")
Back to Journals » Journal of Healthcare Leadership » Volume 16
Navigating the Healthcare Conundrum: Leadership Perspective from a Premier Healthcare Organization in Loma Linda’s Blue Zone
Authors Tan LD , Hilliard AA, Peverini RL, Martin RD, Thomas TL, Wright TG, Edwards LC, Lalas AM, Staples-Evans HM, Sharp BJ, Ahn-Kim SL, Hansen KA, Hart RH
Received 13 December 2023
Accepted for publication 13 February 2024
Published 27 February 2024 Volume 2024:16 Pages 83—91
DOI https://doi.org/10.2147/JHL.S452188
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pavani Rangachari
Laren D Tan,1 Anthony A Hilliard,2 Ricardo L Peverini,3 Robert D Martin,4 Tamara L Thomas,5 Trevor G Wright,6 Lyndon C Edwards,6 Angela M Lalas,6 Helen M Staples-Evans,6 Barbara J Sharp,7 Stella L Ahn-Kim,7 Kent A Hansen,6 Richard H Hart8
1Department of Medicine, Pulmonary, Critical Care, Hyperbaric and Sleep Medicine, Loma Linda University School of Medicine, Loma Linda, CA, USA; 2Department of Medicine, Cardiology, Loma Linda University School of Medicine, Loma Linda, CA, USA; 3Department of Pediatrics, Neonatology, Loma Linda University School of Medicine, Loma Linda, CA, USA; 4Department of Anesthesia, Loma Linda University School of Medicine, Loma Linda, CA, USA; 5Department of Emergency Medicine, Loma Linda University School of Medicine, Loma Linda, CA, USA; 6Loma Linda University Health, Loma Linda, CA, USA; 7Loma Linda University School of Medicine, Loma Linda, CA, USA; 8Department of Preventive Medicine, Loma Linda University School of Medicine, Loma Linda, CA, USA
Correspondence: Laren D Tan, Email [email protected]
Abstract: Navigating the healthcare conundrum in the Blue Zone of Loma Linda, California, requires understanding the unique factors that make this region stand out in terms of health and longevity. But more important is understanding the healthcare system sustaining the Blue Zone in Loma Linda, California. In an era marked by soaring healthcare costs and diminishing reimbursement rates, hospitals and physicians face an unprecedented challenge: providing excellent patient care while maintaining financial sustainability. This leadership perspective publication paper delves into the multifaceted struggles encountered by healthcare and hospital leaders, exploring the root causes, implications, and potential solutions for this complex issue. As we examine the evolving healthcare landscape, we aim to shed light on the critical need for innovative approaches to sustain the future of healthcare excellence in one of the five original Blue Zones.
Keywords: blue zone, Loma Linda, healthcare cost, leadership healthcare, longevity, California
Introduction
Blue Zone Intro
The National Geographic fellow and Blue Zones founder, Dan Buettner, is credited for discovering and creating the concept of Blue Zones. His work designated five locations worldwide as Blue Zones: 1. Japan’s Okinawa; 2. Sardinia, Italy’s Ogliastra Region; 3. Nicoya Peninsula, Costa Rica 4. Ikaria,Greece, and 5. Loma Linda (California).1
Blue Zones, as defined by Dan Buettner’s research, are areas or locations with a high percentage of elderly individuals free of conditions including obesity, cancer, diabetes, and heart issues.2 Using four categories, practices and characteristics in the Blue Zones, Buettner and his team found nine commonalities.
These are: 1. move naturally, right outlook about exercising; 2. purpose in life; 3. downshift the stressors in life; 4. 80% rule: eating wisely and stop eating before being full; 5. plant slant; 6. wine at five (except Adventists); 7. right tribe that supports healthy behavior; 8. loved ones first; and 9. belonging to a faith-based community. These elements, which are grouped together as the Power of 9, are arranged in a triangle with the idea of belonging and the three elements—commonalities or practices—forming the base and move at the top.2,3
Of the five identified Blue Zones, Loma Linda is unique because it also has a large Seventh-day Adventist population, where the average lifespan is higher than it is elsewhere.2 In addition to respecting the biblical teachings of the Sabbath, which is a day set aside for God’s people to enjoy, worship, relax and meditate. The outlook to live as positive examples of God’s love and care, including taking care of their health, has resulted in a high proportion of Adventist’s that follow a vegetarian diet.4 While it is not evident if any one specific factor is the result of longevity, a combination of spiritual and holistic health wellness is likely the reason for the increase in life expectancy. It is also just as essential to have preventative medical interventions as it is inevitable that as we age, medical complications will arise and medical care will be sought after. Within Loma Linda, California (CA) resides Loma Linda University and Loma Linda University Medical Center.
Loma Linda University is part of the Seventh-day Adventist higher education system for more than 1400 medical students, residents and fellows. Founded in 1905, the University was designated by the Seventh-day Adventist Church as a center for educating health professionals like Loma Linda University School of Medicine, to ensure that the healing ministry of Jesus Christ continued through Loma Linda University. Loma Linda University Health (LLUH) was formed and is in the heart of the “Blue Zone” in Loma Linda, California. LLUH is a nonprofit religious corporation in Loma Linda, California, in the southern portion of the US (United States) state of California. It is located within the Inland Empire area. LLUH is the umbrella organization for its core and affiliate organizations that include Loma Linda University, Loma Linda University Medical Center, Loma Linda University Medical Center East Campus, Loma Linda University Surgical Hospital, Loma Linda University Behavioral Medical Center, Loma Linda University Children’s Hospital, Loma Linda University Medical Center – Murrieta, and Loma Linda University School of Medicine’s clinical faculty corporation, Loma Linda University Faculty Medical Group.5
The Health system, with its approximate 1000 faculty physicians and 300 advanced practitioners, is integrated within the LLUH system to provide care in a tertiary medical facility, Level 1 regional trauma center for Inyo, Mono, Riverside and San Bernardino counties and delivers care for approximately 1.5 million patients each year. Loma Linda University serves as a fundamental pillar for the region and is essential for maintaining the well-being of “blue zone” citizens and the surrounding communities by addressing both acute and chronic health issues. Regular access to healthcare facilities, preventive services, and medical professionals is paramount in the early detection and treatment of illnesses, helping curb disease progression before they become life-threatening. In essence, access to healthcare is not just a luxury; it’s a necessity that fosters healthier and more productive communities, contributing to overall societal growth and prosperity.
The healthcare industry in the United States is at a critical crossroads. Unsurprisingly, healthcare in the Inland Empire (the region that includes Loma Linda) is also at a crossroads. Of the approximately 9000 Adventists that make up Loma Linda, California’s Blue Zone,6,7 equates to about 35% of Loma Linda being “blue-zoners” and the remaining 65% being “non-blue zoners”. What is also worth noting is that Loma Linda University Medical Center is the largest academic safety-net hospital for the “non-blue zone” counties of San Bernardino, Riverside, Inyo and Mono. Respectively, Loma Linda University Medical Center serves a combined county population of approximately 4.6 million patients. While Loma Linda University Medical Center is present to service the 0.1% “blue-zoners” its mission and purpose is also to serve the remaining 99.9% “non-blue zones”.
To meet the “blue zoners” and “non-blue zoners” healthcare needs, LLUMC has leveraged medical advances and technological innovations to help deliver higher-quality care. Much like many health systems, the escalating costs of healthcare and dwindling reimbursement rates pose significant hurdles to LLU Health and physicians. This paper examines the key challenges associated with these concurrent trends and highlights the need for adaptive strategies to ensure the continued provision of excellent patient care.
Barriers to a Sustainable Healthcare Model
Escalating Healthcare Costs
Pharmaceutical Costs
Over the last two decades, pharmaceutical costs have rapidly increased as a significant health factor. Medication is one of the main cost items and is considered an essential and integral part of health care. In most countries, pharmaceutical costs form a large share of the government’s public health budget. On average, Organization for Economic Cooperation and Development (OECD) countries spend 17% of their healthcare costs on pharmaceutical affairs.8,9 In the United States, retail prescription drug spending was estimated to account for nearly 12% of total personal healthcare services in 2019 (up from about 7% in the 1990s).10 One of the primary drivers of rising healthcare costs is the exorbitant prices of pharmaceuticals. By the end of 2021, total drug expenses were 28.2% higher than pre-pandemic levels. When taken as a share of all non-labor expenses, drug expenses have grown from approximately 8.2% in January 2019, to 9.3% in January 2021, and to 10.6% in January 2022.11 Costly prescription medications strain hospital budgets and create barriers to patient access.
Labor and Administrative Expenses
Prior to the COVID-19 pandemic in 2020, hospital administration and clinical costs grew by about 4% annually between 2016 and 2019. Whereas the median clinical expenses increased by 0.6%, the median administrative expenditures increased by 6.2% between 2019 and 2020. The yearly growth in clinical expenses prior to COVID-19 of 3.7% (95% CI, 3.5 to 4%) was not different in 2020 (0.5%; 95% CI, −0.3 to 1.4%).12 Administrative expenses (ie, costs associated with invoicing and insurance, claims handling, clinical coding and paperwork, and costs unrelated to invoicing and insurance) grew much faster than clinical expenses, resulting in a larger share of hospital financial resources allocated to administrative activities.12 The astronomical fees that contract staffing companies demanded were the main cause of the additional surge in labor costs associated with healthcare for hospitals and health systems. Hospital labor costs per patient were 19.1% higher than pre-pandemic levels at the end of 2021 (see Figure 1), and they reached a peak of 57% in January 2022. Costs were expected to rise during 2022, with predicted non-labor spending up to $49 billion and labor costs increasing by $86 billion. This would result in approximately $135 billion increase above the previous year level.13
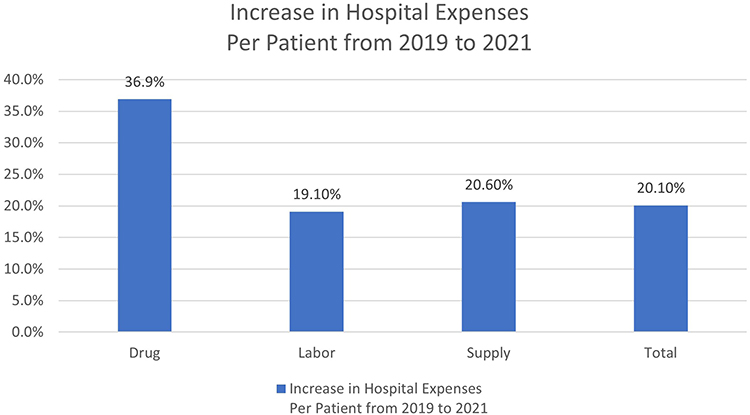 |
Figure 1 Increase in Hospital Expenses Per Patient from 2019 to 2021. Data from KaufmanHall.11 |
The state of California recently added to the increasing labor costs by passing Senate Bill 525 (SB 525) and Senate Bill 616 (SB 616).14,15 SB 525 establishes a $25/hour minimum wage for all California healthcare workers in various health facilities and physician practices with 25 or more physicians. With healthcare reimbursements being essentially flat or decreasing in some instances, identifying areas in healthcare to offset the additional cost is necessary, as this bill will increase healthcare costs by $8 billion annually and the state government alone $4 billion, with half coming from federal funds and another half from California taxpayers through state general funding.16 This also does not consider the millions in cost to private and academic systems in healthcare (see Table 1). SB 616 was also passed in October of 2023, amending California’s paid sick leave law to expand mandatory paid sick leave from three days or twenty-four hours to five days or forty hours.14 The additional two days or sixteen hours will cost approximately $3.3 million for the Loma Linda University Health (LLUH) system. These problems are not unique to LLUH but to all healthcare systems in California and, in some instances, nationally. The ever increasing demand for healthcare services intensifies the need for a skilled workforce, resulting in escalating labor costs and paid sick time leave. Additionally, the complexity of insurance claims and billing necessitates extensive administrative resources, resulting in additional expenses.
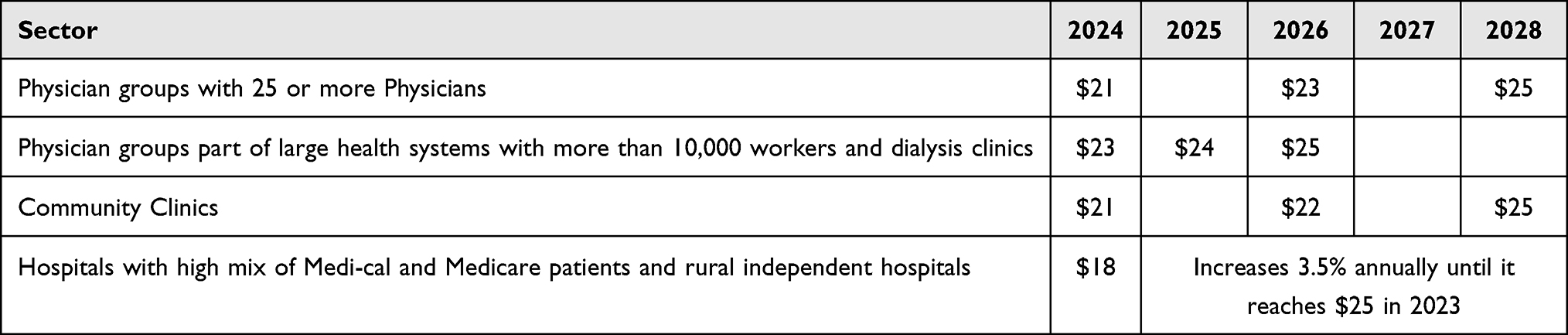 |
Table 1 Senate Bill 52517 |
Technological Advancements
While medical technology advances have improved patient outcomes, the upfront costs of implementing these technologies are substantial, and ongoing maintenance can strain hospital budgets. Technology’s overall effects on healthcare expenses can be far more extensive and offset any potential savings. A capital-embodied technology’s direct costs, which include both the capital cost and the running costs necessary to put it into practice, are frequently overlooked. Because operating and supervisory staff, training, insurance, supplies, and space are required, even the most capital-intensive systems may have higher running expenses than expected. Conversely, a novel medication or apparatus can come with a higher upfront cost but a lower administration cost than its substitutes.18
In addition, new technology may also have an impact on the use of other medical services. These outcomes make up a technology’s “induced” costs and savings. A new diagnostic test may lead to treatments that were not previously thought of,19 or therapies might be skipped all together due to the new technology.20
Declining Reimbursement Rates
Medicare and Medicaid
Despite having the highest per capita healthcare spending of any nation, about 37 million Americans lack health insurance, and another 41 million have insufficient access to care.21 Government programs like Medicare and Medicaid significantly affect healthcare reimbursement. In recent years, these programs have struggled to keep pace with inflation and healthcare cost increases, leading to reduced payments for hospitals and physicians (see Figures 2 and 3). According to the American Hospital Association, Medicare pays hospitals a non-negotiable reimbursement amount that is less than the cost of delivering care. Hospitals saw a −8.5% margin on Medicare services in 2020, according to the Medicare Payment Advisory Commission, and that margin is expected to drop to −9% in 2022. Medicare and Medicaid underpayments to hospitals totaled $100 billion in 2020, up from $76 billion the previous year. The majority of hospital utilization is covered by Medicare and Medicaid, which increases the strain. Healthcare systems are greatly impacted by the ongoing decline in payments, particularly in light of the substantial rise in labor, medication, and supply costs as well as the effects of inflation on hospital viability.13
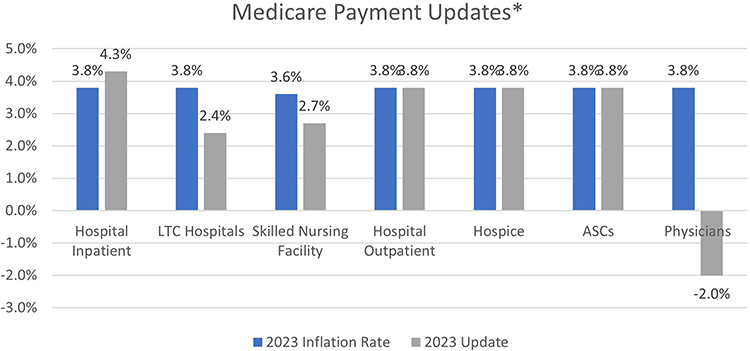 |
Figure 2 Medicare Payment Updates. Reprinted from American Medical Association.22 *Without passage of the Consolidated Appropriations Act of 2023 (PL 117–328), the update for 2023 would have been −4.5%. Abbreviations: LTC, long term care; ASC, ambulatory surgery center. |
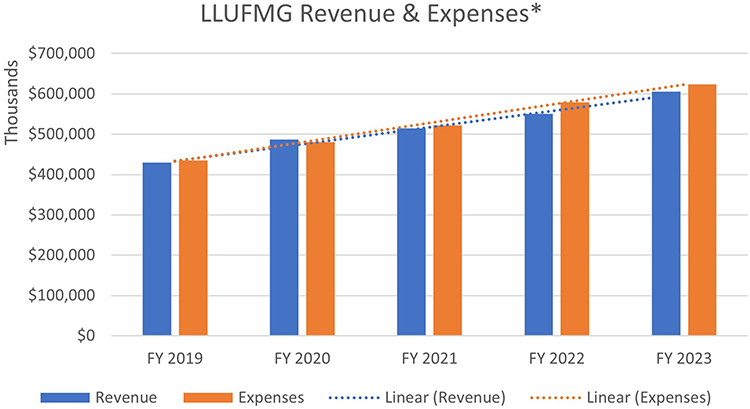 |
Figure 3 Loma Linda University Faculty Medical Group (LLUFMG) – Expenses Exceeding Revenue. *Normalized for volume would slow rate change only. Abbreviation: FY, Fiscal Year. |
Physician compensation under Medicare is not nearly as generous as it formerly was. Medicare physician compensation decreased by 20%, or 1.1% per year, on average, between 2001 and 2021 after accounting for practice cost inflation.23 Market consolidation is encouraged by the growing gap between real payments and the costs of operating a hospital system or medical practice, as well as the administrative and financial strain of being a Medicare participant. This can lead to higher healthcare prices or even system insolvency.22 Medicare payments to doctors having a Centers for Medicare and Medicaid Services (CMS) conversion factor of $32.74 will be lowered by $1.15, or 3.4%, from 2023 to 2024 under the Medicare Physician Fee Schedule rule. Similarly, from 3.8% to 4.6% this year, the Medicare Economic Index (MEI), a government indicator of inflation in medical practice expenses, would rise.24 Substantial reductions in physician reimbursement will only widen the gap between physician practice expenses and reimbursement rates (see Figure 3).
Private Insurance
Private insurers are increasingly shifting the burden of healthcare costs onto patients through higher deductibles and co-pays, leaving healthcare systems and providers with a growing population of underinsured patients.21 Additional steps and denials in authorizations have also led to significant increases in healthcare resources and, in some cases delay in care. In a study performed by Wharam et al, people from lower socioeconomic backgrounds, in the first year after registering in deductible plans, experienced a decline in hospitalization and, in the second year, experienced an increase in hospitalization; but such changes were not found in people from higher socioeconomic backgrounds.25 Delays in healthcare due to increasing required authorizations, high deductibles and co-pays can result in increased mortality and morbidity. The poverty status of San Bernardino County is 13.3%, and Loma Linda approximately 13.6% living below the poverty line, a number higher than the national average of 11.5%.26 A shift in higher deductibles and co-pays can significantly impact healthcare utilization and, due to delayed healthcare visits, an increase in healthcare costs. In addition to higher deductibles and co-pays, health insurance company takeback schemes also cost physicians and hospitals more than $1.6 billion monthly. In contrast, average-size health systems faced 110,000 claim denials due to prior authorization and other factors in 2022.27 Between July and August 2022, payer takebacks averaged 1.8% of monthly debit-account receivables. According to the Crowe report, that is 29% from the 1.4% recorded between January 2021 and June 2022.27,28 Changes by Medicare and Medicaid and challenges faced with private insurances, as mentioned above, also contribute to the widening gap between physician practice expenses and reimbursement rates (see Figure 3).
Implications for Loma Linda University Health and Physicians
Loma Linda, CA, has been found to have an increased concentration of centenarians in addition to clusters of people who have reached old age without disease. The barriers to Loma Linda University Health system as outlined in this paper, as well as financial instability, clinician burnout and access to care constraints (see Figure 4), are leading to an unsustainable healthcare model which could result in the Loma Linda University Health hospitals system being unable to function as a safety-net hospital as well as providing the care necessary for those in the “non-blue zone” and eventual medical care needed for those in the “blue zone”.
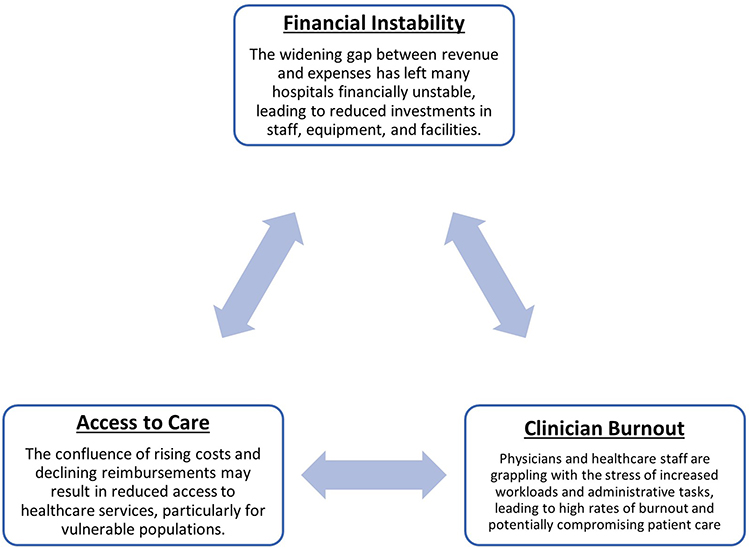 |
Figure 4 Barriers to Loma Linda University Health (LLUH). |
A safety net hospital as defined by the Institute of Medicine by mission or mandate, provides care to a substantial share of vulnerable patients regardless of their ability to pay.29 Since 1905, Loma Linda University has provided care for the most vulnerable without having direct access to taxpayer support, lower costs of capital via municipal bonds, or hospital revenue bonds, which most government-owned and operated facilities have access to. As a result, LLUH hospitals have to be extremely selective on services being provided to the community. In some cases, LLU Health has already closed several clinical services due to financial concerns. Much like many in the nation, our facility is facing significant struggles to remain solvent due to state-mandated healthcare wage increases (ie, SB 525, SB 616), inflationary staffing cost, physician burnout and retention and increased demand for healthcare with a simultaneous decrease in reimbursement. Without a change in reimbursement, early adoption of technology for healthcare, policy reform, deep review of insurers and a focus on living healthy as a community (see Table 2), many healthcare systems will struggle to stay financially solvent and will be unable to provide the services, access and timely care needed, especially for those in the region with limited choices.
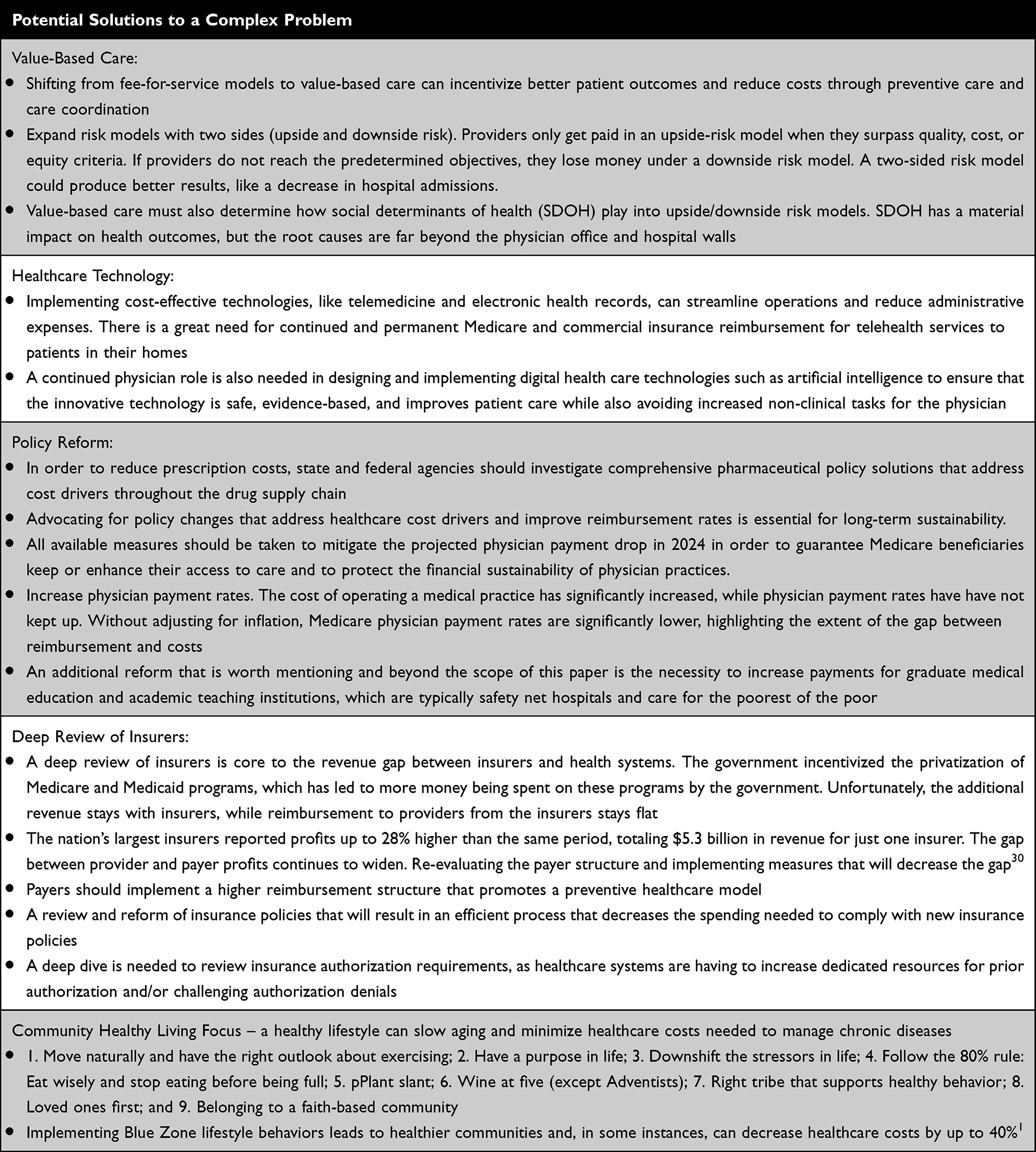 |
Table 2 Potential Solutions to a Complex Problem |
Conclusion
In the face of the relentless surge in healthcare costs and the persistent constraints on reimbursement rates, the challenges that hospitals and physicians confront are undeniable. The road ahead is undeniably arduous, but the importance of this journey cannot be overstated. The commitment to maintaining excellence in patient care is not just a goal but an imperative. Without the necessary changes and adaptations, the healthcare system in the “blue zone” in Loma Linda, California, and indeed across the nation, stands at the precipice of failure. This is a call to action, a plea for change as outlined in Table 2, and an urgent reminder that the health and well-being of communities depend on the collective will and dedication of those within the healthcare system to ensure that excellence in patient care remains an unwavering standard.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Marston HR, Niles-Yokum K, Silva PA. A commentary on blue zones((R)): a critical review of age-friendly environments in the 21st century and beyond. Int J Environ Res Public Health. 2021;18(2):837. doi:10.3390/ijerph18020837
2. Buettner D, Skemp S. Blue zones: lessons from the world’s longest lived. Am J Lifestyle Med. 2016;10(5):318–321. doi:10.1177/1559827616637066
3. Christakis NA, Fowler JH. The spread of obesity in a large social network over 32 years. N Engl J Med. 2007;357(4):370–379. doi:10.1056/NEJMsa066082
4. Liu T, Gatto NM, Chen Z, et al. Vegetarian diets, circulating miRNA expression and healthspan in subjects living in the Blue Zone. Precis Clin Med. 2020;3(4):245–259. doi:10.1093/pcmedi/pbaa037
5. Available from: https://llu.edu/about-llu/about-loma-linda-university-health.
6. Available from: https://www.bluezones.com/explorations/loma-linda-california/.
7. Available from: https://www.census.gov/quickfacts/lomalindacitycalifornia.
8. Available from: https://www.kingsfund.org.uk/sites/default/files/2018-04/Rising-cost-of-medicines.pdf.
9. Brooks E, Geyer R. Can a medical need clause help manage the growing costs of prescription drugs in the EU? Health Econ Policy Law. 2016;11(2):179–192. doi:10.1017/S1744133115000389
10. Available from: https://www.gao.gov/prescription-drug-spending.
11. Available from: https://www.kaufmanhall.com/insights/research-report/national-hospital-flash-report-january-2022.
12. Wang Y, Bai G, Anderson GUS. Hospitals’ administrative expenses increased sharply during COVID-19. J Gen Intern Med. 2023;38(8):1887–1893. doi:10.1007/s11606-023-08158-8
13. Available from: https://www.aha.org/system/files/media/file/2022/04/2022-Hospital-Expenses-Increase-Report-Final-Final.pdf.
14. Available from: https://leginfo.legislature.ca.gov/faces/billNavClient.xhtml?bill_id=202320240SB616.
15. Available from: https://leginfo.legislature.ca.gov/faces/billNavClient.xhtml?bill_id=202320240SB525.
16. Available from: https://calhospital.org/minimum-wage-bill-heads-to-assembly-amendments-fail-to-address-cost-concerns/.
17. Available from: https://www.cmadocs.org/newsroom/news/view/ArticleId/50326/Governor-signs-bill-to-raise-wages-of-health-care-workers-160.
18. Weinstein MC, Read JL, MacKay DN, et al. Cost-effective choice of antimicrobial therapy for serious infections. J Gen Intern Med. 1986;1(6):351–363. doi:10.1007/BF02596417
19. Banta HD, Thacker SB. Assessing the costs and benefits of electronic fetal monitoring. Obstet Gynecol Surv. 1979;34(8):627–642. doi:10.1097/00006254-197908000-00026
20. Gelijns AC, Halm EA. The Changing Economics of Medical Technology. Washington (DC): National Academy Press; 1991.
21. Galvani AP, Parpia AS, Foster EM, Singer BH, Fitzpatrick MC. Improving the prognosis of health care in the USA. Lancet. 2020;395(10223):524–533. doi:10.1016/S0140-6736(19)33019-3
22. Available from: https://www.ama-assn.org/system/files/medicare-provider-updates-chart-2023.pdf.
23. Available from: https://www.ama-assn.org/system/files/medicare-pay-chart-2021.pdf.
24. Available from: https://www.cms.gov/newsroom/fact-sheets/calendar-year-cy-2024-medicare-physician-fee-schedule-final-rule#:~:text=CY%202024%20PFS%20Ratesetting%20and%20Conversion%20Factor&text=CMS%20is%20also%20finalizing%20significant,2023%20conversion%20factor%20of%20%2433.89.
25. Wharam JF, Zhang F, Landon BE, Soumerai SB, Ross-Degnan D. Low-socioeconomic-status enrollees in high-deductible plans reduced high-severity emergency care. Health Aff. 2013;32(8):1398–1406. doi:10.1377/hlthaff.2012.1426
26. Available from: https://www.census.gov/quickfacts/fact/table/lomalindacitycalifornia/INC110221.
27. Available from: https://www.ama-assn.org/practice-management/prior-authorization/health-systems-plagued-payer-takeback-schemes-110000.
28. Available from: https://www.crowe.com/-/media/crowe/llp/widen-media-files-folder/h/hospital-double-whammy-less-cash-in-more-cash-out-chc2305-001b.pdf?rev=178f222e5f7f4ad9b8ed302cf9c6f603&hash=5EC40FBED6F08E2BD52D3A7CF880798C.
29. Ein Lewin M, Altman S. Americas’s Health Care Safety Net: Intact but Endangered. Washington (DC): National Academies Press; 2000.
30. Available from: https://www.beckerspayer.com/payer/the-house-always-wins-health-systems-face-worst-finances-in-decades-as-payers-rake-in-record-profits.html.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.