")
Back to Journals » Patient Preference and Adherence » Volume 18
Patients’ and Relatives’ Preferences for Outpatient and Day Care Services Within End-of-Life Care in Germany – A Discrete Choice Experiment
Authors Apolinarski B, de Jong L, Herbst FA , Huperz C , Röwer HAA , Schneider N, Damm K , Stiel S
Received 21 October 2023
Accepted for publication 8 February 2024
Published 29 February 2024 Volume 2024:18 Pages 519—529
DOI https://doi.org/10.2147/PPA.S442047
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jongwha Chang
Beate Apolinarski,1,* Lea de Jong,2,* Franziska A Herbst,1 Carolin Huperz,1,3 Hanna AA Röwer,1 Nils Schneider,1 Kathrin Damm,2,* Stephanie Stiel1,*
1Institute for General Practice and Palliative Care, Hannover Medical School, Hannover, Germany; 2Center for Health Economics Research Hannover (CHERH), Leibniz University Hannover, Hannover, Germany; 3Faculty of Engineering and Mathematics, Bielefeld University of Applied Sciences, Bielefeld, Germany
*These authors contributed equally to this work
Correspondence: Franziska A Herbst, Hannover Medical School, Institute for General Practice and Palliative Care, Carl-Neuberg-Strasse 1, 30625 Hannover, Germany, Fax +49 511 532 4176, Email [email protected]
Purpose: In Germany, patients with incurable chronic diseases living at home increasingly have the option of using outpatient and day care hospice and specialized palliative care services. The present study examined and compared patients’ and their relatives’ preferences for end-of-life outpatient and day care services.
Patients and Methods: The study used a questionnaire integrating a discrete choice experiment. For six scenarios, participants chose between two hypothetical end-of-life care offers, described by seven attributes. The model compared place of care, frequency and duration of care and support, specialized medical palliative care, accompanied activities, and relieving patient counselling. The model also included optional overnight care and willingness to pay. Patients and the relatives of patients suffering from incurable, chronic diseases who were not yet receiving palliative care were recruited via hospitals and self-help groups (06/2021– 07/2022).
Results: The results were based on data from 436 questionnaires (patients: n=263, relatives: n=173). All attributes had a statistically significant impact on choice decisions, with place of care showing the greatest importance. All respondents highly preferred care in the patient’s home over out-of-home care. Patients stressed the importance of special medical (palliative) care and valued accompanied activities, often facilitated by hospice volunteers. Relatives, but not patients, considered the frequency and duration of care highly relevant.
Conclusion: The results suggest a higher demand for care in the patient’s home than for out-of-home care. Patients’ and relatives’ high preference for special medical care and the relief of family caregiver burden should be considered in the design of day care services.
Keywords: palliative care, hospice care, preferences, discrete choice experiment, medical day care, ambulatory care
Introduction
Patients suffering from advanced, life-limiting illnesses often wish to stay at home for as long as possible and, if possible, to die at home.1–4 In fact, only a minority are cared for in their own home until death. In 2022, a study used health insurance data to examine the place of death of 26,590 people in Germany who lived at home and needed care in the three years prior to their death.5 Overall, only a quarter of those people observed died in their own home (26.6%) while 36.9% died in a hospital. A further 36.5% moved to another care setting and died there.
In the home environment, care is primarily provided by relatives,6 who frequently experience care-related burden and report a need for relief and support.7–9 Patients and their family caregivers can receive support from palliative or hospice outpatient care services within the comfort of their own homes. Frequency and nature of visits are determined in close consultation with the patient and their family. Outpatient hospice services focus on holistic end-of-life support, emphasizing comfort and emotional support with the help of volunteers. In contrast, outpatient palliative care services offer comprehensive medical and psychosocial assistance from professionals tailored to the patient’s specific needs, aiming to enhance overall well-being. The aim of both services is to provide the best support and care possible to enhance the patient’s quality of life and alleviate family burden.
Although the number of palliative and hospice outpatient care services has increased over recent decades, the need for outpatient palliative care is not considered met in Germany: a ratio of one specialized outpatient palliative care service team per 100,000 residents and one outpatient hospice service per 40,000 residents is recommended.10 To meet this demand, twice as many specialized outpatient palliative care service teams and 1.5 times more outpatient hospice care services in Germany are needed.11,12 Apart from this, day hospices and palliative day care clinics are becoming increasingly integrated into the hospice and palliative care landscape in Germany. These services differ from outpatient palliative care services and outpatient hospice services in their approach to care. While outpatient services focus on delivering home-based support, day hospices and palliative day care clinics provide structured daytime care within specialized facilities, offering medical and psychosocial care. These day services aim to offer relief to caregiving relatives and facilitate social interaction for patients with life-limiting illnesses. An inventory analysis revealed that in 2020, 17 hospice or palliative day care facilities existed in Germany, and an additional 16 day care facilities were planned to be established in the near future.13 Regardless of the specific diagnosis (oncological, non-oncological), patients with an advanced, life-limiting illness at the end of life can make use of outpatient or day care hospice or palliative care services. In Germany, the costs of palliative medical or hospice care are generally covered by health insurance, while in some cases, hospice services are financed solely through donations and the work is provided by volunteers.
The present work is part of the ABPATITE project, which aims to align the emerging day care services in hospice and palliative care more closely with the actual needs of patients and their families. It is not yet clear which forms of care patients and their relatives actually prefer at the end of life, and which of the services offered are decisive for their choice of care. Few studies have examined patient preferences for palliative day care. Lehnert et al14 investigated patient preferences for long-term care service packages in Germany regarding home- and community-based care attributes, and Douglas et al15 asked patients who had already received palliative day care in one of four palliative day care centers in England about their preferred services. In both studies, respondents stated a preference for long service hours. Respondents in England also showed a preference for specialist therapies and routine access to a medical doctor. Both studies collected data using a discrete choice experiment. However, they did not explore the preferences of relatives. A study conducted by Hall et al16 focused solely on exploring the preferences of informal caregivers in Australia through a discrete choice experiment. The researchers identified varying needs for support services among family members, depending on the patient’s progression of the illness and the level of care required.
Other studies comparing the views of patients and family caregivers have primarily used qualitative research methods.17,18 To the best of our knowledge, there has been no empirical research on preferences for hospice and palliative day care facilities in Germany.
The development and expansion of new palliative care services should align with patients’ and relatives’ preferences, in order to improve patient and family caregiver satisfaction regarding end-of-life care and quality of life.
Objectives
The present study examined preferences for palliative care services for patients at home at the end of life, among: (1) patients suffering from incurable, chronic diseases with a potentially palliative disease progression who were not yet receiving palliative or hospice care and (2) their relatives. Additionally, the research compared preferences between these groups.
Methods
The methods and findings are reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement.19 A discrete choice experiment questionnaire was administered as part of “ABPATITE” – a mixed-methods multi-perspective study exploring the status of and demand for hospice and palliative day care services in Germany.20 Discrete choice experiments are frequently used in health economics to identify and quantify preferences based on the Random Utility Theory by McFadden21 and the Consumer Demand Theory by Lancaster.22 The underlying assumption of the present research was that healthcare services can be disaggregated and described by a set of attributes at varying levels. Respondents were asked to choose between two or more attribute-based alternatives (ie, “care offers”), and their discrete choices were analyzed using regression models that estimated the relative importance of each underlying attribute or level.23
Attributes and Levels
The results of a literature review and two expert discussions conducted within the “ABPATITE” project were used to identify the most relevant attributes and corresponding levels.20 Seven attributes (ie, 1×2 levels, 5×3 levels, 1×6 levels) were identified to describe a broad range of possible palliative care options. The inclusion of a cost attribute enabled preferences to be converted into monetary terms (ie, willingness to pay). A sufficiently wide level range was classified, as recommended by the literature.24 Table 1 displays the attributes and levels. Supplement 1 provides a description of each attribute.
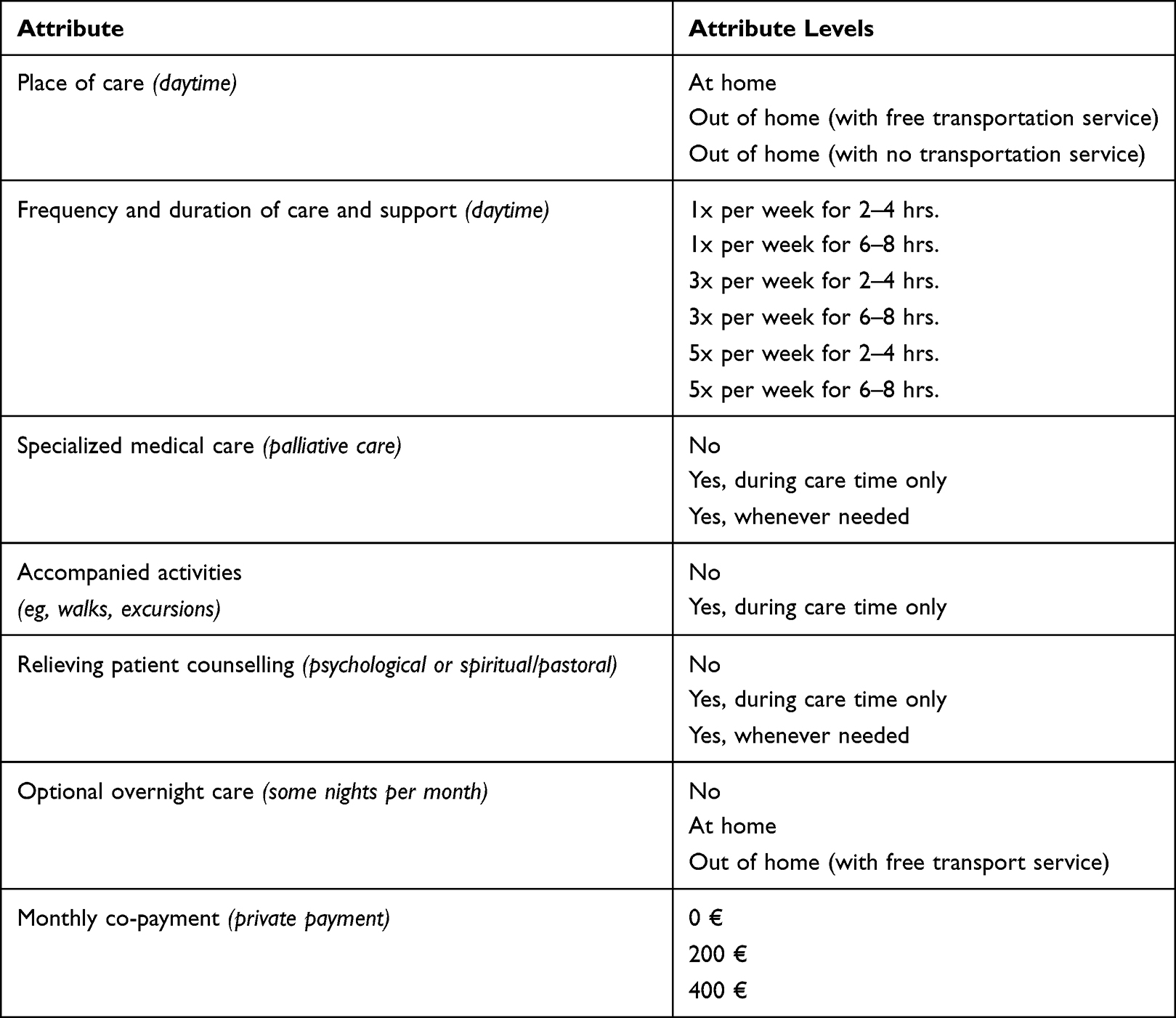 |
Table 1 Discrete Choice Experiment Attributes and Levels |
The comprehensibility and logic of the attributes and levels, as well as the entire questionnaire, were pretested using a stepwise procedure with n=10 patients and n=12 relatives. The questionnaire was modified based on participants’ comments and subsequently retested. In this modification, the questionnaire wording was simplified, but no attributes or levels were replaced.
Experimental Design
The software SAS 9.4 (Enterprise Guide 7.1) was used to create a two-alternative forced-choice design.25 As the full factorial design would have resulted in LA = 2916 possible attribute level combinations, a fractional factorial design with 36 choice sets was created, allowing for the clean estimation of main effects. To reduce respondent burden, the design was blocked into six questionnaire versions, each with six choice sets. All sets were checked for plausibility and randomly assigned to the questionnaire versions. Within these questionnaire versions, there were no correlated attributes. Generic alternatives (ie, offer A vs B) were chosen. The %MktEx macro was used to create the fractional factorial design, and the %ChoicEff macro was used to identify a D-efficient design. A detailed explanation of all macros is provided by Kuhfeld.25 A priori attribute coefficients were set to 0.
Study Population and Sample Size
Currently, only approximate methods exist for sample size estimation in discrete choice experiments. Here, the formula (ie, rule of thumb) by Johnson and Orme (2010) was used to determine a required sample size of n=250. Patients were included who: (1) suffered from incurable, chronic diseases (eg, cancer or non-oncological diseases such as organ insufficiencies or degenerative neurological diseases), (2) had the physical and mental ability to participate, (3) were currently hospitalized or had been hospitalized at some point over the prior 12 months and (4) had not yet received palliative or hospice care. The relatives of these patients were also recruited. Participants were recruited within a 60km radius of the city of Hanover (Germany), predominantly through 11 clinical departments in 5 hospitals. In addition, five self-help groups for terminally ill patients or their relatives were contacted. Finally, participants were recruited via the project website.
The survey was administered between June 2021 and July 2022. Six trained study nurses and research associates contacted prospective participants and conducted the questionnaire-based interviews, predominantly face-to-face. If a face-to-face meeting was not possible, respondents were offered to complete the paper-based questionnaire at home, with a telephone interview (due to the COVID-19 pandemic). Consent was obtained from each study participant prior to the interview. Responses were captured in written form on the questionnaire.
The Questionnaire
The 10-page questionnaire was printed in book format, to facilitate readability. Participants received instructions on how to complete the questionnaire, a detailed description of each attribute and level, and a sample choice decision. Specifically, respondents were asked to imagine the following situation:
For your subsequent decisions between care options A and B, please imagine in each case that:
- You are (your relative is) affected by an advanced, incurable disease, but do (does) not need to be cared for in hospital;
- Care is possible in your own (your relative’s) home;
- You (your relative) can leave your own (their) home independently;
- Basic body-related care (eg, help with body washing or dressing/undressing) is provided by a nursing service; and
- You (your relative) receive(s) basic medical care from a general practitioner, as well as emergency care, if required.
Subsequently, respondents were asked to choose their preferred care offers for six choice tasks (see Figure 1). Different versions of the questionnaire (ie, blocks) were presented to respondents in random order, to ensure that order bias was not systematic across the sample.
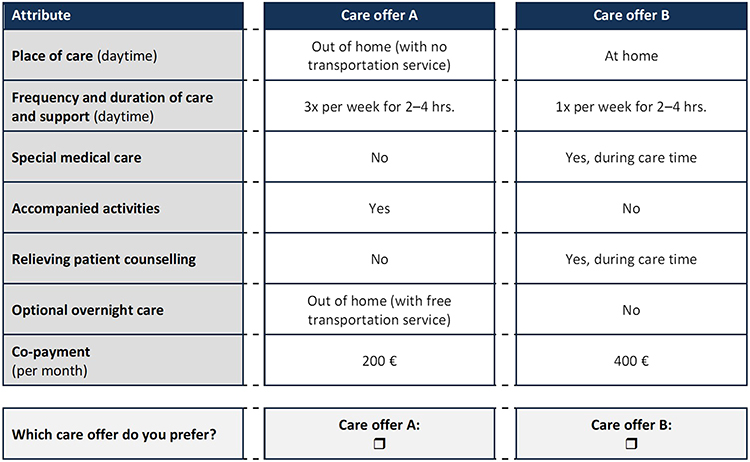 |
Figure 1 Example of a discrete choice experiment choice set. |
After completing the discrete choice experiment, respondents answered 25 additional questions regarding the difficulty of the discrete choice experiment, their end-of-life care wishes (for themselves or their relative), their (or their relative’s) activities in everyday life, their socio-demographic characteristics and their experiences with long-term care and points of contact with hospice care. A blank space was provided for further comments. This manuscript, however, reports only on preferences. Other elements explored in the main study are not reported here.
Data Analysis and Interpretation
The choice data analysis was based on Lancaster’s characteristics theory of demand22 and random utility theory.26 It was assumed that each individual would choose the alternative (ie, care offer) that provided them with the highest utility. The utility U of an individual q choosing alternative i was deconstructed into a deterministic part V and a non-explainable or random component ԑ, and written as:24

For the multivariate analyses, conditional logit models were used. Error terms were assumed to be independently distributed with a type 1 extreme value (Gumbel) distribution. The probability of choosing one alternative i over the other was given by:
All attribute levels were dummy-variable coded, except for the cost attribute. Corresponding coefficients were interpreted as deviations from the predefined reference level. Preference for an attribute level was indicated by a positive coefficient (>0), while a negative coefficient (<0) indicated a non-preference for that attribute level. Statistical significance was assumed for p-values ≤ 0.05. Using the co-payment cost attribute, the marginal willingness to pay (MWTP) for each attribute level was calculated in comparison to the reference level, as follows:

All analyses were conducted using R statistics 4.2.1.27 The study was approved by the Ethics Committee of Hannover Medical School, Germany (8892_BO_S_2020). All respondents provided written consent.
Results
Description of Participants
During the survey period, 769 people (patients: n=455, relatives: n=314) were asked to take part in the study. In total, 453 interviews were conducted (n=274 [63%] face-to-face, n=162 [37%] by telephone). Reasons given for non-participation were the cognitive ability (advanced age) of respondents, or the complexity or length of the questionnaire. Due to missing information on age or gender, or more than two unanswered choice tasks, 17 questionnaires were excluded from further analysis. The resulting (n=436) questionnaires were completed by n=263 patients and n=173 relatives. Of these, 137 (31%) reported a primary oncological diagnosis or a relative with a primary oncological diagnosis. Participants predominantly answered the questionnaire at the time of hospitalization (patients: n=207 [79%]; relatives: n=120 [69%]); for 49 (19%) patients and 38 (22%) relatives, hospitalization had occurred within the prior 7 months. With respect to gender, 126 (48%) patients and 115 (66%) relatives were female. Of the relatives, approximately half were employed full- or part-time. Table 2 presents the participant characteristics in more detail.
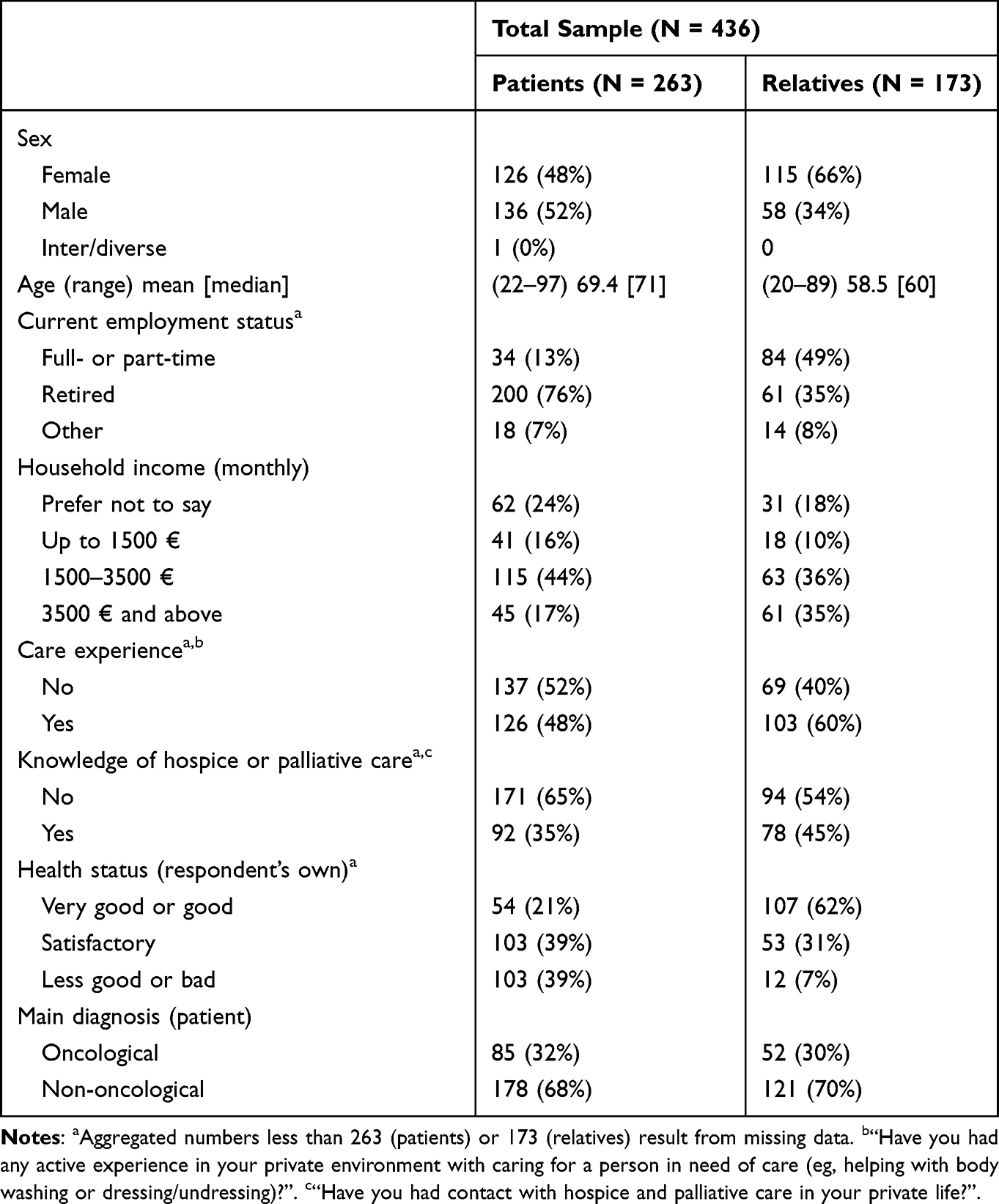 |
Table 2 Participant Characteristics |
Approximately half of the relatives (n=149 [47%]) described that their responses referred to their spouse or partner, 43 (25%) to their mother, 35 (20%) to their father and 10 (6%) to their adult child. Among the relatives, 144 (83%) were willing to participate in caring for the related patient, and 92 (53%) were willing to become the main caregiver. Of the working relatives, 37 (44%) indicated that they would be willing to reduce their working hours or stop working completely to support/care for their terminally ill relative. In contrast, 32 (38%) stated that they would not reduce their working hours, mostly for financial reasons.
Patients’ and Relatives Preferences for Attributes of End-of-Life Care
The results of the conditional logit model showed that, for the entire sample of patients and relatives, all attributes had a statistically significant impact on decisions (see Supplement 2). Separate analyses of patient and relative responses revealed some similarities as well as differences in preferences between the two groups (see Tables 3 and 4). Both groups attributed the greatest importance to place of care, with a clear preference for care in the patient’s home. Out-of-home care with no transportation service was the least preferred. In relation to cost, patients were willing to pay up to 417 € (relatives: 682 €) per month for at-home care, rather than care outside the home (with no transportation service).
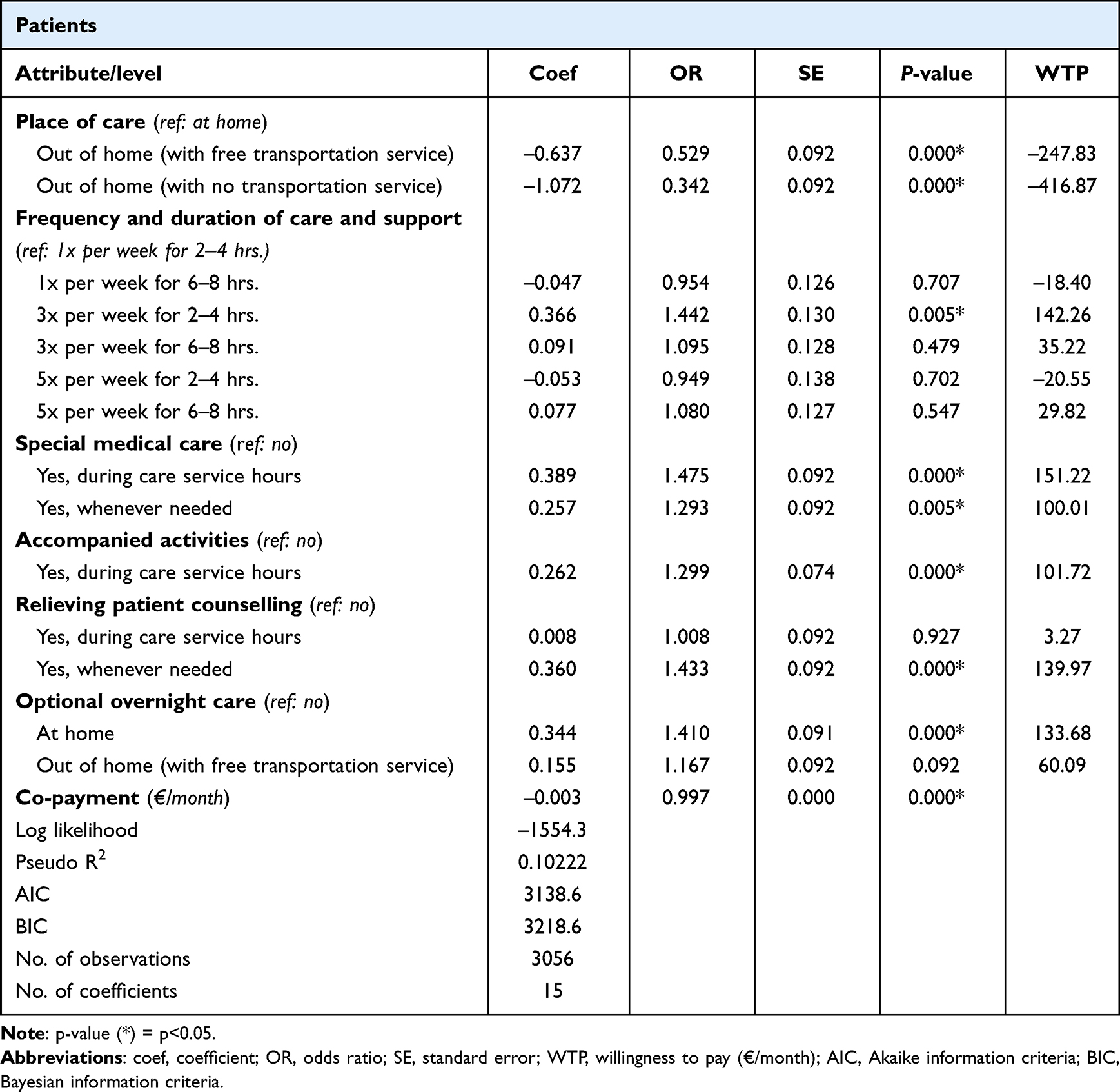 |
Table 3 Patients’ Preferences for End-of-Life Care (Conditional Logit Model) |
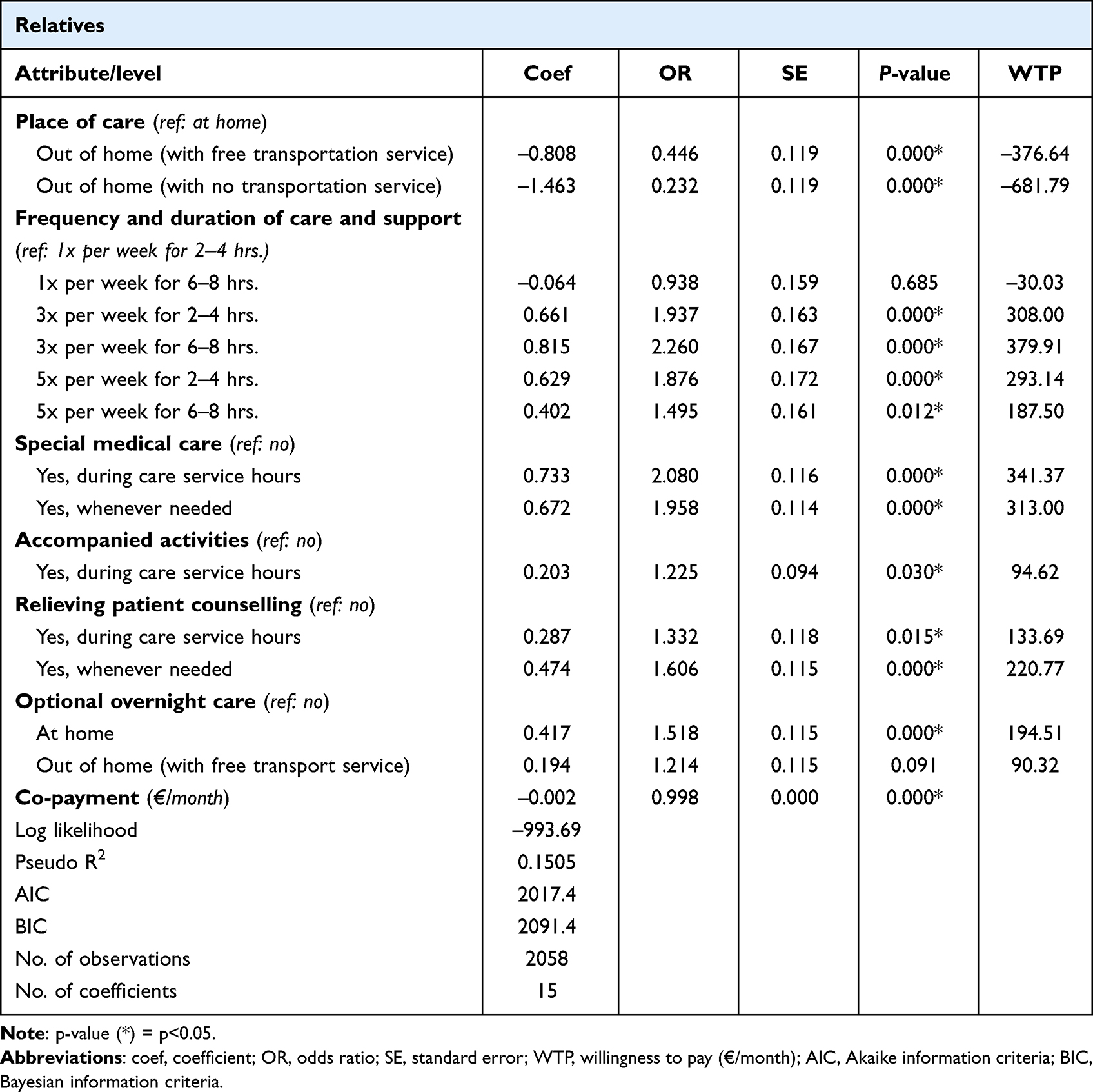 |
Table 4 Relatives’ Preferences for End-of-Life (Conditional Logit Model) |
Patients stressed the importance of special medical (palliative) care, particularly during care service hours, an aspect increasing the odds of selection by the factor 1.48 (OR). Equally important to them was the option of overnight care at home. Patients also wished to have access to patient counselling at any time, when needed. Furthermore, they preferred care service options with accompanying activities, but this was less important to them than the previously mentioned care offers.
With regard to the frequency and duration of care and support, patients considered only one level (ie, 3x per week for 2–4 hrs.) relevant (compared to the referent service time of 1x per week for 2–4 hrs.). No other levels of this attribute were statistically significant. Here, a difference with the choice decisions of relatives was apparent. For relatives, both attribute frequency and duration were important. Specifically, they preferred services that were offered more frequently than once per week, with most preferring a care service offer of three times a week for 6–8 hours at a time. Their corresponding willingness to pay was 380 € per month.
Relatives also placed particular importance on special medical care (OR: 2.08 or 1.96). Furthermore, they considered optional night care at home central, as well as relieving patient counselling at any time. Similar to the patients, they considered the offer of accompanied activities relevant but less important.
Discussion
Main Study Findings
The present study surveyed and compared for the first time the preferences of patients suffering from incurable, chronic diseases and their relatives, with regard to outpatient and day care services in Germany. In particular, similarities and differences in the priority given to certain attributes between patients and their relatives should be emphasized. Patients and relatives most appreciated when care services took place at the patient’s home. This finding aligns with the results of previous studies, reporting that the patient’s home is the preferred care location at the end of life.1–4 The desire to be cared for at home was also expressed by patients and relatives through their willingness to pay a higher amount for home-based care compared to care provided outside the home. Relatives, in particular, show a notable readiness to make financial sacrifices, emphasizing the importance they place on ensuring the highest level of care for their ill family members. In Germany, outpatient and home care are typically cost-free, but the hypothetical amount reflects the emotional value attached to these attributes.
Furthermore, patients and relatives deemed the provision of special medical (palliative) care particularly important, consistent with Douglas et al,15 who reported a significant patient preference for routine access to a medical doctor.
However, differences emerged between the preferences of patients versus relatives. Patients also assessed services such as accompanied activities (primarily delivered by volunteers in the hospice sector) important. In their critical review of patient autonomy at the end of life, Houska and Loučka28 reported that support for patients’ daily activities fulfilled their desire to “be normal” and “take charge” – two core structural domains of patient autonomy.
Relatives showed a preference for services with a high frequency and long duration of care and support, which could relieve their caregiver burden and better enable them to maintain everyday life routines. Hall et al16 similarly reported that family caregivers in Australia preferred services that supported them in their caregiving role.
Despite the preference of many individuals for home care, it is important not to dismiss day care facilities entirely. Certain services, like respite care for family members and particular medical treatments may potentially be implemented more effectively in an external facility than in one’s own residence. According to Apolinarski et al29 interviews with experts suggest that day care services may meet the needs of a specific group of patients more effectively than other forms of care, including the home environment. Moreover, some patients require regular invasive treatments to relieve their symptoms, which can be better carried out in a palliative day care clinic than at the patient’s home.30 In our study, a minority of respondents specifically indicated a preference for receiving care outside their homes. This subgroup was in a slightly better state of health, which may be an explanation.
Strengths and Weaknesses of the Study
A strength of the study is that it examined the preferences of both patients and relatives, enabling a comparison between groups. Additionally, the study design was able to explore what outpatient care should look like in order to meet the needs and wishes of patients and relatives. Finally, the sample was comprised of a very large and diverse group of patients and relatives. By considering people with a wide range of diagnoses and other different participant characteristics (Table 2), as many different perspectives as possible were taken into account.
Nevertheless, some limitations should be acknowledged. First, the preferences listed here represent the respondents’ choice from a limited set of possible answers. Although the attributes shown are based on a comprehensive literature review, the DCE procedure does not allow respondents to add their own points and make them available for selection. Few respondents criticized this in the free text comments. According to the comments, some respondents found it difficult to make a choice of care packages if the stated personal financial contribution was contrary to the perceived service scope.
Second, the present study examined relatives who would not necessarily be primary caregivers at patients’ end of life. If solely actual caregivers had been studied, certain relief attributes (with respect to, eg, the frequency and duration of care and support) might have emerged as more important. Finally, since the data were collected at only one point in time, no temporal or experiential changes in preferences could be measured.
Conclusion
This study contributes to a deeper understanding of preferences in hospice and palliative care for patients living at home. The differences in preferences between patients and relatives underscore the importance of considering individualized approaches in designing hospice and palliative care services, tailoring services to meet the diverse needs of both patients and the burdens faced by their relatives. This is particularly relevant in view of the dynamic development of newly emerging day care facilities in Germany, where the needs and preferences of the target population should always be at the center of attention. Thus, the extent to which relatives can easily integrate the support offering into their everyday lives should be considered in the planning and development of hospice and palliative day care services. Facilities should be open for appropriately long hours, especially since existing facilities do not always offer assisted transport to and from the facility, with the result that the responsibility for transportation often falls on relatives.
Finally, patients’ and relatives’ high preference for special medical care should be considered in the design of day care services. Close cooperation between day care facilities and family physicians or physicians within specialized outpatient palliative care service teams may be relevant in this context.
In summary, the findings provide practical indications for the enhancement of hospice and palliative care services, emphasizing the need for flexibility, accessibility, and a focus on relieving caregiver burden. Integrating these insights into the planning and development of services will contribute to a more responsive and patient-centered approach, ultimately improving the effectiveness and inclusivity of hospice and palliative care in Germany.
Data Sharing Statement
The study datasets are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The study was approved on 25 February 2020 by the Ethics Committee of Hannover Medical School (N° 8892_BO_S_2020) and the appointed data protection officer of Hannover Medical School. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Written informed consent was obtained from all patients and family caregivers included in the study.
Consent for Publication
Written informed consent for publication was obtained from all patients and family caregivers included in the study.
Trial Registration
The present study comprised part of the study ABPATITE and is registered in the German Clinical Trials Register (ID: DRKS00021446; date of registration: April 20, 2020; https://drks.de/search/de/trial/DRKS00021446).
Acknowledgments
The authors thank the cooperating clinics for their commitment and help in recruiting patients and their relatives. They also thank all patients and family caregivers for their participation in the study. Finally, the authors acknowledge Valerie Appleby for her copyediting of the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The present study comprised part of the study “ABPATITE – Improving health care for patients with terminal, progressive illnesses: Status and demand analysis for palliative day care clinics and day hospices and recommendations for health care planning”, financed by the German Innovation Fund of the Federal Joint Committee (Gemeinsamer Bundesausschuss) (Grant N° 01VSF19034). The funding body was not involved in the study design; the collection, analysis and interpretation of study data; or the drafting of this article.
Disclosure
Dr Franziska Herbst reports spokesperson for the Research Working Group of the German Society for Palliative Medicine (DGP) and spokesperson for the Humanities and Social Sciences Professions Section of the German Society for Palliative Medicine (DGP). The authors declare that they have no other conflicts of interest in this work.
References
1. Leng A, Maitland E, Wang S, Nicholas S, Lan K, Wang J. Preferences for end-of-life care among patients with terminal cancer in China. JAMA Network Open. 2022;5(4):e228788–e228788. doi:10.1001/jamanetworkopen.2022.8788
2. Blanchard CL, Ayeni O, O’Neil DS, et al. A prospective cohort study of factors associated with place of death among patients with late-stage cancer in Southern Africa. J Pain Sympt Manage. 2019;57(5):923–932. doi:10.1016/j.jpainsymman.2019.01.014
3. Alsirafy SA, Hammad AM, Ibrahim NY, Farag DE, Zaki O. Preferred place of death for patients with incurable cancer and their family caregivers in Egypt. Am J Hospice Palliative Med®. 2019;36(5):423–428. doi:10.1177/1049909118813990
4. Rainsford S, MacLeod RD, Glasgow NJ. Place of death in rural palliative care: a systematic review. Palliative Medicine. 2016;30(8):745–763. doi:10.1177/0269216316628779
5. Schnakenberg R, Fassmer AM, Allers K, Hoffmann F. Characteristics and place of death in home care recipients in Germany–an analysis of nationwide health insurance claims data. BMC Palliat Care. 2022;21(1):172. doi:10.1186/s12904-022-01060-w
6. Stajduhar KI, Funk L, Toye C, Grande GE, Aoun S, Todd CJ. Part 1: home-based family caregiving at the end of life: a comprehensive review of published quantitative research (1998-2008). Palliative Medicine. 2010;24(6):573–593. doi:10.1177/0269216310371412
7. Veloso VI, Tripodoro VA. Caregivers burden in palliative care patients: a problem to tackle. Curr Opin Support Palliat Care. 2016;10(4):330–335. doi:10.1097/SPC.0000000000000239
8. Bialon LN, Coke S. A study on caregiver burden: stressors, challenges, and possible solutions. Am J Hospice Palliative Med®. 2012;29(3):210–218. doi:10.1177/1049909111416494
9. Washington KT, Benson JJ, Chakurian DE, et al. Comfort needs of cancer family caregivers in outpatient palliative care. J Hosp Palliat Nurs. 2021;23(3):221. doi:10.1097/NJH.0000000000000744
10. Radbruch L, Payne S. Standards und Richtlinien für Hospiz-und Palliativversorgung in Europa: Teil 2. Zeitschrift für Palliativmedizin. 2011;12(06):260–270. doi:10.1055/s-0031-1276957
11. Kassenärztliche Bundesvereinigung. SAPV-Teams, Available from: https://gesundheitsdaten.kbv.de/cms/html/17067.php.
12. Arias-Casais N, Garralda E, Rhee J, et al. EAPC atlas of palliative care in Europe. Romania. 2019;122:77.
13. Apolinarski B, Herbst FA, Röwer HAA, Schneider N, Stiel S. Status quo palliativmedizinischer Tageskliniken und Tageshospize in Deutschland: Ergebnisse einer gemischt-methodischen Studie. Zeitschrift für Palliativmedizin. 2021;22(04):215–224. doi:10.1055/a-1514-8871
14. Lehnert T, Günther OH, Hajek A, Riedel-Heller SG, König HH. Preferences for home-and community-based long-term care services in Germany: a discrete choice experiment. Eur J Health Econ. 2018;19(9):1213–1223. doi:10.1007/s10198-018-0968-0
15. Douglas H-R, Normand CE, Higginson IJ, Goodwin DM. A new approach to eliciting patients’ preferences for palliative day care: the choice experiment method. J Pain Sympt Manage. 2005;29(5):435–445. doi:10.1016/j.jpainsymman.2004.08.017
16. Hall J, Kenny P, Hossain I, Street DJ, Knox SA. Providing informal care in terminal illness: an analysis of preferences for support using a discrete choice experiment. Med Decis Mak. 2014;34(6):731–745. doi:10.1177/0272989X13500719
17. Bergenholtz H, Missel M, Timm H. Talking about death and dying in a hospital setting-a qualitative study of the wishes for end-of-life conversations from the perspective of patients and spouses. BMC Palliat Care. 2020;19(1):1–9. doi:10.1186/s12904-020-00675-1
18. Bollig G, Gjengedal E, Rosland JH. They know!—do they? A qualitative study of residents and relatives views on advance care planning, end-of-life care, and decision-making in nursing homes. Palliative Medicine. 2016;30(5):456–470. doi:10.1177/0269216315605753
19. Vandenbrouckel JP, von EE, Altman DG, et al. Strengthening the reporting of observational studies in epidemiology (STROBE): explanation and elaboration. PLoS Med. 2007;4(10):1628–1655.
20. Herbst FA, Stiel S, Damm K, Jong L D, Stahmeyer JT, Schneider N. Exploring the status of and demand for palliative day-care clinics and day hospices in Germany: a protocol for a mixed-methods study. BMC Palliat Care. 2021;20(1):1–9. doi:10.1186/s12904-021-00792-5
21. McFadden D. Conditional logit analysis of qualitative choice behavior; 1973.
22. Lancaster KJ. A new approach to consumer theory. J Political Econ. 1966;74(2):132–157. doi:10.1086/259131
23. Johnson FR, Lancsar E, Marshall D, et al. Constructing experimental designs for discrete-choice experiments: report of the ISPOR conjoint analysis experimental design good research practices task force. Value Health. 2013;16(1):3–13. doi:10.1016/j.jval.2012.08.2223
24. Lancsar E, Louviere J. Conducting discrete choice experiments to inform healthcare decision making. Pharmacoeconomics. 2008;26(8):661–677. doi:10.2165/00019053-200826080-00004
25. Kuhfeld WF. Marketing research methods in SAS: experimental design, choice, conjoint, and graphical techniques. Cary NC. 2010;1:681–801.
26. Manski CF. The structure of random utility models. Theory Decis. 1977;8(3):229. doi:10.1007/BF00133443
27. The R Foundation. Available from: https://www.r-project.org/foundation/.
28. Houska A, Loučka M. Patients’ autonomy at the end of life: a critical review. J Pain Sympt Manage. 2019;57(4):835–845. doi:10.1016/j.jpainsymman.2018.12.339
29. Apolinarski B, Huperz C, Röwer HAA, Schneider N, Stiel S, Herbst FA. Expert perspectives on the additional benefit of day hospices and palliative day care clinics in Germany: a qualitative approach. Am J Hospice Palliative Med®. 2024;41(2):167–172. doi:10.1177/10499091231168574
30. Müller A, Paul A, Best J, Kunkel S, Voltz R, Strupp J. “My everyday life has returned to normal”-experiences of patients and relatives with a palliative day care clinic: a qualitative evaluation study. BMC Palliat Care. 2023;22(1):1–12. doi:10.1186/s12904-023-01140-5
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.