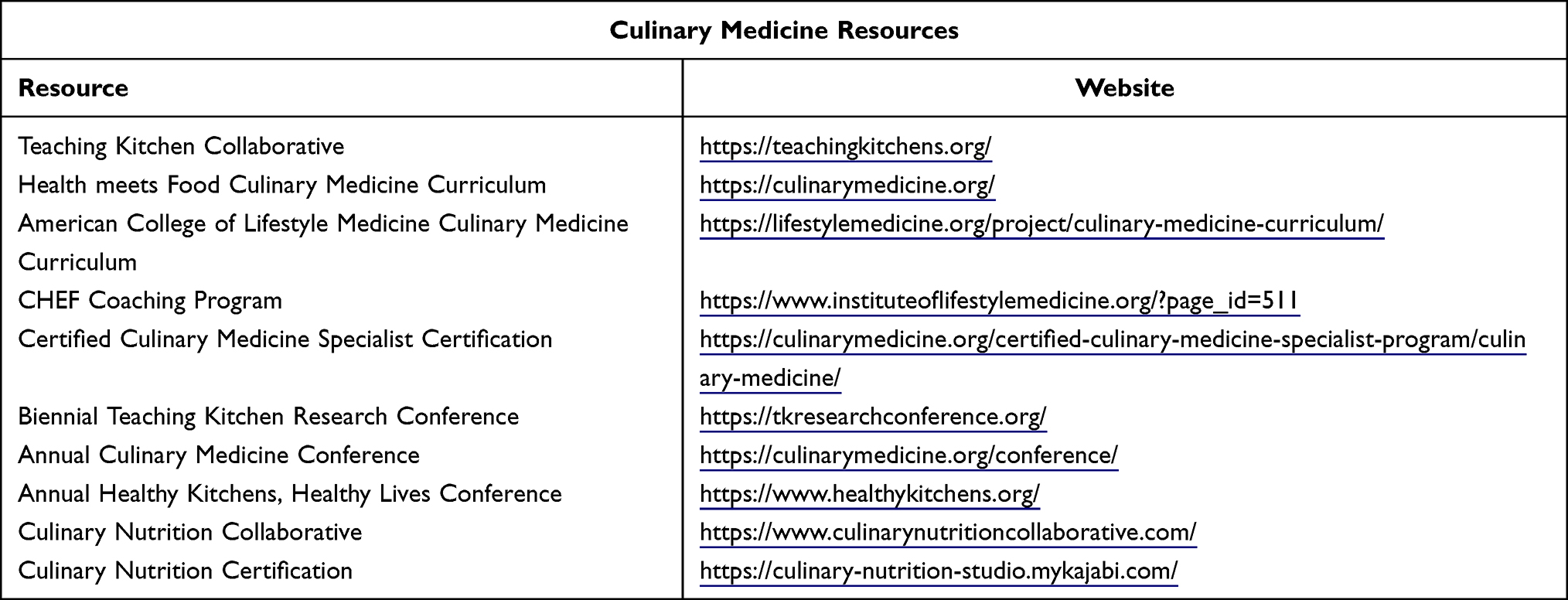 |
Table 1 Resources for Training and Education |
It is clear that one of the biggest root causes of this pandemic of chronic disease is our food environment. Ultra-processed foods laden with salt, oil, and sugar are ubiquitous, from the supermarket to the hospital cafeteria, comprising 73% of the United States’ food supply.8 And while an estimated 12.8% of Americans live in low-income, low-access areas called “food deserts”, where grocery stores are absent and affordable and nutritious food is limited,9 ultra-processed foods are available everywhere. In so-called “food swamps”,10 fast food chains and convenience stores pack streets, and chronic disease is the norm.11
Notably, the geography of these food deserts and swamps reflect systemic inequities, including race12 and other social determinants of health.13 Grocery stores and supermarkets are reluctant to establish locations in the areas that need them most, often citing crime statistics and low incomes.14 Fast food chains and ultra-processed foods, in contrast, exist abundantly in underserved areas and target minoritized populations with their marketing messages.15 These structural barriers to achieving a nourishing dietary pattern increase disparities and perpetuate inequities.
Doctors, being no match for the devolving food environment around them, have been ineffective in addressing our nation’s increasing burden of chronic disease. While patients tend to look to their physicians for dietary advice, doctors are notoriously poorly trained in nutrition.16,17 Some have even argued that this poorly trained physician workforce is a structural contributor to the increasing prevalence of diet-related disease in America.18 Given that poor quality diet is one of the biggest risk factors for chronic disease and represents the leading cause of mortality in the United States,1,19 this is unacceptable.
Registered dietitian nutritionists (RDNs), conversely, are expertly trained in nutrition and dietary counseling. Unfortunately, patient access to RDNs remains limited due to insufficient insurance coverage,20 inappropriately low referral rates from clinicians,21 and an enduring public undervaluing of their knowledge and skills.22 Although recent legislative efforts have sought to remediate this discrepancy by codifying into law provisions that would increase patient access to RDNs, so far these proposals have not passed.23
Another underutilized profession in the fight against poor quality diets and chronic disease is that of chefs. Many culinary professionals aim to develop accessible recipes for food that is both healthy and delicious. Others are responsible for feeding patients health-restoring food in hospitals, nursing homes, and rehabilitation facilities. However, most chefs do not receive nutrition education as part of their training and are therefore unprepared to produce the healthy food and recipes demanded of them. Recent efforts have sought to bring more nutrition training to culinary professionals, a shift that chefs welcome.24
In the pursuit of improved health, food is clearly a problem. Fortunately, food can also be a key solution. By ensuring universal access to healthy food, making evidence-based nutrition education commonplace for both patients and healthcare professionals, and teaching people to cook nourishing food at home, we can improve dietary quality to prevent and treat many chronic diseases (Figure 1). This approach is necessarily multifaceted, requiring efforts to promote food access, build community relationships, increase access to healthcare, transform public policy, foster private partnerships, revamp infrastructure, and more. One essential ingredient in this recipe for diet-supported health, dosed according to a population’s specific needs, is interdisciplinary physician-chef-RDN-led culinary medicine in teaching kitchens (Table 1).
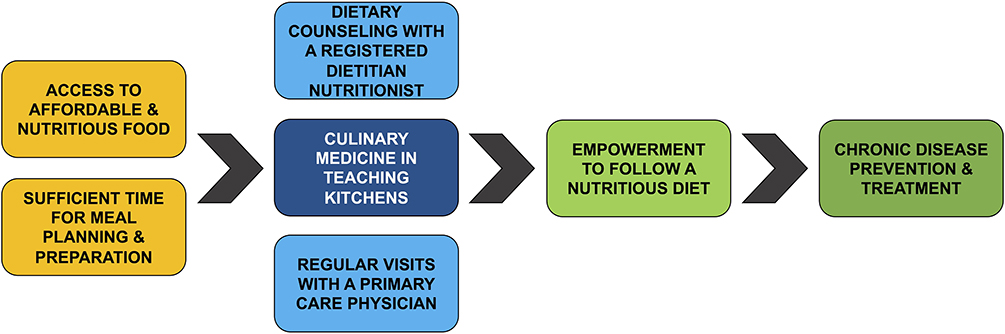 |
Figure 1 The role of culinary medicine in a multifaceted approach to addressing diet-related disease. Effectively preventing and treating diet-related chronic disease will necessitate systemic changes that address food insecurity and time poverty, provide nutrition and culinary education, and ensure access to interprofessional healthcare. As part of this interprofessional healthcare, culinary medicine serves as the vital link in empowering patients to transform healthy ingredients into healthy dietary patterns. |
What is Culinary Medicine?
Culinary medicine is an evidence-based, interprofessional field of medicine that combines culinary arts, nutrition science, and medical education to prevent and treat diet-related disease. It employs hands-on learning through healthy cooking and is typically taught in a teaching kitchen, either in-person or virtually. It can be dosed either as a patient care intervention or as experiential nutrition education for students, medical trainees, and healthcare professionals.
Culinary medicine is necessarily interprofessional. It combines the expertise of physicians, chefs, and RDNs. Frequently, physicians are the first touchpoint for patient care. They are experts in diagnosing disease, devising treatment plans, and leading multidisciplinary medical teams. Chefs are experts in recipe development and the culinary arts, skills that are essential for cooking health-promoting food. RDNs are educated, trained, and licensed in nutrition, dietary assessment, and dietary counseling. The collective expertise of physicians, chefs, and RDNs as an interprofessional team is uniquely suited to assist patients in preventing and treating chronic disease through culinary medicine.
Culinary medicine is hands-on. Culinary medicine curricula include a variety of engaging learning activities,25 including case-based learning, small group work, lectures, discussions, readings, videos, patient simulations, and — by definition — hands-on, interactive cooking experience. Since the field’s inception 20 years ago,26 culinary medicine sessions have been hosted in teaching kitchens. Teaching kitchens are essential, serving as laboratories for the higher-order, kinesthetic learning typified by culinary medicine. However, during the past three years and in the context of the COVID-19 pandemic, virtual teaching kitchens have proliferated.27–29 Making use of remote-learning, these virtual, synchronous culinary medicine classes have proven to be effective similarly to their in-person correlatives. This unique and modern method of virtual teaching has also increased the scalability of culinary medicine interventions.
Culinary medicine is evidence-based, both for patients and for medical trainees. For patients, culinary medicine interventions have been shown to improve diabetes control,27,30 blood pressure,30 serum cholesterol,30 BMI,31,32 adherence to a Mediterranean diet,33 fruit and vegetable intake,32,33 self-esteem,34 self-efficacy,35 socialization,36,37 psychological well-being,38,39 and quality of life.37,40 Among medical trainees, culinary medicine interventions have demonstrated improvements in participants’ interprofessional collaboration, confidence and competence in providing nutritional counseling, cooking and nutrition knowledge, self-efficacy, motivation to eat healthfully, and personal health behaviors.25,41,42
Culinary medicine is fun. Instructors enjoy teaching it, and participants enjoy learning it. These interventions have been demonstrated to be consistently well-received.42 Not only do participants acquire knowledge and skills and improve attitudes and behaviors — they build long-lasting friendships, support networks, and communities. In the wake of the COVID-19 pandemic’s impact on isolation, loneliness, and mental health, this is as enticing as it is important.
The Beneficiaries of Culinary Medicine
Culinary medicine was originally conceptualized as a treatment for patients.26 Although many patients struggle with food insecurity, even those who are food-secure frequently experience barriers to eating healthfully. Gaining access to health-promoting food is only the beginning; buying healthy food begets healthy dietary habits only through healthy cooking (Figure 1). For patients who have gaps in nutrition knowledge or cooking skills, achieving and maintaining a healthy dietary pattern long-term is difficult. By empowering patients with nutrition knowledge and skills to prepare accessible, affordable, easy, nourishing, and delicious meals, culinary medicine interventions can enable positive lifestyle changes to prevent and treat chronic disease.
More recently, culinary medicine has been implemented as a curricular innovation in medical education. The Goldring Center for Culinary Medicine, the first teaching kitchen operated within a medical school, opened in 2012.43 Today, the Health meets Food culinary medicine curriculum has been adopted by over 55 medical schools, residency programs, and nursing schools.44
Culinary medicine education is modern and comprehensive in its approach to preparing a physician workforce capable of addressing diet-related chronic disease. First, trainees learn the basics of nutrition, including the impact of diet on common chronic diseases, including cardiovascular disease, type 2 diabetes, obesity, and cancer. Then, they immediately apply this knowledge by preparing food designed to prevent and treat these very conditions. For this reason, culinary medicine has been likened to the “missing laboratory portion of the historically didactic nutrition curriculum present in most medical schools”.45
Culinary medicine also exposes trainees to innovative care models, including shared medical appointments (SMAs) and interprofessional, team-based care.46 SMA models are emerging platforms used in culinary medicine to empower dietary behavior change through hands-on skills building.46,47 They advance interprofessional collaboration and build communities of people empowered to sustain behavior change.
Beyond medical trainees, culinary medicine could also benefit a variety of healthcare professionals, including physician assistants/associates, nurse practitioners, physical therapists, nurses, clinical pharmacists, social workers, exercise physiologists, and more. Patients engage with an array of healthcare personnel, many of whom have more facetime with patients than physicians. As a result, many of these professionals are faced with nutrition questions or asked to give dietary advice to patients despite their lack of training to do so. Expanding their knowledge base with culinary medicine interventions could allow for the consistent reinforcement of evidence-based nutrition information across patients’ medical teams of providers and professionals.
Implementation Challenges
One of the biggest barriers to the widespread implementation of culinary medicine programming is physical: the need for a teaching kitchen. Fortunately, there are many adaptations of teaching kitchens that can offer hands-on culinary education. Full commercial kitchens found in culinary schools, food service establishments, and other commercial enterprises can emulate the experience of a professional chef. Some innovative culinary medicine programs have made use of food sciences laboratories on undergraduate college campuses.48,49 Universities are increasingly building teaching kitchens, and experts are calling for hospital cafeterias, corporate workplaces, and community centers to follow suit.50 Portable “pop-up” kitchen kits, complete with modest totes of everyday kitchen tools and supplies, can be brought into conference and meeting rooms. In the absence of a physical kitchen, culinary medicine interventions can be conducted in virtual teaching kitchens, with participants cooking together online from their home kitchens. This versatility offers institutions the opportunity to customize their teaching kitchen environment not only to the targeted learner, but also to the realities of budget and resource constraints.
Funding is a nearly universal barrier to implementation. A recent scoping review cited wide variability in funding of culinary medicine programs and that the lack of consistent funding is a barrier to program sustainability.42 At present, culinary medicine programs are largely funded via philanthropy, individual institutions, or external grants. Pairing the educational mission of culinary medicine with clinical care applications offers a promising solution. Group care through SMAs has been shown to enable financial sustainability.51,52 Auxiliary, fee-for-service, clinical one-on-one appointments with dietitians or culinary medicine teams can generate income. Recent innovative clinical models have made use of reimbursable culinary medicine eConsults.53 To ensure long-term sustainability, health systems and medical and public health schools share an opportunity to design innovative funding models that align missions for cost-effective care, impactful research, relevant education, and community engagement.
Due to the newness of the field, another barrier to implementation is the lack of a qualified workforce trained to teach and practice culinary medicine. There is, of course, no residency or fellowship in culinary medicine, and very few culinary medicine programs offer rotation or internship opportunities. Only in the past decade has the Certified Culinary Medicine Specialist program become available.54 Physicians are not adequately trained in nutrition, let alone the culinary arts, and few chefs have medical or formal nutrition training.
Similarly, RDN training is currently focused on didactic, scientific education and medical nutrition therapy, not cooking. Although the field of dietetics historically included education in food preparation, many RDN education programs decreased or eliminated culinary education altogether as the field sought to distance itself from the field of home economics.55 In response, a small-but-growing field of culinary dietitian nutritionists has emerged who will be able to lead culinary medicine initiatives.56,57
When physicians, chefs, and RDNs collaborate, their complementary areas of expertise synchronize and synergize to enable evidence-based culinary medicine programming. Once these programs achieve sustainability, leading teams should prioritize “train the trainer” opportunities to better equip the workforce of tomorrow to teach and practice culinary medicine.
The Dollars and Sense of Culinary Medicine
In the short-term, culinary medicine interventions can be financially sustainable within the confines of our current fee-for-service model. The most common approach to achieve this is to use the teaching kitchen as a site for SMAs. A recent publication46 detailed one such approach that achieved success in incorporating culinary medicine into SMAs held in a teaching kitchen. The authors billed US-based evaluation and management codes for common diet-related health conditions for each weekly appointment, and the program was able to “break even” at a volume of 12 patients per week for 8 weeks — 96 total patient encounters. Most importantly, besides being feasible and cost-effective, SMAs incorporating culinary medicine instruction are well received by patients.47 Teaching kitchens are also well suited to promote community health through a variety of program offerings as part of a non-profit’s institutional mission and in collaboration with community organizations doing similar work.
Teaching kitchens are ripe for research productivity. By addressing exigent health issues facing the American public and engaging in community-based participatory research, particularly in partnership with schools of public health, teaching kitchens represent an additional avenue by which institutions can ensure impactful grant flow.
In the long-term, culinary medicine programs held in teaching kitchens ready healthcare systems for the future of value-based care. As reimbursement strategies evolve, efforts to improve population health and reduce healthcare costs will be increasingly rewarded and thus become central to future healthcare delivery models. Culinary medicine could play an integral role in these efforts, coordinating the care of many patients with a variety of professionals and community resources to combat costly chronic diseases.58 At the same time, culinary medicine interventions could be incorporated into employee health programs, where they could also be expected to reduce healthcare costs and increase employee productivity.
To attract and retain patients, healthcare systems may increasingly feel the pressure to implement culinary medicine programs. The more patients discover opportunities to learn about culinary medicine in teaching kitchens, the more they actively seek out these opportunities. Their healthcare dollars follow where they choose to seek care, and thus patients will likely drive the investment in culinary medicine offerings being implemented in hospitals and clinics.
Beyond the Bucks
In a time where 63% of healthcare professionals suffer from burnout59 and 56% of Americans feel that the United States does not handle health care well,60 culinary medicine could be an antidote. By leading SMAs and culinary medicine interventions, health professional teams can bring investment, authenticity, and passion to patient care. Faculty and staff can find fulfillment in their work, which translates not only to high-quality patient care, but also to employee retention and productivity. Clinicians benefit from a system that values their meaningful, impactful contributions, and patients benefit from multidisciplinary, holistic care aimed at empathetically and pragmatically addressing the root causes of their diseases.
Culinary medicine programs also afford deep connections between healthcare systems and the communities they serve. Teaching kitchens offer an infrastructure in which to foster community co-leadership and develop long-lasting, meaningful relationships. Sharing a meal with someone — “breaking bread” — is a universal demonstration of hospitality and respect understood by cultures across time and space. With mutual trust, patients in the community can be increasingly engaged with healthcare and valued as co-creators of a system devoted to public health promotion and the provision of patient-centered medical care.
Culinary medicine also serves as mental health promotion — fostering community, serving as a form of group therapy, and increasing socialization after an isolating start to the 2020s brought on by the COVID-19 pandemic. These classes, after all, are fun.
Given how enjoyable and effective culinary medicine experiences are, these programs are increasingly being used for recruitment. They are attractive not only to patients, but also to practicing clinicians, learners, and researchers. The teaching kitchen as a “learning laboratory”50 — where culinary arts, medical nutrition therapy, mindfulness and mental health, and behavior change strategies all intersect — is incontrovertibly fascinating and exciting. Intrepid researchers will find that there are many opportunities for further study and innovation. To attract and retain passionate faculty, students, and clinicians, medical schools and healthcare systems of the future should consider supporting teaching kitchens to offer culinary medicine. These programs garner prestige and concretize the forward-thinking, patient-centered approach to care that hospitals and training programs aspire to. As media attention around teaching kitchens increases, healthcare systems will quickly realize — if they have not already — that they should invest in their own culinary medicine programs to avoid being left behind.
The Future of Culinary Medicine
Culinary medicine represents the flavor of innovative strategy that will be key to the future of healthcare. It’s team-based and interprofessional. Physicians, chefs, and RDNs work together, combining their expertise for the betterment of clinicians and patients alike. Physicians advocate for their teammates, sharing the responsibility of patient care and elevating the expertise of their RDN colleagues. Medical trainees educated on the impact of diet on disease are better prepared to engage in scholarship and community-based participatory research, including quality improvement efforts to positively impact patient care. Physicians with culinary medicine experience can further build skills to quash nutrition misinformation in the office and on social media, address diet-related chronic diseases more comprehensively, and lead innovation in care delivery models and community partnerships.
Teaching kitchens integrate a currently disjointed system, serving as a potential hub for education, research, patient care, and community engagement (Figure 2). They are well-poised to develop and expand community partnerships and elevate the voices of community leaders, engendering trust and fostering meaningful relationships with the people they serve. By partnering with social workers, community health workers, food pantries, governmental programs, schools, and community organizations, teaching kitchens can serve as a nucleus for programs that increase food access, reduce disparities, and address social determinants of health.
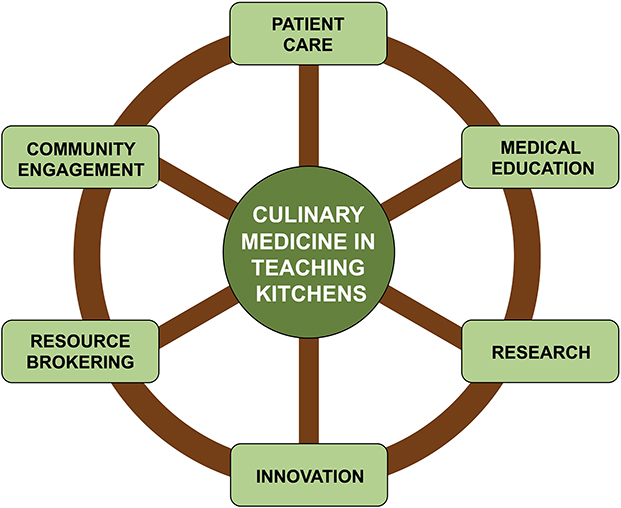 |
Figure 2 Culinary medicine in teaching kitchens as the “hub”. Culinary medicine in teaching kitchens, by its interprofessional and multidisciplinary nature, seamlessly integrates healthcare, academia, and public service. Patients, providers, community members, researchers, universities, insurance companies, and healthcare systems all benefit from this collaboration. |
Culinary medicine in teaching kitchens can ready us for value-based care and other future innovations in healthcare. It makes financial sense. It attracts and supports staff and trainees. It allows preventive healthcare to be prioritized. Hopefully, it can mobilize funding by decreasing the costs of treating diet-related disease. Interprofessional teams of physicians, chefs, and RDNs will be able to support patients in learning practical, evidence-based skills to improve their health using kitchens. Patients could be more actively engaged in maintaining their health. The future of healthcare, perhaps, will start in the kitchen.
Acknowledgments
The authors would like to acknowledge the many individuals whose forward thinking was foundational to building this field. We are grateful to the team at Health meets Food and the Certified Culinary Medicine Specialist board for providing actionable training, curricular resources, and much inspiration. We appreciate the vital role of the American College of Lifestyle Medicine in advancing the field from fringe to mainstream, work through which the relevance and support for culinary medicine has grown. We are also very thankful for the thought leadership of the entire Teaching Kitchen Collaborative team for building connections in this work internationally and always asking questions until we find answers (while eating really delicious and nourishing food).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mokdad AH, Ballestros K, Echko M, et al.; The US Burden of Disease Collaborators. The State of US Health, 1990–2016: burden of diseases, injuries, and risk factors among US states. JAMA. 2018;319(14):1444. doi:10.1001/jama.2018.0158
2. Afshin A, Sur PJ, Fay KA, et al. Health effects of dietary risks in 195 countries, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2019;393(10184):1958–1972. doi:10.1016/S0140-6736(19)30041-8
3. National Center for Health Statistics. Leading Causes of Death, 1900–1998. Atlanta, GA: Centers for Disease Control and Prevention; 1998. Available from: https://www.cdc.gov/nchs/data/dvs/lead1900_98.pdf.
4. Centers for Disease Control and Prevention. National diabetes statistics report, 2020. Atlanta, GA: Centers for Disease Control and Prevention, U.S. Dept of Health and Human Services; 2020. Available from: https://diabetesresearch.org/wp-content/uploads/2022/05/national-diabetes-statistics-report-2020.pdf.
5. Division of Diabetes Translation. Long-term trends in diabetes. Atlanta, GA: Centers for Disease Control and Prevention; 2017. Available from: https://www.cdc.gov/diabetes/statistics/slides/long_term_trends.pdf.
6. Ward ZJ, Bleich SN, Cradock AL, et al. Projected U.S. state-level prevalence of adult obesity and severe obesity. N Engl J Med. 2019;381(25):2440–2450. doi:10.1056/NEJMsa1909301
7. Steele CB, Thomas CC, Henley SJ, et al. Vital signs: trends in incidence of cancers associated with overweight and obesity — United States, 2005–2014. MMWR Morb Mortal Wkly Rep. 2017;66(39):1052–1058. doi:10.15585/mmwr.mm6639e1
8. Menichetti G, Ravandi B, Mozaffarian D, Barabási AL. Machine learning prediction of the degree of food processing. Nat Commun. 2023;14(1):2312. doi:10.1038/s41467-023-37457-1
9. Rhone A, Ver Ploeg M, Dicken C, Williams R, Breneman V. Low-income and low-supermarket-access census tracts, 2010–2015. 2017: EIB–165. Available from: https://www.ers.usda.gov/webdocs/publications/82101/eib-165.pdf?v=3395.3.
10. Rose D, Bodor N, Swalm C, Rice J, Farley T, Hutchinson P. Deserts in New Orleans? Illustrations of Urban Food Access and Implications for Policy. Ann Arbor, MI: University of Michigan National Poverty Center; USDA Economic Research Service Research; 2009.
11. Cooksey-Stowers K, Schwartz M, Brownell K. Food swamps predict obesity rates better than food deserts in the United States. Int J Environ Res Public Health. 2017;14(11):1366. doi:10.3390/ijerph14111366
12. New York Law School Racial Justice Project. Unshared bounty: how structural racism contributes to the creation and persistence of food deserts. (with American Civil Liberties Union). New York, NY: Racial Justice Project. Book 3; 2012. Available from: https://digitalcommons.nyls.edu/cgi/viewcontent.cgi?article=1002&context=racial_justice_project.
13. Bower KM, Thorpe RJ, Rohde C, Gaskin DJ. The intersection of neighborhood racial segregation, poverty, and urbanicity and its impact on food store availability in the United States. Prev Med. 2014;58:33–39. doi:10.1016/j.ypmed.2013.10.010
14. Shaffer A. The persistence of LA’s grocery gap: the need for a new food policy and approach to market development. Los Angeles, CA: Center for Food and Justice, Urban and Environmental Policy Institute, Occidental College; 2002. Available from: https://www.oxy.edu/sites/default/files/assets/UEP/Comps/2002/shaffer.pdf.
15. Grier SA, Kumanyika SK. The context for choice: health implications of targeted food and beverage marketing to African Americans. Am J Public Health. 2008;98(9):1616–1629. doi:10.2105/AJPH.2007.115626
16. Adams KM, Butsch WS, Kohlmeier M. The state of nutrition education at US medical schools. J Biomed Educ. 2015;2015:1–7. doi:10.1155/2015/357627
17. Kris-Etherton PM, Akabas SR, Bales CW, et al. The need to advance nutrition education in the training of health care professionals and recommended research to evaluate implementation and effectiveness. Am J Clin Nutr. 2014;99(5):1153S–1166S. doi:10.3945/ajcn.113.073502
18. Morris NP. The neglect of nutrition in medical education: a firsthand look. JAMA Intern Med. 2014;174(6):841. doi:10.1001/jamainternmed.2014.839
19. Murray CJL. The state of US health, 1990–2010: burden of diseases, injuries, and risk factors. JAMA. 2013;310(6):591. doi:10.1001/jama.2013.13805
20. Martin H, Kushner S, Iles K, Montgomery H. Advocating for expanded access to medical nutrition therapy in medicare. J Acad Nutr Diet. 2022;122(1):175–181. doi:10.1016/j.jand.2021.02.024
21. Devries S, Aggarwal M, Allen K, Kris-Etherton P, Theriot P, Freeman AM. Assessment of the low referral rate of cardiologists to dietitians/nutritionists. Int J Dis Reversal Prev. 2021;4(1):8. doi:10.22230/ijdrp.2021v3n2a303
22. Siopis G, Colagiuri S, Allman-Farinelli M. Dietitians’ experiences and perspectives regarding access to and delivery of dietetic services for people with type 2 diabetes mellitus. Heliyon. 2020;6(2):e03344. doi:10.1016/j.heliyon.2020.e03344
23. Collins S. Medical nutrition therapy act of 2021. United States Senate, 117th Congress; 2021. Available from: https://www.congress.gov/117/bills/s1536/BILLS-117s1536is.pdf.
24. Bertoldo J, Hsu R, Reid T, Righter A, Wolfson JA. Attitudes and beliefs about how chefs can promote nutrition and sustainable food systems among students at a US culinary school. Public Health Nutr. 2021;1–13. doi:10.1017/S1368980021003578
25. Tan J, Atamanchuk L, Rao T, Sato K, Crowley J, Ball L. Exploring culinary medicine as a promising method of nutritional education in medical school: a scoping review. BMC Med Educ. 2022;22(1):441. doi:10.1186/s12909-022-03449-w
26. La Puma J. What is culinary medicine and what does it do? Popul Health Manag. 2016;19(1):1–3. doi:10.1089/pop.2015.0003
27. Sharma SV, McWhorter JW, Chow J, et al. Impact of a virtual culinary medicine curriculum on biometric outcomes, dietary habits, and related psychosocial factors among patients with diabetes participating in a food prescription program. Nutrients. 2021;13(12):4492. doi:10.3390/nu13124492
28. Poulton G, Antono A. A taste of virtual culinary medicine and lifestyle medicine—an online course for medical students. Am J Lifestyle Med. 2022;16(1):57–60. doi:10.1177/15598276211046558
29. Razavi AC, Latoff A, Dyer A, et al. Virtual teaching kitchen classes and cardiovascular disease prevention counselling among medical trainees. BMJ Nutr Prev Health. 2023;e000477. doi:10.1136/bmjnph-2022-000477
30. Monlezun DJ, Kasprowicz E, Tosh KW, et al. Medical school-based teaching kitchen improves HbA1c, blood pressure, and cholesterol for patients with type 2 diabetes: results from a novel randomized controlled trial. Diabetes Res Clin Pract. 2015;109(2):420–426. doi:10.1016/j.diabres.2015.05.007
31. Penn L, Ryan V, White M. Feasibility, acceptability and outcomes at a 12-month follow-up of a novel community-based intervention to prevent type 2 diabetes in adults at high risk: mixed methods pilot study. BMJ Open. 2013;3(11):e003585. doi:10.1136/bmjopen-2013-003585
32. Reicks M, Kocher M, Reeder J. Impact of cooking and home food preparation interventions among adults: a systematic review (2011–2016). J Nutr Educ Behav. 2018;50(2):148–172.e1. doi:10.1016/j.jneb.2017.08.004
33. Stauber Z, Razavi AC, Sarris L, Harlan TS, Monlezun DJ. Multisite medical student–led community culinary medicine classes improve patients’ diets: machine learning–augmented propensity score–adjusted fixed effects cohort analysis of 1381 subjects. Am J Lifestyle Med. 2022;16(2):214–220. doi:10.1177/1559827619893602
34. Flego A, Herbert J, Waters E, et al. Jamie’s ministry of food: quasi-experimental evaluation of immediate and sustained impacts of a cooking skills program in Australia. PLoS One. 2014;9(12):e114673. doi:10.1371/journal.pone.0114673
35. Hasan B, Thompson WG, Almasri J, et al. The effect of culinary interventions (cooking classes) on dietary intake and behavioral change: a systematic review and evidence map. BMC Nutr. 2019;5(1):29. doi:10.1186/s40795-019-0293-8
36. Farmer N, Touchton-Leonard K, Ross A. Psychosocial benefits of cooking interventions: a systematic review. Health Educ Behav. 2018;45(2):167–180. doi:10.1177/1090198117736352
37. Kwon J, Yoshida Y, Yoshida H, Kim H, Suzuki T, Lee Y. Effects of a combined physical training and nutrition intervention on physical performance and health-related quality of life in prefrail older women living in the community: a randomized controlled trial. J Am Med Dir Assoc. 2015;16(3):263.e1–263.e8. doi:10.1016/j.jamda.2014.12.005
38. Jyväkorpi SK, Pitkälä KH, Kautiainen H, Puranen TM, Laakkonen ML, Suominen MH. Nutrition education and cooking classes improve diet quality, nutrient intake, and psychological well-being of home-dwelling older people – a pilot study. Eur Geriatr Med. 2013;4(S1):S130. doi:10.1016/j.eurger.2013.07.428
39. Silver JK, Finkelstein A, Minezaki K, et al. The impact of a culinary coaching telemedicine program on home cooking and emotional well-being during the COVID-19 pandemic. Nutrients. 2021;13(7):2311. doi:10.3390/nu13072311
40. Barak-Nahum A, Haim LB, Ginzburg K. When life gives you lemons: the effectiveness of culinary group intervention among cancer patients. Soc Sci Med. 2016;166:1–8. doi:10.1016/j.socscimed.2016.07.046
41. Asher RC, Shrewsbury VA, Bucher T, Collins CE. Culinary medicine and culinary nutrition education for individuals with the capacity to influence health related behaviour change: a scoping review. J Hum Nutr Diet. 2022;35(2):388–395. doi:10.1111/jhn.12944
42. Newman C, Yan J, Messiah SE, Albin J. Culinary medicine as innovative nutrition education for medical students: a scoping review. Acad Med. 2023;98(2):274–286. doi:10.1097/ACM.0000000000004895
43. Monlezun DJ, Dart L, Vanbeber A, et al. Machine learning-augmented propensity score-adjusted multilevel mixed effects panel analysis of hands-on cooking and nutrition education versus traditional curriculum for medical students as preventive cardiology: multisite cohort study of 3248 trainees over 5 years. BioMed Res Int. 2018;2018:1–10. doi:10.1155/2018/5051289
44. Magallanes E, Sen A, Siler M, Albin J. Nutrition from the kitchen: culinary medicine impacts students’ counseling confidence. BMC Med Educ. 2021;21(1):88. doi:10.1186/s12909-021-02512-2
45. Hauser ME. A novel culinary medicine course for undergraduate medical education. Am J Lifestyle Med. 2019;13(3):262–264. doi:10.1177/1559827619825553
46. Kakareka R, Stone TA, Plsek P, Imamura A, Hwang E. Fresh and savory: integrating teaching kitchens with shared medical appointments. J Altern Complement Med. 2019;25(7):709–718. doi:10.1089/acm.2019.0091
47. Delichatsios HK, Hauser ME, Burgess JD, Eisenberg DM. Shared medical appointments: a portal for nutrition and culinary education in primary care—a pilot feasibility project. Glob Adv Health Med. 2015;4(6):22–26. doi:10.7453/gahmj.2015.060
48. Wood NI. A hands‐on curriculum for teaching practical nutrition. Med Educ. 2019;53(5):520–521. doi:10.1111/medu.13837
49. Wood NI, Gleit RD, Levine DL. Culinary nutrition course equips future physicians to educate patients on a healthy diet: an interventional pilot study. BMC Med Educ. 2021;21(1):280. doi:10.1186/s12909-021-02702-y
50. Eisenberg DM, Imamura A. Teaching kitchens in the learning and work environments: the future is now. Glob Adv Health Med. 2020;9:216495612096244. doi:10.1177/2164956120962442
51. Sidorsky T, Huang Z, Dinulos JGH. A business case for shared medical appointments in dermatology: improving access and the bottom line. Arch Dermatol. 2010;146(4). doi:10.1001/archdermatol.2010.32
52. Cunningham SD, Sutherland RA, Yee CW, et al. Group medical care: a systematic review of health service performance. Int J Environ Res Public Health. 2021;18(23):12726. doi:10.3390/ijerph182312726
53. Albin JL, Siler M, Kitzman H. Culinary medicine econsults pair nutrition and medicine: a feasibility pilot. Nutrients. 2023;15(12):2816. doi:10.3390/nu15122816
54. Culinary Medicine Specialist Board. Certification for Healthcare Professionals (CCMS). Available from: https://culinarymedicine.org/certified-culinary-medicine-specialist-program/why-get-certified/.
55. Begley A, Gallegos D. Should cooking be a dietetic competency? Nutr Diet. 2010;67(1):41–46. doi:10.1111/j.1747-0080.2010.01392.x
56. Webb D. Culinary Medicine. Todays Dietit. 2023;25(1):16–21.
57. Del Coro K, Topol J. About us culinary nutrition collaborative. Available from: https://www.culinarynutritioncollaborative.com/about.
58. National Center for Chronic Disease Prevention and Health Promotion. Health and economic costs of chronic diseases. Atlanta, GA: Centers for Disease Control and Prevention; 2022. Available from: https://www.cdc.gov/chronicdisease/about/costs/index.htm.
59. Shanafelt TD, West CP, Dyrbye LN, et al. Changes in burnout and satisfaction with work-life integration in physicians during the first 2 years of the COVID-19 pandemic. Mayo Clin Proc. 2022;97(12):2248–2258. doi:10.1016/j.mayocp.2022.09.002
60. The Associated Press-NORC Center for Public Affairs Research. Support for greater government role in health care for older adults. Chicago, IL: The Associated Press-NORC Center for Public Affairs Research; 2022. Available from: https://apnorc.org/wp-content/uploads/2022/09/APNORC_TSF_July22_topline-POSTED.pdf.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.