")
Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 14
Pediatric Guillain–Barré Syndrome in a Resource Limited Setting: Clinical Features, Diagnostic and Management Challenges, and Hospital Outcome
Authors Shibeshi MS , Mengesha AA, Gari KT
Received 14 December 2022
Accepted for publication 7 March 2023
Published 22 March 2023 Volume 2023:14 Pages 107—115
DOI https://doi.org/10.2147/PHMT.S401461
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Roosy Aulakh
Mulugeta Sitot Shibeshi,1 Adane Alto Mengesha,2 Kefyalew Taye Gari1
1Department of Pediatrics and Child Health, Hawassa University, Hawassa, Ethiopia; 2Department of Pediatrics and Child Health, Arba Minch University, Arba Minch, Ethiopia
Correspondence: Mulugeta Sitot Shibeshi, Email [email protected]
Background: Guillain–Barré syndrome (GBS) is an acute immune-mediated peripheral neuropathy with a highly variable clinical course and outcome. There remain diagnostic and treatment challenges in resource limited settings. This study aimed to describe the clinical presentation, diagnostic and management challenges, and hospital outcome of children with GBS in southern Ethiopia.
Methods: A retrospective chart review of children aged ≤ 14 years who were admitted with a diagnosis of GBS to Hawassa University Comprehensive Specialized Hospital from 2017 to 2021 was done. Medical records of 102 children who fulfilled the Brighton Criteria for GBS were reviewed, and data on demographic, clinical characteristics, investigation findings, treatment, and outcome were collected. Logistic regression analysis was done to determine factors associated with mortality.
Results: The mean age of the study subjects was 7.25± 3.91 years and 63.7% were male. Antecedent event was present in 48% of the cases, and the most common triggering factor was upper respiratory tract infection (63.8%). The mean Hughes disability score was 4.23± 0.54, 4.48± 0.71, and 4.03± 0.86 at admission, nadir and discharge from hospital, respectively. Cranial nerve involvement was present in 27.5% of patients and bulbar palsy was the most common finding. Dysautonomia was observed in 57.8% of the participants. Sixty-three patients (61.8%) needed ICU care but only 43 of them (68.3%) were admitted to ICU. Similarly, 31 patients (30.4%) required respiratory support but only 24 of them (77.4%) were on mechanical ventilator. No patient had nerve conduction study. Only 5.9% of patients received IVIG. Thirteen patients (12.7%) died of GBS and the presence of respiratory failure was the only determinant of mortality [AOR = 11.40 (95% CI: 1.818, 71.52), p = 0.009].
Conclusion: There is a gap in the diagnosis and management of children with GBS; and mortality from the disease is higher than reports from other settings.
Keywords: Guillain–Barre syndrome, outcome, resource limited setting
Introduction
Guillain–Barré syndrome (GBS) is an acute immune-mediated, mostly post infectious, peripheral neuropathy with a highly variable clinical course and outcome.1 It is the most common cause of acute flaccid paralysis (AFP) worldwide.2 Although the epidemiology of GBS varies from region to region, its annual incidence in children is reported to be 0·6 per 100,000 per year and the disease is more common in males than in females.1,3 The poor hygienic and sanitary conditions in low-income countries are associated with higher rates of exposure to infectious organisms that are capable of triggering GBS.4
The clinical manifestations of GBS vary remarkably. In patients with typical GBS, the key presenting feature is rapidly progressive ascending bilateral symmetrical weakness and areflexia or hyporeflexia, although deep tendon reflexes (DTR) can be normal or even exaggerated in the initial stages of the disease.4 GBS can also have atypical presentation. Weakness may be asymmetrical or descending type, can be predominantly proximal or distal, and can start simultaneously in all limbs. Cranial nerve deficits, autonomic dysfunction, sensory disturbances, ataxia, and muscle pain or radicular pain can be experienced by patients with GBS.5–7
The clinical presentation of GBS is different in children compared with adults.8,9 Preschool children with GBS usually present with nonspecific or atypical clinical features, such as poorly localized pain, refusal to walk, or an unsteady gait that often result in misdiagnosis and delayed diagnosis.6,10
Diagnosis of GBS is mainly based on clinical features, supported by cerebrospinal fluid (CSF) examination and nerve conduction studies.11 The typical CSF finding of GBS is an increased protein level with a normal cell count (albuminocytological dissociation) although the protein level may be normal if CSF is analysed early in the course of illness.12 Nerve conduction study is required to reach the highest level of diagnostic certainty and to distinguish between GBS variants. Although the diagnosis of GBS is usually straightforward, it can be challenging especially in young children, atypical cases, and in low-income countries with poor diagnostic facilities.4
Patients with GBS need immunotherapy (IVIG or plasma exchange) alongside meticulous monitoring and supportive care. However, neither IVIG nor plasma exchange are affordable for the majority of patients in resource poor settings. Though the evidence is limited, there are reports of effective use of cheaper alternatives such as modified therapeutic plasma exchange, exchange blood transfusion, rituximab, and pulse steroid therapy in the treatment of GBS.13
Studies showed that about 20–30% of patients with GBS develop respiratory failure and require admission to intensive care unit (ICU).1,14 However, the number of ICU beds is limited in low-income countries and patients that require ICU care often die. A study in Bangladesh revealed that the absence of ICU support when required was the strongest risk factor for death in patients with GBS.15 Respiratory distress, complications during hospitalization, and ICU requirement were significantly associated with mortality in an Iranian study.16
Deaths from GBS can occur during the acute progressive phase, the plateau phase, or the recovery phase, and most frequently from respiratory or cardiovascular complications.17
Mortality from GBS is higher in low-income as compared to high-income countries; for example, a mortality of 11.5% during the acute phase of the illness was reported from India18 while no mortality was reported in a French19 and a Korean study.20
GBS is under-reported in Ethiopian children; and there has not been any study from the southern part of Ethiopia. This study aimed to describe the clinical presentation, investigation, treatment, and hospital outcome of children with GBS in southern Ethiopia.
Methods and Materials
Study Area
The study was conducted in Hawassa University Comprehensive Specialized Hospital located about 275 km south of Addis Ababa, the capital city of Ethiopia. The hospital is a tertiary care center that provides neurodiagnostic services including electroencephalography, CT scan and MRI; however, nerve conduction study is not available in the hospital.
Study Design, Subjects and Sample
The study was a retrospective study conducted on pediatric patients aged ≤14 years admitted with a diagnosis of GBS to Hawassa University Comprehensive Specialized Hospital. Sample size was not calculated as the target population was limited. The medical records of all children who were evaluated by a pediatric neurologist and had a primary discharge diagnosis of GBS over a 5-year period (2017 to 2021) were reviewed, and a total of 102 children with typical GBS (children with flaccid symmetrical ascending weakness with hyporeflexia or areflexia) were enrolled in the study. Diagnosis of GBS was made using Brighton criteria and classified into different levels of diagnostic certainty ranging from level 1(highest) to level 4(lowest) as shown in Table 1.12
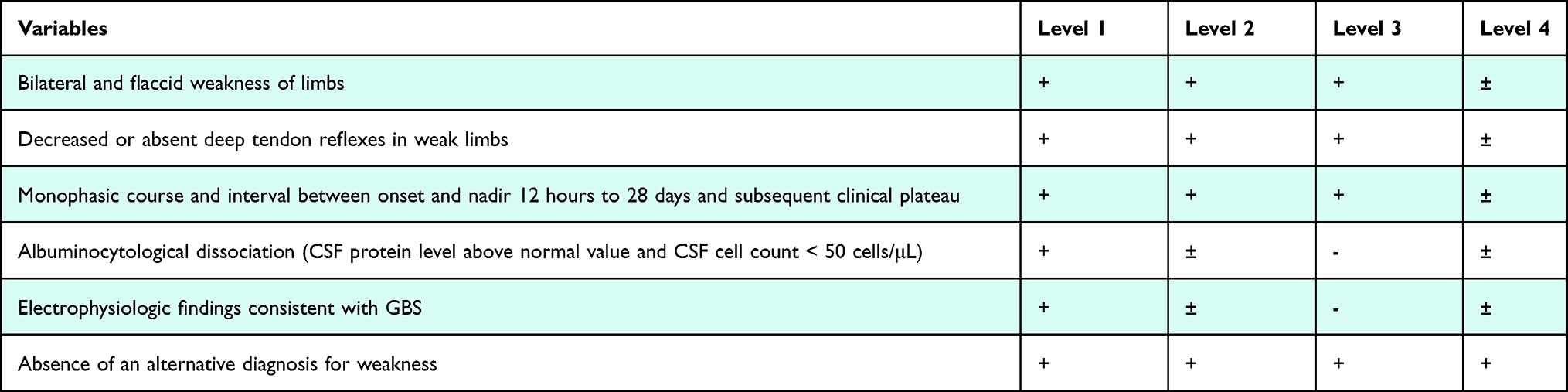 |
Table 1 Brighton Criteria Level of Diagnostic Certainty of GBS |
Children with atypical GBS, CSF WBC count of >50/µL, AFP with sensory level, previous neuromuscular weakness, diphtheria, hypokalaemia, AFP with central nervous system involvement, previous neurologic insult, autoimmune disease, and a progressive neurologic disease were excluded from the study.
Data Collection Procedure
Data were collected using a data collection tool that contained questions about demographic and GBS-related information. Demographic information included age, sex, and residence. GBS-related information included duration of paralysis before admission, triggering factor, vaccination status for polio, season of onset, physical examination findings, CSF analysis results, treatment received, complications, duration of hospital stay, and outcome at discharge. Severity of the disease was evaluated using Hughes GBS disability score that has six levels: 0 = healthy; 1 = minor symptoms and capable of running; 2 = able to walk 5m or more without assistance but unable to run; 3 = able to walk 5m across an open space with help; 4 = bedridden or chair-bound; 5 = requiring assisted ventilation for at least part of the day; 6 = dead.21 The nadir of disease was defined as the highest Hughes GBS disability score.
Data Processing and Analysis
Data were entered in the Statistical Package for Social Sciences (SPSS) software (version 26) for windows and cleaned, and descriptive and analytic statistics were done as applicable. Patients’ sociodemographic characteristics and GBS-related variables were summarized using frequency distribution tables. Mean/median and standard deviation/inter quartile range were calculated for continuous data. Logistic regression analysis was done to determine factors associated with mortality from GBS. A P-value of less than 0.05 was considered statistically significant.
Ethical Considerations
The study was conducted after obtaining ethical clearance from the Institutional Review Board of Hawassa University, College of Medicine and Health Sciences. This study complied with the Declaration of Helsinki. All personal identifications were excluded during data collection.
Results
The medical records of 102 children who fulfilled the Brighton Criteria for GBS were reviewed. The clinical criteria for level 2 of diagnostic certainty of the Brighton Criteria12 were met in 49% of the study subjects while the remaining 51% fulfilled level 3 of diagnostic certainty. No patient met level 1 of diagnostic certainty as electrophysiologic studies were not performed in this setting. The mean age of the study subjects was 7.25±3.91 years (range: 1–14 years) and 63.7% were male. The majority (68.6%) were from rural areas. The median duration of illness before presentation to hospital was 6 days (IQR 3 −10 days). Antecedent event was present in 48% of the study subjects, and the most common triggering factor was upper respiratory tract infection (61.2%). More cases were reported in the month of November than in any other month of the year. The majority (78.4%) of the study participants had quadriplegia while the rest had involvement of only the lower limbs at presentation. The mean Hughes disability score was 4.23±0.54, 4.48±0.71, and 4.03±0.86 at admission, nadir and discharge from hospital, respectively.
Cranial nerve involvement was present in 27.5% of the patients and bulbar palsy was the most common finding. Dysautonomia was observed in 57.8% of the participants. Sixty-three patients (61.8%) needed ICU care but only 43 of them (68.3%) were admitted to ICU. Similarly, 31 patients (30.4%) required respiratory support but only 24 of them (77.4%) were on mechanical ventilator. Lumbar puncture was performed in only 63 patients (61.8%) 1 week after the onset of weakness, and albuminocytological dissociation was observed on CSF analysis in 50 patients (79.4%). Thirteen patients had normal CSF protein, and no repeat lumbar punctures were done. Thirteen patients who presented with respiratory muscle involvement and/or bulbar palsy within few days of the onset of weakness were directly admitted to ICU and were put on ventilator and did not undergo lumbar puncture. The reason why lumbar puncture was not done for the remaining patients was not documented. The median CSF protein was 75 mg/dL (IQR: 51–104 mg/dL) and the median CSF white blood cell count was 0/µL (range: 0–50/µL). No patient had nerve conduction study. No microbiologic studies were performed to identify specific triggers of the disease. Only 5.9% of patients received IVIG. Nineteen of the 24 of patients on mechanical ventilator (79.2%) were treated for ventilator associated pneumonia, 7 of the 13 patients (53.8%) with bladder and bowel dysfunction were treated for UTI, and 10 patients were treated for other hospital acquired infections.
Patients remained in hospital until no more progression of the illness, and the median duration of hospital stay was 9 days (IQR 4–15 days). At discharge from hospital, 44.1% had some improvement of the body weakness and/or the dysautonomia, 40.2% were in the same condition, and 3% had worsening of their body weakness compared to their condition at admission. Thirteen patients (12.7%) died of GBS: 7 from dysautonomia, 5 from respiratory muscle involvement, and 1 from complications of intubation. The demographic and clinical characteristics of the patients are summarized in Table 2.
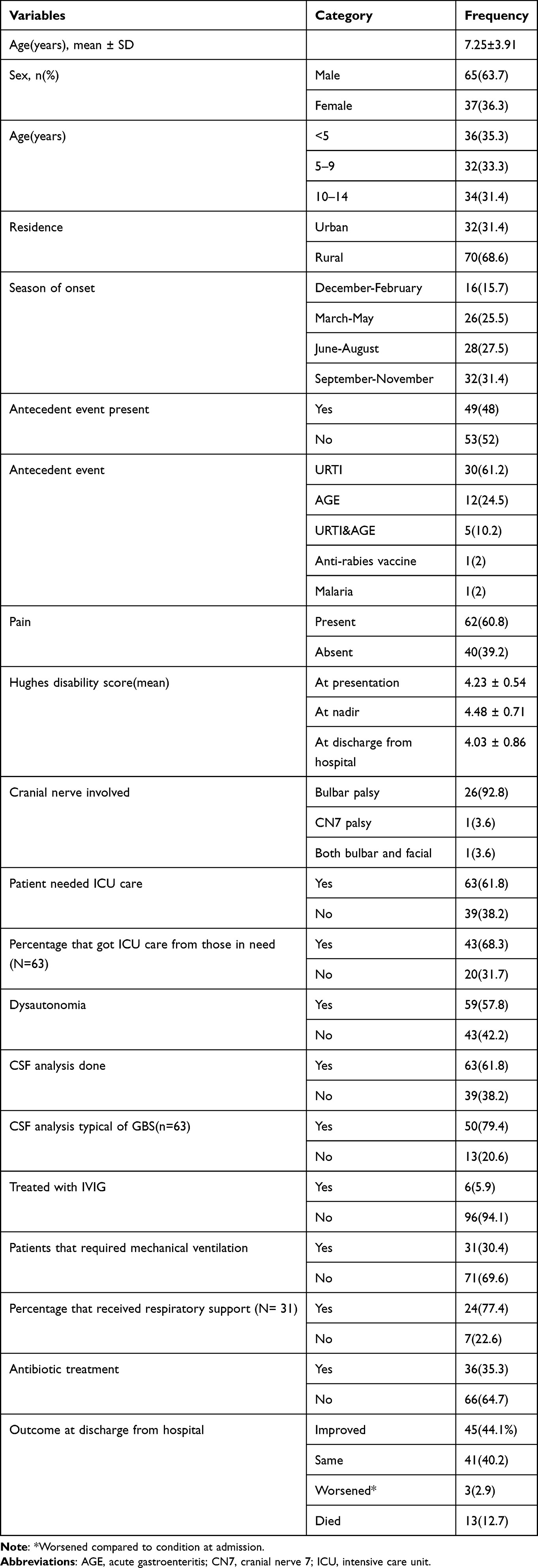 |
Table 2 Demographic and Clinical Characteristics of Children with GBS (n = 102) |
On bivariate logistic regression analysis respiratory failure, cranial nerve involvement, dysautonomia, absent deep tendon reflexes, ICU admission, mechanical ventilation, and duration of paralysis before presentation were associated with mortality; however, only respiratory failure was found to have a statistically significant association with mortality in the multivariable logistic regression model. Children with GBS who had respiratory failure were about eleven times more likely to die than those who had no respiratory failure [AOR = 11.40 (95% CI: 1.818, 71.52), p = 0.009)] (Table 3).
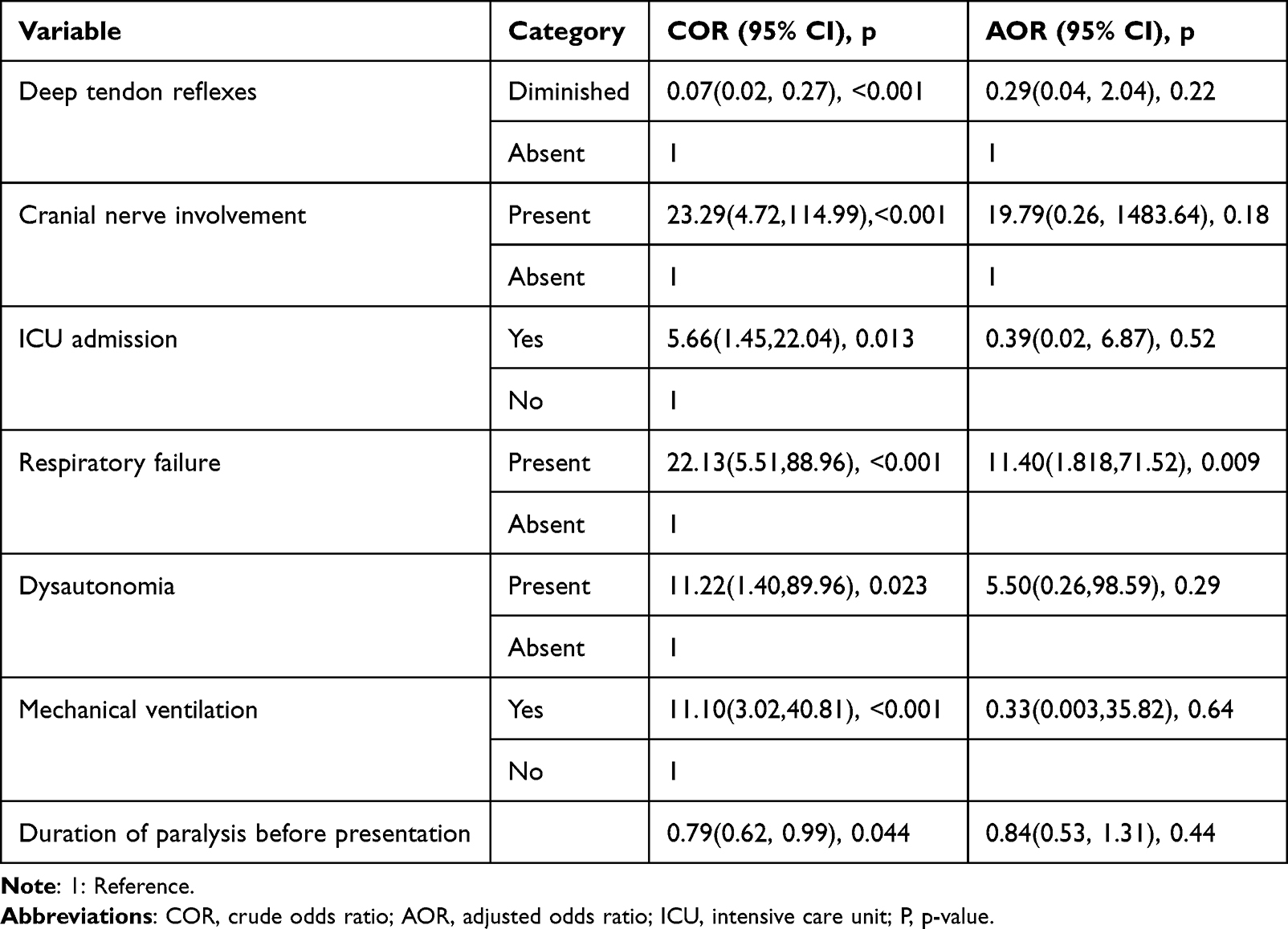 |
Table 3 Logistic Regression Analysis Results of Factors Associated with Mortality in Children with GBS (N = 102) |
Discussion
In this study, we described the clinical characteristics and hospital outcome of 102 children with a clinical diagnosis of GBS. The disease was more common in males (63.7%), and this is consistent with other reports.1,8,14 Unlike adults in whom the incidence of GBS increases linearly with age,22,23 GBS in children is more common in the young. Studies from Denmark and Finland revealed that the incidence of GBS peaked at the age of 2 years.3,24 Similarly, a Chinese study showed that incidence of the disease peaked in children aged 1–4 years.7 In this study, the mean age of the participants (7.25±3.91 years) is in line with findings of other studies;7,13 and 35.3% of them were under 5 years of age which is consistent with a report from China.8
Some studies showed clustering in the incidence of GBS during certain seasons of the year: an observation that can be explained by the seasonality of certain triggers of GBS like gastroenteritis and influenza.6,25 In our study, more cases were observed in the months of September to November, particularly in the month of November, which coincides with the flu season in this setting.26 An antecedent event, an infection or another immune stimulator that induces an aberrant autoimmune response against peripheral nerves, usually precedes the onset of GBS.1 In this study, antecedent event was present in 48% of cases which is comparable to a finding from China7 but lower than an 80% reported in a multicentre study from Europe,6 a 63% reported in a nationwide study from Denmark,3 and a 73.2% reported in a previous study from Ethiopia.27 Although it is suggested that the poor sanitary and hygienic conditions prevalent in developing countries increases the risk of exposure to gastrointestinal pathogens that may increase the incidence of gastroenteritis triggered GBS,4,23 upper respiratory tract infections were the most commonly reported triggers in our setting. Our finding is in line with the findings of the International Guillain-Barre Syndrome Outcome Study,23 and studies from Taiwan14 and Korea.28 However, tests to identify the specific infective pathogens that triggered the illness were not performed in this study.
The diagnosis of GBS in children, especially in resource poor settings where diagnostic facilities are limited, is challenging; and multiple referrals and delay in diagnosis is common.4 In this study, the median duration of illness before presentation to hospital was 6 days- an interval shorter than reports from other similar settings.29 The relatively short median duration before admission could be explained by the presence of a more severe disease in the majority of cases (78.4% had quadriplegia at admission), forcing caretakers to seek medical help early. Pain is very common in children with GBS and has been reported in 35% to 70% of cases.3,6 In our study, 60.8% of patients had documented pain that required treatment; and amitriptyline was the most commonly used drug. Autonomic dysfunction was observed in 57.8% of our patients which is comparable to the finding of a multicentre study in Europe (51%),6 but higher than the 46% reported from the USA5 and the 35% from France.19 However, only blood pressure fluctuations and bladder and bowel dysfunctions were assessed, suggesting that the prevalence of dysautonomia might have been higher if other functions of the autonomic nervous system had also been assessed. In this study, the predominant autonomic dysfunction was blood pressure fluctuation emphasizing the need for close monitoring of the cardiovascular function of children with GBS. The incidence of cranial nerve dysfunction in our patients (27.5%) was lower than that reported from the United States5 and Europe.6,19 Bulbar palsy was the most common cranial nerve dysfunction in this study, a finding similar to that reported from India18 and Pakistan.30 However, facial nerve palsy was the most commonly involved cranial nerve in other studies.19,31 The typical CSF albuminocytological dissociation of GBS was demonstrated in 79.4% of those who underwent lumbar puncture, a finding similar to a report from Denmark (80%),3 but higher than the 73% and lower than the 88% reported from France19 and China,7 respectively.
Admission to ICU is recommended for children with GBS who have rapidly progressive weakness, severe autonomic dysfunction, severe swallowing dysfunction and/or diminished cough reflex or imminent respiratory insufficiency.32 Although 63 (61.8%) of the patients needed ICU care, only 43 of them (68.3%) were admitted to ICU as the number of ICU beds are limited in this setting. Although 31 patients (30.4%) required mechanical ventilation (due to respiratory muscle involvement and/or bulbar palsy), only 24 of them (77.4%) managed to get the service due to shortage of ventilators. The proportion of patients that required mechanical ventilation in this study is higher than the 10% and 13% reported from France19 and Germany,6 respectively. Our finding also showed a higher percentage of GBS cases that required mechanical ventilation compared to what was reported previously from Ethiopia.27
GBS is a potentially life-threatening disease that requires supportive medical care and immunological treatment.1 However, the cost of immunotherapy in low-income countries is unaffordable to the majority of patients. In this setting, only 5.9% of the patients received IVIG while 41.7% and 91% of children with GBS received the treatment according to reports from Mexico33 and France,19 respectively. The big management gap between developing and developed countries underscores the need for designing a mechanism to avail an affordable and effective treatment to children with (at least) the severe forms of GBS in resource-poor settings. In this study, treatment for nosocomial infections was documented in 35.3% of children with GBS - a finding higher than the 20.8% reported from Mexico.33
Mortality from complications of GBS is generally low (1–2%).34 However, it is higher in developing countries than what has been reported from developed countries.4 The 12.7% mortality during the acute phase in our setting was comparable to the 11.5% reported from India18 and the 11% from Bangladesh35 but higher than figures reported from Spain (3.5%),36 Korea (0%)20 and France (0%).19
The high mortality in this setting could partly be related to the small number of patients that received ICU care.15 Several factors were reported to have association with mortality in previous studies. The presence of respiratory distress,16 axonal variant of GBS and severity of weakness,35 and lack of ICU care15 were some of the reported determinants of mortality. In our study, respiratory failure was the only determinant of mortality. We could not evaluate the association between GBS variants and mortality as no patient had NCS; and the absence of other determinants of mortality in this study may be related to the small number of study subjects.
Our study has a number of limitations. First, we were unable to include patients with atypical presentation that could have resulted in selection bias; and the results of the study might have been different if patients with atypical GBS had also been included. As none of the patients included in the study were subjected to NCS-EMG, we could not describe the subtypes of the disease, and the level of diagnostic certainty is reduced with possible inclusion of some GBS mimickers with more severe (or benign) presentations that may affect the prognosis. The other limitation of the study comes from its retrospective nature as some important data (for example, duration from disease onset to nadir, some features of autonomic dysfunction, type and severity of pain, reasons why lumbar puncture was not done for some of the patients) were missed. Moreover, the long-term outcome of our patients was not studied.
Conclusion
The study tried to describe the clinical presentation and short-term outcome of pediatric GBS in a resource poor setting. There is a gap in the diagnosis and management of children with GBS in southern Ethiopia; and mortality from the disease is higher than reports from other settings. Efforts should be undertaken to improve the diagnostic capabilities and to design mechanisms to avail treatment to children with GBS in resource poor settings to improve outcome. We recommend a prospective multicentre study with an adequate follow-up period to determine the variants of GBS and the long-term outcome of children with GBS in this setting.
Abbreviations
AFP, acute flaccid paralysis; GBS, Guillain Barre syndrome; CSF, cerebrospinal fluid; ICU, intensive care unit; SPSS, Statistical Package for Social Sciences; IVIG, intravenous immunoglobulin; MV, mechanical ventilation; IQR, interquartile range; NCS-EMG, nerve conduction study-electromyography.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
The authors are grateful to all individuals who participated in the data collection.
Author Contributions
All authors contributed significantly to this work in the conception, study design, execution, data acquisition, analysis, and interpretation; participated in the drafting, revising, or critical review of the article; gave final approval of the version to be published; agreed on the journal to which the article will be submitted; and agreed to be responsible for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. Willison HJ, Jacobs BC, van Doorn PA. Guillain-Barré syndrome. Lancet. 2016;388(10045):717–727. doi:10.1016/S0140-6736(16)00339-1
2. Yuki N, Hartung H. Review article: Guillain–Barré syndrome. N Engl J Med. 2012;366:2294–2304. doi:10.1056/NEJMra1114525
3. Levison LS, Thomsen RW, Markvardsen LK, Christensen DH, Sindrup SH, Andersen H. Pediatric Guillain-Barré Syndrome in a 30-year nationwide cohort. Pediatr Neurol. 2020;107:57–63. doi:10.1016/j.pediatrneurol.2020.01.017
4. Papri N, Islam Z, Leonhard SE, Mohammad QD, Endtz HP, Jacobs BC. Guillain–Barré syndrome in low-income and middle-income countries: challenges and prospects. Nat Rev Neurol. 2021;17(5):285–296. doi:10.1038/s41582-021-00467-y
5. Hicks CW, Kay B, Worley SE, Moodley M. A clinical picture of Guillain-Barré Syndrome in children in the United States. J Child Neurol. 2010;25(12):1504–1510. doi:10.1177/0883073810370481
6. Korinthenberg R, Schessl J, Kirschner J. Clinical presentation and course of childhood Guillain-Barré syndrome: a prospective multicentre study. Neuropediatrics. 2007;38(1):10–17. doi:10.1055/s-2007-981686
7. Tang J, Dai Y, Li M, et al. Guillain-Barré syndrome in Chinese children: a retrospective analysis. Pediatr Neurol. 2011;45(4):233–237. doi:10.1016/j.pediatrneurol.2011.06.007
8. Van Den Berg B, Walgaard C, Drenthen J, Fokke C, Jacobs BC, Van Doorn PA. Guillain-Barré syndrome: pathogenesis, diagnosis, treatment and prognosis. Nat Rev Neurol. 2014;10(8):469–482. doi:10.1038/nrneurol.2014.121
9. Wu X, Shen D, Li T, et al. Distinct clinical characteristics of pediatric guillain-Barré syndrome: a comparative study between children and adults in Northeast China. PLoS One. 2016;11(3):1–12.
10. Roodbol J, De Wit MCY, Walgaard C, De Hoog M, Catsman-Berrevoets CE, Jacobs BC. Recognizing Guillain-Barré syndrome in preschool children. Neurology. 2011;76(9):807–810. doi:10.1212/WNL.0b013e31820e7b62
11. Asbury AK, Cornblath DR. Assessment of current diagnostic criteria for Guillain‐Barré syndrome. Ann Neurol. 1990;27(1S):S21–4. doi:10.1002/ana.410270707
12. Sejvar JJ, Kohl KS, Gidudu J, et al. Guillain-Barré syndrome and Fisher syndrome: case definitions and guidelines for collection, analysis, and presentation of immunization safety data. Vaccine. 2011;29(3):599–612. doi:10.1016/j.vaccine.2010.06.003
13. Nepal G, Shrestha GS, Shing YK, Yadav JK, Coghlan MA, Ojha R. Low-cost alternatives for the management of Guillain-Barré syndrome in low- and middle-income countries. World Med Heal Policy. 2021;13(4):749–757. doi:10.1002/wmh3.474
14. Care N, Orlikowski D, Prigent H, Sharshar T, Lofaso F, Raphael JC. Respiratory Dysfunction in Guillain-Barré Syndrome. Neurocrit Care. 2004;1:415–422. doi:10.1385/NCC:1:4:415
15. Ishaque T, Jacobs MC, Zhahiru I. High mortality from Guillain-Barré syndrome in Bangladesh. J Peripher Nerv Syst. 2017;22(2):121–126. doi:10.1111/jns.12215
16. Hosseininezhad M, Khatami SS, Saadat S, et al. Ten years evaluation of epidemiology- and mortality-related factors in adults and children with Guillain-Barré syndrome in the north of Iran. Neurol Sci. 2022;43(3):1929–1938. doi:10.1007/s10072-021-05562-y
17. Berg B, Bunschoten C, Doorn PA. Mortality in Guillain-Barré syndrome. Neurology. 2013;80:6–11.
18. Kalra V, Sankhyan N, Sharma S, Gulati S, Choudhry R, Dhawan B. Outcome in childhood Guillain-Barré syndrome. Indian J Pediatr. 2009;76(8):795–799. doi:10.1007/s12098-009-0125-y
19. Estrade S, Guiomard C, Fabry V, et al. Prognostic factors for the sequelae and severity of Guillain-Barré syndrome in children. Muscle Nerve. 2019;60(6):716–723. doi:10.1002/mus.26706
20. Lee JH, Sung IY, Rew IS. Clinical presentation and prognosis of childhood Guillain-Barré syndrome. J Paediatr Child Health. 2008;44(7–8):449–454. doi:10.1111/j.1440-1754.2008.01325.x
21. Hughes RAC, Newsom-Davis JM, Perkin GD, Pierce JM. Controlled Trial of Prednisolone in Acute Polyneuropathy. Lancet. 1978;312(8093):750–753. doi:10.1016/S0140-6736(78)92644-2
22. Korinthenberg R, Trollmann R, Felderhoff-Müser U, et al. Diagnosis and treatment of Guillain-Barré Syndrome in childhood and adolescence: an evidence- and consensus-based guideline. Eur J Paediatr Neurol. 2020;25:5–16. doi:10.1016/j.ejpn.2020.01.003
23. Doets AY, Verboon C, van den Berg B, et al. Regional variation of Guillain-Barré syndrome. Brain. 2018;141(10):2866–2877. doi:10.1093/brain/awy232
24. Sipilä JOT, Soilu-Hänninen M, Ruuskanen JO, Rautava P, Kytö V. Epidemiology of Guillain-Barré syndrome in Finland 2004–2014. J Peripher Nerv Syst. 2017;22(4):440–445. doi:10.1111/jns.12239
25. Mathew T, Srinivas M, Nadig R, Arumugam R, Sarma GRK. Seasonal and monthly trends in the occurrence of Guillain-Barre syndrome over a 5-year period: a tertiary care hospital-based study from South India. Ann Indian Acad Neurol. 2014;17(2):239–241. doi:10.4103/0972-2327.132662
26. Woyessa AB, Mengesha M, Belay D, et al. Epidemiology of influenza in Ethiopia: findings from influenza sentinel surveillance and respiratory infection outbreak investigations, 2009–2015. BMC Infect Dis. 2018;18(1):1–10. doi:10.1186/s12879-018-3365-5
27. Bacha T, Gezahegn W, Amare A. The clinical presentation, epidemiology, and short-term outcome of guillain-barré syndrome in tikuranbessa hospital: a 6-year retrospective study. Ethiop Med J. 2018;56(2):141–146.
28. Kim SH, Samadov F, Mukhamedov A, et al. Clinical characteristics and prognostic factors of children with Guillain-Barré syndrome. Ann Child Neurol. 2019;27(4):113–119. doi:10.26815/acn.2019.00143
29. Howlett WP, Vedeler CA, Nyland H, Aarli JA. Guillain-Barré syndrome in northern Tanzania: a comparison of epidemiological and clinical findings with western Norway. Acta Neurol Scand. 1996;93(1):44–49. doi:10.1111/j.1600-0404.1996.tb00169.x
30. Khan RSY, Ali S, Irfan S, Naseem F. Frequency of cranial nerve involvement in patients with syndrome. Ann Pak Inst Med Sci. 2015;11(3):115–118.
31. Incecik F, Hergüner MO, Altunbasak S. Guillain-Barré syndrome in children. Neurol Sci. 2011;32(3):381–385. doi:10.1007/s10072-010-0434-y
32. Leonhard SE, Mandarakas MR, Gondim FAA, et al. Diagnosis and management of Guillain–Barré syndrome in ten steps. Nat Rev Neurol. 2019;15(11):671–683. doi:10.1038/s41582-019-0250-9
33. Solana-Rojas Á, García-Melo LM, Reyes-Varela MD, et al. Clinical severity and associated complications in pediatric patients with Guillain-Barré syndrome. Rev Mex Neurocienc. 2020;21(1):15–26.
34. Ryan MM. Guillain–Barr ´e syndrome in childhood. J Paediatr Child Health. 2005;41:237–241. doi:10.1111/j.1440-1754.2005.00602.x
35. Hasan I, Papri N, Hayat S, et al. Clinical and serological prognostic factors in childhood Guillain-Barré syndrome: a prospective cohort study in Bangladesh. J Peripher Nerv Syst. 2021;26(1):83–89. doi:10.1111/jns.12434
36. Sedano MJ, Orizaola P, Gallardo E, et al. A unicenter, prospective study of Guillain-Barré syndrome in Spain. Acta Neurol Scand. 2019;139(6):546–554. doi:10.1111/ane.13092
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.