")
Back to Journals » International Journal of Women's Health » Volume 16
Oral GnRH Antagonists in Combination with Estradiol and Norethindrone Acetate for Pain Relief Associated with Endometriosis: A Review of Evidence of a Novel Class of Hormonal Agents
Authors Othman ER, Al-Hendy A, Mostafa R, Lambalk CB , Mijatovic V
Received 27 September 2023
Accepted for publication 22 January 2024
Published 27 February 2024 Volume 2024:16 Pages 309—321
DOI https://doi.org/10.2147/IJWH.S442357
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Essam R Othman,1,2 Ayman Al-Hendy,3 Radwa Mostafa,1 Cornelis B Lambalk,2 Velja Mijatovic2
1OB-GYN Department, Assiut University, Assiut, 71515, Egypt; 2Academic Endometriosis Center, Amsterdam University Medical Center, Vrije Universiteit Amsterdam, Amsterdam, the Netherlands; 3Department of Obstetrics and Gynecology, University of Chicago, Chicago, IL, 60637, USA
Correspondence: Essam R Othman, Department of Obstetrics and Gynecology, Assiut University, Assiut, Egypt, Email [email protected]
Abstract: Current medical treatment options for endometriosis associated pains are inadequate. Evidence on effects of nonsteroidal anti-inflammatory drugs is scarce. Around one third of patients are not responsive to oral contraceptives or progestins due to progesterone resistance. Gonadotropin-releasing hormone (GnRH) agonists can only be used for a short duration because of associated side effects. Oral GnRH antagonists, including elagolix, relugolix, and linzagolix allow oral administration, induce dose dependent reduction of estradiol levels, do not cause initial flare up of endometriosis symptoms, and allow the fast return of ovarian function and menstruation after discontinuation. Elagolix at a low dose of 150 mg once daily, or the higher dose of 200 mg twice daily, significantly increased the proportion of women achieving clinically meaningful decline of dysmenorrhea, noncyclic pelvic pain, and dyspareunia. Relugolix at an oral dose of 40 mg/day results in improvement in different forms of endometriosis related pelvic pain, with an efficacy and side effect profile similar to that of GnRH agonists. Adding 1 mg of estradiol and 0.5 mg of norethindrone to 40 mg of relugolix (relugolix combination therapy) allows extension of treatment to 24 weeks with maintained efficacy and an improved side effect profile. Linzagolix, in a dose of 75 mg/day, can be used alone to treat endometriosis associated pain. For severe pelvic pain and dyspareunia, linzagolix can be used in a high dose of 200 mg/day with hormonal add-back therapy to preserve bone health.
Plain Language Summary: Oral gonadotropin-releasing hormone (GnRH) antagonists, including elagolix, relugolix, and linzagolix, represent a new addition in the armamentarium against endometriosis associated pain. They are given orally, do not cause an initial flare-up of disease symptoms, allow a return of menses quickly after their withdrawal and produce a balance between ability to relieve endometriosis associated pain and side effects profile. The addition of hormonal agents like estradiol 1 mg and norethindrone acetate 0.5 mg to relugolix (relugolix combination therapy) allowed longer use of the medication for relief of endometriosis associated pain while reducing side effects like bone mineral density loss and hot flushes.
Keywords: endometriosis, pain, elagolix, relugolix, linzagolix, estradiol, norethindrone
Endometriosis, the Problem
Endometriosis is a chronic inflammatory estrogen dependent disorder that is defined by the presence of endometrial-like tissue outside the uterine cavity.1 The disease affects 2–10% of women in their reproductive years.2 Endometriosis is associated with subfertility and debilitating painful symptoms including dysmenorrhea, dyspareunia, dysuria, dyschezia, and chronic pelvic pain.3 Other associated comorbidities include chronic pain syndromes, fatigability, anxiety/depression, autoimmune diseases, and an increased risk of certain types of cancers.4 Endometriosis diagnosis is often delayed for 4–11 years after symptoms start.5 Women with endometriosis have impaired quality of life and lose, on average, 11 working hours per week, mainly due to reduced employability at work.6 The financial burden of endometriosis approaches 27,855 USD per patient per year, mounting to 22 billion USD at the country level in the United States alone in treatment, productivity loss and health care costs.7 Symptomatic medical treatment options of endometriosis include analgesia and various hormonal suppression therapies.8,9 Surgical treatment involves excision of endometriotic lesions to reduce pelvic pain, for recovery of organ dysfunction or to enhance fertility. However, nearly 50% of women undergoing endometriosis surgery may need repeat surgery within 5 years for recurrent symptoms, especially if hormonal treatment is avoided.10 Assisted reproductive technologies are often used to treat endometriosis related infertility because of the associated tubal dysfunction, diminished ovarian reserve or inability to have sexual intercourse.11 Although it is traditionally believed that pregnancy has a favorable influence on endometriosis, its negative impact on pregnancy is currently a growing area of concern as well.12
Since a cure for endometriosis is not available, treatment should be adjusted in line with changing life goals, needs and expectations during the reproductive lifespan and beyond. Therefore, not only a multidisciplinary but also a life course approach in endometriosis is currently recommended.8
Available Medical Treatments of Endometriosis
The ideal medication for endometriosis should meet the following criteria: it should be curative rather than suppressive, it treats pain and infertility at the same time, it has an acceptable side effect profile and long-term use is safe and affordable.13 Unfortunately, such a medication still does not exist for women with endometriosis.
Current medical treatment options of endometriosis includes analgesics and anti-inflammatory drugs such as nonsteroidal anti-inflammatory drugs (NSAIDs), which reduce endometriosis related pain and associated inflammation. However, there is limited evidence supporting their effectiveness.14 First line hormonal therapy includes oral contraceptive pills and progestins (oral, IM, or LNG-IUS) which are relatively cheap and usually well tolerated. They affect endometriosis by reducing circulating estrogen, achieving atrophy of the endometriosis implants and reducing the inflammatory reaction. The use of NSAIDs enhances this effect on the inflammatory response.15
However, one fourth to one third of patients are non-responsive to these hormonal agents because of progesterone resistance or they experience intolerable side effects (breakthrough bleeding, depressive symptoms, breast tenderness, bloating, loss of libido, weight gain and headaches).16 For such patients second line hormonal treatment including gonadotropin-releasing hormone (GnRH) agonists, which induce a profound hypoestrogenic milieu, could be used.17,18 GnRH agonists can cause substantial bone mineral density loss with long-term use, hot flushes, dry vagina, and mood swings. Because of their side effect profile, GnRH agonist use should be limited to 6 months if used alone and to one year if used with hormonal add-back therapy to avoid clinically relevant reductions in bone mineral density.19 Aromatase inhibitors represent another second line treatment option to treat endometriosis related pain.20 Although they are off-label for this indication, the use of aromatase inhibitors (usually in combination with oral contraceptives, progestogens, GnRH agonists or GnRH antagonists) is currently recommended to prescribe to women with endometriosis-associated pain refractory to medical or surgical therapy.17 In addition, their prolonged use is limited because of their hypoestrogenic side effects including bone mineral density loss, vaginal dryness, and the occurrence of vasomotor symptoms.21
Oral GnRH Antagonists: A New Class of Agents to Treat Endometriosis Associated Pain
Oral GnRH antagonists are the newest addition to the armamentarium of medications indicated for treatment of endometriosis associated pains. They are orally active, non-peptide antagonists of the gonadotropin-releasing hormone (GnRH) receptors on the pituitary gland. Oral GnRH antagonists block the secretion of pituitary gonadotropins within hours, leading to a drop in ovarian production of estrogen, progesterone, and testosterone.22,23 Several appealing advantages are provided by these novel medications in the treatment of endometriosis associated pain. Firstly, GnRH antagonists are orally administered instead of a depot injection, and therefore are easy to use. Secondly, they do not cause an initial flare-up of gonadotropin secretions like GnRH agonists do, which might lead to the exacerbation of endometriosis symptoms in the first 1–2 weeks of use. Thirdly, unlike GnRH agonists, which induce a complete block of the hypothalamic-pituitary-ovarian axis, with profound hypoestrogenic effect, GnRH antagonists can allow dose dependent lowering of estradiol level, which can adjust a balance between efficacy in treating endometriosis associated pain while avoiding major hypoestrogenic side effects. Fourthly, shortly after discontinuation of the oral GnRH antagonist, the recovery of the menstrual cycle occurs with estrogen levels returning to their normal premenopausal levels.16,24,25 Oral GnRH antagonists have been identified as effective second line treatment of endometriosis associated pain.26,27
Elagolix, the first oral GnRH antagonist
It was approved by the US FDA on the 23rd of July 2018 for the management of moderate to severe pain associated with endometriosis. Elagolix has been labelled as a second-generation GnRH modulator due to its non-peptide and small-molecular nature which allows oral use. Its half-life after oral administration is 2.4–3.6 hours and it is metabolized mainly by the liver and excreted in feces.25,28 Carr et al, in a phase 2 randomized clinical trial, evaluated two regimens of elagolix (elagolix 150 mg once daily, and elagolix 75 mg twice daily) versus depot medroxyprogesterone acetate (DMPA) for the treatment of endometriosis associated pain over a 24 week treatment period. Similar to DMPA, both doses of elagolix had a minimal effect on bone mineral density and had similar efficacy to DMPA in treating endometriosis associated pain.29 Phase 3 clinical trials on elagolix enrolled more than 1600 women with surgically confirmed endometriosis, who complained of moderate to severe pelvic pain. Participants were randomized to receive either elagolix 150 mg/day or elagolix 200 mg twice/day or placebo for a period of 6 months. A significantly higher proportion of women on elagolix, compared to women on placebo, achieved a clinically meaningful improvement in dysmenorrhea and non-menstrual pelvic pain with decreased or stable use of rescue analgesics.30 Extending treatment to 12 months in consecutive trials achieved a sustained improvement in dysmenorrhea, non-menstrual pelvic pain, and dyspareunia.31 The main side effects reported during elagolix clinical trials included hot flushes (at a rate of 24% and 48% for elagolix 150 mg once daily and elagolix 200 mg twice daily, respectively, most were mild to moderate and infrequently resulted in drug discontinuation) and a dose/duration related decrease in bone mineral density. Serum cholesterol, high- and low-density lipoproteins and triglycerides increased in a dose dependent manner with elagolix therapy. Lipid increases occurred within 1 to 2 months after the start of elagolix and remained stable thereafter over 12 months. Especially in patients with preexisting hypertriglyceridemia, an increase in serum triglycerides may lead to pancreatitis. No clinically significant endometrial changes have been reported with elagolix treatment.32 In women with normal liver functions, elagolix is recommended for up to 24 months for the lower dose (150 mg/day) or 6 months for the higher dose (200 mg twice/day).30–32 Amenorrhea is seen in 3.2% and in 4.9% of users in the 150 mg group (Elaris I and Elaris II, respectively) and in almost 5.6% and 8.7% of the elagolix 200 mg twice/day group (Elaris I and Elaris II, respectively)30,32. Pivotal trials of elagolix in treatment of endometriosis related pain are summarized in Table 1.
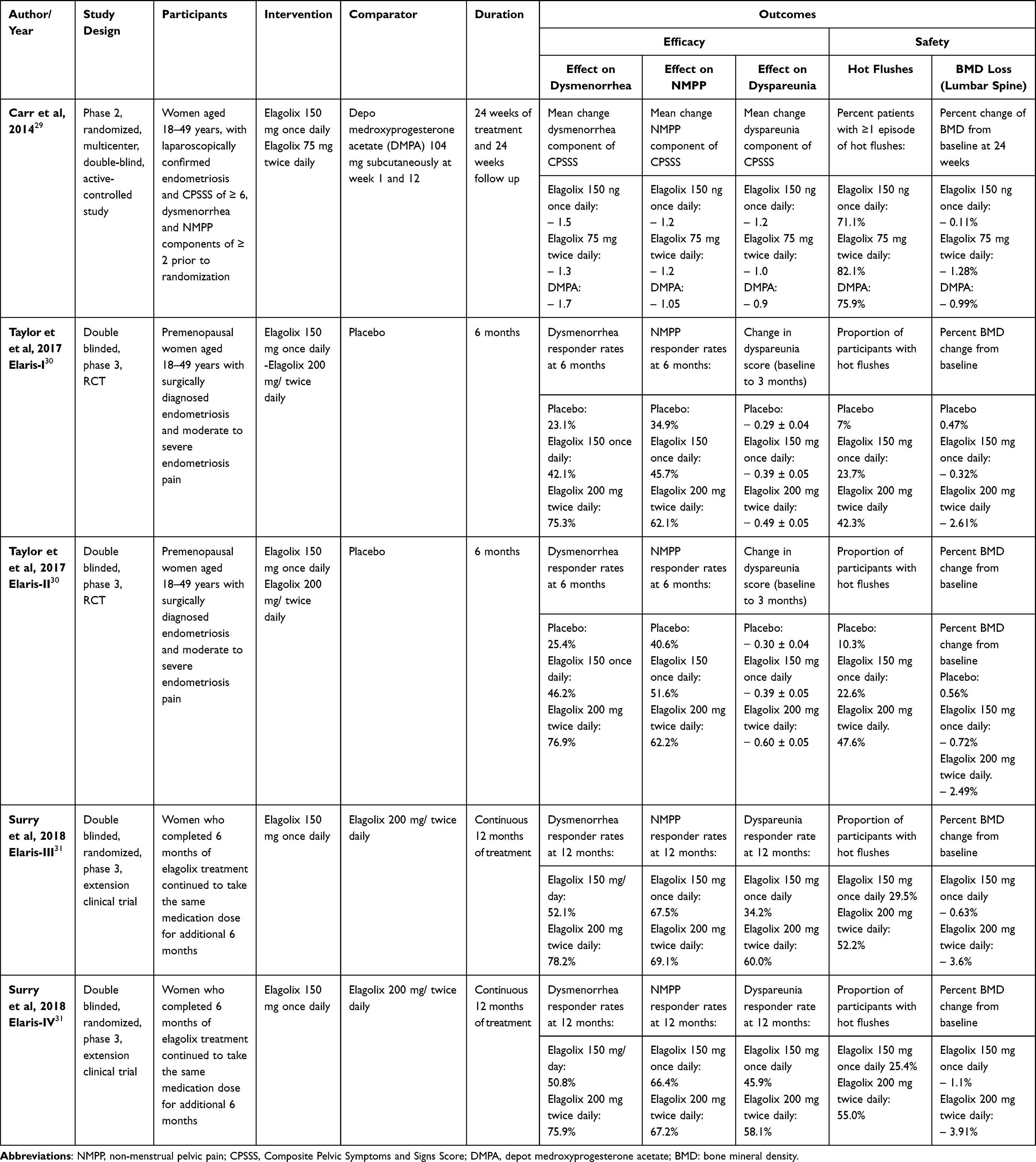 |
Table 1 Summary of Clinical Trials of Elagolix in the Treatment of Endometriosis Associated Pain |
Currently, clinical trials are underway to investigate the efficacy and safety of elagolix plus add back therapy on endometriosis pain (ClinicalTrials.gov identifier, NCT03213457). The introduction of elagolix in the United States and Canada was followed by that of relugolix, the next second-generation GnRH antagonist, during early 2019 in Japan.
Relugolix, a New Oral GnRH Antagonist for Treatment of Endometriosis- Related Pain
Relugolix is an orally active non-peptide GnRH antagonist. It competitively binds to GnRH receptors of the anterior pituitary, preventing the native GnRH molecule from binding to its receptor. Phase I clinical studies showed that multiple doses ≤40 mg can suppress pituitary gonadotropins and sustainably decrease gonadal steroid production.33 The drug was well tolerated without adverse effects of concern. In a phase 2 multicenter trial conducted across 108 clinical sites in Japan, Osuga et al randomized premenopausal women with moderate/severe endometriosis associated dysmenorrhea or pelvic pain to receive daily oral dose of relugolix (10 mg, 20 mg, or 40 mg), or a daily oral dose of placebo, or monthly injection of leuprolin. Endometriosis in this study was diagnosed by surgery or magnetic resonance imaging. Treatment continued for 12 weeks. The primary end point was change in pain intensity from baseline calculated as mean difference on a 0–100 mm visual analogue scale in the last 28 days before the end of treatment. Results showed that patients on the relugolix daily dose of 40 mg/day achieved improvement in pain comparable to that achieved by leuprolin, and significantly better than patients on placebo, on relugolix 10 mg/day or patients on 20 mg/day. Drug emerging adverse effects with a rate >10% included: hot flushes irregular menstruation, metrorrhagia, menorrhagia and hyperhidrosis. Bone mineral density (BMD) loss reached 2% within the 12 weeks treatment period for relugolix at 40 mg dose, which was similar to that observed in the leuprolin group. At the end of the 12 weeks treatment, amenorrhea rates were: 25.2% in women who received relugolix 10 mg/day, 54% in women on relugolix 20 mg/day, 92.2% of women on relugolix 40 mg/day, 97.5% in women on monthly leuprolin and only 2.2% in women on placebo. No clinically significant differences between groups were detected in ECG or laboratory test values.34 In an extension study, women who completed 12 weeks of relugolix treatment in the previous phase 2 trial were randomized to receive relugolix 10, 20, 40 mg/day, oral placebo, or a monthly injection of leuprolin for another 12 weeks. The primary end point was safety including BMD loss and other adverse events. At the end of the 12 weeks extension, improvement in pain scores was similar between women on the 40 mg/day relugolix treatment and those on leuprolin injection. Side effect profile, including BMD loss and hot flushes were also similar. Average durations from the last drug dose to return of menstrual cycles were 21 ± 12.3 days for women on relugolix 10 mg/day, 26 ± 12.93 days for relugolix 20 mg/day, 36.9± 9.49 days for relugolix 40 mg/day, 73.3 ± 21.11 days for leuprolin, and 17.3 ± 8.49 days for women on placebo. No clinically important differences in laboratory values or ECG were detected among study participants.35 Further studying the 40 mg oral daily dose of relugolix, Harada et al evaluated its efficacy and safety against leuprolin, as reference treatment, in women with moderate endometriosis related pain in a phase 3 randomized, double blinded, active control, non-inferiority clinical trial. Endometriosis was diagnosed surgically, using imaging to diagnose ovarian endometrioma or through identifying clinical signs suggestive of endometriosis. The primary end point was a change in VAS from baseline till 28 days before end of treatment. After 24 weeks of treatment, patients on relugolix 40 mg/day had improvement in their VAS for pain and reduction in endometrioma size which were similar to those in patients on leuprolin. Drug related adverse effects included hot flushes, headaches, and abnormal bleeding and had a similar profile between the two groups. Fewer women in the relugolix group (2.9%) discontinued treatment because of adverse events than in the leuprolin group (4.3%). BMD loss at the end of treatment was 4.8% in relugolix group which was similar to that in the leuprolin group. At the end of treatment, 94.2% of women on relugolix, and 100% of women on monthly leuprolin developed amenorrhea. When treatment was stopped, menses returned earlier in women treated with relugolix (median 38 days) than in women who were treated with leuprolin (median 68 days). A case of angina pectoris was reported and thought to be drug related.36 Clinical trials in which relugolix, without hormonal add-back therapy, was used to treat endometriosis related pain are summarized in Table 2.
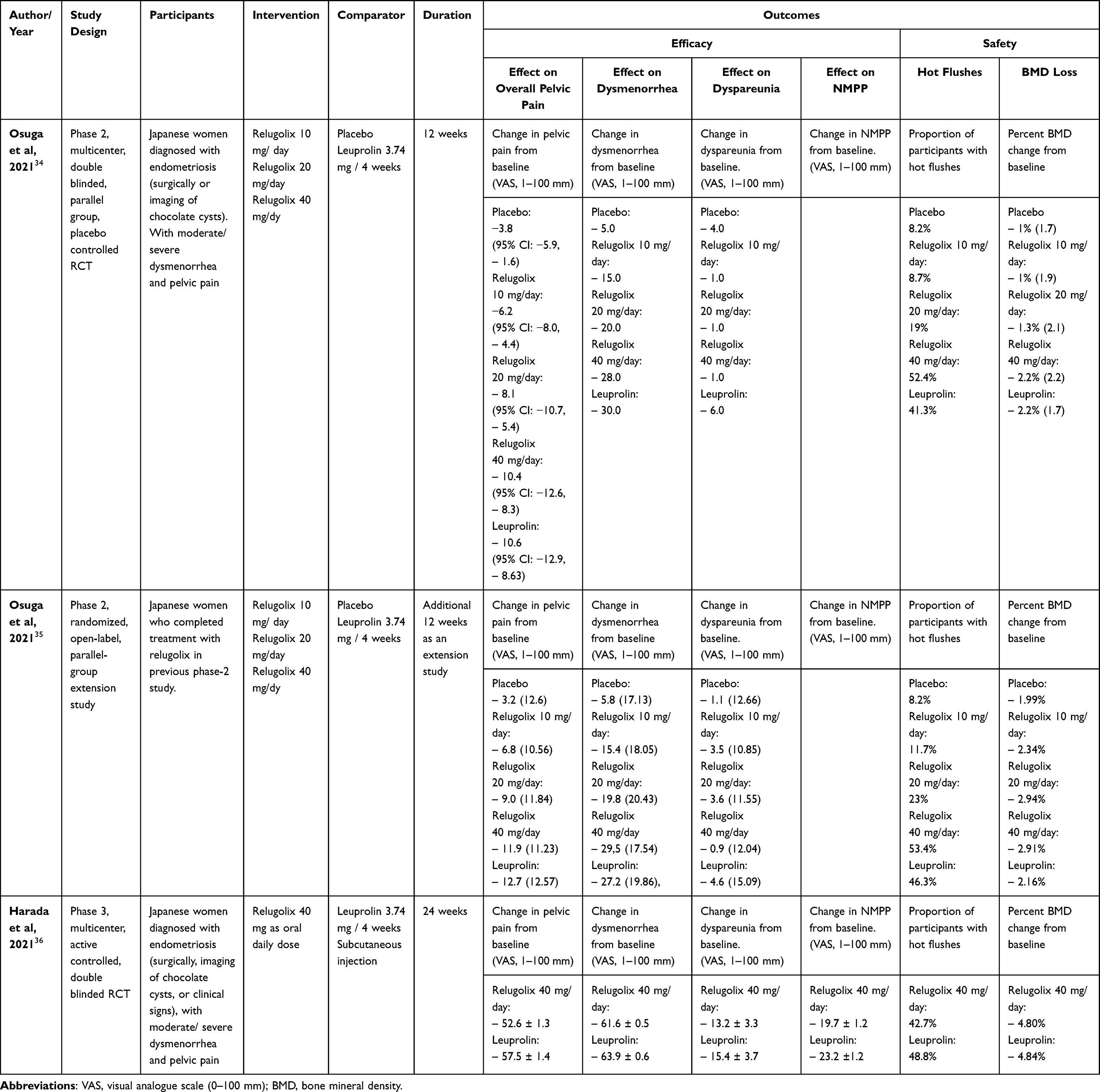 |
Table 2 Clinical Trials of Relugolix Without Hormonal Add-Back in Endometriosis Related Pain |
The above-mentioned studies confirmed the efficacy of relugolix at a daily dose of 40 mg/day in treating moderate to severe endometriosis related pain. Without add-back hormonal therapy, relugolix treatment is recommended to be limited to 24 weeks of treatment to avoid its adverse effects, especially on BMD loss. Two replicate, multicenter, randomized, placebo controlled, double blinded, phase 3 clinical trials (SPIRIT 1 and SPIRIT 2) investigated the safety and efficacy of relugolix 40 mg in combination with 1 mg estradiol and 0.5 mg norethindrone acetate as oral daily dose for the treatment of endometriosis associated pain. Women with moderate/severe dysmenorrhea and with non-menstrual pelvic pain were randomized 1:1:1 to receive placebo, relugolix combination therapy for 24 weeks, or a delayed relugolix regimen (12 weeks of relugolix monotherapy followed by 12 weeks of relugolix combination therapy). After 24 weeks of treatment, a significantly higher proportion of participants on the relugolix combination therapy achieved a clinically meaningful reduction in dysmenorrhea and noncyclic pelvic pain (−2.8 points on NRS) compared to placebo in both trials. Participants on relugolix combination therapy consistently showed improvement in dysmenorrhea, noncyclic pelvic pain, dyspareunia, and improvement in pain domain of EHP-30 compared to placebo. Women in relugolix combination therapy were less likely than the placebo arm to use analgesics or opioids at the end of treatment. Around 75% of participants in relugolix combination therapy developed amenorrhea or infrequent menses. More than 90% of participants resumed menses within 2 months of stopping treatment. BMD loss was less than 1% and was considered clinically insignificant versus baseline. Participants on the delayed relugolix regimen achieved efficacy outcomes similar to relugolix combination therapy, but with a higher proportion of hot flushes and a substantial BMD loss compared to the relugolix combination treatment. No cases of endometrial hyperplasia or endometrial cancer were reported. Laboratory values like liver functions and lipid profiles did not show clinically important differences versus placebo. Fourteen pregnancies were reported during the study period (eight in placebo, four in relugolix combination therapy, and two in delayed relugolix combination therapy groups) Many participants in the SPIRIT 1 and SPIRIT 2 trials entered an extension study in which they continued using relugolix combination therapy for the duration of 80 weeks.37 SPIRIT 1 and SPIRIT 2 clinical trials and their results are summarized in Table 3.
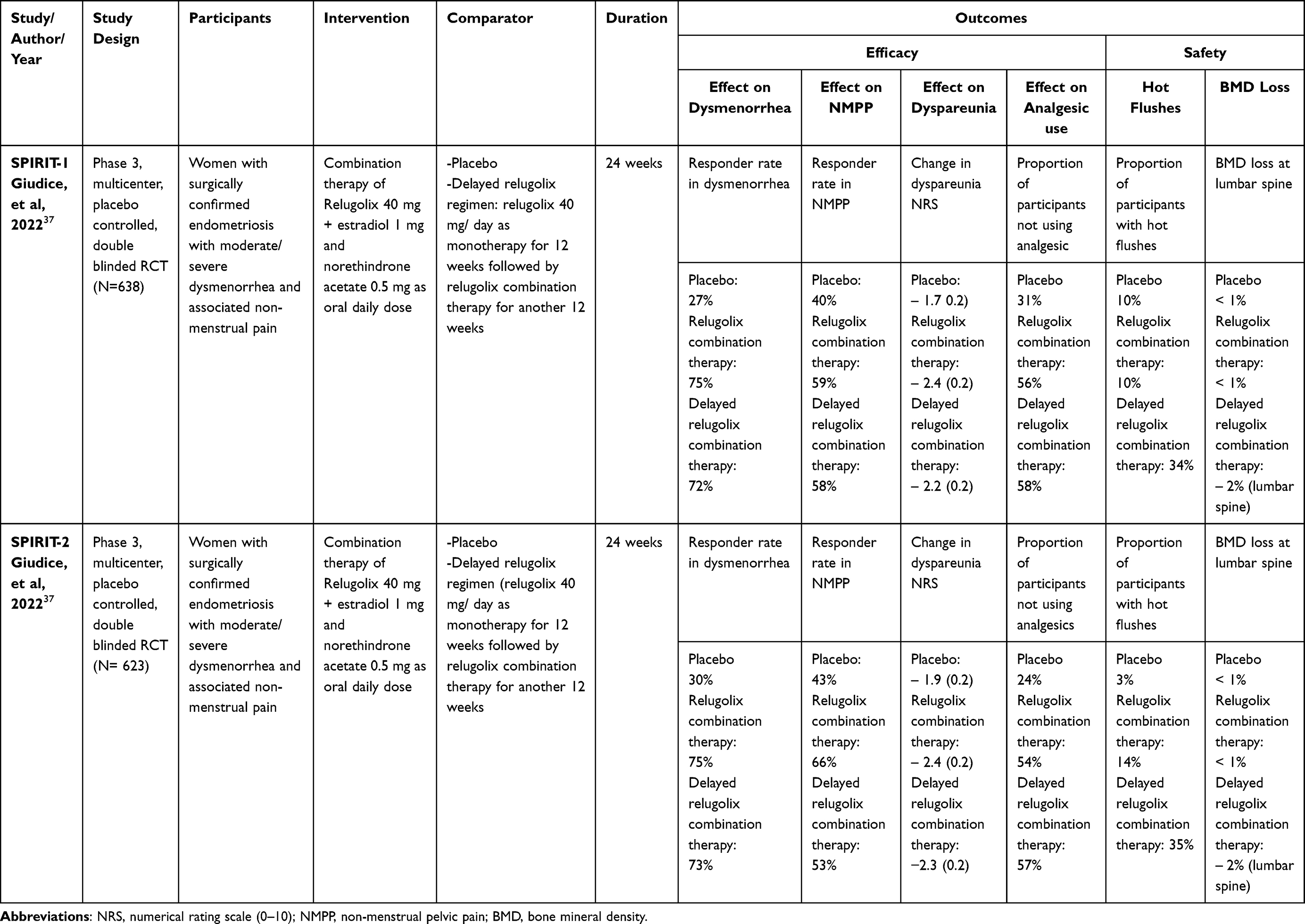 |
Table 3 Summary of Clinical Trials of Relugolix Plus Combination Hormonal Therapy in Endometriosis Related Pain |
Linzagolix, the Third Oral GnRH Antagonist in the Treatment of Endometriosis Associated Pain
Linzagolix is another oral GnRH antagonist with a high bioavailability and a half-life of 15–18 hours.16,22 In the EDELWEISS trial, investigators randomized 328 women complaining of pelvic pain associated with surgically diagnosed endometriosis to receive one of four different doses of oral linzagolix (50, 75, 100 and 200 mg/day) versus placebo for a total duration of 24 weeks. The study was conducted in 61 centers in Europe and US in the period 2016–2017. The proportion of women achieving ≥30% reduction of dysmenorrhea and non-menstrual pelvic pain was significantly higher in all linzagolix doses compared to placebo except the 50 mg dose at 12 and 24 weeks. For women complaining of dyspareunia, only the 200 mg daily dose achieved a statistically significant improvement at 12 weeks compared to the placebo. All linzagolix doses improved pain and powerlessness domains in EHP-30. Only 200 mg dose improved other domains (emotional wellbeing, self-image, and social support). The most common adverse effects were headaches and hot flushes that increased with increasing linzagolix dose. BMD loss increases with higher doses of linzagolix. At 24 weeks, around 52% of women on 200 mg linzagolix daily had a BMD loss >3%.38 Based on these results, linzagolix at a dose of 75 mg daily can be used to treat endometriosis related pain without a significant effect on BMD. A higher dose (200 mg/day) can achieve better control of pelvic pain but requires add-back therapy as BMD loss is substantial.39 Summary of the EDELWEISS clinical trial on the use of linzagolix for the treatment of endometriosis related pain is given in Table 4.
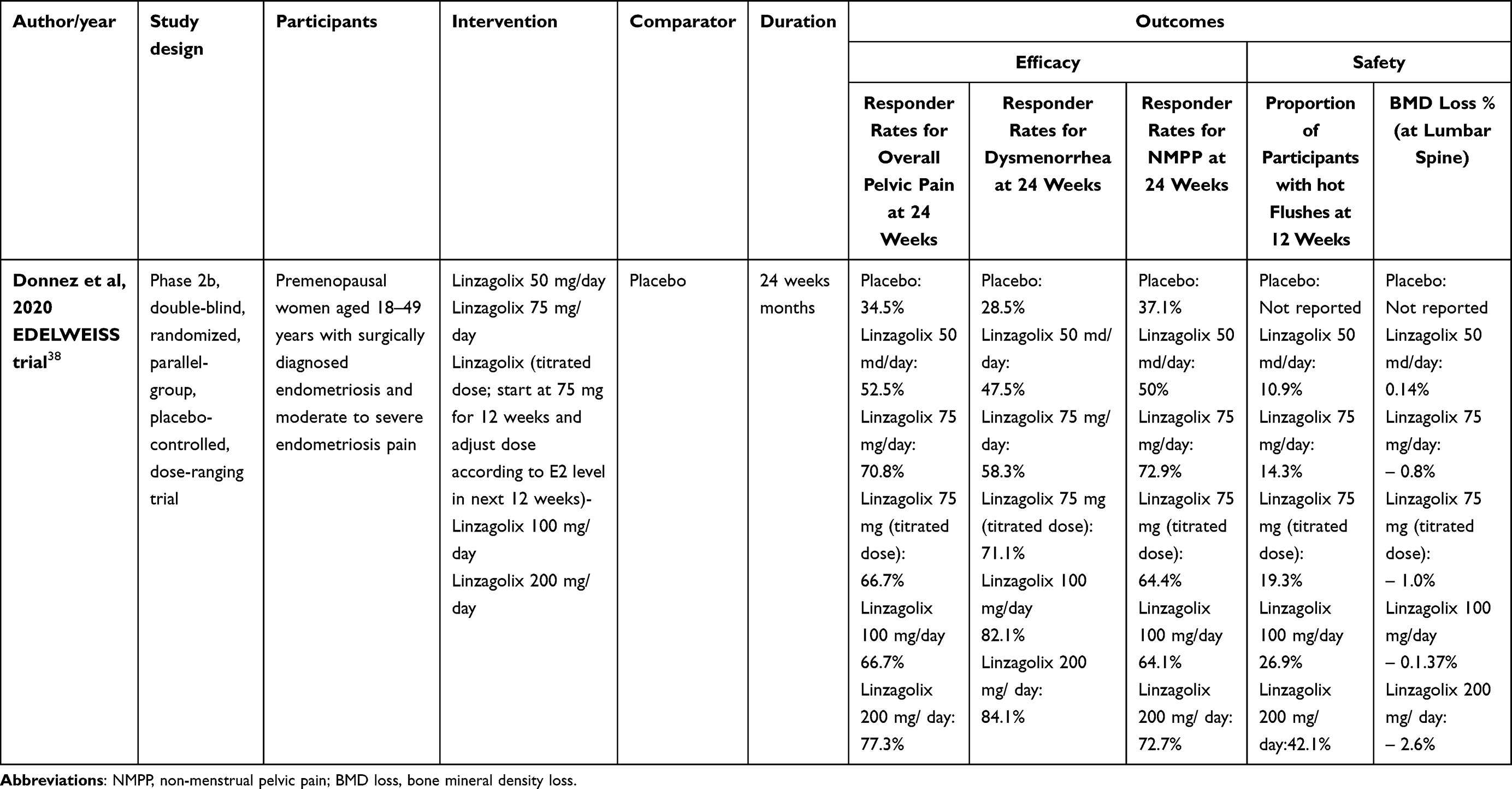 |
Table 4 Summary of EDELWEISS Trial of Linzagolix in Treatment of Endometriosis Associated Pain |
Discussion
Oral GnRH antagonists are a new class of agents for the treatment of endometriosis related pelvic pains. They allow dose dependent decreases in estradiol level which can achieve a balance between efficacy, side effects, and safety. Other advantages include oral administration, avoidance of initial flare effect which typically occurs with GnRH agonist treatment, and relatively rapid return of menses after drug discontinuation. Elagolix at a low dose of 150 mg once daily, or a higher dose of 200 mg twice daily significantly increased the proportion of women achieving clinically meaningful improvement in dysmenorrhea, noncyclic pelvic pain, and dyspareunia. Relugolix, at an oral dose of 40 mg/day is as effective as injectable depot GnRH agonists in treating endometriosis associated pain, with a similar side effect profile. Relugolix with hormonal add-back combination therapy did not reduce the efficacy but ameliorated the side effect profile (including hot flushes and BMD loss) and allowed extending treatment up to 24 weeks. Linzagolix, in a dose of 75 mg/day, is effective in reducing endometriosis associated pain. For severe pelvic pain and dyspareunia, linzagolix can be used in a high dose of 200 mg/day, but hormonal add back therapy is needed to preserve bone health.
Although the results of clinical use of oral GnRH antagonists are encouraging, they need to be interpreted with caution. In SPIRT 1 and SPRIT 2 clinical trials, relugolix combination therapy has been compared to a placebo, and no active comparator. The efficacy and safety of relugolix combination therapy is yet to be compared against first line treatment of endometriosis related pain including oral contraceptive pills and progestins in clinical trials.
Relugolix combination therapy did not completely suppress ovulation and six pregnancies occurred in women on this treatment regimen in SPIRIT 1 and SPIRIT 2 trials.37 For this reason, women using relugolix combination therapy should take the extra treatment burden of using non-hormonal contraception. On the other hand, protection against unwanted pregnancy is a given advantage when using oral contraceptive pills or progestins for controlling endometriosis associated pain.
The added therapeutic value of oral GnRH antagonists over the GnRH agonists is not clear.40 When relugolix was tested against leuprolin, it was non-inferior in efficacy, however, adverse effects (including hypoestrogenic side effects such as hot flushes and BMD loss) were also similar.36 This means the hoped-for delicate balance between efficacy and safety was not realized by using relugolix alone. It then became a logical step to incorporate hormonal add-back therapy with relugolix to mitigate these hypoestrogenic effects,37 in a very similar way to add-back therapy with GnRH agonists.
As endometriosis is a chronic disorder, and women often need to use medical treatment for long periods, future research should focus on extending treatment beyond the 24 weeks mark. An ongoing study is investigating the safety and efficacy of relugolix combination therapy for up to 80 weeks (ClinicalTrials.gov Identifier: NCT03654274). Preliminary data show improved dysmenorrhea and non-menstrual pain with minimal effect on BMD at 52 weeks of treatment.41 Furthermore, it would also be interesting to study particular phenotypes of endometriosis in which relugolix combination therapy is most effective (including patient’s age, clinical presentation, and type of endometriosis lesions).42
Finally, costs of the oral antagonist therapy should be considered before prescribing it to patients. The list price for a 28-day supply of relugolix combination therapy (Myfembree) is $1,086.71.43 One cost effectiveness study concluded that elagolix was cost effective as compared to leuprolide acetate in the treatment of moderate to severe endometriosis related pain over 1- and 2-year time horizons.44 However, no studies investigated the cost effectiveness of elagolix, relugolix (alone or as combination therapy), or linzagolix versus the cheaper first line treatments including oral contraceptive pills or progestins. In addition, the availability of relugolix combination therapy is another issue to consider. It is available in the USA, Canada, and EU. So, relugolix combination therapy is not available to patients in other parts of the world.
In conclusion, oral GnRH antagonists, including elagolix, relugolix alone or in combination therapy, and linzagolix, represent a promising drug addition when treating endometriosis related pain. However, several questions need to be investigated and answered further before they can be correctly positioned in the algorithm of treatment of endometriosis associated pelvic pain.
Disclosure
Professor Ayman Al-Hendy reports grants from the National Institutes of Health (NIH), during the conduct of the study; personal fees from AbbVie, personal fees from Bayer, personal fees from ObsEva, personal fees from Myovant Sciences, outside the submitted work; in addition, Professor Ayman Al-Hendy has a patent: Patent for novel diagnostics and therapeutics for uterine sarcoma pending to US Patent. The authors report no other conflicts of interest in this work.
References
1. Zondervan KT, Becker CM, Missmer SA. Endometriosis. N Engl J Med. 2020;382:1244–1256. doi:10.1056/NEJMra1810764
2. Shafrir AL, Farland LV, Shah DK, et al. Risk for and consequences of endometriosis: a critical epidemiologic review. Best Pract Res Clin Obstet Gynaecol. 2018;51:1–15. doi:10.1016/j.bpobgyn.2018.06.001
3. Prescott J, Farland LV, Tobias DK, et al. A prospective cohort study of endometriosis and subsequent risk of infertility. Hum Reprod. 2016;31(7):1475–1482. doi:10.1093/humrep/dew085
4. Taylor HS, Kotlyar AM, Flores VA. Endometriosis is a chronic systemic disease: clinical challenges and novel innovations. Lancet. 2021;397(10276):839–852. doi:10.1016/S0140-6736(21)00389-5
5. Greene R, Stratton P, Cleary SD, Ballweg ML, Sinaii N. Diagnostic experience among 4334 women reporting surgically diagnosed endometriosis. Fertil Steril. 2009;91:32–39. doi:10.1016/j.fertnstert.2007.11.020
6. Nnoaham KE, Hummelshoj L, Webster P, et al. Impact of endometriosis on quality of life and work productivity: a multicenter study across ten countries. Fertil Steril. 2011;96(2):366–373.e8. doi:10.1016/j.fertnstert.2011.05.090
7. Horne AW, Missmer SA. Pathophysiology, diagnosis, and management of endometriosis. BMJ. 2022;14(379):e070750. doi:10.1136/bmj-2022-070750
8. Chapron C, Marcellin L, Borghese B, Santulli P. Rethinking mechanisms, diagnosis and management of endometriosis. Nat Rev Endocrinol. 2019;15(11):666–682. doi:10.1038/s41574-019-0245-z
9. Becker CM, Gattrell WT, Gude K, Singh SS. Reevaluating response and failure of medical treatment of endometriosis: a systematic review. Fertil Steril. 2017;108(1):125. doi:10.1016/j.fertnstert.2017.05.004
10. Vercellini P, Barbara G, Abbiati A, Somigliana E, Viganò P, Fedele L. Repetitive surgery for recurrent symptomatic endometriosis: what to do? Eur J Obstet Gynecol Reprod Biol. 2009;146:15–21. doi:10.1016/j.ejogrb.2009.05.007
11. de Ziegler D, Pirtea P, Carbonnel M, et al. Assisted reproduction in endometriosis. Best Pract Res Clin Endocrinol Metab. 2019;33(1):47–59. doi:10.1016/j.beem.2018.10.001
12. Lier MCI, Malik RF, Ket JCF, Lambalk CB, Brosens IA, Mijatovic V. Spontaneous hemoperitoneum in pregnancy (SHiP) and endometriosis - A systematic review of the recent literature. Eur J Obstet Gynecol Reprod Biol. 2017;219:57–65. doi:10.1016/j.ejogrb.2017.10.012
13. Bedaiwy MA, Alfaraj S, Yong P, Casper R. New developments in the medical treatment of endometriosis. Fertil Steril. 2017;107(3):555–565. doi:10.1016/j.fertnstert.2016.12.025
14. Barbara G, Buggio L, Facchin F, Vercellini P. Medical treatment for endometriosis: tolerability, quality of life and adherence. Front Glob Women’s Health. 2021;27(2):729601. doi:10.3389/fgwh.2021.729601
15. Vercellini P, Buggio L, Berlanda N, Barbara G, Somigliana E, Bosari S. Estrogen-progestins and progestins for the management of endometriosis. Fertil Steril. 2016;106:1552–1571.e2. doi:10.1016/j.fertnstert.2016.10.022
16. Donnez J, Dolmans MM. Endometriosis and medical therapy: from progestogens to progesterone resistance to GnRH antagonists: a review. J Clin Med. 2021;10:1085. doi:10.3390/jcm10051085
17. Becker CM, Bokor A, Heikinheimo O, et al. ESHRE guideline: endometriosis. Hum Reprod Open. 2022;2022(2):hoac009. doi:10.1093/hropen/hoac009
18. Practice Committee of the American Society for Reproductive Medicine. Treatment of pelvic pain associated with endometriosis: a committee opinion. Fertil Steril. 2014;101:927–935. doi:10.1016/j.fertnstert.2014.02.012
19. Vercellini P, Buggio L, Frattaruolo MP, Borghi A, Dridi D, Somigliana E. Medical treatment of endometriosis-related pain. Best Pract Res Clin Obstet Gynaecol. 2018;51:68–91. doi:10.1016/j.bpobgyn.2018.01.015
20. Ailawadi RK, Jobanputra S, Kataria M, Gurates B, Bulun SE. Treatment of endometriosis and chronic pelvic pain with letrozole and norethindrone acetate: a pilot study. Fertil Steril. 2004;81:290–296. doi:10.1016/j.fertnstert.2003.09.029
21. Ferrero S, Venturini PL, Ragni N, Camerini G, Remorgida V. Pharmacological treatment of endometriosis: experience with aromatase inhibitors. Drugs. 2009;69:943–952. doi:10.2165/00003495-200969080-00001
22. Ng J, Chwalisz K, Carter DC, Klein CE. Dose-dependent suppression of gonadotropins and ovarian hormones by elagolix in healthy premenopausal women. J Clin Endocrinol Metab. 2017;102:1683–1691. doi:10.1210/jc.2016-3845
23. Osuga Y, Enya K, Kudou K, et al. Oral gonadotropin-releasing hormone antagonist relugolix compared with leuprorelin injections for uterine leiomyomas: a randomized controlled trial. Obstet Gynecol. 2019;133:423–433. doi:10.1097/AOG.0000000000003141
24. Donnez J, Dolmans MM. GnRH antagonists with or without add-back therapy: a new alternative in the management of endometriosis? Int J Mol Sci. 2021;22(21):11342. doi:10.3390/ijms222111342
25. Donnez J, Taylor RN, Taylor HS. Partial suppression of estradiol: a new strategy in endometriosis management? Fertil. Steril. 2017;107:568–570. doi:10.1016/j.fertnstert.2017.01.013
26. Mikuš M, Šprem Goldštajn M, Laganà AS, Vukorepa F, Clinical Efficacy ĆM. Pharmacokinetics, and Safety of the available medical options in the treatment of endometriosis-related pelvic pain: a scoping review. Pharmaceuticals. 2023;16(9):1315. doi:10.3390/ph16091315
27. Zajec V, Mikuš M, Vitale SG, et al. Current status and challenges of drug development for hormonal treatment of endometriosis: a systematic review of randomized control trials. Gynecol Endocrinol. 2022;38(9):713–720.
28. Taylor HS, Dun EC, Chwalisz K. Clinical evaluation of the oral gonadotropin-releasing hormone-antagonist elagolix for the management of endometriosis-associated pain. Pain Manag. 2019;9:497–515. doi:10.2217/pmt-2019-0010
29. Carr B, Dmowski WP, O’Brien C, et al. Elagolix, an oral GnRH antagonist, versus subcutaneous depot medroxyprogesterone acetate for the treatment of endometriosis: effects on bone mineral density. Reprod Sci. 2014;21(11):1341–1351. doi:10.1177/1933719114549848
30. Taylor HS, Giudice LC, Lessey BA, et al. Treatment of endometriosis-associated pain with elagolix, an Oral GnRH antagonist. N Engl J Med. 2017;377(1):28–40. doi:10.1056/NEJMoa1700089
31. Surrey E, Taylor HS, Giudice L, et al. Long-term outcomes of elagolix in women with endometriosis: results from two extension studies. Obstet Gynecol. 2018;132(1):147–160. doi:10.1097/AOG.0000000000002675
32. Leyland N, Estes SJ, Lessey BA, Advincula AP, Taylor HS, Clinician’s A. Guide to the Treatment of Endometriosis with Elagolix. J Womens Health. 2021;30(4):569–578. doi:10.1089/jwh.2019.8096
33. Markham A. Relugolix: first Global Approval. Drugs. 2019;79(6):675–679. doi:10.1007/s40265-019-01105-0
34. Osuga Y, Seki Y, Tanimoto M, Kusumoto T, Kudou K, Terakawa N. Relugolix, an oral gonadotropin-releasing hormone receptor antagonist, reduces endometriosis-associated pain in a dose-response manner: a randomized, double-blind, placebo-controlled study. Fertil Steril. 2021;115(2):397–405. doi:10.1016/j.fertnstert.2020.07.055
35. Osuga Y, Seki Y, Tanimoto M, Kusumoto T, Kudou K, Terakawa N. Relugolix, an oral gonadotropin-releasing hormone (GnRH) receptor antagonist, in women with endometriosis-associated pain: phase 2 safety and efficacy 24-week results. BMC Womens Health. 2021;21(1):250. doi:10.1186/s12905-021-01393-3
36. Harada T, Osuga Y, Suzuki Y, Fujisawa M, Fukui M, Kitawaki J. Relugolix, an oral gonadotropin-releasing hormone receptor antagonist, reduces endometriosis-associated pain compared with leuprorelin in Japanese women: a phase 3, randomized, double-blind, noninferiority study. Fertil Steril. 2022;117(3):583–592. doi:10.1016/j.fertnstert.2021.11.013
37. Giudice LC, As-Sanie S, Arjona Ferreira JC, et al. Once daily oral relugolix combination therapy versus placebo in patients with endometriosis-associated pain: two replicate phase 3, randomised, double-blind, studies (SPIRIT 1 and 2). Lancet. 2022;399(10343):2267–2279. doi:10.1016/S0140-6736(22)00622-5
38. Donnez J, Taylor HS, Taylor RN, et al. Treatment of endometriosis-associated pain with linzagolix, an oral gonadotropin- releasing hormone-antagonist: a randomized clinical trial. Fertil Steril. 2020;114(1):44–55. doi:10.1016/j.fertnstert.2020.02.114
39. Buggio L, Dridi D, Barbara G, et al. Novel pharmacological therapies for the treatment of endometriosis. Expert Rev Clin Pharmacol. 2022;15(9):1039–1052. doi:10.1080/17512433.2022.2117155
40. Vercellini P, Viganò P, Barbara G, et al. Elagolix for endometriosis: all that glitters is not gold. Hum Reprod. 2019;34(2):193–199. doi:10.1093/humrep/dey368
41. As-Sanie S, Giudice L, Abrao MS, et al. O-132 sustained efficacy and safety of relugolix combination therapy in women with endometriosis-associated pain: SPIRIT 52-week data. Hum Reprod. 2021;36(suppl 1):
42. Saraswat L, Bhattacharya S. Relugolix combination therapy for endometriosis pain. Lancet. 2022;399(10343):2244–2245. doi:10.1016/S0140-6736(22)00663-8
43. Myovant Sciences GmbH and Pfizer Inc. Cost and support for myfembree: cost guide; 2003. Available from: https://www.myfembree.com/cost-and-support/#download-cost-guide.
44. Wang ST, Johnson SJ, Mitchell D, Soliman AM, Vora JB, Agarwal SK. Cost-effectiveness of elagolix versus leuprolide acetate for treating moderate-to-severe endometriosis pain in the USA. J Comp Eff Res. 2019;8(5):337–355. doi:10.2217/cer-2018-0124
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.