")
Back to Journals » Patient Preference and Adherence » Volume 18
Patient Perceptions of Medical Students’ Involvement in Clinical Classes: A Cross-Sectional Survey
Authors Kaliszewski K , Makles S , Frątczak A , Kisiel M , Lipska P , Stebel A
Received 15 October 2023
Accepted for publication 22 December 2023
Published 3 February 2024 Volume 2024:18 Pages 301—313
DOI https://doi.org/10.2147/PPA.S444797
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Krzysztof Kaliszewski, Szymon Makles, Agnieszka Frątczak, Michał Kisiel, Patrycja Lipska, Agata Stebel
Department of General, Minimally Invasive and Endocrine Surgery, Wroclaw Medical University, Wroclaw, 50-556, Poland
Correspondence: Szymon Makles, Tel +48 662 761 377, Email [email protected]
Introduction: A crucial aspect of the education of prospective medical professionals is their interaction with patients. The study aimed to explore patients’ perspectives on the interaction between medical students and themselves. It sought to understand how patients perceive this dynamic within clinical classes. The goal was to gather insights into the most favorable behavior and demeanor of medical students during these sessions, with the overarching objective of enhancing patient comfort.
Material and Methods: The authors collected a total of 403 surveys from patients of a teaching hospital, regarding their perception of students as healthcare providers. The participants ranged in age from 18 to 92. 53.83% of the participants were female, and 46.17% were male. The surveys were collected between April 8th, 2022, and August 10th, 2022. The results of the anonymous survey undergone statistical analyses using the Mann‒Whitney U-test for comparing two groups and the Kruskal‒Wallis test for comparing more than two groups, because the Shapiro‒Wilk test indicated that the data did not follow a normal distribution.
Results: The study delved into patients’ assessments of students’ external presentation, adherence to behavioral norms, empathetic qualities, consideration during intimate examinations, and preferences for the organization of clinical classes. Our research indicates notable differences in responses based on age. Specifically, the senior demographic prioritizes students’ external presentation, communication and the utilization of courteous language more often than younger individuals (p< 0.05). Attendees exhibit varying levels of interest in participating in educational sessions with students based on the ward. Significantly, individuals in the gynecology ward display the least enthusiasm for engagement (p< 0.05). Notably, the majority of patients perceive their involvement in the education of future healthcare professionals to be essential (83.38%).
Conclusion: The study found that generally, patients voluntarily engage in educational classes with students. The relationship between patients and students is amicable, and the majority of students display a respectful demeanor toward patients. Nonetheless, preserving patient confidentiality and ensuring the proper management of classes remain persistent issues. This is particularly crucial, especially when the clinical classes pertain to intimate and personal health matters of a patient. Upholding and enriching the organization of such sessions, along with the attentiveness and knowledge of medical students regarding patient comfort, assumes heightened significance.
Keywords: medical education, clinical teaching, student-patient relationship, patients’ opinions on students, patient partners
Introduction
Bedside teaching (BST) serves a vital educational purpose within medical education.1,2 BTS, first described by Sir William Osler in 1903, brought teaching medicine to the patient’s bedside.3,4
BST has been shown to reassure and relax patients.5 Generally, patients are pleased with teaching rounds. Patients report that they can understand their illness better during BST than during examinations without BST.6 BST allows the development of both the clinical and interpersonal skills of students.7,8
Effective communication skills of medical staff have a positive impact on the care provided to patients.9–11In spite of the considerable benefits associated with bedside teaching, its prevalence in medical education has experienced a decline, a trend exacerbated by the challenges posed by the COVID-19 pandemic.12 The decrease in time dedicated to BST may have negative consequences on the quality of patient care.13
Patient willingness to assist with student education greatly enhances the quality of teaching.14 Clinical classes should be made as comfortable as possible for patients. Studies have shown that patients derive satisfaction from contributing to the development of medical students.15–17 Student contact can help patients better understand their illness.18 Many patients consent to student participation out of altruism or a desire to support education.19
However, patients have concerns about students accessing their sensitive personal information and the potential breach of medical confidentiality, as well as dissemination of their personal matters by students.15–17 Up to 50% of patients, particularly young women, may hesitate to discuss emotional issues or undergo intimate examinations with medical students before seeing their GP, according to a 2008 study.17 Patients have also reported negative experiences with students who are insecure, disinterested, or unable to communicate effectively.15,16,20 Patients may be less accepting of medical student involvement in specialist clinics such as obstetrics and gynecology or genitourinary medicine due to the intimate nature of the problems addressed and the high level of trust required in medical staff professionalism.19
It is important to teach students clinical empathy, also known as “detached concern”.21 Clinical empathy involves responding to the emotional needs of patients in a clinical setting.22 Clinical empathy is defined as “the act of correctly recognizing another person’s emotional state without experiencing that state yourself”.23 Teaching students clinical empathy can both help students and ensure that the emotional needs of their patients are met. Additional advantages include the observation of exemplary behavior, the provision of constructive feedback in a formative manner, and the integration of patient perspectives into the instructional context.
Our study aimed to discern patients’ perspectives within a teaching hospital on the demeanor and appearance of medical students during clinical classes. We explored patients’ opinions on various aspects, including respect for privacy, communication skills, such as the overuse of medical jargon,24,25 appearance, behavior, clinical empathy, and patients’ altruistic inclinations toward aiding students. Additionally, the study sought to identify potential variations in patient opinions based on gender, age, educational levels, and the specific clinical wards in which they were hospitalized, especially those dealing with intimate health issues (eg, gynecology, urology). This comprehensive examination contributes valuable insights to clinicians involved in medical education, fostering a patient-centric approach that accommodates diverse perspectives based on demographic and clinical characteristics.
Materials and Methods
The study was conducted at a teaching hospital, where clinical classes and student summer internships take place. Clinical classes, led by medical specialists and educators in a hospital setting, involve medical students (typically in groups of 6 or more) in activities including taking patient history, physical examinations, fundamental medical procedures, and discussions on patient findings and documentation. These sessions are conducted under the supervision of medical teachers.
The study population comprised in-patients with prior participation in clinical classes involving medical students. The sample included individuals admitted to a university clinical hospital, selected from wards where daily and regular clinical classes with medical students and patient involvement are conducted. The sample size was calculated to align with the study’s objectives and ensure relevance to the targeted population. Inclusion criteria stipulated: adults above 18 years, admission to specific wards (Department of General, Minimally Invasive and Endocrine Surgery; Department of Internal Medicine, Occupational Diseases and Hypertension; 2nd Department of Gynecology and Obstetrics; Department of Orthopedic and Traumatological Surgery; and Department of Urology and Oncologic Urology), experience in medical classes with students, provision of written informed consent, and physical and mental fitness for survey completion. Exclusion criteria encompassed participants who submitted incomplete or signed questionnaires.
The study was conducted using the diagnostic survey method, with data collection occurring between April 8th, 2022, and August 10th, 2022.
The data collection for this study involved the use of an original questionnaire consisting of two parts: a section on demographics and 30 statements that participants evaluated using a 5-point Likert scale. The questionnaire survey was chosen as an appropriate method for measuring attitudes and opinions in a standardized manner.
The subjects of this study were asked to provide information regarding their age, gender, education, and the ward in which they were staying at the time of data collection.
Five variables were created to analyze the opinions of participants. To study each of the variables, a series of statements were formulated based on a comprehensive review of the literature. These statements were designed to elicit information on the specific topic of interest.
The face validity of these statements in relation to the examined variables was assessed using Kendall’s W-test, with the participation of qualified judges including a doctor of clinical psychology, a medical doctor with experience in teaching students during clinical classes, and a specialist in medical communication.
Of the statements evaluated, the 30 that demonstrated the highest face validity and level of agreement among the judges were selected for inclusion in the questionnaire administered to the control sample.
The questionnaire was formulated in the Polish language and subsequently translated into English for incorporation into this manuscript. It is important to note that the English version was not employed or validated, as all participants in both the control and research groups were native Polish speakers. Therefore, the translation necessitates validation for prospective investigations involving English-speaking populations. An English translation of the questionnaire, along with the original questionnaire in Polish are available in the Supplementary Materials.
The studied variables included: appearance, which examined patients’ views on the appropriateness of the appearance of students during clinical classes; propriety, which assessed patients’ perceptions of appropriate standards of behavior for students during clinical classes; empathy and altruism, which explored patients’ views on the ability of students to understand and respond to their feelings, as well as the altruistic needs of patients with regard to the education of future medical professionals; intimacy and privacy, which assessed patients’ views on the level of care and attention given to their comfort in intimate examinations and their privacy by students during clinical classes; and organization of clinical classes, which examined patients’ opinions on the most comfortable way to organize clinical classes.
A control sample of 40 participants (representing 10% of the planned research sample) was selected for the study, with care taken to ensure that the subjects in this sample were similar in terms of key characteristics such as age, gender and social background to the planned research sample. The control trial was conducted in the same five wards where the research trial was planned. Subjects in the control trial did not participate in the research trial.
In addition to completing the questionnaire, participants in the control sample were asked to paraphrase each of the statements and provide their initial associations with them to verify that the statements were formulated in a clear and understandable manner.
Based on the results of this assessment, the wording of a few items was revised for clarity. The final survey in the research sample included 30 statements related to the studied variables.
Patients hospitalized at the teaching hospital, were informed by the researchers of the opportunity to participate in an anonymous survey. Patients expressing their willingness to participate in the study were provided with a consent form to participate in the study along with information about the study.
The questionnaires were made available in a publicly accessible location in the ward where interested patients could retrieve them for completion. To ensure the anonymity of the participants, the completed questionnaires were collected in a specially prepared, sealed container that was placed in a location accessible to the participants. This method of distributing and collecting the questionnaires was in accordance with the recommendations of the Bioethics Committee at the Wroclaw Medical University for conducting anonymous surveys among participants.
The study received ethical approval from the Bioethics Committee at the Wroclaw Medical University (No: 185/2022). Informed consent was obtained from the authorities of each individual clinic where the questionnaires were collected.
Statistical Analysis
To analyze the responses, the Shapiro‒Wilk test26 was applied to all variables to determine whether the answers to the questions followed a normal distribution. As the test indicated that the data did not follow a normal distribution, we employed nonparametric tests for independent groups to compare each observation to the median.
These tests included the Mann‒Whitney U-test27 for comparing two groups and the Kruskal‒Wallis test28 for comparing more than two groups. If the Kruskal‒Wallis test yielded a statistically significant result, we also conducted post hoc tests, consisting of multiple comparisons of average ranks for all groups. The significance level for each test was set at p=0.05.
Results
Of the 475 participants who were recruited for in our study, 23 refused to participate, 35 were excluded from the sample due to their health condition, and 14 returned incomplete questionnaires.
Ultimately, the research sample included 403 participants undergoing treatment in 5 wards: the Department of General, Minimally Invasive and Endocrine Surgery (20.10%); Department of Internal Medicine, Occupational Diseases and Hypertension (20.84%); 2nd Department of Gynecology and Obstetrics (19.85%); Department of Orthopedic and Traumatological Surgery (19.35%); and Department of Urology and Oncologic Urology (19.85%).
Of the 403 participants in the sample, 53.83% were female, and 46.17% were male; their ages ranged from 18 to 92 years. The study group was divided into five age groups, namely, 18–35 (20.10%), 36–49 (22.08%), 50–64 (20.60%), 65–70 (15.88%), and 71–92 (21.34%) years old. Participants varied in education level: primary (7.69%), secondary (34.74%), higher (37.47%), basic vocational (20.10%). The aforementioned data are presented in Table 1.
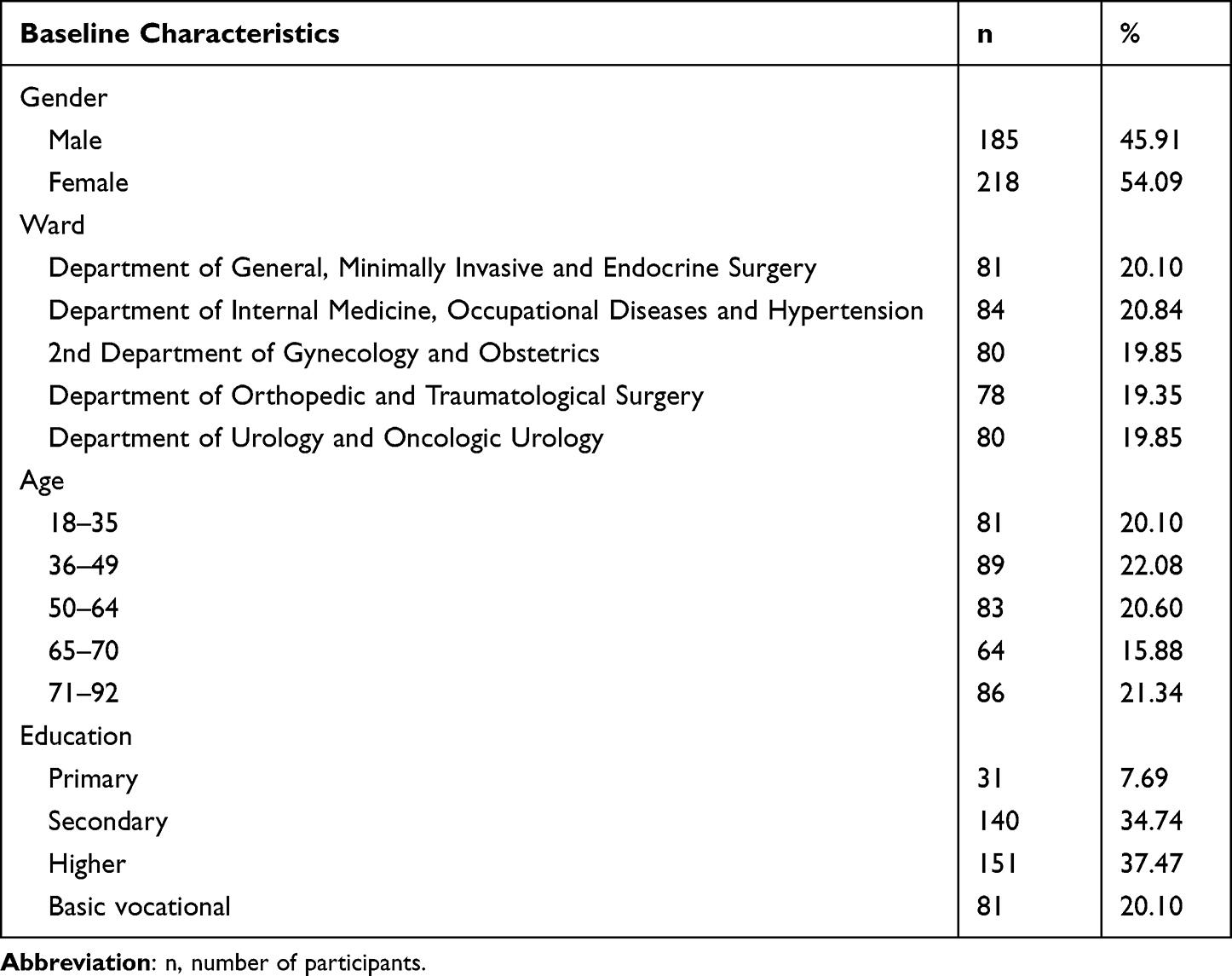 |
Table 1 Division of the Participants Included in the Study |
The study revealed a diverse array of participants’ perspectives regarding the appearance, demeanor and comportment displayed by medical students during clinical classes.
Appearance
A total of 82.13% of participants paid attention to the neatness of medical students’ clothes during classes. Statistically significant differences were found between age groups (p<0.0001). Participants aged 71–92 (93.03%) judged the tidiness of clothing more often than participants aged 18–35 (67.9%, p<0.0001),36–49 (82.02%, p=0.0008) and 50–64 (80.73%, p=0.02).
In total, 46.4% of participants were bothered when medical students kept their hands in their pockets during a conversation. Differences by education level were statistically significant (p=0.038), with more highly educated participants (median answer 4) being more frequently disturbed than those with basic vocational education (median response 3, p=0.043).
Moreover, 34.99% of participants thought that medical students did not seem stressed during clinical classes, 35.48% thought the opposite, and 29.53% had no opinion. No statistically significant differences were observed by age group, gender, ward or education level.
A total of 28.04% of participants believed that medical students should not wear expressive makeup. Statistical analysis revealed significant differences by ward (p=0.026) as well as age group (p<0.0001). In the urology ward, 38.75% of participants held this view compared to 24.36% in the orthopedic ward (p=0.049). These beliefs differed between participants aged 18–35 (4.94%) and those aged 50–64 (24.09%, p=0.034), 65–70 (42.19%, p=0.00003), and 71–92 (46.51%, p=0.000003).
51.61% of participants did not think medical students should cover their tattoos, 22.33% thought the opposite, and 26.05% did not have an opinion. The study showed statistically significant differences among age groups (p<0.0001). A total of 43.03% of participants aged 71–92 exhibited aversion to visible tattoos, while fewer participants aged 18–35 (4.93%, p<0.0001), 36–49 (16.86%, p=0.002) and 50–64 (10.84%, p=0.004) expressed such aversion.
Propriety
A total of 46.41% of participants believed that medical students should always introduce themselves with their full name upon entering the participants’ room. Statistically significant differences were found among age groups (p=0.003), with participants aged 71–92 (mode 5 representing the most common response) more likely to hold this view than participants aged 18–35, who often saw such an introduction as unnecessary (mode 3 representing the most common response, p=0.004).
Eighty-five percent of participants preferred medical students to greet them when entering the room, 5.21% did not find it necessary, and 8.93% had no opinion. We found no statistically significant differences by age group, gender, ward or education level.
23.08% of participants believed that medical students used their mobile phones too often, 41.19% did not observe such a problem, and 35.73% had no opinion. Statistical analysis revealed no significant differences within analyzed groups.
Additionally, 83.13% of participants believed that medical students should always disclose that they are students. The study showed statistically significant differences among age groups (p=0.0001). Participants aged 18–35 (77.77%) paid less attention to such information than participants aged 50–64 (81.93%, p=0.029), 65–70 (84.38%, p=0.009), and 71–92 (83.72%, p=0.0005).
A total of 18.37% of participants believed that medical students used incomprehensible medical jargon too often, 45.66% did not, and 35.98% had no opinion. No statistically significant differences were observed.
In total, 14.39% of participants believed that medical students used overly colloquial language. Differences between age groups were statistically significant (p=0.006), with none of the participants aged 18–35 observing such an issue while 26.74% of participants aged 71–92 noted this issue (p=0.005).
A total of 47.89% of participants judged medical students on the grounds of their approach to the physician conducting clinical classes. Statistical analysis revealed significant differences by age group (p<0.0001) and education level (p=0.008). Participants aged 65–70 (60.94%) and 71–92 (59.13%) judged students on this basis more often than participants aged 18–35 (41.98%, p=0.015 and p=0.002, respectively) and 36–49 (37.08%, p= 0.004 and p=0.0005, respectively). Participants with higher education (42.39%) exhibited this perspective less frequently than participants with basic vocational education (60.49%, p=0.006).
22.58% of participants reported that medical students had loud conversations in ward corridors, 45.66% did not report this issue, and 31.76% had no opinion. Differences by age group, gender, ward, and education level were found to be statistically nonsignificant.
A total of 64.77% of participants preferred medical students who smiled during clinical classes. The study showed statistically significant differences among age groups (p=0.0001). Participants aged 71–92 found smiling to be more important (76.75%) than participants aged 18–35 (55.55%, p=0.0005), 36–49 (60.68%, p=0.008), and 50–64 (57.83%, p=0.031). Participants aged 65–70 (75%) considered smiling more important than participants aged 18–35 (55.55%, p=0.04).
Empathy and Altruism
54.59% of participants found conversations with medical students helpful in dealing with loneliness. Statistical analysis revealed significant differences by ward (p=0.0037), age group (p<0.0001) and education level (p=0.02). Participants in the urology ward (70%) found such conversations more beneficial than participants in the orthopedic (51.28%, p=0.049) and gynecology (45%, p=0.008) wards. Participants aged 65–70 and 71–92 (median response 5) found having such conversations to be more beneficial than participants aged 18–35 (p=0.012 and p=0.002, respectively), 36–49 (p=0.027 and p=0.005, respectively), and 50–64 (p=0.048 and p=0.008, respectively) (median answer 3). Participants with higher education relied on such conversations less (45.69%) than participants with basic vocational education (65.43%, p=0.032).
75.93% of participants considered it important for medical students to recall their previous conversations, 9.93% disagreed, and 14.14% had no opinion. We found no statistically significant differences by studied groups.
In total, 59.8% of participants complained about medical students having a sole interest in participants’ illnesses, 13.65% had no complaints, and 26.55% had no opinion. Statistical analysis revealed no significant differences by age group, gender, ward, or education level.
A total of 83.33% of participants felt that it was necessary to educate future healthcare professionals. Statistically significant differences were found among age groups (p=0.0001) and wards (p=0.009). Participants in the urology ward felt such education was more necessary (median answer 5) than participants in the gynecology ward (median response 4, p=0.029). Moreover, participants aged 18–35 felt this education was less needed (74.08%) than participants aged 65–70 (90.63%, p=0.004) and 71–92 (87.21%, p=0.005).
Moreover, 40.69% of participants believed that medical students should volunteer to perform examinations during clinical classes more frequently. Statistically significant differences were found by gender, age group (p<0.0001), ward (p<0.0001), and education level (p=0.0017). Women (34.87%) were less content with such initiatives than men (47.57%, p=0.037). Participants aged 65–70 (57.81%) and 71–92 (60.46%) were more likely to express this belief than participants aged 18–35 (20.99%, p=0.017 and p=0.0006, respectively) and 36–49 (26.96%, p=0.005 and p=0.0002, respectively). The least interested were participants in the gynecology ward (12.5%) compared to participants in the internal medicine (41.67%, p=0.041), general surgery (45.68%, p=0.009), orthopedic (47.43%, p=0.002) and urology (56.25%, p=0.00003) wards. Participants with primary education (70.97%) preferred students to volunteer more often than participants with secondary (39.29%, p=0.04) or higher education (32.45%, p=0.003).
Intimacy and Privacy
In total, 20.59% of participants believed medical students disregarded participants’ privacy during clinical classes, 37.96% thought the opposite, and 41.44% had no opinion. Differences by age group, gender, ward, and education level were found to be statistically nonsignificant.
A total of 25.80% of participants felt uncomfortable when a physician left them alone with medical students, with a statistically significant difference between genders (p=0.007). In particular, 33.02% of women and 17.3% of men felt uneasy on such occasions.
45.41% of participants did not feel comfortable with medical students examining their intimate areas. The study showed statistically significant differences among genders (p=0.001) and participants of different education levels (p=0.0014). Women most often felt uncomfortable (mode 5 representing the most common response, and the median answer being 4), whereas men most often were indifferent (mode 1 representing the most common response, and the median answer 3). Participants with basic vocational education reported feeling comfortable (mode 1 representing the most common response, and median answer 3) more often than participants with primary (p=0.003) as well as higher education (p=0.015) (mode 5 representing the most common response, and median answer 4 for both groups).
A total of 18.36% of participants worried that medical students would not preserve their medical confidentiality. Differences among participants from different wards were statistically significant (p=0.049), with participants in the gynecology ward (median response 3) being more concerned than participants in the orthopedic ward (median response 2, p=0.045).
Organization of Clinical Classes
In total, 75.44% of participants cared if the physician asked whether they were willing to participate in clinical classes, 11.91% were indifferent, and 12.66% had no opinion. No statistically significant differences were observed by age group, gender, ward or education level.
81.39% of participants preferred medical students to ask for consent before examination, 9.92% did not, and 8.68% had no opinion. We found no statistically significant differences by age group, gender, ward or education level.
60.05% of participants eagerly participated in clinical classes before their procedures. That willingness differed statistically significantly among participants from different wards (p=0.003). Participants in the gynecology ward (47.5%) tended to agree less than participants in the orthopedic (66.66%, p=0.02) and urology (68.75%, p=0.007) wards.
A total of 57.82% of participants gladly participated in clinical classes after their procedures. Differences were statistically significant by ward (p=0.0007) and education level (p=0.011). Participants in the orthopedic (65.39%) and urology (70%) wards agreed to participate more frequently than participants in the internal medicine ward (46.43%, p=0.049 and p=0.004, respectively). Participants in the urology ward (70%) were more eager than participants in the gynecology ward (53.75%, p=0.025). Participants with primary education (74.19%) complied more often than participants with higher education (53.64%, p=0.02).
In total, 11.66% of participants believed they participated in clinical classes too frequently. Differences by ward were statistically significant (p<0.0001). Participants in the urology and orthopedic wards most often indicated that there was no such issue (median answer 1 for both groups), unlike participants in the gynecology ward (median response 3, p=0.005 and p=0.00009, respectively).
A total of 58.81% of participants were comfortable with female medical students examining them. Statistically significant differences were found by gender (p<0001), age group (p=0.0008) and education level (p=0.0016). Women (66.98%) were more often at ease than men (49.19%). Participants aged 71–92 (70.93%) were more comfortable than participants aged 36–49 (51.68%, p=0.01) and 50–64 (51.8%, p=0.0086). Participants with a primary education (87.09%) were more comfortable than participants with a higher level of education (51.65%, p=0.0068).
Finally, 41.19% of participants were comfortable with male medical students examining them. The study showed statistically significant differences by gender (p<0.0001), ward (p=0.0001) and age group (p=0.027). Men (49.19%) were more frequently unbothered than women (34.4%). Participants in the gynecology ward (28.75%) agreed that they were unbothered less often than participants in the urology (48.75%, p=0.013) and orthopedic (60.26%, p=0.0007) wards. Participants in the orthopedic ward (60.26%) were less troubled than participants in the internal medicine ward (33.33%, p=0.013). Participants aged 71–92 (55.82%) were more unbothered than participants aged 36–49 (28.09%, p=0.044).
Limitations
The study, while providing valuable insights, is not immune to certain limitations. First, the recruitment strategy focused on patients receiving care from medical students, which may have inadvertently selected patients who were more compliant with their care and had more positive perceptions of student involvement. Additionally, the use of questionnaires completed by patients prior to discharge may have been impacted by factors such as lack of privacy or external influence from students, staff members, or other patients.
Moreover, the newly developed questionnaire requires further refinement and testing, as evidenced by its Cronbach’s alpha coefficients ranging from 0.55 to 0.65. While a coefficient of 0.60 is considered acceptable for newly developed instruments, this limitation still warrants consideration. Further refinement and testing are required to fully establish the validity and reliability of the newly developed questionnaire.
Furthermore, the sample size was restricted to only 403 patients from one teaching hospital, which may limit the generalizability of the findings. The need for more diverse samples across various countries and cultures is therefore paramount.
Moreover, we were only able to collect data from patients who were healthy enough to independently complete the questionnaire, potentially excluding those with more severe conditions.
While this issue has been examined by numerous researchers globally, the extent of its investigation in the studied population remains limited. As such, comparative analysis with studies conducted on patients from this population could not be effectively performed, highlighting the need for further research in this area.
Last, it is crucial to acknowledge the demographic differences across the wards in which the data were collected, such as the predominance of young women in the gynecology ward and mostly male patients in the urology ward.
Tables depicting the Results section, are available in the Supplementary Materials.
Discussion
Appearance
Patients’ views on the appropriate appearance of students during clinical classes were assessed in an examination that aimed to gauge the importance of various features. In accordance with our survey, a significant proportion (82.13%) of patients paid attention to the neatness of students’ clothes during classes, consistent with a study from a different cultural setting by Kamata et al, in which 61% of Japanese patients believed physician attire to be important. This study also shares with our work unanimous findings concerning greater attentiveness to the cleanliness of students’ clothing among older patients.29 Another similarity is found in the case of a Polish study, which showed that a healthcare worker’s neat appearance inspires greater trust in patients. In reference to Garus-Pakowska A. this is a vital aspect of the doctor‒patient relationship.30 It can be inferred that the same is likely to be true for medical students, regardless of the cultural background. Nearly half of patients were uncomfortable when students talked to them while keeping hands in their pockets. Patients with higher levels of education were more likely to be disturbed by this behavior than those with basic vocational education. A meta-analysis has associated different elements of nonverbal communication with greater patient satisfaction.31 Collins indicated that in the culture of the studied population, placing hands in pockets can signal either a desire to dominate or a lack of courage and may be perceived negatively by recipients.32 Statistical data in our study indicate a clear similarity regarding the negative perception of such demeanor. However, the fact that medical students might tend to talk to patients while keeping their hands in their pockets is confirmed by Martin CT, Chanda N.33 thus it may be desirable to control such behavior. More than half of the patients surveyed did not believe medical students should cover their tattoos during classes, while over 20% preferred they do. Older patients were significantly more opposed to excessive makeup than younger patients. The same trend regarded the preference for tattoo coverage. This observation aligns with the perception of visible tattoos on service personnel by Dean DH.34 Other studies suggest that the presence of tattoos or expressive makeup on a doctor’s body may be perceived differently in various countries. In Pennsylvania, USA, a study found that, tattoos did not significantly impact the patient’s perception of the doctor.35 However, in Italy, the entire sample considered it inappropriate for a doctor to have visible tattoos or heavy makeup.36 In Brazil, patients also had negative views about doctors with heavy makeup.37 Another similarity can be found in a Polish research, which showed that a significant portion of patients viewed tattoos negatively, with 49% believing that doctors should cover their tattoos and 29.7% advocating for a categorical ban on doctors showing tattoos.38 Essentially, medical students should be aware of patients’ preferences for their appearance and behavior to establish positive patient interactions and build trust.
Propriety
In regards to propriety, our study examined patients’ perceptions of appropriate standards of behavior for students during clinical classes. Large majority of patients (85%) considered it important for students to greet them upon entering the room, yet only patients aged 71–92 believed medical students should introduce themselves with their full name when entering the room. Studies have found that over half of patients want physicians to introduce themselves using their first and last names.39–41 Another study found that 76% of patients preferred physicians to introduce themselves with their full name and academic degree.42 As there is not enough literature on the application of those principles to medical students, our study has confirmed they are of specific importance to patients, but in certain circumstances full introduction may be unnecessary. Over 80% of patients felt that medical students should always identify themselves as such, with younger patients placing less importance on this. According to a last year’s study, only 28% of patients stated that students had adequately introduced themselves.43 The comparison of aforementioned results raises concerns whether medical students are adequately presented with the etiquette of the clinical setting. Almost one in four patients felt that students overused their phones during clinical classes. A Chinese study found that mobile phone addiction is prevalent among medical students and negatively influences their academic achievement, concentration and performance.44 According to a Polish study, 92% of surveyed nursing students used a smartphone at least once per hour.45 Given the fact that mobile phones are a well-known source of pathogen transmission, including drug-resistant bacteria,46 medical students may want to reduce their phone usage in the clinical environment. Less than 20% of patients believed medical students used incomprehensible jargon during clinical classes. Studies have demonstrated that the usage of complex medical language is prevalent among physicians.47,48 It is commonly stated that such jargon can hinder communication between doctors and patients.24,25 Fortunately, a US study shows that medical students are more likely to presume that patients are not familiar with medical jargon.49 This approach is likely reflected in the findings of our study. Half of respondents evaluated students based on their approach toward their clinician. Older patients and those with vocational education place more importance on the student’s approach to the teacher. Limited research exists on this topic, albeit the course of clinical classes, which is inevitably influenced by the student-clinician relationship, holds undeniable significance.
Empathy and Altruism
The empathy and altruism variable explored patients’ perceptions of the ability of medical students to understand and respond to their feelings, as well as the altruistic desires of patients to contribute to the education of future healthcare professionals. Over 60% of patients considered it important for medical students to smile during interactions, suggesting that smiling may be valued by patients as a nonverbal sign of empathy and concern in medical settings. Patients perceive healthcare providers to be more approachable when they smile, as shown by previous research conducted by Lill MM, Wilkinson TJ.50 The authors reached similar conclusions when assessing the impact of a smile, which positively influenced the evaluator’s assessment. The study found that approximately 50% of patients found talking to medical students helpful in loneliness, with older patients benefiting more. This finding suggests that age may affect the effectiveness of verbal communication in addressing loneliness in medical settings. This may be associated with the fact that loneliness tends to affect older individuals, who usually spend extended periods of time in the hospital. A similar correlation was observed in another study,51 indicating that prevalence rates of loneliness in older people residing in long-term care settings are generally high. Additionally, the desire for a conversation with a clinician regarding loneliness is affirmed by various research,52 which unequivocally demonstrates that, similar to our study, engaging in conversation is a fundamental aspect of attention that should be devoted to patients to mitigate loneliness. Regardless of gender, department, age, or education level, 75% of patients emphasized the importance of medical students remembering previous conversations. Over half of the patients surveyed expressed discontent with students focusing exclusively on their illnesses, indicating the need for greater consideration of patient preferences and empathetic student-patient communication. Therefore, it is crucial for students to view patients as people, not just the subject of their disease. A resonating perspective aligns with K. Wojtyła’s contributions to Catholic bioethics.53 The work highlights that patients value being treated as individuals, not just in terms of their health condition. This echoes the essence of our findings. The synergy between effective communication and the cultivated empathetic image of physicians, enhancing overall efficiency54 draws intriguing parallels with the yearning for empathetic discourse discerned in our research. In our study, 83% of patients felt important in the education of future doctors, with a stronger sentiment expressed by patients over 65. Another study confirms that medical training could not occur without the contributions of patients.55 Their essential role in medical education provides meaningful benefits to both students and patients and has the potential to infuse elements of humanism into medical training. Forty percent of patients desired more frequent student volunteering for examinations during classes, with gender, ward, and age influencing patient preferences for hands-on learning. Males and urology ward patients were more willing to participate than those in the gynecology ward, confirming that women were less content with such initiatives than men. Participants with primary education preferred students to volunteer more often than participants with higher education. The lack of literature on this topic necessitates consideration of these factors for comprehensive education of future healthcare professionals.
Intimacy and Privacy
Our study examined how medical students respected patients’ privacy during clinical classes as it is essential for students, similar to licensed physicians, to uphold ethical and legal standards to protect patient confidentiality.56 20% of patients felt that their privacy was not prioritized enough by medical students. Similarly, nearly 20% of patients had concerns about medical confidentiality breaches by medical students with gynecology patients being more worried. Additionally, almost half of patients reported discomfort during intimate examinations involving students, with women being more uncomfortable than men. In diverse cultural settings studies have shown a noticeable lack of knowledge and proper attitude toward patients’ privacy and medical confidentiality among medical students.57,58 Any neglections in this matter may pose a threat to the willingness of patients to participate in clinical teaching.59 Shifting focus to such a crucial aspect of the student-patient relationship seems to be necessary in the process of educating future medical professionals. A quarter of patients felt uncomfortable when left alone with students. An older study has presented that one-third of patients did not want students to examine them without a tutor present. Only 20% of patients consented to students viewing their medical history without a tutor, compared to 60%, who agreed with supervision.60 More research would prove useful for a valid, more in-depth exploration of the matter.
Organization of Clinical Classes
The study investigated patients’ opinions on the organization of clinical classes with medical student involvement. 75% of patients valued being asked for consent before participating in clinical classes with students and over 80% of patients wanted students to always ask for permission before examining them. Similar patient needs were observed in other studies.43,61 One of them emphasized the fact that patients are often not asked about fundamental elements ensuring comfort during medical procedures.43 Teaching hospitals frequently overlook the importance of obtaining consent for student-patient interactions,61 highlighting the relevance of our investigation in this matter and the urgent need to ensure that these principles are applied. 11.66% of all patients believed that they participated in classes with students too often. This suggests that the majority of patients are not overwhelmed during their stay in clinical hospitals. Similar sentiments were presented by participants in a study conducted in Uganda.62 It was inferred that patients are generally comfortable with medical students’ involvement in their care. They even prefer to seek care in hospitals where medical students are trained so that the students may contribute to their care, although Polish research lacks a confirmation of such a trend. Our study found that almost 60% of patients felt comfortable with a female student examining them. Notably, almost 20% fewer patients felt comfortable being examined by a male student. Female patients and older patients were more likely to prefer to be examined by a female student. Patients in the gynecology ward were less comfortable with male students than patients in other departments. Younger patients were less comfortable with male examinations than older patients. Similarly, to our research, as found in studies by Haffling and Håkansson,20 female patients prefer same-gender students. Another similarity is observed in the study on students’ communication skills with patients.63 Male students were rated lower, which is a clear correlation with the comfort experienced by patients during examinations. Efforts should be implemented to eradicate such a propensity.
Conclusions
The study explored patient perspectives on medical students’ conduct and appearance during clinical classes, aiming to inform educational enhancements and elevate patient comfort. The findings underscore the significance of elements such as neat attire, formal introductions, and clear communication, particularly appreciated by older patients. Notably, patient discomfort during intimate examinations emphasizes the imperative for reinforced privacy measures. Confidentiality concerns necessitate enhanced patient consent procedures and closer supervision of medical students. While patients generally exhibit positive engagement in medical education, the study underscores the nuanced considerations required based on department, patient age, or gender. The recommendations include further research to comprehensively delineate factors influencing patient comfort during medical classes in regions with limited existing studies.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The study received ethical approval from the Bioethics Committee at the Wroclaw Medical University (No: 185/2022). Signed informed consent form was obtained from all study participants. The study complies with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. General Medical Council. Tomorrow’s Doctors. Recommendations on Undergraduate Medical Curriculum. London, UK: General Medical Council; 1993.
2. Simpson JG, Furnace J, Crosby J, et al. The Scottish doctor--learning outcomes for the medical undergraduate in Scotland: a foundation for competent and reflective practitioners. Med Teach. 2002;24(2):136–143. doi:10.1080/01421590220120713
3. Osler W. Aequanimitas: With Other Addresses to Medical Students, Nurses and Practitioners of Medicine. Philadelphia, PA: P. Blakiston’s Son & Company; 1910. doi:10.5962/bhl.title.2395
4. Belkin BM, Neelon FA. The art of observation: William Osler and the method of Zadig. Ann Intern Med. 1992;116(10):863–866. doi:10.7326/0003-4819-116-10-863
5. Simons RJ, Baily RG, Zelis R, Zwillich CW. The physiologic and psychological effects of the bedside presentation. N Engl J Med. 1989;321(18):1273–1275. doi:10.1056/nejm198911023211821
6. Linfors EW, Neelon FA. Sounding boards. The case of bedside rounds. N Engl J Med. 1980;303(21):1230–1233. doi:10.1056/nejm198011203032110
7. Chipp E, Stoneley S, Cooper K. Clinical placements for medical students: factors affecting patients’ involvement in medical education. Med Teach. 2004;26(2):114–119. doi:10.1080/01421590410001665636
8. Janicik RW, Fletcher KE. Teaching at the bedside: a new model. Med Teach. 2003;25(2):127–130. doi:10.1080/0142159031000092490
9. Langlois JP, Thach S. Teaching at the bedside. Fam Med. 2000;32(8):528–530.
10. Salam A, Perdaus AFM, Isa SHM, et al. UKM medical graduates’ perception of their communication skills during housemanship. Med Health. 2008;3:54–58.
11. Rider EA, Keefer CH. Communication skills competencies: definitions and a teaching toolbox. Med Educ. 2006;40(7):624–629. doi:10.1111/j.1365-2929.2006.02500.x
12. Ajab S, Pearson E, Dumont S, et al. An alternative to traditional bedside teaching during COVID-19: high-fidelity simulation-based study. JMIR Medical Education. 2022;8(2):e33565.
13. Ahmed M. What is happening to bedside clinical teaching? Med Educ. 2002;36(12):1185–1188. doi:10.1046/j.1365-2923.2002.01372.x
14. Atchley DW. The role of the patient in medical education. JAMA. 1963;185(5):396–398. doi:10.1001/jama.1963.03060050074025
15. Debyser B, Grypdonck MH, Defloor T, Verhaeghe ST. Involvement of inpatient mental health clients in the practical training and assessment of mental health nursing students: can it benefit clients and students? Nurse Educ Today. 2011;31(2):198–203. doi:10.1016/j.nedt.2010.06.001
16. McLachlan E, King N, Wenger E, Dornan T. Phenomenological analysis of patient experiences of medical student teaching encounters. Med Educ. 2012;46(10):963–973. doi:10.1111/j.1365-2923.2012.04332.x
17. Morgan A, Jones D. Perceptions of service user and carer involvement in healthcare education and impact on students’ knowledge and practice: a literature review. Med Teach. 2009;31(2):82–95. doi:10.1080/01421590802526946
18. Towle A, Bainbridge L, Godolphin W, et al. Active patient involvement in the education of health professionals. Med Educ. 2010;44(1):64–74. doi:10.1111/j.1365-2923.2009.03530.x
19. Sayed-Hassan RM, Bashour HN, Koudsi AY. Patient attitudes towards medical students at Damascus University teaching hospitals. BMC Med Educ. 2012;12(1):13. doi:10.1186/1472-6920-12-13
20. Haffling AC, Håkansson A. Patients consulting with students in general practice: survey of patients’ satisfaction and their role in teaching. Med Teach. 2008;30(6):622–629. doi:10.1080/01421590802043827
21. Halpern J. From idealized clinical empathy to empathic communication in medical care. Med Health Care Philos. 2014;17(2):301–311. doi:10.1007/s11019-013-9510-4
22. Halpern J. What is clinical empathy? J Gen Intern Med. 2003;18(8):670–674. doi:10.1046/j.1525-1497.2003.21017.x
23. Markakis K, Frankel R, Beckman H, Suchman A. Teaching empathy: it can be done. In: Annual Meeting of the Society of General Internal Medicine. San Francisco, CA: Society of General Internal Medicine; 1999.
24. Links AR, Callon W, Wasserman C, Walsh J, Beach MC, Boss EF. Surgeon use of medical jargon with parents in the outpatient setting. Patient Educ Couns. 2019;102(6):1111–1118. doi:10.1016/j.pec.2019.02.002
25. Schnitzler L, Smith SK, Shepherd HL, et al. Communication during radiation therapy education sessions: the role of medical jargon and emotional support in clarifying patient confusion. Patient Educ Couns. 2017;100(1):112–120. doi:10.1016/j.pec.2016.08.006
26. Hanusz Z, Tarasinska J, Zielinski W. Shapiro-Wilk test with known mean. Revstat Stat J. 2016;14(1):89–100. doi:10.57805/revstat.v14i1.180
27. McKnight PE, Najab J. Mann-Whitney U test. In: Weiner I, Craighead W, editors. The Corsini Encyclopedia of Psychology. Hoboken, NJ: John Wiley & Sons, Inc; 2010:1. doi:10.1002/9780470479216.corpsy0524
28. McKnight PE, Najab J. Kruskal-Wallis test. In: Weiner I, Craighead W, editors. The Corsini Encyclopedia of Psychology. Hoboken, NJ: John Wiley & Sons, Inc; 2010:1. doi:10.1002/9780470479216.corpsy0491
29. Kamata K, Kuriyama A, Chopra V, et al. Patient preferences for physician attire: a multicenter study in Japan. J Hosp Med. 2020;15(4):204–210. doi:10.12788/jhm.3350
30. Garus-Pakowska A. Estetyka higieniczna personelu medycznego. Probl Hig Epidemiol. 2015;96(2):510–516.
31. Henry SG, Fuhrel-Forbis A, Rogers MA, Eggly S. Association between nonverbal communication during clinical interactions and outcomes: a systematic review and meta-analysis. Patient Educ Couns. 2012;86(3):297–315. doi:10.1016/j.pec.2011.07.006
32. Collins A. Mowa Ciała: Co Znaczą Nasze Gesty? Warsaw, Poland: Rytm; 2002.
33. Martin CT, Chanda N. Mental health clinical simulation: therapeutic communication. Clin Simul Nurs. 2016;12(6):209–214. doi:10.1016/j.ecns.2016.02.007
34. Dean DH. Consumer perceptions of visible tattoos on service personnel. Manag Serv Qual Int J. 2010;20(3):294–308. doi:10.1108/09604521011041998
35. Cohen M, Jeanmonod D, Stankewicz H, Habeeb K, Berrios M, Jeanmonod R. An observational study of patients’ attitudes to tattoos and piercings on their physicians: the ART study. Emerg Med J. 2018;35(9):538–543. doi:10.1136/emermed-2017-206887
36. Sotgiu G, Nieddu P, Mameli L, et al. Evidence for preferences of Italian patients for physician attire. Patient Prefer Adherence. 2012;6:361–367. doi:10.2147/ppa.s29587
37. Yonekura CL, Certain L, Karen SKK, et al. Impressões de pacientes, médicos e estudantes de medicina quanto a aparência dos médicos. Rev Assoc Méd Bras. 2013;59(5):452–459. doi:10.1016/j.ramb.2013.04.005
38. Brodowska E, Burzyńska A, Gruszczyńska M. Wytatuowany personel medyczny z perspektywy pacjentów. Ann Univ Paedagog Crac Stud Psychol. 2018;11:150–158. doi:10.24917/20845596.11.10
39. Makoul G, Zick A, Green M. An evidence-based perspective on greetings in medical encounters. Arch Intern Med. 2007;167(11):1172–1176. doi:10.1001/archinte.167.11.1172
40. Wallace LS, Cassada DC, Ergen WF, Goldman MH. Setting the stage: surgery patients’ expectations for greetings during routine office visits. J Surg Res. 2009;157(1):91–95. doi:10.1016/j.jss.2009.03.065
41. Golz A, Kim A, Murphy M, Salazar D. Patient attitudes and preferences for orthopaedic surgeon greetings. J Am Acad Orthop Surg. 2021;29(3):e126–e131. doi:10.5435/jaaos-d-20-00230
42. Limon D, Perry S, Granot T, et al. ReCAP: perspectives of patients, caregivers, and medical staff on greetings in oncology practice: a prospective survey. J Oncol Pract. 2016;12(2):170–171; e188–e196. doi:10.1200/jop.2015.006049
43. Gil-Santos I, Santos CC, Duarte I. Medical education: patients’ perspectives on clinical training and informed consent. Int J Environ Res Public Health. 2022;19(13):7611. doi:10.3390/ijerph19137611
44. Tian J, Zhao JY, Xu JM, et al. Mobile phone addiction and academic procrastination negatively impact academic achievement among Chinese medical students. Front Psychol. 2021;12:758303. doi:10.3389/fpsyg.2021.758303
45. Augustowska-Kruszyńska K, Kruszyńsk P, Kruszyński G, Pabiś M. Smartfon w rękach studentów pielęgniarstwa–złodziej czasu czy niezbędny gadżet? [Smartphone in the Hands of Nursing Students - a Time Thief or a necessary Gadget?] Wyzwania Wspólczesnego Pielegniarstwa; 2021:127.
46. Nieto-Carhuamaca A, Castañeda-Japan J, Dámaso-Mata B, Panduro-Correa V, Arteaga-Livias K. Bacterial resistance in cell phone cultures of medical students. Infez Med. 2019;27(4):374–379.
47. Miller AN, Bharathan A, Duvuuri VNS, et al. Use of seven types of medical jargon by male and female primary care providers at a university health center. Patient Educ Couns. 2022;105(5):1261–1267. doi:10.1016/j.pec.2021.08.018
48. Charpentier V, Gotlieb R, Praska CE, Hendrickson M, Pitt MB, Marmet JSW. Quantifying and classifying jargon use during inpatient rounds. Hosp Pediatr. 2021;11(4):406–410. doi:10.1542/hpeds.2020-002790
49. LeBlanc TW, Hesson A, Williams A, et al. Patient understanding of medical jargon: a survey study of U.S. medical students. Patient Educ Couns. 2014;95(2):238–242. doi:10.1016/j.pec.2014.01.014
50. Lill MM, Wilkinson TJ. Judging a book by its cover: descriptive survey of patients’ preferences for doctors’ appearance and mode of address. BMJ. 2005;331(7531):1524–1527. doi:10.1136/bmj.331.7531.1524
51. Elias SMS. Prevalence of loneliness, anxiety, and depression among older people living in long-term care: a review. Int J Care Sch. 2018;1(1):39–43. doi:10.31436/ijcs.v1i1.44
52. Mullen RA, Tong S, Sabo RT, et al. Loneliness in primary care patients: a prevalence study. Ann Fam Med. 2019;17(2):108–115. doi:10.1370/afm.2358
53. Crosby JF. Karol Wojtyla on treating patients as persons. In: Tollefsen C, editor. John Paul Ii’s Contribution to Catholic Bioethics. Dordrecht, Netherlands: Springer; 2004:151–168.
54. Decety J. Empathy in medicine: what it is, and how much we really need it. Am J Med. 2020;133(5):561–566. doi:10.1016/j.amjmed.2019.12.012
55. Hayes V, Bing-You R, Pitts D, Manning L. The benefits of honoring patients as teachers: a qualitative study. PRiMER. 2018;2:4. doi:10.22454/PRiMER.2018.242345
56. Beltran-Aroca CM, Ruiz-Montero R, Labella F, Girela-López E. The role of undergraduate medical students training in respect for patient confidentiality. BMC Med Educ. 2021;21(1):273. doi:10.1186/s12909-021-02689-6
57. Terán AÁ, Palazuelos C, Dierssen-Sotos T, Alonso-Molero J, Llorca J, Gómez-Acebo I. Evolution of medical students’ perception of the patient’s right to privacy. Int J Environ Res Public Health. 2022;19(17):11067. doi:10.3390/ijerph191711067
58. Hosseini-Ghavam-Abad L, Asghari F, Bandehagh A, Najafipour S, Bigdeli S. Patient privacy: awareness and attitudes of Iran University of Medical Sciences medical students. Med J Islam Repub Iran. 2019;33:12. doi:10.34171/mjiri.33.12
59. Vaughn JL, Rickborn LR, Davis JA. Patients’ attitudes toward medical student participation across specialties: a systematic review. Teach Learn Med. 2015;27(3):245–253. doi:10.1080/10401334.2015.1044750
60. Monnickendam SM, Vinker S, Zalewski S, Cohen O, Kitai E. Patients’ attitudes towards the presence of medical students in family practice consultations. Isr Med Assoc J. 2001;3(12):903–906.
61. Mwaka AD, Taremwa S, Adoch W, et al. Patients’ attitudes towards involvement of medical students in their care at university teaching hospitals of three public universities in Uganda: a cross sectional study. BMC Med Educ. 2022;22(1):519. doi:10.1186/s12909-022-03576-4
62. Huang CC, Huang CC, Yang YY, Lin SJ, Chen JW. The influence of gender on the communication skills assessment of medical students. Eur J Intern Med. 2015;26(9):670–674. doi:10.1016/j.ejim.2015.06.017
63. Ravishankar S. Are patients comfortable with medical students examining them? Indian J Med Ethics. 2022;VII(1):1–4. doi:10.20529/IJME.2021.038
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.