")
Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 14
Nutritional Rickets Among Children: A Retrospective Study from Saudi Arabia
Authors Darraj H , Hakami KM , Maghrabi R, Bakri N, Alhazmi MH, Names AA , Akkur A , Sayegh M, Alhazmi A, Khubrani SM, Gohal G , Alomar AH, Alhazmi AH
Received 11 June 2023
Accepted for publication 4 October 2023
Published 11 October 2023 Volume 2023:14 Pages 301—308
DOI https://doi.org/10.2147/PHMT.S425459
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Hussam Darraj,1 Khalid M Hakami,1 Rawan Maghrabi,1 Nawaf Bakri,1 Mohammed H Alhazmi,1 Abdellh A Names,1 Ahmed Akkur,1 Maram Sayegh,1 Asma Alhazmi,1 Saad M Khubrani,1 Gassem Gohal,1 Amro H Alomar,2 Abdulaziz H Alhazmi1
1Faculty of Medicine, Jazan University, Jazan, 45142, Saudi Arabia; 2King Fahad Central Hospital, Ministry of Health, Jazan, 85534, Saudi Arabia
Correspondence: Abdulaziz H Alhazmi, Email [email protected]
Background: Nutritional rickets remains a significant concern in certain countries, with increasing prevalence attributed to factors such as limited sunlight exposure and undernourishment. This study aimed to identify the factors associated with rickets due to nutritional deficiency in children from Jazan Province, southwestern Saudi Arabia.
Methods: A retrospective cross-sectional study was conducted using descriptive data from medical records at a tertiary hospital in Jazan Province. Records of patients diagnosed with rickets between January 2010 and December 2020 were analyzed. Symptomatic rickets cases from pediatric clinics were included, and diagnoses were based on biochemical and clinical tests. Risk factors were assessed using patient medical records. Data were analyzed using percentages, mean, and standard deviation.
Results: The study included 84 patients with rickets (53 females and 31 males), primarily between 11– 18 years old. The mean body mass index (BMI) of the participants was 21.21. The most common risk factor was nutritional deficiencies, including vitamin D deficiency or calcium deficiency, with 75 patients reporting a family history of vitamin D deficiency. The children had limited sunlight exposure and low levels of calcium and vitamin D. Malnutrition was identified as the highest risk factor for rickets in the study population.
Conclusion: Nutritional rickets appears to be prevalent in the Jazan Province, emphasizing the need for government organizations to address this preventable disease. Adequate sun exposure and recommended dietary vitamin D intake are crucial to prevent rickets, as this study detected inadequate levels of calcium and vitamin D in children. National studies are required to further identify risk factors and develop appropriate strategies.
Keywords: nutritional rickets, vitamin D, breastfeeding, Saudi Arabia
Introduction
Rickets is an ailment in which the bones of a growing child are affected. It can be due to a lack of enough calcium and phosphate in the body, also known as nutritional rickets. Calcium and phosphate are the two elements that are crucial for the proper growth of bone. Nutritional rickets can be caused due to less intake of food containing calcium and phosphate or absorption from the gastrointestinal tract.1
In underdeveloped nations worldwide, the deficiency of cholecalciferol, also known as vitamin D, is among the primary causes of nutritional rickets, which is considered among the top five pediatric diseases.2,3 The prevalence of nutritional rickets is still alarming in developed nations.2,4–7 The prevalence of rickets has increased in Europe and North America, where the yearly frequency is around 3 in every 100,000 children of every age.8–11
The physical comorbidities associated with rickets tend to stay throughout late childhood and adolescence of the child as well as pose acute life-threatening consequences that make rickets a significant health burden.12 Even in the most industrialized countries, there are currently no effective community-based preventive interventions to prevent rickets.12 Because the initial symptoms of rickets are not easily noticeable, and an early diagnosis is still a challenge.13 Children suffering from rickets frequently exhibit paleness, agitation, insomnia, and excessive perspiration.13 The other reported symptoms are flaring of the lower anterior thoracic wall, prominence of the costochondral junction (rachitic rosary), and frontal bossing. Genu valgum or genu varum is a condition that develops once the child with rickets learns how to walk and carry weight. Malnutrition leading to muscular atrophy and increased susceptibility to infection are considered some examples of systemic symptoms of rickets.14
Multiple other risk factors have been linked to nutritional rickets, including exclusive breastfeeding, cow milk consumption, lack of sunlight exposure, malnutrition, and poor maternal nutritional status during pregnancy.15 In Saudi Arabia, cases of nutritional rickets are still seen in pediatric clinics, with a prevalence rate of 15%,16 and may be attributed to behavioral factors such as less exposure to the sun despite the sunny weather. Due to the scarcity of published reports about the epidemiology of this disease or its associated factors, this study aims to determine the predisposed factors contributing to causing nutritional rickets in children of Jazan province, Saudi Arabia.
Materials and Methods
Study Design
This was a retrospective, observational study using descriptive data from the medical records of a tertiary hospital in Jazan. This study was conducted among children in the Jazan region, located in the southwest of Saudi Arabia, north of Yemen, with a population of 1.6 million people. The collection of data was from the admitted patients diagnosed with rickets from January 2010 to December 2020 in the King Fahad Central Hospital, Jazan. Eighty-four participants were included in the current study, the record of which indicated that they were suffering from rickets. The study included data from participants of both genders and pediatric age groups (from the age group of 1–18 years), and the King Fahd Central Hospital’s medical records inquiry system identified all patients who had undergone a 25 (OH)Vit D test in the past 10 years. The criteria we used in this study depended on the following articles16,17
Data Collection
The collection of data was conducted from the self-managed patient records of the hospital. The following data were collected: age, gender, nationality, diagnosis, comorbidities, predisposing factors, and radiological findings. Additionally, the results of the biochemical tests (calcium, phosphorus, alkaline phosphatase, vitamin D, PTH, albumin, AST, ALP eGFR, and creatinine) and their serum reference values from the confirmed cases were also collected from the hospital records.
Statistical Analyses
The data were analyzed using SPSS version 23 software. Frequency, percentage, mean, and standard deviation for the findings were estimated.
Ethical Considerations
The study protocol was approved by the internal review board of the Ethics Committee of the Ministry of Health in the Jazan Region. Approval No: 22055; date: 15 June 2022. Strict confidentiality measures were implemented to safeguard the collected data. The research involved a secondary analysis of routinely collected anonymized monitoring data, adhering to the ethical principles of the Helsinki Declaration and the specific guidelines stipulated by the National Committee of Bioethics in Saudi Arabia. Data were sourced from patient charts and/or laboratory databases as part of routine clinical procedures. Personal information and identifiable details of participants were excluded from the study to ensure anonymity and privacy
Results
Baseline Characteristics of the Participants
Out of the total participants (n=84), the majority of them were female (63.10%) and the remaining were males (36.90%). We classified the participants into three age groups: 1 to 5 years representing 16.67%, 6 to 11 years representing 25% of the total participants, and the rest of the participants (58.33%) were from 11 to 18 years. Most of the participants reside in Abu-Arish or Jazan (28.57%, and 23.81% respectively).
In terms of sun exposure as a factor, 72.81% of the patients acknowledged that they were exposed to the sun 1 to 2 times a day while 26.19% stated that they were not exposed to the sun. Additionally, the birth weight and height of the patients were also documented and showed average body weight at birth was 2.74±2.23 kg (ranging from 2.50 to 3.5 kg). At the time of presentation to the hospital, the mean height was 131±28.3 cm, weight was 38±21.45 kg, and BMI of 21.21 ±9.30, respectively. We classified the participants into four BMI groups: 34% of the participants were underweight, 33.33% were in the normal range, 14.29% of the participants were overweight and the rest of the participants (11.90%) were obese as shown in Table 1.
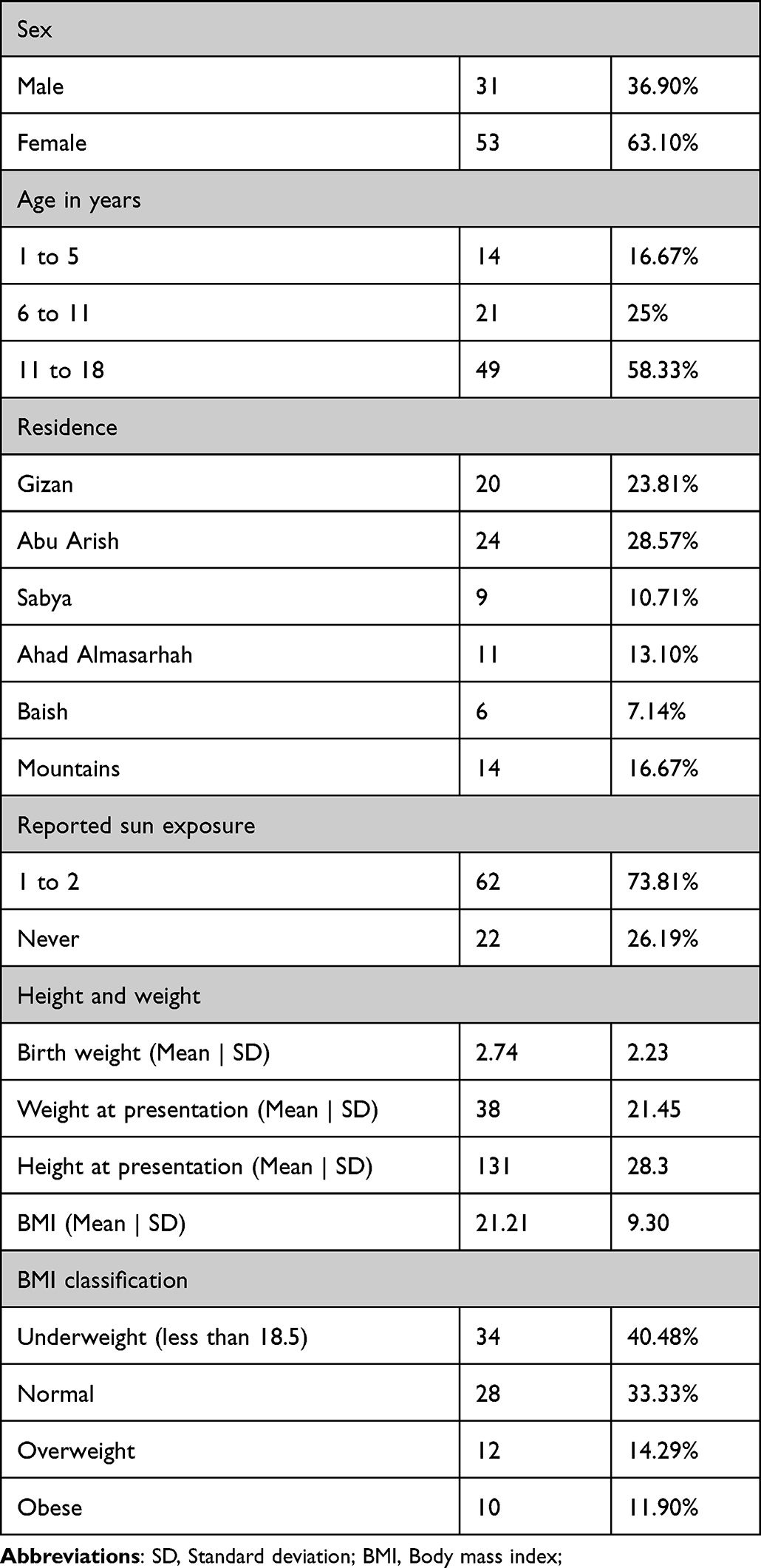 |
Table 1 Demographic Characteristics of the Participants (n=84) |
Laboratory Data of the Participants at the Time of Admission
The data indicated that the laboratory investigations of all the participants were conducted at the time of admission. The mean value of the lab values of vitamin D, serum calcium, phosphate, liver enzymes, albumin, PTH, creatinine, and EGFR are shown in Table 2. Low levels of vitamin D were present in all the participants with a mean of 16.91 ±9.54 mmol/L (normal range: above 50 mmol/L), high level of PTH with a mean of 79.39 ±9.73 pmol/L (normal; 1.95–49), a level of Phosphate was 1.36± 1.67 mmol/L (normal; 0.81–1.58), ALP of 205 ±43.79U/L (normal; 100–560), CA of 0.4089±2.27 mmol/L (normal 2.1–2.55), EGFR of 104,44 ±18.31 mL/min/1.73m^2 (normal ≥90) were present.
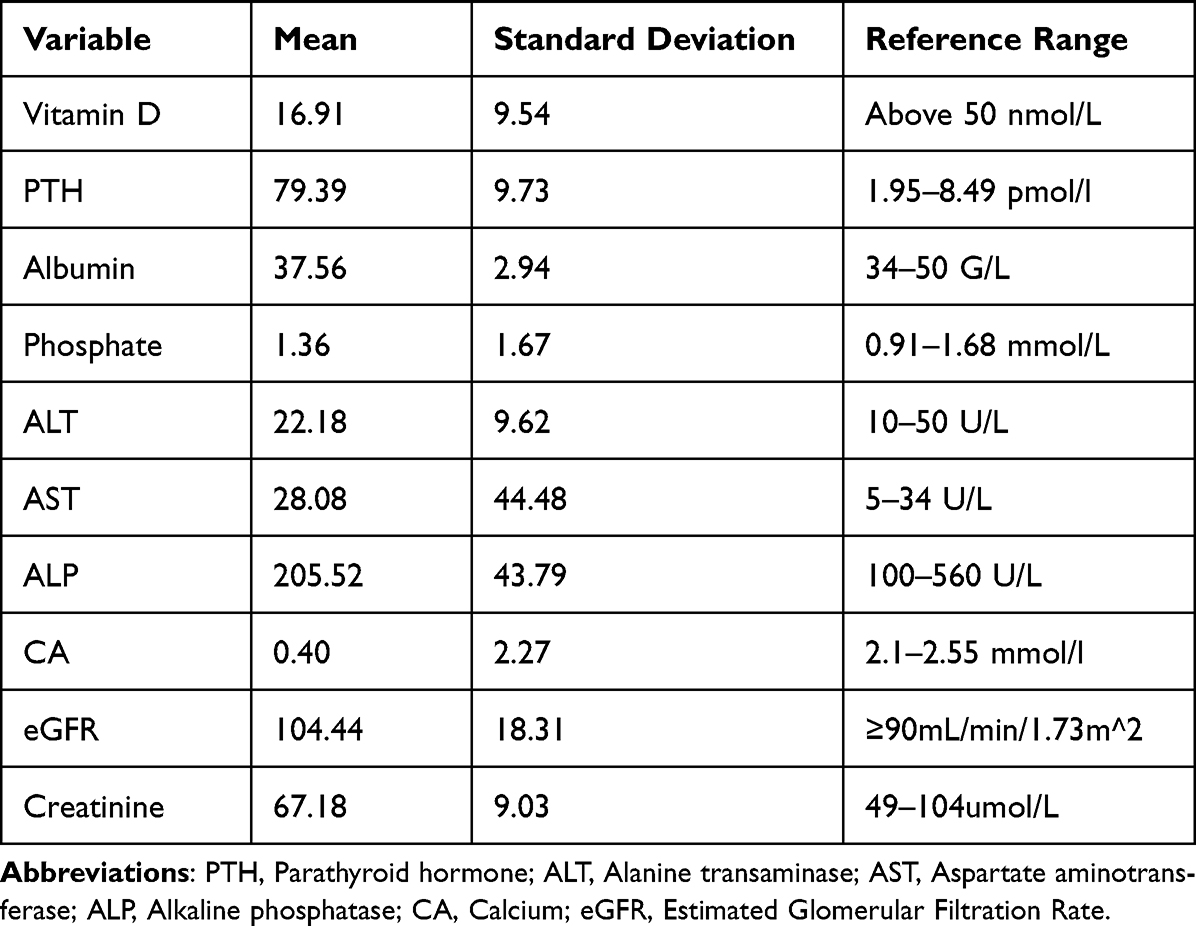 |
Table 2 Laboratory Data of the Participants at the Time of Admission |
Risk Factors Among Participants
In terms of risk factors, 89.29% (n=75) of the patients have a history of vitamin D deficiency in their family members while 76.19% (n=64) of them were malnourished or low milk or dairy.
Exclusively breastfed infants were found to be 8.33% (n=7) and the dark-skinned ethnic population was only 2.38% (n=2) of the patients. Medications such as steroids or anticonvulsants were used by only 2.38% (n=2) of the patients, while 16.67% (n=14) of them were premature or small for their gestational age. However, other risk factors, including living in a cold environment which was found to affect 15.48% (n=13), respectively as documented in Table 3.
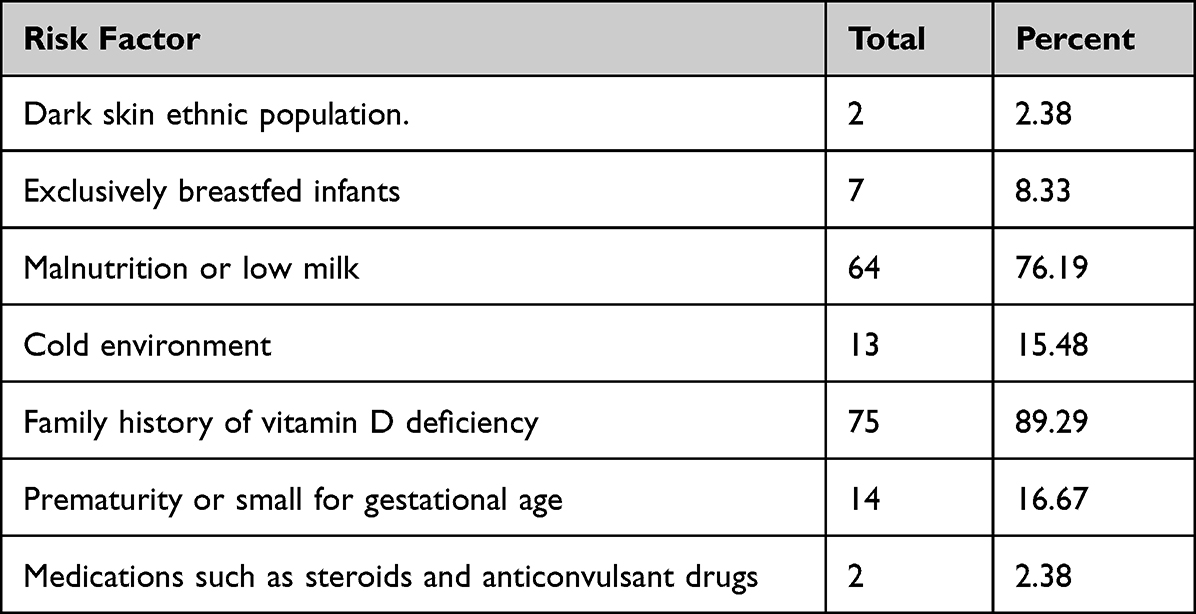 |
Table 3 Risk Factors Associated with Nutritional Rickets |
Clinical Manifestation Among Participants
The most frequent clinical signs among children included craniotabes (53.57%); frontal bossing (16.67%); rachitic rosary (14.29%); parietal bossing (14.29%) thickened epiphysis (13.10%) respectively, as documented in Table 4.
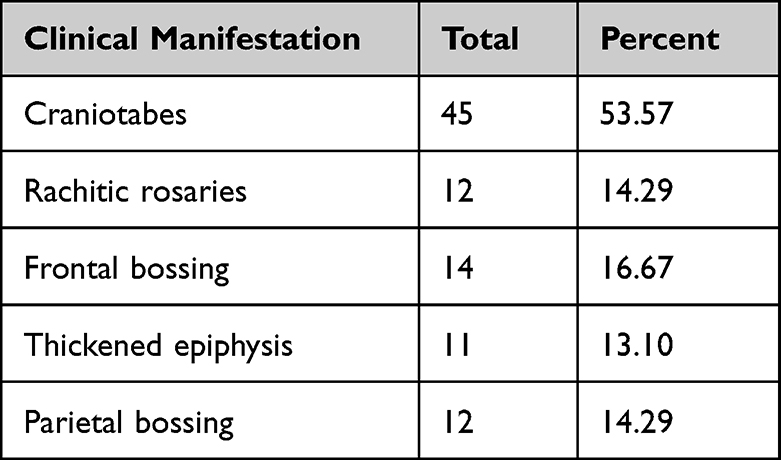 |
Table 4 Clinical Manifestations Associated with Nutritional Rickets |
Discussion
Rickets is a significant problem during a child’s early growth, mainly when there is a deficiency in vitamin D and other minerals necessary for bone calcification and mineralization.18,19 While Jazan Province in Saudi Arabia enjoys year-round sunny weather, which suggests much UV radiation for vitamin D production, several investigations at the national level have revealed decreased levels of 25-hydroxy-VitD in the majority of rickets-associated cases.16,20–22 These cases may be due to behavioral causes as Saudis prefer to stay indoors. The incidence of rickets in Jazan Province remains unknown and only a single study conducted over ten years involving 84 individuals indicated a deficiency in vitamin D in all cases.16 However, this rate appears low compared to other studies conducted at the national and international levels, possibly due to differences in study nature, methodology, timing, or missed cases.16,21–27
It is well-established that children are at higher risk of nutritional rickets, with the most affected age groups in our study falling between 11–18 years, consistent with previous research conducted in Saudi Arabia.28 Adolescents and young adults have higher mineral requirements for proper bone growth and are more prone to vitamin D deficiency-associated diseases.29–31 It has been observed that children not exposed to sunlight are more susceptible to rickets, as sunlight is the primary source of vitamin D.32–35 Restricted sunlight exposure is recognized as a significant risk factor for vitamin D deficiency, and our study indicated that 73.81% of participants had limited exposure to sunlight. At the same time, the rest denied any sun exposure. This finding aligns with previous studies conducted in Saudi Arabia and Libya, where many children with rickets had limited or no sunlight exposure.21,36–38 Thus, further investigations are required and interventions must be prioritized by health officials.
Although obesity contributes to vitamin D deficiency due to the sequestration of vitamin D by extensive fat reserves, our study found that most individuals with rickets were underweight (40.48%). This contrasts with studies conducted in Qatar, Pakistan, and Sudan, which reported higher percentages of underweight children.39–41 Additionally, our study revealed a lower mean birth weight than studies conducted in Kuwait and the United States, emphasizing the complex relationship between body weight and rickets.13,42,43 Nonetheless, maintaining an average body weight appears to be a protective factor even at a young age, highlighting the need for increased awareness among health officials regarding the benefits of average body weight in children.
Laboratory analysis revealed different abnormal results associated with nutritional rickets. Vitamin D deficiency is a known cause of calcium deficiency, as it decreases calcium absorption from the intestine. Inadequate calcium intake in the diet reduces calcium availability, leading to hypocalcemia. The body responds by producing parathormone, which regulates serum calcium levels by increasing the activity of 1-hydroxylase in the kidney, forming calcitriol from calcidiol. Calcitriol, in turn, enhances calcium absorption from the intestine. However, secondary hyperparathyroidism, caused by increased parathormone levels, leads to bone resorption and further restricts calcium excretion from the kidney, resulting in hypophosphatemia and, ultimately, rickets.44–48 Our study found similar associations between vitamin D deficiency, rickets, and hypophosphatemia, as reported in previous research.16 Similarly, calcium levels varied across studies, with our findings aligning with those in Sudan but differing from studies conducted in Riyadh, Pakistan, and India.16,24,40,41 These inconsistencies indicate the need for further investigations to understand the pathophysiology of nutritional rickets in the region.
The role of breastfeeding in rickets remains debatable, with ethnic differences and other factors influencing the outcomes. Our study observed a low percentage (8.33%) of breastfed children with rickets, consistent with findings from different regions of Saudi Arabia.49,50 While breastfeeding is generally associated with lower vitamin D levels in infants, it is also a protective factor against nutritional rickets due to the presence of other essential nutrients.51,52 However, maternal vitamin D deficiency and a lack of sunlight exposure in breastfeeding mothers can contribute to vitamin D deficiency in their infants.53 Furthermore, a higher percentage of rickets cases in our study had a family history of vitamin D deficiency (89.29%) and malnutrition (76.19%), suggesting a possible genetic predisposition and the influence of environmental factors.53,54 Premature birth and living in cold environments were also identified as potential risk factors for nutritional rickets.44,53 Clinical signs of rickets, such as rickety rosary (enlargement of the costochondral junction) and craniotabes (softening of the skull), were present in a majority of the children in our study (67.87%), similar to findings from other regions.54 Recognizing these clinical signs is crucial for prompt diagnosis and intervention to prevent further complications associated with rickets, such as skeletal deformities and impaired growth.54
Despite being one of the few studies on nutritional rickets in the region, our study has several limitations. Firstly, the sample size was relatively small, limiting the generalizability of the findings. Additionally, the study relied on hospital records, which may not capture all instances of rickets in the population. The retrospective nature of the study introduces inherent biases, and there is a possibility of missed cases. Detailed nutritional data, such as dietary intake and vitamin D supplementation, were not available, which could have provided further insights into the causes of rickets. Furthermore, the study was conducted in Jazan Province, and the findings may not be representative of the entire country or other regions with different demographics and environmental factors. To fully understand the factors contributing to nutritional rickets and develop effective preventive strategies, further research with larger sample sizes and prospective designs is needed.
Conclusions
Rickets is a preventable disease when it is due to a nutritional etiology, and it can be otherwise caused due to various reasons that must be confirmed on a scientific basis. Efforts from government agencies are required to prevent this disease. The most affected children in this study were between 11–18 years old. It was found that the exposure of these children to sunlight was limited, which is one of the key factors causing vitamin D deficiency. In addition, it was noted that the children had low calcium and vitamin D levels. Malnutrition had the highest risk ratio present in children with rickets. More studies are needed to be done so that better and more reliable findings can be established so that proper risk factors can be assessed, and policies can be made to prevent this disease.
Institutional Review Board Statement
The study protocol was approved by the internal review board of the Ethics Committee of the Ministry of Health in the Jazan Region. Approval No: 22055; date: 15 June 2022.
Informed Consent Statement
Waived, due to the nature retrospective study and Patients’ files were relied upon without their names
Data Sharing Statement
Data is available upon request from researchers. Kindly contact the first author privately through e-mail.
Acknowledgments
The authors would like to thank the data collectors, nurses, and pediatricians at King Fahad Central Hospital for their help.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work received no external funds.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Lerch C, Meissner T. Interventions for the prevention of nutritional rickets in term born children. Coch Data Syst Rev. 2007;2007(4):CD006164. doi:10.1002/14651858.CD006164.pub2
2. Welch TR, Bergstrom WH, Tsang RC. Vitamin D-deficient rickets: the reemergence of a once-conquered disease. J Pediat. 2000;137(2):143–145. doi:10.1067/mpd.2000.109008
3. Wagner CL, Greer FR. Prevention of rickets and vitamin D deficiency in infants, children, and adolescents. American academy of pediatrics section on breastfeeding; American academy of pediatrics committee on nutrition. Pediatrics. 2008;122:1142–1152. doi:10.1542/peds.2008-1862
4. David L. Common Vitamin D-Deficiency Rickets. New York, NY, USA: Raven Press; 1991:107–122.
5. Kreiter SR, Schwartz RP, N. H, Kirkman PAC Jr, Calikoglu AS, Davenport ML. Nutritional rickets in African American breast-fed infants. J Pediat. 2000;137(2):153–157. doi:10.1067/mpd.2000.109009
6. DeLucia MC, Mitnick ME, Carpenter TO. Nutri- tional rickets with normal circulating 25-hydroxyvitamin D: a call for reexamining the role of dietary calcium intake in North American infants. J Clin Endocrinol Metab. 2003;88:3539–3545. doi:10.1210/jc.2002-021935
7. Bener A, Alsaied A, Al-Ali M, et al. Impact of lifestyle and dietary habits on hypovitaminosis D in type 1 diabetes mellitus and healthy children from Qatar, a sun-rich country. Ann Nutr Metab. 2009;53(3–4):215–222. doi:10.1159/000184439
8. Goldacre M, Hall N, Yeates DG. Hospitalisation for children with rickets in England: a historical perspective. Lancet. 2014;383(9917):597–598. doi:10.1016/S0140-6736(14)60211-7
9. Ward LM, Gaboury I, Ladhani M, Zlotkin S. Vitamin D–deficiency rickets among children in Canada. CMAJ. 2007;177(2):161–166. doi:10.1503/cmaj.061377
10. Högberg U, Winbo J, Fellman V. Population‐based register study of children born in Sweden from 1997 to 2014 showed an increase in rickets during infancy. Acta Paediatrica. 2019;108(11):2034–2040. doi:10.1111/apa.14835
11. 83642813085 DH (1979): VD metabolism and function; 1979:53. Available from: https://www.springer.com/gp/book/9.
12. Creo AL, Thacher TD, Pettifor JM. Strand MA FPN rickets around the world: an update. PICH. 2017;37(2):84–98.
13. Majid Molla A, Badawi MH, Al-yaish S, Sharma P, El-salam R S, Majid Molla A. Risk factors for nutritional rickets among children in Kuwait. Pediat Internat. 2000;42(3):280–284
14. MGHC. AWRD of bone mineralization. MGHC; 2003:2156–2160.
15. Tariq A, Cheema AN, Qaisar AM, Riaz L, Faryad N, Hussain K. Predisposing factors for nutritional rickets in children presenting in Shaikh Zayed hospital, Lahore. Pakistan J Med Heal Sci. 2022;16(6):62–63. doi:10.53350/pjmhs2216662
16. Al Jurayyan NAM, Mohamed S, Al Issa SDA, Al Jurayyan ANA. Rickets and oestomalacia in Saudi children and adolescents original article rickets and osteomalacia in Saudi children and adolescents attending endocrine clinic. Riyadh. 2015;12(September):56–63.
17. Haffner D, Leifheit-Nestler M, Grund A, Schnabel D. Rickets guidance: part I—diagnostic workup. Pediatr Nephrol. 2022;37(9):2013–2036. doi:10.1007/s00467-021-05328-w
18. Sedrani SH. Are Saudis at risk of developing Vitamin D deficiency? Saudi Med J. 1986;7:427–433.
19. Husby S, Koletzko S, Korponay-Szabó IR, et al. European society for pediatric gastroenterology, hepatology, and nutrition guidelines for the diagnosis of coeliac disease. J of PG and N. 2012;54:136–160.
20. Al-Saleh Y, Al-Daghri NM, Khan N, et al. VD status in S school children based on knowledge. BMC Pediatr. 2015;15(1):1. doi:10.1186/s12887-015-0369-9
21. Almezani AM, Alshlaqy AS, Alsiraa MNN, Alenazy GAG, Al Ghamdi SASK. The prevalence of rickets disorder among children in Saudi Arabia. Egypt J Hosp Med. 2018;73(6):6943–6947. doi:10.21608/ejhm.2018.17207
22. Fida NM. Assessment of nutritional rickets in Western Saudi Arabia. Saudi Med J. 2003;24(4):337–340.
23. Mahmoud AO, Ahmed AY, H-T-AM A. The prevalence of active nutritional rickets in Egyptian infants in Cairo. Egypt Pediatr Assoc Gaz. 2016;64(3):105–110.
24. Jose S, B A. Nutritional rickets among children of Northern Kerala, India. Int J Contemp Pediatr. 2017;5(1):14. doi:10.18203/2349-3291.ijcp20175057
25. Weisberg P, Scanlon KS, Li R, et al. Nutritional rickets among infants in the United States: review of cases reported between 1986 and 2003. Am J Clin Nutr. 2004;80(6):1697–705S. doi:10.1093/ajcn/80.6.1697S
26. Shaw NJ, Pal BR. Vitamin D deficiency in UK Asian families: activating a new concern. Arch Dis Child. 2002;86:147–149. doi:10.1136/adc.86.3.147
27. Beck-Nielsen SS, Brock-Jacobsen B, Gram J, Brixen K, Jensen TK. Incidence and prevalence of nutritional and hereditary rickets in southern Denmark. Eur J Endocrinol. 2009;160(3):491–497. doi:10.1530/EJE-08-0818
28. Abdullah MA, Salhi HS, Bakry LA, et al. Adolescent rickets in Saudi Arabia: a rich and sunny country. J Pediatr Endocrinol Metab. 2002;15(7):1017–1025. doi:10.1515/JPEM.2002.15.7.1017
29. Agarwal A, Gulati D. Early adolescent nutritional rickets. J Orthop Surg. 2009;17(3):340–345. doi:10.1177/230949900901700320
30. Dahifar H, Faraji A, Ghorbani A, Yassobi S. Impact of dietary and lifestyle on vitamin D in healthy student girls aged 11–15 years. J Med Investig. 2006;53:204–208. doi:10.2152/jmi.53.204
31. Chanchlani R, Nemer P, Sinha R, et al. An overview of rickets in children. Kidney Int Reports. 2020;5(7):980–990. doi:10.1016/j.ekir.2020.03.025
32. Diamond M, Friedman BW. Migraine in the emergency department. Migraine Other Headache Disord. 2016;336(june):413–429.
33. Gedamu H, Tafere Y. Assessment of knowledge, attitude, and practice of sunlight exposure of infants among mothers attending in governmental health facilities in farta district, South Gondar Zone, North West Ethiopia, 2018. Int J Reprod Med. 2019;2019:1–7. doi:10.1155/2019/2638190
34. Rhodes LE, Webb AR, Fraser HI, et al. Recommended summer sunlight exposure levels can produce sufficient (≥20 ng mL-1) but not the proposed optimal (≥32 ng mL-1) 25(OH)D levels at UK latitudes. J Invest Dermatol. 2010;130(5):1411–1418. doi:10.1038/jid.2009.417
35. Cicarma E, Porojnicu AC, Lagunova Z, Dahlback A, Juzeniene A, Moan J. Sun and sun beds: inducers of vitamin D and skin cancer. Anticancer Res. 2009;29(9):3495–3500.
36. Binobead MA, Al-Qahtani WH, Al Bader NA, Alsedairy SA, Arzoo S. Prevalence of Vitamin D deficiency and the effect of anthropometric and lifestyle factors on theVitamin D statuses of healthy women residing in Riyadh. Prog Nutr. 2019;21(2):299–308.
37. Al-Othman A, Al-Musharaf S, Al-Daghri NM, et al. Effect of physical activity and sun exposure on vitamin D status of Saudi children and adolescents. BMC Pediatr. 2012;12:12. doi:10.1186/1471-2431-12-12
38. Altaib RM, Yonis KO, Akrim FA, et al. Nutritional rickets among children admitted with wheezy chest at al-bieda medical. Age. 2021;3389:379–384.
39. Bener A, Hoffmann GF. Nutritional Rickets among Children in a Sun Rich Country. Int J Pediatr Endocrinol. 2010;2010:1–7. doi:10.1155/2010/410502
40. Shazia F, Abbas K, Falak Z, et al. Nutritional status assessment of children with nutritional rickets under five years at district headquarter hospital, upper dir- Pakistan. J Nutr Heal Sci. 2017;4(2):1–7.
41. Ahmed Tayrab EM, Abbas M, Tayrab J, Mohamed K, Salih A. Characteristics of rickets in a referral hospital in Khartoum-Sudan. J Pediatr Neonatal Care. 2018;8(5):236–239. doi:10.15406/jpnc.2018.08.00348
42. Thacher TD, Fischer PR, Tebben PJ, et al. Increasing incidence of nutritional rickets: a population-based study in Olmsted County, Minnesota. Mayo Clin Proc. 2013;88(2):176–183. doi:10.1016/j.mayocp.2012.10.018
43. Choi YJ, Lee SM, Shin JE, et al. Risk factors for rickets of prematurity in extremely low birth weight infants. Neonatal Med. 2015;22(4):192. doi:10.5385/nm.2015.22.4.192
44. Sahay M, Sahay R. Rickets-vitamin D deficiency and dependency. Indian J Endocrinol Metab. 2012;16(2):164. doi:10.4103/2230-8210.93732
45. Ryan JW, Anderson PH. Turner AG MHVD activities and metabolic bone disease. CCA. 2013;425:148–152.
46. Thacher TD, Fischer PR, Singh RJ, Roizen J. LMCMIG of 25-hydroxyvitamin D and C an AF of VDDJCEM; 2015.
47. Durmaz E, Zou M, Al-Rijjal RA, Bircan I, Akcurin S. Meyer B SYC and genetic analysis of patients with vitamin D rickets type 1A. CE. 2012;9:1.
48. Aggarwal A, Mehta S, Gupta D, et al. Clinical & immunological erythematosus patients characteristics in systemic lupus Maryam. J Dent Educ. 2012;76(11):1532–1539. doi:10.1002/j.0022-0337.2012.76.11.tb05416.x
49. Flot C, Porquet-Bordes V, Bacchetta J, et al. Demographic Characteristics, risk factors, and presenting features of children with symptomatic nutritional rickets: a French series. Horm Res Paediatr. 2020;93(5):304–312. doi:10.1159/000511419
50. Strand MA, Perry J, Jin M, et al. Diagnosis of rickets and reassessment of prevalence among rural children in northern China. Pediatr Int. 2007;49(2):202–209. doi:10.1111/j.1442-200X.2007.02343.x
51. Al-Sekait MA. “A study of the factors influencing breastfeeding patterns in SA. SMJ. 1988;9:596–601.
52. Saied H, Mohamed A, Suliman A, Al Anazi W. Breastfeeding knowledge, attitude and Barriers among Saudi women in Riyadh. J Nat Sci Res. 2013;3:12.
53. Alisherovna RN, Sobirovich RA, Xaitovich SR, Maxmudovna AM, Tashbekovna IL. Criteria for studying the risk factors for rickets and its effect on the level of 25 (OH) D in blood serum in children. Eur J Mol Clin Med. 2021;8(2):2150–2153.
54. Siddiqui TS, Rai MI. Presentation and predisposing factors of nutritional rickets in children of Hazara Division. J Ayub Med Coll Abbottabad. 2005;17(3):29–32.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.