")
Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 14
Patterns and Clinico-Radiological Characteristics of Primary Liver Masses in Children Treated at a Tertiary Referral Hospital, in Ethiopia
Authors Ayllo M , Tamire AH, Legas MB, Arega G
Received 1 September 2023
Accepted for publication 28 November 2023
Published 4 December 2023 Volume 2023:14 Pages 455—464
DOI https://doi.org/10.2147/PHMT.S433460
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Roosy Aulakh
Melese Ayllo,1 Abebe Habtamu Tamire,2 Mohammed Bereinto Legas,3 Gashaw Arega2
1Department of Pediatrics and Child Health, University of Gondar, Gondar, Ethiopia; 2Department of Pediatrics and Child Health, Addis Ababa University, Addis Ababa, Ethiopia; 3Department of Maternity and Reproductive Health, Tikur Anbessa Hospital, Addis Ababa, Ethiopia
Correspondence: Gashaw Arega, Email [email protected]
Background: Liver masses are a cause of morbidity and mortality in children worldwide. Although the patterns and clinical-radiological characteristics of primary liver masses have been studied in developed countries, few studies have been conducted in developing countries. Studying the patterns of liver mass in children helps to improve the outcome of liver masses and to design preventive strategies if the identified risk factors are preventable.
Material and Method: A hospital-based cross-sectional study was conducted on children who met the inclusion criteria, using a self-administered structured questionnaire. The collected data were analyzed using the Statistical Package for Social Sciences (SPSS) version 25. Statistical significance was set at P < 0.05. Descriptive and logistic regression analyses were used to assess the determinant factors.
Results: A total of 74 children were included, with most patients being males (60.8%). More than one-third (n = 27) of the participants were between 1 and 4 years of age and the mean age at diagnosis of the liver mass was 4.6 years. The duration of illness at presentation to Tikur Anbessa Specialized Hospital was between 4 and 8 weeks, in 42% of the patients. The most common presenting symptom was abdominal swelling, accounting for 70.3% (n = 52) of the patients. Benign hepatic mass lesions accounted for 57.5% (n = 42), and 43.2% (n = 32) were malignant liver masses. Most lesions were solitary and involved the right lobe of the liver. The common benign hepatic masses were pyogenic liver abscesses (38.1%), and the most common malignant hepatic masses were hepatoblastomas (78.1%).
Conclusion: Pyogenic liver abscess was the most common benign hepatic mass and hepatoblastoma was the most common malignant hepatic mass in our study. Most lesions were solitary and involved the right lobe. Understanding the patterns of liver masses will help in the early diagnosis and improve treatment outcomes in children with liver masses.
Keywords: liver mass, liver abscess, hepatoblastoma, TASH, Ethiopia
Introduction
A wide variety of liver masses can be observed in the pediatric population and are one of the causes of morbidity and mortality in children and adolescents. Pediatric liver lesions are a heterogeneous group including infiltrative lesions that cause mass effects. Hepatic lesions can be congenital, infectious, or neoplastic.1–4
The liver accounts for 5–6% of all intra-abdominal masses in children, and one-third of the masses are benign, whereas the two-thirds are malignant.5,6 Among these malignant causes, hepatoblastomas are the most common, followed by hepatocellular carcinoma and other rare tumors, such as soft tissue sarcoma and extragonadal germ cell tumors.7 The benign liver masses usually present during infancy and include hemangiomas, hamartomas, and hemangioendotheliomas2,7 The patterns of the different types of infectious hepatic lesions vary from place to place and are related to the prevalence of hepatitis B virus (HBV) and human immunodeficiency virus (HIV).4
Hepatic lesions present a relatively common clinical dilemma, particularly with the increasing use of various imaging modalities for the diagnosis of abdominal and other vague symptoms.8 Accurate and reliable determination of the nature of the hepatic lesion is important, not only to reassure individuals with benign masses but also to ensure that malignant lesions are diagnosed accurately with noninvasive modalities like abdominal ultrasound.8–11 Abdominal CT and MRI also help better delineate the characteristics and nature of liver masses.12–14 In developing countries in Africa, where access to medical care and sophisticated imaging technologies is limited, deep-seated hepatic tumors often grow to an enormous size before they are diagnosed and treated. Little is known about the epidemiology and outcomes of liver tumor management in children in Ethiopia.4,15 Appropriate diagnosis of hepatic masses allows the appropriate selection of optimal management, which is frequently reassured or followed up for benign hepatic lesions. For malignant liver masses or those at risk of malignant transformation, treatment depends on tissue biopsy, tumor staging, functional status of the free liver, and availability of medical and surgical management options.8,16,17
Patients and Methods
Study Area
This study was conducted at the Tikur Anbessa Specialized Hospital, School of Medicine, College of Health Sciences, Addis Ababa University, which is the largest referral hospital in Ethiopia. It was established in 1964 and is now the main teaching center for both clinical and preclinical training in most disciplines. It is also an institution in which specialized clinical services that are not available in other public or private institutions are rendered nationwide. It is a tertiary hospital where pediatric liver masses are treated by a gastroenterologist and a hemato-oncologist.
Study Design and Methodology
A retrospective cross-sectional study was conducted in children aged ≤ equal to 14 years, who had been treated for primary liver mass at Tikur Anbessa specialized hospital from June 2017 to May 2022, using a structured questionnaire that included sociodemographic characteristics and clinical, laboratory, and radiological imaging of children diagnosed with primary liver masses.
Data Collection and Analysis
Data were collected by the principal investigator using structured questionnaires. Data were analyzed using the Statistical Package for Social Sciences (SPSS) version 25. Statistical significance was set at P < 0.05.
Results
Sociodemographic Characteristics of the Study Participants
Among the study patients, 45/74 (60.8%) were male, with a male-to-female ratio of 1.6:1. The mean age of the patients at presentation was 4.6 years. The majority of the cases; 27/72 (36.5%) were between 1 and 4 years and 18 (24.3%) were infants. Sixty percent (n = 44) of the study participants were from outside Addis Ababa. Almost all of the study cases, 73/74 (98.6%), did not have a sibling or parents who had a similar illness, two (2.7%) had HIV cases and one (1.4%) had a previous history of Hepatitis B (HBV) infection. The demographic characteristics of the children are presented in Table 1.
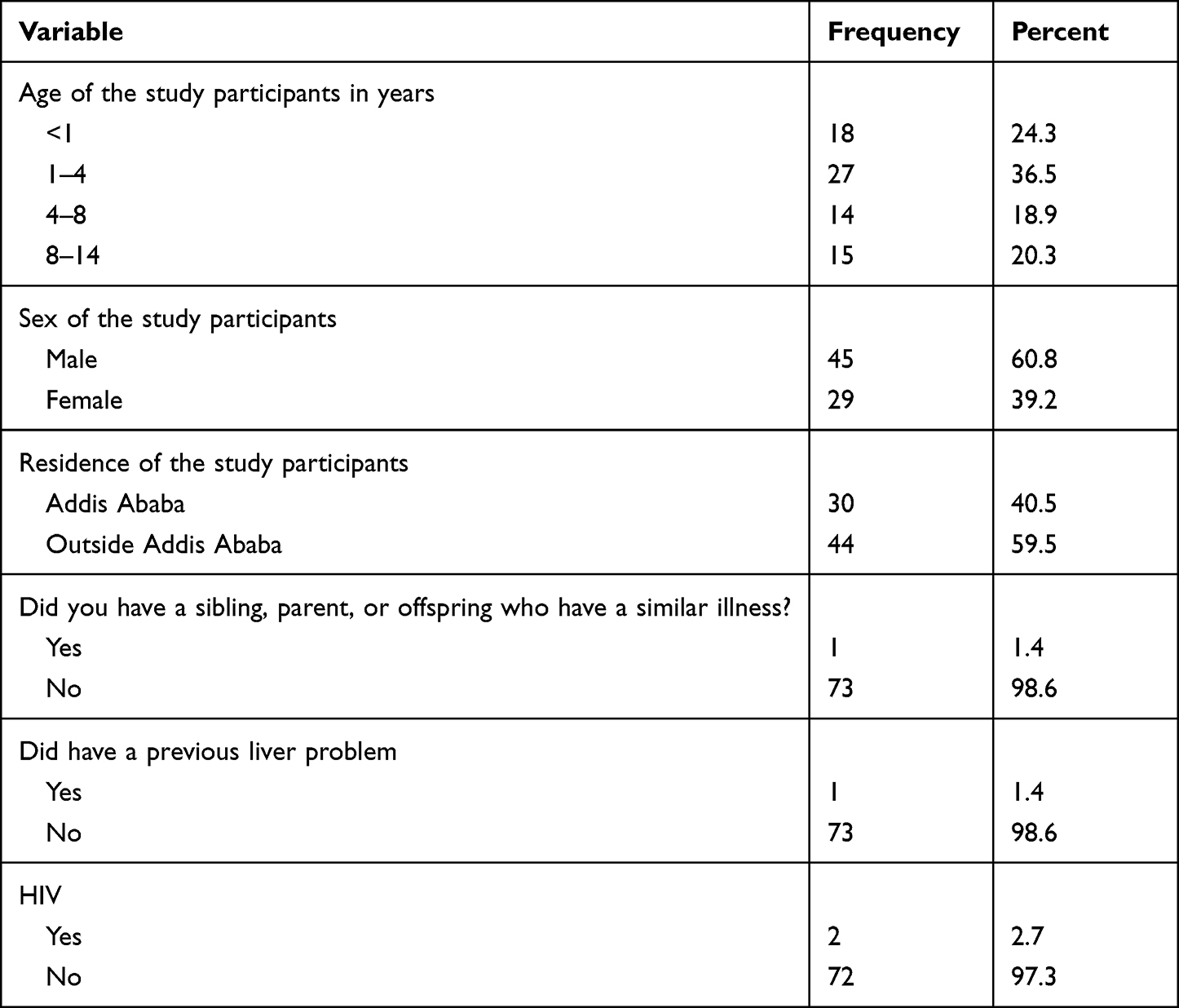 |
Table 1 Demographic Characteristics of Children with Primary Liver Mass Attending at Tertiary Care Center, Addis Ababa, Ethiopia |
Clinical Presentation of the Study Participants with Primary Liver Mass
Seventy cases (94.6%) had presenting symptoms, and the remaining four (5.4%) were incidental findings. Approximately 42% (n = 31) of the study participants had an illness duration of 4–8 weeks. Abdominal swelling (70.3%) was the common presenting symptom in 52/74 (70.3%) of children, followed by abdominal pain, in 29/74 (39.2%) (Table 2).
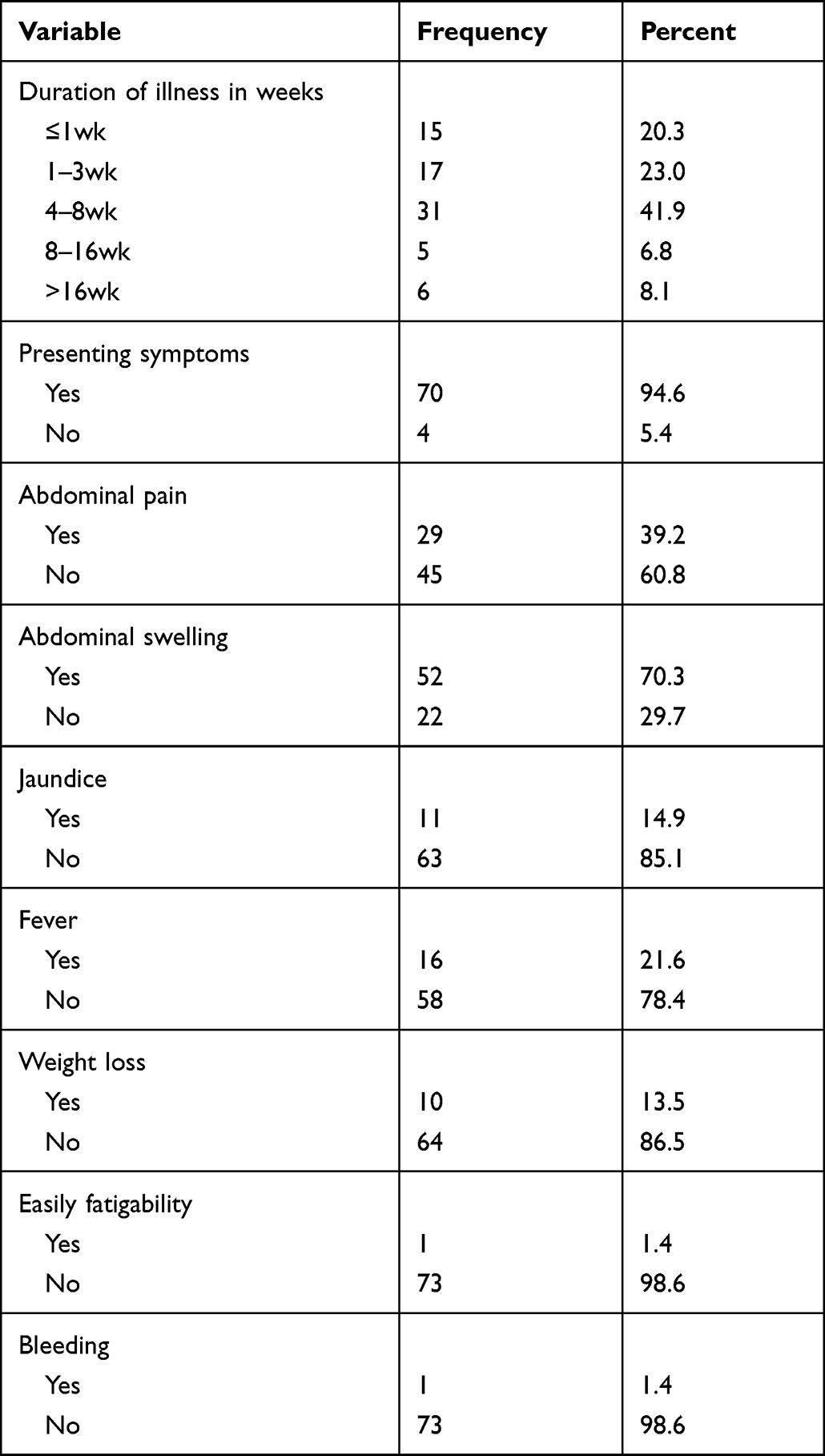 |
Table 2 Presenting Symptoms of Patients with Primary Liver Mass Who Were on Follow-Up in a Tertiary Care Center, in Addis Ababa, Ethiopia |
The Laboratory Characteristics of the Study Patients
Basic laboratory investigations were performed in children with primary liver masses. AST was elevated in 42 (58.3%), ALT was elevated in 24 (17.8%), and ALP was elevated in 70 (94.4%). INR was prolonged in 26 (61.9%), and AFP was high in 20 (45%) of patients. Forty-five (60.8%) patients were anemic, ESR was elevated in 37 (52%), and LDH was elevated in 42 (60.9%) of patients at presentation. Only one case was HBVsAg positive as shown in Table 3.
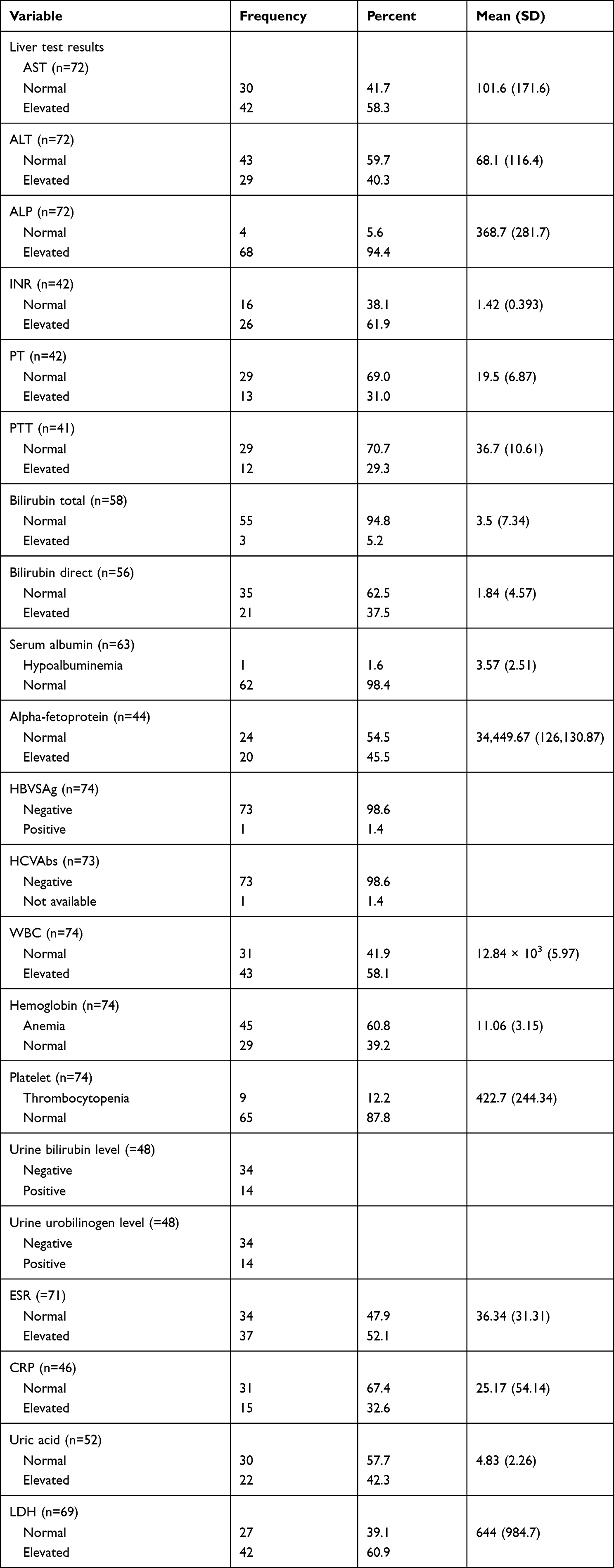 |
Table 3 Frequency of Laboratory Parameters in Patients with Liver Mass Who Were on Follow-Up in a Tertiary Care Center, Addis Ababa, Ethiopia |
Imaging Pattern of the Study Patients
An abdominal ultrasound was performed; benign hepatic mass lesions accounted for 42 (57.5%) and 32 (43.2%) were malignant liver masses. The common benign hepatic mass was pyogenic liver abscess, 16/42 (38.1%), and the common malignant hepatic mass was hepatoblastoma, 25/32 (78.1%). The right lobe of the liver was involved in 48 (64.9%), the left lobe was involved in 12 (16.2%), and both lobes were involved in 14 (18.9%) of cases (Table 4).
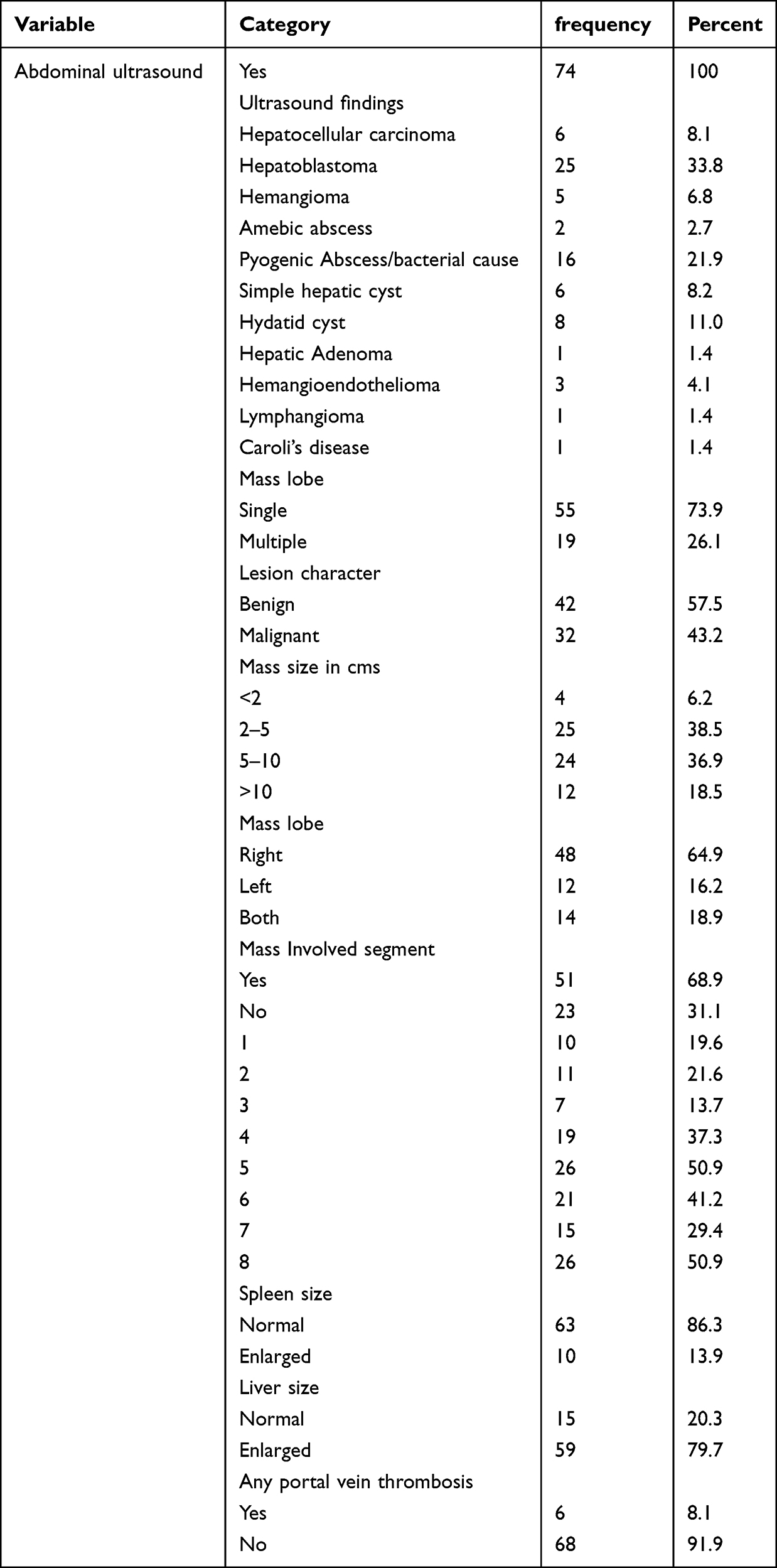 |
Table 4 Frequency of Abdominal Ultrasound Parameters in Patients with Liver Mass Who Were on Follow-Up in a Tertiary Care Center, Addis Ababa, Ethiopia |
The size of the majority of lesions, 25 (38.5%) were between 2 and 5 cm, and 24 (36%) ranged 5–10 cm. Portal vein thrombosis was detected in 6 (8.1%), hepatomegaly in 59 (79.7%), and splenomegaly in 10 (13.9%), respectively.
Abdominal MRI scans were performed for eight patients; 62.5% were benign, and hepatoblastoma was the common malignant liver tumor (Table 5).
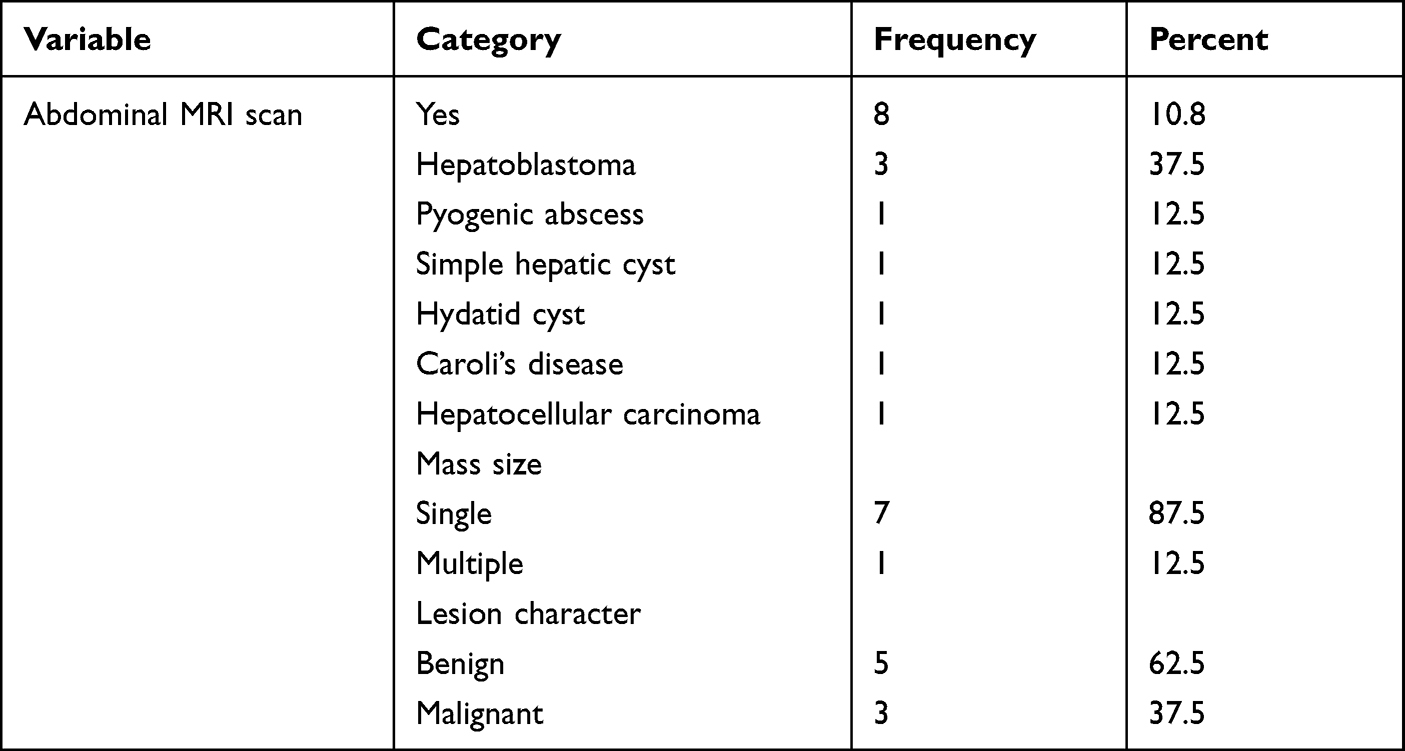 |
Table 5 Frequency of Abdominal MRI Scan Parameters in Patients with Liver Mass Who Were on Follow-Up in a Tertiary Care Center, Addis Ababa, Ethiopia |
The Association of Independent Variables on Pyogenic Liver Abscess
In the binary logistic regression, residence, abdominal pain, and fever were statistically significant (P = 0.05). In multivariate logistic regression analysis, abdominal swelling and fever were significantly associated with pyogenic abscesses (P = 0.05) as shown in Table 6.
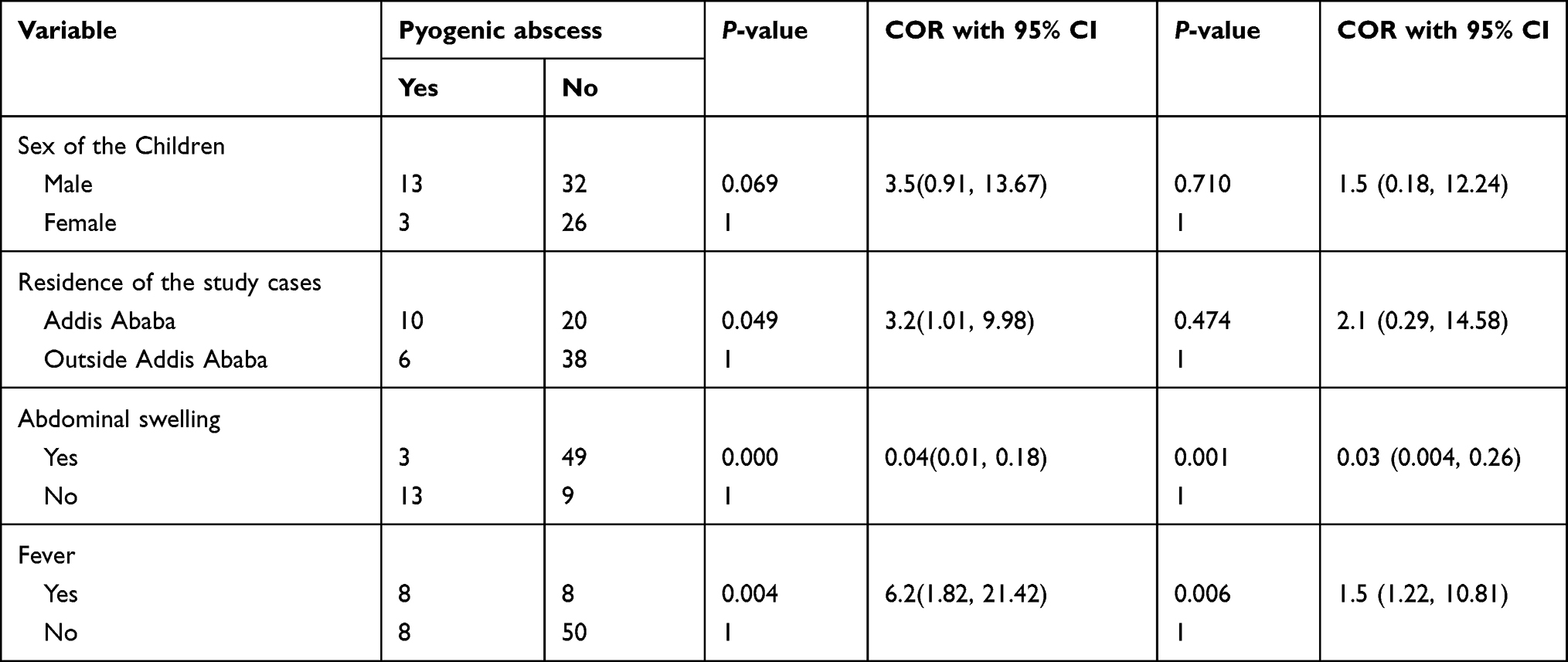 |
Table 6 Bivariate and Multivariate Logistic Regression in Patients with Liver Mass Who Were on Follow-Up in a Tertiary Care Center, in Addis Ababa, Ethiopia |
The Association of Independent Variables with Hepatoblastoma
In the binary logistic regression, age, sex, residence, duration of illness, and AST and LDH levels were statistically significant (P = 0.05). Infants had a 17.1-fold risk of developing hepatoblastoma disease compared to children aged >8 years (AOR = 17.1, 95% CI: 1.84, 3.49), and patients with an elevated LDH level had a 6.9-fold higher chance of having hepatoblastoma than those with normal LDH levels (AOR = 6.9, 95% CI: 2.20, 219.4), shown in Table 7.
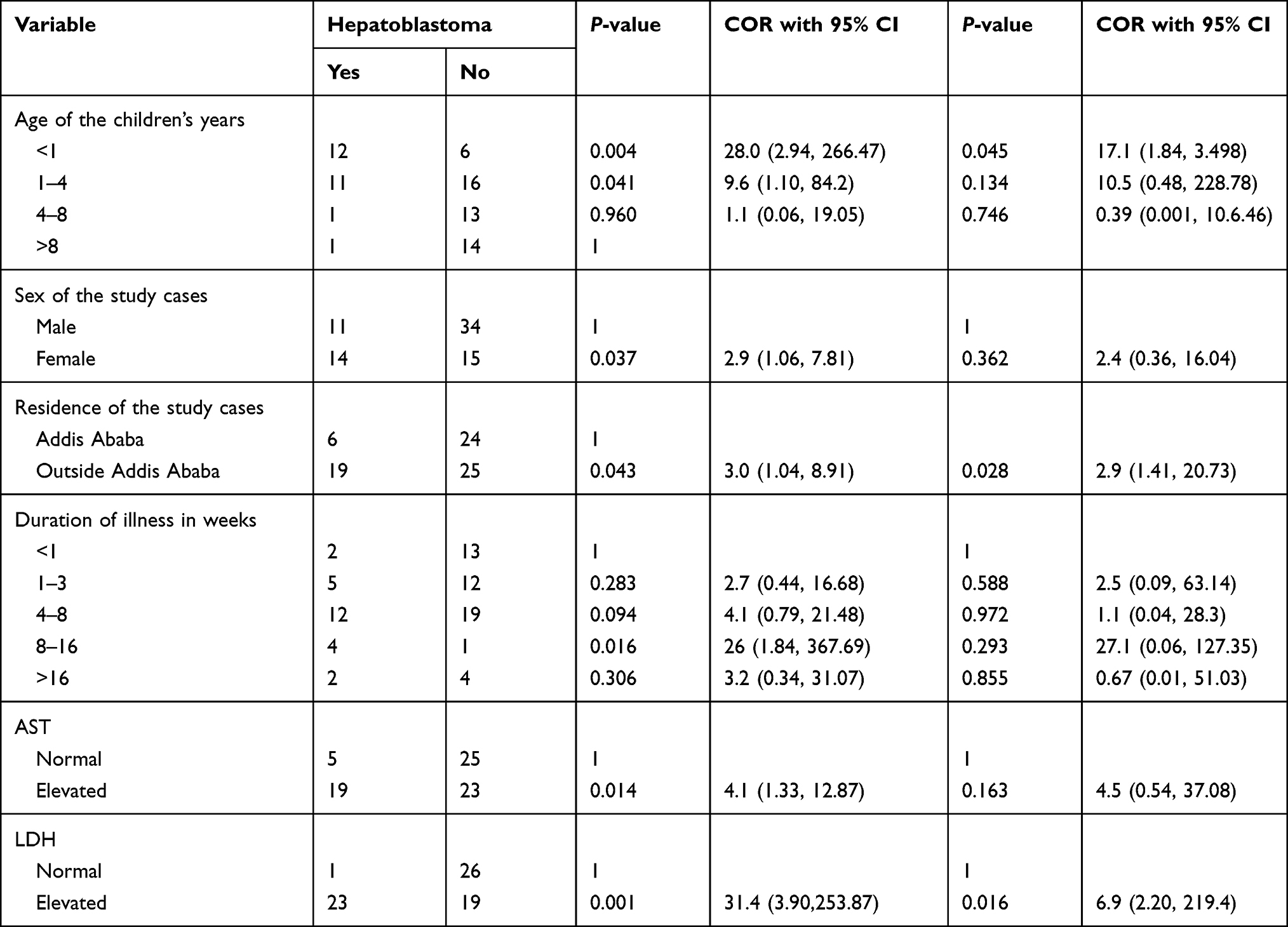 |
Table 7 Bivariate and Multivariate Logistic Regression Showing the Association of Independent Variables on Hepatoblastoma in Patients with Liver Mass Who Were on Follow-Up in a Tertiary Care Center, in Addis Ababa, Ethiopia |
Discussion
Our study showed that the mean age at diagnosis of a liver mass was 4.6 years and more than one-third of the children were between 1 and 4 years. The duration of illness from the onset of symptoms to the tertiary treatment center ranged from 4 to 8 weeks in nearly half of the patients. The most common presenting symptom was abdominal pain (74.8%), and based on ultrasound findings benign hepatic lesions accounted for 42 (57.5%) of the cases. Right lobe liver was involved in 48 (64.9%), and the left lobe was involved in 12 (16.2%) which is in line with other studies.18–20 The common benign hepatic mass was a pyogenic liver abscess, 16/42 (38.1%) in our study. The Multivariate logistic regression showed abdominal swelling and fever were significantly associated with pyogenic liver abscess at P-value of 0.05 (P = 0.001 COR, 95% CI: 0.03 (0.004, 0.26)) and 0.05 (P = 0.006; 95% CI: 1.5 (1.22, 10.81)), respectively.
Our study also showed that hepatoblastoma was the most common malignant tumor, which is similar to other studies.21–23 Patients aged <1 year had 17.1-fold high risk of hepatoblastoma diagnosis than children aged >8 years (AOR = 17.1, 95% CI: 1.84, 3.49), those with abdominal swelling had 6.7-fold increase in hepatoblastoma cases than the opposite compartment (AOR = 6.7, 95% CI: 2.15, 300), and patients with an elevated LDH level had 6.9-fold higher chance of hepatoblastoma than those with a normal LDH level.
In our study, the determinant factors that were significantly indicated for the presence of malignancy were female sex: had 2.1-fold malignant liver tumors than males (AOR = 2.1, 95% CI: 1.62, 7.08), and abdominal swelling; had 11.7-fold increased risk of malignancy (AOR = 11.7, 95% CI: 1.79, 7.17).
Conclusion
In our study, more than one-third of children with liver masses were aged 1–4 years with a mean age of 4.6 years. Benign hepatic masses were the most common. Pyogenic liver abscess was the most common benign hepatic lesion, whereas hepatoblastoma was the most common malignant liver tumor in children. Most lesions were solitary and involved the right lobe. Knowing the patterns of liver masses will help in early diagnosis and decrease the morbidity and mortality in children with liver masses.
Strengths and Limitations of the Study
The study was conducted in only one tertiary hospital, and the results may not reflect the exact characteristics of liver masses in Ethiopia. However, the results can be assumed to reflect the characteristics of liver mass, as the survey was carried out at the nation’s largest referral tertiary hospital, where most cases were referred from all corners of Ethiopia.
Data Sharing Statement
Data are available on request from the corresponding author.
Ethical Approval
Ethical approval was obtained from the Research and Publication Committee of the Pediatrics and Child Health Department, School of Medicine, College of Health Sciences, Addis Ababa University, and College Institutional Review Board (IRB). The study was compiled with the Declaration of Helsinki and the requirement for informed consent was waived because of the anonymous nature of the data. Confidentiality was fully maintained during data collection and analysis.
Acknowledgment
We thank the Department of Pediatrics and Child Health for allowing us to complete this study. We express our deep sense of gratitude and respect to the patients and their attendants, who passed through challenges in their treatment course and disease state.
Funding
This study did not receive any funding.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Jones J, Bell D, Lall N, et al. Liver lesions (pediatric). Reference article. Radiopaedia.org; 2023.
2. Lucas B, Ravishankar S, Pateva I. pediatric primary hepatic tumors: diagnostic considerations. Diagnostics. 2021;11(2):333. PMID: 33670452; PMCID: PMC7922091. doi:10.3390/diagnostics11020333
3. Chiorean L, Cui XW, Tannapfel A, et al. Benign liver tumors in pediatric patients - Review with emphasis on imaging features. World J Gastroenterol. 2015;21(28):8541–8561. PMID: 26229397; PMCID: PMC4515836. doi:10.3748/wjg.v21.i28.8541
4. Global HELP Organization. HELP (Health Education using Low-cost Publication); Paediatric Surgery: a Comprehensive Text For Africa; CHAPTER 107; Liver Tumours; Graeme Pitcher, V. T. Joseph; 2011:622–632.
5. Potisek NM, Antoon JW. Abdominal Masses. Pediatr Rev. 2017;38:101–103. doi:10.1542/pir.2016-0087
6. Ng K, Mogul DB. Pediatric Liver Tumors. Clin Liver Dis. 2018;22:753–772. doi:10.1016/j.cld.2018.06.008
7. Tarek N, Herzog CE. Neoplasms of the Liver. In: Nelson Textbook of Pediatrics. Philadelphia; 2019.
8. Venkatesh SK, Chandan V, Roberts LR. Liver masses: a clinical, radiologic, and pathologic perspective. Clin Gastroenterol Hepatol. 2014;12(9):1414–1429. PMID: 24055987; PMCID: PMC3959647. doi:10.1016/j.cgh.2013.09.017
9. De Lope CR, Reig ME, Darnell A, Forner A. Approach of the patient with a liver mass. Frontline Gastroenterol. 2012;3(4):252–262. doi:10.1136/flgastro-2012-100146
10. Ishak KG, Anthonly PP, Niederau C. Nakanuma Y Mesenchymal tumors of the liver. In: Hamilton SR, Aatonen LA, editors. World Health Organization Classification of Tumors: Tumors of the Digestive System. Wiley and Sons; 1976.
11. Bhaijee F, Oshima K, Anders RA. Hepatic mass lesions: challenges and pitfalls. Diagn Histopathol. 2017;23(12):544–552. doi:10.1016/j.mpdhp.2017.11.002
12. Segura Grau A, Valero López I, Díaz Rodríguez N, Segura Cabral JM. [Liver ultrasound: focal lesions and diffuse diseases]. Semergen. 2016;42(5):307–314. Spanish. doi:10.1016/j.semerg.2014.10.012
13. Hansen N, Weadock W, Morani A, Carlos R. Liver lesions discovered incidentally on ultrasound: evaluation of reader ability to characterize lesions on MRI without intravenous contrast. Acad Radiol. 2012;19(9):1087–1093. doi:10.1016/j.acra.2012.06.001
14. Hapani H, Kalola J, Trivedi A, Chawla A. Ultrasound evaluation of focal hepatic lesions. IOSR J Dent Med Sci. 2014;13(12):40–45. doi:10.9790/0853-131244045
15. Amare Woldie. Clinical and imaging characterization of patients with focal liver lesions with emphasis on hepatocellular carcinoma at TASH from August 1, 2019, to July 30, 2020; 2021.
16. Chung EM, Cube R, Lewis RB, et al. Pediatric liver masses: radiologic-pathologic correlation, Benign tumors. RadioGraphics. 2010;30:801–826. doi:10.1148/rg.303095173
17. Schima W, Kölblinger C, Ba-Ssalamah A. Non-invasive diagnosis of focal liver lesions: an individualized approach. Cancer Imaging. 2012;12(2):365. doi:10.1102/1470-7330.2012.9025
18. Urban BA, Fishman EK, Kuhlman JE, Kawashima A, Hennessey JG, Siegelman SS. Detection of focal hepatic lesions with spiral CT: comparison of 4-and 8-mm interscan spacing. Am J Roentgenol. 1993;160(4):783–785. doi:10.2214/ajr.160.4.8456665
19. Kuszyk BS, Bluemke DA, Urban BA, et al. Portal-phase contrast-enhanced helical CT for the detection of malignant hepatic tumors: sensitivity based on comparison with intraoperative and pathologic findings. Am J Roentgenol. 1996;166(1):91–95. doi:10.2214/ajr.166.1.8571914
20. Butler TJ, McCarthy CF. Pyogenic liver abscess. Gut. 1969;10(5):389–399. PMID: 5771671; PMCID: PMC1552853. doi:10.1136/gut.10.5.389
21. Geramizadeh B, Bahador A, Foroutan HR, Banani A, Nikeghbalian S, Malek-Hosseini SA. Pathology of pediatric liver tumors, a single center experience from south of Iran. Indian J Pathol Microbiol. 2010;53(3):422. doi:10.4103/0377-4929.68258
22. Litten JB, Tomlinson GE. Liver tumors in children. Oncologist. 2008;13(7):812–820. doi:10.1634/theoncologist.2008-0011
23. Moore SW, Davidson A, Hadley GP, et al. Malignant liver tumors in South African children: a national audit. World J Surg. 2008;32(7):1389–1395. doi:10.1007/s00268-008-9526-8
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.