")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 20
Perspectives from Adults with Tourette Syndrome on Research Priorities and Registry Development: A Focus Group Study
Authors Isaacs DA , Bonnet K , Eckland MR, Markowitz K , Pena M, Schlundt DG
Received 3 October 2023
Accepted for publication 27 December 2023
Published 9 February 2024 Volume 2024:20 Pages 257—269
DOI https://doi.org/10.2147/NDT.S442131
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Richard J Porter
David A Isaacs,1,2 Kemberlee Bonnet,3 Michelle R Eckland,1 Kimberly Markowitz,4 Maria Pena,5 David G Schlundt3
1Department of Neurology, Vanderbilt University Medical Center, Nashville, TN, USA; 2Department of Pediatrics, Division of Pediatric Neurology, Monroe Carell Jr. Children’s Hospital at Vanderbilt, Nashville, TN, USA; 3Department of Psychology, Vanderbilt University, Nashville, TN, USA; 4Department of Neuroscience, Vanderbilt University, Nashville, TN, USA; 5College of Nursing, University of Florida, Gainesville, FL, USA
Correspondence: David A Isaacs, Department of Neurology, Vanderbilt University Medical Center, 1161 21st Ave South, A-0118 MCN, Nashville, TN, 37232, USA, Tel +1 615 936.2025, Fax +1 615 936 1229, Email [email protected]
Purpose: Adults with Tourette syndrome (TS) have worse mental health, physical health, and quality of life than the general population. The factors contributing to negative outcomes across multiple health domains in adults with TS remain uncertain, in part due to a lack of longitudinal studies in this population. In attempt to address these knowledge gaps, our center has initiated development of a regional registry for adults with TS. During the goal-setting and design phase of registry development, we conducted focus groups with adults with TS to identify research issues of greatest importance to this population and to obtain feedback on design and implementation of an adult TS registry.
Patients and Methods: Participants were recruited from a tertiary care adult TS clinic and from institutional research registries. Focus groups were conducted online and were moderated by a qualitative research expert. Qualitative data analysis was performed using an iterative inductive/deductive approach.
Results: Across four focus groups, adult TS participants (n=22) expressed a variety of research priorities, including developing more effective treatments for tics, identifying risk factors for tic persistence into adulthood, clarifying the interaction between TS symptoms and women’s health, clarifying the relationships between TS and other mental and physical health disorders, and addressing day-to-day living issues. Focus group participants were generally enthusiastic about creation of an adult TS registry. They indicated that adults with TS are more likely to engage with a registry that logistically accommodates participants (eg, by offering a wide range of visit times, by providing telehealth options) and that fosters bidirectional interaction (eg, by disseminating results regularly, by involving participants in registry design and implementation, by notifying participants of support resources).
Conclusion: Focus group input clarifies the research priorities of adults with TS and will inform the ongoing development of an adult TS registry.
Keywords: tic disorder, patient registry, neurodevelopmental disorder, movement disorder
Introduction
Tourette syndrome (TS) is a neurodevelopmental disorder that affects 0.3–1% of the global population.1 TS is clinically defined by the presence of motor and vocal tics, with onset of tics in childhood and persistence of tics for more than one year.1 Tics typically first emerge between 4–8 years of age, peak in severity between 10–14 years of age, and diminish in severity during later adolescence,1 though tics rarely remit completely.2 Focusing on the natural history of tics, one might assume the impact of TS lessens in adulthood. However, as many as one-third of individuals with TS continue to experience bothersome tics into adulthood.3 Moreover, mounting evidence reveals widespread mental,4,5 social,6–8 and physical7,9 health impairment among the adult TS population. Lifetime prevalence rates of mood disorders, anxiety disorders, obsessive-compulsive disorder (OCD), and attention-deficit/hyperactivity disorder (ADHD) for adults with TS are 60%, 40%, 55%, and 36%, respectively.4 One-third of adults with TS report inadequate support from their families,8 and at least 40% avoid social situations because of tics.7 Relative to the general population, adults with TS are at heightened risk of cardiovascular disease,10 metabolic disorders,10 autoimmune disorders,11 accidents,12 suicide,13 substance abuse,14 and global perceived disability.7 Furthermore, adults with TS have a 1.8-fold higher risk of premature death compared to the general population, even after controlling for comorbid psychiatric diagnoses.9 The combined burden of poor mental, social, and physical health likely contributes to the poor quality of life repeatedly observed in adult TS samples.5,15
The factors contributing to negative outcomes across multiple health domains in adults with TS remain uncertain, in part due to a lack of longitudinal investigations in this population. Health outcomes data for adults with TS have been predominantly obtained from cross-sectional studies4,6–8,16 and electronic health record-based cohort studies.9,10,12–14 Several longitudinal studies have followed children with TS into adulthood,2 but adult follow-up assessments in these studies were conducted at a single timepoint and focused primarily on tic severity and psychiatric diagnoses commonly comorbid with TS.17–24 Critically, for most of these longitudinal studies, participant mean age at follow-up was younger than 25 years,17–24 notable since, per biologically-informed conceptions of development, adulthood begins around 25 years of age.25 Of the two longitudinal studies with mean age at assessment older than 25 years, both were exclusively survey-based.26,27 Thus, knowledge of the evolution of core TS symptoms in adulthood remains limited, and even less is known about the broader mental, social, and physical health trajectories in this population. Longitudinal investigations involving repeated, comprehensive biopsychosocial assessments of adults with TS are crucial to expand understanding of the TS phenotype and to identify risk factors for poor health and quality of life in this population.
In attempt to address gaps in our knowledge of the health and quality of life of this population, our center initiated development of a longitudinal, patient-centered registry for adults with TS in 2022. The Agency for Healthcare Research and Quality (AHRQ) defines a patient registry as “an organized system that uses observational study methods to collect uniform data (clinical and other) to evaluate specified outcomes for a population defined by a particular disease, condition, or exposure, and that serves one or more predetermined scientific, clinical, or policy purposes”.28 Two TS-focused registries currently exist that enroll adults: the Calgary Adult Tic Disorders Registry29 and the International Deep Brain Stimulation Registry and Database for TS.30 The former collects clinical outcomes at baseline and again at 12 months, but longer-term outcomes are not collected;29 the latter collects outcomes in the small subset of patients with refractory TS who have undergone deep brain stimulation.30 To our knowledge, no patient-centered registry exists that collects longer-term outcome for the broader adult TS community. During the initial goal-setting and design phase of registry development, our center sought input from adults with TS, in accord with recommendations from the AHRQ31 and the Patient-Centered Outcomes Research Institute (PCORI).32 Prior studies investigating the research priorities of adults with TS have been restricted to survey-based methods,33 but such methods do not afford the same qualitative insights as focus group discussions.34 We thus conducted a series of focus groups with adults with TS to achieve two aims: 1) identify research issues of greatest importance to this population and 2) obtain feedback on design and implementation of an adult TS registry.
Materials and Methods
Recruitment Methods
Focus group participants were recruited from our institution’s Adult Tourette Syndrome Clinic and from institutional research registries in January and February 2022. Eligibility criteria for participation included: confirmed diagnosis of TS, chronic motor tic disorder, or chronic vocal tic disorder, based on Diagnostic and Statistical Manual of Mental Disorders, 5th Edition criteria; age 18 years or older; capacity to provide verbal informed consent; and English fluency. Notably, TS, chronic motor tic disorder, and chronic vocal tic disorder exist on a single clinical spectrum.35 Eligible individuals were approached about study participation during face-to-face encounters, by telephone call, and/or by email. All participants were previously interviewed and examined by a movement disorders neurologist (D.I.) as part of routine clinical care and/or other research initiatives.
Focus Group Logistics
The desired size for each focus group was pre-set at 4–10 participants, with anticipated need for 4–6 focus groups to achieve thematic saturation based on focus group methodology recommendations34 and research.36 Focus groups were conducted online, via Zoom. The date and time of focus group sessions were determined in advance, and eligible participants selected a session based on their availability. The number of participants in each focus group was arbitrary, being determined by the number of participants who opted for that particular focus group session. Prior to each focus group session, participants were sent an email with information about the topics to be discussed (see Supplementary Material 1). This email also contained a participant-specific hyperlink to a Research Electronic Data Capture (REDCap)37 survey with questions concerning demographic and clinical information. Each focus group lasted 90 minutes and was moderated by a trained expert (K.B. or D.S.) from the Vanderbilt Qualitative Research Core. The moderator used a script to guide each session (see Supplementary Material 2). The script was developed by members of the research team prior to study recruitment. Script content was derived from clinical knowledge of TS and from federal guidelines on patient-centered research.31,32 The script provided background information on TS, motivations for establishing an adult TS registry, and a series of open-ended questions about research priorities for TS (aim 1) and design and implementation of an adult TS registry (aim 2). The moderator asked follow-up questions for clarity purposes and to facilitate detailed discussion. A TS specialist (D.I.), with established clinical and/or research relationships with each of the participants, was present for all focus group sessions to address TS-specific questions or concerns raised by participants. Sessions were audio-recorded to permit dialogue transcription. After four focus groups were conducted, the study team convened to discuss unique and common themes across the sessions, and it was determined that thematic saturation had been achieved and no additional focus groups were warranted.
Data Analysis
Data analysis and results are reported per the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines.38 Focus group session audio files were submitted to an IRB-approved transcription service (rev.com). Transcripts, quotations, and codes were managed using Microsoft Excel 2016 and SPSS version 28.0. We used an iterative inductive/deductive approach to qualitative data analysis,39–41 developing a hierarchical coding system based on preliminary review of transcripts (inductive) and moderator script questions (deductive). Major coding system categories included living with TS, quality of life, coping with TS, emotions and feelings, experience with the health system, characterization of treatments, barriers and facilitators, attitudes and beliefs, communication, results/status of registry or studies, registry elements, registry involvement, specific examples, suggestions, and clarifying questions (see Supplementary Material 3). Most major categories were further divided into subcategories, with some subcategories having additional levels of hierarchical division. Definitions and rules were written for use of coding categories. Each transcript statement was treated as a separate quote and could be assigned multiple different codes. Two experienced qualitative coders coded each focus group transcript, comparing their results and reconciling any discrepancies. Analysis was based on reconciled codes. Focus group participants did not provide feedback on results of the qualitative analysis.
The study was approved by the Vanderbilt Institutional Research Board (IRB) and was conducted in accordance with the 1964 Declaration of Helsinki and its later amendments. All participants verbally consented to the study and to publication of anonymized responses; participants waived the right to document written consent. The verbal consent process was approved by the Vanderbilt IRB. Participants were compensated $50 for their time and effort.
Results
Twenty-two individuals (12 men, 10 women) participated across four focus groups. The cohort was predominantly non-Hispanic, white (91%). Demographic and clinical characteristics of the participant sample are presented in Table 1.
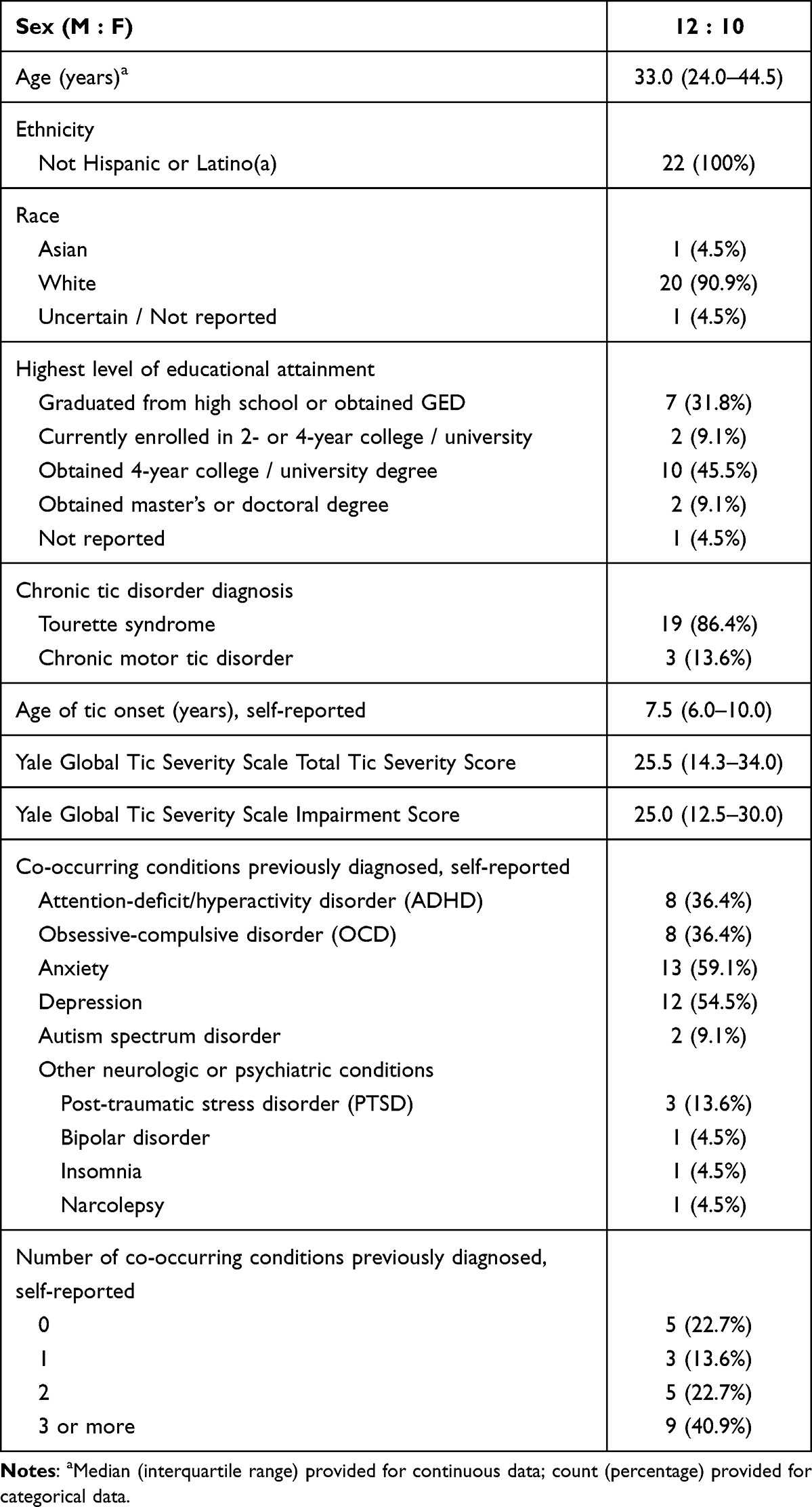 |
Table 1 Clinical Characteristics of Focus Group Participants |
The two overarching thematic categories were research priorities of adults with TS (aim 1) and registry design and implementation features likely to promote engagement of adults with TS (aim 2). In the remainder of the results, we will discuss each theme and its subcategories and illustrate the discussion with participant quotes.
Theme 1: Research Priorities
Participants perceived that much remained unknown about TS at multiple levels of inquiry, ranging from the disorder’s neurobiological basis to the clinical care of affected individuals. Participants expressed a variety of priorities for TS research, including clarifying disorder mechanisms, developing more effective treatments for tics, predicting long-term clinical trajectories and short-term symptom exacerbations, clarifying the interrelationship between TS and other conditions, and addressing practical day-to-day living issues.
Mechanisms and Treatments
Several participants preferred researchers to focus on clarifying the etiology of TS and, in doing so, to develop more effective treatments:
I honestly do think one of the most important questions is where [Tourette syndrome] starts and where it comes from…I’ve noticed my three-year-old cousin is starting to show some of the same symptoms that I had when I was three…So figuring out where it comes from and having something for him, or even to stop it at a younger age, like to help him…[avoid] the situations that we’ve all had to go through and endure. (Participant 3.3, Female, Age 18)
I would love to know what causes it…[T]hat’s the main question…[I]f we knew that, I feel like we’d kind of figure out how to treat it properly. And that’s…the biggest thing right now is we don’t really know how to treat it. (Participant 3.4, Male, Age 34)
Clinical Trajectories and Tic Fluctuations
The following participants prioritized research that examines why tic severity diminishes during adolescence for some individuals with TS but not for others:
Is there any relationship between the age of onset or when your symptoms start becoming more… severe, and whether you outgrow it, or whether it continues to get worse as you age…? (Participant 4.1, Female, Age 50)
[M]ine’s actually gotten worse over time….I don’t think as an adult, it gets better. I feel like I get new or worsening tics. Kind of like per month they’ll change, or I’ll get…a different one…[I] want to know why a new one starts…[o]r what causes that. (Participant 3.1, Female, Age 27)
Many participants expressed interest in identifying the factors that ameliorate or exacerbate their tics:
[I]s there something that makes your tics temporarily go away? I go to [a camp for children and adolescents with tic disorders] and we have kids with these amazing talents and they say, ‘Yeah, I work on it really hard because it’s the only time I get relief.’ And a lot of it’s music, instruments, singing, dancing, art. They’re very creative, and I know I experienced this, and I know a lot of my friends with Tourette’s experience just this one activity that is just their passion and their tics temporarily go away. (Participant 2.4, Female, Age 19)
I’d be curious to know what the role of nutrition and exercise and things like that are in improving or not the tic disorder. (Participant 2.1, Male, Age 43)
I went through a lot of what could be triggering all of my tics. I went through the month-long trial, no meat for a month, no plastics, didn’t touch anything. No makeup, no sugars, no alcohol, no anything. Just trying to see what would possibly make it a little bit better, a little bit worse. Nothing really fixed anything which was disappointing. (Participant 4.7, Female, Age 43)
I think a big thing to ask is people’s environments, does that contribute to making it worse? A stressful day, stressful job, people around you, judgmental people, people staring at you. Does that actively make it worse? I mean, if you’re home all the time and nobody’s really interacting with you, does it help get better? Does it calm you down? (Participant 3.4, Male, Age 34)
Multiple female participants discussed the need for research focusing on the relationship between TS symptoms and women’s health:
I’ve started into perimenopause, and I’m really finding…, as my hormonal levels are changing and shifting around, that my Tourette syndrome is also changing and shifting quite a bit…[T]here’s so little research…about adults, period, [and particularly about] adult women [with Tourette syndrome], especially in that period of life. I just, I wish I understood more, what was happening with how my hormones are dealing with my Tourette and how those all sort of play nice or not so nice with each other during this time. (Participant 1.3, Female, Age 45)
I definitely noticed an increase in symptoms around the time of my period, my menstrual cycle. I would love to see more research on that. Could hormone replacement therapy be a therapy? (Participant 4.1, Female, Age 50)
Interrelationship Between TS and Other Disorders
Many participants struggled with other mental and physical health disorders and expressed a desire to understand the connection between these disorders and TS:
I’d [like] to hear some questions related to mood disorders…such as depression. How it’s connected with Tourette. Is it the same kind of depression? Does it have the same duration? Is it lifelong? (Participant 1.5, Male, Age 65)
I have huge structural issues. Like, arthritis in my neck, arthritis in my lower back and all sorts of structural issues in my hip. And I know they have to be tic-related, but I also have some minor scoliosis. And so there’s always the question of whether my tics are causing it or the discomfort that I’m in is causing the tics. Like, which came first type of questions…That’s something I’d be very curious to know more about. (Participant 1.3, Female, Age 45)
As per the moderator script, focus group participants were informed during the session that individuals with TS have an increased risk of metabolic and cardiovascular disorders.10 One participant indicated a need for further research identifying the reasons adults with TS have worse physical health outcomes:
This whole idea of having comorbidities that occur later in life like heart disease…Is it because we’re more likely to overeat to cope with our feelings or is it because we are less likely to take care of ourselves because we’re depressed? I’d be curious to know things like that. (Participant 2.1, Male, Age 43)
Day-to-Day Living Issues
Many participants expressed a desire for practical resources and strategies to better navigate work, relationships, and other aspects of daily living:
I would be interested in studies…for adults with Tourette’s…of coping mechanisms. Not just psychological coping mechanisms, but practical, logistical life hacks for people with Tourette’s. How do you get through the things that are harder for us [than] everyone else. Job interviews, relationships, all these parts of life that are made more difficult. (Participant 4.6, Male, Age 51)
Any kind of research into…how to get around in a workplace. [T]here’s not really structure for a condition [like] mine to where it’s not super predictable, it’s hard to build a schedule or official accommodation around it. It’s not every day or not the [same] severity every day. So, how to be out in the world and be an adult like every other adult in the workplace… (Participant 1.6, Female, Age 27)
I think the most important questions to be asking…are probably the ones…about how it impacts your day-to-day. Because what I’ve learned from speaking with other people and reading, is that my tics impact me probably quite differently or at least somewhat differently than anyone else…And it sounds [like] this is a type of disease or affliction where there’s not necessarily a cure on the horizon. So focusing on how to help an individual patient cope with their specific tics and how they impact them. (Participant 1.2, Male, Age 28)
Theme 2: Registry Design and Implementation
The majority of participants were enthusiastic about an adult TS registry. They believed such a registry would generate knowledge directly relevant to their own lives and to the entire TS community. We will now review focus group participant input regarding select aspects of design and implementation of an adult TS registry.
Registry Visit Logistics
Focus group participants were presented with a tentative registry protocol involving annual study visits, with anticipated visit length of two hours for the first visit and one hour for follow-up visits. Participants indicated this visit frequency and duration seemed reasonable, though they did emphasize the need for flexibility with visit scheduling and location:
I’m a father of four, and…I was just lucky tonight that I didn’t have anything scheduled, but typically I’m at a ball game or something to that nature. So yeah, just [provide]…more [time] options for [people] to be able to do it. (Participant 2.3, Male, Age 40)
This participant suggested pairing registry visits with medical appointments to reduce participant burden:
I think it would be good if we could pair the [registry visit] with our actual appointment. We go once a year or…twice a year. And that way it’s not so much. (Participant 2.1, Male, Age 43)
Many participants commented on their preferences for virtual versus in-person registry visits:
I would be interested in are you all able to do it virtually? Because not everyone can, say, take off work and visit their neurologist. So having a virtual option would make participating easier logistically for the participants…Maybe for the first initial visit…, go to your neurologist…But maybe the follow-ups each year, maybe they could be done virtually as an option in case they can’t drive. Because my neurologist is two hours away and that’s a bit of a trek. (Participant 2.4, Female, Age 19)
I prefer…telehealth…because…I really don’t like driving an hour through…traffic all the way down just for what, like 30 minutes, hour, hour and a half of talking about Tourette’s, twitching more than usual, then driving another hour back. (Participant 2.2, Male, Age 20)
This participant preferred virtual visits because he felt his natural environment would provide a more realistic assessment of his tics:
I…think it should be telehealth because for me, when I’m lying down in my bed, that’s when most of my tics come out. So I think you would get a better result if you do it in [the participant’s] natural habitat. (Participant 3.2, Male, Age 22)
Conversely, this participant felt an in-person visit would be beneficial due to the improved quality of observational data from in-person interaction:
I think there’s definitely a difference for me when I’m on telehealth or I’m in person. When I’m in person, I feel like my tics are worse and you can actually see all the tics and be able to really understand them as opposed to just doing telehealth. (Participant 3.4, Male, Age 34)
Sharing Sensitive Information
Participants were informed, as per the moderator script, that adverse childhood experiences are associated with poor mental and physical health outcomes in adulthood, an association which may have implications for adults with TS.42 The moderator asked focus group participants their level of comfort providing information about adverse childhood experiences to the research team. Participants generally voiced willingness to share such sensitive information, though some indicated this would be contingent on specific factors. This participant wanted to ensure the research team would be trauma-informed:
My concern is making sure that whoever I’m talking to can kind of respond correctly…to hearing about trauma…I definitely think that making sure that there’s…some training with that to make sure that, if someone is going to open up about trauma for research purposes, then they don’t leave feeling maybe triggered or shame or anything like that. (Participant 1.1, Female, Age 23)
This participant expressed a need for an established relationship with the researcher prior to disclosing sensitive information:
I’m…willing to just talk about my experiences openly to people. But I think from a confidentiality standpoint, it would be more beneficial for people to realistically just talk about it with someone…they trust. (Participant 2.2, Male, Age 20)
This participant wanted assurance of confidentiality when sharing information about her childhood:
I didn’t have the best childhood. I don’t have a problem telling people that as long as it doesn’t broadcast…everywhere. (Participant 4.7, Female, Age 43)
Results Dissemination
Participants were asked their degree of interest in receiving personal and/or aggregate (de-identified) registry results periodically. Participants indicated a strong desire for timely feedback that showed their registry data in relation to their peers’ data. Many felt such self-peer comparison would reduce their sense of isolation and foster a sense of community:
I think that would be phenomenal just to see if we’re on a plane with other people that are experiencing the same issues that we are. How many people experience it the way I experience it? How many people with similar tics, or with tics that are not exactly like mine, how do they perceive their daily life or things to that nature? I think that would be a great perception to understand. (Participant 2.3, Male, Age 40)
I like the idea of feedback, however often it happens to be. Even just being in this focus group tonight has been an eye-opener for me…It gives me a little peace. To know there’s a range of this, and there are those [of] us that can hide it and those of us that can’t, those that struggle all day…and get home and just tic for an hour. So seeing how some statistics might play out across all of the participants, I think would be helpful for everybody. (Participant 4.2, Male, Age 42)
If I were to submit a whole bunch of information to you, and then it came back to me where 86% of the people are having the same issue. I don’t feel like I’d feel as alone in my struggles. To go, ‘Oh, okay. So, there are lots of people who are dealing with this. I’m not a freak, or something’s wrong with me.’ It’s a group thing. So yeah, I would be very encouraged to just know where I rank in that, and how everybody else does, too. (Participant 4.7, Female, Age 43)
[S]eeing other people, a pie graph of everyone who participated, what percentage of them are female versus male? How many of them are Caucasian or Asian or Hispanic? It’d be very interesting to see of the community and…what everyone else is like there…[Y]ou can feel like, ‘Oh, it’s just me.’ But if you look at the big picture, 1% is a small percentage, but it’s not a minuscule amount of people that have Tourette’s syndrome. (Participant 2.4, Female, Age 19)
Several focus group participants stated that timely results dissemination would incentivize registry engagement, by instilling in individual registry participants a sense of connection with and contribution to the broader TS community:
I was just thinking that maybe…you could tie in the information people are providing to the results they receive. If I know I’m going to get results about anxiety, I don’t have a problem ranking my anxiety once a week, or once a month. There’s an incentive there for me to continue doing these activities, or these asks, if I know that’s going to result in me learning more about the community and what my place is inside of it. (Participant 4.2, Male, Age 42)
[S]eeing results would make people want to [participate] because it lets them realize how much their information is helping…[I]f you’re just doing this and you never hear about it ever again until the [registry visit the] next year, it might feel pointless…So having maybe a yearly summary of what y’all have learned or something would help people see what their time commitment is going into. (Participant 2.4, Female, Age 19)
This participant commented that dissemination of certain registry results might support individuals’ ability to advocate for their own medical care:
I…would like to see in the summary…what are the most popular treatments for Tourette’s. [W]hat medications or therapies or even surgeries, what are other people doing? Because sometimes doctors don’t know what to do with [people with Tourette syndrome], but they need care. [G]iving them ideas of what to do might be helpful. (Participant 2.4, Female, Age 19)
Involvement of Adults with TS in Registry Design and Implementation
When asked about involvement of adults with TS in registry design and implementation, focus group participants were enthusiastically in favor, indicating that such adult TS involvement would enhance trust in the registry and ensure relevance of registry results to the TS community:
[I]t’s really hard to explain what Tourette’s feels like. So if you know that there’s someone who has Tourette’s and knows what it feels like [involved],…it would help a lot with the trust. (Participant 2.2, Male, Age 20)
I think that’s a good idea having professionals and patients [involved]…I would want to see somebody with Tourette’s that was involved in it…to…help guide along the professionals. It would make me more intrigued to want to do it because there is someone on the team with Tourette’s. (Participant 3.3, Female, Age 18)
I think it’s a good idea to involve people with Tourette’s as it develops, to make sure that the direction that the study is going is still going to be relevant to people who have it. (Participant 4.4, Male, Age 46)
You’re gathering all this information from people like us to move forward, but as dynamic of a thing [as] this…might be, it might be helpful to have the input on a more consistent basis as you’re pivoting from one thing to the next. Maybe it stays the same, maybe it changes, but to have some voices you can draw on to participate in another focus group or to answer questions might be helpful. (Participant 4.2, Male, Age 42)
Notification Options
The moderator informed focus group participants that the registry could potentially serve as a means of notifying participants of other research studies and/or support resources. Regarding the former, participants expressed varied levels of interest in receiving research recruitment notifications from the registry team. This participant described the need for personalization of such notifications:
I think that it should be you can opt in at the start, and then if you are a part of the registry, maybe send something out and let them opt in and out on occasions. I think that would be a nice driving factor for people to join. (Participant 2.3, Male, Age 40)
Participants consistently indicated strong interest in receiving information from the registry team about support resources and social networking opportunities with other adults with TS. Many participants desired social connection and community to help navigate such a stigmatized illness:
One of the things that I hear a lot from other people with Tourette’s, and I feel this is the worst part about Tourette’s, is feeling alone because you’re the only one that tics. There’s 1% of the population, but you don’t know. We’re scattered…[A] lot of people don’t feel they have a…community, and it doesn’t have to be the Tourette’s syndrome community, although that’s really great. I’m lucky I have a great community and they help me exponentially… (Participant 2.4, Female, Age 19)
I would love to have access to other people who are having a similar life experience…Just to talk to other adults like a support group kind of thing. Again, no support groups in my area for adults with Tourette’s… (Participant 4.1, Female, Age 50)
Recruitment of Underrepresented Populations
To increase recruitment of adults with TS from underrepresented populations, focus group participants suggested partnering with advocacy organizations (eg, the Tourette Association of America), health clinics, churches, universities, and civic agencies. Several participants advised recruiting via social media platforms, through online TS support groups and targeted advertisements. Participants noted specific challenges to recruiting individuals from minority populations, rural populations, and populations not receiving regular medical care:
I think this is an interesting problem that you have with recruitment, especially if you’re trying to reach out to a rural community and minority communities, underserved communities, because you’ve got a lot of people who are probably untreated. (Participant 2.1, Male, Age 43)
I’ve worked in healthcare in rural settings…[P]art of the problem is, people don’t go to the doctor, people don’t acknowledge that they have problems…or they [are]…dismissed if they are trying to seek help. So I don’t really know the best way to [reach] them because they either don’t have…the financial resources, the education, or they’re being actively discouraged from [using them]. (Participant 1.6, Female, Age 27)
This participant recommended that individuals within minority populations be recruited by other members of the same minority population:
If you’re trying to recruit people of color, have people of color do the recruiting. If you’re trying to recruit Spanish-speakers, have Spanish-speakers recruit, you know what I mean? It helps to have people from the community do the outreach. (Participant 4.1, Female, Age 50)
Compensation
Participants provided input on financial incentives to motivate registry enrollment and retention. Many participants indicated a willingness to participate in a registry without compensation, though almost all agreed that financial compensation would further incentivize engagement. This participant expressed the need to cover registry visit travel expenses, as the cost of commuting may be prohibitive for some individuals:
[W]hen you’re dealing with underserved populations…, there would have to be some compensation. You may find people need that gas money. It’s very little money for [the medical institution], but it may be a huge deal for the participants in the study. (Participant 2.1, Male, Age 43)
Discussion
In this focus group study, we identified research priorities of adults with TS and obtained feedback on design and implementation of an adult TS registry. We will discuss each of these overarching themes in turn.
Focus group participants expressed numerous research priorities. Frequently discussed priorities included the following: developing more effective treatments for tics, identifying risk factors for tic persistence into adulthood, clarifying the interaction between TS symptoms and women’s health, clarifying the relationships between TS and other mental and physical health disorders, and addressing day-to-day living issues. Many of these priorities appear to align with those of clinical researchers, based on the number of published studies dedicated to these topics in recent decades.2–5,10,11,43–49 Research priorities identified by focus group participants also generally coincide with those identified in the recent survey-based study conducted by Anderson et al across multiple European countries.33 In Anderson et al’s study, respondents were permitted to select multiple research priorities, and of the 725 adult TS participants, 64% desired research into the treatment of TS, and 36% desired research into the etiology of TS.33 Critically, participants in our study, as in Anderson et al’s study,33 emphasized the need for research addressing practical daily living issues. In Anderson et al’s study, 28% of adults with TS ranked daily living issues (“dealing with TS at home, work and school”) as the highest research priority.33 Of all research priorities listed in that study, daily living issues received the largest share of top-priority votes. Over the past two decades, progressively more attention has been devoted to the daily functioning and quality of life of individuals with TS,5,15 but much clinical research continues to focus on tic severity without assessing the broader impact of TS or TS-targeted interventions on daily living. While greater tic severity is linked with worse disability and quality of life in adults with TS,7 non-tic manifestations, particularly psychiatric symptoms, are more strongly associated with quality of life in this population.15,16,50 Ultimately, understanding the diverse research priorities of adults with TS is key to pursuing research that is relevant to this community and that, in turn, promotes research engagement.
An adult TS registry promises to facilitate progress for many of the aforementioned research priorities. Focus group participants in our study were generally enthusiastic about creation of a registry. They perceived significant gaps in the scientific knowledge and clinical care of adults with TS and believed a registry holds potential to begin addressing many of these gaps. Numerous focus group participants supported the registry from a motivation to improve the quality of care and quality of life for themselves and others with TS. Incorporating outcomes devoted to daily living issues and quality of life is essential to an adult TS registry that is truly patient-centered. Moreover, clear communication of such registry priorities to the adult TS community is likely to bolster participant engagement.
Focus group participants indicated multiple other registry features likely to motivate adults with TS to engage with the registry. Participants enthusiastically favored timely results feedback, particularly feedback that compared their individual data to data from other adults with TS in the registry. Multiple participants indicated that such results feedback would reduce their sense of isolation. Another registry feature that garnered widespread support from focus group participants was involvement of adults with TS in registry design and implementation. Participants emphasized that such adult TS involvement would increase their trust in the registry. These participant perspectives on timely results dissemination and patient involvement in registry design and implementation align with recommendations from federal agencies (eg, AHRQ28 and PCORI32) on the conduct of patient-centered research. Iterative, active engagement between researchers and registry participants over time is essential for the registry to remain centered on the priorities of adults with TS, even as those priorities evolve in response to new issues (eg, rise in prevalence of functional tic disorders29) and research (eg, clinical trial findings, registry results). Additional registry features likely to enhance adult TS engagement, per focus group participants, include opportunities to learn about social and support resources, opportunities to learn about other research studies, and financial compensation. Ultimately, a registry that fosters bidirectional interaction between researchers and adults with TS is most likely to address the priorities of all involved.
Focus group participants identified several barriers to adult TS engagement with a registry. Frequently discussed barriers were related to logistical factors. Focus group participants indicated that annual registry visits, one to two hours in duration, would not be overly burdensome, but they noted that the ability of registry researchers to accommodate participants would be key to enrollment and retention. Participants endorsed multiple practical strategies to address scheduling barriers, including pairing registry visits with medical appointments, providing visit time options outside of standard business hours, and offering virtual visits when feasible. Another barrier identified was recruitment of underrepresented populations, specifically minority populations and rural populations, a challenge widely acknowledged across clinical research disciplines.51–54 While focus group participants noted recruitment challenges common to the entire adult TS population (due to, for example, insufficient knowledge about TS in medical and lay communities and stigma associated with the TS diagnosis), they perceived additional impediments to recruiting minority and/or rural populations: lack of healthcare access; inadequate transportation, technological, and financial resources; and mistrust of researchers. Focus group participants emphasized that overcoming such barriers would require close collaboration with national and local organizations, including patient advocacy groups, healthcare facilities, government agencies, and religious communities, as well as creation of a diverse research team to enhance participant diversity, recommendations that align with existing guidelines.28 Notably, participants did not indicate that requests to share sensitive information, such as information about adverse childhood experiences, would deter their participation in the registry, consistent with input from other clinical populations,55,56 but participants did express that disclosure of sensitive information would be contingent on the research team establishing trust and assuring confidentiality.
Our focus group study had several limitations. First, participants were adults with TS who agreed to participate in a virtual focus group so their perspectives may not generalize to adults with TS who are less technologically capable and/or less capable or willing to engage in group discussion. Second, the majority of focus group participants were white, non-Hispanic individuals recruited from a specialty TS clinic so their perspectives may not generalize to a racially diverse and/or non-clinical adult TS population. Last, while key aspects of registry design and implementation were discussed during focus group sessions, other aspects (eg, specific patient-reported outcome measures) were not discussed due to time constraints.
Conclusion
In conclusion, a longitudinal, patient-centered registry promises to address many research priorities of direct relevance to the adult TS community. Adults with TS are more likely to engage with a registry that accommodates their needs and that fosters bidirectional interaction. Focus group input will inform the next stages of registry development.
Ethics Approval and Informed Consent
The study was approved by the Vanderbilt University IRB (study #21210) and was conducted in accordance with the 1964 Declaration of Helsinki and its later amendments. All participants verbally consented and waived the right to document written consent.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Tourette Association of America (072720), the National Center for Advancing Translational Sciences (UL1TR002243), and the National Institute of Neurological Disorders and Stroke (1K23NS131592-01). The funding sources were not involved in study design; data collection, analysis, or interpretation; manuscript preparation; or decision to submit the article for publication.
Disclosure
David Isaacs receives grant funding from Teva Branded Pharmaceutical Products, R&D, Inc. The authors report no other conflicts of interest in this work.
References
1. Cohen SC, Leckman JF, Bloch MH. Clinical assessment of Tourette syndrome and tic disorders. Neurosci Biobehav Rev. 2013;37:997–1007. doi:10.1016/j.neubiorev.2012.11.013
2. Reagan S, Myers NS, McGuire JF. The developmental trajectories and long-term outcomes of childhood Tourette syndrome: a systematic review. Curr Dev Disord Rep. 2022;9:156–168. doi:10.1007/s40474-022-00258-0
3. Bloch MH, Leckman JF. Clinical course of Tourette syndrome. J Psychosom Res. 2009;67:497–501. doi:10.1016/j.jpsychores.2009.09.002
4. Hirschtritt ME, Lee PC, Pauls DL, et al. Lifetime prevalence, age of risk, and genetic relationships of comorbid psychiatric disorders in Tourette syndrome. JAMA Psychiatry. 2015;72:325. doi:10.1001/jamapsychiatry.2014.2650
5. Eapen V, Cavanna AE, Robertson MM. Comorbidities, social impact, and quality of life in Tourette syndrome. Front Psychiatry. 2016;7(97). doi:10.3389/fpsyt.2016.00097
6. Eddy CM, Cavanna AE. Altered social cognition in Tourette syndrome: nature and implications. Behav Neurol. 2013;27:15–22. doi:10.1155/2013/417516
7. Conelea CA. The impact of Tourette syndrome in adults: results from the Tourette syndrome impact survey. Community Ment Health J. 2013;49:110–120. doi:10.1007/s10597-011-9465-y
8. Elstner K, Selai CE, Trimble MR, Robertson MM. Quality of Life (QOL) of patients with Gilles de la Tourette’s syndrome. Acta Psychiatr Scand. 2001;103:52–59. doi:10.1111/j.1600-0447.2001.00147.x
9. Meier SM, Dalsgaard S, Mortensen PB, Leckman JF, Plessen KJ. Mortality risk in a nationwide cohort of individuals with tic disorders and with Tourette syndrome. Mov Disord. 2017;32:605–609. doi:10.1002/mds.26939
10. Brander G, Isomura K, Chang Z, et al. Association of Tourette syndrome and chronic tic disorder with metabolic and cardiovascular disorders. JAMA Neurol. 2019;76:454–461. doi:10.1001/jamaneurol.2018.4279
11. Fernández de la Cruz L, Mataix-Cols D. General health and mortality in Tourette syndrome and chronic tic disorder: a mini-review. Neurosci Biobehav Rev. 2020;119:514–520. doi:10.1016/j.neubiorev.2020.11.005
12. Mataix-Cols D, Brander G, Chang Z, et al. Serious transport accidents in Tourette syndrome or chronic tic disorder. Mov Disord. 2021;36:188–195. doi:10.1002/mds.28301
13. Fernández de la Cruz L, Rydell M, Runeson B, et al. Suicide in Tourette’s and chronic tic disorders. Biol Psychiatry. 2017;82:111–118.
14. Virtanen S, Sidorchuk A, Fernández de la Cruz L, et al. Association of Tourette syndrome and chronic tic disorder with subsequent risk of alcohol- or drug-related disorders, criminal convictions, and death: a population-based family study. Biol Psychiatry. 2021;89:407–414. doi:10.1016/j.biopsych.2020.09.014
15. Evans J, Seri S, Cavanna AE. The effects of Gilles de la Tourette syndrome and other chronic tic disorders on quality of life across the lifespan: a systematic review. Eur Child Adolesc Psychiatry. 2016;25:939–948. doi:10.1007/s00787-016-0823-8
16. Isaacs DA, Riordan HR, Claassen DO. Clinical correlates of health-related quality of life in adults with chronic tic disorder. Front Psychiatry. 2021;12:260. doi:10.3389/fpsyt.2021.619854
17. Ricketts EJ, Woods DW, Espil FM, et al. Childhood predictors of long-term tic severity and tic impairment in Tourette’s disorder. Behav Ther. 2022;53:1250–1264. doi:10.1016/j.beth.2022.07.002
18. Groth C, Mol Debes N, Rask CU, Lange T, Skov L. Course of Tourette syndrome and comorbidities in a large prospective clinical study. J Am Acad Child Adolesc Psychiatry. 2017;56:304–312. doi:10.1016/j.jaac.2017.01.010
19. Shprecher DR, Rubenstein LA, Gannon K, Frank SA, Kurlan R. Temporal Course of the Tourette Syndrome Clinical Triad. Tremor Other Hyperkinet Mov. 2014;4:243.
20. Bloch MH, Peterson BS, Scahill L, et al. Adulthood outcome of tic and obsessive-compulsive symptom severity in children with Tourette syndrome. Arch Pediatr Adolesc Med. 2006;160:65–69. doi:10.1001/archpedi.160.1.65
21. Corbett JA, Mathews AM, Connell PH, Shapiro DA. Tics and Gilles de la Tourette’s syndrome: a Follow@up Study and critical review. Br J Psychiatry. 1969;115:1229–1241. doi:10.1192/bjp.115.528.1229
22. Leckman JF, Zhang H, Vitale A, et al. Course of tic severity in Tourette syndrome: the first two decades. Pediatrics. 1998;102:14–19. doi:10.1542/peds.102.1.14
23. Burd L, Kerbeshian J, Barth A, et al. Long-term follow-up of an epidemiologically defined cohort of patients with Tourette syndrome. 2016;16:431–437. doi:10.1177/088307380101600609
24. Pappert EJ, Goetz CG, Louis ED, Blasucci L, Leurgans S. Objective assessments of longitudinal outcome in Gilles de la Tourette’s syndrome. Neurology. 2003;61:936–940. doi:10.1212/01.WNL.0000086370.10186.7C
25. Sawyer SM, Azzopardi PS, Wickremarathne D, Patton GC. The age of adolescence. Lancet Child Adolesc Health. 2018;2:223–228. doi:10.1016/S2352-4642(18)30022-1
26. Lowe TL, Capriotti MR, McBurnett K. Long-term follow-up of patients with Tourette’s syndrome. Mov Disord Clin Pract. 2019;6:40–45. doi:10.1002/mdc3.12696
27. Byler DL, Chan L, Lehman E, et al. Tourette syndrome: a general pediatrician’s 35-year experience at a single center with follow-up in adulthood. Clin Pediatr. 2015;54:138–144. doi:10.1177/0009922814550396
28. Gliklich R, Leavy M, Dreyer N. Registries for evaluating patient outcomes: a user’s guide, 4th ed; 2020. Available from: https://effectivehealthcare.ahrq.gov/products/registries-guide-4th-edition/users-guide.
29. Pringsheim T, Martino D. Rapid onset of functional tic-like behaviours in young adults during the COVID-19 pandemic. Eur J Neurol. 2021;28:3805–3808. doi:10.1111/ene.15034
30. Deeb W, Rossi PJ, Porta M, et al. The international deep brain stimulation registry and database for Gilles de la Tourette syndrome: how does it work? Front Neurosci. 2016;10:195148. doi:10.3389/fnins.2016.00170
31. Registries for evaluating patient outcomes: a user’s guide; 2020. Available from: https://effectivehealthcare.ahrq.gov/products/registries-guide-4th-edition/users-guide.
32. Sheridan S, Schrandt S, Forsythe L, Hilliard TS, Paez KA. The PCORI engagement rubric: promising practices for partnering in research. Ann Fam Med. 2017;15:165–170. doi:10.1370/afm.2042
33. Anderson SM. European clinical guidelines for Tourette syndrome and other tic disorders: patients’ perspectives on research and treatment. Eur Child Adolesc Psychiatry. 2021. doi:10.1007/s00787-021-01854-y
34. Morgan DL. Focus groups. Annu Rev Sociol. 1996;22:129–152. doi:10.1146/annurev.soc.22.1.129
35. Claudio-Campos K, Stevens D, Koo SW, et al. Is persistent motor or vocal tic disorder a milder form of Tourette syndrome? Mov Disord. 2021;36:1899–1910. doi:10.1002/mds.28593
36. Guest G, Namey E, McKenna K. How many focus groups are enough? Building an evidence base for nonprobability sample sizes. Field Methods. 2017;29:3–22. doi:10.1177/1525822X16639015
37. Harris PA, Taylor R, Thielke R, et al. Research electronic data capture (REDCap)-A metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42:377–381. doi:10.1016/j.jbi.2008.08.010
38. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Heal Care. 2007;19:349–357. doi:10.1093/intqhc/mzm042
39. Fereday J, Muir-Cochrane E. Demonstrating rigor using thematic analysis: a hybrid approach of inductive and deductive coding and theme development. Int J Qual Methods. 2006;5:80–92. doi:10.1177/160940690600500107
40. Azungah T. Qualitative research: deductive and inductive approaches to data analysis. Qual Res J. 2018;18:383–400. doi:10.1108/QRJ-D-18-00035
41. Tjora A. Qualitative Research as Stepwise-Deductive Induction. Routledge; 2018.
42. Yang K, Essa A, Noriega D, et al. Relationship between adverse childhood experiences and symptom severity in adult men with Tourette syndrome. J Psychiatr Res. 2022;155:252–259. doi:10.1016/j.jpsychires.2022.08.024
43. Garris J, Quigg M. The female Tourette patient: sex differences in Tourette disorder. Neurosci Biobehav Rev. 2021;129:261–268. doi:10.1016/j.neubiorev.2021.08.001
44. Ganos C, Martino D, Pringsheim T. Tics in the pediatric population: pragmatic management. Mov Disord Clin Pract. 2017;4:160–172. doi:10.1002/mdc3.12428
45. Pringsheim T, Okun MS, Müller-Vahl K, et al. Practice guideline recommendations summary: treatment of tics in people with Tourette syndrome and chronic tic disorders. Neurology. 2019;92:896–906. doi:10.1212/WNL.0000000000007466
46. Yang C, Kang BY, Yu D, Zhao L, Zhang L. Effectiveness and safety of a clonidine adhesive patch for children with tic disorders: study in a real-world practice. Front Neurol. 2020;11:361. doi:10.3389/fneur.2020.00361
47. Dreison KC, Lagges AM. Effectiveness of the comprehensive Behavioral Intervention for Tics (CBIT) in a pediatric psychiatry clinic: a retrospective chart review. Clin Pract Pediatr Psychol. 2017;5:180–185.
48. Kompoliti K, Goetz CG, Leurgans S, Raman R, Comella CL. Estrogen, progesterone, and tic severity in women with Gilles de la Tourette syndrome. Neurology. 2001;57:1519. doi:10.1212/WNL.57.8.1519
49. Lewin AB, Murphy TK, Storch EA, et al. A phenomenological investigation of women with Tourette or other chronic tic disorders. Compr Psychiatry. 2012;53:525–534.
50. Huisman‐van Dijk HM, Matthijssen SJMA, Stockmann RTS, Fritz AV, Cath DC. Effects of comorbidity on Tourette’s tic severity and quality of life. Acta Neurol Scand. 2019;140:390–398. doi:10.1111/ane.13155
51. Paskett ED, Reeves KW, McLaughlin JM, et al. Recruitment of minority and underserved populations in the United States: the centers for population health and health disparities experience. Contemp Clin Trials. 2008;29:847–861. doi:10.1016/j.cct.2008.07.006
52. Yancey AK, Ortega AN, Kumanyika SK. Effective recruitment and retention of minority research participants. Ann Rev Public Health. 2006;27:1–28. doi:10.1146/annurev.publhealth.27.021405.102113
53. Lim CS, Follansbee-Junger KW, Crawford MS, Janicke DM. Treatment outcome research in rural pediatric populations: the challenge of recruitment. J Pediatr Psychol. 2011;36:696–707. doi:10.1093/jpepsy/jsr018
54. Dibartolo MC, McCrone S. Recruitment of rural community-dwelling older adults: barriers, challenges, and strategies. Aging Mental Health. 2010;7:75–82. doi:10.1080/1360786031000072295
55. Flanagan T, Alabaster A, McCaw B, et al. Feasibility and acceptability of screening for adverse childhood experiences in prenatal care. J Womens Health 277 903–911 (2018).
56. Rariden C, SmithBattle L, Yoo JH, Cibulka N, Loman D. Screening for adverse childhood experiences: literature review and practice implications. J Nurse Pract. 2021;17:98–104. doi:10.1016/j.nurpra.2020.08.002
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.