")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 17
Multiple Eruptive Dermatofibroma: A Case Report
Authors Yao MX, Wang YT, Zhou NH
Received 7 June 2023
Accepted for publication 12 December 2023
Published 19 February 2024 Volume 2024:17 Pages 457—461
DOI https://doi.org/10.2147/CCID.S424707
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Man-Xue Yao,* Yu-Ting Wang,* Nai-Hui Zhou
Department of Dermatology, the First Affiliated Hospital of Soochow University, Suzhou, Jiangsu Province, 215006, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Nai-Hui Zhou, Department of Dermatology, the First Affiliated Hospital of Soochow University, Suzhou, Jiangsu Province, 215006, People’s Republic of China, Email [email protected]
Background: Multiple eruptive dermatofibroma (MEDF) is a rare presentation of dermatofibroma which is frequently associated with underlying diseases such as human immunodeficiency virus infection or systemic lupus erythematosus. It generally presents a characteristic histology with hyperplasia of the epidermis, prominent bundles of collagen and a diffuse proliferation of fibrocytes.
Case Summary: We report a case of MEDF in a 30-year-old man who presented with a large number of dark brownish red maculopapules distributed over the trunk and extremities for more than 10 years. According to the pathology, the patient was diagnosed with MEDF. Infections and autoimmune diseases were ruled out. As he had no clinical symptoms, and presented with lesions widely distributed over the body, we gave no special treatment, but suggested a regular examination.
Conclusion: Patients with MEDF usually have no pain and pruritus. If human immunodeficiency virus infection and systemic lupus erythematosus and other causes are ruled out, and lesions are widely distributed over the body, regular check-up is recommended without specific treatment.
Keywords: multiple eruptive dermatofibroma, histopathology, immune dysfunction, skin neoplasms, case report
Introduction
Dermatofibroma is a common benign tumor of the skin, which may occur naturally or develop due to trauma or mosquito bites. Dermatofibroma is usually single, and more than five is uncommon.1 Multiple dermatofibroma is defined by the presence of more than 15 dermatofibromas all over the body.2 Multiple dermatofibroma is rare and accounts for less than 0.3% of all dermatofibromas.3
There are four types of multiple dermatofibroma: multiple dermatofibromas (MDF), multiple eruptive dermatofibroma (MEDF), multiple cluster dermatofibroma (MCDF), and giant combined dermatofibromas (GCDF).4 MCDF lesions are confined to one anatomical site and are clinically manifested as multiple nodules in a group or linear arrangement, mainly in the lower half of the body. Patients with MEDF usually have pruritus. 66.7% of the MCDF patients were otherwise healthy individuals.4,5 MDF and MEDF are related to immune dysfunction, mostly in patients with systemic lupus erythematosus, HIV infection, autoimmune diseases, occur in a short period of time, can involve any part of the body, trunk and limbs are more common, no clustering, no clinical symptoms. 83% and 91% of MDF and MEDF cases, respectively, have an underlying condition.4 MEDF has been defined as the presence of five to eight dermatofibromas that arise in a four-month period.6,7 A pedunculated lesion larger than 5 cm is considered GCDF.
MEDF is generally presents a characteristic histology with hyperplasia of the epidermis, prominent bundles of collagen and a diffuse proliferation of fibrocytes. Herein, we present a case of MEDF for more than 10 years.
Case Presentation
Chief Complaints
A 30-year-old male patient with dark brownish red maculopapules on the trunk and extremities for more than 10 years was admitted to our hospital in November 2020.
History of Present Illness
More than 10 years ago, the patient developed dark red maculopapules on his trunk without definite inducement. As these skin rashes had no obvious pain or itching, he did not consult a doctor. Subsequently, the number of skin lesions gradually increased, and his limbs were also involved. The patient had more than 50 lesions in the first few months, and then increased to more than 200 lesions, and over the next 10 years, the lesions were relatively stable 258 lesions were found at the time of visit.
History of Past Illness
The patient was in good health prior to the occurrence of these lesions, and no similar diseases were observed in his family.
Physical Examination
Physical examination revealed multiple dark reddish-brown maculopapules on the trunk and limbs, without scaling. The maculopapules varied in size from a grain of rice to a mung bean (Figure 1).
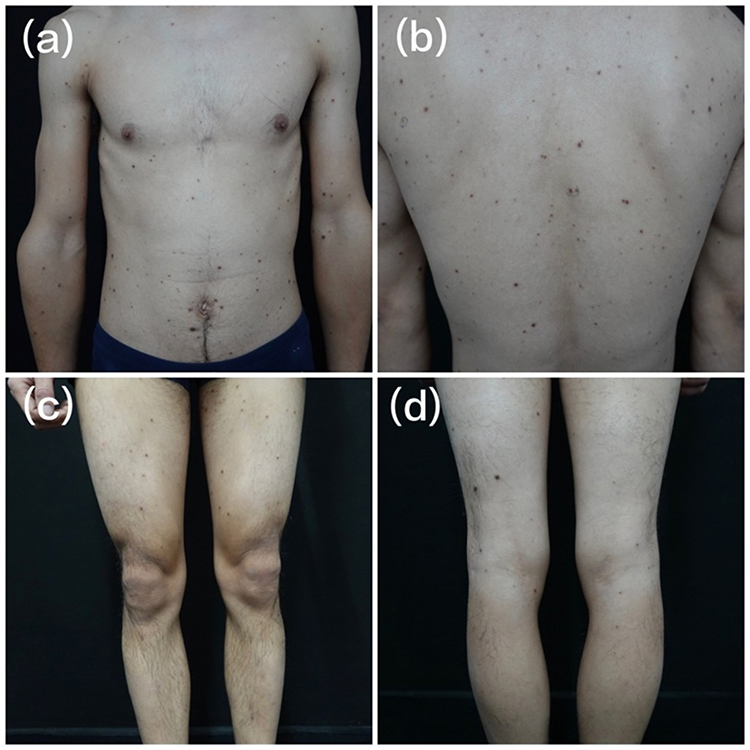 |
Figure 1 Clinical manifestation. Dark brownish red maculopapules were distributed on the trunk and extremities. (a) front of trunk, (b) dorsal side f trunk, (c) extensor side of lower limbs, (d) flexor side of lower limbs. |
Laboratory Examinations
Laboratory tests showed negative results for the whole set of anti-nuclear antibodies, HIV and tumor.
Imaging Examinations
Dermoscopy showed a red homogeneous pattern in the center with a brown pigment network around it (Figure 2).
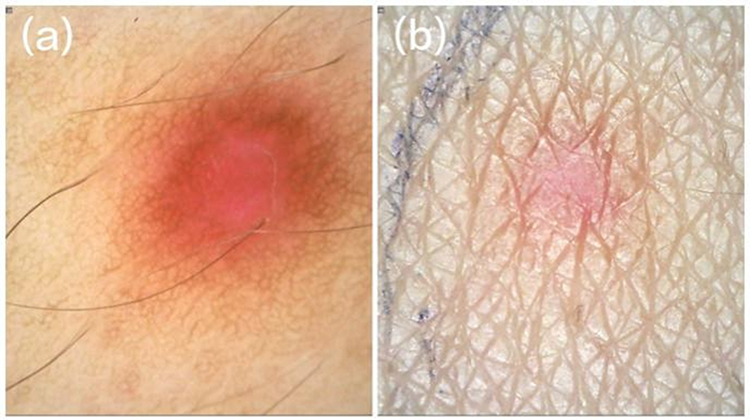 |
Figure 2 Dermoscopic findings. The center of the lesion showed a red homogeneous pattern surrounded with a brown pigment network. (a) polarized light, (b) non-polarized light. |
Further Diagnostic Work-Up
Histopathological examination of the skin lesions showed epidermal hyperplasia and the rete ridges extended downward in the shape of high-heeled shoes with increased pigment in the basal layer. Hyperplasia of collagen fibers and fibroblasts in the middle and lower dermal layers was found, mixed with histiocytes (Figure 3).
 |
Figure 3 Histopathological findings. Epidermal hyperplasia and rete ridges extending downward in the shape of high-heeled shoes were seen with increased pigment in the basal layer. Hyperplasia of collagen fibers and fibroblasts were seen in the middle and lower dermal layer, mixed with histiocytes (H&E (a): 40x, (b): 100x). |
Final Diagnosis
The final diagnosis in this patient was MEDF.
Treatment
We ruled out infections and autoimmune diseases in this patient. As the patient had no clinical symptoms, and there were too many lesions over the body, we did not give him any special treatment, but recommended a regular examination.
Discussion
Multiple cluster dermatofibroma is more common in healthy individuals with normal immune function, but MEDF is usually associated with immune disorders.8 The most frequently reported diseases associated with MEDF are SLE and HIV infection. Other related diseases include dermatomyositis, myasthenia gravis, hematologic malignancies, etc. MEDF has also been reported in patients receiving immunosuppressive therapy.9–11 However, we did not find any potential related diseases in this patient, but long-term follow-up and observation are still required.
MEDF should be differentiated from dermatofibrosarcoma protuberans, leiomyoma and Kaposi’s sarcoma. Histopathology and immunohistochemistry are the keys to correct diagnosis.12 Dermatofibrosarcoma protuberans grows diffusely in the dermis and irregularly invades subcutaneous fat. The tumor cells are large and fusiform, and are arranged into characteristic mat-like structures around collagen fibers and blood vessels. Leiomyomas are located in the dermis with unclear boundaries. Tumor cells are fusiform, and the nuclei are round at both ends. Kaposi’s sarcoma shows proliferation of intradermal blood vessels and vascular endothelial cells, deposition of red blood cells and hemosiderin in the stroma. In immunocompromised patients, MEDF can be clinically confused with other papular lesions such as leukemic infiltration of the skin, bacillary angiomatosis and so on.7
Currently, there is no specific treatment for MEDF. Surgery and laser treatment may be feasible in some cases. Although our patient had a large number of lesions, he did not complain of any discomfort; thus, no special treatment was given.
Conclusion
Patients with MEDF usually have no pain and pruritus. If HIV infection and SLE and other causes are ruled out, and lesions are widely distributed over the body, regular check-up is recommended without specific treatment.
Core Tip: We report a case of multiple eruptive dermatofibroma (MEDF) in a 30-year-old man who presented with a large number of dark brownish red maculopapules distributed over the trunk and extremities for more than 10 years. MEDF is usually associated with immune disorders such as human immunodeficiency virus infection or systemic lupus erythematosus. The diagnosis is based primarily on clinical presentation and pathology. Currently, there is no specific treatment for MEDF. Surgery and laser treatment may be feasible in some cases. As our patient had a large number of lesions and did not complain of any discomfort, we did not give him any treatment.
Patient Consent
Consent for the publication of recognizable patient photographs or other identifiable material was obtained by the authors and included at the time of article submission to the journal stating that all patients gave consent with the understanding that this information may be publicly available.
Informed Consent Statement
Informed written consent was obtained from the patient for publication of this report and any accompanying images.
Funding
Supported by the National Natural Science Foundation of China (81703144).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Berklite L, Ranganathan S, John I, et al. Fibrous histiocytoma/dermatofibroma in children: the same as adults? Hum Pathol. 2020;99:107–115. PMID: 32246988. doi:10.1016/j.humpath.2020.03.012
2. Baraf CS, Shapiro L. Multiple histiocytomas. Report of a case. Arch Dermatol. 1970;101(5):588–590. PMID: 4315412.
3. Massone C, Parodi A, Virno G, et al. Multiple eruptive dermatofibromas in patients with systemic lupus erythematosus treated with prednisone. Int J Dermatol. 2002;41(5):279–281. PMID: 12100703. doi:10.1046/j.1365-4362.2002.01493.x
4. Seifi G, Kalantari Y, Etesami I. Multiple dermatofibromas, associated clinical and histological characteristics: a systematic review. J Dtsch Dermatol Ges. 2022;20(12):1569–1579. PMID: 36464809. doi:10.1111/ddg.14888
5. Higaki-Mori H, Yoshida Y, Hisaoka M, et al. Unusual congenital multiple clustered dermatofibroma: first reported case on the face. Acta Derm Venereol. 2019;99(3):341–342. PMID: 30543382. doi:10.2340/00015555-3109
6. Niiyama S, Katsuoka K, Happle R, et al. Multiple eruptive dermatofibromas: a review of the literature. Acta Derm Venereol. 2002;82(4):241–244. PMID: 12361125. doi:10.1080/000155502320323171
7. Zaccaria E, Rebora A, Rongioletti F. Multiple eruptive dermatofibromas and immunosuppression: report of two cases and review of the literature. Int J Dermatol. 2008;47(7):723–727. PMID: 18613883. doi:10.1111/j.1365-4632.2008.03575.x
8. Gershtenson PC, Krunic AL, Chen HM. Multiple clustered dermatofibroma: case report and review of the literature. J Cutan Pathol. 2010;37(9):e42–e45. PMID: 19614987. doi:10.1111/j.1600-0560.2009.01325.x
9. Llamas-Velasco M, Fraga J, Solano-López GE, et al. Multiple eruptive dermatofibromas related to imatinib treatment. J Eur Acad Dermatol Venereol. 2014;28(7):979–981. PMID: 24321053. doi:10.1111/jdv.12328
10. Panou E, Watchorn R, Bakkour W, et al. Multiple eruptive dermatofibromas in HIV: an immune reconstitution associated disease? J Eur Acad Dermatol Venereol. 2020;34(2):e100–e101. PMID: 31625625. doi:10.1111/jdv.16015
11. Callahan S, Matires K, Shvartsbeyn M, et al. Multiple eruptive dermatofibromas. Dermatol Online J. 2015;21(12):13030. PMID: 26990339.
12. Zaouak A, Chamli A, Khanchel F, et al. Multiple eruptive dermatofibromas. Presse Med. 2019;48(11 Pt 1):1353–1354. PMID: 31727483. doi:10.1016/j.lpm.2019.09.002
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.