")
Back to Journals » Risk Management and Healthcare Policy » Volume 13
Perioperative Medical Emergencies in a 23-Hour Surgical Procedure Unit
Authors De Zylva J , Osborn K
Received 30 June 2020
Accepted for publication 28 September 2020
Published 3 November 2020 Volume 2020:13 Pages 2439—2447
DOI https://doi.org/10.2147/RMHP.S268938
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Joseph De Zylva, Kym Osborn
Department of Anaesthesia, Lyell McEwin Hospital and Modbury Public Hospital, Northern Adelaide Local Health Network, Adelaide, South Australia, Australia
Correspondence: Joseph De Zylva
Department of Anaesthesia, Lyell McEwin Hospital and Modbury Public Hospital, Northern Adelaide Local Health Network, Haydown Road, Elizabeth Vale SA 5112, Adelaide, South Australia, Australia
Tel +61 8 8182 9806
Fax +61 8 8182 9830
Email [email protected]
Purpose: Our 174-bed hospital operates a 23-hour/day procedure unit without a dedicated on-site high dependency unit or intensive care unit. The purpose of this investigation is to assess the incidence of medical emergency response (MER) and Code Blue (CB) events over 12 months.
Patients and Methods: A retrospective analysis of hospital records was conducted. Patients were identified using the medical emergency team (MET) database. Information pertaining to whether the patient was pre-operative, post-operative (including time and characteristics of the operation), or medical short stay overflow was obtained, in addition to the reason for the MER/CB event and outcome of the event.
Results: Of all hospital events, 8.45% (47 of 550) occurred in the perioperative ward. The incidence rate of events was 0.76% (95% CI: 0.53% to 0.99%) of all scheduled operations. The surgical procedure cancellation rate due to pre-operative MER/CB events was 0.11% (95% CI: 0.02% to 0.20%). Orthopedic surgery and ENT surgery were associated with the highest incidence of MER/CB events. Post-operative hypotension and reduced consciousness associated with vasovagal episodes were the most common clusters. The mean time after the operation for events to occur was 5.21 hours. 25.5% of events occurred outside of standard day surgery operating hours when there was limited access to onsite consultant anaesthetic or surgical staff (17:00 to 08:00).
Conclusion: This study highlights the anticipated medical emergencies for a 23-hour procedural unit and is of particular interest for evaluation by other short stay surgical, outpatient procedural, or rural hospital surgical units with limited after hours on-site critical care support.
Keywords: medical emergency response, critical care, perioperative, 23-hour surgical
Introduction
The implementation of an in-hospital medical emergency team (MET) has shown to improve the detection of deteriorating patients, thereby preventing cardiac arrests and unanticipated intensive care unit (ICU) or high dependency unit (HDU) admissions.1,2 The MET team is generally summoned in response to abnormal vital sign observations recorded by nursing staff as part of a rapid response system.3
Our 174-bed acute care teaching public hospital has an emergency department, inpatient units including short stay medical, rehabilitation, geriatrics and palliative care. In addition, there is a 23-hour surgical procedure unit with four operating theatres and a procedural room. Our hospital does not currently have the facilities to manage patients requiring ICU or HDU level care. Patients requiring these admissions are transported to our partnered tertiary hospital, 14 kilometres away. The surgical unit has recorded 5381 indexed admissions for procedures in 2019.
Our hospital has a two-tiered medical emergency response (MER) system. The MET team consists of a medical registrar, medical intern/resident, MET nurse and hospital clinical nursing lead. This team attends in response to escalation of care from abnormal vital signs recorded on the Rapid Detection and Response (RDR) observation chart (Figure 1). The Code Blue team consists of the aforementioned team plus a second MET nurse and an airway trained medical officer from the emergency department. In tertiary hospital centers, this position is generally fulfilled by an ICU registrar ± anesthetics support. A Code Blue (CB) is an imminent medical emergency in response to criteria outlined in Table 1. The criteria for MER call or CB is in concordance with guidelines from the Australian Commission on Safety and Quality in Healthcare.4 The hospital MET subcommittee monitors data from all emergency response incidents occurring within the hospital boundary and meets on a monthly basis for the purpose of quality control, evaluation and feedback. This is concordant with recommendations from the Third International Consensus on Rapid Response Systems, which recommends ten metrics related to structure, process and outcomes of rapid response systems to maintain critical evaluation, feedback and improvement.5
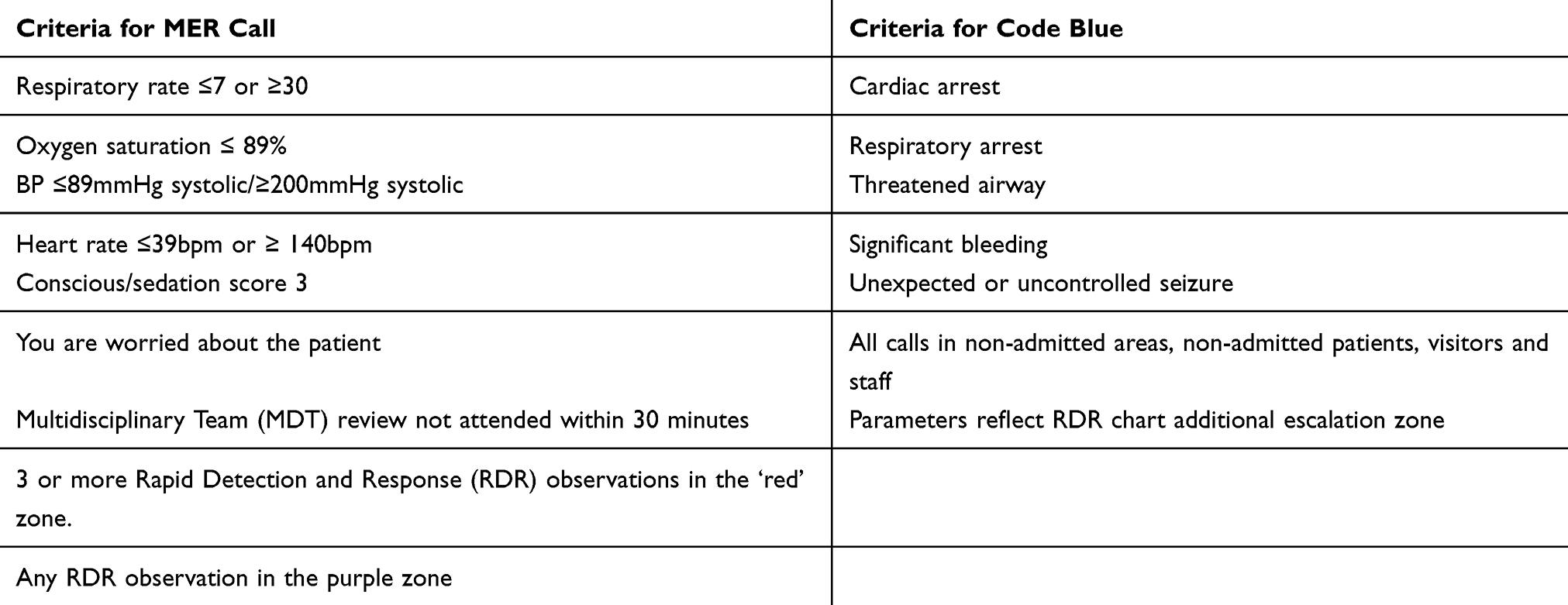 |
Table 1 Criteria for Initiating a Medical Emergency Response (MER) Call vs a Code Blue |
 |
Figure 1 Rapid Detection and Observation (RDR) charts used in in this hospital. |
The purpose of this investigation is to evaluate the reasons for medical emergency response (MER) incidents in the perioperative setting, which may assist in future evaluation for a high dependency unit, identification of patients at greatest risk of requiring a medical emergency response and training or availability of staff to respond to these incidents.
Aim
To identify the incidence of MER/CB events in a 23-hour perioperative unit. To identify the most commonly associated MER/CB criteria used by hospital staff to declare these events.
Method
Criteria for Inclusion
Population
Any person in whom a MER/CB event was triggered
Time
January to December 2019
Location
Twenty-three-hour surgical unit
Criteria for Exclusion
Patients who meet any of the following criteria are deemed unsuitable for treatment at this 23-hour unit and are referred to a partnered tertiary hospital:
- Body Mass Index (BMI) ≥ 50.
- American Society of Anesthesiologists Physical Status Classification (ASA) ≥ 4.
- Pediatric surgery, neurosurgery, cardiology and cardiothoracic surgery, vascular surgery, obstetrics.
- Operations where high dependency or intensive care level monitoring are routinely required or anticipated.
Perioperative Screening
All patients complete a detailed pre-operative assessment questionnaire once they are placed on the surgical waiting list. The obtained information includes any medical conditions, past procedures, medication, functional status and discharge arrangements. Patients subsequently receive a phone call from a pre-operative nurse to confirm the details of the questionnaire which is used to screen for patients who require an outpatient assessment by an anesthetist and ensure suitability for the procedure at the facility.
Data Collection and Analysis
A retrospective audit was performed. Patients were identified using the MET database and a review of case notes was performed. Data pertaining to MER/CB events from January to December 2019 were obtained. Data were de-identified to maintain patient confidentiality. Information pertaining to whether the patient was pre-operative, post-operative (including time and characteristics of the operation), or medical short stay overflow was obtained, in addition to the reason for the MER/CB event and outcome of the event. The Poisson rate distribution 95% confidence interval for incidence rates was calculated.
Data pertaining to operative admissions were obtained via the operating theatre admission database; this was used to determine the incidence rate of MER/CB events by sub-specialty.
Results
There were 47 logged MER/CB events pertaining to the perioperative unit from a total of 550 events occurring across all areas of the hospital in 2019.
Perioperative ward MER/CB events constituted 8.45% (47 of 550) of all events occurring in the hospital premises (Figure 2). There were no recorded events involving staff members, visitors or pre-operative clinic. The incidence rate of MER/CB events for all perioperative admissions was 0.76% (95% CI: 0.53% to 0.99%) or 1 in 131 scheduled operations. The average age was 63 years and median age 67 years.
 |
Table 2 Post-Operative Incidents by Specialty, with Respects to the Total Number of Admissions for Operations in 2019 |
 |
Figure 2 MER/CB events. The 47 perioperative ward events pertained to 41 pre- and post-operative patients. |
The abnormal RDR parameters initiating the escalation to MER/CB are outlined in Table 3.
 |
Table 3 Abnormal RDR Parameters Pertaining to Each MER/CB Event |
The vital sign parameters responsible for triggering these MER/CB events with respects to the time the event was triggered is exhibited in Figure 3. Criteria for triggering the MER/CB event included a single abnormal parameter (n=41), and two or more parameters (n=4).
 |
Figure 3 Reasons for initiating the MER/CB events with respects to the time the incident was called. One in four incidents occur outside of standard day procedure unit working hours (8am to 5pm). |
Pre-Operative
The pre-operative incidence rate was 0.19% (95% CI: 0.07% to 0.30%) or 1 in 538 admissions. Six operations were cancelled as a direct result of these events, indicating a cancellation rate of 0.11% (95% CI: 0.02% to 0.20%) or 1 in 897 scheduled operations. Of the pre-operative cancellations, the causes include two cases of seizures, single cases of hypotension attributed to hypovolemia, supra-ventricular tachycardia, rapid atrial fibrillation, and pneumonia requiring intravenous antibiotics.
Post-Operative
The post-operative incidence rate was 0.58% (95% CI: 0.37% to 0.78%) or 1 in 174 admissions. Thirty-two events involving 31 patients occurred in the post-operative setting. The mean time after the operation was 5.21 hours. The median time was 3.72 hours (IQR: 1.87–6.37 hours).
The number of post-operative MER/CB events with respects to the total number of operations over the study period was determined (Table 2). The parameters for triggering a MER/CB with respects to the time after the completion of the operation are shown in Figure 4. The single most common cluster was post-operative hypotension, associated with 25.5% (16 of 45) of events.
 |
Figure 4 Post-operative MER/CB events. The number of hours after the operation when the incident was called. |
The second most prominent cluster was post-operative reduced consciousness, associated with 15.6% (7 of 45) events; 5 out of 7 of these events were attributed to vasovagal episodes, 2 of 7 were attributed to sedation associated with opioids. Two incidents for reduced level of consciousness/sedation and reduced respiratory rate were attributed to opiate toxicity; one of these received reversal with intravenous naloxone.
Code Blue
There were six CB events. These involved hypotension (n=3), seizure (n=1), rapid atrial fibrillation (=1), vasovagal episode (n=1). There were no Code Blue respiratory or cardiac arrest episodes requiring cardiopulmonary resuscitation.
The vasovagal and hypotensive episodes were managed with intravenous fluids and monitoring, with the exception of a patient with a post-operative bleed after a septoplasty and turbinate reduction that received tranexamic acid and was transferred to a partnered tertiary hospital. The seizure incident that required benzodiazepine therapy was transferred to the emergency department and discharged home the same day with neurology outpatient follow-up. The case of rapid atrial fibrillation involved a patient who had received bowel preparation; this was managed with intravenous fluid rehydration, intravenous magnesium sulfate and admission under a general medical team overnight with discharge home the following day.
Hospital Transfers
Eight patients required inter-hospital transfer and intra-hospital transfer as identified in Table 4. Intra-hospital transfers include the short stay (acute) general medicine unit (n=2), the emergency department with subsequent discharge home (n=2). Inter-hospital transfers to a tertiary facility include cardiology (n=1) for bradycardia attributed to digoxin toxicity, orthopedics (n=1) for post-operative pain, gastroenterology (n=1) with pre-operative tachycardia attributed to colon preparation, general surgery (n=1) after a post-operative hypotensive episode requiring further monitoring with post-operative ileus and acute urine retention. There were no transfers to ICU or HDU.
 |
Table 4 Four Inter-Hospital Transfers and Four Intra-Hospital Transfers |
Multiple Events
Repeated MER/CB events for the same admission were a minor occurrence in this study. Two patients had two events during the same indexed admissions. In the first patient, the events were initiated 4.5 hours apart; the first episode was a vasovagal incident and the second was for hypotension without a vasovagal episode but with associated dizziness. In the second patient, a MER call was subsequently escalated to a CB for loss of consciousness secondary to a seizure.
Discussion
Our report outlines the incidence rate for activation of MER/CB events in a 23 hour surgical unit, and associated criteria for activation by diurnal variation. A US-based retrospective case–control study involving 105 345 post-operative patients at a tertiary hospital center found an incidence rate of 0.76% for emergency response activation, which is concordant but slightly higher than the incidence rate in our investigation.6 This likely reflects a higher baseline medical comorbid complexity, and greater procedural complexity undertaken for patients receiving operations at a major tertiary center with the potential for intensive care monitoring compared to a 23-hour unit. This is further supported by the incidence rate of only 0.0012% in an outpatient procedural clinic of a major Korean dental hospital.7 The physiological systems affected by the 45 MER/CB events include cardiovascular (66%), respiratory with reduced level of consciousness/sedation (9%), isolated neurological (24%). Hospital-wide medical emergency triggers based on USA data include cardiovascular 37.4%, respiratory 38%, neurological 30.7%.8
The standard day procedure working hours at our institution are 08:00 to 17:00. Nine MER call and three CB events occurred outside of standard day procedure working hours, representing 25.5% of MER/CB events in the unit, and 1.63% of all events in the hospital. All three CB events included post-operative hypotension. The most common MER event at night involves bradycardia. There were three of these incidents, with pulse rates 38–49bpm. An earlier observational study has demonstrated MET team activations in the evening or night-time to be associated with significantly higher short-term serious outcomes such as unplanned ICU admission and death.9 An Australian-based retrospective observational study demonstrated that 53% of hospital-wide MET activations occurred out of peak staffing hours.10 Our lower after hours incidence can be attributed to patient selection and the types of procedures performed.
Despite the lower incidence in our facility, the MER/CB events as outlined in Figure 2 justify the requisite for a 24-hour on-site emergency response service.
Three incidents involved uncontrolled pain. One of these was for chest pain treated with glyceryl trinitrate, with subsequently normal serial troponins and ECG. One incident remained overnight for further analgesia. In one incident, involving an orthopedic patient with a knee debridement and tibial cyst bone graft; the pain was uncontrolled with conventional post-operative analgesia and the patient was transported to our partnered tertiary hospital facility with a ketamine infusion. This patient should not have had surgery at the facility. The facility’s incident monitoring system was used to highlight this failure to minimize a recurrence. Although it is not considered routine practice to initiate a MER for pain; this escalation can be triggered on the basis of a medical review not performed within 30 minutes or if staff are concerned or worried about the patient. System activations from staff members who are concerned or ‘worried’ about the patient account for 14–25% of activations.8,11
Post-operative hypotension was the single most common RDR parameter (n=16). With the exception of the case involving a septoplasty and turbinate reduction, all other cases were managed on the ward with intravenous fluids ± further investigations such as bloods and ECG without transfer. One patient (inguinal hernia repair) was transferred to the partnered tertiary hospital center for further intravenous fluids and monitoring. The results of the audit were fed back to both anaesthetic and recovery nursing staff highlighting need to consider the optimal intravenous fluid management in this patient group to minimize this problem. Of the eight isolated events of reduced consciousness, three were pre-operative seizures with normal measured blood glucose readings, and five were vasovagal episodes. All five vasovagal episodes responded to intravenous fluids and further monitoring.
General surgery constitutes the most common specialty for all post-operative incidents. A total of 2055 general surgery procedures were performed, including 214 cholecystectomy procedures. The procedures with the highest rates include inguinal or umbilical hernia repair (n=4) and laparoscopic cholecystectomy (n=4). Orthopedic surgery and ENT surgery were associated with a higher percentage incidence rate, which may reflect the longer duration of operative time in these procedures compared to the large number of relatively short procedures under urology, ophthalmology and gynecology. Of the 495 scheduled endoscopy unit procedures (pan-endoscopy or colonoscopy), 3 incidents (0.6% of total) occurred; these were all pre-operative. These included supraventricular tachycardia, rapid atrial fibrillation, and a seizure. Electrolyte disturbance attributed to dehydration and colon preparation may have predisposed these patients to developing these conditions.12
There are limited published data relating to post-operative surgical transfer rates. A 1998 Australian study involving a 470-bed general hospital found that 17% of post-operative medical emergencies received HDU/ICU transfer.13 A US-based retrospective audit for a general hospital including all medical and surgical wards showed a transfer rate of 30% to ICU and 7.4% to a dedicated monitored bed.8 The importance of the availability of HDU facilities is emphasized by a UK-based retrospective audit that showed post-operative surgical patients who require HDU, but are admitted to the general surgical ward tend to receive inadequate nursing intervention and monitoring.14
Our data provides an illustration of the medical emergencies that occur in a 23 hour surgery unit.
This could be used for evaluation and planning by other 23 hour/day surgery units where after hours critical care staff is limited, with ICU/HDU staff and facilities not located on site. It demonstrates the value of appropriate service design, evaluation and feedback in improving delivery of patient care.
Conclusion
MER Call/Code Blue incidents comprise a relatively low proportion of the total number of events at our hospital. However, care should be given to the monitoring and prevention of post-operative hypotension and vasovagal episodes for patients undergoing procedures with surgical time of greater than one hour, including hernia repair, cholecystectomy, ENT and orthopedic surgery.
This audit highlights the need for ongoing evaluation with feedback and education of medical and nursing staff in optimizing patient selection, perioperative fluids, post-operative mobilization, pain management, and the recognition of patients at risk of deterioration and early intervention to optimize patient outcomes.
Abbreviations
MER, medical emergency response; CB, Code Blue; MET, medical emergency team; ICU, intensive care unit; HDU, high dependency unit.
Ethics
Ethics approval was sought and granted by Central Adelaide Hospital Local Network Human Research and Ethics Committee (reference number 13,358).
Acknowledgments
We would like to acknowledge Ms Victoria Eaton, Nurse Consultant in Critical Care for maintaining the MET database. We would also like to acknowledge Dr James Chua, Chair of Modbury Hospital MET subcommittee.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jones D, Bellomo R, Bates S, et al. Long term effect of a medical emergency team on cardiac arrests in a teaching hospital. Crit Care. 2005;9(6):808–815.
2. Bristow PJ, Hillman KM, Chey T, et al. Rates of in-hospital arrests, deaths and intensive care admissions: the effect of a medical emergency team. Med J Aust. 2000;173(5):236–240. doi:10.5694/j.1326-5377.2000.tb125627.x
3. Hillman KM, Chen J, Jones D. Rapid response systems. Med J Aust. 2014;201(9):519–521. doi:10.5694/mja14.01088
4. Australian Commission on Safety and Quality in Healthcare. Recognising and Responding to Clinical Deterioration: background Paper [Internet]. ACSQHC. 2008.
5. Subbe CP, Bannard-Smith J, Bunch J, et al. Quality metrics for the evaluation of rapid response systems: proceedings from the third international consensus conference on rapid response systems. Resuscitation. 2019;141(1):1–12. doi:10.1016/j.resuscitation.2019.05.012
6. Hardman MI, Kruthiventi SC, Schmugge MR, et al. Risk factors and outcomes of postoperative emergency response team activation: a matched case-control study. Crit Care Resusc. 2020;22(1):6–14.
7. Ha SW, Choi YJ, Lee SE, et al. Emergency response team activation in the outpatient clinic of a single dental teaching hospital in Korea: a retrospective study of 10 years’ records. J Dent Anesth Pain Med. 2015;15(2):77–83.
8. Lyons PG, Edelson DP, Carey KA, et al. Characteristics of rapid response calls in the United States: an analysis of the first 402,023 adult cases from the get with the guidelines resuscitation-Medical emergency team registry. Crit Care Med. 2019;47(10):1283–1289. doi:10.1097/CCM.0000000000003912
9. Kurita T, Nakada T, Kawaguchi R, Shinozaki K, Abe R, Oda S. Timing and location of medical emergency team activation is associated with seriousness of outcome: an observational study in a tertiary care hospital. PLoS One. 2016;11(12):e0168729.
10. Jones D, Bates S, Warrillow S, et al. Circadian pattern of activation of the medical emergency team in a teaching hospital. Crit Care. 2005;9(4):R303–R6. doi:10.1186/cc3537
11. Chen J, Bellomo R, Hillman K, Flabouris A. Triggers for emergency team activation: a multicenter assessment. J Crit Care. 2010;10(2):
12. Lichtenstein GR, Cohen LB, Uribarri J. Review article: bowel preparation for colonoscopy – the importance of adequate hydration. Aliment Pharmacol Ther. 2007;26(5):633–641. doi:10.1111/j.1365-2036.2007.03406.x
13. Lee A, Lum ME, O’Regan WJ, Hillman KM. Early postoperative emergencies requiring an intensive care team intervention. Anaesthesia. 1998;53(6):529–535. doi:10.1046/j.1365-2044.1998.00395.x
14. Coggins RP. Delivery of surgical care in a district general hospital without high dependency unit facilities. Postgrad Med J. 2000;76(894):223–226. doi:10.1136/pmj.76.894.223
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.