")
Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 15
Parental Willingness and Factors Influencing COVID-19 Vaccination for Children in Saudi Arabia
Authors AlMuammar S , Alshora W, Sadik Gari A, Bahaj RK, Alansari BA
Received 25 October 2023
Accepted for publication 9 January 2024
Published 16 January 2024 Volume 2024:15 Pages 29—48
DOI https://doi.org/10.2147/PHMT.S443272
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Sarah AlMuammar,1 Weam Alshora,2 Atheer Sadik Gari,1 Reem Khalid Bahaj,1 Bayan Abdullah Alansari1
1Family Medicine Department, King Abdulaziz University, Jeddah, Saudi Arabia; 2Family Medicine Department, King Abdulaziz University Hospital, Jeddah, Saudi Arabia
Correspondence: Sarah AlMuammar, Email [email protected]
Purpose: The study aimed to examine the parents’ willingness and its association with demographic factors, attitudes, and practices to vaccinate their child against COVID-19.
Patients and Methods: The study involved 2500 participants from various regions of Saudi Arabia and was conducted between July 1, 2021, and August 31, 2021. Information was gathered via an online questionnaire comprising 26 questions, distributed across social media platforms. Informed consent was obtained from all participants before the commencement of the study. A chi-square test was applied to analyze the association among variables, utilizing a subset of 2127 participants based on study inclusion criteria. A chi-square test was applied to observe the association.
Results: The willingness of parents to vaccinae their children against COVID-19 was found 61%. The main reason for taking was “Protect the child” by 1094 (51.4%%) and the main reason for refusing was “Side effects/safety concerns” by 477 (22.4%). 1846 (86.8%) participants, received the COVID-19 vaccine or were planning to receive it.
Conclusion: Our study concluded that parent’s willingness to vaccinate their children against COVID-19 was relatively high in our sample as about two-thirds of them accept the vaccine for their child once it is available. The use of the health belief model demonstrated the urgent requirement for awareness and education campaigns in the private and public sectors to increase awareness of parents not only related to COVID-19 but also to cater to any unexpected or suspected pandemic of infectious disease in the future full capacity.
Keywords: attitude, immunization, practices, vaccination, well-being
Introduction
The outbreak of COVID-19, caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), was first reported in December 2019. By January 12, 2020, the virus had affected millions of people globally.1,2 Many concerns developed as the infection was transmitted predominantly among individuals who were in close contact. Therefore, public health authorities worldwide took initiatives to reduce the spread of the virus by encouraging social distancing, wearing masks in public, and washing hands frequently.3,4
As of September 2022, COVID-19 caused 813,986 confirmed cases and 9309 fatalities in Saudi Arabia.5 Due to changes in the virus genome, new SARS-COV-2 variants jeopardized the vaccine’s effectiveness.6 Total of 66,700,629 vaccination doses were administered throughout the Kingdom,7 before returning to work, traveling abroad, or attending healthcare facilities and shopping centers. Saudi Arabia began administering of COVID-19 vaccine to children aged 12–18 years and 5–11 years in June and December 2021.8,9
Vaccinations are widely considered the most successful therapies to aid the prevention and control of infectious diseases and effectively build herd immunity. Parental refusal or postponement of vaccinations for children increased during the past ten years, and poor vaccination rates have contributed to the recurrence of numerous diseases that can be prevented by vaccination.10 Global acceptance of parents towards COVID-19 vaccination for their children aged between 0 and 18 years (mean age: 8.45) showed parental adoptability prevalence pooled estimate of 57% [95% Confidence Interval: 52–62%, I2: 99.92%].11 A cross-sectional study that interviewed parents visiting outpatient clinics in Saudi Arabia reported that 20% of parents had skeptical beliefs about children’s immunization.12 The assessment of parents’ intention to vaccinate offspring against COVID-19 reported lower willingness among Arab parents to vaccinate their children. Other factors included misconceptions about the severity of COVID-19 [73%; 95% CI: 73–79], efficacy and safety of vaccines [53%; 95% CI: 50 −56], parents’ young age [AOR:2.40; CI: 1.50–3.83], vaccination history [AOR: 16.47; CI: 8.39–32.33] and high fear among family members [AOR: 2.35; CI: 1.38–4.02].13,14 Misinformation leading to vaccination reluctance could endanger public health and make dealing with the current situation more difficult.15 Studies also reported the potential role of healthcare providers (HCPs) to ensure evidence-based effective communication with parents about focused health education strategies to change their perception towards vaccination.16–18 The self-perception of HCPs about COVID-19 vaccination also influences their convincing power to satisfy parents. The evaluation of HCPs’ attitudes towards the administration of COVID-19 vaccination showed 57.2% of HCPs confident while getting vaccinated and hesitancy was observed in 32% of HCPs (p < 0.05) based on perception of COVID-19, clinical and demographic characteristics of HCPs.19
According to the Saudi Ministry of Health, the majority of vaccines’ side effects are mild to moderate, manifest within three days of vaccination, and resolve on their own.9 Similarly, as per World Health Organization, COVID-19 vaccinations demonstrated minor or moderate side effects and subsided on their own after a few days.20 Recent studies reported population threshold for establishing COVID-19 herd immunity ranges between 55% and 82%, depending on the biological, environmental, and socio-behavioral factors.21 Evidence has suggested improved safety and effectivity of the COVID-19 vaccine, as a study in Taiwan reported improved physical and mental quality of life in patients with COVID-19 and flu vaccination in comparison to participants who remained unvaccinated.22 The willingness to vaccinate could be studied through different potential theoretical models including the Health Belief Model (HBM),23 theory of planned behavior,24 protection motivation theory,25 and trust in the healthcare system.26 Our study used HBM to estimate parents’ intention to get their child vaccinated as their health behavior. HBM evaluate individual beliefs and perception in terms of the perceived risk versus benefit ratio of vaccine, susceptibility, perceived barriers, efficacy, and severity and these factors influence a person’s action.27,28
Considering parent’s apprehension about their children’s well-being, allowing a child to participate in a vaccination study was a difficult decision, especially for children below the age of 18; since parents were usually the guardians responsible for them. As a result, it’s critical to comprehend parents’ acceptance of their children’s COVID-19 immunization. Few studies conducted in 2020 showed more than half of parents’ willingness to have their children vaccinated against COVID-19.29,30 While earlier studies indicated considerable parental willingness, there is a need for updated insights regarding the attitudes of parents in the distinct regions. This study aims to address this gap by assessing parental willingness across five regions in Saudi Arabia, considering demographic factors, attitudes, and vaccination practices concerning COVID-19 for children.
Materials and Methods
The cross-sectional study was conducted among five regions of Saudi Arabia including the southern, western, eastern, northern, and central regions—adhered to the principles of the Declaration of Helsinki. The study was approved by the Institutional Review Board (IRB) of King Abdul-Aziz University on Tuesday. July 13. 2021 under the reference number (Reference No 3B1-21).
Inclusion and Exclusion Criteria
The study included parents residing in the southern, western, eastern, northern, and central regions of Saudi Arabia, having children under the age of 12. Participation was voluntary, requiring informed consent from parents who completed the survey questionnaire distributed online via social media platforms. The survey was voluntary and anonymous, participants provided informed consent by voluntarily engaging in the survey after being explained about the study’s purpose. Exclusion criteria comprised parents residing outside the specified regions, those with children over 12 years old, and individuals unwilling to provide informed consent. Incomplete survey responses or failure to comply with survey instructions led to exclusion from the analysis.
Sample Size and Participants
Samples were recruited using a purposive sampling technique and the sample size was calculated based on the minimum sample required for a prevalence study.31 Moreover, using the Rao soft calculator, the sample size was found to be at least 315 with a margin of error of 5% and a confidence level of 95%. Hence, a total number of 2500 participants completed the survey of which 2127 were recruited for analysis based on study inclusion criteria.
The detailed study objective was explained by an independent researcher to all study participants and upon agreement informed consent was obtained from the participants.
Study Questionnaire
The Health Belief Model (HBM) framework was used to construct the questionnaire for our study. In terms of diversity of beliefs, such as perceived susceptibility, perceived severity, perceived benefits, perceived barriers, and cues to action, the HBM is a crucial theoretical framework for predicting the preventive health behavior of an individual.32 These HBM constructions have also been widely utilized to forecast readiness to receive influenza vaccinations.33 HBM constructions were linked to individuals’ desire to receive the COVID-19 vaccine. The objective of the current study was to observe the willingness of parents to get their children vaccinated against COVID-19. In this context, perceived susceptibility refers to parents’ overall perceptions of their children’s sensitivity to COVID-19 while discussing their desire to let them receive the COVID-19 vaccine. Parents’ perceptions of the COVID-19 adverse effects are referred to as perceived severity. Parents’ perceptions of the advantages of vaccinations, such as protecting their health are referred to as perceived benefits. Parental perceptions of the risks associated with vaccinations, including their side effects, are referred to as perceived barriers. Cues to action are the factors that motivate parents to immunize their children.34,35 By using the HBM theoretical framework, a 26-item questionnaire was developed. HBM questionnaire was previously validated by different studies36,37 but our study designed a questionnaire using ten questions about demographics, eight questions about factors that would influence the caregivers’ decision to vaccinate, and two were about the caregivers’ plans to get the Vaccine and vaccinate their children. The HBM section of the questionnaire was graded on a Likert scale ranging from 1 (disagree) to 3 (agree), which allowed a concise and user-friendly response format. It was chosen to encourage simplicity and ease of participant engagement; although it limited the spectrum of possible attitudes compared to higher-point scales. The use of a shorter scale aimed to reduce respondent burden and potential confusion associated with more gradations that resulted in higher response rates in capturing the general attitudes of parents toward their children’s COVID-19 vaccination.
The questionnaire was constructed in Arabic, the primary language spoken in Saudi Arabia. While this choice facilitated engagement with a majority of the population, it might have excluded residents who do not speak Arabic fluently.
Data Collection
The online questionnaire, being a convenient and widely accessible tool, was chosen as the mode of data collection from July 1, 2021, to August 31, 2021. This defined timeframe allowed for a focused data collection period, ensuring a specific window for participant engagement and data compilation within the specified duration. The online questionnaires were distributed as Google Forms and circulated through social media platforms, offering a convenient and accessible platform for data collection among a diverse population. There was the possibility of multiple responses from the same individual in online surveys and this issue was by implementing restrictions to limit multiple submissions from the same device or IP address. This minimized the likelihood of duplicate responses from participants.
For a detailed breakdown of the questionnaire items, see Appendix A.
Statistical Analysis
The data were analyzed by an independent researcher using Microsoft Excel 2016. Data was collected for age, gender, nationality, level of education, residence, marital status, family income, and whether the caregiver’s children have any medical issues were included in the demographic section. Cronbach alpha was computed for the reliability of the overall questionnaire and it was found 0.80. The Cronbach’s alpha for each subscale including perceived barrier was 0.76, perceived benefit eas 0.71, perceived susceptibility was 0.85, perceived severity was 0.81, and combined indices were 0.85, respectively.
Statistical Package for Social Science (SPSS) version 23.0 was used to analyze the data. The normality of data was not performed as there was no quantitative outcome variable in the study. Frequency and percentages were calculated for qualitative variables. The chi-square test was used to observe the association between two categorical variables and a P-value of <0.05 was considered to be statistically significant.
Results
Demographic Details
Two thousand five hundred surveys were completed online by caregivers; 2127 children less than 12 years old were included in this study. Table 1 provided demographic information that included females as the predominant gender; 1579 (74.2%), and almost two-thirds 1559 (73.3%) were from groups aged 26–35 and 36–45 years. The majority of 2055 (96.7%) were Saudi, and in 1975 (92.9%) were married. More than half, 1284 (60.4%) had bachelor’s degrees, and 1313 (61.7%) had monthly income between 5001–12,000 and 12,001–20,000. Less than a fifth, of 337 (15.8%) worked in the healthcare field.
 |
Table 1 Demographic Characteristics of Participants |
Medical History of Children
Table 2 depicts information about children’s medical history. Almost four of the children, 478 (22.5%), had a chronic illness, the most common were breathing problems (37%), and obesity (34.9%). A total of 190 (8.9%) received medications. Most caregivers (89.2%) reported that their children were up to date on vaccinations, and 2045 (96.1%) said, “Agree with the imposition of those vaccines for the child”. Among the participants who refused the imposition of those vaccines for the child, the main reasons were “Safety concerns” by 69 (41.3%) and “A desire for more information from healthcare providers” by 63 (37.7%), only forth children 540 (25.4%) received a flu vaccination.
 |
Table 2 Medical History of Children |
COVID-19 Vaccine Experience and Attitude
Table 3 provides information about the COVID-19 vaccine experience and attitude, most of the participants 1846 (86.8%) received the COVID-19 Vaccine or planning to receive it. More than half 1299 (61.1%) accepted giving the COVID-19 Vaccine to children; the main reasons for accepting the Vaccine were “Protect the child” by 1094 (51.4%%) and “Desire to return to normal life” by 1033 (48.6%). While the main reasons for refusing the Vaccine were “Side effects/safety concerns” by 477 (22.4%) and “Perceived child not at risk to contract COVID-19” by 281 (13.2%). Third, the participants confirmed that the child’s age influenced their decision to give them the COVID-19 Vaccine. More than half agree with the following statements: “If the Doctor Recommends That the Child Receive the COVID-19 Vaccine, Then the Child Will be Vaccinated.” by 1273 (59.8%). Followed by “The development of a COVID-19 vaccine is too rushed to properly test its safety” by 1170 (55.0%), then “Worry that the child Will Get Sick or Have Side Effects from a COVID-19 Vaccine” by 1141 (53.6%), and “the imposition of COVID-19 vaccine for children as a requirement to attend school as a precautionary measure for student safety” by 1077 (50.6%). The results of our study also showed a lack of awareness and certainty towards action post-vaccination of their child, as 51.7% had no idea about the safe return of child after vaccination to school in normal health status. 42.3% were neutral and 30% disagreed due to unawareness that even if WHO recommend they will not get their child vaccinated.
 |
Table 3 Attitudes and Practices of Parents Regarding COVID-19 Vaccination |
The analysis of medical records of children, attitudes, and awareness of parents concerning gender, age, and level of education has been illustrated in Figures 1–3.
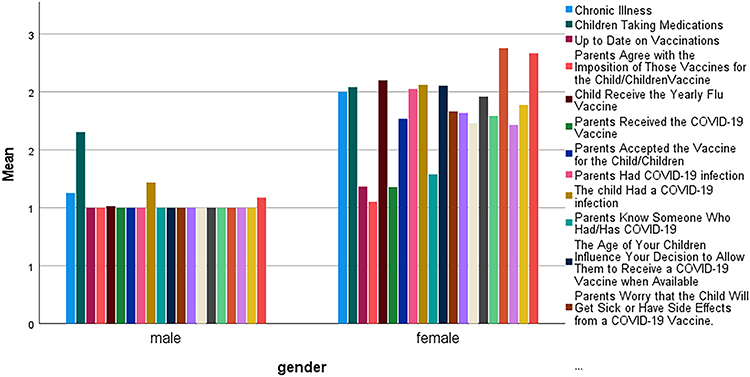 |
Figure 1 Analyzing medical records of children, attitudes, and awareness of parents concerning gender. |
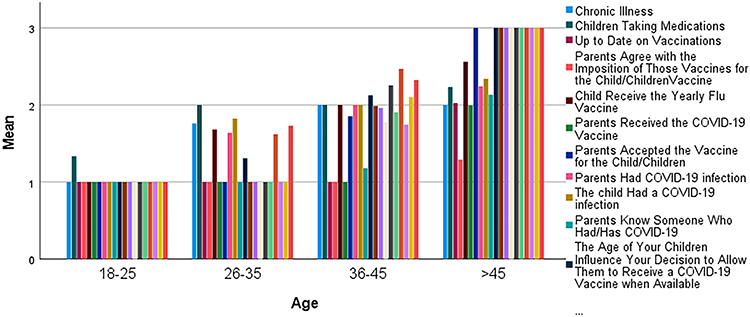 |
Figure 2 Analyzing medical records of children, attitudes, and awareness of parents concerning age. |
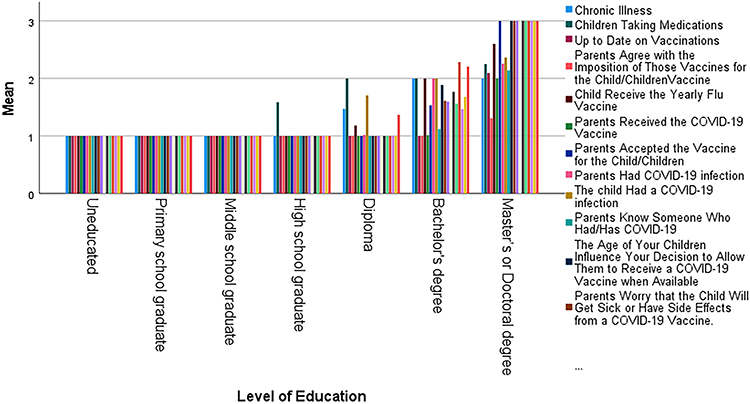 |
Figure 3 Analyzing medical records of children, attitudes, and awareness of parents concerning level of education. |
Association of Demographics with COVID-19 Vaccination Acceptance
Table 4 provides the association of demographic characteristics with the willingness for COVID-19 vaccination for their children. It revealed a significant association between” Accepting the Vaccine for the child/children” and gender, nationality, educational level, and region (p = 0.002, p = 0.016, p = 0.001, and p < 0.0001) respectively”. In addition, there was no significant association between” Accepting the Vaccine for the child/children” and age, marital status, family income, and being healthcare workers.
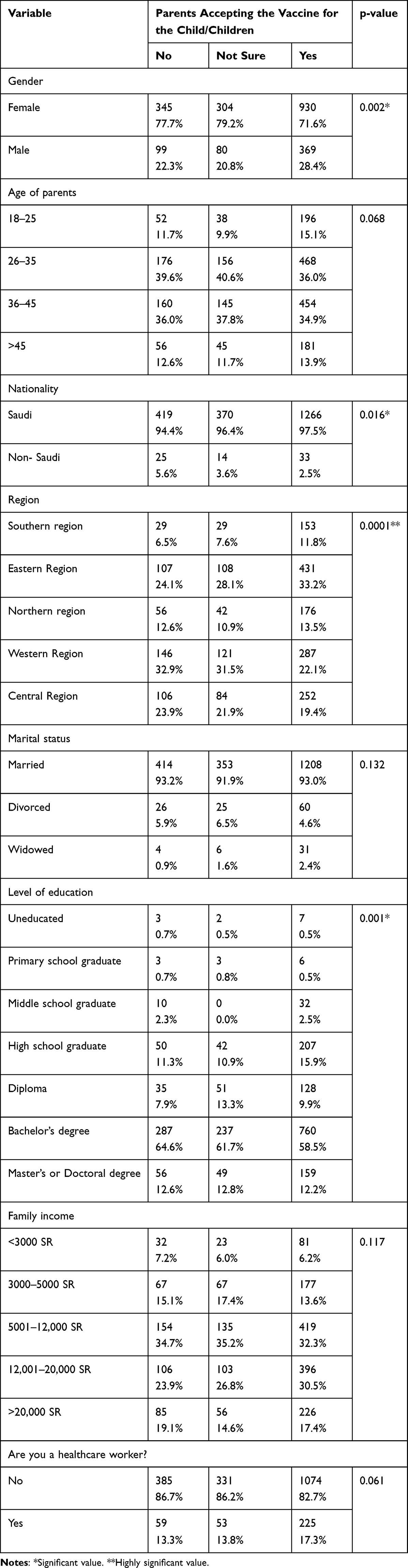 |
Table 4 Association of Demographic Characteristics with the Willingness to COVID-19 Vaccination for Their Children |
Parents’ Attitudes and Practices Towards COVID-19 Vaccination
Table 5 shows the association of parents’ attitudes and practices towards COVID-19 vaccination with the willingness to COVID-19 vaccination for their children. The results revealed a significant association in the group who received the COVID-19 Vaccine, those who had children, who did not suffer from COVID-19, those who knew someone hospitalized with COVID-19, those who reported that the age of the child did not influence their decision to give them COVID-19 Vaccine: those who agreed “If the Doctor Recommends That the Child Receive the COVID-19 Vaccine, Then the Child Will be Vaccinated”. “The development of a COVID-19 vaccine is too rushed to test its safety properly”, and “Worry that the child Will Get Sick or Have Side Effects from a COVID-19 Vaccine” (p < 0.0001).
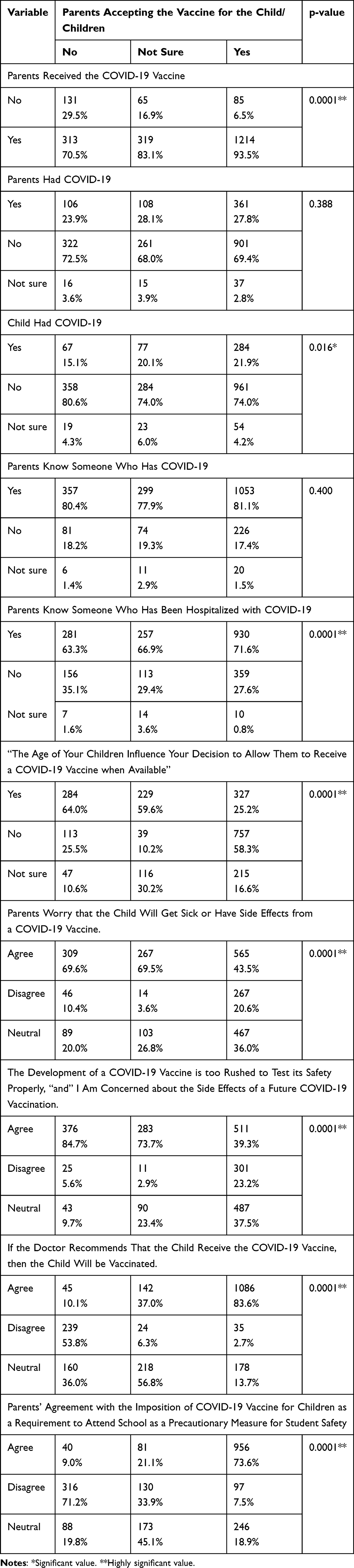 |
Table 5 Association of Parents’ Attitudes and Practices Towards COVID-19 Vaccination with the Willingness to COVID-19 Vaccination for Their Children |
Multivariate Analysis
Table 6 presents the results of a multivariate analysis examining the effects of different variables on vaccination willingness among the surveyed population. The Wilks’ Lambda values in the multivariate analysis table signify the extent of variance in the willingness to vaccinate attributed to each variable. Higher Wilks’ Lambda values near 1 suggest a more substantial association between the variable and vaccination willingness. In this context, gender exhibits a Wilks’ Lambda of 0.556, indicating that gender accounts for approximately 44.4% of the variance in vaccination willingness, implying a notable but not exclusive influence. On the other hand, age demonstrates a markedly higher Wilks’ Lambda of 0.008, suggesting that age plays a more dominant role, accounting for around 80.2% of the variance in vaccination willingness among the surveyed population. Similarly, the level of education presents a Wilks’ Lambda of 0.122, signifying that education level contributes to about 29.6% of the variance in vaccination willingness, indicating a moderate impact compared to other variables assessed in the analysis.
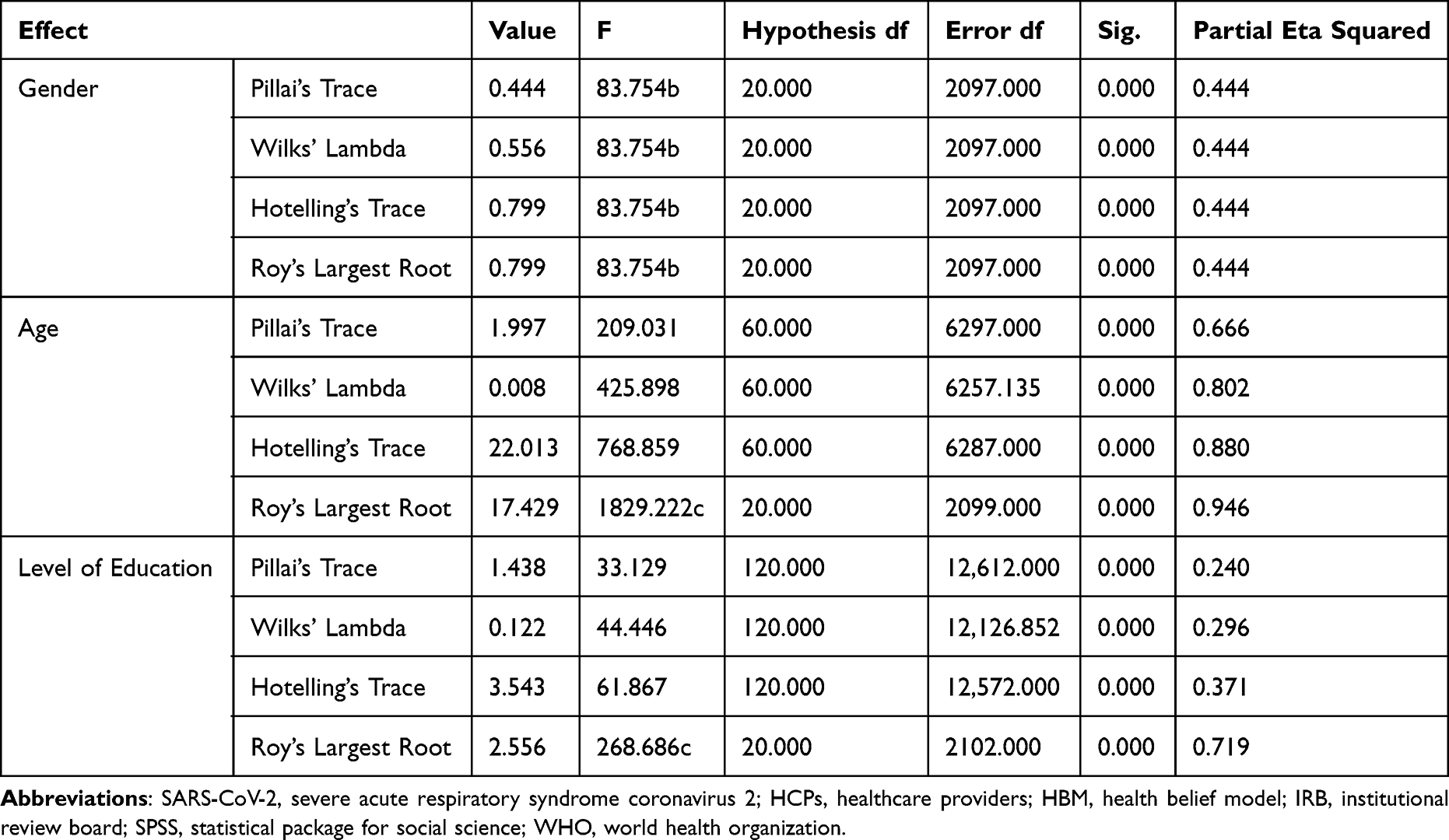 |
Table 6 Multivariate Analysis |
Discussion
The study aimed to assess whether parents were willing to vaccinate their children against COVID-19 and the association of demographic characteristics, attitudes, and practices of parents with the willingness to vaccinate their children. Our results demonstrated that 61% of parents were willing to vaccinate their children against COVID-19, where most caregivers were females. The key option for mitigating the effects of COVID-19 is immunization. Children under the age of 14 account for around 25% of the global population38 and account for approximately 10% of total COVID-19 cases.39 Vaccinating children is an important step in achieving more comprehensive herd immunity against COVID-19. One of the most critical variables influencing how many children will be covered by the COVID-19 immunization campaign is parents’ willingness to allow their children to receive the vaccines. In Saudi Arabia, cultural and religious beliefs often intersect with healthcare decisions, including vaccination. Additionally, government policies, public health campaigns, and access to healthcare services contribute to the overall vaccination landscape. However, Saudi Arabia’s efforts in promoting healthcare, vaccination campaigns, and initiatives play a crucial role in shaping parental attitudes. The government’s support and endorsement of vaccinations, including COVID-19 vaccines significantly influence parental willingness to vaccinate their children.
A meta-analysis, however, discovered that only about 57% of parents intend to vaccinate their children, and this rate varies substantially across nations.40 A survey based on a small sample of Hong Kong parents discovered that only 21% of parents would vaccinate their children if COVID-19 vaccines were formally authorized for use.41 This rate is nearly the lowest among those found in other countries.42–44 In contrast to our study, a recent study in Saudi Arabia reported that only 28% of 1000 caregivers were ready to vaccinate their children.45
In a study, the income of parents affected the decision to have the vaccination for their child which was contrary to our findings and was not found significant.10 Our sample’s predominant motivation for COVID-19 vaccination was fear of the pandemic’s severity, like previous parental plans to protect their children against seasonal influenza.46 “Protection of the child” was the most common reason for vaccine acceptance in our study which was in concordance with other previous studies, followed by “desire to return to normal life” and “perceived pandemic severity”. Nevertheless, the main reason for rejecting the vaccine in our study was the vaccine’s side effects. The second most common reason for rejection was the child was not at risk of having COVID-19. The World Health Organization (WHO) suggests that only 8.5% of children under 18 years got infected with COVID-19 or are thought to be asymptomatic.47 Therefore, they are the least likely to contract the disease. Our study showed that caregivers with a bachelor’s degree are more willing to vaccinate their children. Similar findings were reported by a study in which a higher academic level correlates to much better health and grasping of information related to vaccines.48 Our study results also showed that due to lack of awareness and training sessions, 51.7% had no idea about the safe return of children after vaccination to school in normal health status. 42.3% were neutral, and 30% were unwilling due to unawareness that even if WHO recommend they will not get their child vaccinated. The increase in parental willingness could be attained through different aspects, such as using Zoom-focused education and minimizing the pay for the vaccine.49 An introduction of ZOOM sessions and empowerment of parents to ask their concerns related to vaccines to HCPs during these sessions reported 65% improved vaccination compliance in Hong Kong preschoolers.50 Clear and appropriate communication with caregivers and parents related to the benefits of vaccination and awareness related to safety precautions help improve the rate of vaccination among children.51
In a recent survey in Saudi Arabia,52 65% of adults revealed that they would plan to get vaccinated against COVID-19.53 Similar findings were reported from three-quarters of an online sample from France,54 and 69% in the United Kingdom.55 The Ministry of Health recorded that more than 23 million individuals in Saudi Arabia had received the COVID-19 Vaccine. Therefore, of 2127, 1846 received the COVID-19 Vaccine, and 1214 were willing to give their children the COVID-19 Vaccine. The severity of the pandemic and the complications associated with the contraction of COVID-19 instilled concerns in the general population and motivated them to opt for vaccination which also enhanced the parents’ willingness to immunize their children.9,56 Thus, parents who vaccinated themselves against COVID-19 were more willing to vaccinate their children probably due to their previous experience in vaccination and confidence in accepting the idea of vaccination and considered it as the most effective measure in preventing infections.
Parents may be more likely to vaccinate their children against COVID-19 if they have social legitimacy57 following large groups getting vaccinated and hearing recommendations from healthcare practitioners.19 Same as our study, which showed that caregivers are more intent to give their child the Vaccine if the doctor recommends it. During the COVID-19 pandemic, a global epidemic of misinformation emerged through social media, posing obstacles to future COVID-19 immunization initiatives.58,59 Thus, public health authorities should modify misinformation about the COVID-19 vaccine and create a positive perception of the vaccine.
It has been shown that a significant portion (approximately two-thirds) of parents having children affected by kidney disease or hypertension expressed reluctance when vaccinating their child against COVID-19.60 Interestingly, a similar level of hesitancy was observed towards routine childhood vaccinations and the influenza vaccine among the same group of parents. This link between hesitation towards different vaccines suggests a potential connection in attitudes. Another study by Del Giudice et al61 showed that parents exhibiting worrisome attitudes regarding the safety of COVID-19 vaccines, postponed at least one dose of a recommended vaccine for their child, and did not receive a minimum of three doses of the SARS-CoV-2 vaccine were prone to displaying increased levels of hesitancy towards vaccination in Italy. The findings of a study by Zhou et al62 revealed a considerable delay in vaccination among both parents and their children, irrespective of eligibility for the booster dose. This highlighted the need for increased awareness regarding the scientific evidence backing the efficacy and safety of all the vaccines not just COVID-19, particularly among individuals with poor health conditions and parents having young children. Moreover, a study showed concern for parents’ readiness to vaccinate children aged 5 to 11 years.63 This highlighted the need to guide policymakers across nations to formulate effective strategies to promote childhood vaccination.
The strengths include the large sample size which was conducted in five regions of Saudi Arabia. However, this study has some limitations. Firstly, the sample may not fully represent all caregiver perspectives in Saudi Arabia, potentially introducing selection bias. Being a cross-sectional study, it captured a snapshot of attitudes at a specific time, limiting the ability to draw causal relationships or generalize findings beyond the study period. The survey being exclusively in Arabic posed a language barrier, excluding individuals unable to read Arabic, possibly introducing language bias and limiting the inclusivity of diverse linguistic groups. Moreover, the survey’s distribution via social media might have excluded caregivers without access to smart devices, potentially leading to socioeconomic bias. Importantly, this study was conducted in 2021, and as vaccination approval for children might have changed since then, the findings might not reflect the current landscape. However, it serves as a valuable baseline for understanding initial perspectives before vaccine authorization for children. The findings provide a foundational insight into parental willingness, offering a starting point for monitoring shifts in attitudes post-authorization and guiding future research and public health strategies. Additionally, the questionnaire, while based on the Health Belief Model, underwent pilot testing but lacked full validation before implementation, possibly affecting the accuracy and reliability of responses.
Conclusion
In conclusion, the study revealed a notably high prevalence of parental acceptance of COVID-19 vaccination for their children, with approximately two-thirds expressing willingness once the vaccine became available. The Health Belief Model highlighted the need for robust awareness and education campaigns across public and private sectors, emphasizing not only COVID-19 but also preparedness for potential future infectious disease pandemics. However, future research employing in-person interviews and stringent eligibility criteria is recommended to investigate parents’ perspectives deeply and further refine the understanding of parental attitudes toward childhood vaccinations.
Acknowledgments
The author is thankful to all the associated personnel who contributed to this study by any means.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Marquez RR, Gosnell ES, Thikkurissy S, Schwartz SB, Cully JL. Caregiver acceptance of an anticipated COVID-19 vaccination. J Am Dent Assoc. 2021;152(1):1–10. doi:10.1016/j.adaj.2021.03.004
2. Corman VM, Landt O, Kaiser M, et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Eurosurveillance. 2020;25(3). doi:10.2807/1560-7917.ES.2020.25.3.2000045
3. Goldman RD, Staubli G, Cotanda CP, et al. Factors associated with parents’ willingness to enroll their children in trials for COVID-19 vaccination. Hum Vaccines Immunother. 2021;17(6):1607–1611. doi:10.1080/21645515.2020.1834325
4. Bults M, Beaujean DJMA, Richardus JH, Voeten HACM. Perceptions and behavioral responses of the general public during the 2009 influenza A (H1N1) pandemic: a systematic review. Disaster Med Public Health Prep. 2015;9(2):207–219. doi:10.1017/dmp.2014.160
5. Saudi Arabia: WHO Coronavirus Disease (COVID-19) Dashboard with Vaccination Data. Available from: https://covid19.who.
6. CDC COVID Data Tracker. Available from: https://covid.cdc.gov/covid-data-tracker/.
7. Saudi Arabia Situation. Available from: https://covid19.who.int/region/emro/country/sa.
8. Saudi Arabia Starts Giving Covid-19 Vaccines to Children Aged 5–11. Available from: https://saudigazette.com.sa/article/614992.
9. Ministry of Health Saudi Arabia. Available from: https://www.moh.gov.sa/en/CCC/Pages/default.aspx.
10. Al-Qahtani AM, Mannasaheb BA, Shaikh MA, et al. Parental willingness for COVID-19 vaccination among children aged 5 to 11 Years in Riyadh City, Saudi Arabia: a Cross-Sectional Study. Vaccines. 2022;10(12):1979. doi:10.3390/vaccines10121979
11. Alimoradi Z, Lin CY, Pakpour AH. Worldwide estimation of parental acceptance of COVID-19 vaccine for their children: a systematic review and meta-analysis. Vaccines. 2023;11(3):533. doi:10.3390/vaccines11030533
12. Alsubaie SS, Gosadi IM, Alsaadi BM, et al. Vaccine hesitancy among Saudi parents and its determinants: result from the WHO SAGE working group on vaccine hesitancy survey tool. Saudi Med J. 2019;40(12):1242. doi:10.15537/smj.2019.12.24653
13. Morozov NG, Dror AA, Daoud A, et al. Reasons underlying the intention to vaccinate children aged 5-11 against COVID-19: a cross-sectional study of parents in Israel, November 2021. Hum Vaccin Immunother. 2022;18(6):2112879. doi:10.1080/21645515.2022.2112879
14. Bateyi Mustafa SH, Kabamba M, Onyango RO. Determinants of parents’ intention to vaccinate their children aged 12–17 years against COVID-19 in North Kivu (Democratic Republic of Congo). Hum Vaccin Immunother. 2023;19(1):2179788. doi:10.1080/21645515.2023.2179788
15. Garfin DR, Silver RC, Holman EA. The novel coronavirus (COVID-2019) outbreak: amplification of public health consequences by media exposure. Health Psychol. 2020;39(5):355. doi:10.1037/hea0000875
16. Goulding M, Ryan GW, Minkah P, et al. Parental perceptions of the COVID-19 vaccine for 5-to 11-year-old children: focus group findings from Worcester Massachusetts. Hum Vaccin Immunother. 2022;18(6):2120721. doi:10.1080/21645515.2022.2120721
17. Zheng M, Zhong W, Chen X, et al. Factors influencing parents’ willingness to vaccinate their preschool children against COVID-19: results from the mixed-method study in China. Hum Vaccin Immunother. 2022;18(6):2090776. doi:10.1080/21645515.2022.2090776
18. Kotecha IS, Vasavada DA, Kumar P, Nerli LM, Tiwari DS, Parmar DV. Knowledge, attitude, and belief of healthcare workers toward COVID-19 vaccine at a tertiary care center in India. Asian J Soc Health Behav. 2022;5(2):63. doi:10.4103/shb.shb_20_21
19. Rad MK, Fakhri A, Stein LA, Araban M. Health-care staff beliefs and coronavirus disease 2019 vaccinations: a cross-sectional study from Iran. Asian J Soc Health Behav. 2022;5(1):40. doi:10.4103/shb.shb_13_22
20. World Health Organization. COVID-19 vaccines; 2022. Available from: https://www.who.
21. DeRoo SS, Pudalov NJ, Fu LY. Planning for a COVID-19 vaccination program. JAMA. 2020;323(24):2458–2459. doi:10.1001/jama.2020.8711
22. Lin CY, Fan CW, Ahorsu DK, Lin YC, Weng HC, Griffiths MD. Associations between vaccination and quality of life among Taiwan general population: a comparison between COVID-19 vaccines and flu vaccines. Hum Vaccin Immunother. 2022;18(5):2079344. doi:10.1080/21645515.2022.2079344
23. Li JB, Lau EY, Chan DK. Why do Hong Kong parents have low intention to vaccinate their children against COVID-19? Testing health belief model and theory of planned behavior in a large-scale survey. Vaccine. 2022;40(19):2772–2780. doi:10.1016/j.vaccine.2022.03.040
24. Fan CW, Chen IH, Ko NY, et al. An extended theory of planned behavior in explaining the intention to COVID-19 vaccination uptake among mainland Chinese university students: an online survey study. Hum Vaccin Immunother. 2021;17(10):3413–3420. doi:10.1080/21645515.2021.1933687
25. Huang PC, Chen IH, Barlassina L, et al. Expanding Protection Motivation Theory to explain vaccine uptake among United Kingdom and Taiwan populations. Hum Vaccin Immunother. 2023;19(1):2211319. doi:10.1080/21645515.2023.2211319
26. Vashishtha VM. Is ‘original antigenic sin’complicating Indian vaccination drive against COVID-19? Hum Vaccin Immunother. 2021;17(10):3314–3315. doi:10.1080/21645515.2021.1945904
27. Reindl D, Catma S. A pre-vaccine analysis using the Health Belief Model to explain parents’ willingness to vaccinate (WTV) their children in the United States: implications for vaccination programs. Expert Rev Pharmacoecon Outcomes Res. 2022;22(5):753–761. doi:10.1080/14737167.2022.2045957
28. Rajeh MT, Farsi DJ, Farsi NJ, Mosli HH, Mosli MH. Are parents willing to vaccinate their children against COVID-19? A qualitative study based on the Health Belief Model. Hum Vaccin Immunother. 2023;19(1):2177068. doi:10.1080/21645515.2023.2177068
29. Brandstetter S, Böhmer MM, Pawellek M, et al. Parents’ intention to get vaccinated and to have their child vaccinated against COVID-19: cross-sectional analyses using data from the KUNO-Kids health study. Eur J Pediatr. 2021;180(11):3405–3410. doi:10.1007/s00431-021-04094-z
30. Goldman RD, Yan TD, Seiler M, et al. Caregiver willingness to vaccinate their children against COVID-19: cross-sectional survey. Vaccine. 2020;38(48):7668–7673. doi:10.1016/j.vaccine.2020.09.084
31. Naing NN. Determination of sample size. MJMS. 2003;10:84.
32. Rosenstock IM. Historical origins of the health belief model. Health Educ Monogr. 1974;2(4):328–335. doi:10.1177/109019817400200403
33. Bish A, Yardley L, Nicoll A, Michie S. Factors associated with uptake of vaccination against pandemic influenza: a systematic review. Vaccine. 2011;29(38):6472–6484. doi:10.1016/j.vaccine.2011.06.107
34. Hossain MB, Alam MZ, Islam MS, et al. Health belief model, theory of planned behavior, or psychological antecedents: what predicts COVID-19 vaccine hesitancy better among Bangladeshi adults? Front Public Health. 2021;9:711066. doi:10.3389/fpubh.2021.711066
35. Shmueli L. Predicting intention to receive COVID-19 vaccine among the general population using the health belief model and the theory of planned behavior model. BMC Public Health. 2021;21(1):1–13. doi:10.1186/s12889-021-10816-7
36. Saunders GH, Frederick MT, Silverman S, Papesh M. Application of the health belief model: development of the hearing beliefs questionnaire (HBQ) and its associations with hearing health behaviors. Int J Audiol. 2013;52(8):558–567. doi:10.3109/14992027.2013.791030
37. Shaw AR, Vidoni ED, Sullivan DK, Berkley-Patton J, Burns J. Developing a culturally tailored brain healthy diet intervention for older midwestern African Americans: a qualitative and quantitative study. medRxiv. 2022;1:2022–2026.
38. The World Bank. Population ages 0-14 (% of total population); 2022. Available from: https://data.worldbank.org/indicator/SP.POP.0014.TO.ZS.
39. UNICEF. COVID-19 confirmed cases and deaths; 2022. Available from: https://data.unicef.org/resources/covid-19-confirmed-cases-and-deaths-dashboard/.
40. Galanis P, Vraka I, Siskou O, Konstantakopoulou O, Katsiroumpa A, Kaitelidou D. Willingness and influential factors of parents to vaccinate their children against the COVID-19: a systematic review and meta-analysis. medRxiv. 2021;2021–2028. doi:10.1101/2021.08.25.21262586
41. Kwok KO, Li KK, Wei WI, et al. Likelihood of COVID-19 vaccination among primary school students in Hong Kong. Clin Microbiol Inf. 2022;28(1):142–144. doi:10.1016/j.cmi.2021.09.029
42. Evans S, Klas A, Mikocka-Walus A, et al. “Poison” or “protection”? A mixed methods exploration of Australian parents’ COVID-19 vaccination intentions. J Psychosom Res. 2021;150:110626. doi:10.1016/j.jpsychores.2021.11062
43. Urrunaga-Pastor D, Herrera-Añazco P, Uyen-Cateriano A, et al. Prevalence and factors associated with parents’ non-intention to vaccinate their children and adolescents against COVID-19 in Latin America and the Caribbean. Vaccines. 2021;9(11):1303. doi:10.3390/vaccines9111303
44. Teasdale CA, Borrell LN, Shen Y, et al. Parental plans to vaccinate children for COVID-19 in New York City. Vaccine. 2021;39(36):5082–5086. doi:10.1016/j.vaccine.2021.07.058
45. Almusbah Z, Alhajji Z, Alshayeb Z, et al. Caregivers’ willingness to vaccinate their children against COVID-19 in Saudi Arabia: a cross-sectional survey. Cureus. 2021:13. doi:10.7759/cureus.17243
46. Rubin GJ, Potts HWW, Michie S. Likely uptake of swine and seasonal flu vaccines among healthcare workers. A cross-sectional analysis of UK telephone survey data. Vaccine. 2011;29(13):2421–2428. doi:10.1016/j.vaccine.2011.01.035
47. Ludvigsson JF. A systematic review of COVID-19 in children shows milder cases and a better prognosis than in adults. Acta Paediatr. 2020;109(6):1088–1095. doi:10.1111/apa.15270
48. Anjum Q, Omair A, Inam SN, Ahmed Y, Usman Y, Shaikh S. Improving vaccination status of children under five through health education. J Pak Med Assoc. 2004;54(12):610–613. doi:10.1016/j.vaccine.2011.01.035
49. Huang CL, Chen JY, Lin XQ, Deng JS, Tung TH, Zhu JS. Parent’s willingness to pay for their children’s COVID-19 vaccine in Taiwan, China: a cross-sectional study. Hum Vaccin Immunother. 2023;19(1):2168936. doi:10.1080/21645515.2023.2168936
50. Wong WH, So HK, Rosa Duque JS, et al. Impact of a focus education in Zoom on COVID-19 vaccine hesitancy in Hong Kong parents of preschoolers. Hum Vaccin Immunother. 2022;18(5):2081460. doi:10.1080/21645515.2022.2081460
51. Tan L, Safadi MA, Horn M, et al. Pandemic’s influence on parents’ attitudes and behaviors toward meningococcal vaccination. Hum Vaccin Immunother. 2023;19(1):2179840. doi:10.1080/21645515.2023.2179840
52. Padhi BK, Al-Mohaithef M. Determinants of COVID-19 vaccine acceptance in Saudi Arabia: a web-based national survey. medRxiv. 2020;23:1657–1663.
53. Faasse K, Newby J. Public perceptions of COVID-19 in Australia: perceived risk, knowledge, health-protective behaviors, and vaccine intentions. Front Psychol. 2020;11:551004. doi:10.3389/fpsyg.2020.551004
54. Ward J, Alleaume C, Peretti-Watel P, et al. The French public’s attitudes to a future COVID-19 vaccine: the politicization of a public health issue. SocArXiv. 2020. doi:10.1016/j.socscimed.2020.113414
55. Murphy J, Vallières F, Bentall RP, et al. Preparing for a COVID-19 vaccine: identifying and psychologically profiling those who are Vaccine hesitant or resistant in two general population samples. PsyArXiv. 2020;2:1.
56. Setbon M, Raude J. Factors in vaccination intention against the pandemic influenza A/H1N1. Eur J Public Health. 2010;20(5):490–494. doi:10.1093/eurpub/ckq054
57. Jung M, Lin L, Viswanath K. Associations between health communication behaviors, neighborhood social capital, vaccine knowledge, and parents’ H1N1 vaccination of their children. Vaccine. 2013;31(42):4860–4866. doi:10.1016/j.vaccine.2013.07.068
58. Tangcharoensathien V, Calleja N, Nguyen T, et al. Framework for Managing the COVID-19 Infodemic: methods and Results of an Online, Crowdsourced WHO Technical Consultation. J Med Internet Res. 2020:
59. Bao H, Cao B, Xiong Y, Tang W. Digital media’s role in the COVID-19 pandemic. JMIR Mhealth Uhealth. 2020;8(9):e20156. doi:10.2196/20156
60. Wang CS, Doma R, Westbrook AL, et al. Vaccine attitudes and COVID-19 vaccine intention among parents of children with kidney disease or primary hypertension. Am J Kidney Dis. 2023;81(1):25–35. doi:10.1053/j.ajkd.2022.04.011
61. Del Giudice GM, Della Polla G, Postiglione M, et al. Willingness and hesitancy of parents to vaccinate against COVID-19 their children ages 6 months to 4 years with frail conditions in Italy. Front Public Health. 2023;7:11.
62. Zhou Y, Li GX, Zhao TS, et al. Parents’ willingness to vaccinate themselves and their children with the booster vaccine against SARS‐CoV‐2: a cross‐sectional study in Puyang City, China. J Med Virol. 2023;95(1):e28256. doi:10.1002/jmv.28256
63. Mayyas F. Parental willingness to COVID-19 vaccination among 5-to 11-year-old children in Jordan. J Pharm Health Serv Res. 2023;14(2):103–111. doi:10.1093/jphsr/rmad022
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.