")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 16
Pharmacoeconomic Evaluation of Costs of Myelomeningocele and Meningocele Treatment and Screening
Authors Hoxha M , Malaj V, Zappacosta B, Firza N
Received 4 October 2023
Accepted for publication 18 January 2024
Published 9 February 2024 Volume 2024:16 Pages 69—80
DOI https://doi.org/10.2147/CEOR.S443120
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Dean Smith
Malvina Hoxha,1 Visar Malaj,2,3 Bruno Zappacosta,1 Najada Firza4,5
1Department of Chemical-Toxicological and Pharmacological Evaluation of Drugs, Catholic University Our Lady of Good Counsel, Tirana, Albania; 2Department of Economics, University of Tirana, Tirana, Albania; 3CERGE-EI, Center for Economic Research and Graduate Education-Economics Institute, Prague, Czech Republic; 4Department of Economics and Finance, University of Bari ”Aldo Moro”, Bari, Italy; 5Department of Economics and Business, Catholic University Our Lady of Good Counsel, Tirana, Albania
Correspondence: Malvina Hoxha, Tel +355-42-273-290, Email [email protected]
Background: The prevention of myelomeningocele (MMC) and meningocele (MC) is a public health concern. A systematic review on economic factors associated with MMC and MC can help the policy makers to evaluate the cost-effectiveness of screening and treatment. To our knowledge, this is the first systematic review to provide up-to date pharmacoeconomic evidence of all economic studies present in literature on different aspects of MMC and MC.
Methods: We searched in the National Health Service Economic Evaluation Database (NHSEED), PubMed, Cost-effectiveness Analysis Registry (CEA Registry), Centre for Reviews and Dissemination (CRD), Health Technology Assessment Database (HTAD), Cochrane Library, and Econlit. The PRISMA guidelines were followed in the search and evaluation of literature. Only articles in English not limited by the year of publication that fulfilled the eligibility criteria were included in this systematic review.
Results: Nineteen papers were included in the study. The studies were very heterogeneous and reported a comparison of the costs between prenatal versus postnatal repair, the cost of fetoscopic approach versus open surgery, the cost of ventriculoperitoneal shunting (VPS) versus endoscopic third ventriculostomy (ETV), and ETV with choroid plexus cauterization (ETV/CPC), the cost of hospitalization, and the cost of diagnosis for MMC.
Conclusion: The results of this study can help in implementing new policies in different countries to assist MC and MMC patients with the cost of treatment and screening.
Keywords: cost, myelomeningocele, meningocele, neural tube defects, pharmacoeconomic
Background
The neural tube, which is the precursor of the brain and spinal cord, is formed by a series of events, known as neurulation.1,2 Neural tube defects (NTDs), caused by a defect in the closure of the embryonic neural tube, are a major cause of neonatal mortality and morbidity.3 NTDs are associated with folate intake, obesity, age, and genetic factors. In many countries the fortification of wheat and maize flour with folic acid has become mandatory to prevent neural tube defects. Spina bifida is a form of NTD that results from a defect of primary neurulation, and affects one in every 1000 births in Europe.1,4 This condition is caused by problems in the closure of the neural tube, respectively from failure of fusion in the caudal region of the neural tube that results in an opening everywhere along the spine. This process causes severe neurological problems due to damage of the spinal cord and nerves. There are three types of spina bifida, respectively: myelomeningocele (MMC), meningocele (MC), and spina bifida occulta. Neurogenic bladder dysfunction is a major cause of morbidity in patients with spina bifida.5
Myelomeningocele is the most common form of neural tube defect, a life-threatening condition that can bring about serious disabilities. In MMC the neural tissue, spinal cord, and meninges are completely exposed due to the lack of soft tissue, skin and bone.6 The majority of MMC fetuses develop the Arnold–Chiari malformation and hydrocephalus. Cognitive dysfunction, lower extremities paralysis, increased intracranial pressure, sleep apnea, and dysphagia are some of the symptoms that bring MMC patients to shunt insertion.6,7 In MMC patients, urinary and fecal incontinence is another potential problem that should be evaluated. Assessing serum creatinine helps in protecting the kidneys of these patients.8 Pre- or post-natal surgery combined with ventricular shunt are the MMC treatment alternatives. Being overweight is also a frequent problem that patients affected by MMC face.
Meningocele is another type of neural tube defect detected in middle-age adults,9,10 characterized by an anomalous paravertebral cystic mass, formed as a result of a defect in the vertebral body, or by herniation of leptomeninges into an intervertebral foramen.9 Although MC and MMC are very similar from a macroscopical point of view, MC is not associated with hydrocephalus and Chiari type II malformation.11 In MC the spinal cord is not involved in the protrusion.11 Patients with meningocele are characterized by a normal function of the brain, and usually do not have neurologic problems, sphincter dysfunction, and deformity of the lower extremities.11,12 The prognosis of MC patients is outstanding, with a surgical correction,13 compared to MMC that is characterized by poor prognosis and lower survival rates.14
Meningoencephalocele (MEC), or frontoethmoidal meningocele, commonly present in some countries of southeast Asia, is caused by a defect in the posterior part of the spine, when the spinal fluid-filled sac protrudes. Herniation of the meninges, cerebrospinal fluid, and parts of the anterior frontal lobes, are the result of a defect in the frontal and ethmoidal bones in the skull.15 There are three types of meningoencephalocele, classified according to the site of herniation, namely nasofrontal, nasoorbital, and nasoethmoidal.16 The deformity in the face, usually in the eye, and nose are not usually correlated to neurological problems. Different studies evidence the presence of meningoencephalocele in Cambodia, Vietnam, Burma, and other southeast Asian countries.17 Thu et al revealed that aflatoxin, present in the rice taken by pregnant women, may have a role in the metabolism of folic acid, and can cause MEC. Patients with MEC can have epiphora, amblyopic eyes, neurological complications, and serious social and educational consequences.18,19
Different studies report the cost of treatment or screening in MC and MMC, including the cost of the fetoscopic approach versus open surgery, the cost between prenatal versus postnatal repair, or the comparison of different procedures, such as ventriculoperitoneal shunting, and endoscopic third ventriculostomy. The prenatal MMC repair is either cost-effective or cost saving ($2,066,778 per 100 cases repaired), compared to postnatal myelomeningocele repair.20 The aim of our study is to provide up-to-date pharmacoeconomic evidence of the economic studies present in literature on myelomeningocele and meningocele that can help the policy makers to evaluate the cost-effectiveness of MMC and MC screening and treatment.
Methods
This systematic review followed the Preferred Reporting Items for Systematic Reviews (PRISMA) guidelines to identify economic evaluation studies on both myelomeningocele and meningocele.
Literature Search and Presentation of the Full Search Strategies for All Databases
We searched in the National Health Service Economic Evaluation Database (NHSEED), PubMed, Cost-effectiveness Analysis Registry (CEA Registry), Centre for Reviews and Dissemination (CRD), Health Technology Assessment Database (HTAD), Cochrane Library, and Econlit using the following texts “myelomeningocele”, “meningocele”, “economic evaluation”, “health economic”, “cost analysis”, “cost-effectiveness analysis”, “direct cost”, “indirect cost”, “cost utility”, “cost benefit”. Only articles in English, not limited by the year of publication, were included in this systematic review. Reviews, systematic reviews, posters, abstracts, and letters to the editor were not included in this study. Two of the reviewers (BZ, MH) independently screened all the articles.
Eligibility
Studies that reported cost-effectiveness, cost-utility, cost-minimization, and cost-benefit analysis were considered eligible, either if they reported full or partial economic evaluation in costs and outcomes. Studies that did not report data on health economics were excluded. Articles that reported cost-effectiveness and cost benefit analysis on the management of MMC and MC performed in different countries were included in this paper. All articles that described the MMC and MC symptomatology and social burdens with no economic interventions for treatment or screening were excluded.
Intervention
The interventions were kept broad, and all screening and treatment strategies were included.
Comparators
Cost of screening (tomography scan, magnetic resonance imaging), cost of surgery (fetoscopic surgical approach, open repair MMC, prenatal/postnatal MMC repair, ventriculoperitoneal shunting), and cost of hospitalization were used as interventions/comparators. No screening strategy was also used as a comparator.
Synthesis (Methods)
The studies were classified into two different tables, MC, and MMC economic studies, respectively. Both reviewers (MH and BZ) checked the results of each study to guarantee the quality of data. Discrepancies were double checked and discussed between MH and BZ.
Data Extraction
A total of 576 articles were initially identified, of which 19 were selected for inclusion in our systematic review. We extracted several data from the studies, including country of publication, duration, target group, population, study type, discount rate, incremental cost-effectiveness ratios (ICERs), quality adjusted life years (QALY), time range, and outcomes.
Results
Overview of Selected Studies
We identified a total number of 576 records, of which 356 were eliminated as duplicates (Figure 1). Reviews, systematic reviews, poster presentation, and other studies that did not report either full or partial economic evaluation of MMC and MC were excluded (n = 65). Only 19 studies met the inclusion criteria.
 |
Figure 1 PRISMA flow diagram of literature search and selection for articles included in this systematic review. *Studies not eligible excluded based on their abstracts. **Abstracts, conference papers, reviews, systematic reviews, posters, protocols, and letters to the editors were excluded. |
The studies were very heterogeneous, and a summary of all eligible articles are reported in Table 1 and Table 2. The country where the studies were performed, year of publication, population, intervention duration, study design, outcomes, perspectives, ICER/QALY/disability-adjusted life year (DALY) were different.
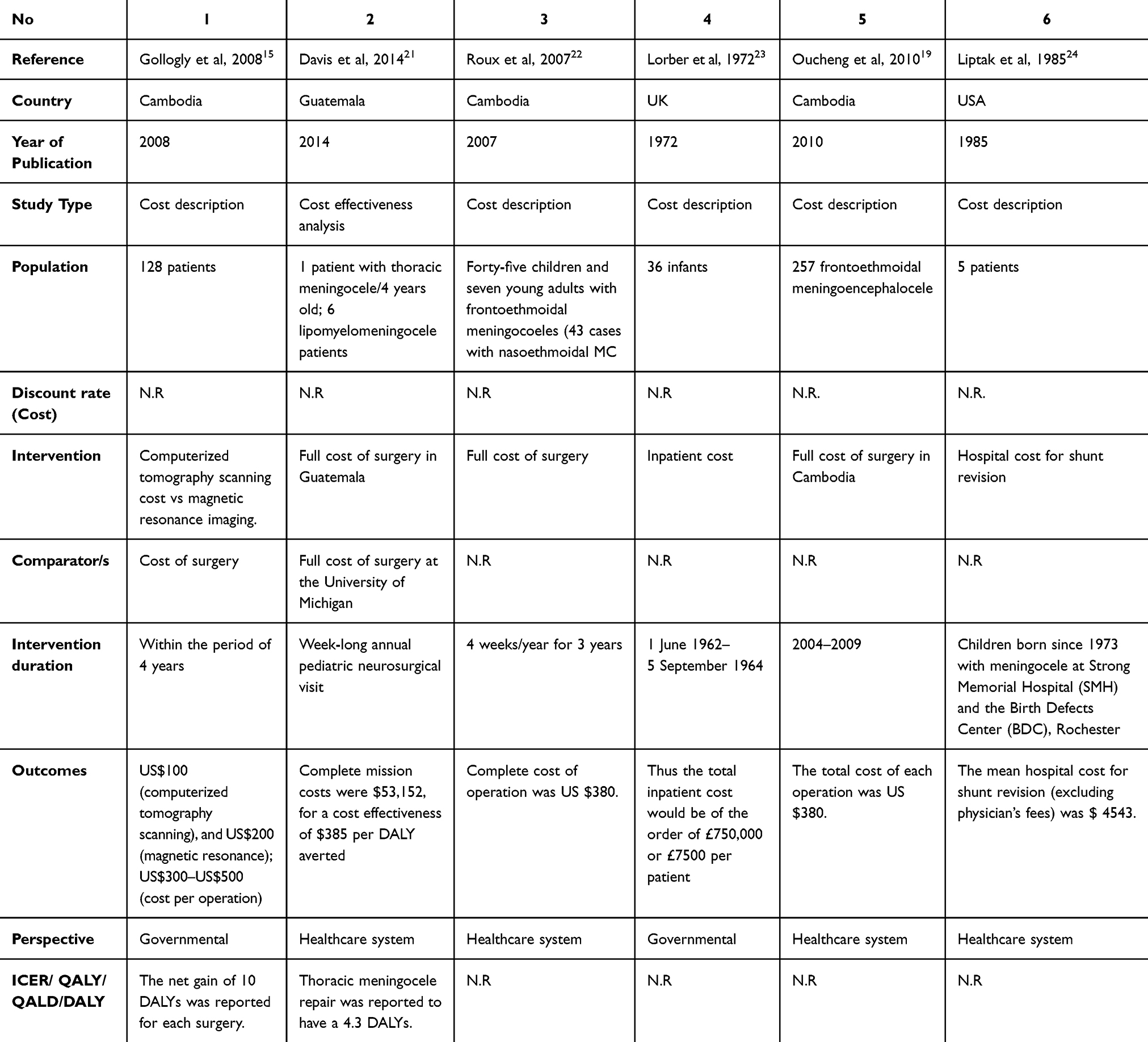 |
Table 1 An Overview of All the Economic Studies on the Meningocele Included in This Review |
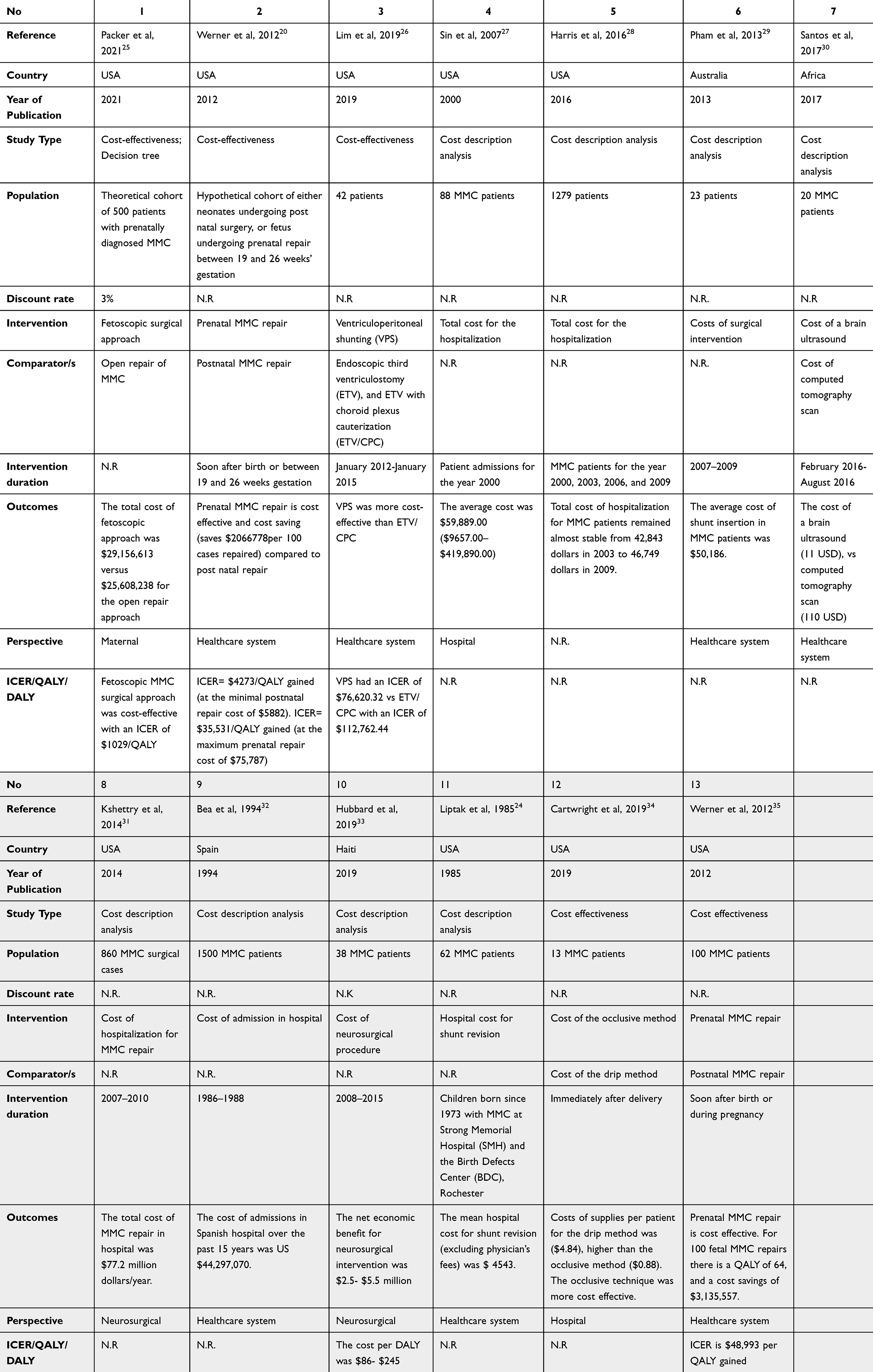 |
Table 2 An Overview of All the Economic Studies on the Myelomeningocele Included in This Review |
Meningocele
Only six studies meet the eligibility criteria. three studies were carried out in Cambodia,15,19,22 one in Guatemala,21 one in the UK,23 and one in the USA.24 The time of publications varied from 1985 to 2014, and the currency reported is US$ and £. The disability adjusted life years (DALYs) were reported in two studies.15,21 There is a lack of health economic data reported in the last years. Only one study reported a cost effectiveness analysis.
Gollogly et al, cost description study, reported the cost of surgery in 128 patients operated within 4 years in different periods. In addition, the study showed that the costs of imaging, respectively computerized tomography scanning, and magnetic resonance, necessary for the understanding of the disease, were: US$100, and US$200, respectively.15 The cost for frontoethmoidal meningoencephalocele (MEC) operations varied from US$300 to US$500 in Cambodia, resulting in a net gain of 10 or more disability adjusted life years (DALYs).15 The cost of foreign surgical teams assisting the Cambodian doctors was also reported and included travel, accommodation, and living expenses. The cost of surgery for MEC (US$380) was also reported in Oucheng et al, study performed in Cambodia in a larger cohort (257 examined patients, versus 200 treated ones).19 The same cost of operation $380 (US dollars) was also reported in Roux et al, study, which also showed the cost of $90 (US dollars) for the computed tomography scanning in Cambodia. Once again, this study showed that the lack of skilled neurosurgeons limits the treatment of patients with MEC. All of the studies reported the same surgical techniques, similar costs of operation, as well as pointed out the importance of training local surgeons to perform the operation in Cambodia, rather than transferring these patients abroad, which was very expensive considering the surgical and hospital charges, respectively US$70,000/patient in USA, US$35,000/patient in Canada, and US$20,000 each for four patients treated in Singapore.15 These results outline the benefits of offering foreign expertise in training local Cambodian staff, and adapting to local conditions, which is very important for the treatment and follow-up of a larger number of patients.
In line with these findings, a cost effectiveness study reported the cost of surgery in Guatemala for patients with thoracic meningocele, lipomyelomeningocele, and myelomeningocele.21 The surgery was provided by a foreign neurosurgical team in Guatemala. Thoracic meningocele repair was reported to have a 4.3 DALYs, versus 10.4 DALYs for each ventriculoperitoneal shunt calculated. For a cost/effectiveness of $385 per DALY the full mission costs were $53,152 in Guatemala, versus $679,427 for a cost effectiveness of $4920 per DALY averted at the University of Michigan.21 In addition, the authors reported that the respective DALY averted ($385) can be compared with the cost-effectiveness ratios in a trauma hospital in Cambodia of a short-term orthopedic surgical brigade ($77.40 per DALY averted).21,36,37 Although the surgery was paid by the foreign surgeons team in Guatemala, the patients spent around $226 (range, $36-$538) for the travel, food and accommodation, and lost wages, which is a significant fee for patients with very low-income.21
Another study reported the hospital cost for shunt revision in the USA.24 Children born since 1973 with meningocele at Strong Memorial Hospital (SMH) and the Birth Defects Center (BDC), Rochester, USA were studied. Shunt failure is a serious issue that is related to expensive hospital stays, loss of function, and increased rates of mortality and morbidity.24 In 1982 the mean hospital cost for nine days of stay for the shunt revision was $ 4543.24
Earlier, another study performed in the UK in 270 cases with spina bifida, of which 36 with meningocele, reported that the total inpatient cost would be around £7500 per patient.23 Moreover, this cost increases considering the outpatient cost, such as the travelling, usually from long distance and by ambulance (around £50/child/journey), the cost of therapy, orthopaedic and renal instruments, and other necessary items.23 The average cost per children per year, including either hospital treatment cost, or schooling cost would be £3000.23 This cost-description study reports the cost for children with spina bifida, either with MMC or MC. We must emphasize that the study was performed many years ago, hence new studies showing the actual inpatient and outpatient cost, separately for each of the categories, for either MMC or MC should be carried out.
Myelomeningocele
Thirteen studies that reported the pharmacoeconomic evidence of MMC patients were identified (Table 2). One study was inserted in both tables as it reported data either for MMC or meningocele patients.24
Only one study reported a discount rate of 3%.25 Of the 13 eligible papers, 38.5% used a cost-effectiveness analysis (n = 5).25,26,34,35 Eight studies employed a cost description analysis,24,27–33 and only one study reported a decision tree model.25 The time range of publications varied from 1985 to 2021. Nine (69.2%) studies were carried out in the USA,24–28,31,34,35 one in Australia,29 one in Africa,30 one in Spain,32 and one in Haiti.33
Packer et al reported that in a theoretical cohort of 500 patients, the fetoscopic surgical approach cost more than the open repair approach of MMC, however it was cost-effective with an incremental cost effectiveness ratio (ICER) of $1029 per QALY.25
Werner et al showed that prenatal surgical repair of MMC is cost saving (saves $2,066,778 per 100 cases repaired), and cost effective compared to postnatal repair.20
In a cohort of 42 MMC American patients, where hydrocephalus was secondary to a myelomeningocele diagnosis, three corrective techniques, namely ventriculoperitoneal shunting (VPS), endoscopic third ventriculostomy (ETV), and ETV with choroid plexus cauterization (ETV/CPC), were analyzed by conducting a cost-effectiveness study. VPS was more cost-effective (ICER of $76,620.32) than ETV/CPC (ICER $112,762.44).26 Pham et al showed that the average cost of shunt insertion in MMC Australian patients was $50,186.29
Sin et al reported that the average cost of hospitalization for MMC patients was $59,889.00 ($9657.00 – $419,890.00).27 In line with this study, sixteen years later, Harris et al reported that the total cost of hospitalization for MMC patients remained almost stable from $42,843 in 2003 to $46,749 in 2009.28 The cost of admission for MMC patients has also been reported in a Spanish study.32 The cost of MMC repair in hospital was also reported in other studies.31,33
In terms of imaging used for diagnosis, the cost of a brain ultrasound (11 USD) and computed tomography scan (110 USD) was reported in a cost descriptive study carried out in Tanzania.30
Cartwright et al demonstrated that among two techniques used to cover the defect of MMC neonates until surgery, the occlusive technique in which a sterile saline gauze was used and covered with an occlusive transparent dressing was more cost-effective than the dripp method, where a saline sterile solution was dripped in a gauze to cover the MMC defect.34
Discussion
This systematic review is the first to report a summary of all health economics data on MMC and MC. The studies were very heterogeneous and report the economic evaluation of different aspects of MMC and MC; one study reported a comparison of the costs between prenatal versus postnatal repair, another study reported the fetoscopic approach versus open surgery, two other studies reported an economic confrontation of three procedures, respectively ventriculoperitoneal shunting (VPS) versus endoscopic third ventriculostomy (ETV), and ETV with choroid plexus cauterization (ETV/CPC), two studies report the cost of hospitalization in MMC, another study reports the cost of diagnosis for MMC. The majority of the studies on MC reported the cost of surgery and hospitalization.
A few studies were based on the same principle, the acquired experience from foreign neurosurgeons have been conducted also in other countries of southeast Asia, such as in Papua New Guinea, however without reporting any cost.38 These studies were not included in our paper.
Magnetic resonance and computerized tomography scanning are essential tools for evaluating the lesions.
The open fetal surgery, first tried in the 1970s and 1980s, requires great surgical skills and organizational resources to reduce the risks for both fetus and mother.39 The first human case of prenatal closure of fetal MMC took place in the 1990s at the Vanderbilt University, Tennessee.40,41 MOMS trial outcome brought about an increased number of fetal surgeries.42 Fetoscopic surgery has shown lower risks compared to the open fetal surgery approach in MMC patients. Despite fetoscopic surgery being more costly than open fetal surgery, it also has benefits on future pregnancies, and long term outcomes in respect to the preterm birth risk, or uterine rupture.25
The postnatal surgical repair should be performed immediately after birth (within 0–2 days to reduce the risk of nerve damage). The longer the period is delayed, the higher is the risk of meningitis and other problems.43,44 However we must also consider the postoperative complications such as leakage of cerebrospinal fluid, hydrocephalus, double incontinence, wound infection, etc. Studies have shown that prenatal MMC repair is cost-saving, saving either $2,066,778 or $3,135,557 per 100 cases repaired, compared to post natal repair.20,35 In addition, prenatal surgical repair is also cost effective, with a QALY of 64 for 100 fetal MMC repairs.35
The treatment of MMC was revolutionized by the shunt development.43 MMC patients go through multiple surgeries; however there are many cases of failure, or ventriculoperitoneal shunt infections. The alleviation of the burden on families and on the healthcare system is a major public health concern. The earliest study reporting the mean hospital cost of $ 4543 for the shunt revision excluding the physician’s fees for a mean of nine days of stay in the hospital, was published in 1985. Twenty eight years later, the average cost of shunt insertion in patients with MMC in Australia was reported to be $50,186.29 Each ventriculoperitoneal shunt was shown to avert 10.4 DALYs.21 In addition, it was shown that VPS is also a cost-effective procedure compared to ETV/CPC (ICER of $76,620.32 versus ICER $112,762.44 respectively).26
The studies reported are heterogeneous in terms of intervention and comparators. Moreover, the time of publication varies considerably, and outcomes provided are different. ICER and DALY were only reported in a few studies. Despite the heterogeneity of the data, we can conclude that prenatal MMC repair is cost-saving and cost effective compared to postnatal repair. Despite being more costly than open fetal surgery, fetoscopic surgery, has significant benefits on future pregnancies and long term outcomes. In addition, VPS is a cost-effective procedure compared to ETV/CPC.
Conclusion
There are many limitations in this review, including the quality of data, which is very heterogeneous and not recent. The information should not only be updated, but also studies should be performed in many countries. Language is also a limitation; the search was restricted only to articles published in English. The lack of the risk of bias and of health economic findings with unfavorable results is also a significant limitation.
There are still evidence gaps that need to be addressed, and we believe that it would be of great interest to report updated cost economic evaluations of the current cost of MMC and MC in different countries, which may help in implementing new policies to help not only patients in their cost of treatment (orthopedic, neurological, urological, physical, psychological), but also their families.
Abbreviations
MC, meningocele; MEC, meningoencephalocele; MMC, myelomeningocele; NTD, Neural tube defects.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests for this work.
References
1. Mitchell LE, Adzick NS, Melchionne J, Pasquariello PS, Sutton LN, Whitehead AS. Spina bifida. Lancet. 2004;364(9448):1885–1895. doi:10.1016/S0140-6736(04)17445-X
2. Werner JM, Negesse MY, Brooks DL, et al. Hallmarks of primary neurulation are conserved in the zebrafish forebrain. Commun Biol. 2021;4(1):147. doi:10.1038/s42003-021-01655-8
3. Botto LD, Moore CA, Khoury MJ, Erickson JD. Neural-tube defects. N Engl J Med. 1999;341(20):1509–1519. PMID: 10559453. doi:10.1056/NEJM199911113412006
4. Gulve K, Kuchewar V. Spina bifida: a rare clinical image. Pan Afr Med J. 2022;42:258.
5. Snow-Lisy DC, Yerkes EB, Cheng EY. Update on urological management of spina bifida from prenatal diagnosis to adulthood. J Urol. 2015;194(2):288–296.
6. Maassel N, Farrelly J, Coman D, et al. Diffusion weighted imaging as a biomarker of retinoic acid induced myelomeningocele. PLoS One. 2021;16(6):e0253583. doi:10.1371/journal.pone.0253583
7. Naidich TP, McLone DG, Fulling KH. The Chiari II malformation: part IV. The hindbrain deformity. Neuroradiology. 1983;25(4):179–197. doi:10.1007/BF00540232
8. Jackson MJ, N’Dow J, Pickard R. The importance of patient-reported outcome measures in reconstructive urology. Curr Opin Urol. 2010;20(6):495–499. doi:10.1097/MOU.0b013e32833cf4a5
9. Park JW, Jeong WG, Lee JE, et al. Pictorial review of mediastinal masses with an emphasis on magnetic resonance imaging. Korean J Radiol. 2021;22(1):139–154. PMID: 32783412; PMCID: PMC7772375. doi:10.3348/kjr.2019.0897
10. Miles J, Pennybacker J, Sheldon P. Intrathoracic meningocele. Its development and association with neurofibromatosis. J Neurol Neurosurg Psychiatry. 1969;32:99–110. doi:10.1136/jnnp.32.2.99
11. Avagliano L, Massa V, George TM, Qureshy S, Bulfamante GP, Finnell RH. Overview on neural tube defects: from development to physical characteristics. Birth Defects Res. 2019;111(19):1455–1467. doi:10.1002/bdr2.1380
12. McComb JG. A practical clinical classification of spinal neural tube defects. Childs Nerv Syst. 2015;31(10):1641–1657. doi:10.1007/s00381-015-2845-9
13. Nethi S, Arya K. Meningocele. StatPearls [Internet]. Treasure Island (FL):StatPearls Publishing; 2023; Available from: https://www.ncbi.nlm.nih.gov/books/NBK562174/.
14. Alruwaili AA, Das M, Myelomeningocele J. StatPearls [Internet]. Treasure Island (FL):StatPearls Publishing; 2023. Available from: https://www.ncbi.nlm.nih.gov/books/NBK546696/.
15. Gollogly J, Oucheng N, Lauer G. Frontoethmoidal meningoencephalocoele repair in Cambodia: outcomes and cost comparisons. Trop doctor. 2008;38(3):167–170. doi:10.1258/td.2007.070124
16. Samii M, Draf W. Surgery of malformations of the anterior skull base. In: Samii M, Draf W, editors. Surgery of the Skull Base. Berlin: Springer-Verlag; 1989:114–126.
17. Suwanwela C, Sukabote C, Suwanwela N. Frontoethmoidal encephalomeningocele. Surgery. 1971;69:617–625.
18. Pinzer T, Lauer G, Gollogly J, Schackert G. A complex therapy for treatment of frontoethmoidal meningoencephalocele in a developing third world country: neurosurgical aspects. J Neurosurg. 2006;104(5 Suppl):326–331. doi:10.3171/ped.2006.104.5.326
19. Oucheng N, Lauwers F, Gollogly J, et al. Frontoethmoidal meningoencephalocele: appraisal of 200 operated cases. Journal of Neurosurgery. Pediatrics. 2010;6(6):541–549. doi:10.3171/2010.9.PEDS1043
20. Werner EF, Han CS, Burd I, et al. Evaluating the cost-effectiveness of prenatal surgery for myelomeningocele: a decision analysis. Ultrasound Obstet Gynecol. 2012;40(2):158–164. doi:10.1002/uog.11176
21. Davis MC, Than KD, Garton HJ, et al. Cost effectiveness of a short-term pediatric neurosurgical brigade to Guatemala. World Neurosurg. 2014;82(6):974–979. doi:10.1016/j.wneu.2014.08.038
22. Roux F-E, Lauwers F, Oucheng N, et al. Treatment of frontoethmoidal meningoencephalocele in Cambodia: a low-cost procedure for developing countries. J Neurosurg. 2007;107(1 Suppl):11–21. doi:10.3171/PED-07/07/011
23. Lorber J. Spina bifida cystica. Results of treatment of 270 consecutive cases with criteria for selection for the future. Arch Dis childhood. 1972;47(256):854–873. doi:10.1136/adc.47.256.854
24. Liptak GS, Masiulis BS, McDonald JV, et al. Ventricular shunt survival in children with neural tube defects. Acta neurochirurgica. 1985;74(3–4):113–117. doi:10.1007/BF0141879
25. Packer CH, Hersh AR, Caughey AB. Fetoscopic compared with open repair of myelomeningocele: a 2-delivery cost-effectiveness analysis. Am J Clin Exp Obstet Gynecol. 2021;3(6):100434. doi:10.1016/j.ajogmf.2021.100434
26. Lim J, Tang AR, Liles C, et al. The cost of hydrocephalus: a cost-effectiveness model for evaluating surgical techniques. J Neurosurg Pediatr. 2023;23(1):109–118. doi:10.3171/2018.6.PEDS17654
27. Sin AH, Rashidi M, Caldito G, et al. Surgical treatment of myelomeningocele: year 2000 hospitalization, outcome, and cost analysis in the US. Childs Nerv Syst. 2007;23(10):1125–1127. doi:10.1007/s00381-007-0375-9
28. Harris DA, Cherian J, LoPresti M, et al. Trends in epidemiology and hospitalization utilization for myelomeningocele repair from 2000 to 2009. Childs Nerv Syst. 2016;32(7):1273–1279. doi:10.1007/s00381-016-3091-5
29. Pham ACQ, Fan C, Owler BK, et al. Treating pediatric hydrocephalus in Australia: a 3-year hospital-based cost analysis and comparison with other studies. J Neurosurg Pediatr. 2013;11(4):398–401. doi:10.3171/2013.1.PEDS12233
30. Santos MM, Rubagumya DK, Dominic I, et al. Infant hydrocephalus in sub-Saharan Africa: the reality on the Tanzanian side of the lake. J Neurosurg Pediatr. 2017;20(5):423–431. doi:10.3171/2017.5.PEDS1755
31. Kshettry VR, Kelly ML, Rosenbaum BP, et al. Myelomeningocele: surgical trends and predictors of outcome in the United States, 1988–2010. J Neurosurg Pediatr. 2014;13(6):666–678. doi:10.3171/2014.3.PEDS13597
32. Bea Muñoz M, Diaz Llopis I, Martinez Agullo E, et al. A multicentre study of the hospital care of 1500 patients with myelomeningocele. Paraplegia. 1994;32(8):561–564. doi:10.1038/sc.1994.88
33. Hubbard ZS, Shah AH, Ragheb M, et al. Economic benefit of neurosurgical intervention for infant hydrocephalus in Haiti. J Neurosurg Pediatr. 2019:1–9. doi:10.3171/2019.4.PEDS18563
34. Cartwright CC, Igbaseimokumo U, Olsen S, et al. A comparison of dressing techniques for presurgical closure of myelomeningocele in the Neonate. J Neurosci Nurs. 2019;51(5):217–220. doi:10.1097/JNN.0000000000000461
35. Werner EF, Lipkind H, Copel JA, et al. A cost effective analysis of prenatal surgery for myelomeningocele.
36. Gosselin RA, Gialamas G, Atkin DM. Comparing the cost-effectiveness of short orthopedic missions in elective and relief situations in developing countries. World J Surg. 2011;35:951–955. doi:10.1007/s00268-010-0947-9
37. Gosselin RA, Heitto M. Cost-effectiveness of a district trauma hospital in Battambang, Cambodia. World J Surg. 2008;32:2450–2453. doi:10.1007/s00268-008-9708-4
38. Rosenfeld JV, Watters DAK. Surgery in developing countries. J Neurosurg Pediatr. 2008;1(1):108. doi:10.3171/PED-08/01/108
39. van Lith JM, Johnson MP, Wilson RD. Current controversies in prenatal diagnosis 3: fetal surgery after MOMS: is fetal therapy better than neonatal? PrenatDiagn. 2013;33(1):13–16. PMID: 23296715. doi:10.1002/pd.4037
40. Tulipan N, Bruner JP. Myelomeningocele repair in utero: a report of three cases. Pediatr Neurosurg. 1998;28(4):177–180. doi:10.1159/000028645
41. Radic JA, Illes J, McDonald PJ. Fetal repair of open neural tube defects: ethical, legal, and social issues. Camb Q Healthc Ethics. 2019;28(3):476–487. doi:10.1017/S0963180119000409
42. Adzick NS, Thom EA, Spong CY, et al. A randomized trial of prenatal versus postnatal repair of myelomeningocele. N Engl J Med. 2011;364(11):993–1004. doi:10.1056/NEJMoa1014379
43. Macnab GH. The development of the knowledge and treatment of hydrocephalus. Dev Med Child Neurol. 1966;8(suppl 11):1–9.
44. Watson JC, Tye G, Ward JD. Delayed repair of myelomeningoceles. World Neurosurg. 2014;81(02):428–430. doi:10.1016/j.wneu.2013.01.022
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.