")
Back to Journals » Psoriasis: Targets and Therapy » Volume 13
Palmoplantar Pustulosis: A Systematic Review of Risk Factors and Therapies
Authors Heidemeyer K, May Lee M , Cazzaniga S , Yawalkar N, Naldi L
Received 20 July 2023
Accepted for publication 16 September 2023
Published 22 September 2023 Volume 2023:13 Pages 33—58
DOI https://doi.org/10.2147/PTT.S400402
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Uwe Wollina
Kristine Heidemeyer,1,2 Marco May Lee,3 Simone Cazzaniga,1,2 Nikhil Yawalkar,1 Luigi Naldi2,4
1Department of Dermatology, Inselspital University Hospital of Bern, Bern, Switzerland; 2Centro Studi GISED, Bergamo, Italy; 3Section of Dermatology, Department of Clinical and Experimental Medicine, University of Parma, Parma, Italy; 4Dermatology Department, S. Bortolo Hospital, Vicenza, Italy
Correspondence: Kristine Heidemeyer, Department of Dermatology, Inselspital University Hospital of Bern, Freiburgstrasse 34, Bern, CH-3010, Switzerland, Tel +41 31 632 20 94, Email [email protected]
Abstract: Palmoplantar pustulosis (PPP) is a chronic, relapsing, inflammatory disease that can occur alone or in association with arthritis. There is still controversy about whether it should be separated from psoriasis or classified as pustular psoriasis. Furthermore, drug-induced paradoxical PPP is a special variant of PPP that differs from classic PPP in several ways. Treatment of PPP is still challenging, and there are a number of treatment-resistant cases. This review summarizes the risk factors for the development of PPP and the currently available treatment modalities. Female sex, smokers or ex-smokers, obesity, thyroid dysfunction, and treatment with a tumor necrosis factor (TNF)-α inhibitor have been identified as risk factors for the disease’s development, severity, and course. Topical treatments and phototherapy are effective for some patients and are used as a first-line or adjuvant treatment modality. Conventional treatments including retinoids and fumaric acid show good effects and can increase the efficacy of treatment with psoralen + ultraviolet light therapy (PUVA). Ciclosporin is fast acting, but relapse mostly occurs immediately after cessation. TNF-α inhibitors are efficient, and an even better response can be achieved with IL-17 and IL-23 blockers as well as apremilast. The effect of Janus kinase inhibitors seems to be promising according to case reports, but further investigations with larger cohorts are needed.
Keywords: palmoplantar, pustulosis, psoriasis, treatment, risk factors
Introduction
Palmoplantar pustulosis (PPP) is a chronic, recurrent, inflammatory skin disease that has a significant impact on quality of life.1,2 It is characterized by sterile pustules on an erythematous scaly base on the palms and soles, and hyperkeratotic plaques and fissures can appear as well. Pustules can disappear within days and leave brown scabs.1,3 Nail involvement occurs in 30–76% of cases and mainly includes onycholysis, pitting, onychodystrophy, subungual hyperkeratosis or pustulation, ridging, thickening, discoloration, and splinter hemorrhage.4
The prevalence of PPP is estimated as 0.005 to 0.12% and is clearly higher in Japan than in Western countries.1,4–6 There is a prominent female predominance, the mean age of patients is 40–58 years, and earlier onset occurs in patients with a positive family history of psoriasis.4,7 PPP can appear isolated, but in up to 10–30% of cases, it occurs in association with pustulotic arthro-osteitis (Sonozaki-Syndrome), which has mainly been reported in Japan, as well as syndromes such as SAPHO (synovitis, acne, pustulosis, hyperostosis, osteitis) syndrome.1,8 There is still debate in the literature about whether PPP should be considered as a variant of pustular psoriasis, as stated in a consensus by the European Rare and Severe Psoriasis Expert Network, or whether it is a different entity that has to be separated from even palmoplantar pustular psoriasis.3,7 Palmoplantar pustular psoriasis has been suggested for patients with palmoplantar pustulosis and concomitant psoriasis, psoriasis arthritis, or a positive family history of psoriasis.2 This discordance could also lead to variations in results regarding triggers and associated diseases, as well as treatment response.
Psoriasis and PPP share some genetic and pathogenetic similarities. Although PPP is not associated with the PSORS1 locus as in the case of psoriasis vulgaris (PV), mutations in the CARD14, AP1S3, and ATG16 L1 genes have been found in PPP, PV, and generalized pustular psoriasis (GPP). Interestingly, a mutation in the IL36RN gene is only found in 2% of PPP patients, and its relationship is controversial.1,3 This gene codes for the IL-36 receptor antagonist, which is frequently involved in other phenotypes of pustular psoriasis, such as GPP and acrodermatitis continua of Hallopeau.
The exact pathogenesis of PPP is still not fully understood. Besides genetic factors, several environmental factors and immune dysregulation are hypothesized. Bacteria and antimicrobial peptides (ie, LL-37) contribute to the pathogenesis of PPP by induction of inflammation.2,9 IL-36 and IL-8 are a chemoattractant and activator of neutrophils and have recently been suggested to be important for pustule formation in the acrosyringium.4,9,10 The IL23-Th17 axis and IL-36 participate in the exacerbation of the disease by inducing positive feedback,9 which has motivated the development and use of targeted therapies.
The severity of PPP is usually evaluated using adapted variants of the Psoriasis Area and Severity Index (PASI) and the Palmoplantar Pustulosis Area and Severity Index (PPPASI). The calculations are based on a subjective scoring of the severity of erythema (0–4), desquamation (0–4), infiltration and pustules (0–4), and the percentage of the affected area (0–6).11 The modified PPPASI considers each of these variables separately for the palms and soles.12 The evaluations also include subjective global assessment scores such as the Physician Global Assessment (PGA) with a grading of severity of the disease (0–5).13
Topical therapies including corticosteroids and vitamin D derivatives remain first-line therapies for PPP. Furthermore, UV therapies such as UVA and UVB therapies, excimer laser, and psoralen and UVA (PUVA) treatment are widely recommended.5 In the early 1980s, retinoid etretinate showed good efficacy in PPP. Nowadays, etretinate is no longer licensed in most Western countries, but the next-generation systemic retinoid acitretin is still one of the most frequently applied systemic therapies.5 The introduction of new biologics and optimized treatment protocols has been a significant development in the treatment of plaque psoriasis.14,15 However, although these medications are also used for PPP, breakthrough therapies are still limited. Several comorbidities, lifestyle habits, and medications have been described as triggers, associated factors, or risk factors for disease onset or aggravation. This review summarizes possible risk factors for the development and severity of PPP or its progression, as well as available treatment modalities.
Methods
Literature Search Strategy
This systematic review was conducted in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). Articles published until February 2023 were included. The literature search was conducted on the 15th of February using the MEDLINE, EMBASE, and Cochrane databases. The search terms included “palmoplantar pustulosis” AND “treatment”, as well as “palmoplantar pustulosis” AND “risk factor”.
Inclusion and Exclusion Criteria
All reports in English or German language were included in the analysis. Case reports (<5 patients), articles in other languages, and articles not matching the topic were excluded. Studies that did not distinguish between palmoplantar pustulosis and palmoplantar psoriasis without pustular eruption were excluded after review of the article, while studies on palmoplantar pustular psoriasis were retained. Studies involving etretinate and arotinoid were not included as the medications are no longer available in the US or Europe. Furthermore, studies were excluded if they had a design examining associated factors but not risk factors and non-clinical factors such as genetics.
Data Extraction, Analysis, and Quality Assessment
Review of the abstracts and data extraction were performed by two independent dermatologists (KH, MML). The data extracted for risk factors included the author, year of publication, study design, risk factor, number of patients, characteristics of population, outcome, and NIH study rating. The data extracted for treatment included the author, year, study type, drug/therapy, treatment duration, number of patients, scoring tool, outcome, adverse effects (AEs), and study rating. Any disagreements among the reviewers regarding study selection and quality were resolved by consensus (KH, MML). Duplicates and articles including results from the same patients were removed. Nondetailed data, such as aggregated data, were not considered. Studies were rated according to the NIH rating scale.
Results
Screening results
The preliminary search identified 1137 studies, and 447 duplicates were removed. After abstract screening, 418 articles were excluded, and after reading the full text, 195 articles were removed (Figure 1). Finally, 72 studies were included in the review (63 treatment studies and 9 studies about risk factors).
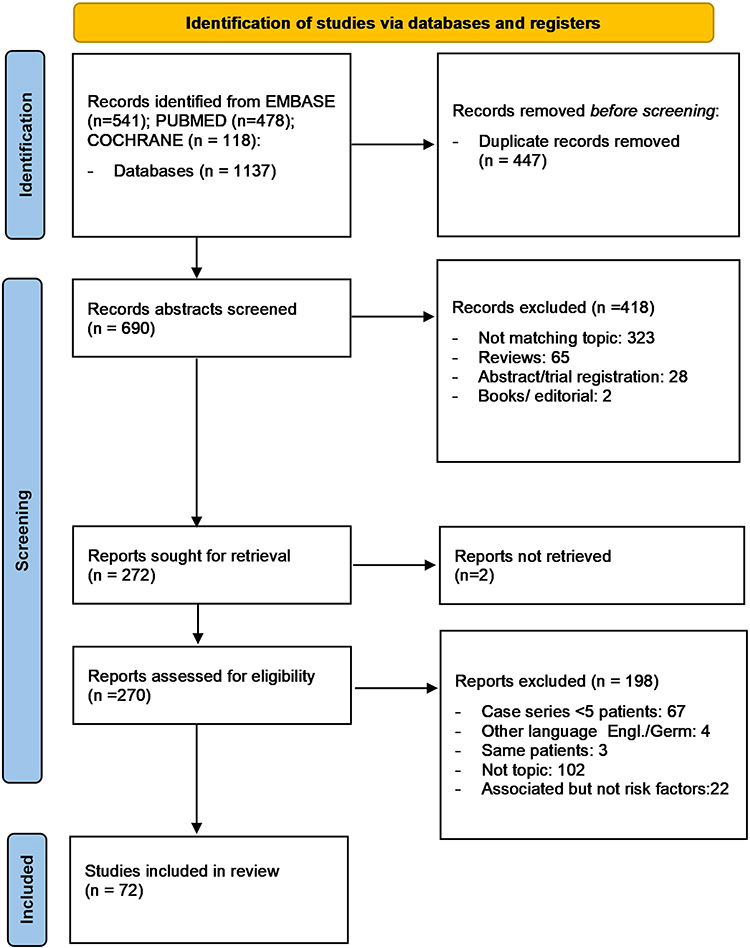 |
Figure 1 Identification of studies via databases. |
Risk Factors
Study Description
There were 12 studies on clinical risk factors of PPP, including 4 case control studies, 2 cross-sectional studies, and 4 cohort studies. There were 3 studies on genetic risk factors and 19 studies describing associated factors, which were excluded. Major risk factors were female sex, smoking, obesity, and thyroid dysfunction (Table 1).
 |
Table 1 Risk Factors for Development of PPP and Disease Severity |
Sex and Lifestyle
Female sex is a predictive risk factor with an 8.8-fold higher risk for PPP (OR 141.7, p<0.0001).16,18 Smoking is another risk factor with a 32.7-fold increased risk for the development of PPP (OR 147.6, p=0.006).7,16,18,19 Smokers were 43–95.23% of the cohorts, and higher package-years and a longer period of smoking were associated with higher risk.7,16,18,19 Smokers were significantly more prevalent in the PPP cohort than the PV cohort.18
Obesity/high body mass index (BMI) is another risk factor for PPP (OR 1.21, p=0.0009).16,17,24 However, it is unclear whether obese people have a higher risk for the development of PPP than PV, with higher risk reported in a cross-sectional study but not in a case-control study.7,24 Disease severity (PPPASI) is predicted by BMI (p=0.0444).17 Other alimentary risk factors are listed in Table 1.17 Insulin resistance was not a risk factor.16 Heavy drinkers had a lower risk for the development of PPP than PV.18 Menopause and pregnancy did not influence PPP.7
Medication and Comorbidities
The use of tumor necrosis factor (TNF)-α inhibitors, including infliximab, adalimumab, and etanercept, is a risk factor for the development of psoriasiform lesions (mainly PPP).19–22 In cohort studies, 1.56% of patients developed psoriasiform lesions, and 0.12% developed PPP.20,22 In the cohort of patients with TNF-α-induced psoriasiform lesions, 41–71.3% of the lesions were PPP.19,20 TNF-α-induced non-pustular psoriasis had a higher risk of occurring than PPP, but PPP had a higher relative risk (HR 6.5, p<0.001).22 In contrast to PPP occurring independently of TNF-α inhibitors, TNF-α-induced PPP was more common in men (HR 19.682) and younger patients (HR 14.318).21
Thyroid dysfunction and elevated anti-TPO levels are also possible risk factors (OR 5.4, p=0.004 and OR 4.2, p=0.025) compared to control patients and patients with PV.7,16,18 A positive patch test, especially for nickel, chlorides, and fragrances, is significantly more common in patients with PPP than those with PV.7 Kim et al described nail involvement as a risk factor for higher PPP severity.18
Treatment
Study Description
Of the 63 studies analyzed, 21 were randomized controlled trials (RCTs), 12 were retrospective cohort studies, 15 were clinical trials (not controlled), and 5 were case series (≥ 5 patients).
Topical and Intralesional Therapies
Topical clobetasol propionate led to complete clearance of PPP in 1–7 weeks in 18/19 patients in an older study.25 Maxacalcitol ointment showed highly and significantly better improvement compared to a placebo.26 The combination of maxacalcitol and betamethasone butyrate (BBP) ointment led to a significant improvement of PPP and a significantly better improvement of pustules than MBBP alone.27 Triamcinolone acetonide led to complete or near complete clearance of lesions in 5/5 patients after intralesional injection28 and in 63% of patients after topical application under hydrocolloid dressing. A significantly higher rate of clearance was achieved compared to clobetasol propionate.29 An oral rinse with ozone nanobubble water over 6 months led to complete clearance of PPP in 6/7 patients in a case series.30 Adjuvant treatment with jumihaidokuto significantly decreased disease activity.31
Light, Laser, and Radiation Therapies
Two RCTs, three clinical trials, and a retrospective study have reported controversial results about the efficacy of PUVA in PPP. While one RCT demonstrated no significant difference from a placebo, another reported clearance in 12/22 patients after PUVA, whereas no clearance occurred in the placebo group.32,33 Partial or complete response and good or excellent improvement occurred in 46.7% and 10–80% of patients, respectively.34–36 Another clinical trial showed better response on the palms compared to the soles (complete clearance occurred in 31/36 palms but only in 5/34 soles).37
UVA1 has shown good efficacy for PPP with PPASI 75 occurring in 72.6% of patients38 and significant superiority to UVB,39 but it was significantly inferior to PUVA.40 However, after nbUVB treatment, 40% of patients achieved PPASI 75 in another trial.41 The efficacy of excimer laser and light treatment was demonstrated in 3 clinical trials, which achieved PPPASI 50 in 60% of patients and PPPASI 75 in 6/34 patients, respectively. Success regarding PPPASI was dose dependent and ranged from 8.3 to 95%, with 95% being achieved using 6 times the minimal erythema dose (MEDI).42–44 A retrospective study with Grenz rays showed marked improvement in 9/9 patients,45 but an RCT with superficial X-ray therapy showed only little or no effect on PPP46 (Table 2).
 |
Table 2 Laser-and Light Therapies, Topical Treatments, Surgical Interventions, and Other Systemic Therapies |
Tonsillectomy, Dental Fillings, and Dental Infection Control
The effect of tonsillectomy, dental infection control, and removal of dental fillings was examined in 2 retrospective studies. Tonsillectomy led to complete clearance in 78% of patients after 2 years,47 and PPPASI 75 was reached by 84% of patients.48 Removal of dental fillings and control of dental infection led to PPPASI 75 in 11% and 63% of patients, respectively48 (Table 2).
Conventional Therapies
Oral acitretin at 25–55 mg/d has demonstrated a clinical improvement and reduction of pustule count within 3–6 months in two clinical trials, and better results occurred with higher dosage.52,53 In a clinical trial, acitretin at 25–50 mg/d was combined with PUVA and achieved 87% improvement of mPASI, but after cessation of acitretin, all patients relapsed within 2 weeks while continuing PUVA.54 In another clinical trial, this combination therapy led to PPPASI 90 in 90% of patients.55
Alitretinoin at 30 mg/d was not significantly superior to a placebo over 24 weeks in an RCT.56 But in a retrospective study, it was reported to result in a PGA of “almost clear” or “clear” in 4/10 patients, and better results occurred for hyperkeratotic lesions.57 Two RCTs described a significant reduction of pustules compared to a placebo (p< 0.001 and p=0.001, respectively) after 4 and 18 weeks of cyclosporine treatment at 2.5 or 1–4 mg/kg.58,59 Two other clinical trials showed clinical improvement and PPPASI 60 in 45.8% of patients after 15 days to 6 months of treatment with ciclosporin at 3 mg/kg.60,61 Colchicine led to no significant improvement of PPP in 2 RCTs over 6 weeks and 3 months62,63 Dimethylfumarate combined with PUVA resulted in PPPASI 90 in 81.8% of patients at week 38 in one clinical trial, and there was no significant difference from treatment using acitretin + PUVA.55 (Table 3).
 |
Table 3 Conventional Therapies for the Treatment of PPP |
Further Systemic Therapies
Liarozole improved PPPASI significantly over 12 weeks in an RCT.51 Itraconazole was demonstrated to lead to a complete clearance of pustules in 3/6 patients over 8 weeks, but relapse occurred quickly after cessation.49 The antibiotic clomocycline had a significantly higher number of responders compared to a placebo over 3 months in an RCT.50
Biologics and Small Molecules
The effect of the IL23 inhibitors guselkumab, risankizumab, and tildrakizumab was investigated in a retrospective study, which led to PPPASI 75 in 25% of patients after 12 weeks and in 43.8% of patients after one year of treatment.65 In 3 RCTs, guselkumab showed good efficacy with PPPASI 50 achieved by 60% of patients and PPPASI 75 achieved by 11.5–20.4% of patients at week 16. At weeks 52 and 84, PPPASI 75 was achieved by 55.6–59.6% and 71.4% of patients, respectively.66–68 The response to a 200-mg dose of guselkumab was no better than that of a 100-mg dose at week 16.67,68
The long-term effect of the IL-17 antagonist secukinumab has been demonstrated in an RCT, and PPPASI 75 occurred in 26.6% of patients at week 16, 41.8% (300 mg) and 35.0% (150 mg) of patients at week 52, and 75–100% of patients at week 148.69,70 In a retrospective cohort study, 47% of patients were responders at 32 months, and 100% of patients were responders after 18 and 24 months.71 The effect of the IL-12/23-antagonist ustekinumab is controversial and showed no significant difference in the rate of PPPASI 50 achieved at week 16 in an RCT.72 But clearance occurred in 5/9 patients and 5/5 patients, complete or partial response occurred in 45% of patients, and PPPASI 75 occurred in 4/9 patients in 2 retrospective cohort studies and 2 case series.73–76
Etanercept led to a significantly higher PPPASI reduction compared to the control group in an RCT.77 In another RCT, 2 different doses of the IL-36 inhibitor spesolimab were not significantly more effective than a placebo. Other retrospective studies examining different biologics and conventional therapies are listed in Table 4.78,79
 |
Table 4 Biologics and Small Molecules for the Treatment of PPP |
Alefacept at 15–30 mg/week led to PSI 50 in 10/14 patients, PPPASI 50 in 53.3% of patients, and PPPASI 75 in 26.7% of patients in two clinical trials.13,82 Anakinra was not superior to a placebo in an RCT.88 The phosphodiesterase 4 inhibitor apremilast showed PPPASI 50 in 61.9% and PPPASI 75 in 14.3% of patients after 20 weeks in a clinical trial,84 as well as a significant PPPASI reduction after 2 weeks in a retrospective study.85 Furthermore, a case series and a clinical trial showed a reduction in PGA after 18 months86 and a reduction in serum levels of IL-19 after 20 weeks.83
Discussion
PPP is a still a very challenging chronic inflammatory disease. Its pathogenesis is not fully understood yet, and knowledge of proven predictive risk factors is limited. Although the therapies for psoriasis have shown impressive improvements, there has been no breakthrough treatment option for PPP. Several genetic alterations have been found, such as mutations in the CARD14, AP1S3, and ATG16 L1 genes, as well as the IL36RN gene (2–14.3%), although the latter is controversial.1,3 Furthermore, variations of genes in the IL-19 subfamily of cytokines and TNFβ2 have been hypothesized to influence susceptibility to PPP, and 2 bins with 5 different genes (LOC 100129540, MIR599, MIR875, RASGRF1, and VPS13B) have been suggested to be associated with higher risk for the development of PPP under TNF-α inhibitor therapy.71,89–91
Many conditions and drugs have been associated with PPP. These include increased IgA antibodies against gliadin, moderate to severe anxiety (p<0.001), dysbiosis of the oral biota, infections of the oral cavity (mainly the tonsils), thyroid disease, metabolic syndrome, arthritis (such as pustulotic arthro-osteitis or psoriatic arthritis), and PV.18,84,92–101 PPP has also been identified as a predictor for the development of psoriatic arthritis in patients with psoriasis.102 However, some authors separate palmoplantar pustular psoriasis from palmoplantar pustulosis in cases of psoriatic features such as plaques, generalized pustules, psoriatic arthritis, or a positive family history of psoriasis. Thus, the association of PPP with psoriasis features is difficult to describe.3,4 In our review, we focused on risk factors instead of associated factors.
Women have an 8.8-fold higher risk for the development of PPP, but hormonal changes such as menopause and pregnancy do not influence the risk.7 Interestingly, in the case of TNF-α-inhibitor-induced PPP, there is a predominance of males.21 The most relevant lifestyle factor is smoking. Smokers have a 32.7-fold increased risk for the development of PPP, and ex-smokers also have increased risk. The duration and amount of smoking influence the risk and disease severity.7,16,101,103 Quitting smoking leads to a clinical improvement of PPP (p=0.007) and improves treatment efficacy.9,104
The pathomechanism regarding smoking is not fully understood, but the following factors have been considered. Nicotine accumulates in the sweat glands of smokers and stimulates neutrophils to produce IL-8.105 Furthermore, PPP lesions of smokers have shown alterations in keratinocyte nicotinic acetylcholine receptors, and 42% of patients with PPP were found to have elevated serum levels of nicotinic acetylcholine receptor antibodies.105,106 The effects of cigarette smoke on the IL-17/IL-36 axis could also be involved in the pathogenesis of PPP.107 Kobayashi et al demonstrated that cigarette smoke can enhance the expression of IL-17A-induced cytokines, including IL-8 and IL-36 in the tonsillar epithelium.103,107
The second lifestyle factors influencing the risk of development of PPP are high BMI and obesity. Obese patients have a higher risk for the development and higher severity of PPP, but there is controversy about whether the risk is higher for PPP than other variants of psoriasis.16,17,24 Thyroid dysfunction seems to be associated with an increased risk for PPP.16,24 In contrast, the suspected association with increased IgA antibodies against gliadin is controversial.7,94 A positive patch test (mainly for nickel chloride and fragrances) has been found in 30.77% of patients in a cohort with PPP.7 Nakamura et al described an exacerbation of pustules and increased levels of leukotriene B4 in pustules and serum, as well as at 48 h after a metal patch test in 7 PPP patients with a positive patch test for certain metals.108 This could indicate that metal allergies increase the risk of flare-up of PPP.
Under treatment with TNF-α inhibitors, paradoxical psoriasiform lesions occur in 1.56% of treated patients or 2–5% according to a recently published review about biological-induced PPP.109 Although non-pustular variants are the most frequent paradoxical reaction, the relative risk of development of PPP is the highest.22 In cohorts of patients treated with TNF-α inhibitors, PPP appeared in 0.12–0.66% of patients with a mean onset after 6 months of treatment.22,110 After treatment, 80% had a relapse with a second TNF-α inhibitor.110
One possible explanation is that TNF-α inhibition leads to specific patients having a higher expression of INF-α, resulting in T-cell activation and higher release of TNF-α.109 Others have hypothesized that an overexpression of CXCR3 occurs with recruitment of auto-reactive T cells and increased release of INF-α.109 Adalimumab and infliximab followed by etanercept are the most frequently reported causative TNF-α inhibitors.19 However, there are also reports about certolizumab and other biologics, including secukinumab, brodalumab, ustekinumab, rituximab, atezolizumab, and tocilizumab, as well as the JAK inhibitors tofacitinib and baricitinib.111–117 Smoking is a risk factor for the development of paradoxical PPP, but interestingly, it is not a risk factor for other paradoxical psoriasiform lesions.19 Paradoxical PPP differs from classic PPP in some ways. The risk is higher among men and younger patients, and DLQI is higher than in classic PPP.21,118
The efficacy of therapies for PPP is difficult to compare as the endpoints and cohort selection of different studies vary in treatment duration, disease severity, and previous treatment. Topical steroids such as clobetasol propionate ointment, betamethasone butyrate propionate ointment, and triamcinolone acetonide applied intralesionally or under occlusion have shown good efficacy, leading to complete clearance in 21–100% of patients.25,27–29 Maxacalcitol ointment can improve lesions significantly and enhance the effect of betamethasone butyrate propionate ointment.26,27
Phototherapy has an advantage of lacking systemic side effects and has been used for decades for the treatment of PPP. Among phototherapies, PUVA is the most efficient treatment.35,38–40,119 Although one RCT showed no better improvement compared to a placebo, several other trials showed moderate to excellent response in the majority of patients.32,35,38–40,119 PUVA is superior to UVA1 and UVBnb and is more efficient on the palms than the soles.35,37–40,119 Excimer laser can improve PPP, especially with higher dose regimes.44
Among systemic therapies, retinoids are the most commonly used, especially acitretin in recent decades. Acitretin has shown good efficacy in several clinical trials, especially at higher doses, but relapse occurs after cessation. It may also increase the efficacy of PUVA.53,54 The effect of alitretinoin has to be investigated more precisely as the results are controversial. It seems to mainly affect hyperkeratotic lesions.56,57 Ciclosporin A seems to have good and fast efficacy for the treatment of PPP, but relapse can occur after cessation, and due to side effects, long-term treatments are not always optimal.58,59
In a retrospective study, Kromer et al demonstrated the response of PPP to conventional therapies with the best efficacy. PPPASI 75 was achieved in 51.4% of patients with ciclosporin, 22.6% with alitretinoin, 19.5% with acitretin, 17.7% with fumaric acid, and 16.8% with methotrexate.79 In this analysis, ciclosporin reached PPASI `75 at comparable rates to those of apremilast (31.4%), infliximab (40.6%), adalimumab (33.3%), certolizumab (62.5), golimumab (41.7%), secukinumab (29%), and ustekinumab (31%).79 The oral selective phosphodiesterase 4 inhibitor apremilast has been shown to be fast (2 weeks) and to have long-term efficacy (18 months) in case series.85,86 However, a clinical trial showed the achievement of PPPASI 50 in 61.9% and PPPASI 75 in 14.3% of patients after 20 weeks of treatment, which do not seem to be superior to the results of conventional therapies described thus far.84 Nevertheless, apremilast had the longest drug survival among non-biologic agents in a retrospective analysis by Kromer et al.79
In a very recent phase-2 RCT that was published after the literature screening for this review, apremilast showed improved results with achievement of PPPASI 50 in 78.3% of patients at week 16, which was significantly higher compared to the results of a placebo (P = 0.0003). PPPASI 75 was achieved by 43.5% of patients.120 These findings are comparable with the results of biologics. Among biologics, a recombinant interleukin (IL)-1 receptor antagonist, anakinra, has demonstrated good effectiveness in neutrophilic dermatosis by blocking the activity of IL-1a and IL-1b. These two cytokines have been repeatedly linked to neutrophil activation and extravasation. However, anakinra has failed to show effectiveness in PPP.88
Among small molecules, Janus kinase (JAK) inhibitors are being examined for the treatment of various inflammatory skin diseases. Due to a lack of clinical trials, we did not include them in the result section, but tofacitinib (a JAK 1/2 inhibitor) has shown impressive improvement of PPP in 5 cases, and baricitinib (a JAK 1/3 inhibitor) has been used in 1 case of PPP and in cases of resistance to biologics and paradoxical PPP.121–124 In a review, Gleeson et al suggested that tofacitinib may be beneficial for PPP and could be considered for patients with an acceptable comorbidity indication. However, routine use cannot be recommended due to the limited evidence and uncertain safety profile of JAK inhibitors.125
Despite the observed side effects of paradoxical PPP, TNF-α inhibitors have been successfully used for the treatment of PPP.78,126 In a retrospective analysis, Husson et al found no difference in the percentage of complete clearance between TNF-α inhibitors, with 13.3% clearance achieved using etanercept, 17.6% achieved using adalimumab, and 19.0% achieved using infliximab.78 In the case of TNF-α-induced PPP, a review by Li et al suggested that possible considerations include a treat-through strategy (resolution in 26–41% of cases), switching to another TNF-α inhibitor, or switching to another conventional or biologic therapy.127
The therapeutic effects of IL-17 and IL-23 blockers have been investigated due to findings supporting the importance of the IL23-TH17 axis in the pathogenesis of PPP. Patients with PPP have shown an increased level of IL-17A in the acrosyringium of the palms and soles, increased IL-17 serum levels, and increased mRNA encoding IL-17, IL-22, IL-23, and IL-8 in the lesional skin of PPP patients.2,70,128 Among biologic agents, the anti-IL-23 antibody guselkumab is the first to be approved for the treatment of PPP in Japan.2 In 3 RCTs, guselkumab was significantly superior to a placebo at week 16, at which it achieved PPPASI 50 in 60% of cases and PPASI 75 in 11.5–20.4% of cases. The efficacy increased over time, with PPASI 75 occurring in 55.6-59.6% of cases at week 52 and 61.9-81.4% of cases at week 84.66–68 Patients who received prior phototherapy or non-biologic therapies had a tendency toward worse response, and non-smokers tended to sustain efficacy for a longer time.66 An RCT evaluating the efficacy of risankizumab, another IL-23 inhibitor, is under way.129
Ustekinumab at 45 mg was not superior to placebo at week 16 in an RCT.72 However, retrospective studies and case series with longer observation periods showed complete or partial clearance in 44–100% of patients, suggesting a need for further long-term trials. Secukinumab has demonstrated a fast response (16 weeks) and long-term effect (148 weeks) in 2 RCTs.69,70 The effect of brodalumab, another IL-17 inhibitor, is still under investigation. The IL-1 inhibitor anakinra does not seem to be efficient for the treatment of PPP.130
Regarding IL-36 inhibitors, spesolimab showed no significant superiority to a placebo in an RCT, and imsidolimab did not induce any relevant improvement in a single case.81,131 In case reports, the effectiveness of dupilumab, brodalumab, and vedolizumab has been suggested, but there is a lack of evidence in the literature.132–134 Recently, RIST 4721, a CXC chemokine receptor type 2 (CXCR2) inhibitor, was investigated for the treatment of PPP in a phase-2A study. RIST 4721 is hypothesized to prevent neutrophil migration by blocking CXCR2 ligands including IL-8, but it was not significantly superior to a placebo.135 Another trial is under way. Its potential efficacy could not be excluded in a subgroup analysis.135 New therapies such as the TYK2 inhibitor deucravacitinib are being examined.136
Conclusion
Compared to the large list of known factors associated with PPP, little is known about real risk factors for the development of PPP and its severity. Smoking remains the most obvious risk factor, and the fact that PPP improves after cessation should motivate patients to stop smoking. The second lifestyle factor influencing not only the risk of development but also disease severity of PPP is obesity. Therefore, patients should be motivated to achieve a normal BMI. Regarding therapies, topical therapies and phototherapies can result in good improvement in some cases and remain as the first-line therapy. As a second step, retinoids can be prescribed. In cases of side-effects or non-response, conventional therapies such as ciclosporin can show good efficacy, but they are limited by long-term side-effects and immediate relapse after cessation. In these cases, biologics (namely TNF-α-inhibitors, IL-17 and IL-23 blockers, and apremilast) can show good effectiveness in some patients. Due to the lack of comparative trials, however, it is difficult to name a preferable biologic. IL-17 inhibitors and IL-23 inhibitors have shown good results, but they are used off-label in most countries. An advantage for the IL-23-inhibitor guselkumab could be that it is licensed for PPP in Japan. In general, treatments with biologics should be continued over 1 year in cases of partial response as the efficacy increases with the duration of treatment, and the response is rather slow compared to that of PV. Recent case reports about JAK inhibitors show promising results, but clinical trials and comparative trials with well-established treatments are needed.
Funding
There is no funding to report.
Disclosure
Dr Kristine Heidemeyer reports personal fees from Sanofi, Amgen, Almirall, UCB, and Abbvie, outside the submitted work. Prof. Dr. Nikhil Yawalkar reports personal fees from Abbvie, Almirall, Amgen, Boehringer Ingelheim, Celgene, MSD, Janssen, Leo, Lilly, Novartis, Pfizer, and UCB, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Brunasso AMG, Massone C. Recent advances in palmoplantar pustulosis. Fac Rev. 2021;10:62. doi:10.12703/r/10-62
2. Murakami M. Guselkumab for the treatment of palmoplantar pustulosis. Expert Opin Biol Ther. 2020;20(8):841–852. doi:10.1080/14712598.2020.1760244
3. Navarini AA, Burden AD, Capon F, et al. European consensus statement on phenotypes of pustular psoriasis. J Eur Acad Dermatol Venereol. 2017;31(11):1792–1799. doi:10.1111/jdv.14386
4. Misiak-Galazka M, Zozula J, Rudnicka L. Palmoplantar Pustulosis: recent Advances in Etiopathogenesis and Emerging Treatments. Am J Clin Dermatol. 2020;21(3):355–370. doi:10.1007/s40257-020-00503-5
5. Xu JM, Wang HM, Jin HZ. An update on therapeutic options for palmoplantar pustulosis: a narrative review and expert recommendations. Expert Rev Clin Immunol. 2023;19(5):499–516. doi:10.1080/1744666X.2023.2185775
6. Andersen YMF, Augustin M, Petersen J, et al. Characteristics and prevalence of plaque psoriasis in patients with palmoplantar pustulosis. Br J Dermatol. 2019;181(5):976–982. doi:10.1111/bjd.17832
7. Misiak-Galazka M, Wolska H, Galazka A, Kwiek B, Rudnicka L. General Characteristics and Comorbidities in Patients with Palmoplantar Pustulosis. Acta Dermatovenerol Croat. 2018;26(2):109–118.
8. Yamamoto T. Pustulotic arthro-osteitis associated with palmoplantar pustulosis. J Dermatol. 2013;40(11):857–863. doi:10.1111/1346-8138.12272
9. Fukasawa T, Yoshizaki-Ogawa A, Enomoto A, Miyagawa K, Sato S, Yoshizaki A. Involvement of Molecular Mechanisms between T/B Cells and IL-23: from Palmoplantar Pustulosis to Autoimmune Diseases. Int J Mol Sci. 2022;23(15):8261. doi:10.3390/ijms23158261
10. Xiaoling Y, Chao W, Wenming W, Feng L, Hongzhong J. Interleukin (IL)-8 and IL-36γ but not IL-36Ra are related to acrosyringia in pustule formation associated with palmoplantar pustulosis. Clin Exp Dermatol. 2019;44(1):52–57. doi:10.1111/ced.13689
11. Paik K, Kim BR, Youn SW. Evaluation of the area subscore of the Palmoplantar Pustulosis Area and Severity Index using an attention U-net deep learning algorithm. J Dermatol. 2023;50(6):787–792. doi:10.1111/1346-8138.16752
12. Nagendran A, Hanumanthu V, Dogra S, Narang T, Venkata Maha Pinnaka L. Validation and usability of modified palmoplantar psoriasis area and severity index in patients with palmoplantar psoriasis: a prospective longitudinal cohort study. Indian J Dermatol Venereol Leprol. 2023;1–8. doi:10.25259/IJDVL_712_2022
13. Carr D, Tusa MG, Carroll CL, et al. Open label trial of alefacept in palmoplantar pustular psoriasis. J Dermatol Treatment. 2008;19(2):97–100. doi:10.1080/09546630701364776
14. Benzaquen M, Munshi M, Bossart S, et al. Long-Term Dose Optimization of Adalimumab via Dose Spacing in Patients with Psoriasis. Bioengineering. 2022;9(8). doi:10.3390/bioengineering9080387
15. Shear NH, Betts KA, Soliman AM, et al. Comparative safety and benefit-risk profile of biologics and oral treatment for moderate-to-severe plaque psoriasis: a network meta-analysis of clinical trial data. J Am Acad Dermatol. 2021;85(3):572–581. doi:10.1016/j.jaad.2021.02.057
16. Ataş H, Gönül M. Insulin resistance, diabetes mellitus and thyroid dysfunction in patients with palmoplantar pustulosis: a case-controlled study. Postepy Dermat Alergologii. 2017;34(3):268–272. doi:10.5114/pdia.2016.61630
17. Serizawa N, Okazaki S, Otsuka Y, et al. Dietary habits in Japanese patients with palmoplantar pustulosis. J Dermatol. 2021;48(3):366–375. doi:10.1111/1346-8138.15719
18. Kim DH, Lee JY, Cho SI, Jo SJ. Risks of Comorbidities in Patients With Palmoplantar Pustulosis vs Patients With Psoriasis Vulgaris or Pompholyx in Korea. JAMA Dermatol. 2022;158(6):650–660. doi:10.1001/jamadermatol.2022.1081
19. Mazloom SE, Yan D, Hu JZ, et al. TNF-α inhibitor-induced psoriasis: a decade of experience at the Cleveland Clinic. J Am Acad Dermatol. 2020;83(6):1590–1598. doi:10.1016/j.jaad.2018.12.018
20. López-Robles A, Queiro R, Alperi M, Alonso S, Riestra JL, Ballina J. Psoriasis and psoriasiform lesions induced by TNFα antagonists: the experience of a tertiary care hospital from northern Spain. Rheumatol Int. 2012;32(12):3779–3783. doi:10.1007/s00296-011-2265-4
21. Bae JM, Lee HH, Lee BI, et al. Incidence of psoriasiform diseases secondary to tumour necrosis factor antagonists in patients with inflammatory bowel disease: a nationwide population-based cohort study. Aliment Pharmacol Ther. 2018;48(2):196–205. doi:10.1111/apt.14822
22. Thein D, Egeberg A, Skov L, Loft N. Absolute and Relative Risk of New-Onset Psoriasis Associated With Tumor Necrosis Factor-α Inhibitor Treatment in Patients With Immune-Mediated Inflammatory Diseases: a Danish Nationwide Cohort Study. JAMA Dermatol. 2022;158(9):997–1004. doi:10.1001/jamadermatol.2022.2360
23. Kim M, Yang S, Kim BR, Youn SW. Nail involvement features in palmoplantar pustulosis. J Dermatol. 2021;48(3):360–365. doi:10.1111/1346-8138.15716
24. Kim YC, Lee ES, Chung PS, Rhee CK. Recalcitrant palmoplantar pustular psoriasis successfully treated with topical 5-aminolaevulinic acid photodynamic therapy [14]. Clin Exp Dermatol. 2005;30(6):723–724. doi:10.1111/j.1365-2230.2005.01905.x
25. Volden G. Successful treatment of chronic skin diseases with clobetasol propionate and a hydrocolloid occlusive dressing. Acta Derm Venereol. 1992;72(1):69–71. doi:10.2340/00015555726971
26. Umezawa Y, Nakagawa H, Tamaki K. Phase III clinical study of maxacalcitol ointment in patients with palmoplantar pustulosis: a randomized, double-blind, placebo-controlled trial. J Dermatol. 2016;43(3):288–293. doi:10.1111/1346-8138.13064
27. Muro M, Kawakami H, Matsumoto Y, Abe N, Tsuboi R, Okubo Y. Topical combination therapy with vitamin D3 and corticosteroid ointment for palmoplantar pustulosis: a prospective, randomized, left-right comparison study. J Dermatolog Treat. 2016;27(1):51–53. doi:10.3109/09546634.2015.1052036
28. Goette DK, Morgan AM, Fox BJ, Horn RT. Treatment of palmoplantar pustulosis with intralesional triamcinolone injections. Arch Dermatol. 1984;120(3):319–323. doi:10.1001/archderm.1984.01650390041008
29. Kragballe K, Larsen FG. A hydrocolloid occlusive dressing plus triamcinolone acetonide cream is superior to clobetasol cream in palmo-plantar pustulosis. Acta Derm Venereol. 1991;71(6):540–542. doi:10.2340/0001555571540542
30. Horiuchi Y. Palmoplantar pustulosis treated with oral rinse using ozone nanobubble water: a case series. Dermatol Ther. 2020;33(6). doi:10.1111/dth.13924
31. Mizawa M, Makino T, Inami C, Shimizu T. Jumihaidokuto (Shi-Wei-Ba-Du-Tang), a kampo formula, decreases the disease activity of palmoplantar pustulosis. Dermatol Res Pract. 2016;2016:1–4. doi:10.1155/2016/4060673
32. Layton AM, Sheehan-Dare R, Cunliffe WJ. A double-blind, placebo-controlled trial of topical PUVA in persistent palmoplantar pustulosis. Br J Dermatol. 1991;124(6):581–584. doi:10.1111/j.1365-2133.1991.tb04955.x
33. Murray D, Warin AP. Photochemotherapy for persistent palmoplantar pustulosis (PPP) [proceedings]. Br J Dermatol. 1979;101(Suppl 17):13–14.
34. Jansén CT, Malmiharju T. Inefficacy of topical methoxalen plus UVA for palmoplantar pustulosis. Acta Derm Venereol. 1981;61(4):354–356. doi:10.2340/0001555561354356
35. Paul R, Jansén CT. Suppression of palmoplantar pustulosis symptoms with oral 8-methoxypsoralen and high-intensity UVA irradiation. Dermatologica. 1983;167(5):283–285. doi:10.1159/000249798
36. Riad K, Felix P, Dorit S, Gregory K, Nadim K, Henri T. The use of topical PUVA for palmoplantar dermatoses. J Dermatolog Treat. 2006;17(5):304–307. doi:10.1080/09546630600866442
37. Agren-Jonsson S, Tegner E. PUVA therapy for palmoplantar pustulosis. Acta Derm Venereol. 1985;65(6):531–535. doi:10.2340/0001555565531535
38. Su LN, Xu X, Tang L, Yu N, Ding YF. UVA1 phototherapy in the treatment of palmoplantar pustulosis: a pilot prospective study. Lasers Med Sci. 2016;31(8):1641–1643. doi:10.1007/s10103-016-2031-7
39. Su LN, Ren J, Cheng SM, Liu JL, Ding YF, Zhu NW. UVA1 vs. narrowband UVB phototherapy in the treatment of palmoplantar pustulosis: a pilot randomized controlled study. Lasers Med Sci. 2017;32(8):1819–1823. doi:10.1007/s10103-017-2280-0
40. Engin B, Oguz O. Evaluation of time-dependent response to psoralen plus UVA (PUVA) treatment with topical 8-methoxypsoralen (8-MOP) gel in palmoplantar dermatoses. Int J Dermatol. 2005;44(4):337–339. doi:10.1111/j.1365-4632.2004.02153.x
41. Kawada A, Matsuda H, Oiso N. Efficacy and safety of targeted narrowband ultraviolet B therapy using a flat-type fluorescent lamp for the treatment of palmoplantar pustulosis. J Dermatol. 2013;40(9):754–755. doi:10.1111/1346-8138.12228
42. Fumimori T, Tsuruta D, Kawakami T, Ohata C, Furumura M, Hashimoto T. Effect of monochromatic excimer light on palmoplantar pustulosis: a clinical study performed in a private clinic by a dermatological specialist. J Dermatol. 2013;40(12):1004–1007. doi:10.1111/1346-8138.12302
43. Furuhashi T, Torii K, Kato H, Nishida E, Saito C, Morita A. Efficacy of excimer light therapy (308 nm) for palmoplantar pustulosis with the induction of circulating regulatory T cells. Exp Dermatol. 2011;20(9):768–770. doi:10.1111/j.1600-0625.2011.01316.x
44. Peng C, Hu Y, Chen W, et al. A randomized prospective study of different dose regimens using the 308-nm excimer laser in the treatment of palmoplantar pustulosis. Dermatol Ther. 2021;34(5):e15079. doi:10.1111/dth.15079
45. Fenton L, Dawe RS. Six years’ experience of grenz ray therapy for the treatment of inflammatory skin conditions. Clin Exp Dermatol. 2016;41(8):864–870. doi:10.1111/ced.12960
46. Fairris GM, Jones DH, Mack DP, Rowell NR. Superficial X-ray therapy in the treatment of palmoplantar pustulosis. Br J Dermatol. 1984;111(4):499–500. doi:10.1111/j.1365-2133.1984.tb06615.x
47. Takahara M, Hirata Y, Nagato T, et al. Treatment outcome and prognostic factors of tonsillectomy for palmoplantar pustulosis and pustulotic arthro-osteitis: a retrospective subjective and objective quantitative analysis of 138 patients. J Dermatol. 2018;45(7):812–823. doi:10.1111/1346-8138.14348
48. Kouno M, Nishiyama A, Minabe M, et al. Retrospective analysis of the clinical response of palmoplantar pustulosis after dental infection control and dental metal removal. J Dermatol. 2017;44(6):695–698. doi:10.1111/1346-8138.13751
49. V’Lckova-Laskoska MT, Caca-Biljanovska NG, Laskoski DS, Kamberova SJ. Palmoplantar pustulosis treated with itraconazole: a single, active-arm pilot study. Dermatol Ther. 2009;22(1):85–89. doi:10.1111/j.1529-8019.2008.01219.x
50. Ward JM, Corbett MF, Hanna MJ. A double-blind trial of clomocycline in the treatment of persistent palmoplantar pustulosis. Br J Dermatol. 1976;95(3):317–322. doi:10.1111/j.1365-2133.1976.tb07020.x
51. Bhushan M, Burden AD, McElhone K, James R, Vanhoutte FP, Griffiths CEM. Oral liarozole in the treatment of palmoplantar pustular psoriasis: a randomized, double-blind, placebo-controlled study. Br J Dermatol. 2001;145(4):546–553. doi:10.1046/j.1365-2133.2001.04411.x
52. Lassus A, Geiger JM. Acitretin and etretinate in the treatment of palmoplantar pustulosis: a double-blind comparative trial. Br J Dermatol. 1988;119(6):755–759. doi:10.1111/j.1365-2133.1988.tb03499.x
53. van de Kerkhof PC, Chang A, van Dooren-Greebe R, Geiger JM, Happle R. Intra-epidermal accumulation of polymorphonuclear leukocytes in persistent palmoplantar pustulosis during treatment with Acitretin. Acta Derm Venereol. 1988;68(6):
54. Ettler K, Benakova N, Zimova V. Acitretin therapy of palmoplantar pustulosis combined with UV-a and 8- MOP topically. Cesko-Slovenska Dermatologie. 1999;74(4):150–152.
55. Aichelburg MC, Pinkowicz A, Holzer G, Radakovic S, Sator PG, Tanew A. Short- and long-term efficacy of fumaric acid esters or Acitretin in combination with a 12-week course of PUVA in the treatment of palmoplantar pustulosis: results from a prospective randomized trial. J Eur Acad Dermatol Venereol. 2021;35(3):
56. Reich K, Graff O, Mehta N. Oral alitretinoin treatment in patients with palmoplantar pustulosis inadequately responding to standard topical treatment: a randomized Phase II study. Br J Dermatol. 2016;174(6):1277–1281. doi:10.1111/bjd.14401
57. Lee JS, Park HS, Yoon HS, Cho S. Efficacy and Safety of Oral Alitretinoin in Hand Eczema and Palmoplantar Pustulosis in Korean Patients. Ann Dermatol. 2019;31(2):139–145. doi:10.5021/ad.2019.31.2.139
58. Erkko P, Granlund H, Remitz A, et al. Double-blind placebo-controlled study of long-term low-dose cyclosporin in the treatment of palmoplantar pustulosis. Br J Dermatol. 1998;139(6):997–1004. doi:10.1046/j.1365-2133.1998.02555.x
59. Reitamo S, Erkko P, Remitz A, Lauerma AI, Montonen O, Harjula K. Cyclosporine in the treatment of palmoplantar pustulosis. A randomized, double-blind, placebo-controlled study. Arch Dermatol. 1993;129(10):1273–1279. doi:10.1001/archderm.1993.01680310043006
60. Jin XH, Chen X, Mou Y, Xia JX. Effects of Cyclosporine on Palmoplantar Pustulosis and Serum Expression of IL-17, IL-23, and TNF-α. Dermatol Ther (Heidelb). 2019;9(3):547–552. doi:10.1007/s13555-019-0308-z
61. Remitz A, Lauerma AI, Erkko P, Reitamo S. Delayed-type hypersensitivity in palmoplantar pustulosis: effect of cyclosporin A treatment on skin testing with recall antigens. Acta Derm Venereol. 1996;76(4):310–313. doi:10.2340/0001555576310313
62. English JS, Fenton DA, Wilkinson JD. Failure of colchicine for palmo-plantar pustulosis. Clin Exp Dermatol. 1983;8(2):207–208. doi:10.1111/j.1365-2230.1983.tb01770.x
63. Mann RJ. Failure of colchicine for palmo-plantar pustulosis. Br J Dermatol. 1982;106(3):373. doi:10.1111/j.1365-2133.1982.tb01740.x
64. Ettler K, Richards B. Acitretin therapy for palmoplantar pustulosis combined with UVA and topical 8-MOP. Int J Dermatol. 2001;40(8):541–542. doi:10.1046/j.1365-4362.2001.01094-3.x
65. Poortinga S, Balakirski G, Kromer C, et al. The challenge of palmoplantar pustulosis therapy: are Interleukin-23 inhibitors an option? J Eur Acad Dermatol Venereol. 2021;35(12):e907–e911. doi:10.1111/jdv.17560
66. Okubo Y, Morishima H, Zheng R, Terui T. Sustained efficacy and safety of guselkumab in patients with palmoplantar pustulosis through 1.5 years in a randomized Phase 3 study. J Dermatol. 2021;48(12):1838–1853. doi:10.1111/1346-8138.16132
67. Terui T, Kobayashi S, Okubo Y, Murakami M, Hirose K, Kubo H. Efficacy and Safety of Guselkumab, an Anti-interleukin 23 Monoclonal Antibody, for Palmoplantar Pustulosis: a Randomized Clinical Trial. JAMA Dermatol. 2018;154(3):309–316. doi:10.1001/jamadermatol.2017.5937
68. Terui T, Kobayashi S, Okubo Y, et al. Efficacy and Safety of Guselkumab in Japanese Patients With Palmoplantar Pustulosis: a Phase 3 Randomized Clinical Trial. JAMA Dermatol. 2019;155(10):1153–1161. doi:10.1001/jamadermatol.2019.1394
69. Mrowietz U, Bachelez H, Burden AD, et al. Secukinumab for moderate-to-severe palmoplantar pustular psoriasis: results of the 2PRECISE study. J Am Acad Dermatol. 2019;80(5):1344–1352. doi:10.1016/j.jaad.2019.01.066
70. Mrowietz U, Bachelez H, Burden AD, et al. Efficacy and safety of secukinumab in moderate to severe palmoplantar pustular psoriasis over 148 weeks: extension of the 2PRECISE study. J Am Acad Dermatol. 2021;84(2):552–554. doi:10.1016/j.jaad.2020.06.038
71. Reolid A, Sahuquillo-Torralba A, Sanz-García A, et al. CNVs Associated with Different Clinical Phenotypes of Psoriasis and Anti-TNF-Induced Palmoplantar Pustulosis. J Pers Med. 2022;12(9):1452. doi:10.3390/jpm12091452
72. Bissonnette R, Nigen S, Langley RG, et al. Increased expression of IL-17A and limited involvement of IL-23 in patients with palmo-plantar (PP) pustular psoriasis or PP pustulosis; results from a randomised controlled trial. J Eur Acad Dermatol Venereol. 2014;28(10):
73. Buder V, Herberger K, Jacobi A, Augustin M, Radtke MA. Ustekinumab in the treatment of palmoplantar pustular psoriasis – a case series of nine patients. J German Soc Dermatol. 2016;14(11):1109–1115. doi:10.1111/ddg.12825_g
74. Morales-Múnera C, Vilarrasa E, Puig L. Efficacy of ustekinumab in refractory palmoplantar pustular psoriasis. Br J Dermatol. 2013;168(4):820–824. doi:10.1111/bjd.12150
75. Bertelsen T, Kragballe K, Johansen C, Iversen L. Efficacy of ustekinumab in palmoplantar pustulosis and palmoplantar pustular psoriasis. Int J Dermatol. 2014;53(10):e464–466. doi:10.1111/ijd.12511
76. Hegazy S, Konstantinou MP, Bulai Livideanu C, Tauber M, Uthurriague C, Paul C. Efficacy of ustekinumab in palmoplantar pustulosis. J Eur Acad Dermatol Venereol. 2018;32(5):e204–e206. doi:10.1111/jdv.14718
77. Bissonnette R, Poulin Y, Bolduc C, et al. Etanercept in the treatment of palmoplantar pustulosis. J Drugs Dermatol. 2008;7(10):
78. Husson B, Barbe C, Hegazy S, et al. Efficacy and safety of TNF blockers and of ustekinumab in palmoplantar pustulosis and in acrodermatitis continua of Hallopeau. J Eur Acad Dermatol Venereol. 2020;34(10):2330–2338. doi:10.1111/jdv.16265
79. Kromer C, Wilsmann-Theis D, Gerdes S, et al. Drug survival and reasons for drug discontinuation in palmoplantar pustulosis: a retrospective multicenter study. J Dtsch Dermatol Ges. 2019;17(5):503–516.
80. Reolid A, Armesto S, Sahuquillo-Torralba A, et al. Secukinumab is effective in the treatment of recalcitrant palmoplantar psoriasis and palmoplantar pustular psoriasis in a daily practice setting. J Am Acad Dermatol. 2022;87(3):705–709. doi:10.1016/j.jaad.2022.05.047
81. Mrowietz U, Burden AD, Pinter A, et al. Spesolimab, an Anti-Interleukin-36 Receptor Antibody, in Patients with Palmoplantar Pustulosis: results of a Phase IIa, Multicenter, Double-Blind, Randomized, Placebo-Controlled Pilot Study. Dermatol Ther (Heidelb). 2021;11(2):571–585. doi:10.1007/s13555-021-00504-0
82. Guenther LC. Alefacept is safe and efficacious in the treatment of palmar plantar pustulosis. J Cutan Med Surg. 2007;11(6):202–205. doi:10.2310/7750.2007.00036
83. Wolk K, Wilsmann-Theis D, Witte K, et al. Interleukin-19 Levels Are Increased in Palmoplantar Pustulosis and Reduced following Apremilast Treatment. Int J Mol Sci. 2023;24(2):1276. doi:10.3390/ijms24021276
84. Wilsmann-Theis D, Kromer C, Gerdes S, et al. A multicentre open-label study of apremilast in palmoplantar pustulosis (APLANTUS). J Eur Acad Dermatol Venereol. 2021;35(10):2045–2050. doi:10.1111/jdv.17441
85. Kato N, Takama H, Ando Y, et al. Immediate response to apremilast in patients with palmoplantar pustulosis: a retrospective pilot study. Int J Dermatol. 2021;60(5):570–578. doi:10.1111/ijd.15382
86. Ständer S, Syring F, Ludwig RJ, Thaçi D. Successful Treatment of Refractory Palmoplantar Pustular Psoriasis With Apremilast: a Case Series. Front Med. 2020;7. doi:10.3389/fmed.2020.543944
87. Soufila KT, Thakur V, Narang T, Dogra S, Handa S. Apremilast in treatment of palmoplantar pustulosis – a case series. Int J Dermatol. 2021;60(6):e247–e248. doi:10.1111/ijd.15398
88. Cro S, Cornelius VR, Pink AE, et al. Anakinra for palmoplantar pustulosis: results from a randomized, double-blind, multicentre, two-staged, adaptive placebo-controlled trial (APRICOT). Br J Dermatol. 2021;186(2):245–256. doi:10.1111/bjd.20653
89. Kingo K, Mössner R, Kõks S, et al. Association analysis of IL19, IL20 and IL24 genes in palmoplantar pustulosis. Br J Dermatol. 2007;156(4):646–652. doi:10.1111/j.1365-2133.2006.07731.x
90. Hashigucci K, Yokoyama M, Niizeki H, et al. Polymorphism in the tumor necrosis factor B gene is associated with Palmoplantar pustulosis. Tissue Antigens. 1999;54(3):288–290. doi:10.1034/j.1399-0039.1999.540312.x
91. Wang TS, Chiu HY, Hong JB, Chan CC, Lin SJ, Tsai TF. Correlation of IL36RN mutation with different clinical features of pustular psoriasis in Chinese patients. Arch Dermatol Res. 2016;308(1):55–63. doi:10.1007/s00403-015-1611-x
92. Eriksson MO, Hagforsen E, Lundin IP, Michaëlsson G. Palmoplantar pustulosis: a clinical and immunohistological study. Br J Dermatol. 1998;138(3):390–398. doi:10.1046/j.1365-2133.1998.02113.x
93. Kageyama Y, Shimokawa Y, Kawauchi K, et al. Dysbiosis of Oral Microbiota Associated with Palmoplantar Pustulosis. Dermatology. 2021;237(3):347–356. doi:10.1159/000511622
94. Michaëlsson G, Kristjánsson G, Pihl Lundin I, Hagforsen E. Palmoplantar pustulosis and gluten sensitivity: a study of serum antibodies against gliadin and tissue transglutaminase, the duodenal mucosa and effects of gluten-free diet. Br J Dermatol. 2007;156(4):659–666. doi:10.1111/j.1365-2133.2006.07725.x
95. Sáez-Rodríguez M, Noda-Cabrera A, García-Bustínduy M, et al. Palmoplantar pustulosis associated with gastric helicobacter pylori infection [6]. Clin Exp Dermatol. 2002;27(8):720. doi:10.1046/j.1365-2230.2002.01102_6.x
96. Huang CM, Tsai TF. Clinical characteristics, genetics, comorbidities and treatment of palmoplantar pustulosis: a retrospective analysis of 66 cases in a single center in Taiwan. J Dermatol. 2020;47(9):1046–1049.
97. Gimenéz-García R, Sánchez-Ramón S, Cuellar-Olmedo LA. Palmoplantar pustulosis: a clinicoepidemiological study. The relationship between tobacco use and thyroid function. J Eur Acad Dermatol Venereol. 2003;17(3):276–279. doi:10.1046/j.1468-3083.2003.00510.x
98. Guerra I, Algaba A, Pérez-Calle JL, et al. Induction of psoriasis with anti-TNF agents in patients with inflammatory bowel disease: a report of 21 cases. J Crohns Colitis. 2012;6(5):518–523. doi:10.1016/j.crohns.2011.10.007
99. Noe MH, Wan MT, Mostaghimi A, et al. Evaluation of a Case Series of Patients With Palmoplantar Pustulosis in the United States. JAMA Dermatol. 2022;158(1):68–72. doi:10.1001/jamadermatol.2021.4635
100. Olazagasti JM, Ma JE, Wetter DA. Clinical Features, Etiologic Factors, Associated Disorders, and Treatment of Palmoplantar Pustulosis: the Mayo Clinic Experience, 1996-2013. Mayo Clinic Proce. 2017;92(9):1351–1358. doi:10.1016/j.mayocp.2017.05.029
101. Putra-Szczepaniak M, Reich A, Jankowska-Konsur A, Czarnecka A, Bagłaj-Oleszczuk M, Hryncewicz-Gwóźdź A. Pack-year cigarette smoking affects the course of palmoplantar pustulosis. Adv Clin Exp Med. 2021;30(2):189–195. doi:10.17219/acem/131750
102. Heidemeyer K, Cazzaniga S, Dondi L, et al. Variables associated with joint involvement and development of a prediction rule for arthritis in patients with psoriasis. An analysis of the Italian PsoReal database. J Am Acad Dermatol. 2023;89(1):53–61. doi:10.1016/j.jaad.2023.02.059
103. Kobayashi K, Kamekura R, Kato J, et al. Cigarette Smoke Underlies the Pathogenesis of Palmoplantar Pustulosis via an IL-17A-Induced Production of IL-36γ in Tonsillar Epithelial Cells. J Invest Dermatol. 2021;141(6):1533–1541 e1534. doi:10.1016/j.jid.2020.09.028
104. Michaëlsson G, Gustafsson K, Hagforsen E. The psoriasis variant palmoplantar pustulosis can be improved after cessation of smoking. J Am Acad Dermatol. 2006;54(4):737–738. doi:10.1016/j.jaad.2005.07.024
105. Reddy V, Bhutani T. Palmoplantar Pustulosis in Electronic Cigarette Users: a Potential for Concern. Dermatology. 2019;235(6):525–526. doi:10.1159/000503385
106. Hagforsen E, Awder M, Lefvert AK, Nordlind K, Michaëlsson G. Palmoplantar pustulosis: an autoimmune disease precipitated by smoking? Acta Derm Venereol. 2002;82(5):341–346. doi:10.1080/000155502320624069
107. Kobayashi K, Kamekura R, Kamiya S, et al. Effect of cigarette smoke on interleukin-17A- and interleukin-17F-driven skin inflammation: an in vitro study. J Dermatol Sci. 2023;110(3):99–102. doi:10.1016/j.jdermsci.2023.05.002
108. Nakamura K, Imakado S, Takizawa M, et al. Exacerbation of pustulosis palmaris et plantaris after topical application of metals accompanied by elevated levels of leukotriene B4 in pustules. J Am Acad Dermatol. 2000;42(6):1021–1025. doi:10.1067/mjd.2000.104305
109. Lu JD, Lytvyn Y, Mufti A, et al. Biologic therapies associated with development of palmoplantar pustulosis and palmoplantar pustular psoriasis: a systematic review. Int J Dermatol. 2023;62(1):12–21. doi:10.1111/ijd.16064
110. Ruwaard J, Wolbink G. Differences in Palmoplantar Pustulosis and Psoriasis Vulgaris in Patients with Rheumatoid Arthritis or Ankylosing Spondylitis Treated with Biological Therapy. J Rheumatol. 2019;46(1):117–118. doi:10.3899/jrheum.180566
111. Benzaquen M, Flachaire B, Rouby F, Berbis P, Guis S. Paradoxical pustular psoriasis induced by ustekinumab in a patient with Crohn’s disease-associated spondyloarthropathy. Rheumatol Int. 2018;38(7):1297–1299. doi:10.1007/s00296-018-4034-0
112. Koumaki D, Koumaki V, Lagoudaki E, Bertsias G. Palmoplantar Pustulosis-like Eruption Induced by Baricitinib for Treatment of Rheumatoid Arthritis. Eur J Case Rep Intern Med. 2020;7(1):001383. doi:10.12890/2019_001383
113. Onishi Y, Arakawa Y, Tamagawa-Mineoka R, Ohshita A, Masuda K, Katoh N. Occurrence of palmoplantar pustulosis during atezolizumab therapy for non-small cell lung cancer. J Dermatol. 2021;48(11):e570–e571. doi:10.1111/1346-8138.16144
114. Penalba-Torres M, Rivera-Díaz R. Palmoplantar pustulosis under secukinumab in two patients without psoriasis. J Dtsch Dermatol Ges. 2022;20(1):106–109.
115. Shibata T, Muto J, Hirano Y, et al. Palmoplantar pustulosis-like eruption following tofacitinib therapy for juvenile idiopathic arthritis. JAAD Case Rep. 2019;5(6):518–521. doi:10.1016/j.jdcr.2019.03.024
116. Venables ZC, Swart SS, Soon CS. Palmoplantar pustulosis secondary to rituximab: a case report and literature review. Clin Exp Dermatol. 2015;40(4):451–452. doi:10.1111/ced.12527
117. Villalobos-Sánchez L, Larena-Grijalba C, Alía-Jiménez A, Sifuentes-Giraldo WA. Certolizumab pegol-induced palmoplantar pustulosis: a case report and review of the literature. Reumatol Clin. 2019;15(6):e163–e165. doi:10.1016/j.reuma.2017.12.004
118. Sarıkaya Solak S, Kara Polat A, Kilic S, et al. Clinical characteristics, quality of life and risk factors for severity in palmoplantar pustulosis: a cross-sectional, multicentre study of 263 patients. Clin Exp Dermatol. 2022;47(1):63–71. doi:10.1111/ced.14829
119. Murray D, Corbett MF, Warin AP. A controlled trial of photochemotherapy for persistent palmoplantar pustulosis. Br J Dermatol. 1980;102(6):659–663. doi:10.1111/j.1365-2133.1980.tb06565.x
120. Terui T, Okubo Y, Kobayashi S. 33142 Efficacy and safety of apremilast for the treatment of Japanese patients with palmoplantar pustulosis: results from a phase 2, randomized, placebo-controlled study. J Am Acad Dermatol. 2022;87(3):
121. Haynes D, Topham C, Hagstrom E, Greiling T. Tofacitinib for the treatment of recalcitrant palmoplantar pustulosis: a case report. Australas J Dermatol. 2020;61(1):e108–e110. doi:10.1111/ajd.13117
122. Imafuku S, Maeyama A. Remission of anti-tumor necrosis factor-α antibody-induced palmoplantar pustulosis with the Janus kinase inhibitor baricitinib in a patient with rheumatoid arthritis. J Dermatol. 2021;48(5):e240–e241. doi:10.1111/1346-8138.15860
123. Koga T, Sato T, Umeda M, et al. Successful treatment of palmoplantar pustulosis with rheumatoid arthritis, with tofacitinib: impact of this JAK inhibitor on T-cell differentiation. Clin Immunol. 2016;173:147–148. doi:10.1016/j.clim.2016.10.003
124. Mössner R, Hoff P, Mohr J, Wilsmann-Theis D. Successful therapy of palmoplantar pustulosis with tofacitinib-Report on three cases. Dermatol Ther. 2020;33(4):e13753. doi:10.1111/dth.13753
125. Gleeson D, Barker J, Capon F, et al. Are Janus kinase inhibitors an effective treatment for palmoplantar pustulosis? A critically appraised topic. Br J Dermatol. 2022. doi:10.1111/bjd.20781
126. Yawalkar N, Hunger RE. Successful treatment of recalcitrant palmoplantar pustular psoriasis with sequential use of infliximab and Adalimumab. Dermatology. 2009;218(1):79–83. doi:10.1159/000167802
127. Li SJ, Perez-Chada LM, Merola JF. TNF Inhibitor-Induced Psoriasis: proposed Algorithm for Treatment and Management. J Psoriasis Psoriatic Arthritis. 2019;4(2):70–80. doi:10.1177/2475530318810851
128. Murakami M, Hagforsen E, Morhenn V, Ishida-Yamamoto A, Iizuka H. Patients with palmoplantar pustulosis have increased IL-17 and IL-22 levels both in the lesion and serum. Exp Dermatol. 2011;20(10):845–847. doi:10.1111/j.1600-0625.2011.01325.x
129. Study of Subcutaneous Risankizumab Injection to Assess Change in Palmoplantar Pustulosis Area and Severity Index [PPPASI] in Adult Japanese Participants With Palmoplantar Pustulosis; Identifier, NCT04451720. Available from: https://www.clinicaltrials.gov/study/NCT04451720.
130. Cro S, Cornelius V, Capon F, et al. Efficacy and Mechanism Evaluation. The Interleukin 1 Receptor Antagonist Anakinra to Reduce Disease Severity of Palmoplantar Pustulosis in Adults: APRICOT RCT and PLUM Mechanistic Study. Southampton (UK): NIHR Journals Library.
131. Fukaura R, Akiyama M. Targeting IL-36 in Inflammatory Skin Diseases. BioDrugs. 2023;37(3):279–293. doi:10.1007/s40259-023-00587-5
132. Nakao M, Asano Y, Kamata M, Yoshizaki A, Sato S. Successful treatment of palmoplantar pustular psoriasis with brodalumab. Eur J Dermatol. 2018;28(4):538–539. doi:10.1684/ejd.2018.3325
133. Terui H, Moroi R, Masamune A, Aiba S, Yamasaki K. Possible Efficacy of Vedolizumab, an Anti-α4β7 Integrin Antibody, in Palmoplantar Pustulosis. Case Rep Dermatol. 2023;15(1):22–25. doi:10.1159/000529080
134. Zheng YX, Zheng M, Cai SQ. Successful treatment of secukinumab-resistant palmoplantar pustulosis by Dupilumab: a case report. Dermatol Ther. 2022;35(11):e15781. doi:10.1111/dth.15781
135. Bissonnette R, Maari C, Tsianakas A, et al. A Randomized, Double-Blind, Placebo-Controlled, Phase 2a Study to Evaluate the Efficacy and Safety of RIST4721 in Subjects with Palmoplantar Pustulosis. Dermatol Ther (Heidelb). 2021;11(6):2179–2193. doi:10.1007/s13555-021-00632-7
136. Deucravacitinib for the Treatment of Palmoplantar Pustulosis; IdentifierNCT05710185. Available from: https://wwwclinicaltrialsgov/study/NCT05710185.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.