")
Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 14
Pediatric Magnet Ingestion with Delayed Presentation: Case Series from Tertiary Center in Saudi Arabia
Authors Alareefy A , Barnawi E, Alrashed R, Alamri A, Aleidan AM, Alghofaily M, Alkhelaif M, Kanfar S
Received 3 April 2023
Accepted for publication 18 July 2023
Published 24 July 2023 Volume 2023:14 Pages 231—236
DOI https://doi.org/10.2147/PHMT.S411079
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Laurens Holmes, Jr
Abdulaziz Alareefy,1 Esam Barnawi,1 Rawan Alrashed,1 Abdulelah Alamri,1 Ahmed M Aleidan,2 Mazen Alghofaily,3 Mayada Alkhelaif,3 Sara Kanfar4
1Pediatric Emergency Department, King Fahad Medical City, Riyadh Second Health Cluster, Riyadh, Saudi Arabia; 2Pediatric Pulmonology Department, King Fahad Medical City, Riyadh Second Health Cluster, Riyadh, Saudi Arabia; 3General Pediatric Department, King Fahad Medical City, Riyadh Second Health Cluster, Riyadh, Saudi Arabia; 4Pediatric Surgery Department, King Fahad Medical City, Riyadh Second Health Cluster, Riyadh, Saudi Arabia
Correspondence: Abdulaziz Alareefy, Pediatric Emergency Department, King Fahad Medical City, Central Second Health Cluster, Ministry of Health, P.O. Box. 59046, Riyadh, 11525, Saudi Arabia, Email [email protected]
Abstract: Swallowing foreign bodies is common in young kids, especially those aged 6 months to 6 years. Magnet ingestion is a hazardous health issue that extremely jeopardizes the most vulnerable group, children, to risks of intestinal obstruction and worse, perforation. We, hereby, report 3 cases of magnet ingestion in the pediatric age group who had multiple beaded magnets stuck inside their GI tract over a variable period of 1 to 10 months before their presentation to the Emergency Department, King Fahad Medical City Riyadh, Saudi Arabia.
Keywords: magnet ingestion, pediatric, emergency, foreign body, Saudi Arabia
Introduction
Swallowing foreign bodies is common in young children, especially those ages from 6 months to 6 years.1 Magnet ingestion is a hazardous health problem that extremely jeopardizes the most vulnerable age group of children, who are at risks of intestinal obstruction and worse perforation.2
Ingestion of foreign bodies (FB) of different shapes and structures is a commonly encountered problem, particularly in children between 6 months and 3 years of age.3 The vast majority of pediatric ingestions are accidental and the most common objects are coins, followed by toys, toy parts, sharp objects, batteries, and magnets.4 Approximately 80% of the ingested foreign body passes without any problems through the alimentary tract causing no obstructive damage or necessity for surgical intervention.5 However, magnet ingestion is unique as in the case of multiple magnets swallowed, they may attract each other across the intestinal wall leading to potential insult in the form of intestinal obstruction, ischemia, and perforation.6 Globally, a description of magnet ingestion was extremely uncommon in the 1990s, as it only surfaced through case reports in the year 2000.7 The number of magnet ingestion in pediatrics increased significantly throughout the last 20 years.8 The management of magnet ingestion varies based on the object ingested, its location, and the patient’s age and size as it is usually expected to be passed spontaneously if the magnet is not too large.9 Nonetheless, most of the patients especially the ones with gastrointestinal symptoms such as vomiting, gagging, choking, and abdominal pain need intervention for removal either by endoscopy or surgery.10,11 Here, we present a case series of 3 pediatric patients who ingested a magnet and the management plan in a tertiary hospital in Riyadh, Saudi Arabia.
Case Series
Case 1
A healthy 3-year-old boy was brought by his parents to the Emergency Department with complaints of vomiting and abdominal pain. His parents did not have any idea if he had ingested any foreign body supported by his unremarkable physical examination, evidenced by a soft, non-distended, and non-tender abdomen with no presence of entry and exit site injury. His level of sensorium was preserved too, in addition to a normal chest and cardiac exam.
The abdominal radiograph showed intra-abdominal foreign subjects with mild dilatation of the proximal bowel loops demonstrating multiple air-fluid levels suggesting partial lower intestinal obstruction (Figure 1B, C and D). The patient had a history of ingesting FB as there was a previous abdominal radiograph dated one year before this presentation (Figure 1A), where the patient reported to ED with similar symptoms, complaining of vomiting and abdominal pain. The abdominal radiograph at that time depicted no signs of intestinal obstruction, yet a radiopaque foreign body was present (probably representing an external artifact). In between the two admissions, and over 10 months, there were no interval symptoms and the child was thriving well with no issues until he presented to the hospital for the second time. The management plan included surgical intervention as he underwent an Open Laparotomy which showed 2 proximal ileum loops adherent to each other with fistula formation, enterotomy, magnets removal, and fistula closure was done. The child was discharged home in stable condition after 2 days with no medications. A follow-up encounter at the surgical clinic was of no concern.
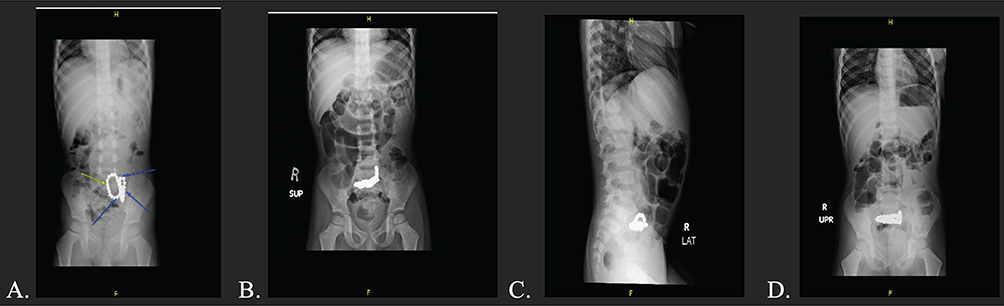 |
Figure 1 (A) Nonspecific abdominal bowel gas pattern and distribution with no radiological signs of intestinal obstruction or free intraperitoneal air. Radiopaque dated foreign body projects over the region of the midline in the pelvis (probably represent an external artifact well as indicated by arrows on the image). (B, C and D) The previously noted beaded foreign object is again seen suggesting it is intra-abdominal. There is mild dilatation of the proximal bowel loops with multiple air-fluid levels suggesting partial lower intestinal obstruction. Air was noted within the rectum. No pneumoperitoneum. |
Case 2
Another child, 4 years old who had a history of foreign body ingested about 4 months ago presented to a private hospital after symptoms of flu appeared and after week when his mother noticed that he was snoring and nasal discharge, she took him back to the same private hospital and found after gross visualization of the nose that he had a magnetic object (bracelet) inside his nostrils removed by ENT specialist, after that presentation, by about six weeks, the child complained of abdominal pain at night followed by morning vomiting, decreased activity, and distended abdomen, parents sought medical advice at another private hospital and patient was admitted to do an abdominal x-ray, ultrasound and CT scan. The ultrasound result was suggestive of ileo-cecal intussusception for further urgent CT correlation. X-ray depicted a right lower abdominal region foreign body with subsequent few central air-fluid levels with suspicion of bowel obstruction. CT scan demonstrated a foreign body at the cecum/terminal ileum with subsequent partial obstruction and moderate intra-peritoneal free fluid. The patient was admitted for 5 days observed there and repeated x-ray noted a radio-opaque Foreign body in the pelvis with no air-fluid level or gas collection. Parents were instructed to be seen after 1 week when he has his x-ray repeated and it showed that the foreign body remained notable in the left iliac region, then the attending physician advised the parents to refer the patient to a tertiary hospital, so they came to KFMC where he was evaluated and found to have mild abdominal pain with no abdominal distention or tenderness, new abdominal X-ray was done which again showed a radio-opaque structure at the right lower quadrant of the abdomen (Figure 2A).
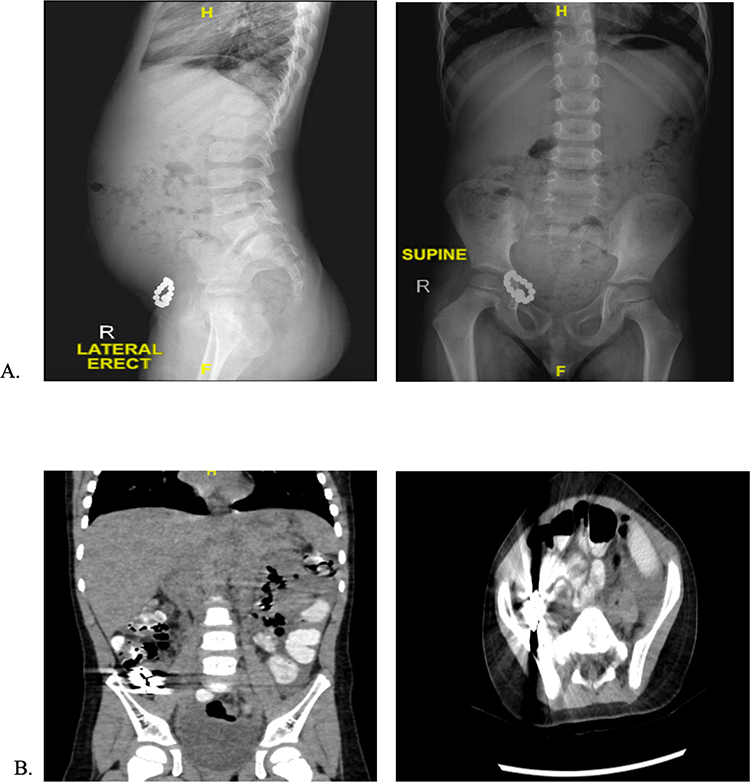 |
Figure 2 (A) Multiple rounded radiopaque foreign body is noted in the right lower quadrant suggestive of magnet toy, on lateral view it appears anterior in location and away from the rectum. No signs of bowel perforation or obstruction with severe noted constipation. (B) CT of the child showed an Impacted foreign body in the distal small bowel at the ileocecal junction with a proximal mild to moderate small bowel loop dilatation. No signs of free intraperitoneal air. |
So the patient was admitted under pediatric surgery service where he was observed for 2 days with no change in Foreign body location on subsequent X-rays or repeated CT scans (Figure 2B), therefore the child underwent exploratory laparotomy, and 13 magnetic pieces removed with no obvious intestinal complications.
He then was discharged on day 5 after his procedure in good condition with no complaint in his follow-up appointment 2 weeks afterward.
Case 3
The last baby we are reporting is a 22-month-old healthy baby girl, who presented to the Emergency Department in KFMC complaining of a 1-day history of vomiting, it was greenish then became coffee ground, neither projectile nor related to food. The girl had vomited more than 10 times before reporting to the ED. It was associated with abdominal pain, decreased oral intake, and low activity. The mother gave a history of upper respiratory tract infection symptoms that appeared 2 days ago which was associated with fever measured at 39 C. She initially presented to a private clinic and treated conservatively with antipyretic and antibiotic medications. A history of changes in bowel movement, bleeding per rectum or urinary symptoms were not observed. Upon examining her, she looked well and was vitally stable, but had a distended and deeply tender abdomen. She was admitted under general pediatrics to investigate for upper gastrointestinal bleeding. X-ray was done and showed multiple air-fluid levels with evident foreign bodies that looked like 6 magnetic balls (Figure 3). When the family was interviewed again, they revealed a witnessed magnet swallowing 1 month ago, but as she had no complaints at the time, they did not seek medical advice hoping it would pass spontaneously. She was started on Pantoprazole, Cefotaxime, Metronidazole and Ampicillin. She was then taken for Laparoscopic-assisted removal of the magnets. On the 5th post-operative day, she started to safely consume orally and was discharged on the 7th day of her hospitalization. Unfortunately, she missed her follow-up to trace her improvement.
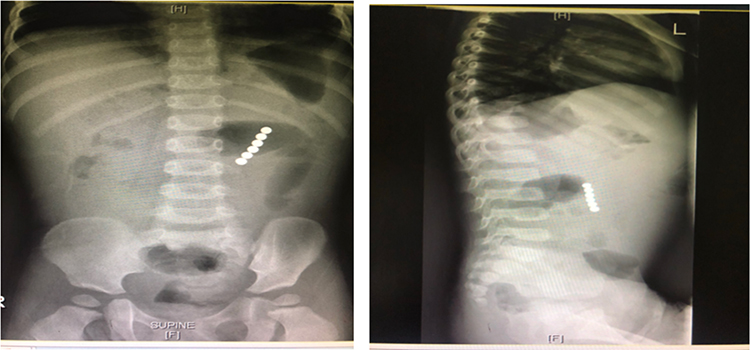 |
Figure 3 Supine and decubitus views of abdominal X-ray of the child showed multiple magnets in the upper portion of small intestines. |
Discussion
Foreign body ingestion is common among children, particularly toddlers as they begin exploring the surrounding environment. Different objects can be ingested on a huge spectrum from coins, batteries, and toys to even sharp objects and magnets.
The uniqueness of magnet/s ingestion as opposed to other foreign bodies is that reports on it are relatively recent and scant in the literature. Since the first report by McCormick et al in 2002,12 other reported cases follow, although under-reported owing to the unnoticed, safe and uncomplicated course of ingestion initially in most children.
It has evolved to be more common over time. Single magnet ingestion, like any inert solo foreign body, is not a critically serious condition that requires surgical intervention. On the other hand, ingestion of multiple magnets can lead to danger-imposing complications such as obstruction and perforation as a result of the attraction of multiple pieces through the intestinal wall.11
In Taiwan, and across a span of 9 years from 2009 to 2018, a retrospective analysis of 13 patients, 10 of which had multiple magnets ingestion revealed the need for surgical intervention in 3 cases that happened to have been complicated with intestinal perforation.13 In Turkey, a similar case of a 4-year girl who ingested multiple magnets and ended up in the ED one and a half hours later with eventual operative intervention,14 and a similar report from the nearby Gulf region in Kuwait.15 However, the timeline of all formerly reported cases was from hours to 4 days before the presentation, which is shorter than what we have reported.
On the contrary, and in light of its associated risks, a study from the US surveyed the frequency of encountered Pediatric magnet ingestion in ED with a significant decline after the governmental ban on magnets in 2012 in the response to Consumer Product Safety Commission (CPSC) issued the first warning announcing the hazards of high-powered magnets used in children’s toys, which had been increasing exponentially.16 A follow-up, multicenter retrospective cohort study conducted between the years of 2017 and 2019 revealed a rise in magnet ingestion cases among pediatric patients in the US after the ban was lifted by a federal court.17
A cohort study done in China showed a significant rise in magnet ingestion over 2 years (2017 and 2019) in comparison to previous years.6
A recent position paper by the European Society for Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHN) emphasized the importance of public and community awareness about the potential harms of magnet ingestions.11
Over a couple of months, our indexed cases contracted a prolonged symptomless course of multiple magnet ingestion, through which they maintained their well-being with no effect on daily life activities until all symptoms became evident. It is difficult to tell if the ingestion caused an intestinal wall injury rather than an isolated picture of intestinal obstruction; however, it has been reported by the operating surgeon in case 1 that 2 loops adhering to each other with fistula formation, the other two cases did not have similar intestinal complications. We hereby present a genuine example of how difficult it can be to identify such cases, especially when a good quality of life is maintained.
Conclusion
Owing to its variably serious complications lying through a wide range of spectrum exemplified by fistula formation, obstruction, ischemia, and perforation, magnets impose a critical threat on children of the explorative phase. Cases might evolve rapidly to life-threatening statuses that might eventually require a prompt surgical salvage if misdiagnosed or unnoticed early. Luckily, our indexed cases did not have major intestinal complications despite the first case who had a fistula formation. We urge physicians to be enlightened about the early recognition of such cases.
Ethical Considerations
Written consent for publication of case details and images was obtained and signed by the parents of the children for full disclosure while maintaining strict confidentiality with respect to the patient’s medical information and images under the approval of the King Fahad Medical City (KFMC) research center ethical committee.
Acknowledgment
The authors would like to acknowledge the Parents of the child, Children Specialized Hospital (CSH) at King Fahad Medical City (KFMC) staff for their contribution to the completion of this case report. The authors would like to thank the Research Center at King Fahd Medical City, Riyadh, for their editing of this article. The abstract of this paper was presented as a poster at the research day symposium in King Fahad Medical City (KFMC).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding source.
Disclosure
All authors have no conflicts of interest to disclose.
References
1. Ambe P, Weber SA, Schauer M, Knoefel WT. Swallowed foreign bodies in adults. Dtsch Arztebl Int. 2012;109:869–875. doi:10.3238/arztebl.2012.0869
2. Hussain SZ, Bousvaros A, Gilger M. Management of ingested magnets in children. JPGN. 2012;55(3):239–242.
3. Litovitz TL, Klein-Schwartz W, White S, et al. 2000 annual report of the American Association of Poison Control Centers Toxic Exposure Surveillance System. Am J Emerg Med. 2001;19:337–395. doi:10.1053/ajem.2001.25272
4. Kay M, Wyllie R. Pediatric foreign bodies and their management. Curr Gastroenterol Rep. 2005;7(3):212–218. doi:10.1007/s11894-005-0037-6
5. Erbes J, Babbitt DP. Foreign bodies in the alimentary tract of infants and children. Appl Ther. 1965;7:1103–1109.
6. Wang K, Zhang D, Li X, et al. Multicenter investigation of pediatric gastrointestinal tract magnets ingestion in China. BMC Pediatr. 2020;20:95. doi:10.1186/s12887-020-1990-9.
7. Sahin C, Alver D, Gulcin N, et al. A rare cause of intestinal perforation: ingestion of magnet. World J Pediatr. 2010;6:369–371. doi:10.1007/s12519-010-0237-5
8. Naji H, Isaacson D, Svensson J, et al. Bowel injuries caused by ingestion of multiple magnets in children: a growing hazard. Pediatr Surg Int. 2012;28:367–374. doi:10.1007/s00383-011-3026-x
9. Lee JH. Foreign body ingestion in children. Clin Endosc. 2018;51(2):129. doi:10.5946/ce.2018.039
10. Altokhais T. Magnet ingestion in children management guidelines and prevention. Front Pediatr. 2021;2021:804.
11. Nugud AA, Tzivinikos C, Assa A; The Gastrointestinal Committee of ESPGHAN. Pediatric magnet ingestion, diagnosis, management, and prevention: a European Society for Paediatric Gastroenterology Hepatology and Nutrition (ESPGHAN) position paper. J Pediatr Gastroenterol Nutr. 2023;76(4):523–532. doi:10.1097/MPG.0000000000003702
12. McCormick S, Brennan P, Yassa J, Shawis R. Children and mini-magnets: an almost fatal attraction. Emerg Med J. 2002;19:71–73. doi:10.1136/emj.19.1.71.
13. Lai -H-H, Lin H-Y, Chang C-H. Magnet ingestion by children: a retrospective study in a medical center in Taiwan. Pediatr Neonatol. 2020;61(5):542–547. doi:10.1016/j.pedneo.2020.06.003
14. Arslan M, Uyar M, Peker SC, et al. A child patient who ingested multiple magnets: case report. Turk J Acad Gastroenterol. 2021;20:181–184. doi:10.17941/agd.1055252.
15. Kumar S, Gupta V, Al Fadli W. Magnet ingestion: a case report and review of literature. Kuwait Med J. 2015;47(2):153–154.
16. Reeves PT, Nylund CM, Krishnamurthy J, Noel RA, Abbas MI. Trends of magnet ingestion in children, an ironic attraction. J Pediatr Gastroenterol Nutr. 2018;66(5):e116–e121. doi:10.1097/MPG.0000000000001830.
17. Middelberg LK, Leonard JC, Shi J, et al. High-powered magnet exposures in children: a multi-center cohort study. Pediatrics. 2022;149(3):e2021054543. doi:10.1542/peds.2021-054543
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.