")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Patient Experience Pre-Implementation of an Enhanced Recovery After Surgery Protocol: A Qualitative Investigation
Authors Poletti B, Stringer G, Furness K
Received 5 December 2023
Accepted for publication 19 February 2024
Published 14 March 2024 Volume 2024:17 Pages 1147—1158
DOI https://doi.org/10.2147/JMDH.S453467
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Bianca Poletti,1 Georgia Stringer,2 Kate Furness3,4
1Faculty of Health Science (Biomedical Science), Swinburne University of Technology, Hawthorn, Victoria, 3122, Australia; 2Department of Nutrition and Dietetics, Eastern Health, Melbourne, Australia; 3Department of Nursing and Allied Health, Swinburne University of Technology, Hawthorn, Victoria, 3122, Australia; 4Department Sport, Exercise and Nutrition Sciences, School of Allied Health, Human Services and Sport, La Trobe University, Bundoora, Victoria, 3086, Australia
Correspondence: Kate Furness, La Trobe University, Department of Sport, Exercise and Nutrition Sciences, School of Allied Health, Human Services and Sport, Bundoora, Victoria, 3086, Australia, Email [email protected]
Objective: This study explores the experience of adults undergoing major abdominal surgery pre-implementation of an Enhanced Recovery after Surgery program at a tertiary hospital in Melbourne, Australia, to enhance health promotion in Australian hospitals.
Methodology: Patients who were undergoing major abdominal surgery and who consented to participate were recruited in this study. Patients were chosen based on an inclusion-exclusion criterion. In-depth, semi-structured qualitative interviews were conducted by telephone and transcribed verbatim by the primary researcher. Thematic analysis was used and synthesised into five inductive themes. Eighteen participants aged between 51 and 82 years were interviewed. Codes were categorised into inductive themes: 1) preparedness for surgery; 2) communication; 3) aftercare; 4) expectations of surgery; and 5) overall experience utilising an iterative process. The following themes and subthemes emerged from the qualitative synthesis.
Results: Patients undergo a variety of experiences throughout the perioperative care period. Patient care and experience may be improved through increased access to patient engagement, information and communication, use of multimedia and teach-back method, optimization of the hospital environment and through providing adequate planning and support on discharge.
Conclusion: Evidence of barriers to enhancing patient surgical experience can be used to guide the implementation of Enhanced Recovery after Surgery protocols in Australian hospitals and therefore may limit its generalizability. This will improve health promotion as these findings provide valuable insights into integrative methods that can be considered to be important for achieving person-centred care. This knowledge can be useful in clinical practice, implementation and education programs for ERAS.
Keywords: patient care, perioperative care, patient engagement, communication, surgery
Introduction
Enhanced Recovery after Surgery (ERAS) protocols are evidenced-based frameworks that aim to reduce morbidity and mortality.1 ERAS programs are founded on a well-built multidisciplinary team who work collaboratively to coordinate optimal compliance with each step of the protocol. Preoperative counselling, early mobilisation, early feeding and optimal pain control represent a few of the key steps within an ERAS pathway. When combined, these steps help to expedite recovery and decrease the length of hospital stay.2 Partnering with patients is a fundamental component to delivering patient-centred care. ERAS programs promote increased patient participation and increased engagement with the multidisciplinary team.3 Early pre-operative counselling and prehabilitation is recommended to ensure that the patient is provided with an opportunity to prepare physically and psychologically before surgery.
Patient experience is a measure of quality of care that encompasses interactions between patients and the health system.4 Features of patient experience include the healthcare environment, care experiences, clinical interactions, and organisational features of care and process measures.5 The ‘sum of all interactions’ refers to the dynamic interaction of features that comprise patient experience as a whole.5 ERAS pathways comprise elements that may improve patient experience, such as an increase in counselling and an earlier return to the home environment.
Despite the clear benefits to patients and the broader healthcare system, there has been a slow uptake of ERAS protocols in Australia. Lack of resourcing, resistance to change and external factors are barriers to implementation of ERAS in Australian hospitals.6 Each healthcare setting comprises its own set of resources that may be used to overcome unique organisational barriers. A motivated group of clinicians is essential to gather momentum and drive sustainable change towards embracing ERAS in the long term.7 Partnering with consumers in the design and implementation of change in healthcare is endorsed by the Australian Commission on Safety and Quality in Healthcare.8 Consumers are instrumental in the development of ERAS pathways that meet the needs of the patient.
Previous research has investigated patient experience in early mobilisation after abdominal surgery. Findings demonstrate that patients will ‘do what it takes’ to get home sooner after surgery and that patients were motivated to improve their physical and mental wellbeing.9 Other research demonstrates varying satisfaction with ERAS programs, with better access to information and aftercare identified as areas for improvement.10 Peer support and clearer explanations of ERAS protocols were identified by participants as important.11 These varying findings support the need for consumer involvement in the development of tailored ERAS programs that suit a given environment. Most qualitative literature on patient experience and ERAS programs exists internationally, which is unsurprising given the lack of uptake of ERAS in Australia. A follow-up qualitative investigation of post-implementation patient experience will be conducted post implementation of the ERAS protocol. The aim of this research was to investigate the experience of adults undergoing major elective abdominal surgery pre-implementation of an ERAS program at a tertiary hospital in Melbourne, Australia. The findings may be used to support hospitals in developing suitable ERAS programs in Australian hospitals.
Methods
A single-centred study was conducted throughout 2022 at Eastern Health, Melbourne, Australia. Qualitative, semi-structured interviews were undertaken with patients post major abdominal surgery to explore the breadth of patient experience throughout their surgical journey. The types of abdominal surgeries conducted include those of the target digestive organs, including the stomach, small and large bowel, pancreas, liver, spleen, biliary tract and gallbladder.12 This methodology adopted a subjective paradigm to understand patient values, beliefs, and experiences during their surgical journey.13,14
Purposive sampling was used to recruit participants based on the expectation that their surgical experiences would provide detailed and unique responses.15 Consecutive patients undergoing major abdominal surgery that fulfilled the inclusion criteria (refer to Table 1) were considered eligible to participate in this study.
 |
Table 1 Inclusion and Exclusion Criteria |
Major abdominal surgeries have been defined as, but are not limited to, pancreaticoduodenectomy, oesophagectomy, total and subtotal gastrectomy, stoma revision, reversal or formation, high anterior large bowel resection, low anterior large bowel resection, proctosigmoidectomy, colectomy, subtotal colectomy, splenectomy, liver resection, hepatectomy, and pancreatectomy. A consensus definition of abdominal surgery was determined by two senior gastrointestinal surgical dietitians.
A daily nursing handover list was used to identify eligible participants to approach for consent to the study. The primary researcher was trained to identify eligible participants through training with a senior gastrointestinal surgery dietitian.
The primary researcher was a Health Science honours student at a public university in Melbourne with no prior knowledge of ERAS protocols. The duration of this qualitative investigation started in March and was finalized in September 2022. The primary researcher conducted this study as an outsider. There was little knowledge about ERAS and therefore a low emotional investment. The outsider positioning was used as an advantage during the initial face-to-face meeting to inherit a trust and sense of security.
Standardised interview questions were developed prior to commencement of interviews to improve rigor in data collection. Pilot studies were conducted with two patients who were external to the study to refine interview questions. This was done to train the primary interviewer to respond to the diverse and emotive responses anticipated from participants.16 Pilot studies were also used to refine the questions and prompts. A wide variety of participants across surgical units and different major abdominal surgeries, of varied gender and age, increased the dependability of the data collection. Verbatim transcription of interview audio recordings and data analysis verification by a blinded secondary and tertiary author supported accuracy and reliability.
Participants were approached face-to-face on the surgical ward by the primary researcher with a patient information statement (PIS). Participants were given time to read, discuss and ask any questions they had prior to giving written consent. Patients were informed that they could withdraw consent at any time during the study, including during the interview. Participants who provided informed consent also understood and consented to having their anonymized responses published.
An interview guide was developed by the tertiary researcher with review and refining by the secondary researcher (Table 2). These questions were used to guide participants to share and reflect on their surgical experiences. Simplified/unbiased prompts were used to clarify any confusion or misunderstandings with the questions at hand and/or were used to elicit more in-depth responses.16 Field notes were made during the interviews so that the primary researcher could reflect on the interviews. Interviews were conducted between April and June 2022 for the use of primary data. Participants were recruited at a single tertiary metropolitan Melbourne hospital. One-on-one participant telephone interviews occurred within two weeks of their hospital discharge. Interviews ran between 7 and 42 minutes and no repeat interviews were carried out. Transcripts were not returned to participants.
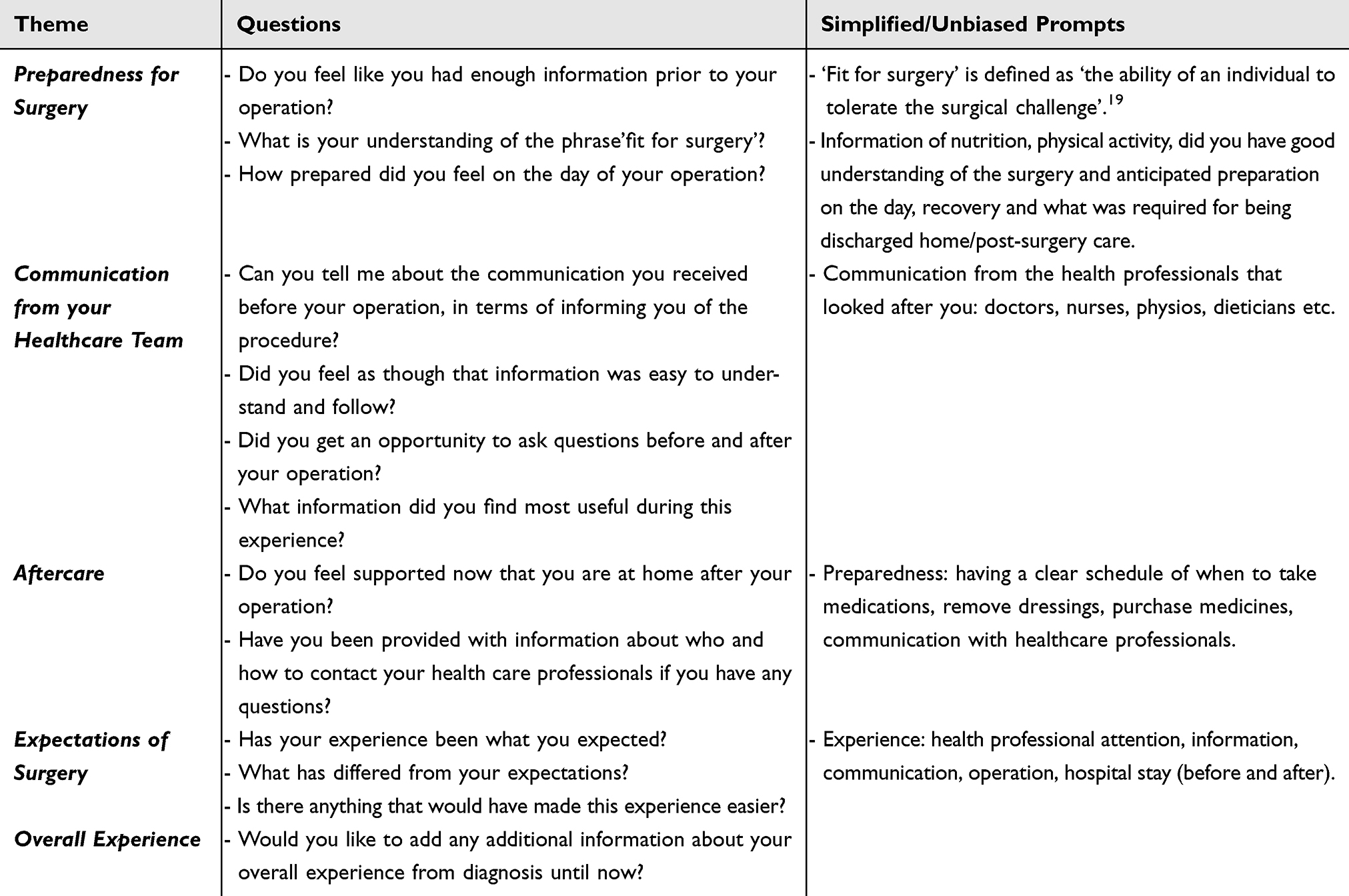 |
Table 2 Interview Questionnaire17 |
All interviews were recorded, uploaded to a secure cloud-based repository, and then removed from the audio device. The interviews were deidentified using a unique study identification number (USIN) and transcribed verbatim.
Local Eastern Health service ethics was approved (HREC: LR22-003-80774). The institutional board was also sought and approved (HREC: 20226380–9442). This study complied with the Declaration of Helsinki.
Thematic analysis was chosen as a framework to assist with robust coding and constructing themes from the interview data to accurately reflect the patterns across the data set: patient experience.17 Descriptive phenomenology was used to clarify and understand the themes of patient experience. The data analysis framework was based on the five domains from the interview questionnaire: 1) preparedness for surgery; 2) communication; 3) aftercare; 4) expectations of surgery; and 5) overall experience (Table 2).
Hand coding in Microsoft Excel was used to analyse the raw interview data, with the primary researcher completing the initial coding into inductive themes. All the data generated from the participants’ interviews were reviewed utilising a cyclical and iterative process such that no important details were omitted. Two researchers hand coded one blinded transcript into codes and categorised into inductive themes. The research team met to discuss the accuracy of code categorisation into themes until a consensus was reached. This allowed careful re-examination of the data.
Results
Twenty-one participants consented to be interviewed, and a total of 18 interviews were completed, providing a total response rate of 86%. There were two participants who were unable to be contacted via telephone despite consenting to be contacted for interviews, and these participants were non-responders. One participant subsequently withdrew their initial consent to participate (Figure 1).
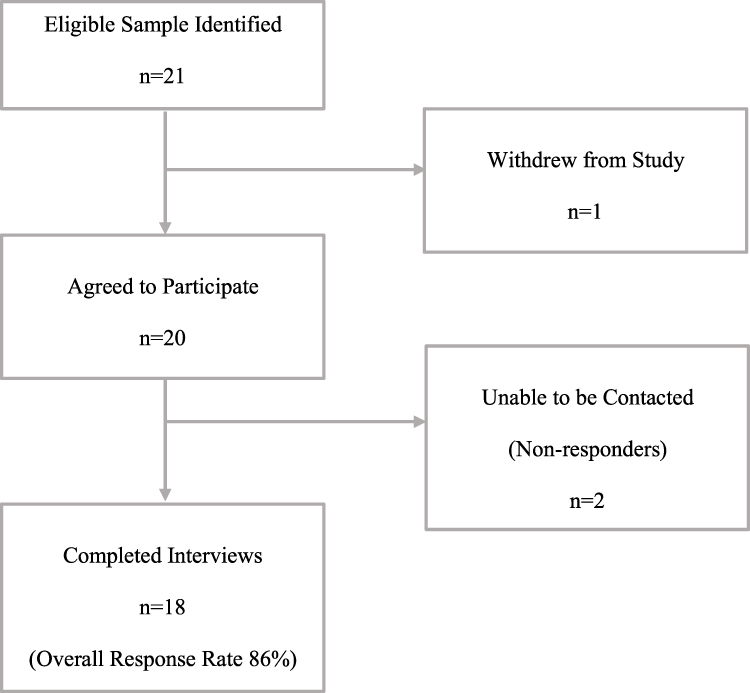 |
Figure 1 Interview Samples. |
Sample size was determined by information power, a tool described by Malterud et al.18 Information power is relevant to this study as the number of participants was based on the depth and relevance of the information provided. Therefore, a lower number of participants were used because the information provided by the sample was ample and held adequate power.18
Eighteen participants were interviewed (five women and 13 men, aged between 51 and 82 years) with a mean age of 66 years. Thirteen participants were patients managed under the colorectal unit, and five participants were managed under the upper gastrointestinal unit. Ten participants had a confirmed cancer diagnosis (four pancreatic and six colorectal), shown in Table 3: Demographic information of Interview participants.
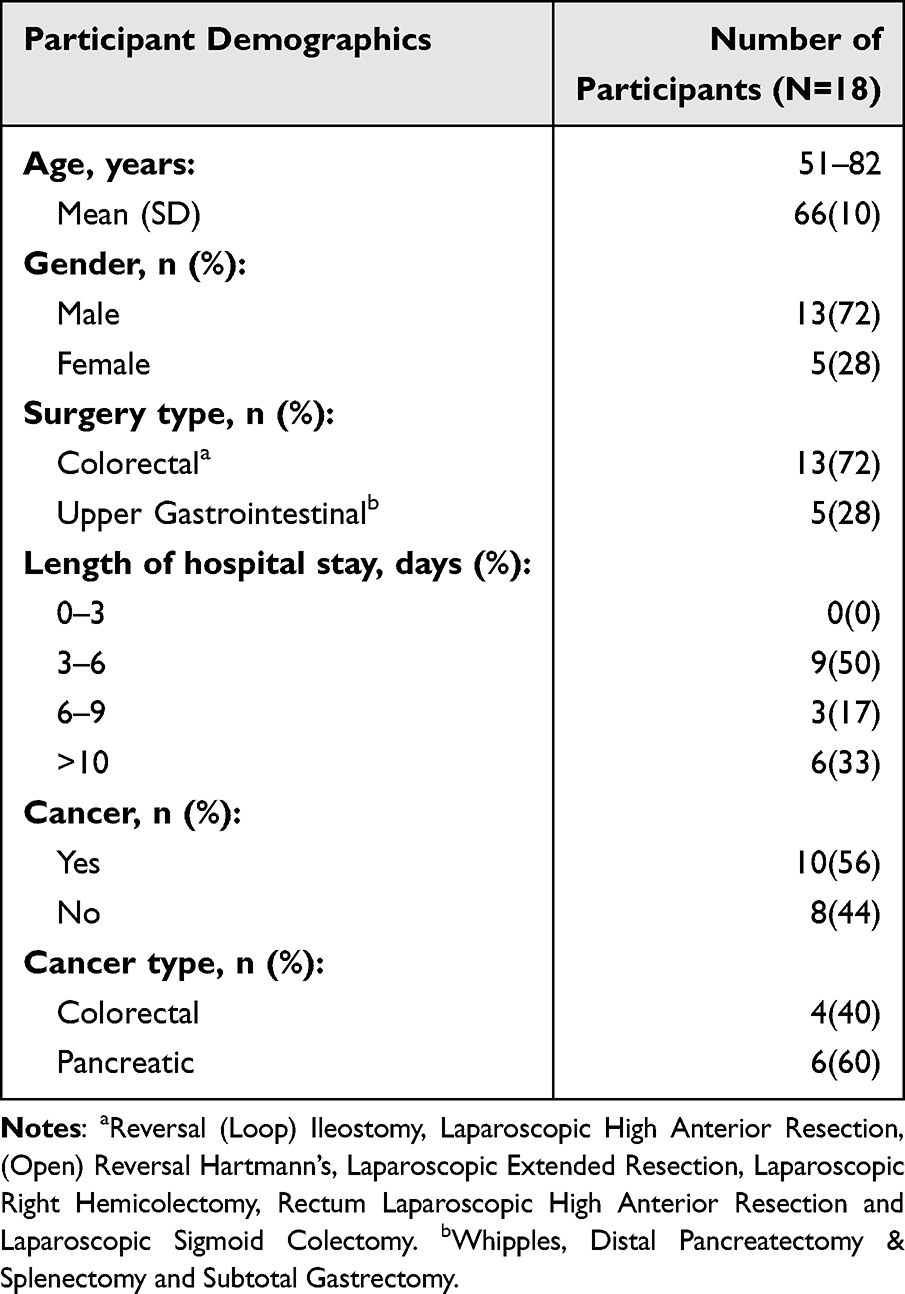 |
Table 3 Demographic Information of Interview Participants |
A variety of methods of information sharing and knowledge acquisition are required for patient preparedness for surgery.
Overwhelmingly, participants reported that they were prepared for their surgery with good communication of what was required of them, that messaging between clinicians was echoed and that both verbal and written mediums were used to confer this information with visual and verbal cues. Participants felt that healthcare professionals reassured them when they disclosed their anxieties about their upcoming surgery. Results are shown in Table 4: Themes and Subthemes.
Umm very prepared…they sort of make recommendations, but I was aware of what was going to happen. They made me aware of what was going to happen [Participant 12, male, 65]
I did get a backup from my GP and he echoed what he (the surgeon) said. I was like a lot more comfortable [Participant 11, male, 65]
 |
Table 4 Qualitative Analysis: Themes and Subthemes |
Participants who felt that they were not prepared for their surgeries reported mixed messages creating confusion and poor communication, either verbal or written, with inadequate time provided to grasp complex concepts and ask questions. Whilst some participants reported that they may have been able to ask questions, they were unable to articulate what they needed to ask, know or understand. Results are shown in Table 4: Themes and Subthemes.
You don’t really understand any of it… as soon as you’re introduced to cancer you start learning and hearing a lot of words you haven’t heard before. [Participant 8, male, 59]
Yes, but of course, you get an opportunity, but you’re lost at that time. Things are not going well; you just feel like you’re lost. [Participant 7, male, 58]
All of the information has been very confusing, very limited. Yes, I understand that you do not want to give too much information so that would confuse people, but I do feel they need a little bit more than what was actually given out [Participant 2, female, 62]
Participants on the whole were not provided with any detail on the physical and metabolic requirements of surgical preparation such as physical activity or nutrition and were required to be fasted from midnight. Results are shown in Table 4: Themes and Subthemes.
No information about nutrition, physical activity… I didn’t get a good understanding on anticipated preparation. [Participant 2, female, 62]
Timeliness was a challenge, where patients saw their clinicians a long way in advance of their actual scheduled surgery. This significant time lapse meant that patients often forgot important information that was previously provided to them. Results are shown in Table 4: Themes and Subthemes.
I saw the surgeon on the 5th of January, and he went through as much as he possibly could in the limited time. But that was such a long time away from when I actually had my surgery... that was 5 months oh, 4 or 5 months that you tend to forget it. [Participant 2, female, 62]
Prior experience either in hospital or with another surgery assisted with participants preparation of and setting expectations for their recovery. Results are shown in Table 4: Themes and Subthemes.
Oh, what I expected, definitely. I have been in Box Hill before. I know what to take, what to make me comfortable and to make my stay a lot easier. I expected it because I had been a patient before [Participant 2, female, 62]
Many participants recognised that they need to play a role in their preparation with self-education and advocacy, with health professionals being key to improving their knowledge and actualising self-management, including in the postoperative period.
I think that I was not aware, and I think that’s my own fault. The information is all there on the internet. I think I could’ve been given more information… but I’m hesitant to complain because if they’re on the internet you really should use your own mouse [Participant 3, male, 82]
These participants found information and support through a variety of mediums including Facebook cancer support groups, the internet, and printed documents. Results are shown in Table 4: Themes and Subthemes.
…I know cancer groups on Facebook. I found that I got my knowledge through those, through other people who have been through it themselves or carers and stuff…I just ask questions in my group and you know, people answer it. [Participant 8, male, 59]
Postoperative information, time, care, and attention are required for patient understanding and recovery. Most participants reported that there could have been improvements in the provision of the postoperative care by nurses, medical staff and other ward staff. Being woken by surgical ward rounds disrupted their ability to process and understand information, often having questions that were thought of later. Some started preparing for these interactions the day before, writing down questions that were important to them and that they did not want to forget. Results are shown in Table 4: Themes and Subthemes.
Especially if they come in the morning and I guess, you are just waking up as well. For some patients who are not going to be fully awake, I guess, understand what they are going to say because you’ve just woken up. [Participant 2, female, 62]
These patients acknowledged the time pressures that health professionals were facing, noting that often caring for demanding or complex patients took time away from them. Many expressed a feeling that they could not or should not bother staff as they were too busy to attend to their needs including showering, toileting, and pain management. Results are shown in Table 4: Themes and Subthemes.
Umm, nurses were lovely umm, I could tell in their eyes that they were under the pump. Umm, they were under a lot of stress, which I thought was pretty ordinary. Umm, they’re understaffed so I left them alone as much as I could. [Participant 16, male, 54]
A number of participants also described a feeling that they were not an individual with individual needs. They described knowledge of patient-centred care and the idea that they should have been respected, consulted, and actively allowed to participate in decision-making about their care. Results are shown in Table 4: Themes and Subthemes.
Like to me, I was a number and not a person. [Participant 1, female, 62]
And the person, the person-centred idea was very distant. [Participant 13, male, 52]
Some participants reported that they were not provided with adequate information about their postoperative course, especially where complications arose. They described feeling that they had to press for information to aid in their understanding and reduce their concerns about their trajectory. Results are shown in Table 4: Themes and Subthemes.
I felt that they weren’t answering my questions. And I really had to push for information about what they were concerned about. [Participant 13, male, 52]
Recuperation at home requires comprehensive discharge planning and post-discharge support. Results are shown in Table 4: Themes and Subthemes.
Half of the participants reported that they felt that they were well prepared to be discharged from hospital and understood how to manage their postoperative wounds and potential symptoms and complications. These participants reported that they had abundant contact with their healthcare team post discharge and were provided with instructive written information with follow-up appointments made and clearly documented for them. Having contact details of someone to call if things were not going well was important to reassure participants that they could get help whenever they required it. Written information was also useful to refer to and assist with aftercare requirements such as dressing removals and medication management. Results are shown in Table 4: Themes and Subthemes.
I have got their number for the colorectal department and the number for the Box Hill hospital, and they said if I have any troubles or if I feel really crook or if it gets infected to just give them a ring. [Participant 10, male, 60]
I had to go back on a couple of occasions (to the written information) to make sure that those little things were adhered to as per the information they gave me before I departed from the hospital. [Participant 11, male, 65]
The other half of participants reported that support from clinicians post discharge was poor, with a feeling of having to fend for yourself, not having any contact details of any healthcare professional and feeling unsure of what to do if they had any concerns. One participant expressed concern that he could not discuss his displeasure around his discharge due to being worried about this impacting on his future care. Results are shown in Table 4: Themes and Subthemes.
The only one is that really is the one that when you get sent home and then you are just left to flounder, and you don’t know what’s going on. Like I get sent home with a hole, you know a 35mm diameter hole in my stomach [Participant 8, male, 59]
It finishes and then you just go home, and you like, and now what?. [Participant 8, male, 59]
I left the hospital without a report, I left the hospital without bandages. That’s how angry I am, then you have to go face them and put a happy face because you don’t want to cause trouble or get shifted back. [Participant 7, male, 58]
Mixed feelings were reported about the ability of the participants general practitioner (GP) being able to assist and manage their recovery postoperatively. Results are shown in Table 4: Themes and Subthemes.
I get more information from my local GP than my own doctor. [Participant 7, male, 58]
… if I go to my GP, she won’t have a clue. [Participant 2, female, 62]
Hospital systems and the environment directly affected patient experience. The COVID-19 pandemic (COVID) and the strict hospital requirements regarding no visitors impacted patients significantly with many expressing distress and loneliness. They also reported limited time with their healthcare team intensified these feelings and some felt a decline in previously good mental health, and this was perceived to have made their recovery more difficult and prolonged. Results are shown in Table 4: Themes and Subthemes.
It’s the loneliest feeling you’ll ever have, and it not only affects me, but it affects my partner. [Participant 7, male, 58].
Only the lack of being able to have visitors… and maybe a little more one to one contact with staff. An extra 10 minutes a day. [Participant 3, male, 82]
COVID also created significant delays in timeliness to care, particularly surgeries, where category two and three surgeries were cancelled in Victoria for months on end, creating a backlog of cases. Results are shown in Table 4: Themes and Subthemes.
It’s probably the waiting period that I had to wait when diagnosed from 2020… to get operated on in 2022. [Participant 12, male, 65]
The hospital environment and services including cold air conditioning, noise, and staff disruptions (particularly when sleeping), food choices and requirement to pay for television were discussed as areas for improvement to enhance their overall experience. Some people reported that these challenges directly impacted on their recovery. Results are shown in Table 4: Themes and Subthemes.
The thing I really hate about hospitals is that air conditioners are on 24/7. I’ve left the hospital shaking and basically my body temperature for the last 2 weeks has not been able to stabilise. [Participant 7, male, 58]
Several participants discussed the idea of an individual who could act as an advisor, information provider or guide throughout their journey. Some reported that this person could have also provided them with much-needed company due to long periods of isolation. Results are shown in Table 4: Themes and Subthemes.
They just need one person to go around and be that mmm I guess that information person. [Participant 2, female, 62]
Other participants described a sense of gratitude for being looked after well by their healthcare team and the hospital, noting that it was a public hospital and that they were getting high-quality care for free. Results are shown in Table 4: Themes and Subthemes.
I have no complaints, Box Hill Hospital, they’ve got the sweetest staff on earth in that place, I think. I really do. I’ve got not one complaint. [Participant 8, male, 59]
The whole system works quite well I think for a public patient it’s pretty good and the hospital is always clean. [Participant 15, male, 69]
Discussion
The surgical journey of patients undergoing major abdominal surgeries at a tertiary hospital in Melbourne, Australia, was explored in this study, with a focus on their overall experience. Patients described a myriad of positive and negative experiences of the pre, peri and postoperative period, of both the health system and the health professionals working within it. In preparation for surgery, patients required a variety of different information and knowledge acquisition methods, both verbal and written, delivered to them synchronously, either face-to-face or via telephone. During the postoperative period, patients felt a need for ongoing communication of their progress in a timely manner, to be cared about and for concerns to be discussed with them to allow effective recovery. Discharge planning communication and preparation with the patient needed to begin early to enhance efficacy of self-management.
Patients who had prior experience in hospitals felt as though they knew what to expect and were more comfortable in asking and discussing concerns during health professional consultations. Conversely, participants who had not had previous experience expressed a lack of understanding felt overwhelmed, lost, and unprepared preoperatively when they experienced mixed messages and perceived lack of time to ask questions. The feeling of unpreparedness can cause anxiety and may therefore delay postoperative recovery.19 Good communication integrates both patient- and doctor-centred strategies, comprising shared perceptions regarding the problem, treatment objectives, and psychological support.19
A health professional’s interpersonal, and communication aptitude encompasses the ability to translate information to patients.20 This facilitates an accurate diagnosis, effective counselling, provides them with treatment instructions and builds trusting relationships with them.20 The human mind can neglect certain information when in stressful situations.21 To improve recollection, patients need structured, easy to understand information provided verbally along with written and visual cues.22 This may include educational tools like the teach back method to ensure comprehensibility of delivered information, improving patient understanding, engagement, and limiting forgetfulness of information from the duration of wait time from diagnosis to surgery.23
Participants described that they had to “fend for themselves”, had no support, and felt lonely, much of which was directly related to the strict hospital protocols of COVID, where no visitors were allowed to ensure patient safety during the conduct of this study.24 Timeliness of care reduces anxiety and enhances patient preparation, patient satisfaction and lowers LOS.25 A key nurse contact or patient care navigator (PCN) may be a valuable patient advocate assisting transference of information, act as a liaison between health professionals and families, and enable better access to a range of health and social care services.26,27
Established systems embedded into hospitals like early morning surgical ward rounds, and standard food and fluid delivery with lack of mealtime assistance significantly impacted a patient’s stay in hospital. Noise, ward lighting, and interference from health professionals and other patients disturbed sleep, which can lead to an adverse surgical recovery.28 Adopting protected mealtimes and/or on-demand food service systems ensures adequate, supported meals and snacks while designated rest periods with low lighting and noise allow for sleep and recuperation.29
There are several limitations to our study that should be considered. To reduce the impact of measurement bias, the primary researcher was rigorously trained in interviewing techniques from piloting to detect flaws in the interview questions.30 Anonymity from telephone interviews may have reduced patient bias and therefore elicited increased truthfulness.31 This study was conducted at one tertiary metropolitan Melbourne hospital with those from a primarily English-speaking background. This may limit its generalizability to other hospitals in Australia and globally, as well as to other surgical cohorts.
Conclusion
There is an impetus for Australian hospitals to focus on the rapid expansion and implementation of ERAS protocols to improve patient experience, morbidity, and mortality. Evidence of barriers to a positive patient experience from this study can be used to enhance tailored implementation of ERAS protocols. Alongside the mitigation of current system and health professional barriers, ERAS champions are required to enable the long-term sustainability of ERAS protocols.
Relevance for Clinical Practice
The findings provide valuable insights into integrative methods from patient experience that can be considered to be important for achieving person-centred care. This knowledge can be useful in clinical practice, implementation and education programs for ERAS.
Key Points
- This study explored patient experience throughout the perioperative period prior to the implementation of an Enhanced Recovery after Surgery Program, using qualitative methods.
- Key areas of focus for improving patient care and experience were identified, including increased access to patient engagement, information and communication, use of multimedia and teach-back methods, optimisation of the hospital environment and through adequate support on discharge.
- Results from this study provide valuable insights on patient experience and may be useful in the implementation of Enhanced Recovery after Surgery programs by other hospitals.
Abbreviation
ERAS, Enhanced recovery after surgery; LOS, Length of stay; PCN, Patient care navigator.
Ethics
Eastern Health Human Ethics committee approval (HREC: LR22-003-80774). Swinburne University of Technology ethics was also sought and approved (HREC: 20226380-9442).
Statement of Authorship
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas, took part in drafting, revising or critically reviewing the article, gave final approval of the version to have published, have agreed on the journal to which the article has been submitted and agreed to be accountable for all aspects of the work.
Acknowledgments
We thank the participants and the dietetics department at Eastern Health. This work was supported by Swinburne University of Technology and Eastern Health.
Funding
There is no funding to report.
Disclosure
All authors declare that they have no known financial or interpersonal conflicts that would have appeared to have an impact on the research presented in this work.
References
1. Kehlet H. Multimodal approach to control postoperative pathophysiology and rehabilitation. Br J Anaesth. 1997;78(5):606–617. doi:10.1093/bja/78.5.606
2. Ni X, Jia D, Guo Y, Sun X, Suo J. The efficacy and safety of enhanced recovery after surgery (ERAS) program in laparoscopic digestive system surgery: a meta-analysis of randomized controlled trials. Int J Surg. 2019;69:108–115. doi:10.1016/j.ijsu.2019.07.034
3. Graffigna G, Barello S. Patient Health Engagement (PHE) model in enhanced recovery after surgery (ERAS): monitoring patients’ engagement and psychological resilience in minimally invasive thoracic surgery. J Thoracic Dis. 2018;10(4):517–528. doi:10.21037/jtd.2017.12.84
4. Wolf JA, Niederhauser V, Marshburn D, LaVela SL. Defining patient experience. Patient Experience j. 2014;1(1):7–19.
5. Larson E, Sharma J, Bohren MA, Tunçalp Ö. When the patient is the expert: measuring patient experience and satisfaction with care. Bulletin World Health Org. 2019;97(8):563.
6. Duff J. Enhanced recovery after surgery in Australia: a classic example of an evidence–practice gap. J Perioperative Nursing. 2020;33(4):1–2.
7. Kahokehr A, Sammour T, Zargar-Shoshtari K, Thompson L, Hill AG. Implementation of ERAS and how to overcome barriers. Int j Surg. 2009;7(1):16–19. doi:10.1016/j.ijsu.2008.11.004
8. Australian Commission on Safety and Quality in Health Care. Safety and Quality Improvement Guide Standard 2: Partnering with Consumers. Sydney: ACSQJHC; 2012.
9. Svensson-Raskh A, Schandl A, Holdar U, Fagevik OM, Nygren-Bonnier M. I have everything to win and nothing to lose: patient experiences of mobilisation out of bed immediately after abdominal surgery. Physical Therapy. 2020;100(12):2079–2089. doi:10.1093/ptj/pzaa168
10. Blazeby JM, Soulsby M, Winstone K, King PM, Bulley S, Kennedy RH. A qualitative evaluation of patients’ experiences of an enhanced recovery programme for colorectal cancer. Colorectal Dis. 2010;12(10):236–242. doi:10.1111/j.1463-1318.2009.02104.x
11. Gillis C, Gill M, Marlett N, et al. Patients as partners in enhanced recovery after surgery: a qualitative patient-led study. BMJ open. 2017;7(6):1–10. doi:10.1136/bmjopen-2017-017002
12. Chai T, Tsang JG, Bruel BM. Cancer-Related Abdominal Pain. Chronic Abdominal Pain. 2015. doi:10.1007/978-1-4939-1992-5_13
13. Williamson K, Bernath V, Wright S, Sullivan J. Research students in the electronic age: impacts of changing information behavior on information literacy needs. Commun Information Literacy. 2008;1(2):46–63. doi:10.15760/comminfolit.2008.1.2.9
14. Fassinger RE. Paradigms, praxis, problems, and promise: grounded theory in counseling psychology research. J Counseling Psychol. 2005;52(2):156–166. doi:10.1037/0022-0167.52.2.156
15. Etikan I, Musa SA, Alkassim RS. Comparison of Convenience Sampling and Purposive Sampling. Am j Theoretic Appl Stat. 2016;5(9):1–4. doi:10.11648/j.ajtas.20160501.11
16. Bourgeault I, Dingwall R, De Vries RG. Qualitative interviewing techniques and styles. In: The SAGE Handbook of Qualitative Methods in Health Research. Sage Publications Ltd; 2010:307–326.
17. Braun V, Clarke V. What can “thematic analysis” offer health and wellbeing researchers? Int j Qualitative Studies Health Well-Being. 2014;9(1):1–2. doi:10.3402/qhw.v9.26152
18. Malterud K, Siersma VD, Guassora AD. Sample size in qualitative interview studies: guided by information power. Qualitative Health Res. 2016;26(13):1753–1760. doi:10.1177/1049732315617444
19. Dawdy K, Bonin K, Russell S, et al. Developing and evaluating multimedia patient education tools to better prepare prostate-cancer patients for radiotherapy treatment (randomized study). J Cancer Educ. 2018;33(3):551–556. doi:10.1007/s13187-016-1091-5
20. Ha JF, Longnecker N. Doctor-patient communication: a review. Ochsner J. 2010;10(1):38–43.
21. Hughes J. Denial in Cancer Patients. In: Coping with Cancer Stress. Springer; 1986:63–66.
22. Samuels-Kalow ME, Stack AM, Porter SC. Effective discharge communication in the emergency department. Ann Emergency Med. 2012;60(2):152–159. doi:10.1016/j.annemergmed.2011.10.023
23. Anderson KM, Leister S, De Rego R. The 5Ts for teach back: an operational definition for teach-back training. Health Literacy Res Practice. 2020;4(2):94–103. doi:10.3928/24748307-20200318-01
24. Wasilewski MB, Szigeti Z, Sheppard CL, et al. Infection prevention and control across the continuum of COVID‐19 care: a qualitative study of patients’, caregivers’ and providers’ experiences. Health Expectations. 2022:1–9. doi:10.1111/hex.13558
25. Crane-Okada R. Evaluation and outcome measures in patient navigation. Seminars in Oncology Nursing. WB Saunders. 2013;Vol. 29(2):128–140. doi:10.1016/j.soncn.2013.02.008
26. Budde H, Williams GA, Scarpetti G, Kroezen M, Maier CB. What are patient navigators and how can they improve integration of care? Eur Observatory Health Sys Policies. 2021;2021;1–32. World Health Organization 2022 (acting as the host organization for, and secretariat of, the European Observatory on Health Systems and Policies.
27. Crezee IH, Roat CE. Bilingual patient navigator or healthcare interpreter: what’s the difference and why does it matter? Cogent Med. 2019;6(1):1–15. doi:10.1080/2331205X.2019.1582576
28. Delaney LJ, Currie MJ, Huang HC, Lopez V, Van Haren F. “They can rest at home”: an observational study of patients’ quality of sleep in an Australian hospital. BMC Health Serv Res. 2018;18(1):1–9. doi:10.1186/s12913-018-3201-z
29. Sarrafi-Zadeh S, Dharwadkar SB, Singh R, et al. Nutritional modulators of sleep disorders. Open Nutraceuticals j. 2012;10(5):1–14. doi:10.2174/1876396001205010001
30. Dikko M. Establishing construct validity and reliability: pilot testing of a qualitative interview for research in Takaful (Islamic insurance). Qual Rep. 2016;21(3):521–529. doi:10.46743/2160-3715/2016.2243
31. Rahman R. Comparison of telephone and in-person interviews for data collection in qualitative human research. Interdisciplinary Undergraduate Res J. 2015;1(1):10–13.
32. Mythen M. Fit for surgery? Anesthesia Analg. 2011;112(5):1002–1004.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.