")
Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 15
Oral Health Knowledge, Attitude, and Behavior Among Health Professions’ Students at Kabul University of Medical Sciences
Authors Ehsan H , Ahmadzai N , Orfani Z, Rezayee BM, Wally M, Daftani S
Received 10 October 2023
Accepted for publication 7 December 2023
Published 13 December 2023 Volume 2023:15 Pages 349—358
DOI https://doi.org/10.2147/CCIDE.S444093
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Hedayatullah Ehsan,1,2 Nazera Ahmadzai,3 Zarlasht Orfani,2 Bibi Marwa Rezayee,2 Moqadasa Wally,2 Sardara Daftani2
1Medical Sciences Research Center, Ghalib University, Kabul, Afghanistan; 2School of Stomatology, Kabul University of Medical Sciences, Kabul, Afghanistan; 3Department of Pediatric Dentistry, Kabul University of Medical Sciences, Kabul, Afghanistan
Correspondence: Hedayatullah Ehsan, Speen Kalay, Khushal Khan Mina, Kabul, 1010, Afghanistan, Tel +93775816022, Email [email protected]
Background: Numerous investigations have revealed that oral issues are quite common among young Afghans. Knowledge, attitudes, and behavior are the three oral health-related population dimensions that need to be assessed in order to design effective public health awareness programs.
Objective: The study’s goal was to find out how much health professions’ students at Kabul University of Medical Sciences knew about oral health, as well as their attitudes and behaviors toward dental health and oral hygiene routines.
Materials and Methods: From September 2022 to December 2022, cross-sectional research was conducted at Kabul University of Medical Sciences. A total of 496 health professions’ students (312 females and 184 males) aged 18– 25 years old from 5 colleges of health and medical-related disciplines were addressed. All participants were given a thorough questionnaire with 30 amended items modified from Peterson et al and Stenberg et al.
Results: 44.5% (n=220) of the participants brushed their teeth twice per day, 41.3% (n=204) once per day, and 9.31% (n=46) more than twice per day, while just 4.7% (n=23) cleaned their teeth less than once per day. Surprisingly, the majority of participants (91% or n=451) were aware of the significance of routine dental visits, and 51.3% (n=252) of participants reported visiting the dentist while they experienced pain. 94% of students were of the opinion that brushing their teeth prevents dental decay. 93% (n=461) of them agreed that using fluoride strengthens teeth, and 96% (n=476) said that sweets are bad for teeth.
Conclusion: Oral health knowledge, attitudes, and behaviours are related to an individual’s level of education. Female and generally dental professions’ participants, rather than other health professions participants, were more likely to be concerned about their oral health than male participants.
Keywords: oral health, dental care, knowledge, attitudes, students, public health
A Letter to the Editor has been published for this article.
A Response to Letter by Miss Shahid has been published for this article.
Introduction
Oral health has been connected to challenges related to sleep, behavior, and developmental milestones in children with long-term quality-of-life concerns.1 It is essential for one’s general health, attractiveness, and sense of wellbeing. Since maintaining proper oral hygiene is necessary to treat dental caries and periodontal disease, the two most common oral illnesses, they are classified as behavioral disorders.1,2
Oral health knowledge is considered to be a prerequisite for health-related behavior. The first step to creating a habit is educating patients about oral health prevention and giving them relevant information.3 Dental students are expected to be role models for oral health behavior after completing an undergraduate dental curriculum. Instilling proper oral habits in patients to prevent oral diseases is a crucial duty for oral health practitioners. It has been asserted that oral health practitioners’ behaviors and attitudes about their own oral health are indicative of how seriously they take the importance of preventative dental care and maintaining the oral health of their target audience.4
While studies have shown that educational interventions based on the KAP (knowledge-attitude-practice) paradigm greatly improved oral health practice,4–6 a positive correlation between low knowledge and the prevalence of dental caries was observed7 and other study results have shown that adults with low oral health attitudes and behaviors were more likely to have dental caries than adults with higher oral health attitudes and behaviors.8,9 However, a different study revealed that other characteristics should be taken into account in addition to knowledge, attitude, and the KAP model when predicting oral health practices.5,10
The oral health system in Afghanistan is currently changing. The knowledge of our people’s attitudes toward oral illnesses and their prevention is poor. Planning for public oral healthcare requires systematic data. This study is novel because information about Afghan university students’ oral health knowledge, attitudes, and hygiene practices is sparse.
The study aimed to discover and determine self-reported knowledge about oral health, attitudes, and personal behaviours toward oral hygiene routines of select health profession students at Kabul University of Medical Sciences and examine their attitudes and practices toward oral health.
Research Questions
- How are the Afghan health professional students’ oral hygiene practices in general? (18–25 years).
- Is there a gender difference in oral hygiene practice among health professional students at Kabul University?
- Which of the professions were best informed about oral health and hygiene practices?
Methods and Materials
Between September and December 2022, 496 health profession students from Kabul University of Medical Sciences’ faculties including medicine, dentistry, public health, pharmacy, midwifery, and nursing participated in this cross-sectional study, with 37% (n = 184) male students and 64% (n = 312) female students. Students were reached in classes, on the university campus, in reading rooms, and in the cafeteria and asked to complete an anonymous, structured questionnaire covering the following topics: age, gender, toothbrushing, flossing, use of mouthwash, regularity of dental visits, consumption of sugar-containing and sugar-free products, academic standing, study year, and assessment of financial situation are sociodemographic characteristics.
After the evaluation of the proposal for this study by the research and ethical committee of Kabul University of Medical Sciences, the directorate of the university approved and gave its permission to proceed with this study. The surveyor inquired to inform the students about the study. All of those students who were under 18 years old were rejected for participating in this study. The study was affirmed by the ethics and research board at Kabul University of Medical Sciences with the approval #41. Before starting our survey, we obtained university approval and informed consent from the students.
All participants were given a detailed questionnaire adapted from Peterson et al and Stenberg et al for which this questionnaire is available online.11 The survey included 33 questions designed to assess students’ attitudes, behaviors, and knowledge of oral health and dental care. However, we did not include all 33 items in the questionnaire since three of them were deemed inappropriate for students pursuing health professions; as a result, we assessed those things on the survey’s 30 questions. Meanwhile, the translation of this questionnaire is accessible for anyone by request and with the permission of research committee of Kabul University of Medical Sciences. By doing this, the knowledge of participants regarding oral health was tested based on different topics, including the influences of fluoride utilization and brushing on dentition, the reason for the bleeding gums and how to stop it, the consequences of dental plaque, the number of temporary and permanent teeth, the impacts of sweets and soft drinks on the dentition, and the influence of caries on the aesthetic appearance of teeth.
Brushing habits of participants (such as recurrence, term, and time), dental knowledge, and dental visits were also evaluated (such as consistency, reason behind the visit, impact of torment and financial matters on dental participation, data on the visit to begin with, and looking for medications). Treatment uneasiness, treatment sentiments, treatment inclusion considerations, opinions, and attitudes regarding the dentist and dental care, attitudes toward dental care and body care in general, and states of mind toward customary dental visits were utilized to evaluate participants’ attitudes about dental care.
In the end, a strategy for reacting to each item was given, and subjects were taught to follow it. A constrained choice arrangement was utilized, in which members had to write their answers, select from a list of alternatives, or combine the two. The subjects were given careful clarification of how to score their answers and were instructed that a few things had multiple answering designs. On several occasions, the subjects were given the choice of selecting more than one answer to a given question. This explains why, for certain items in the result tables, the values in the recurrence columns do not constantly coordinate with the overall test measure.
The data were examined using the Statistical Package for Social Science 26.0 (SPSS 26.0).
Result
The study embraced about 496 health profession students (Figure 1), among whom 37% (n = 184) were male and 64% (n = 312) were female students. The age of students ranged from 18 to 25 years; most of them were in the range of 20 to 21 years, and the level ranged from 1 to 7, with most of them in fourth grade of health professions’ faculty (senior students). Data were collected from four different faculty students: curative medicine (24%; n = 129), dentistry (47% n = 254), public health (18%) (n = 96), and nursing (11%) (n = 62).
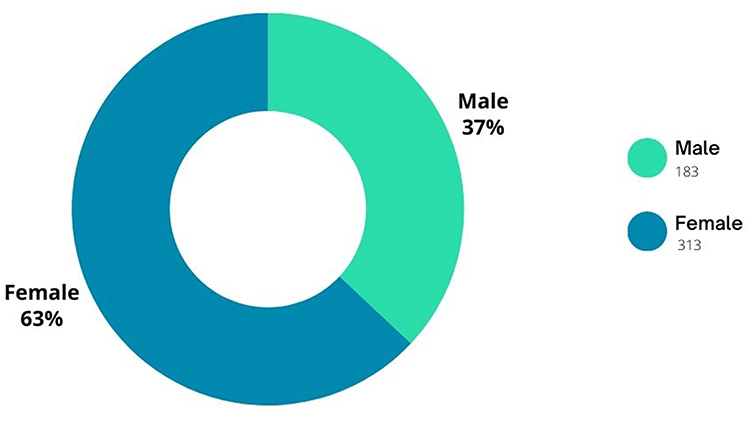 |
Figure 1 Shows the percentage of participants according to gender. |
According to the survey, 44.5% (n=220) of the participants brushed their teeth twice a day, 41.3% (n=204) once per day, and 9.31% (n=46) more than twice daily, while just 4.7% (n=23) brushed less than once daily. The majority (74.6%=370) used a toothbrush and toothpaste to clean their teeth; 46.8% (n=232) of participants brushed their teeth before going to bed and 44.8% (n=222) in the morning. 40.1% (n=199) of the participants brushed their teeth for 2 min, 26.4% (n=131) for 1 min, 25.7% (n=127) for more than 2 min, and 9.7% (n=48) for less than 1 min.
The majority of participants (76%=377) believed that bleeding in gums is a sign of inflamed gum; 29.1% (n=144) of participants believed that for protecting gums from bleeding, using a toothbrush, toothpaste, and dental floss is vital and necessary; 5.6% (n=27) believed that using soft food is important; 58% (n=287) of the participants had the same belief about using vitamin C; and 7.1% (n=35) did not know how to protect.
The most frequent reason for students’ last dental visit (62.9%=312) (Table 1) was dental caries, and other reasons for visiting the dentist included family and friends’ advice (8.2%=40), the dentist’s advice (14.1%=70), and their own internal trigger and interest (14.6%=71).
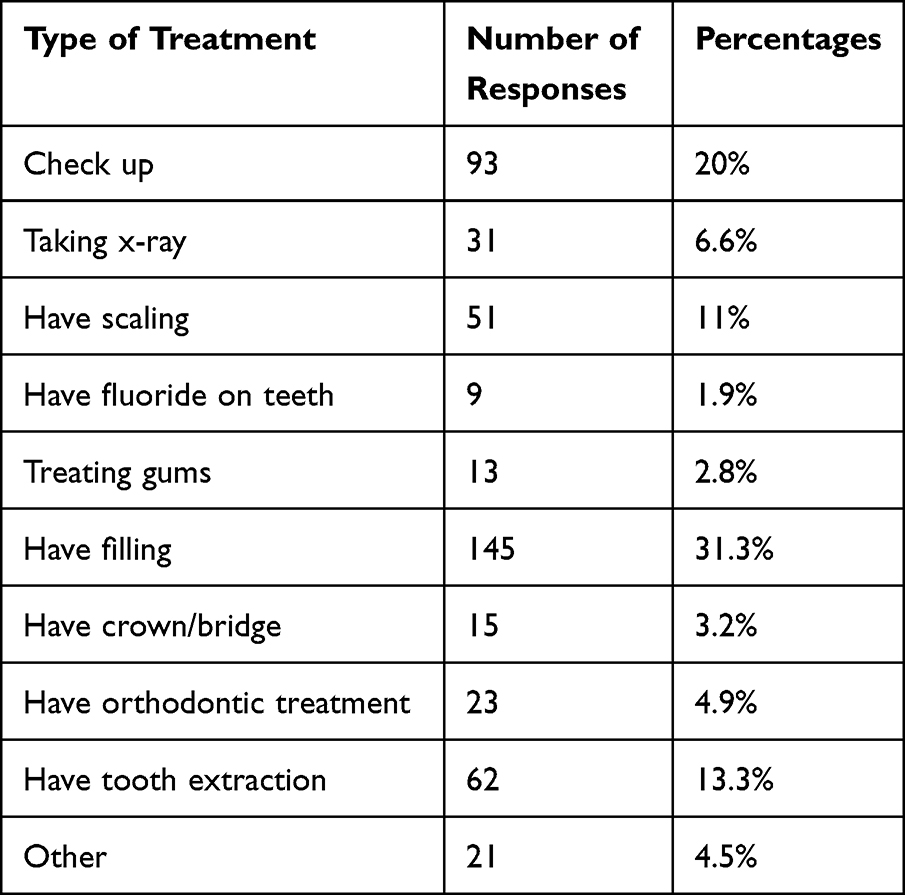 |
Table 1 Shows the Treatments Sought During Student’s Last Dental Visit |
19.8% (n=98) of the participants who filled out the questionnaire visited their dentist regularly every 6–12 months (Table 2), 12.7% (n=63) visited occasionally, 53.3% (n=264) visited their dentist when they had pain, and 14.1% never visited the dentist in their entire life, respectively.
 |
Table 2 Shows the Last Time When Participants Visited Their Dentist |
Students’ perspectives on visiting a dentist (Table 3) about their first dental appointment ranged from worried and hesitant, slightly afraid, very slightly afraid, to never fearful (19.7%=98, 13.8%=68, and 21.4%=106 to 44.9%=223).
 |
Table 3 Shows the First Impression of Participants from Their First Dental Visit |
Participants’ knowledge toward the number of deciduous and permanent teeth was different; 9% (n=44) of them believed that the number of deciduous teeth is less than 20, 6% (n=30) believed that the number of deciduous teeth is more than 20, and only 75.2% (n=373) of students accepted that the number of deciduous teeth is 20, and 9.6% (n=47) of them did not have any idea regarding it. And about the permanent teeth: 5% (n=24) for less than 32 teeth, 86.7% (n=430) of them responded with the number of 32 for permanent teeth, and 8.1% (n=40) of them did not know about the number of permanent teeth.
44.9% (223) of participants did not have carious teeth (Figure 2), 31.1% (n=154) had one or two carious teeth, 16.7% (n=82) had three or four carious teeth, 4.3% (n=21) had five or six carious teeth, 0.9% (n=4) had seven or eight carious teeth, and 1.8% (n=9) had nine or ten carious teeth. 49.3% (n=244) of the participants had no filled teeth, 32.1% (n=159) had one or two filled teeth, 12% (n=59) had three or four filled teeth, and 6.4% (n=31) had five or six filled teeth.
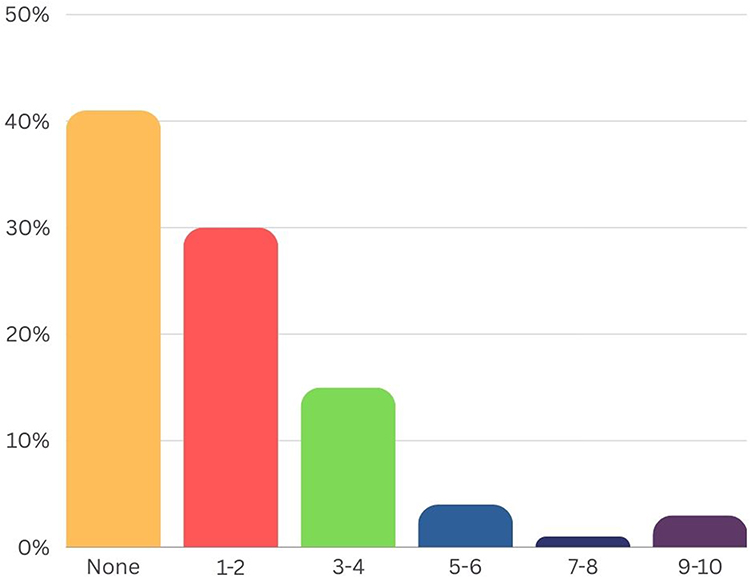 |
Figure 2 Shows the number of carious teeth of the participants. |
According to the poll, 94.5% (n=469) of participants who completed the questionnaire felt that carious teeth can alter the look of teeth, while 4.5% (n=22) claimed that it did not.
94% (n=466) of students had the opinion that brushing teeth prevents dental decay, while only 6% (n=30) have disagreed. When asked if using fluoride strengthens teeth, 93% (n=461) said yes, while 7% (n=34) said no. 96% (n=450) of participants agreed that sweets are bad for teeth, and 97% (n=481) agreed that fizzy beverages are bad for teeth.
Based on the study, 91% (n=451) of students agreed that regular visits to the dentist are necessary, whereas 9% (n=44) were opposed. 79% believed that dentists always explain the dental problem and solve it; on the other hand, 21% (n=104) did not. 92% (n=456) mentioned that the dentist examines and takes care of his or her patients, and 8% had a negative response to this. There is a remarkable percentage of 68% (n=426) who believe that what the dentist cares about is treatment, not prevention, but 32% (n=158) believe that it is not.
95.5% (n=473) of the participants believed that general body health has a relationship to oral and dental diseases, whereas only 5% (n=24) believed that there is not.
96% (n=450) of the students who filled out the questionnaire mentioned that they care about their teeth as much as any other part of their body, while 4% (n=19) said that they do not.
According to the students’ answers, most dentistry students (65% or n=322)—rather than students in other health professions—performed better than all other health students on comparable issues. In general, 63% (n=312) of participants in this study were females, and the percentage of them in each criterion was higher and different than that of males from question to question of the questionnaire.
Discussion
To the best of our knowledge, this study is the first of its type to look into these concerns among health professions’ students in Afghanistan. It provided a thorough analysis of oral health behavior, knowledge, and attitudes among medical university students aged 18 to 25. Previous studies involving Afghans have shown that they have bad oral hygiene, attitudes, and knowledge.12 When the results of this study were compared to European populations,13–15 European students demonstrated better dental knowledge, attitudes, and health than Afghans.
Although health professions’ students (in curative medicine) have never received such information, second- and higher-year dental students have received knowledge and skills to help them understand the role of preventive dentistry and oral health care in the management of common oral health problems, such as dental caries, gingivitis, tooth wear, and so on.
The fact that dental students’ mean scores based on surveys were higher than those of health professions’ students suggested that the course information relating to oral health education may have had a positive impact on dental students’ levels of oral self-care. The findings of this study agreed with those of a survey employing the HU-DBI conducted by Kawamura et al,16 which found that second-year dental hygiene students had significantly higher mean HU-DBI scores than second-year nursing students. Our sample size was rather small, which was a restriction in our study even if the results were statistically significant; a subsequent investigation with a larger sample population may reveal stronger relationships than those described here.
Based on our study, gender was a significant factor affecting the percentage of agree/disagree responses for items (I worry about the color of my teeth, have noticed some white sticky deposits on my teeth, and often check my teeth in a mirror after brushing). Compared to their male counterparts, female dental students displayed a substantially better attitude. This result is in line with earlier studies.17,18
Typically, females are more inclined to practice good self-care behaviors for internal psychosocial factors, such as to enhance their physical attractiveness and self-esteem.
The dentist’s job should extend beyond the delivery of dental care because oral health encompasses much more than just having good teeth.19 Consequently, dental health education programs that aim to improve oral health practices among the population are very important. Improving public awareness of periodontal health is an essential public health goal in Afghanistan.
Most of the participants in this study, according to the poll, clean their teeth at least once every day (Table 2). The participants also mentioned irregular dental brushing schedules. The failure of non-dental students to plan or support their toothbrushing efforts aligned with findings from a prior study that showed adults had unacceptable levels of periodontal disease knowledge and awareness.14 It was discovered that mouthwash and tooth floss were rarely used; this could possibly be attributable to the absence of oral health education and/or the high cost of such products.
The findings of this study revealed knowledge of gingival bleeding as a sign of periodontal disease (represented by gingivitis), which was similar to the findings of a study conducted among Jordanian students.20 Most participants in the study did not make the connection between gingivitis and dental plaque or understand the significance of brushing in the management of gingivitis.
Most participants (91%) were aware of the significance of routine dental visits, and 51.3% reported visiting the dentist while they experienced pain, and this conclusion is similar to that of a study on the Afghan population,1 while only 14% of non-Afghan participants in a different survey who are not health professions’ students or practitioners expressed a strong desire to visit a dentist.8 Surprisingly, the majority of participants (91%) were aware of the significance of routine dental visits. Certain findings of this study may offer a justification for the individuals’ sporadic dental visits. A significant part of the subjects claimed that they did not attend because of their dread of dental procedures, the high cost of dental care, and the absence of toothaches.
Additionally, dental services are typically not covered by Afghanistan’s medical insurance system, which may be the cause of the low rates of dental clinic visits. Tradition and a lack of official healthcare in the community may also be to blame. The extra time needed for frequent visits might not be acceptable, or there may have been a prior negative dental experience (Table 4). Since one’s knowledge of and attitude toward proper health care are crucial components of the preventative cycle, a lack of adequate dental education may be a contributing factor.21–25 To address this, a planned intervention is required. This could result in an improvement in oral and dental health status by raising population awareness and altering attitudes, behaviors, and lifestyle choices.
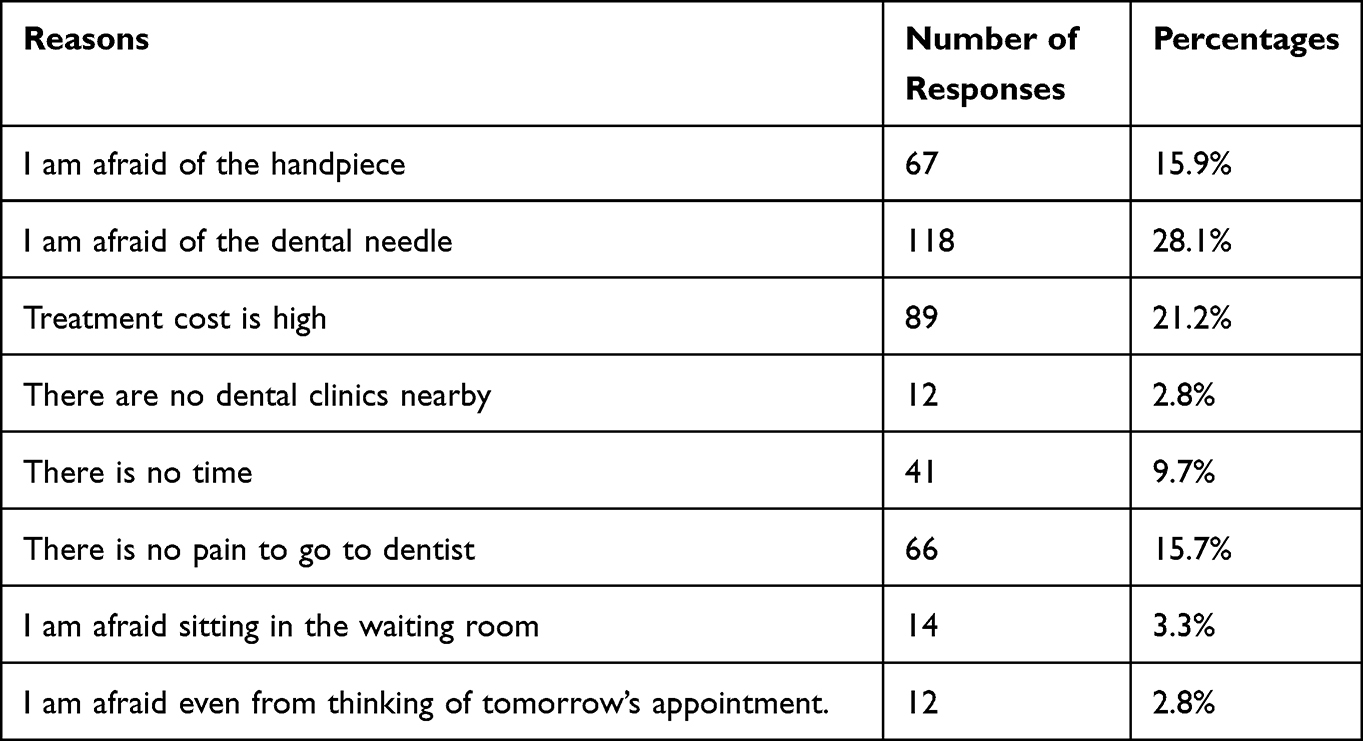 |
Table 4 Shows the Reasons Why Participants Do Not Want or are Afraid of Visiting Their Dentist |
Another finding found in this study was that most of the subjects showed a critical level of dental treatment anxiety, which is closer to the finding of another study not among Afghans.10 This may be due to the absence of adequate education programs on oral health, which, together with the aforementioned factors, made dental care unpopular.
The majority of participants (95.5%) had favourable opinions toward their dental practitioners and specialists and high levels of understanding of the connection between dental health and overall health. This means that Afghan medical and dental institutions have been supporting and educating young patients about the importance of prevention and appropriate treatments by taking into account systemic well-being and psychological factors. It is vital to note that highlighting the connection between oral health and overall health may aid in promoting oral health awareness and oral self-care among the general public. Nonetheless, a few institutional medical and dental institutes and dental schools in Afghanistan have mostly delivered educational oral health programs to the general population on a small scale. In order to enhance oral health practices, knowledge, and attitudes among the general public, comprehensive national educational initiatives are required. Unfortunately, these attempts are fragmented and insufficient nationwide.
Strengths and Limitations
The strength of this research is that it is the first study of its kind undertaken in Afghanistan among health professions’ students, with no previous reports. Furthermore, this study was supervised and confirmed in accordance with the ethical principles (10 specific Helsinki principles: scientific requirements and research protocols, informed consent, privacy and confidentiality, research registration and publications, and so on) of Kabul University of Medical Sciences’ research ethics committee.
This data is not sufficient to resolve and find the whole answers to questions; it is just a sample of data from Kabul. So, there is a need for broader data to cover most of the Afghan population.
Conclusion
The study found a correlation between adult education and oral health awareness, with improved education leading to better oral health. Non-dental students had lower awareness, while female students at Kabul University of Medical Sciences were more concerned. However, most students lacked understanding of dental caries and periodontal disorders.
Clinical Relevance
- Scientific Rationale for study:
Knowledge and information will lead individuals, and the whole community to the exact destination they are looking for.
Research studies collect important information about behaviours, risk factors, and disease trends. The study findings can be utilized to support lobbying activities and to justify public health funding. Overall, public health is concerned with the well-being of whole communities. These populations might range from a tiny neighbourhood to an entire country or part of the planet.
This paper gathers information about oral health knowledge, attitudes, and behaviours of medical and dental students for exploring and evaluating their knowledge, attitudes and behaviours toward oral health, and their general health and compare them with other populations who are not medical and dental students.
Principle Findings and Practical Implications
Surprisingly, all previous studies and papers that were used in this article conducted their investigations among non-health professions’ students, and their findings varied from nation to nation, but most of them were similar, whereas this article, which was conducted among medical and dental students, revealed a high percentage of well knowledge, appropriate attitudes, and behaviour toward their oral and overall health, indicating that knowledge of something is important. According to this study, if we wish to lead the community to excellent health, we must improve people’s knowledge and information.
Data Sharing Statement
The data that support the findings of this study are available from research ethics committee of Kabul University of Medical Sciences but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are available from the first author of this paper upon reasonable request and with the permission of only Hedaytullah Ehsan.
Ethical Approval and Consent to Participate
Prior to the start of this study, the research protocol (proposal in local language) was submitted for review to the research ethics committee of Kabul University of Medical Sciences. This committee usually consists of qualified experts from different faculties, including curative medicine, dentistry, public health, midwifery, and nursing, who transparently provide comment, guidance, and approval of research. This study was supervised and confirmed based on the ethical principles (10 specific principles of Helsinki: scientific requirements and research protocols, informed consent, privacy and confidentiality, research registration and publications, and so on) of this committee. All data from this study, in conjunction with the participants’ informed consent, is stored for ethical issues with this committee. The supervision and registration of this study within the research ethics committee of Kabul University of Medical Sciences were done by three professors from the Dentistry Faculty that are responsible for oral and dental studies in this research committee. The first supervisor and mentor of this research is Assistant Prof. Drs. Nazera Ahmadzai; the second supervisor and mentor is Prof. Razia Rabizada; and the last one is Assistant Prof. Ahmad Milad Stanikzai.
For more details and confirmation, these supervisors and mentors from the research committee are responsible for giving confirmation, so the Journal of Publication can make contact with the supervisors of this study, whose more details are below:
1. Assistant Prof. Nazera Ahmadzai, MD
Head of Pediatric Dentistry Department, Kabul University of Medical Sciences, Email: [email protected]
2. Prof. Razia Rabizada, MD
Head of Oral Medicine Department, Dentistry Faculty, Kabul University of Medical Sciences, Email: [email protected]
3. Assistant Prof. Ahmad Milad Stanikzai, MD
Dean of Dentistry Faculty, Department of Endodontics, Kabul University of Medical Sciences, Email: [email protected].
Consent for Publication
Before we collected our data from students, the whole process and goal of the study were completely explained, and a separate consent sheet for publication was distributed for giving their consent, of which some samples attached in the related files. So, all of them gave their consent for publication.
Acknowledgments
The authors are extremely grateful to the completion of our study would not have been possible without the support and nurturing of our research mentors (Prof. Razia Rabizada, MD, and Assistant Prof. Tamana Barakaty, MD, MsCs) for guiding us.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare no competing interests in this work.
References
1. Rimondini L, Zolfanelli B, Bernardi F, Bez C. Self-preventive oral behavior in an Italian university student population. J Clin Periodontol. 2001;28(3):207–211. doi:10.1034/j.1600-051x.2001.028003207.x
2. Hedman E, Ringberg K, Gabre P. Oral health education for schoolchildren: a qualitative study of dental care professionals’ view of knowledge and learning. Int J Dent Hyg. 2009;7(3):204–211. doi:10.1111/j.1601-5037.2009.00391.x
3. Levin L, Shenkman A. The relationship between dental caries status and oral health attitudes and behavior in young Israeli adults. J Dent Educ. 2004;68(11):1185–1191. doi:10.1002/j.0022-0337.2004.68.11.tb03864.x
4. Peker I, Alkurt MT. Oral health attitudes and behavior among a group of Turkish dental students. Eur J Dent. 2009;3(1):24–31. doi:10.1055/s-0039-1697402
5. Suprabha BS, Rao A, Shenoy R, Khanal S. Utility of knowledge, attitude, and practice survey, and prevalence of dental caries among 11- to 13-year-old children in an urban community in India. Glob Health Action. 2013;6:20750. doi:10.3402/gha.v6i0.20750
6. Shenoy RP, Sequeira PS. Effectiveness of a school dental education program in improving oral health knowledge and oral hygiene practices and status of 12- to 13-year-old school children. Indian J Dent Res. 2010;21(2):253–259. doi:10.4103/0970-9290.66652
7. D’Cruz AM, Aradhya S. Impact of oral health education on oral hygiene knowledge, practices, plaque control and gingival health of 13- to 15-year-old school children in Bangalore city. Int J Dent Hyg. 2013;11(2):126–133. doi:10.1111/j.1601-5037.2012.00563.x
8. Diwan S, Saxena V, Bansal S, et al. Oral health: knowledge and practices in rural community. Indian J Community Health. 2011;23(1):29–31.
9. Bashiru BO, Omotola OE, et al. Oral health knowledge, attitude and behavior of medical, pharmacy and nursing students at the University of Port Harcourt, Nigeria. J Oral Res Rev. 2016;8(2):66–71. doi:10.4103/2249-4987.192209
10. Oliveira ER, Narendran D, Williamson D. Oral health knowledge, attitudes and preventive practices of third grade school children. Pediatr Dent. 2000;22(5):395–400.
11. Al‐Omiri MK, Al‐Wahadni AM, Saeed KN. Oral health attitudes, knowledge, and behavior among school children in North Jordan. J Dent Educ. 2006;70(2):179–187. doi:10.1002/j.0022-0337.2006.70.2.tb04074.x
12. Qadir SA, Muhammad S, Khattak MI, et al. Self-reported oral health status and associated factors among Afghan refugees in Peshawar Pakistan; a pilot study. Rehman J Health Sci. 2021;2(2):40–45. doi:10.52442/rjhs.v2i2.72
13. Downer MC. The improving dental health of United Kingdom adults and prospects for the future. Br Dent J. 1991;170(4):154–158. doi:10.1038/sj.bdj.4807452
14. Petersen PE, Aleksejuniene J, Christensen LB, Eriksen HM, Kalo I. Oral health behavior and attitudes of adults in Lithuania. Acta Odontol Scand. 2000;58(6):243–248. doi:10.1080/00016350050217073
15. Stenberg P, Håkansson J, Åkerman S. Attitudes to dental health and care among 20 to 25-year-old Swedes: results from a questionnaire. Acta Odontol Scand. 2000;58(3):102–106. doi:10.1080/000163500429217
16. Kawamura M, Ikeda‐Nakaoka Y, Sasahara H. An assessment of oral self-care level among Japanese dental hygiene students and general nursing students using the Hiroshima University--Dental Behavioural Inventory (HU-DBI): surveys in 1990/1999. Eur J Dent Educ. 2000;4(2):82–88. doi:10.1034/j.1600-0579.2000.040206.x
17. Al-Omari QD, Hamasha AA-H. Gender-specific oral health attitudes and behavior among dental students in Jordan. J Contemp Dent Pract. 2005;6(1):107–114. doi:10.5005/jcdp-6-1-107
18. Porat D, Kawamura M, Eli I. Effect of professional training on dental health attitudes of Israeli dental students. Refu’at Ha-Peh Veha-Shinayim. 2001;18(2):51–63.
19. Berg-Warman A, Schiffman IK, Zusman SP, Natapov L. Oral health of the 65+ age group in Israel-2020. Isr J Health Policy Res. 2021;10(1):58. doi:10.1186/s13584-021-00494-6
20. Taani DQ, Alhaija ESJA. Self-assessed bleeding as an indicator of gingival health among 12-14-year-old children. J Oral Rehabil. 2003;30(1):78–81. doi:10.1046/j.1365-2842.2003.01021.x
21. Al-Wahadni AM, AL-Omiri MK, Kawamura M, et al. Differences in self-reported oral health behavior between dental students and dental technology/dental hygiene students in Jordan. J Oral Sci. 2004;46(3):191–197. doi:10.2334/josnusd.46.191
22. Barrieshi-Nusair K, Alomari Q, Said K, et al. Dental health attitudes and behaviour among dental students in Jordan. Community Dent Health. 2006;23(3):147–151.
23. Dagli RJ, Tadakamadla S, Dhanni C, et al. Self reported dental health attitude and behavior of dental students in India. J Oral Sci. 2008;50(3):267–272. doi:10.2334/josnusd.50.267
24. Jaramillo JA, Jaramillo F, Kador I, et al. A comparative study of oral health attitudes and behavior using the Hiroshima University-Dental Behavioral Inventory (HU-DBI) between dental and civil engineering students in Colombia. J Oral Sci. 2013;55(1):23–28. doi:10.2334/josnusd.55.23
25. Kumar H, Behura SS, Ramachandra S, et al. Oral health knowledge, attitude, and practices among dental and medical students in eastern India - a comparative study. J Int Soc Prev Community Dent. 2017;7(1):58–63. doi:10.4103/jispcd.JISPCD_30_17
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.