")
Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 14
Pediatric Autologous Hematopoietic Stem Cell Transplantation: Safety, Efficacy, and Patient Outcomes. Literature Review
Authors Testi AM , Moleti ML , Angi A, Bianchi S, Barberi W , Capria S
Received 20 January 2023
Accepted for publication 12 May 2023
Published 31 May 2023 Volume 2023:14 Pages 197—215
DOI https://doi.org/10.2147/PHMT.S366636
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Anna Maria Testi, Maria Luisa Moleti, Alessia Angi, Simona Bianchi, Walter Barberi, Saveria Capria
Department of Translational and Precision Medicine, Sapienza, University of Rome, Rome, Italy
Correspondence: Anna Maria Testi, Hematology, Department of Translational and Precision Medicine, Sapienza University of Rome, Via Benevento 6, Rome, 00161, Italy, Tel +39-06-49974731, Fax +39-06-44241984, Email [email protected]
Abstract: Autologous stem cell transplantation (auto-HSCT) is a part of the therapeutic strategy for various oncohematological diseases. The auto-HSCT procedure enables hematological recovery after high-dose chemotherapy, otherwise not tolerable, by the infusion of autologous hematopoietic stem cells. Unlike allogeneic transplant (allo-HSCT), auto-HSCT has the advantage of lacking acute-graft-versus-host disease (GVHD) and prolonged immunosuppression, however, these advantages are counterbalanced by the absence of graft-versus-leukemia. Moreover, in hematological malignancies, the autologous hematopoietic stem cell source may be contaminated by neoplastic cells, leading to disease reappearance. In recent years, allogeneic transplant-related mortality (TRM) has progressively decreased, almost approaching auto-TRM, and many alternative donor sources are available for the majority of patients eligible for transplant procedures. In adults, the role of auto-HSCT compared to conventional chemotherapy (CT) in hematological malignancies has been well defined in many extended randomized trials; however, such trials are lacking in pediatric cohorts. Therefore, the role of auto-HSCT in pediatric oncohematology is limited, in both first- and second-line therapies and still remains to be defined. Nowadays, the accurate stratification in risk groups, according to the biological characteristics of the tumors and therapy response, and the introduction of new biological therapies, have to be taken into account in order to assign auto-HSCT a precise role in the therapeutic strategies, also considering that in the developmental age, auto-HSCT has a clear advantage over allo-HSCT, in terms of late sequelae, such as organ damage and second neoplasms. The purpose of this review is to report the results obtained with auto-HSCT in the different pediatric oncohematological diseases, focusing on the most significant literature data in the context of the various diseases and discussing this data in the light of the current therapeutic landscape.
Keywords: autologous stem cell transplant, pediatric age, acute leukemia, chronic myeloid leukemia, Hodgkin lymphoma, non-Hodgkin lymphoma
Acute Myeloid Leukemia (AML)
The current probability of event-free survival (EFS) and overall survival (OS), for children with acute myeloid leukemia (AML) ranges between 45–50% and 65–70%, at 3–10 years, respectively.1 Improvement of prognosis in children, but also adults, is due to better patient stratification in risk groups, which has made it possible to adapt the treatment to the clinical-biological characteristics of the disease. Allo-HSCT has increasingly been used in high-risk (HR) patients, and the improvement of supportive therapy and the optimization of induction and consolidation strategies have decreased therapy-related toxicity. Currently, new target therapies are also beginning to be used in pediatric age.2
Over the past years, randomized studies have been carried out to clarify the role of auto-HSCT in AML patients in first remission (CR1) (Table 1).2 Two previous meta-analyses showed that auto-HSCT, compared with standard consolidation CT, improved the EFS but not the OS.3–5 In children with AML in CR1, auto-HSCT seemed to decrease the number of relapses and, consequently, improve disease-free survival (DFS) and OS.6 Data from 13 studies of 12 randomized controlled trials (12 adult, 9 pediatric), including a total of 3027 patients (377 children), were collected.3,4 The conditioning regimen usually included Busulfan (BU) and Cyclophosphamide (CY), however, in one trial bone marrow cells were in vitro chemo-purged with 4-hydroperoxycyclophosphamide (4-HC). Auto-HSCT, in adult AML patients in CR1, improved DFS compared with CT (HR = 0.98; 95% CI = 0.80–0.98); in children, there were no statistical differences in relapse incidence, TRM, DFS and OS (Table 1).7–11 The authors concluded that in children and adolescents with CR1 AML, auto-HSCT does not add benefit compared to CT. Furthermore, the late toxicity associated with the pre-auto-HSCT conditioning regimen has to be considered in young patients who have a longer life expectancy.12
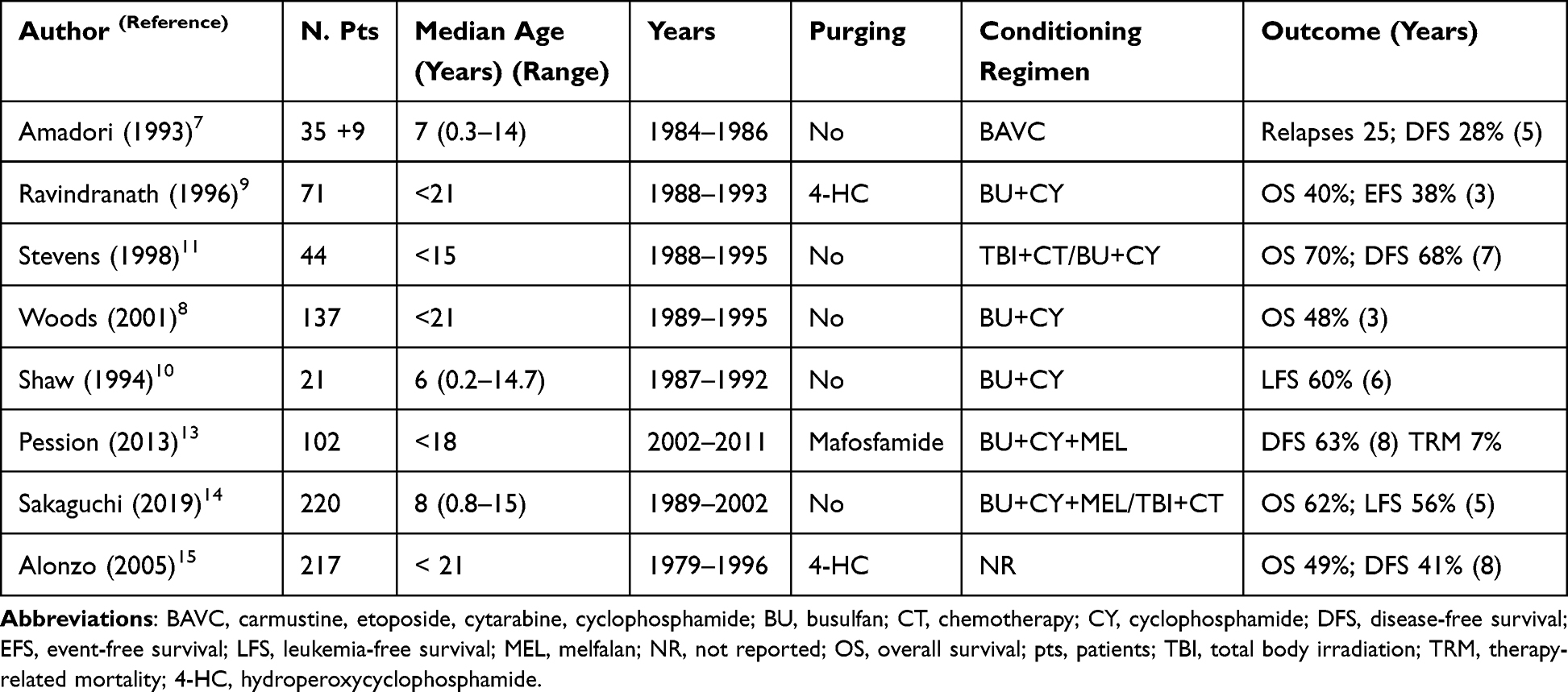 |
Table 1 Results of Autologous Hematopoietic Stem Cell Transplant in Pediatric Acute Myeloid Leukemia in First Complete Remission |
Subsequently, Pession et al published data on 482 children with de novo AML treated with the Associazione Italiana di Ematologia e Oncologia Pediatrica (AIEOP) 2002/2001 protocol from December 2002 to June 2011.13 In this trial, the children were stratified into risk groups and the transplant procedures, either allo- or auto-HSCT, were reserved for those at HR. One hundred and forty-one children received allo-HSCT, and 102 were autotransplanted after induction and consolidation therapy. The 8-year DFS was 73% and 63% for allo- and auto-HSCT, respectively; the 8-year cumulative incidence (CI) of relapse was 17% versus 28% and no difference in the CI of TRM was observed (7% in both cohorts) (Table 1).
In the attempt to identify the optimal conditioning regimen before auto-HSCT in children with AML in CR1, the Pediatric AML Working Group of the Japan Society for Hematopoietic Cell Transplantation (JSHCT) analyzed 220 children autotransplanted between 1989 and 2022.14 Different conditioning regimens were employed and included: BU+melfalan (MEL), BU+CY±etoposide (ETP), BU+Cytarabine (CA)+ETP, BU+CY+CA, and BU+MEL+ETP or total-body irradiation (TBI). The 5-year OS was 62% and 61% for children receiving CT and TBI, respectively. However, more favorable results were obtained by patients receiving BU+MEL and BU+CY+ETP compared to those treated with TBI, or other BU-based regimens: the OS rates were 74%, 49% and 61%, respectively. A higher relapse rate was observed in the other BU-based regimens, and the non-relapse mortality (NRM) was higher after TBI (Table 1). Also in this paper, the authors argue in favor of conditioning regimens that do not include TBI, responsible for major short- and long-term toxicity.
In the same years, other published papers reported the results of several trials comparing consolidation CT with auto-HSCT in children with CR1 AML; all of them agreed that auto-HSCT offered no benefit over CT.12,15–18 In these studies, the high NRM associated with auto-HSCT was probably due to the use of bone marrow (BM) stem cells source and TBI in the conditioning regimen.
Over the last three decades, the introduction of peripheral blood stem cells (PBSC) leading to a faster hematologic recovery and the improvement in supportive care, with better management of infections, lowered the TRM of auto-HSCT. Moreover, due to recent advances in understanding the leukemogenesis mechanisms that have led to new prognostic risk stratification, and to the highly sensitive techniques for minimal residual disease (MRD) monitoring, auto-HSCT has gained a place in selected categories of adult patients. On the contrary, at least in the major childhood AML study groups, where the genomic landscape of the disease drives the modern therapeutic strategies, auto-HSCT is no longer used as post-remission AML therapy. Currently, children with favorable risk AML are supposed to receive intensive consolidation CT without transplant, while patients with HR genetic features are directed to allo-HCT in CR1.
Treatment of AML is quickly changing in adults, yet advances in pediatrics are slower to evolve. Tailored drugs, such as gemtuzumab-ozogamicin (GO) and FLT3 inhibitors, have only recently been incorporated into pediatric trials, and the optimal way to include them in therapy is still under investigation.2 In the future, the role of auto-HSCT could be re-defined, as a consequence of the implementation of new drugs in the initial treatment phases, even in pediatric age.
Take Home Messages
- Several pediatric studies have reported that auto-HSCT during CR1 in patients not HR had no major advantage over CT alone; allo-HSCT is recommended for those at HR
- In most pediatric AML study groups, auto-HSCT is no longer used in consolidation therapy
- The role of auto-HSCT could be re-defined as a consequence of the implementation of new drugs in the initial treatment phases, even in children
Acute Promyelocytic Leukemia (APL)
The current combination of all-trans retinoic acid (ATRA) and arsenic trioxide (ATO) with, or without low dose CT, achieves cure rate in more than 90% of children and adults with acute promyelocytic leukemia (APL), and disease recurrence has become a very rare event. HSCT is no longer part of first-line therapy in these patients. HSCT, either allogeneic or autologous, has been successfully used as consolidation for patients in second remission (CR2) and appears to offer better results than CT.19–21 The Acute Leukemia Working Party (ALWP) of the European Society for Blood and Marrow Transplantation (EBMT) reported the results of 341 and 228 patients with APL in CR2 consolidated with auto- and allo-HSCT, respectively.21,22 The probability of EFS was significantly higher in autotransplanted patients compared to those who underwent allo-HSCT (5-year EFS: 75% vs 55%). Similar results have been reported in other large patient series and all confirm the best OS in autotransplant patients.20–23 Peripheral blood was the preferred stem cell source in most of these studies.
Most of the data refers to adult patients with relapsed/refractory APL. Small pediatric series were reported: 5 children in molecular CR2, after ATO salvage therapy, underwent auto-HSCT and all of them were in continuous CR2 at the time of the analysis;24 another 9 children were salvaged with ATO followed by consolidation auto-HSCT that allowed long-term survival in 5 of them.24 Dvorak et al described 32 pediatric cases with relapsed/refractory APL; the 5-year EFS and OS for the 11 children consolidated with auto-HSCT were 82% and 76% and the incidence of TRM and CI of relapse were 0% and 19% (Table 2).25
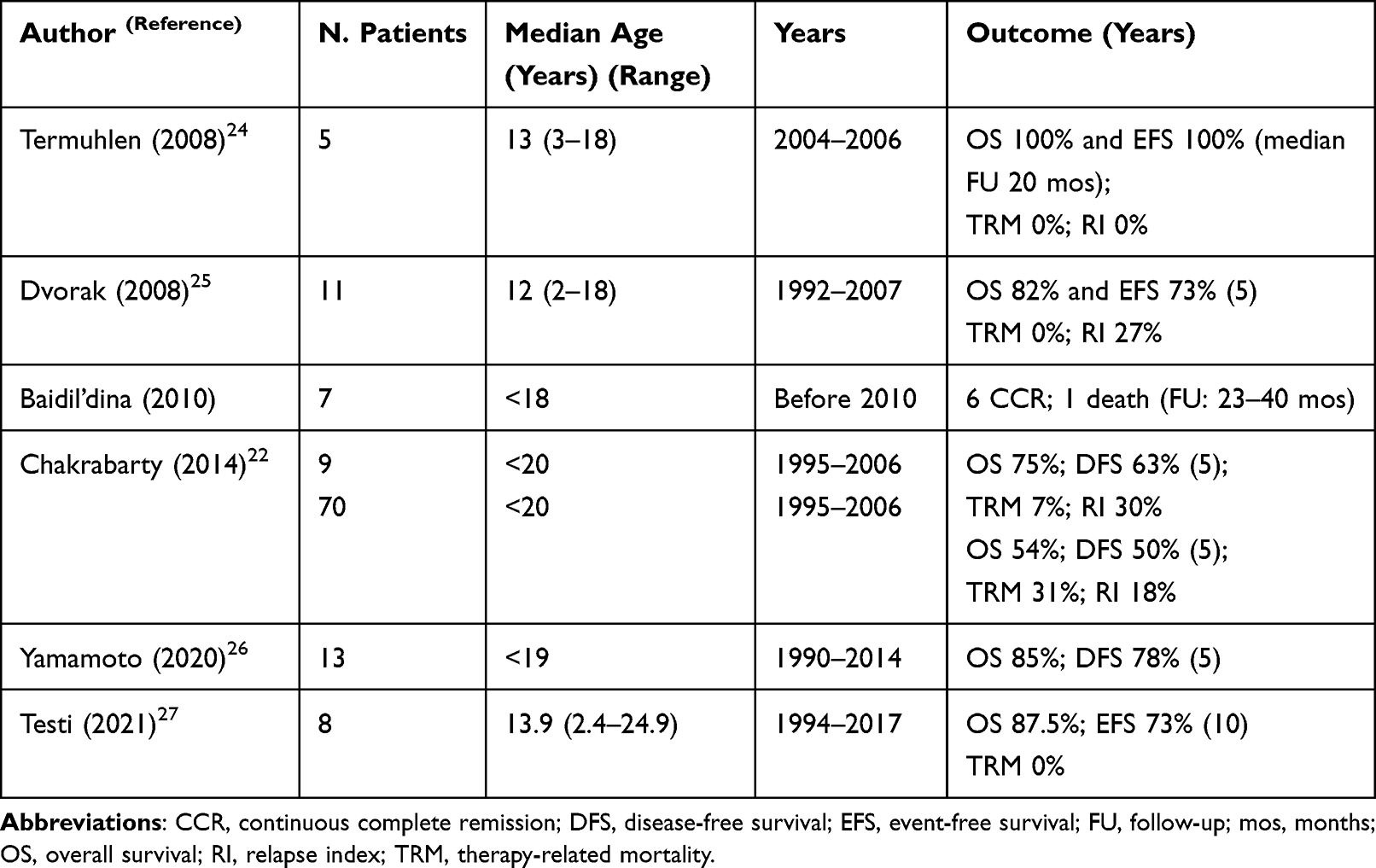 |
Table 2 Results of Autologous Hematopoietic Stem Cell Transplant in Pediatric Acute Promyelocytic Leukemia in Second Complete Remission |
A large number of patients (294 cases; 79 of them aged <20 years) with APL in CR2 receiving allo-HSCT (232), or auto-HSCT (62) as consolidation, were retrospectively analyzed.22 The 5-year OS and DFS favoured autologous transplant compared to allo-HSCT (75% vs 54% and 63% vs 50%, respectively). The use of ATO pre-HSCT and molecular or cytogenetically positive grafts were not associated with an increased risk of relapse and overall mortality (Table 2). The largest pediatric APL series (95 children treated between 1990 and 2014) was reported by the Japan Society of Hematopoietic Cell Transplantation (JSHCT); 40 children underwent transplant in CR1, 41 in CR2, 3 in CR3 and 11 with persistent disease.26 Both auto- and allo-HSCT were effective in children transplanted in CR2 (5-year OS 85% vs 78%; DFS 76% vs 75%). Data on salvage induction therapy and pre-transplant molecular response were not reported in this study.
This data has been confirmed by the 25-year Italian experience on relapsed/refractory children and adolescents with APL.27 Eight patients in CR2 were consolidated with auto-HSCT and 17 with allo-HSCT. No significant differences between the two transplant procedures have been observed; the 10-year OS and EFS were 87.5% vs 76% and 72.9% vs 70.6%, respectively (Table 2).
Members of the North American Childrens’ Oncology Group (COG) and International Berlin-Frankfurt-Munster Study Group (I-BFM-SG) reported recommendations on pediatric APL salvage therapy.23 According to previous publications and personal experiences, the following characteristics have been considered unfavourable for patient outcomes: short time to relapse, previous ATO treatment and failure to clean PML-RARA transcript. Consolidation auto-HSCT is recommended for children not previously treated with ATO, an early relapse, and a molecular CR2. Auto-HSCT is also included in consolidation phase for pediatric patients previously treated with ATO, a late relapse and a molecular CR2 after consolidation. Recommended conditioning regimens do not include TBI, but BU + CY ± MEL.
The best management of children with APL and an extramedullary relapse remains to be determined.23 The European LeukemiaNet, in 2009, suggested HSCT for patients with central nervous system (CNS) relapse.19
In these patients, HD-CA followed by auto-HSCT had been previously employed successfully.28 More recently, the use of ATO, which can reach therapeutic levels in the CNS, would seem to be of greater benefit in localization of the disease in the CNS.
Take Home Messages
- The current treatment with ATRA/ATO, in combination, or not, with CT, has significantly improved the prognosis of children and adults with APL, and auto-HSCT is no longer indicated as first-line treatment consolidation
- For patients in CR2, consolidation with auto-HSCT has resulted in better outcomes than non-transplant strategies
- The outcome of patients autotransplanted in CR2 is particularly favourable, if molecularly negative cells are collected
- No impact of ATO-containing versus no-ATO salvage regimens pre-auto-HSCT on the relapse risk after transplant was observed
- The role of auto-HSCT in children with extramedullary relapse is still controversial, although it was recommended by the European LeukemiaNET in 2009
Acute Lymphoblastic Leukemia (ALL)
Currently, allo-HSCT is considered the best consolidation treatment for adults and children with very HR (VHR) acute lymphoblastic leukemia (ALL) in CR1, and for those in second or subsequent remission. Auto-HSCT has been reserved for patients who were ineligible for allo-HSCT, or for those who did not have a matched related or unrelated donor. In an attempt to eliminate pathological cells from the marrow taken from patients, specific drugs such as mafosfamide (4-HC), or monoclonal antibodies (MoAbs), directed against leukemia cell antigens have been used in vitro, with similar results.29,30 Pre-HSCT conditioning regimens frequently included TBI (80% of patients); the 3-year DFS ranged from 25% to 35% and TRM from 5% to 21%, but most patients had disease recurrence. Unsatisfactory results were obtained mainly in children undergoing auto-HSCT after early relapses or in third/subsequent remissions (Table 3).29,30 For late relapses (>2 years from diagnosis) of B precursor ALL, the prognosis after auto-HSCT consolidation appeared better with 3-year EFS of more than 50%. The Spanish Pediatric BM Transplant Units reported data of 55 children with ALL in CR2, undergoing auto-HSCT with in vitro BM stem cells purged (MoAbs and complement, or magnetic microsphere).31 Pre-transplant conditioning regimens included CT associated, or not, to TBI; the 6-year EFS probability was 46%; first CR duration statistically influenced the patients’ outcome (Table 3). TBI included conditioning regimen resulted in better results.
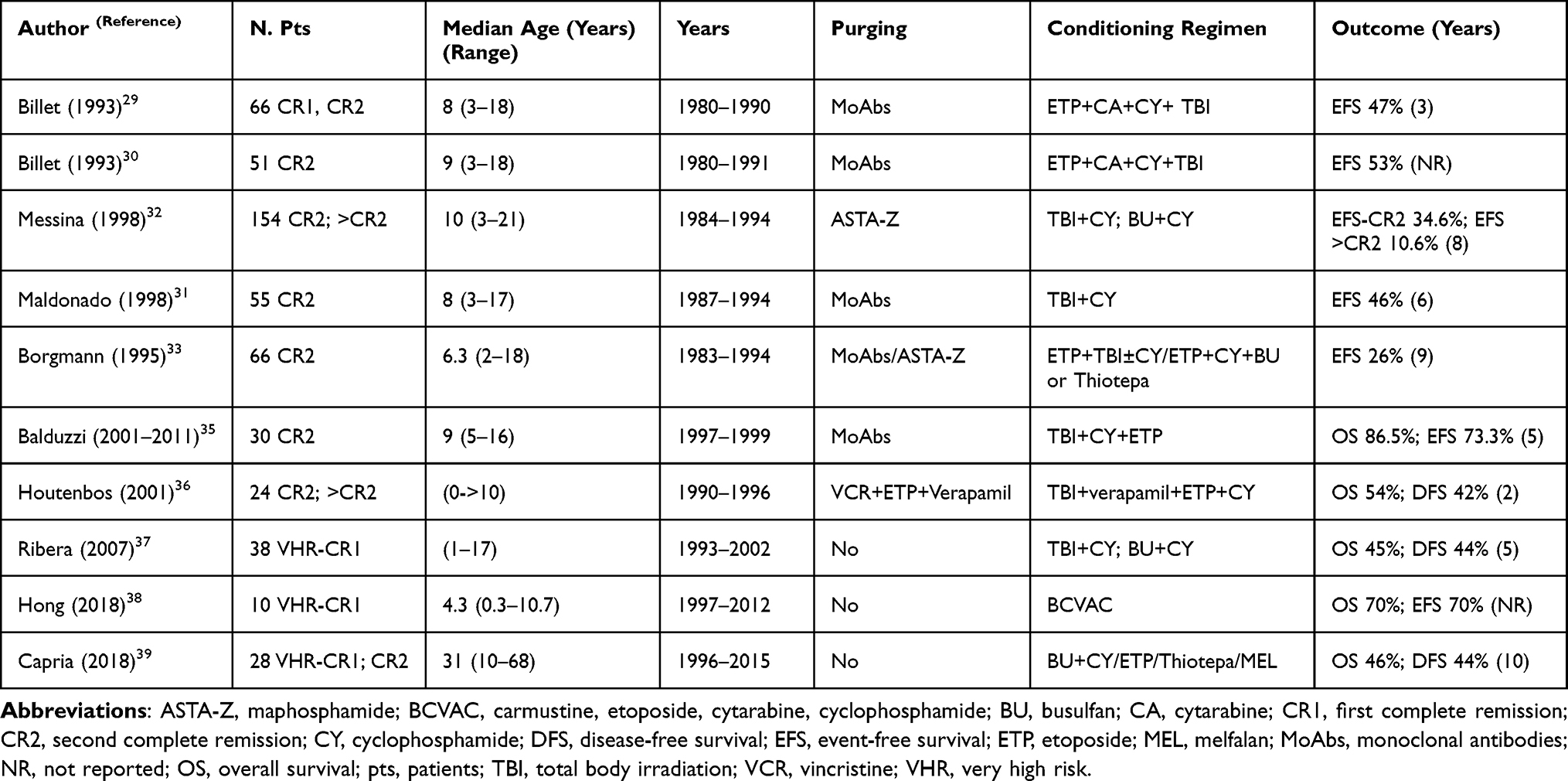 |
Table 3 Results of Autologous Hematopoietic Stem Cell Transplant in Pediatric Acute Lymphoblastic Leukemia in CR2 and VHR CR1 |
In 10 Italian pediatric centres, 154 children with ALL in second, or subsequent remission, underwent auto-HSCT. Indications to autologous transplant were as follows: relapse within 30 months from diagnosis, HR criteria at diagnosis, lack of any suitable donor, and third or subsequent CR. TRM occurred in 9.7% of patients and the 8-year EFS was 34.6% for children transplanted in CR2, and 10.6% for those in subsequent CR. As in the previous Spanish reports, better results were obtained in children receiving TBI including conditioning regimen (8-year EFS 48% vs 15.4%; p = 0.0023), and in those with extramedullary relapse, compared with patients with BM relapse (8-year EFS 68% vs 18%) (Table 3).32
Treatment results for children who underwent auto-HSCT, and for those who had CT in CR2, were retrospectively compared (BFM).33 Eight hundred and eighty-nine patients (age <18 years), with first ALL relapse were enrolled in the BFM multicenter trials; 682 received conventional CT-radiotherapy, 207 underwent HSCT (66 auto-, 141 allo-HSCT). Patients with early BM relapse, or with T-cell ALL, lacking a matched donor, were submitted to auto-HSCT. After a median follow-up of 55 months, the 9-year EFS rates were 32% and 26% for patients receiving CT and auto-HSCT, respectively. Similar results were achieved in the 38 patients treated with late relapse: the 9-year EFS were 55% and 41% and TRM 2% and 4%, respectively for CT and auto-HSCT. However, aside from acute procedure-related toxicity, the authors expressed their concerns regarding the late sequelae in transplant survivors (infertility, growth retardation, endocrine defects, or marrow function), less likely to occur after conventional CT.33
The results of children with ALL who underwent auto-HSCT with in vitro purified leukoapheretic products were subsequently reported. In an Italian center, BM collected cells treated with MoAbs were utilized in 11 children with late relapse of B precursor ALL, in CR2.34 The efficacy of in vitro leukemia eradication was assessed by polymerase-chain reaction (PCR) and children rescued with PCR negative cells had 2-year EFS of 89%. These results were confirmed in 30 Italian children with B-cell precursor ALL, in CR2 after isolated extramedullary relapse and/or late relapse.35
Subsequently, 103 children treated in the same period with CT (BFM best salvage chemotherapeutic schema) were compared to the 30 autotransplanted patients. The 103 control cases matched the 30 autografted patients, according to site of relapse, CR1 duration, time elapsed in CR2 and period of relapse. The 5-year EFS and OS were 73.3% and 86.5% for autotransplanted cases, and 40% and 62.5% for CT-treated controls. The final analysis showed an advantage of purified auto-HSCT, compared with CT in low-risk relapsed ALL, possibly explained by the single-centre effect, the myeloablation of TBI, and the stem cell isolation procedure (Table 3).35
In the USA, in the attempt to reduce the relapse rate associated with auto-HSCT, five children with HR ALL in CR1, and 19 in second, or subsequent CR, lacking matched family allogeneic donors underwent auto-HSCT with chemopurged BM, utilizing verapamil, vincristine (VCR) and ETP. Conditioning regimen included TBI, verapamil bolus, ETP and CY.36 Additionally, based on previous adult experiences demonstrating that post-transplant immune-CT may reduce the risk of relapse, seven children received cyclosporine A (CsA) and alpha-interferon (αIFN), 13 patients CsA, and six alternating cycles of αIFN and CT, plus six additional CT cycles (VCR, ETP, CA, prednisone) and, the last four patients, CsA, alone. The 2-year DFS and OS were 42% and 54%, respectively. Patients receiving post-transplant immune-CT compared with those receiving immunotherapy alone, had a better 2-year DFS and OS (69% versus 13% and 85% versus 25%, respectively). Chemopurged auto-HSCT, combining with post-transplant immune-CT, usually well tolerated, represented an alternative approach in the treatment of a subset of children with HR ALL in CR1, CR2 and subsequent CR, lacking allogeneic donor. The immune-CT after transplant may be a method to eradicate residual leukemic disease and consequently, to decrease the high relapse rate associated with auto-HSCT.36
In the past years, auto-HSCT was part of the consolidation therapy for children in CR1 with VHR ALL. The Programa Espanol de Tratamientos en Hematologia (PETHEMA) ALL-93 trial compared intensive CT, allo-HSCT and auto-HSCT for ALL children with the following characteristics: age <1 year, B-lineage ALL with initial WBC ≥300.0x109/L, T-lineage ALL with diagnostic WBC ≥100.0x109/L, t(9;22), t(4;11) or other 11q23 rearrangements.37 Patients in CR with an HLA-identical sibling received allo-HSCT, whereas the remaining patients were randomly assigned to auto-HSCT, or delayed intensification CT and maintenance. The three groups were comparable in the main pre-treatment ALL characteristics. No differences for donor versus no donor in the 5-year DFS (45%), as well as for auto-HSCT versus CT comparison (5-year DFS: 44% vs 46%), were found (Table 3); similar outcomes were observed within the different ALL subgroups (Table 3). However, the overall results obtained in this trial confirmed the poor prognosis of these VHR-ALL children.
The Japanese Society of Hematology reported the results achieved in children with VHR ALL lacking HLA-matched allogeneic donors and treated with HD-CT, auto-HSCT followed by maintenance CT.38 Between 1997 and 2012, patients in CR1 received HD-CA and ETP, and G-CSF for peripheral blood stem cells mobilization; BAVC (carmustine, ETP, CA and CY) was used as pre-transplant conditioning regimen. The OS and EFS for the 10 treated children were 70% (median follow-up 7.4 years) (Table 3). No severe adverse events were observed during treatment.
In more recent years, the ALL therapeutic protocols, first for children and then also for adults, have included the evaluation of MRD assessed by flow cytometry (MFC) and/or PCR in the early phases of treatment (at the end of induction and consolidation). This has allowed a more precise classification of patients into risk categories, and a better identification of patients who need to undergo allo-HSCT.39 In addition, the improvement of MRD detection strategies may help to identify a specific subgroup of ALL cases, MRD-negative and ineligible for allogeneic transplantation that could be considered for auto-HSCT. In our centre, 28 ALL patients (adults and children; 20 in CR1 and 8 in CR2) were treated with HD-CT and auto-HSCT, followed by standard maintenance and intrathecal CT for 1 year. Pre-transplant MRD was tested in BM by MFC (11 cases), and PCR-based assay in 17 cases (Table 3).39 Twenty-two patients were MRD negative and six were positive. MRD was also investigated in the apheretic product in 22 patients and proved negative in 20 of them. The 10-year DFS was 59% for patients MRD negative compared to 0% for MRD positive ones (all patients MRD positive relapsed). Moreover, the DFS was 83% for patients MRD negative by PCR.
Patients with isolated extramedullary relapse appeared to benefit from HD-CT and auto-HSCT. Despite the relatively small number of patients, these results confirmed the role of molecular negativity at the time of transplant and corroborated the concept that patients with isolated extramedullary relapse may have an excellent likelihood of achieving long-term DFS with consolidation auto-HSCT.
Take Home Messages
- Allo-HSCT is currently the standard of care for HR ALL children in CR1, or subsequent CR
- Different techniques, either pharmacologic or immunologic, to purge stem cell collection, have been used, and comparable results have been reported
- Patients with isolated extramedullary relapse achieve long-term DFS with auto-HSCT, if they present a molecular negative disease at the time of transplant
- In the future, the improvement of MRD detection strategies may help to identify a specific ALL subgroup that may be considered for auto-HSCT, if lacking an allogeneic donor, or are not eligible for allo-HSCT
Chronic Myeloid Leukemia (CML)
Chronic myeloid leukemia (CML) is a rare pathology in childhood and represents 2–3% of all leukemias in children and adolescents.40,41 It occurs more frequently in adolescents than in younger children and, at onset, shows more aggressive clinical features (elevated WBC, significant splenomegaly, advanced phase) than adult CML.40–43 The history of the disease has changed completely with the advent of tyrosine kinase inhibitors (TKIs), a class medication that inhibits the BCR-ABL1 oncoprotein. In adults, the use of these orally administered drugs has significantly improved the expectation and quality of life which is currently comparable to that of the healthy population.44,45 Imatinib was the first TKI used in the treatment of CML. This was followed by second-generation TKIs, such as dasatinib, nilotinib, recently approved as first-line therapy and designed to be active in imatinib-resistant or intolerant patients.40–42,46,47 Successful experiences in adults have also been transferred to children, where TKIs have confirmed their effectiveness. In children, however, the prolonged use of these drugs has led to the appearance of some side effects, such as growth disturbances, which were not evident in adulthood.48–50
In adult patients who showed a prolonged and profound molecular response with TKIs therapy, it was possible to discontinue the treatment. Even in pediatric age, some positive experiences of therapy discontinuation have been reported which are sometimes due to an attempt to reduce therapy-related side effects.51–53
Before the development of TKIs, standard treatment of CML involved CT, particularly hydroxyurea, αIFN and allo-HSCT. In the 1990s, in Europe, auto-HSCT was used in patients with chronic CML phase and preliminary results suggested that, in some patients, it was possible to obtain a cytogenetic response and to prolong survival.54–57 Subsequently, several centres reported their experience of auto-HSCT in CML using in vivo or in vitro manipulation of BM designed to increase the overall response rate.58,59 During the chronic phase, HD-CT was used to mobilize negative BCR-ABL cells; the cryopreserved cells were reinfused into the patient in chronic or accelerated phase, or frank blast crisis. In addition to in vivo purging approaches, in vitro manipulations such as cultures with cytotoxic agents, use of MoAbs directed against the BCR-ABL fusion protein, antisense oligonucleotides directed against the BCR-ABL oncogene, or the Myb gene were performed.58,59 The results, mainly reported in adults, were controversial.
After the advent of TKIs, some adult patients in cytogenetic remission (CCyR), treated with imatinib, have had attempts made at stem cell harvesting. Fifty-eight patients in CCyR received G-CSF during imatinib treatment; 84% of them had a BCR-ABL negative collection.60 These results, reported by the United Kingdom (UK) CML Working Party, were confirmed by the German and Italian CML groups with an identical strategy.61,62 None of these studies included pediatric patients alone.
In the era of TKIs, the role of HSCT, both allogeneic and autologous, has been considerably limited; allo-HSCT is currently reserved for patients, both children and adults, resistant or intolerant to TKIs; auto-HSCT, with collected BCR-ABL negative stem cells, in CCyR patients could represent a further therapeutic option.
Take Home Messages
- The advent of TKIs has dramatically improved the outcome of patients with CML
- The majority of TKI responders can have a BCR-ABL negative stem cell collection
- Auto-HSCT with BCR-ABL negative stem cells, collected in CCyR, may represent a therapeutic option for some pediatric patients showing TKIs toxicity or disease resistance
Non-Hodgkin Lymphoma (NHL)
In pediatric non-Hodgkin lymphoma (NHL), the cure rates range from 75% to more than 90% according to histological subtypes.63,64 With the current protocols, HSCT, either autologous or allogeneic, is reserved for refractory/relapsed cases. The results of the largest study analyzing international strategies on re-induction treatment, and the employment of HSCT in pediatric relapsed/refractory NHL, were recently published.65 Of the 639 evaluable patients, 23% underwent auto-HSCT, 39% allo-HSCT, and 37% were not transplanted. The 8-year OS from relapse was 34% for the entire population, 55% for autotransplanted, 47% for allotransplanted and only 8% for not transplanted patients. The remission status at HSCT was highly associated with the outcome, and no clear advantage for allo- versus auto-HSCT was observed. Significant differences were found in the different histological subtypes, with OS ranging from 57% for primary mediastinal large B-cell NHL (PMBCL) to 28% for Burkitt lymphoma (BL)/B-cell acute leukemia (BAL) and 27% for T-lymphoblastic lymphoma (T-LBL).
Aggressive B-Cell NHL
Children and adolescents with B-cell NHL account for about 60% of pediatric NHL. Currently, short intensive CTs, modulated according to the extent of the disease, associated to anti-CD20 (rituximab) in HR patients, provide an EFS rate of 90%, at 3–4 years.64,66,67 Very few patients experience a relapsed/refractory disease. However, the prognosis of these patients is still poor, with survival rates less than 50% in most reports. The outcome is particularly poor for those children with primary refractory to first-line therapy, or those not responding to salvage schemas.
Auto-HSCT and allo-HSCT are considered the best options for patients responding to salvage therapies. However, in the reported pediatric experiences, the proportion of patients treated with different salvage regimens which could be submitted to an HSCT ranged from 21% to 63%.68–74 Most of the data is limited to retrospective analyses or single/few-centre experiences, mostly including patients with B- and with T-cell NHL submitted to auto- or allo-HSCT with heterogeneous conditioning regimens. The EFS rates ranged from 27% to 59% and the OS from 27% to 58%, at 4–5-year (Table 4). No clear differences between auto or allografted patients were reported and the disease remission at HSCT was the only predictive factor for better survival.68–75 The outcome of BL/BAL patients treated with strategies including HSCT was recently analyzed by Woessmann for the BFM group.76 Seventy-one patients, who relapsed after 2001, were included; the 3-year OS was 25% for 20 autotransplanted patients compared with 58% for 26 allotransplanted patients (p = 0.026). Twenty-five patients were unable to receive an HSCT because of disease progression and all of them died. No conclusions regarding the efficacy of auto-HSCT versus allo-HSCT were drawn by the authors76 (Table 4).
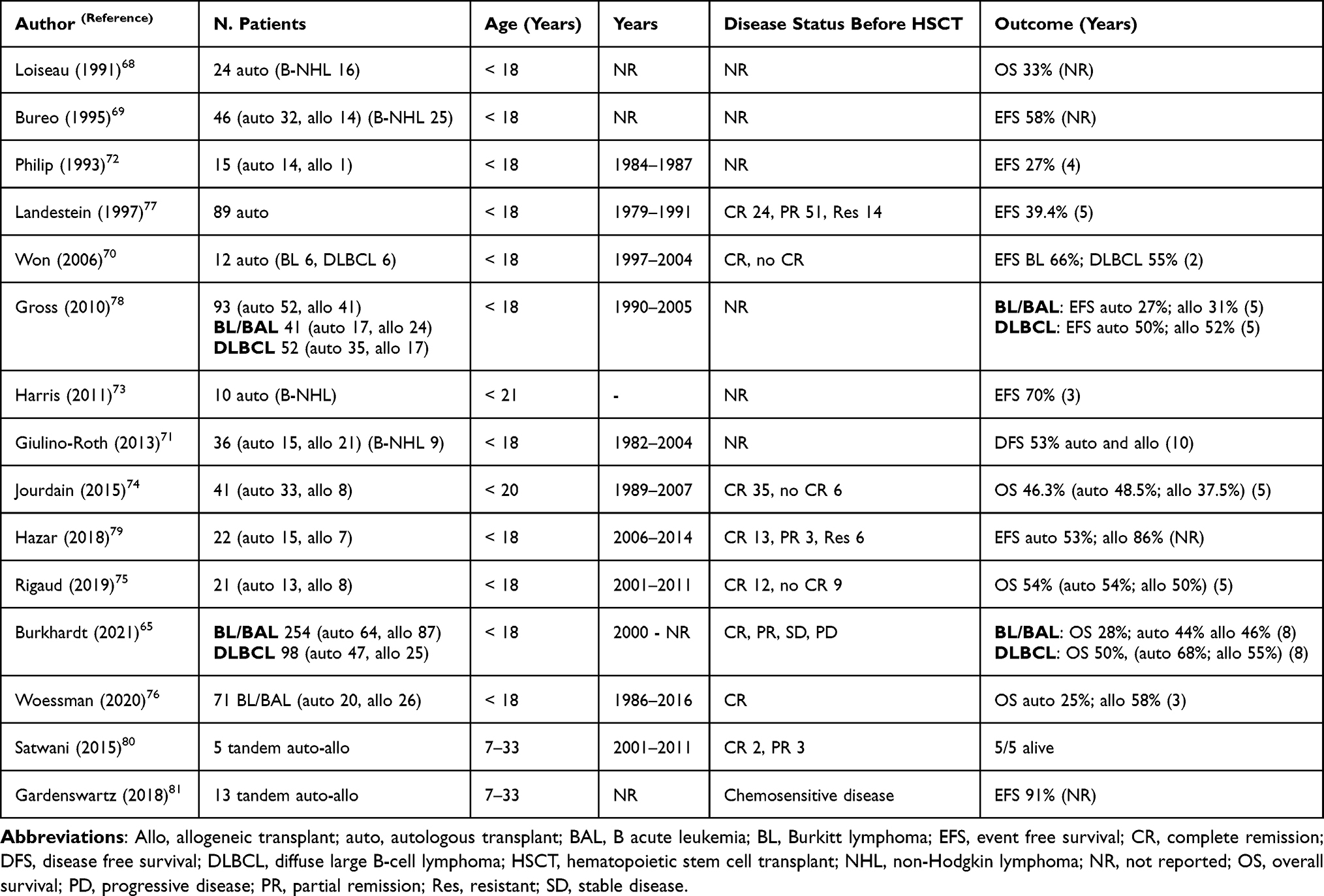 |
Table 4 Results of Autologous Hematopoietic Stem Cell Transplant in Pediatric Relapsed/Refractory Aggressive B-Cell Lymphoma |
Larger series of relapsed/refractory pediatric NHL from HSCT registries have been published.77–79 The European Bone Marrow Transplantation Registry (EBMTR) reported 89 patients who received an auto-HSCT between 1979 and 1991; the 5-year EFS was 39.4% and was significantly associated with the degree of response prior to transplant.77 Gross reported the outcome of pediatric patients with relapsed/refractory NHL transplanted between 1990 and 2005, with data obtained from the Centre for International Blood and Marrow Transplant Research (CIBMTR).78 The 5-year EFS was 27% after auto- and 31% after allo-HSCT for 41 patients with BL, and 50% after auto- and 52% after allo-HSCT for the 52 patients with diffuse large B-cell NHL (DLBCL) (Table 4).
In the recent international study on pediatric relapsed/refractory NHL, the 8-year OS was 28% for the 254 patients with BL/BAL. HD-CT followed by HSCT was planned for all patients; however, 38% of them could not reach HSCT. The survival rate for the 103 BL/BAL patients not transplanted was 3% compared with 44% for the 64 autotransplanted, and 46% for 87 patients submitted to allo-HSCT.65 The 8-year OS was 50% for the 98 relapsed/refractory DLBCL and, in particular, 13%, for 26 not transplanted, 68% for 47 autotransplanted, and 55% for the last 25 patients who received allo-HSCT.65
In order to improve the prognosis in these patients, a multicenter prospective study of myeloablative conditioning (MAC) and auto-HSCT, followed by a reduced intensity conditioning (RIC) and allo-HSCT in children, adolescents, and young adults with poor risk refractory, or recurrent NHL, was designed.80,81 Conditioning for MAC consisted of carmustine/ETP/CY; RIC included BU/fludarabine. Thirty patients, 16 Hodgkin lymphoma (HL) and 14 NHL, with a median age of 16 years and median follow-up of 5 years were enrolled. Twenty-three patients completed both MAC auto-HSCT and RIC allo-HSCT. Allogeneic donor sources included unrelated cord blood (n = 9), unrelated donor (n = 8), and matched siblings (n = 6). The incidence of TRM following RIC allo-HSCT was 12%. In patients with NHL, the 10-year EFS was 70% (Table 4). The approach was safe and encouraging for young patients with poor prognostic characteristics.
Numerous novel therapies are currently being tested in adults with relapsed/refractory B-NHL with promising results, but for several reasons, new agents are difficult to test in the pediatric population. However, in children and adolescents, some selected new agents (new targets, next-generation MoAbs and novel approaches in cellular therapy) are starting to be used. The creation of an international working group to develop clinical trial strategies in refractory/relapsed B-cell NHL is recommended.
Lymphoblastic Lymphoma (LBL)
Lymphoblastic lymphoma (LBL) is the second most common type of NHL in childhood and adolescents, accounting for 25–35% of all cases. The majority (70–80%) is of T-lymphoblastic origin, while 20–25% arise from B-lymphoblasts.82,83 The application of ALL-like treatment regimens, including hyper-CVAD (fractionated CY, VCR, doxorubicin and dexamethasone) and BFM protocols, has led to a significant improvement of the outcome, with OS rates exceeding 80% of pediatric T-cell LBL.82,83 The role of HSCT consolidation remains unclear, especially in the modern ALL-like regimens setting. However, the cure rates for patients with relapsed/refractory disease remain dismal with survival rates of 10–30%.83,84 According to the limited data available in literature, only patients receiving HD-treatment followed by auto- or allo-HSCT, have a chance of cure. In a Japanese cohort of patients with relapsed/refractory LBL, 19 underwent allo-HSCT. At 3 years, ten survived in CR, six relapsed, and three died of TRM. Six patients received auto-HSCT: four relapsed and two survived85 (Table 5).
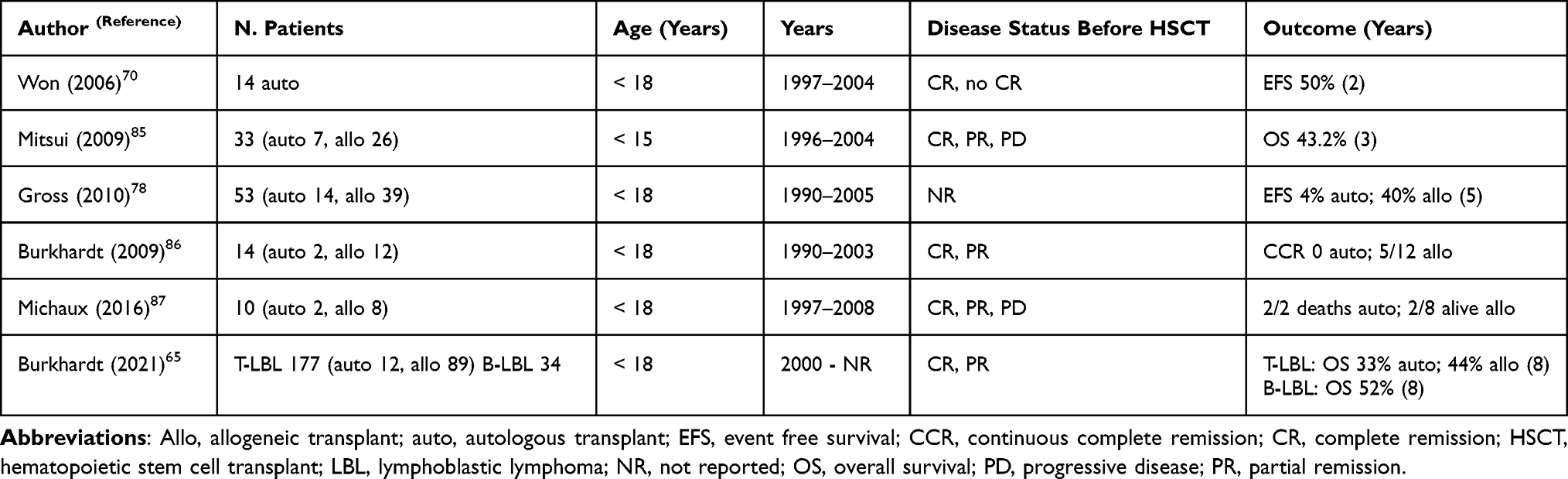 |
Table 5 Results of Autologous Hematopoietic Stem Cell Transplant in Pediatric Relapsed/Refractory Lymphoblastic Lymphoma |
The role of HSCT was analyzed by the CIBMTR of North America: 53 pediatric LBL received allo-HSCT (39 children) or auto-HSCT (14 children) between 1990 and 2005.78 The 5-year EFS for 39 allotransplanted patients was 40% compared with 4% in the 14 autotransplanted patients. In Korea, 14 children with relapsed/refractory LBL received consolidation auto-HSCT and the 2-year EFS was 50%.70
The NHL-BFM group reported 12/34 patients with relapsed LBL who received allo-HSCT. Five survived, six died after relapse, and two of TRM. Two other patients underwent auto-HSCT and both died due to disease progression.86 Similar results were reported by Michaux with 5/12 patients alive after allo-HSCT and neither of the two autotransplanted patients (Table 5).87
Recent results published by the International Study of relapsed/refractory pediatric NHL show an 8-year OS of 27%, for the 177 T-cell LBL. A high proportion of patients (43%) could not receive any HSCT, due to disease progression before transplant procedure. The 8-year OS for not-transplanted patients was significantly lower compared to the 12 patients treated with auto-HSCT (OS 6% and 33%; respectively) (Table 5).65
Concerning the discussion on whether allo- or auto-HSCT is superior, there is a trend for higher TRM, but also a higher probability of DFS after allo-HSCT compared to auto-HSCT. Auto-HSCT does not seem to have a major role in the treatment of relapsed/refractory LBL. However, the total number of cases in literature is too small to draw definitive conclusions.
Anaplastic Large Cell Lymphoma (ALCL)
Anaplastic large cell lymphoma (ALCL) accounts for about 15% of pediatric NHL. Currently, with different intensive multiagent CT regimens, EFS rates, vary between 65% and 75%, and OS rates between 70% and 90%, at 3–8 years.88–91 A second disease response is obtained in most relapsed patients. Consolidation strategies based on auto- or allo-HSCT have been analyzed in some retrospective studies. The French Group reported the outcome of 41 ALCL relapse. DFS was 45% for 15 ALCL patients who received HSCT (14 auto-HSCT, 1 allo-HSCT) in CR2.92 An initial Japanese study on 26 relapsed ALCL patients reported better results in those patients in CR2 consolidated with allo-HSCT (6 cases), compared to auto-HSCT (8 cases).93 A second study, also from Japan, described the outcome of 47 ALCL relapsed patients receiving HSCT: 23 auto-HSCT, 24 allo-HSCT. The 5-year EFS was 38% and 50%, respectively, for auto- and allo-HSCT.94 The analysis of 36 relapsed/refractory ALCL patients from CIBMTR showed a 5-year RFS of 35% for 24 patients who were consolidated with auto-HSCT, compared to 46% 5-year EFS for 12 allotransplanted patients.78 The BFM group reported a large retrospective cohort of 74 children with first relapse of ALCL after front-line BFM-NHL therapy. CT followed by auto-HSCT was planned for all patients; the 5-year EFS and OS for the 39 children who were autotransplanted were 59% and 77%, respectively (Table 6). The results were strongly influenced by the time to relapse and the CD3 positivity.95
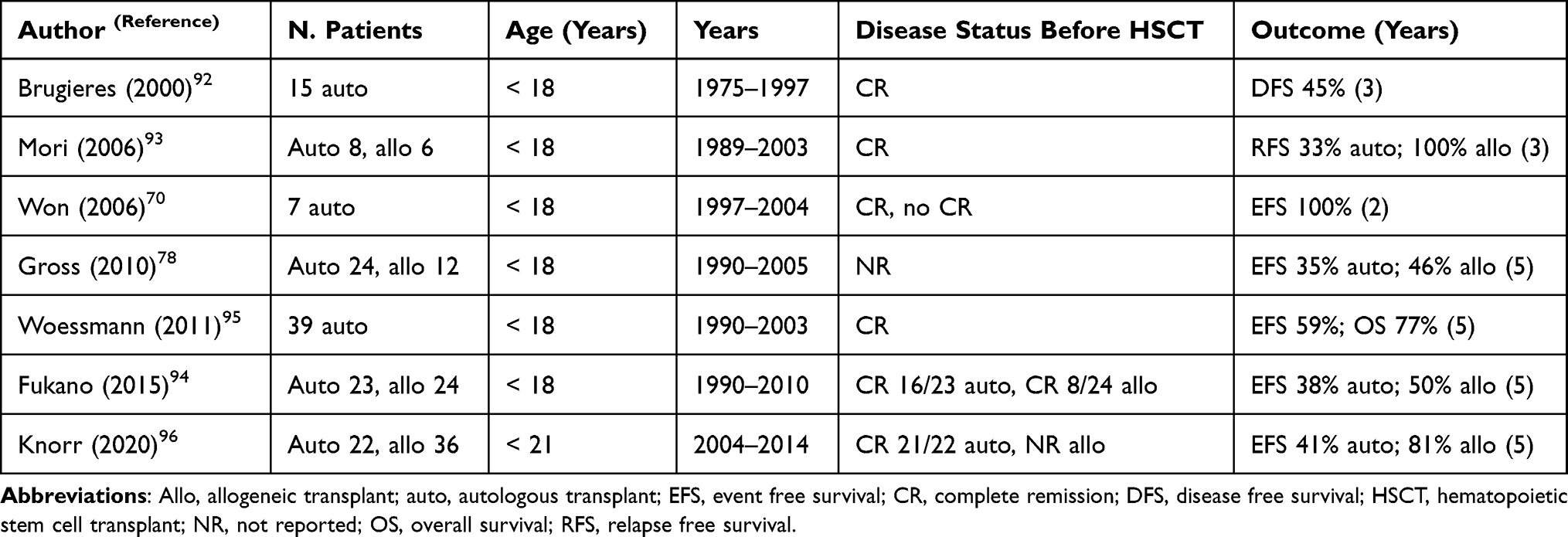 |
Table 6 Results of Autologous Hematopoietic Stem Cell Transplant in Pediatric Relapsed/Refractory Anaplastic Large Cell Lymphoma |
The role of auto- and allo-HSCT in relapsed/refractory ALCL was more recently analyzed in the International prospective ALCL-relapse trial (NCT00317408) for children and adolescents with relapsed ALCL.96 The trial was based on different strategies for 4 risk groups, defined as VHR, HR, intermediate and low risk, according to time to relapse, CD3 expression, and prior vinblastine treatment. Low-risk patients received vinblastine alone; all the other risk groups were treated with CT followed by allo-HSCT for those at VHR and HR, and auto-HSCT for the intermediate risk group, or HR patients without an available donor. Allo-HSCT, performed in 36 patients, confirmed its efficacy as consolidation therapy for HR relapsed ALCL, the 5-year OS and EFS were 83% and 81%, respectively. Auto-HSCT was performed in 22 patients. The 5-year OS and EFS rates were 82% and 41% (Table 6).
The high rate of events in patients scheduled for auto-HSCT led to the abandonment of this procedure in 2012, and the authors concluded that auto-HSCT is not indicated as consolidation therapy for children with relapsed/refractory ALCL.
Nonanaplastic Peripheral T-Cell Lymphomas (PTCL)
Nonanaplastic peripheral T-cell lymphomas (PTCLs) are very rare in children and adolescents comprising 0.9% of NHL.97 The literature available on PTCL in children and adolescents shows that survival rates with conventional CT and HSCT are still poor compared to other NHL subentities, but also that treatment results vary among different PTCL subgroups. Five-year EFS and OS were 45% and 56%, respectively, for the 143 patients of the BFM study.98 Outcomes varied among the histopathological subgroups, suggesting that a subtype-specific treatment approach might be indicated. However, solid basic therapy principles based on prospective randomized trials are completely lacking in children and adolescents, so treatment recommendations are merely based on adult experience and retrospective pediatric series. There is no standardized treatment for pediatric PTCL-Not-otherwise-specified-(NOS) that receive block-like mature B-cell NHL- or ALCL-type therapy ± maintenance, or T-cell ALL treatment. No difference in EFS and OS among the different groups of treatments has been found (5-year OS 56%–75%; EFS 47%–55%, respectively).98 While consolidation therapy with auto- or allo-HSCT in CR1 is recommended in adults, its role in children and adolescents with PTCL is still a matter of debate. Few experiences reported small numbers of children transplanted in CR1, or CR2, or with disease progression; most of them received allo-HSCT and the OS rate was almost 50%. While the indication for allo-HSCT in CR1 seems to be clear, auto-HSCT does not seem to have a role in CR1 and CR2.
Take Home Messages
- Currently, excellent results are achieved in children and adolescents with B-cell NHL combining CT and rituximab
- International trials have reported better results in pediatric patients with relapsed/refractory B-cell NHL consolidated with both auto- or allo-HSCT compared to non-transplanted patients
- The remission status at HSCT has been highly associated with the outcome and no clear advantage of allo- versus auto-HSCT was observed
- A new approach with myeloablative conditioning and auto-HSCT, followed by a reduced intensity conditioning and allo-HSCT, in relapsed/refractory children and adolescents with very poor prognostic characteristics has demonstrated to be safe, with encouraging results in this poor category of patients
- Auto-HSCT does not seem to have a major role in the treatment of relapsed/refractory LBL and ALCL.
Hodgkin Lymphoma (HL)
The prognosis of children and adolescents with Hodgkin Lymphoma (HL) has progressively improved, reaching an OS of more than 90%, at 5–10 years. In children and adolescents, the first-line strategies have changed over the past decades with the aim of reducing the serious late effects and maintaining their high efficacy. Use of radiotherapy (RT) was progressively reduced in terms of doses and irradiation fields and is reserved for patients with an inadequate early or late response assessment by metabolic imaging (fluorodeoxyglucose positron emission computed tomography-FDG-PET scans). However, despite the improvements in outcomes, up to 15% of patients present relapse or refractory disease. Cure may be achieved also in these settings, but in children and adolescents, there is still no defined salvage treatment, and randomized trials comparing standard-dose CT (SD-CT) to HD-CT and auto-HSCT are lacking. However, HD-CT followed by auto-HSCT, which represents the standard of care for adults with relapsed/refractory disease, is largely employed also in pediatric age.99–102 Two adult randomized studies compared SD-CT with HD-CT in patients with HL first relapse.101,103 The British National Lymphoma Investigation (BNLI) trial randomized HD-BEAM (carmustine, ETP, CA, MEL) and auto-HSCT or mini-BEAM and CT in 40 adult patients not responding to conventional CT. The German Hodgkin’s Lymphoma Study Group (GHSG) and the Lymphoma Working Party of the European Society for Blood and Marrow Transplantation (EBMT)-HDR1 trial compared BEAM and auto-HSCT with Dexamethasone-BEAM in 117 adults with CT-sensitive relapse. Both studies showed superior progression-free survival (PFS) for salvage regimen including auto-HSCT versus CT.101,103,104
In pediatric relapsed/refractory HL, in the absence of randomized studies to evaluate the role of auto-HSCT, data on the outcome and potential prognostic factors can be inferred from the literature in one prospective and some retrospective studies.
Older series have included both children and adults (Table 7). The impact of auto-HSCT was evaluated in 81 pediatric patients (<16 years at diagnosis) and 81 adults (16–50 years). There was no significant difference in the outcome between the two groups in terms of PFS (39% vs 48%; p = 0.64, at a median follow-up of 37 months) and relapse rate (52% vs 40%; p = 0.65).105 Several other studies reported retrospective series of pediatric patients; the 5-year EFS were 45–65% and the 5-year OS 55%-74%.106–112 The prospective multicenter German-Austrian pediatric nonrandomized salvage therapy (ST-HD-86 trial) reported a 10-year OS of 51% in 53 children treated with auto-HSCT out of 176 relapsed/refractory HL.113 A more recent review of the CIBMTR reported a lower 10-year PFS of 41% in auto-transplanted pediatric and young adults HL owing to late relapses and late toxicity.114 The Memorial Sloan Kettering Cancer Center (MSKCC) retrospectively analyzed 36 consecutive pediatric patients with relapsed or refractory HL, auto-transplanted between 1989 and 2013.115 All patients underwent a disease evaluation before auto-HSCT. The majority of them were transplanted in CR (61%) or partial response (14%). The 10-year OS was 74.1% and EFS 67.1%. Univariate analysis showed that sensitive disease at HSCT (EFS and OS: HR 0.18, p = 0.0039 and 0.22, p = 0.0219, respectively) and the absence of B symptoms (EFS and OS: HR 0.12, p = 0.0015 and 0.18, p = 0.0170, respectively) were associated with improved outcome. In this paper, patients were divided between those who underwent auto-HSCT before 1997, and those transplanted from 1998; this last cohort of patients had a superior outcome for both EFS and OS (85.8% and 91.7%, respectively, compared to 48.8% and 59.1%) (Table 7). Other retrospective series of children and adolescents with HL have reported potential factors associated with a poor outcome. All concluded that prognostic factors for risk of further relapse were chemo-refractory disease, both primary or after salvage treatment, and short remission duration.110,116,117 Other poor prognostic factors emerged from various studies, such as extra-nodal disease, mediastinal bulk, B symptoms, anemia, elevated erythrocyte sedimentation rate, elevated lactate dehydrogenase at relapse.110,113,116–119 The Childhood Hodgkin Lymphoma International Prognostic score (CHIPS), developed by COG to stratify patients in risk categories at diagnosis, was also predictive for children at relapse, with a better OS for patients with a lower R-CHIPS.115 The stratification of pediatric patients with refractory/relapsed HL will help to select the patients that may benefit of SD-CT plus RT, or are candidate to auto-HSCT, or need alternative therapies. In fact, in the past years, in children with relapsed HL, some studies showed that non-transplant salvage therapy with SD-CT plus RT is effective for a good risk subset of patients that do not require HD-CT and auto-HSCT. The prospective pediatric ST-HD-86 relapse trial reported 10-year DFS of 86% with SD-CT and RT in patients with late relapse (>12 months).113 These results were confirmed by other studies, such as the UK HD3 trial, and the United States (US) St. Jude study, that reported 5-year 74% DFS and 10-year 80% DFS in late relapse, and 5-year 100% DFS in children responding to first salvage CT (Table 7).118,120 A survival benefit with HD-CT followed by auto-HSCT was instead observed in children with primary refractory and multiple relapsed disease.109,121 In order to standardized recommendations for salvage therapy in children with relapsed/refractory HL, a risk stratification at the time of relapse, was published by the European (EuroNet) Pediatric Hodgkin Lymphoma Group.104 Patients were divided into 3 risk-groups, based on time to relapse, prior first-line CT treatment, and disease stage at relapse: low-risk (late relapse), HR (primary resistant) and intermediate-risk (all the others). HD-CT and auto-HSCT should be reserved for the intermediate-group still PDG/PET positive after the first 2 courses of salvage CT, or to low-risk and intermediate-risk patients achieving a complete metabolic response only after 4 courses of SD-CT. For HR children, the best salvage treatment remains undefined, and could include HD-CT and auto- or allo-HSCT, or new drugs.
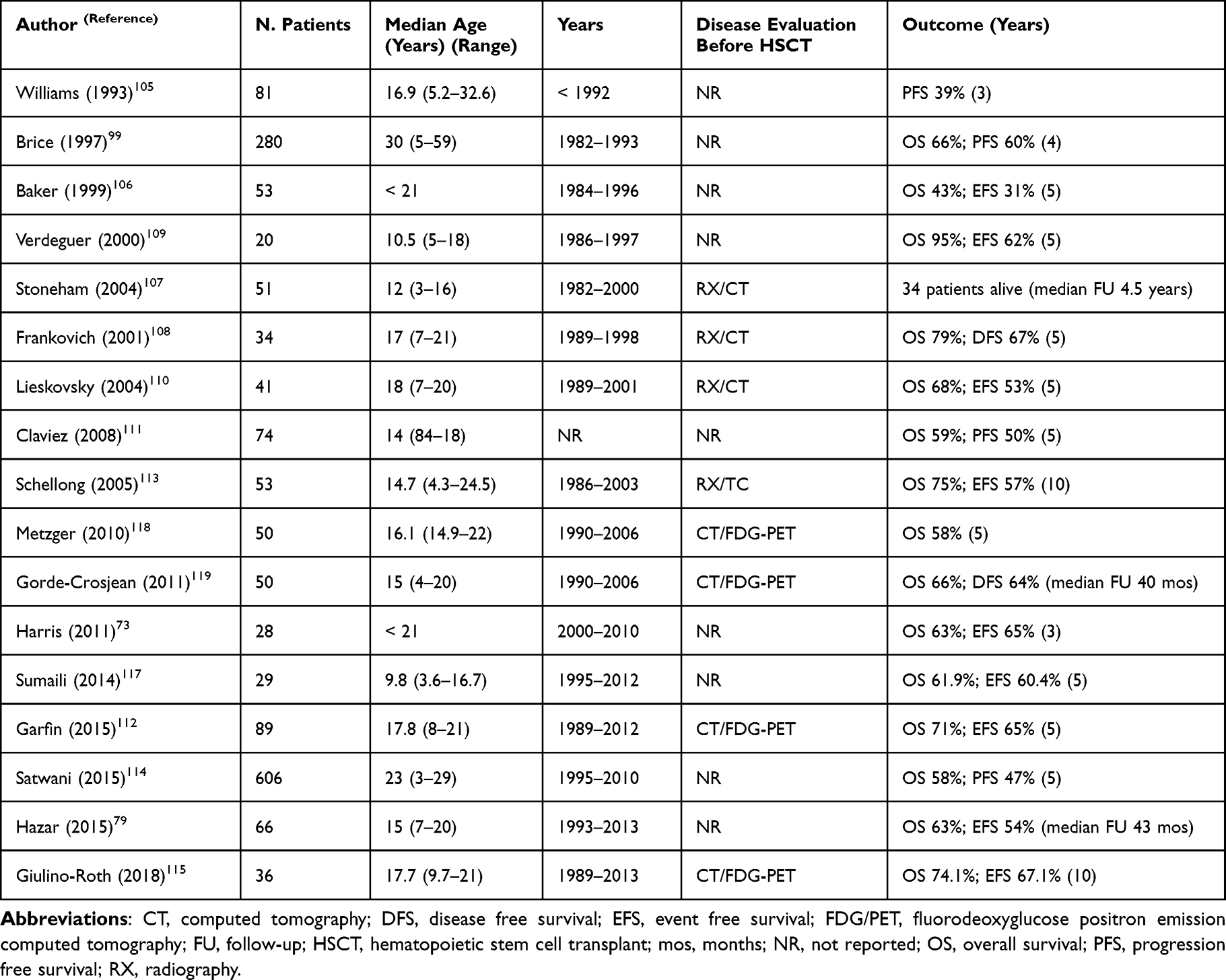 |
Table 7 Results of Autologous Hematopoietic Stem Cell Transplant in Pediatric Relapsed/Refractory Hodgkin Lymphoma |
Recently, the efficacy of new target immune therapies, like brentuximab vedotin (BV) and checkpoint inhibitors, has been demonstrated both for adults and children with relapsed/refractory HL.122,123 BV has been approved, not only as first-part of salvage treatment, but also as consolidation after auto-HSCT, with the role of reducing the further disease progression.122–125 Checkpoint inhibitors, such as pembrolizumab, are currently under evaluation as maintenance therapy after auto-HSCT, in children and adolescents with HL (NCT02362997).
All these new agents, along with auto-HSCT will soon be part of the strategies for pediatric refractory/relapsed HL, adapted according to the correct evaluation of the childhood risk category.
Take Home Messages
- HD-CT followed by auto-HSCT is the standard of care of adults with relapsed/refractory HL. Optimal salvage strategy has still to be defined in pediatric age
- The European Pediatric Hodgkin Lymphoma Group has recently published recommendations for salvage therapy in children and adolescents, dividing patients into risk-groups according to time of relapse, prior therapy, and disease stage at time of relapse. Auto-HSCT should be reserved for those children at intermediate-risk still PDG/PET positive after two courses of salvage CT, or those at low or intermediate-risk, with a complete metabolic response only after 4 courses
- Recent target therapies are currently in evaluation as maintenance therapy after auto-HSCT, with the role of reducing the further disease progression
Comments
Since the first patient received auto-HSCT, 60 years ago, progress in this procedure has been remarkable. Mobilized peripheral blood cells have replaced bone marrow as stem cell source, the pre-HSCT conditioning regimens have been adapted to the different pathologies, and the support therapy has considerably improved, thus allowing the use of this procedure, not only in oncological diseases, but also in autoimmune conditions. Moreover, the improvements of MRD detection strategies in acute leukemias, and of methods for disease response evaluation in lymphomas, have helped to identify better selected categories of patients that could benefit from auto-HSCT. However, with the recent identification of extremely effective and less toxic target therapies in the pediatric age, the use of auto-HSCT in first- and second-line therapies is limited. This is essentially due to the need to reduce the long-term side effects in a growing population, which, even if minor compared to allogeneic transplantation, are to be attributed to conditioning therapies. Replacing toxic therapies with precisely targeted therapies promises to improve not only the cure rate but also the quality of life of patients.
Abbreviations
4-HC, 4-hydroperoxycyclophosphamide; αIFN, alpha interferon; AIEOP, associazione italiana Ematologia Oncologia Pediatrica; ALCL, Anaplastic large cell lymphoma; ALL, acute lymphoblastic leukemia; Allo-HSCT, allogeneic hematopoietic stem cell transplant; ALWP, Acute Leukemia Working Party; AML, acute myeloid leukemia; APL, acute promyelocytic leukemia; ATO, arsenic trioxide; ATRA, all-trans retinoic acid; Auto-HSCT, autologous hematopoietic stem cell transplant; BAL, B-cell acute leukemia; BCR-ABL1, breakpoint cluster region-Abelson 1; BL, Burkitt Lymphoma; BM, bone marrow; BU, Busulfan; CA, cytarabine; CCyR, cytogenetic complete remission; CI, Cumulative Incidence; CIBMTR, Center for International Blood and Marrow Transplant Research; CML, Chronic myeloid leukemia; CNS, central nervous system; COG, Childrens’ Oncology Group; CR, complete remission; CR2, second-complete remission; CsA, cyclosporine A; CT, Chemotherapy; CT scan, computed tomography; CY, Cyclophosphamide; DFS, disease-free survival; DLBCL, diffuse large B-cell NHL; DP, disease progression; EBMT, European Blood Bone Marrow Transplantation; EBMTR, European Bone Marrow Transplantation Registry; EFS, event-free survival; ETP, Etoposide; G-CSF, granulocyte-colony stimulating factor; GHSG, German Hodgkin’s Lymphoma Study Group; GO, gemtuzumab ozogamicin; GVL, graft-versus-leukemia; HD, high dose; HL, Hodgkin Lymphoma; I-BFM-SG, International Berlin-Frankfurt-Munster Study Group; JSHCT, Japan Society for Hematopoietic Cell Transplantation; LBL, Lymphoblastic lymphoma; MAC, myeloablative conditioning; MEL, Melphalan; MFC, multiparametric flow cytometry; MoAbs, monoclonal antibodies; MRD, minimal residual disease; MSKCC, Memorial Sloan Kettering Cancer Center; NHL, non-Hodgkin lymphoma; NRM, Non-relapse Mortality; OS, overall survival; PBSC, peripheral blood stem cells; PFS, progression-free survival; PMBCL, primary mediastinal large B-cell NHL; PML-RARA, Promyelocytic Leukemia-Retinoic acid receptor; PR, partial remissione; PRC, polymerase-chain reaction; PTCL, Nonanaplastic peripheral T-cell lymphomas; RIC, reduced intensity conditioning; SD, stable disease; SD-CT, standard-dose chemotherapy; TBI, total body irradiation; TKIs, tyrosine kinase inhibitors; T-LBL, T-lymphoblastic lymphoma; TRM, transplant-related mortality; VCR, Vincristine; VHR, very-high risk.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation; took part in drafting and in critically reviewing the article. All authors gave final approval of the version to be published. The authors have agreed on the journal to which the article has been submitted and agree to be accountable for all aspects of the work. Our main text and Tables have been edited and revised by a native English teacher.
Funding
No financial support was received for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Elgarten CW, Aplenc R. Pediatric acute myeloid leukemia: updates on biology, risk stratification, and therapy. Curr Opin Pediatr. 2020;32(1):57–66. doi:10.1097/MOP.0000000000000855
2. Conneely SE, Stevens AM. Acute myeloid leukemia in children: emerging paradigms in genetics and new approaches to therapy. Curr Oncol Rep. 2021;23:16. doi:10.1007/s11912-020-01009-3
3. Wang J, Ouyang J, Zhou R, Chen B, Yang Y. Autologous hematopoietic stem cell transplantation for acute myeloid leukemia in first complete remission: a meta-analysis of randomized trials. Acta Haematol. 2010;124:61–71. doi:10.1159/000314273
4. Nathan PC, Sung L, Crump M, Beyene J. Consolidation therapy with autologous bone marrow transplantation in adults with acute myeloid leukemia: a meta-analysis. J Natl Cancer Inst. 2004;96:38–45. doi:10.1093/jnci/djh003
5. Levi I, Grotto I, Yerushalmi R, Ben-Bassat I, Shpilberg O. Meta-analysis of autologous bone marrow transplantation versus chemotherapy in adult patients with acute myeloid leukemia in first remission. Leuk Res. 2004;28:605–612. doi:10.1016/j.leukres.2003.10.029
6. Bleakley M, Lau L, Shaw PJ, Kaufman A. Bone marrow transplantation for paediatric AML in first remission: a systematic review and meta-analysis. Bone Marrow Transplant. 2002;29:843–852. doi:10.1038/sj.bmt.1703528
7. Amadori S, Testi AM, Aricò M, et al. Prospective comparative study of bone marrow transplantation and postremission chemotherapy for childhood acute myelogenous leukemia. J Clin Oncol. 1995;11(6):1046–1054. doi:10.1200/JCO.1993.11.6.1046
8. Woods WG, Neudorf S, Gold S, et al. A comparison of allogeneic bone marrow transplantation, autologous bone marrow transplantation, and aggressive chemotherapy in children with acute myeloid leukemia in remission: a report from Children’s Cancer Group. Blood. 2001;97(1):56–62. doi:10.1182/blood.v97.1.56
9. Ravindranath Y, Yeager AM, Chang MN, et al. Autologous bone marrow transplantation versus intensive consolidation chemotherapy for acute myeloid leukemia in childhood. Pediatric Oncology Group. N Engl J Med. 1996;334:1428–1434. doi:10.1056/NEJM199605303342203
10. Shaw PJ, Bergin ME, Burgess MA, et al. Childhood acute myeloid leukemia: outcome in a single center using chemotherapy and consolidation with busulfan/cyclophosphamide for bone marrow transplantation. J Clin Oncol. 1994;12(10):2138–2145. doi:10.1200/JCO.1994.12.10.2138
11. Stevens RF, Hann IM, Wheatley K, Gray RG. Marked improvements in outcome with chemotherapy alone in pediatric acute myeloid leukemia: results of the United Kingdom Medical Research Council’s 10th AML trial. Br J Haematol. 1998;101:130–140. doi:10.1046/j.1365-2141.1998.00677.x
12. Creutzig U, van den Heuvel-Eibrink MM, Gibson B, et al. Diagnosis and management of acute myeloid leukemia in children and adolescents: recommendations from an international expert panel. Blood. 2012;120:3187–3205. doi:10.1182/blood-2012-03-362608
13. Pession A, Masetti R, Rizzari C, et al. Results of the AIEOP AML 2002/01 multicenter prospective trial for the treatment of children with acute myeloid leukemia. Blood. 2013;122(2):170–178. doi:10.1182/blood-2013-03-491621
14. Sakaguchi H, Muramatsu H, Hasegawa D, et al. Comparison of conditioning regimens for autologous stem cell transplantation in children with acute myeloid leukemia: a nationwide retrospective study in Japan. Pediatr Blood Cancer. 2019;66:e27459. doi:10.1002/pbc.27459
15. Alonzo TA, Wells RJ, Woods WG, et al. Postremission therapy for children with acute myeloid leukemia: the Children’s Cancer Group experience in the transplant era. Leukemia. 2005;19:965–970. doi:10.1038/sj.leu.2403763
16. Zittoun RA, Mandelli F, Willemze R, et al. Autologous or allogeneic bone marrow transplantation compared with intensive chemotherapy in acute myelogenous leukemia. European Organization for Research and Treatment of Cancer (EORTC) and the Gruppo Italiano Malattie Ematologiche Maligne dell’Adulto (GIMEMA) Leukemia Cooperative Groups. N Engl J Med. 1995;332:217–223. doi:10.1056/NEJM199501263320403
17. Pession A, Rondelli R, Basso G, et al. Treatment and long-term results in children with acute myeloid leukaemia treated according to the AIEOP AML protocols. Leukemia. 2005;19:2043–2053. doi:10.1038/sj.leu.2403869
18. Oliansky DM, Rizzo JD, Aplan PD, et al. The role of cytotoxic therapy with hematopoietic stem cell transplantation in the therapy of acute myeloid leukemia in children: an evidence-based review. Biol Blood Marrow Transplant. 2007;13:1–25. doi:10.1016/j.bbmt.2006.10.024
19. Sanz MA, Grimwade D, Tallman MS, et al. Management of acute promyelocytic leukemia: recommendation from an expert panel on behalf of the European Leukemia Net. Blood. 2009;113(9):1875–1891. doi:10.1182/blood-2008-04-150250
20. Sanz J, Montesinos P, Sanz AM. Role of hematopoietic stem cell transplant in acute promyelocytic leukemia. Front Oncol. 2021;11:614215e.
21. Sanz J, Labopin M, Sanz MA, et al. Hematopoietic stem cell transplantation for adults with relapsed acute promyelocytic leukemia in second complete remission. Bone Marrow Transplant. 2021;56(6):1272–1280. doi:10.1038/s41409-020-01162-0
22. Chakrabarty JLH, Rubinger M, Le Rademacher J, et al. Autologous is superior to allogeneic hematopoietic cell transplantation for acute promyelocytic leukemia in second complete remission. Biol Blood Marrow Transplant. 2014;20(7):
23. Abla O, Kutney MA, Testi AM, et al. Management of relapsed and refractory childhood acute promyelocytic leukemia: recommendation from an international expert panel. Br J Haematol. 2016;175:588–601. doi:10.1111/bjh.14313
24. Termulhen AM, Klopfenstein K, Olshefski R, et al. Mobilization of PML-RARA negative blood stem cell transplantation in children with relapsed acute promyelocytic leukemia. Pediatr Blood Cancer. 2008;51:521–524. doi:10.1002/pbc.21514
25. Dvorak CC, Agaewal MA, Dahl GV, Gregory JJ, Feusner JH. Hematopoietic stem cell transplant for pediatric acute promyelocytic leukemia. Biol Blood Marrow Transplant. 2008;14:824–830. doi:10.1016/j.bbmt.2008.04.015
26. Yamamoto S, Tomizawa D, Kudo K, et al. Hematopoietic stem cell transplantation for pediatric acute promyelocytic leukemia in Japan. Pediatr Blood Cancer. 2020;67(5):e28181. doi:10.1002/pbc.28181
27. Testi AM, Mohamed S, Diverio D, et al. Outcome of relapsed/refractory acute promyelocytic leukemia in children, adolescents and young adult patients – a 25-year Italian experience. Br J Haematol. 2021;195(2):278–283. doi:10.1111/bjh.17637
28. Scheinemann K, Weitzman S, Hitzler J, Doyle J, Abla O. Isolated central nervous system relapse in childhood acute promyelocytic leukemia. J Pediatr Hematol Oncol. 2008;30(2):160–162. doi:10.1097/MPH.0b013c318159a582
29. Billet AL, Kornmehl E, Tabell NJ, et al. Autologous bone marrow transplantation after a long first remission for children with recurrent acute lymphoblastic leukemia. Blood. 1993;81(6):1651–1657.
30. Billet AL, Sallan SE. Autologous bone marrow transplantation in childhood acute lymphoid leukemia with use of purging. Am J Pediatr Hematol Oncol. 1993;15(2):162–168.
31. Maldonado MS, Diaz-Heredia C, Badell J, et al. Autologous bone marrow transplantation with monoclonal antibody purged marrow for children with acute lymphoblastic leukemia in second remission. Bone Marrow Transplant. 1998;22:1043–1047. doi:10.1038/sj.bmt.1701507
32. Messina C, Cesaro S, Rondelli R, et al. Autologous bone marrow transplantation for childhood acute lymphoblastic leukemia in Italy. Bone Marrow Transplant. 1998;21:1015–1021.
33. Borgmann A, Schmid H, Hartmann R, et al. Autologous bone-marrow transplants compared with chemotherapy for children with acute lymphoblastic leukaemia in a second remission: a matched-pair analysis. Lancet. 1995;346:873–876. doi:10.1016/s0140-6736(95)92710-7
34. Balduzzi A, Gaipa G, Bonanomi S, et al. Purified autologous grafting in childhood acute lymphoblastic leukemia in second remission: evidence for long-term clinical and molecular remissions. Leukemia. 2001;15:50–56. doi:10.1038/sj.leu.2402004
35. Balduzzi A, Galimberti S, Valsecchi MG, et al. Autologous purified peripheral blood stem cell transplantation compare to chemotherapy in childhood acute lymphoblastic leukemia after low-risk relapse. Pediatr Blood Cancer. 2011;57:654–659. doi:10.1002/pbc.23169
36. Houtenbos I, Bracho F, Davenport V, et al. Autologous bone marrow transplantation for childhood acute lymphoblastic leukemia: a novel combined approach consisting of ex vivo marrow purging, modulation of multi-drug resistance, induction of autograft vs leukemia effect, and post-transplant immune- and chemotherapy (PTIC). Bone Marrow Transplant. 2001;27:145–153. doi:10.1038/sj.bmt.1702750
37. Ribera JM, Ortega JJ, Oriol A, et al. Comparison of intensive chemotherapy, allogeneic, or autologous stem-cell transplantation as postremission treatment for children with very high risk acute lymphoblastic leukemia: PETHEMA ALL-93 Trial. J Clin Oncol. 2007;25(1):16–24. doi:10.1200/JCO.2006.06.8312
38. Hong CR, Kang HJ, Park KD, Shin HY, Ahn HS. High-dose chemotherapy and autologous peripheral blood stem cell transplantation with BCVAC regimen followed by maintenance chemotherapy for children with very high risk acute lymphoblastic leukemia. J Hematol. 2018;107:355–362. doi:10.1007/s12185-017-2355-5
39. Capria V, Pepe S, Trisolini SM, et al. Autologous stem cell transplant in acute lymphoblastic leukemia: prognostic impact of pre-transplant minimal residual disease. Leuk Lymphoma. 2019;60(1):274–276. doi:10.1080/10428194.2018.1468895
40. Smith SM, Hijiya N, Sakamoto KM. Chronic Myelogenous Leukemia in childhood. Curr Oncol Rep. 2021;23:40. doi:10.1007/s11912-021-01025-x
41. Howlader N, Noone AM, Krapcho M, et al. SEER cancer statistics review. 1975–2017. National Cancer Institute Bethesda, MD, based on November 2019 SEER data submission, posted to the SEER web site, April 2020. Available from: https://seercancergrov/197529017/.
42. Hijiya N, Suttorp M. How I treat chronic myeloid leukemia in children and adolescents. Blood. 2019;133(22):2374–2384. doi:10.1182/blood.2018882233
43. Athale U, Hijiya N, Patterson BC, et al. Management of chronic myeloid leukemia (CML) in children and adolescents: recommendations from the Children’s Oncology Group CML Working Group. Pediatr Blood Cancer. 2019;66(9):e27827. doi:10.1002/pbc.27827
44. Bower H, Biorkholm M, Dickman PW, Hoglund M, Lambert PC, Andersson TM-L. Life expectancy of patients with chronic myeloid leukemia approaches the life expectancy of the general population. J Clin Oncol. 2016;34(24):2851–2857. doi:10.1200/JCO.2015.66.2866
45. Sasaki K, Strom SS, O’Brien S, et al. Relative survival in patients with chronic-phase chronic myeloid leukemia in tyrosine-kinase inhibitor era: analysis of patient data from six prospective clinical trials. Lancet Haematol. 2015;2(5):c186–c193. doi:10.1016/S2352-3026(15)00048-4
46. Gore L, Kearns PR, de Martino ML, et al. Dasatinib in pediatric patients with chronic myeloid leukemia in chronic phase: results from a Phase II trial. J Clin Oncol. 2018;36(13):1330–1338. doi:10.1200/JCO.2017.75.9597
47. Hijiya N, Maschan A, Rizzari C, et al. Efficacy and safety of nilotinib in pediatric patients with Philadelphia chromosome-positive (PH+) chronic myeloid leukemia (CML): results from a Phase 2 trial (abstract). Pediatr Blood Cancer. 2017;64(S3):Abstract S22.
48. Shima H, Tokuyama M, Tanizawa A, et al. Distinct impact of imatinib on growth at pre-pubertal and pubertal age of children with chronic myeloid leukemia. J Pediatr. 2011;159(4):676–681. doi:10.1016/j.jpeds.2011.03.046
49. Bansal D, Shava U, Verma N, Trehan A, Marwaha RK. Imatinib has adverse effect on growth in children with chronic myeloid leukemia. Pediatr Blood Cancer. 2012;59(3):481–484. doi:10.1002/pbc.23389
50. Samis J, Lee P, Zimmerman D, Arceci RJ, Suttorp M, Hijiya N. Recognizing endo-crinopathies associated with tyrosine kinase inhibitor therapy in children with chronic myelogenous leukemia. Pediatr Blood Cancer. 2016;63(8):1332–1338. doi:10.1002/pbc.26028
51. Shima H, Kada A, Tanizawa A, et al. Discontinuation of tyrosine kinase inhibitor in children with chronic myeloid leukemia (JPLSG STKI-14 Study). Blood. 2019;134(Supplement1):25. doi:10.1182/blood.2019-122623
52. Millot F, Claviez A, Leverger G, Corbaciglu S, Groll AH, Suttorp M. Imatinib cessation in children and adolescents with chronic myeloid leukemia in chronic phase: imatinib cessation in children with CML. Pediatr Blood Cancer. 2014;61(2):355–357. doi:10.1002/pbc.24521
53. Giona F, Malaspina F, Putti MC, et al. Results and outcome of intermittent imatinib (ON/OFF schedule) in children and adolescents with chronic myeloid leukemia. Br J Haematol. 2020;188(6):e101–e105. doi:10.1111/bjh.16388
54. Meloni G, De Fabritiis P, Alimena G, et al. Autologous bone marrow transplantation or peripheral blood stem cell transplantation for patients with chronic myelogenous leukemia in chronic phase. Bone Marrow Transplant. 1880;4:92–94.
55. Hoyle C, Gray R, Gpòdman J. Autografting for patients with CML in chronic phase: an update. Br J Haematol. 1994;86:76–81. doi:10.1111/j.1365-2141.1994.tb03255.x
56. Pigneux A, Faberes C, Boiron JM, et al. Autologous stem cell transplantation in chronic myeloid leukemia: a single center experience. Bone Marrow Transplant. 1999;24:265–270. doi:10.1038/sj.bmt.1701871
57. Olavarria E, Reiffers J, Boque C, et al. The post-transplant cytogenetic response to interferon is a major determinant of survival after autologous stem cell transplantation for chronic myeloid leukemia in chronic phase. Br J Haematol. 2002;118:762–770. doi:10.1046/j.1365-2141.2002.03600.x
58. Olavarria E. Autologous stem cell transplantation in chronic myeloid leukemia. Semin Hematol. 2007;44(4):252–258. doi:10.1053/j.seminhematol.2007.08.003
59. Bhatia R, McGlave PB. Autologous hematopoietic cell transplantation for chronic myelogenous leukemia. Hematol Oncol Clin North Am. 2004;18:715–732. doi:10.1016/j.hoc.2004.03.006
60. Drummond MW, Marin D, Clark RE, Byrne JL, Holyoake TL, Lennard A; United Kingdom Chronic Myeloid Leukemia (UK CML) Working Party. Mobilization of Ph chromosome-negative peripheral blood stem cells in chronic myeloid leukemia patients with imatinib mesylate-induced complete cytogenetic remission. Br J Haematol. 2003;123:479–483. doi:10.1046/j.1365-2141.2003.04599.x
61. Kreuzer KA, Kluhs C, Baskaynak G, Novassaghi K, Dorken B, le Coutre P. Filgrastim-induced stem cell mobilization in chronic myeloid leukemia patients during imatinib therapy: safety, feasibility and evidence for an efficient in vivo purging. Br J Haematol. 2004;124:195–199. doi:10.1046/j.1365-2141.2003.04756.x
62. Perseghin P, Gambacorti-Passerini C, Tornaghi C, et al. Peripheral blood progenitor cell collection in chronic myeloid leukemia patients with complete cytogenetic response after treatment with imatinib mesylate. Transfusion. 2005;45:1214–1229. doi:10.1111/j.1537-2995.2005.00175.x
63. Cairo MS, Beishuizen A. Childhood, adolescents and young adults with non-Hodgkin lymphoma: current perspectives. Br J Haematol. 2019;185(6):1021–1042. doi:10.1111/bjh.15764
64. Egan G, Goldman S, Alexander S. Mature B-NHL in children, adolescents and young adults: current therapeutic approach and emerging treatment strategies. Br J Hematol. 2019;185:1071–1085. doi:10.1111/bjh.15734
65. Burkhardt B, Taj M, Garnier N, et al. Treatment and outcome analysis of 639 relapsed non-Hodgkin lymphomas in children and adolescents and resulting treatment recommendations. Cancers. 2021;13(9):2075. doi:10.3390/cancers13092075
66. Goldman S, Smith L, Anderson JR, et al. Rituximab and FAB/LMB 96 chemotherapy in children with stage III/IV B-cell non-Hodgkin lymphoma: a Children’s Oncology Group Report. Leukemia. 2013;27:1174–1177. doi:10.1038/leu.2012.255
67. Goldman S, Smith L, Galardy P, et al. Rituximab with chemotherapy in children and adolescents with central nervous system and/or bone marrow-positive Burkitt lymphoma/leukaemia: a Children’s Oncology report. Br J Haematol. 2014;167:394–401. doi:10.1111/bjh.13040
68. Loiseau HA, Hartmann O, Valteau D, et al. High-dose chemotherapy containing busulfan followed by bone marrow transplantation in 24 children with refractory or relapsed non-Hodgkin’s lymphoma. Bone Marrow Transplant. 1991;8(6):465–472.
69. Bureo E, Ortega JJ, Munoz A, et al. Bone marrow transplantation in 46 pediatric patients with non-Hodgkin lymphoma. Spanish Working Party for Bone Marrow transplantation in children. Bone Marrow Transplant. 1995;15:353–359.
70. Won SC, Han JW, Known SY, et al. Autologous peripheral blood stem cell transplantation in children with non-Hodgkin’s lymphoma: a report from Korean society of pediatric hematology-oncology. Ann Hematol. 2006;85:787–794. doi:10.1007/s00277-006-0169-2
71. Giulino-Roth L, Ricafort L, Keman NA, et al. Ten-year follow up of pediatric patients with non-Hodgkin lymphoma treated with allogeneic or autologous stem cell transplantation. Pediatr Blood Cancer. 2013;60(12):2018–2024. doi:10.1002/pbc.24722
72. Philip T, Bergeron C, Frappaz D. Management of paediatric lymphoma. Baillieres Clin Haematol. 1996;9(4):769–797. doi:10.1016/s0950-3536(96)80053-9
73. Harris RE, Termuhlen AM, Smith ML, et al. Autologous peripheral blood stem cell transplantation in children with relapsed or refractory lymphoma: results of Children’s Oncology Group Study A5962. Biol Blood Marrow Transplant. 2011;17(2):249–258. doi:10.1016/j.bbmt.2010.07.002
74. Jourdan A, Auperin A, Minard-Colin V, et al. Outcome and prognostic factors for relapse in children and adolescents with mature B-cell lymphoma and leukemia treated in three consecutive prospective “Lymphomes Malins B” protocols. A Societè Francaise des Cancers de l’Enfant Study. Haematologica. 2015;100(6):810–817. doi:10.3324/haematol.2014.121434
75. Rigaud C, Auperin A, Jourdain A, et al. Outcome of relapse in children and adolescents with B-cell non-Hodgkin lymphoma and mature acute leukemia: a report from the French LMB study. Pediatr Blood Cancer. 2019;66(9):e27873. doi:10.1002/pbc.27873
76. Woessmann W, Zimmermann M, Meinhardt A, et al. Progressive or relapsed Burkitt lymphoma or leukemia in children and adolescents after BFM-type first-line therapy. Blood. 2020;135(14):1124–1132. doi:10.1182/blood.2019003591
77. Ladenstein R, Pearce R, Hartmann O, Patte C, Goldstone T, Philip T. High-dose chemotherapy with autologous bone marrow rescue in children with poor-risk Burkitt’s lymphoma: a report from the European Lymphoma Bone Marrow Transplantation registry. Blood. 1997;90:2921–2930.
78. Gross TG, Hale GA, He W, et al. Hematopoietic stem cell transplantation for refractory or recurrent non-Hodgkin lymphoma in children and adolescents. Biol Blood Marrow Transplant. 2010;16:223–230. doi:10.1016/j.bbmt.2009.09.021
79. Hazar V, Kesik V, Karasu GT, et al. Risk factors predicting the survival of pediatric patients with relapsed/refractory non-Hodgkin lymphoma who underwent hematopoietic stem cell transplantation: a retrospective study from the Turkish pediatric bone marrow transplantation registry. Leuk Lymphoma. 2018;59(1):85–96. doi:10.1080/10428194.2017.1330472
80. Satwani P, Jin Z, Martin PL, et al. Sequential myeloablative autologous stem cell transplantation and reduced intensity allogeneic hematopoietic cell transplantation is safe and feasible in children, adolescents and young adults with poor-risk refractory or recurrent Hodgkin and non-Hodgkin lymphoma. Leukemia. 2015;29:448–455. doi:10.1038/leu.2014.194
81. Gardenswartz A, Mehta B, El-Mallawany N, et al. Safety and efficacy of myeloablative conditioning autologous stem cell transplantation, target immunotherapy, and reduced intensity conditioning allogeneic stem cell transplantation in children, adolescents, and young adults with relapsed/refractory mature B-cell non Hodgkin lymphoma. Br J Haematol. 2018;182(Suppl. 1):
82. Landmann E, Burkhardt B, Zimmermann M, et al. Results and conclusion of the European Intergroup EURO-LB02 trial in children and adolescents with lymphoblastic lymphoma. Haematologica. 2017;102:2086–2096. doi:10.3324/haematol.2015.139162
83. Burkhardt B, Hemiston ML. Lymphoblastic lymphoma in children and adolescents: review of current challenges and future opportunities. Br J Haematol. 2019;185(6):1158–1170. doi:10.1111/bjh.15793
84. Schmidt E, Burkhardt B. Lymphoblastic lymphoma in childhood and adolescents. Pediatr Hematol Oncol. 2013;30:484–508. doi:10.3109/08880018.2013.789574
85. Mitsui T, Mori T, Fujita N, Inada H, Horibe K, Tsurusawa M. Lymphoma Committee, Japanese Pediatric Leukemia/Lymphoma Study Group. Retrospective analysis of relapsed or primary refractory childhood lymphoblastic lymphoma in Japan. Pediatr Blood Cancer. 2009;52:591–595. doi:10.1002/pbc.21941
86. Burkhardt B, Reiter A, Landmann E, et al. Poor outcome of children and adolescents with progressive disease or relapse of lymphoblastic lymphoma: a report from Berlin-Frankfurt- Muenster Group. J Clin Oncol. 2009;27:3363–3369. doi:10.1200/JCO.2008.19.3367
87. Michaux K, Bergeron C, Gandemer V, Mechinaud F, Uyttebroeck A, Bertrand Y; SFCE: the EORTC Children Leukemia Group. Relapsed or refractory lymphoblastic lymphoma in children: results and analysis of 23 patients in the EOTC 58951 and the LMT96 protocols. Pediatr Blood Cancer. 2016;63:1214–1221. doi:10.1002/pbc.25990
88. Brugieres L, Deley MC, Pacquement H, et al. CD30 (+) anaplastic large-cell lymphoma in children: analysis of 82 patients enrolled in two consecutive studies of the French Society of Pediatric Oncology. Blood. 1998;92:3591–3598.
89. Seidemann K, Tiemann M, Schrappe M, et al. Short-pulse B-non-Hodgkin lymphoma-type chemotherapy is efficacious treatment for pediatric anaplastic large cell lymphoma: a report of the Berlin-Frankfurt- Munster Group Trial NHL-BFM 90. Blood. 2001;97:3699–3706. doi:10.1182/blood.v97.12.3699
90. Rosolen A, Pillon M, Garaventa A, et al. Anaplastic large cell lymphoma treated with a leukemia-like therapy: a report from the Italian Association of Pediatric Hematology and Oncology (AIEOP) LNH-92 protocol. Cancer. 2005;104:2133–2140. doi:10.1002/cncr.21438
91. Lowe EJ, Sposto R, Perkins SL, et al. Intensive chemotherapy for systemic anaplastic large cell lymphoma in children and adolescents: final results of Children’s Cancer Group Study 5941. Pediatr Blood Cancer. 2009;52:335–339. doi:10.1002/pbc.21817
92. Brugieres L, Quartier P, Le Deley MC, et al. Relapses of childhood anaplastic large-cell lymphoma: treatment results in a series of 41 children – a report from French Society of Pediatric Oncology. Ann Oncol. 2000;11:53–58. doi:10.1023/a:
93. Mori T, Takimoto T, Katano N, et al. Recurrent childhood anaplastic large cell lymphoma: a retrospective analysis of registered cases in Japan. Br J Haematol. 2006;132:594–597. doi:10.1111/j.1365-2141.2005.05910.x
94. Fukano R, Mori T, Kobayashi R, et al. Hematopoietic stem cell transplantation for relapsed or refractory anaplastic large cell lymphoma: a study of children and adolescents in Japan. Br J Haematol. 2015;168(4):557–563. doi:10.1111/bjh.13167
95. Woessmann W, Zimmermann M, Lenhard M, et al. Relapsed or refractory anaplastic large-cell lymphoma in children and adolescents after Berlin-Frankfurt-Muenster (BFM)-type first-line therapy: a BFM-group study. J Clin Oncol. 2011;29(22):3065–3071. doi:10.1200/JCO.2011.34.8417
96. Knorr F, Brugieres L, Pillon M, et al. European Intergroup for Childhood Non-Hodgkin Lymphoma. Stem cell transplant and vinblastine monotherapy for relapsed pediatric anaplastic large cell lymphoma: results of the International, prospective ALCL-relapse trial. J Clin Oncol. 2020;38(34):3999–4009. doi:10.1200/JCO.20.00157
97. Attarbaschi A, Abla O, Padilla LA, et al. Rare non-Hodgkin lymphoma of childhood and adolescents: a consensus diagnostic and therapeutic approach to pediatric-type follicular lymphoma, marginal zone lymphoma and nonanaplastic peripheral T-cell lymphoma. Pediatr Blood Cancer. 2020;67(8):e28416. doi:10.1002/pbc.28416
98. Mellgren K, Attarbashi A, Abla O, et al. Non-anaplastic peripheral T cell lymphoma in children and adolescents – an international review of 143 cases. Ann Hematol. 2016;9588:1295–1305. doi:10.1007/s00277-016-2722-y
99. Brice P, Bouabdallah R, Moreau P, et al. Prognostic factors for survival after high-dose therapy and autologous stem cell transplantation for patients with relapsing Hodgkin’s disease: analysis of 280 patients from the French registry. Bone Marrow Transplant. 1997;20:21–26. doi:10.1038/sj.bmt.1700838
100. Czyz J, Dziadziuszko R, Knopinska-Postuszuy W, et al. Outcomes and prognostic factors in advanced Hodgkin’s disease treated with high-dose chemotherapy and autologous stem cell transplantation: a study of 341 patients. Ann Oncol. 2004;15(8):1222–1230. doi:10.1093/annonc/mdh304
101. Schmitz N, Pfistner B, Sextro M, et al. Aggressive conventional chemotherapy compared with high-dose chemotherapy with autologous haemopoietic stem-cell transplantation for relapsed chemosensitive Hodgkin’s disease: a randomised trial. Lancet. 2002;359(9323):2065–2071. doi:10.1016/S0140-6736(02)08938-9
102. Wadehra N, Farag S, Bolwell B, et al. Long-term outcome of Hodgkin disease patients following high-dose busulfan, etoposide, cyclophosphamide, and autologous stem cell transplantation. Biol Blood Marrow Transplant. 2006;12(12):1343–1349. doi:10.1016/j.bbmt.2006.08.039
103. Linch DC, Goldstone AH, McMillan A, et al. Dose intensification with autologous bone-marrow transplantation in relapsed and resistant Hodgkin’s disease: results of a BNLI randomised trial. Lancet. 1993;341(8852):1051–1054. doi:10.1016/0140-6736(93)92411-l
104. Daw S, Hasenclever D, Mascarin M, et al. Risk and response adapted treatment guidelines for managing first relapsed and refractory classical Hodgkin lymphoma in children and young people. Recommendations from the EuroNet Pediatric Hodgkin Lymphoma Group. HemaSphere. 2020;4(1):e329. doi:10.1097/HS9.0000000000000329
105. Williams CD, Goldstone AH, Pearce R, et al. Autologous bone marrow transplantation for pediatric Hodgkin’s disease: a case-matched comparison with adult patients by the European Bone Marrow Transplant Group Lymphoma Registry. J Clin Oncol. 1993;11(11):2243–2249. doi:10.1200/JCO.1993.11.11.2243
106. Baker KS, Gordon BG, Gross TG, et al. Autologous hematopoietic stem-cell transplantation for relapsed or refractory Hodgkin disease in children and adolescents. J Clin Oncol. 1999;17:825–831. doi:10.1200/JCO.1999.17.3.825
107. Stoneham S, Ashley S, Pinkerton CR, Wallace WH, Shankar AG; United Kingdom Children’s Cancer Study Group. Outcome after autologous hemopoietic stem cell transplantation in relapsed or refractory childhood Hodgkin disease. J Pediatr Hematol Oncol. 2004;26:740–745. doi:10.1097/00043426-200411000-00010
108. Frankovich J, Donaldson SS, Lee Y, Wong RM, Amylon M, Verneris MR. High-dose therapy and autologous hematopoietic cell transplantation in children with primary refractory and relapsed Hodgkin’s disease: atopy predicts idiopathic diffuse lung injury syndromes. Biol Blood Marrow Transplant. 2001;7:49–57. doi:10.1053/bbmt.2001.v7.pm11215699
109. Verdeguer A, Pardo N, Madero L, et al. Autologous stem cell transplantation for advanced Hodgkin’s disease in children. Spanish group for BMT in children (GETMON), Spain. Bone Marrow Transplant. 2000;25:31–34. doi:10.1038/sj.bmt.1702094
110. Lieskovsky YE, Donaldson SS, Torres MA, et al. High-dose therapy and autologous hematopoietic stem-cell transplantation for recurrent or refractory pediatric Hodgkin’s disease: results and prognostic indices. J Clin Oncol. 2004;22:4532–4540. doi:10.1200/JCO.2004.02.121
111. Claviez A, Sureda A, Schmitz N. Haematopoietic SCT for children and adolescents with relapsed and refractory Hodgkin’s lymphoma. Bone Marrow Transplant. 2008;42(Suppl 2):S16–S24. doi:10.1038/bmt.2008.278
112. Garfin PM, Link MP, Donaldson SS, et al. Improved outcomes after autologous bone marrow transplantation for children with relapsed or refractory Hodgkin lymphoma. Biol Blood Bone Marrow Transplant. 2015;21:326–334. doi:10.1016/j.bbmt.2014.10.020
113. Schellong G, Dorffel W, Claviez A, et al. Salvage therapy of progressive and recurrent Hodgkin’s disease: results from a multicenter study of the pediatric DAL/GPOH-HD Study Group. J Clin Ocol. 2005;23(25):6181–6189. doi:10.1200/JCO.2005.07.930
114. Satwani P, Ahn KW, Carreras J, et al. A prognostic model predicting autologous transplantation outcomes in children, adolescents and young adults with Hodgkin lymphoma. Bone Marrow Transplant. 2015;50:1416–1423. doi:10.1038/bmt.2015.177
115. Giulino-Roth L, O’Donohue T, Chen Z, et al. Outcome of children and adolescents with relapsed Hodgkin lymphoma treated with high dose therapy and autologous stem cell transplantation: the Memorial Sloan Kettering Cancer Center experience. Leuk Lymphoma. 2018;59(8):1861–1870. doi:10.1080/10428194.2017.1403601
116. Shafer JA, Heslop HE, Brenner MK, et al. Outcome of hematopoietic stem cell transplant as salvage therapy for Hodgkin’s lymphoma in adolescents and young adults at a single institution. Leuk Lymphoma. 2010;51:664–670. doi:10.3109/10428190903580410
117. Sumaili H, Al-Kofide A, Al-Seraihi A, et al. Outcome of pediatric patients with lymphoma following stem cell transplant: a single institution report. Leuk Lymphoma. 2015;56(5):1327–1334. doi:10.3109/10428194.2014.951846
118. Metzger ML, Hudson MM, Krasin MJ, et al. Initial response to salvage therapy determines prognosis in relapsed pediatric Hodgkin lymphoma patients. Cancer. 2010;116:4376–4384. doi:10.1002/cncr.25225
119. Gorde-Grosjean S, Oberlin O, Leblanc T, et al. Outcome of children and adolescents with recurrent/refractory classical Hodgkin lymphoma, a study from the Societe Francaise de Lutte centre le Cancer des Enfants et des Adolescents (SFCE). Br J Haematol. 2012;158:649–656. doi:10.1111/j.1365-2141.2012.09199.x
120. Shankar A, Hayward J, Kirkwood A, et al. Treatment outcome in children and adolescents with relapsed Hodgkin lymphoma – results of the UK HD3 relapse treatment strategy. Br J Haematol. 2014;165:534–544. doi:10.1111/bjh.12768
121. Belgaumi A, Al-Kofide AA, Jamil-Malik R, Joseph N, Khafaga Y, Sabbah R. Outcome of second line therapy for pediatric patients with Hodgkin lymphoma who relapse following ABVD based therapy. Blood. 2009;114(22):
122. Talleur AC, Flerlage JE, Shook DR, et al. Autologous hematopoietic cell transplantation for the treatment of relapsed/refractory pediatric, adolescent, and young adult Hodgkin lymphoma: a single institutional experience. Bone Marrow Transplant. 2020;55(7):1357–1366. doi:10.1038/s41409-020-0879-4
123. Locatelli F, Mauz-Koerholz C, Neville K, et al. Brentuximab vedotin for paediatric relapsed or refractory Hodgkin’s lymphoma and anaplastic large-cell lymphoma: a multicenter, open-label, phase ½ study. Lancet Haematol. 2018;5(10):e450–e461. doi:10.1016/S2352-3026(18)30153-4
124. Hagenbeek A, Mooij H, Zijlstra J, et al. Phase I dose-escalation study of brentuximab-vedotin combined with dexamethasone, high-dose cytarabine and cisplatin, as salvage treatment in relapsed/refractory classical Hodgkin lymphoma: the HOVON/LLPC transplant brave study. Haematologica. 2019;104(4):e151–e153. doi:10.3324/haematol.2018.196899
125. Moskowitz CH, Nademanee A, Masszi T, et al. Brentuximab vedotin as consolidation therapy after autologous stem-cell transplantation in patients with Hodgkin’s lymphoma at risk of relapse or progression (AETHERA): a randomized, double-blind, placebo-controlled, Phase 3 trial. Lancet. 2015;385(9980):1853–1862. doi:10.1016/S0140-6736(15)60165-9
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.