")
Back to Journals » Infection and Drug Resistance » Volume 17
Model-Informed Precision Dosing of Imipenem in an Obese Adolescent Patient with Augmented Renal Clearance and History of Schizophrenia
Authors Chen Y, Han Y, Guo F, Yu Z
Received 16 November 2023
Accepted for publication 21 February 2024
Published 27 February 2024 Volume 2024:17 Pages 761—767
DOI https://doi.org/10.2147/IDR.S450294
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Yueliang Chen,1,* Yun Han,2,3,* Feng Guo,1 Zhenwei Yu2,3
1Intensive Care Unit, Sir Run Run Shaw Hospital, School of Medicine, Zhejiang University, Hangzhou, Zhejiang, People’s Republic of China; 2Department of Pharmacy, Sir Run Run Shaw Hospital, School of Medicine, Zhejiang University, Hangzhou, Zhejiang, People’s Republic of China; 3Research Center for Clinical Pharmacy, Zhejiang University, Hangzhou, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Feng Guo; Zhenwei Yu, Email [email protected]; [email protected]
Abstract: Imipenem is a broad-spectrum antibiotic that has been used in treating severe infections and exhibits a time-dependent PK/PD profile. Its dose should be adjusted based on renal function. However, there is little experience with imipenem dosing in obese adolescent patients with augmented renal clearance (ARC) and history of schizophrenia. This case reported successful dosing of imipenem in an obese adolescent patient with ARC based on therapeutic drug monitoring (TDM) and model-informed precision dosing (MIPD). A 15-year-old male adolescent patient with history of schizophrenia was diagnosed with ventilator-associated pneumonia due to carbapenem-susceptible Klebsiella pneumoniae and received imipenem treatment (0.5 g every 8 hours with a 1-hour infusion). However, the exposure of imipenem was suboptimal due to ARC, and there is no available model for MIPD in this patient. Thus, we utilized prediction error to find a population pharmacokinetic model that fit this patient and ran Maximum a posteriori Bayesian estimation and Monte Carlo simulation based on screened models to predict changes in drug concentrations. The dose of imipenem was adjusted to 0.5 g every 6 hours with a 2-hour infusion, and subsequent TDM revealed that dosing adjustment was accurate and successful. Finally, the patient’s status of infection improved. This study will be beneficial to imipenem dosing in similar cases in the future, thereby improving the safety and effectiveness of imipenem or other antibiotics.
Keywords: case report, imipenem, therapeutic drug monitoring, population pharmacokinetic
Introduction
Imipenem is a broad-spectrum and highly effective antibiotic that can treat severe infections with advantages.1,2 Imipenem is also a time-dependent antibiotic, and the pharmacokinetic pharmacodynamic (PK/PD) index that is related to its efficacy is the fraction of time that the free drug concentration remains above the minimum inhibitory concentration (MIC) during a dosing interval (%fT>MIC).3,4 It is mainly eliminated through the kidney, and the dose should be adjusted based on renal clearance. Augmented renal clearance (ARC) is measured as urinary clearance ≥130 mL∙min−1∙1.73 m−2 in adults.5 Some studies have continued to use adult standards for pediatric patients,6,7 while others have defined ARC for pediatric patients as eGFR above media value (≥160 mL∙min−1∙1.73 m−2) through logistic regression analysis.8,9 In a study on the vancomycin in children with ARC, the subtherapeutic cutoff value of eGFR was set to 110.51 mL∙min−1∙1.73 m−2.10 ARC is common in intensive care unit (ICU) patients, while trauma, young age, male sex, admission with central nervous system disease, use of mechanical ventilation, and use of vasopressor were independent risk factors for ARC.11,12 These patients may have insufficient drugs exposure due to excessive elimination. Adolescent critically ill patients with ARC and history of schizophrenia were not clinically typical, and there were few case reports of imipenem dose adjustment in these patients.13 Model-informed precise dosing (MIPD) is proven to be better in PK/PD target attainment than empiric dosing when prescribing antibiotics.14 However, there are also few model data about the PK of imipenem in ARC patients, especially adolescents.15 We herein report on an exceptional adolescent critically ill patient with ARC and obesity who used therapeutic drug monitoring (TDM) and the MIPD method to achieve optimal imipenem exposure.
Patient Information
A 15-year-old male pediatric patient was admitted to the intensive care unit (ICU) because of his severe acute pancreatitis and secondary respiratory failure. Although the patient was 15 years old, he had obesity with a weight of 87 kg and height of 177 cm. He had a previous history of schizophrenia over 3 years and fatty liver and sinusitis over 1 year. He was treated with olanzapine 20 mg daily and clozapine 50 mg daily before admission. Because of persistent pain in the upper abdomen and vomiting, he went to the local clinic for treatment 2 days before admission. However, the patient’s abdominal pain worsened, and he gradually developed chest tightness, shortness of breath, and oliguria. Then, he was transferred to our hospital.
Treatment Description
After admission, the patient had poor mental status, fast heart rate (144 beats/min) and respiratory rate (38/min). His saturation of pulse oxygen was 96% under the support of noninvasive ventilation. He also had acute kidney injury. Then, he was tubed and received mechanical ventilation. He also received fluid therapy and organ support therapy. This patient achieved hemodynamic stability on the second day after admission, and his renal function recovered gradually. However, his intraabdominal pressure was approximately 20–25 mmHg, and the ventilator could not be removed. He then received a series of symptomatic treatments.
Thirty-two days after admission (defined as D1 of this wave of infection), sputum culture and blood culture revealed K. pneumoniae infection (susceptible to imipenem with an MIC of 1 mg/L). Body temperature and laboratory test results are shown in Table 1. His clinical features also indicated pulmonary infection. Then, he was diagnosed with ventilator-associated pneumonia caused by carbapenem-susceptible Klebsiella pneumoniae. Thus, considering the case history of schizophrenia and the central nervous system adverse events of imipenem,16 he received imipenem treatment at a conservative empiric dose of 0.5 g every 8 hours with a 1-hour infusion, which is commonly used in China. His infection improved but was not eradicated in the following days. He received laparoscopic surgery to remove peripancreatic necrotic tissues on D11. After surgery, his biomarkers of infection climbed, and his body temperature was high, but cultures were negative.
 |
Table 1 Body Temperature and Laboratory Test After Receiving Imipenem |
Then, we noticed that his serum creatinine had a decline from 148 μmol/L (first day after admission) to 37 μmol/L (after three weeks), which indicated that he had augmented renal clearance (CCR 175 mL∙min−1∙1.73m−2 by CKD-EPI, due to lack of Cystatin C information, we cannot using the fittest CKiD-U25 calculator17). There was a high probability that imipenem exposure was suboptimal and led to the failure of infection control. The TDM results (sampled on D17) revealed that imipenem concentrations at 4 and 8 hours were 0.98 mg/L and <0.5 mg/L, respectively. The patient had not achieved any recognized PK/PD target for imipenem (fT>MIC 50%, fT>4×MIC 50%).18–20
We tried to apply MIPD to optimize imipenem dosing, but there is no available population pharmacokinetic (PPK) model for this kind of patient. Thus, we searched reported PPK models for imipenem in patients with similar characteristics and compared the suitability of the model by mean absolute prediction error (MAPE) using the existing TDM results.21–25 The calculation method for MAPE is as follows: first, we calculated the difference rPE (relative prediction errors) between the observed values and predicted values of TDM (rPEi = 2*(Cpred-Cobs, i)/(Cpred+Cobs, i), i: individual simulation value). Then, we calculated the absolute values of these rPE (|rPEi|), and finally average the absolute values of these differences to obtain MAPE. A smaller MAPE value represented a higher prediction accuracy of the model, which was more suitable for this patient.26,27 NONMEM (ICON Development Solution, version 7.5.0) software was used in the study. Figure 1 shows the MPAEs of three models, which were developed in children (Dong’s Model22), adult patients with ARC (Fratoni’s Model21), and general adult patients (Bai’s Model23). In Dong’s Model, the PK parameters consisted of V1, V2, Q and CL (V1, central volume of distribution; V2, peripheral volume of distribution; Q, intercompartmental clearance; CL, clearance). The CLCR, current weight and the age were informative covariates for the CL. In Fratoni’s Model, the PK parameters consisted of VC, CL, k12 and k21 (VC, volume of the central compartment; k12, intercompartmental transfer constant; k21, intercom partmental transfer constant; CL, total body clearance). In Bai’s Model, V1, V2, Q and CL were the PK parameters of their model, and CLCR was the informative covariates for the CL. It can be seen from the figure that Bai’s model had a larger MAPE, and the other two models were similar in MAPE. Thus, we simulated based on these two models to optimize imipenem dosing. The proposed regimen for simulation was to shorten the dosing interval or prolong the infusion time to 2 hours. The pharmacokinetic-pharmacodynamic target was set as 50% fT>MIC, and the probable target attainment (PTA) was set as 90%. After 1000 Monte Carlo simulations of each different dosing regimen (Figure 2), only 500 mg every six hours with 2-hour infusion had PTA over 90% in both model simulations.
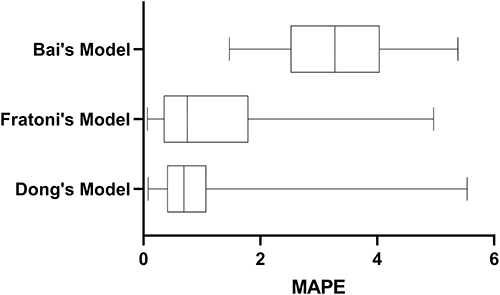 |
Figure 1 MAPE of the different pharmacokinetic models. Dong’s Model: Population pharmacokinetics and dosing optimization of imipenem in children with hematological malignancies. Fratoni’s Model: Population pharmacokinetics and dosing optimization of imipenem in critically ill patients with augmented renal clearance. Bai’s Model: Population pharmacokinetics and dosing optimization of imipenem in critically ill adult patients. Abbreviations:MAPE: mean absolute prediction error. |
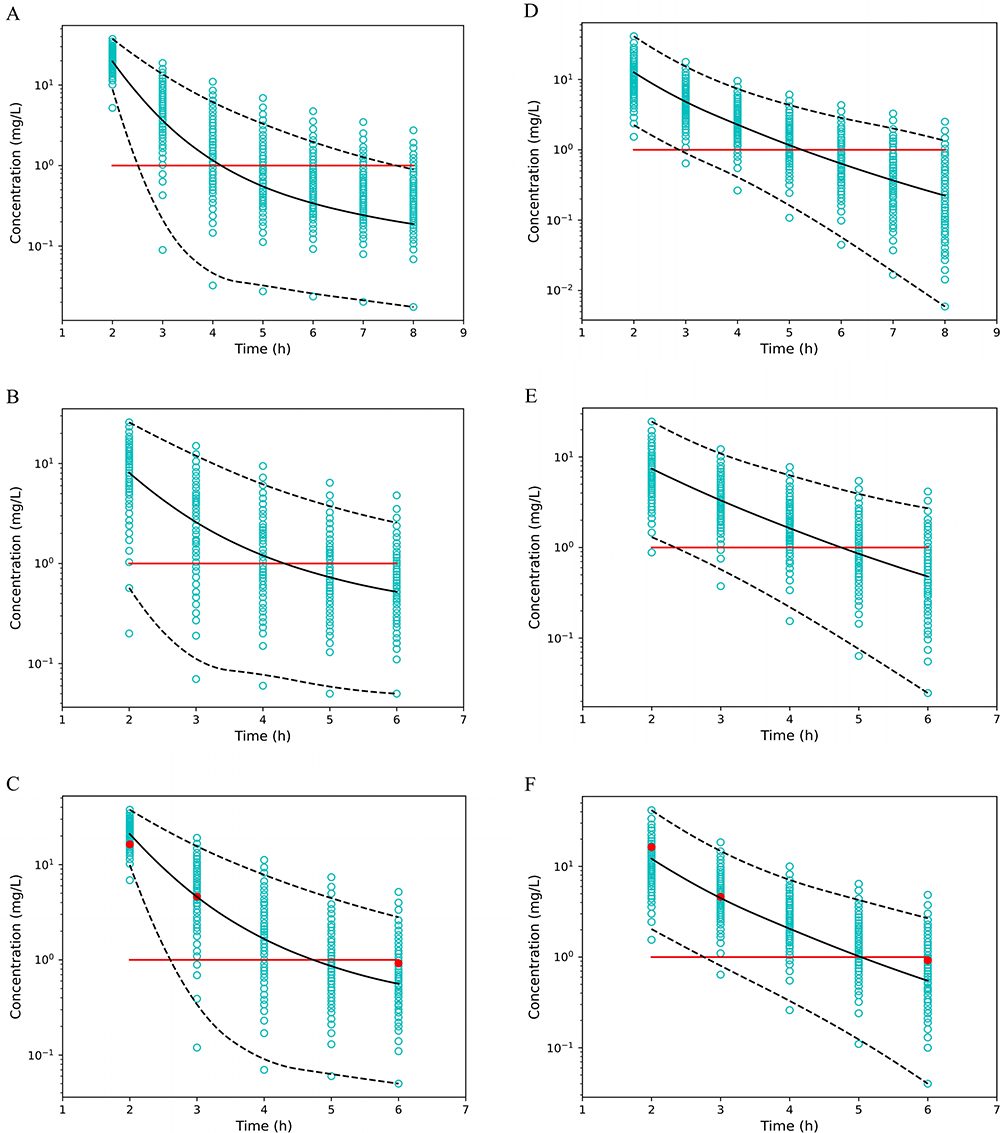 |
Figure 2 1000Monte Carlo simulations of imipenem concentration under different conditions. The black solid line is the mean predicted log concentration after 1000 Monte Carlo simulations. Black dashed lines are the 5% and 95% of the predicted log concentration. The red line is the MIC concentration. Red points are the actual blood concentration of the patient after 6 days. Probability of target attainment (PAT) was calculated using fT>MIC 50% threshold. (A) 500 mg every 8 hours with 2-hour infusion, simulated with Dong’s Model. PTA=61.1%. (B) 500 mg every 6 hours with a 1-hour infusion, simulated with Dong’s model. PTA=73.2%. (C) 500 mg every 6 hours with 2-hour infusion, simulated with Dong’s Model. PTA=90.8%. (D) 500 mg every 8 hours with a 2-hour infusion, simulated with Fratoni’s model. PTA=87.8%. (E) 500 mg every 6 hours with a 1-hour infusion, simulated with Fratoni’s model. PTA=93.8%. (F) 500 mg every 6 hours with a 2-hour infusion, simulated with Fratoni’s model. PTA=98.2%. |
Meanwhile, maximum a posteriori (MAP) Bayesian estimation is a common method of MIPD that integrates population data and a posteriori TDM information of patients to inform an optimal dosing.28 The MAP-Bayesian estimations are shown that 0.5 g every 6 hours with infusion for 2 hours could reach 50% fT>MIC, 50% fT>4×MIC (4.41 ng/mL), while 0.5 g every 8 hours with infusion for 2 hours and 0.5 g every 6 hours with infusion for 1 hours just reached 50% fT>MIC (1.26 ng/mL and 1.87 ng/mL respectively).
Based on the simulation results, the dosing of imipenem was adjusted to 0.5 g every 6 hours with infusion for 2 hours on D18. Moreover, the patient received tigecycline therapy for potential infection with carbapenem-resistant organisms. The consequent TDM (sampled on D24) showed that this method could not only achieve 50%fT>MIC but even 50%fT>4×MIC, and all concentrations were close to our previous prediction (red point in Figure 2C and F, 16.33 ng/mL at 2 h, 4.61 ng/mL at 3 h, 0.92 ng/mL at 6 h).
This indicated that dosing optimization based on MIPD for imipenem in ARC adolescents was successful. After 20 days of treatment, the infection was controlled, and antibiotics were de-escalated to piperacillin-tazobactam (4.5g every 8h with 2h infusion and the treatment duration was 4 days).
Discussion
This study reported a case of successful imipenem dosing using TDM and the MIPD method in an obese adolescent with ARC. The results highlighted the need to apply TDM to discover potential suboptimal exposure to imipenem in ARC patients, and MIPD was a promising tool for precision dosing in patients with special pathophysiological conditions. Moreover, there is a lack of perfect available model for this special patient, thus we made a comparison between different PPK models with similar characteristics to be an alternative.
The occurrence of ARC in ICU patients has gained much more attention in recent years. A study found that the overall prevalence of ARC in patients older than 18 years was as high as 24.6%.12,28 The risk factors for the occurrence of ARC are also including trauma, young age, and male sex which were exist in this patient.11 Another multivariate analysis identified younger age, male sex, lower serum creatinine at admission, admission with central nervous system disease, no medical history, use of mechanical ventilation, and use of vasopressor as onset factors for ARC.12 This patient had several risk factors including younger age, male sex, vasopressor use and use of mechanically assisted ventilation. For ARC patients exposed to β-lactam antibiotics, the drug concentration is easily lower than the therapeutic target.29 A retrospective cohort study showed that suboptimal concentrations of imipenem lead to treatment failure.30 Therefore, caution should be taken for these patients to avoid suboptimal drug exposure. This patient also had obesity, but obesity was a factor that had little impact on β-lactam PK and was not taken into consideration when adjusting dose.31 TDM is an essential tool to verify whether the plasma drug concentration is appropriate. The initial TDM result indicated that the dose for this patient was inadequate and justified the previous concerns.
The traditional dosing of imipenem for adults with normal renal function was 0.5 g every 6 hours. When dosing imipenem for this patient, a relatively low dose was applied due to the concern of young age and possible adverse events, which was proven to be inappropriate by TDM. MIPD uses computer modeling and simulation to predict drug dose regimens according to the personal characteristics of patients, which can produce better effects than traditional dosing.25,32,33 However, it was difficult to imply MIPD in this patient. A major obstacle is that there are also few PPK models of imipenem in ARC patients, especially adolescents. We searched available models based on external validation using MAPE as an index and finally found that Dong’s model and Bai’s model might be suitable. In this model, the age range of pediatric patients was 2–12 years old, and the average weight was only 19 kg, but the average CLCR of these pediatric patients reached 223 mL/min.22 In Bai’s two-compartment model including ARC adults, the average weight of the included patients was 89 kg, and the average CLCR was 193 mL/min, which was close to this case except for the age range.23 Although the age ranges of these two models do not cover this case and the patient populations are different, the two models both included patients with high CLCR levels, and the prediction efficacies were satisfactory. For special patients with no available PPK model, multiple models for patients with similar characteristics could be screened for comprehensive consideration and used for MIPD.
The PK/PD target of imipenem is generally set as 50% fT>MIC, 100% fT>MIC, 50% fT>4×MIC, or even 100% fT>4×MIC in severe infection.18–20 Considering the schizophrenia history of this patient and the central nervous system adverse effect of imipenem, we set the PK/PD target to 50% fT>MIC. Based on the simulation result of simulation, just prolonging the infusion time only (0.5 g every 8 hours with infusion for 2 hours) is not sufficient to achieve satisfactory PTA in these patients. Yoshizawa et al found that shorter dosing intervals (keep the daily dose the same) could lead to greater PK-PD breakpoints and a reduction in excessive maximum plasma concentrations under different dosing methods, which is a better way to optimize the dosing regimen and is similar to our simulation results.34 The repeated TDM showed that the actual imipenem concentrations were close to median estimation and proved the accuracy of the simulation. Compared with the traditional monitoring of drug concentration, MIPD is a more reliable method of dosing. In general, the effectiveness and safety of imipenem for the treatment of adolescent patients with abnormal renal function can be guaranteed by modeling the dose adjustment.
The study also had some limitations. It was not timely to adjust the dose when laboratory tests indicated that the patients had ARC. The association between PK/PD target attainment and clinical efficacy was not strong enough, and further studies involving more patients should be performed. Those used models also lack validation for this type of patients. In the future, a PPK model of imipenem covering these patients is needed.
Conclusion
Here, we report an adolescent case with obesity and ARC in which TDM and MIPD were applied to achieve adequate dosing of imipenem. This result indicated that caution should be taken to avoid suboptimal exposure to imipenem in ARC patients. Dong’s model or Bai’s model could fit the pharmacokinetics of this patient by a prediction error test, which highlighted the possibility to use models for similar patients when no model is available. Then, optimal dosing was achieved using an integrated TDM and MIPD method in this patient. TDM and MIPD are useful tools that propose suitable dosing for patients with special physico-pathological conditions and improve efficacy.
Data Sharing Statement
All data are within the manuscript.
Ethic Approval and Informed Consent
This study was approved by Ethic committee of Sir Run Run Shaw Hospital, School of Medicine, Zhejiang University (reference number KEYAN20210122-32). Written informed consent for publication was obtained from patient’s guardian.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Titov I, Wunderink RG, Roquilly A, et al. A randomized, double-blind, multicenter trial comparing efficacy and safety of imipenem/cilastatin/relebactam versus piperacillin/tazobactam in adults with hospital-acquired or ventilator-associated bacterial pneumonia (RESTORE-IMI 2 Study). Clin Infect Dis. 2021;73(11):e4539–e4548. doi:10.1093/cid/ciaa803
2. Tamma PD, Aitken SL, Bonomo RA, Mathers AJ, van Duin D, Clancy CJ. Infectious diseases society of America 2022 guidance on the treatment of Extended-Spectrum beta-lactamase Producing Enterobacterales (ESBL-E), Carbapenem-Resistant Enterobacterales (CRE), and Pseudomonas aeruginosa with Difficult-to-Treat Resistance (DTR-P. aeruginosa). Clin Infect Dis. 2022;75(2):187–212. doi:10.1093/cid/ciac268
3. Buckley MM, Brogden RN, Barradell LB, Goa KL. Imipenem/cilastatin. A reappraisal of its antibacterial activity, pharmacokinetic properties and therapeutic efficacy. Drugs. 1992;44(3):408–444. doi:10.2165/00003495-199244030-00008
4. Li S, Xie F. Population pharmacokinetics and simulations of imipenem in critically ill patients undergoing continuous renal replacement therapy. Int J Antimicrob Agents. 2019;53(1):98–105. doi:10.1016/j.ijantimicag.2018.10.006
5. Van Der Heggen T, Dhont E, Peperstraete H, et al. Augmented renal clearance: a common condition in critically ill children. Pediatr Nephrol. 2019;34(6):1099–1106. doi:10.1007/s00467-019-04205-x
6. Avedissian SN, Bradley E, Zhang D, et al. Augmented renal clearance using population-based pharmacokinetic modeling in critically ill pediatric patients. Pediatr Crit Care Med. 2017;18(9):e388–e394. doi:10.1097/PCC.0000000000001228
7. Beranger A, Oualha M, Urien S, et al. Population pharmacokinetic model to optimize cefotaxime dosing regimen in critically ill children. Clin Pharmacokinet. 2018;57(7):867–875. doi:10.1007/s40262-017-0602-9
8. Hirai K, Ihara S, Kinae A, et al. Augmented renal clearance in pediatric patients with febrile neutropenia associated with vancomycin clearance. Ther Drug Monit. 2016;38(3):393–397. doi:10.1097/FTD.0000000000000270
9. Avedissian SN, Skochko SM, Le J, et al. Use of simulation strategies to predict subtherapeutic meropenem exposure caused by augmented renal clearance in critically ill pediatric patients with sepsis. J Pediatr Pharmacol Ther. 2020;25(5):413–422. doi:10.5863/1551-6776-25.5.413
10. Lee B, Kim J, Park JD, Kang HM, Cho YS, Kim KS. Predicting augmented renal clearance using estimated glomerular filtration rate in critically-ill children. Clin Nephrol. 2017;88(9):148–155. doi:10.5414/CN109216
11. Baptista JP, Martins PJ, Marques M, Pimentel JM. Prevalence and risk factors for augmented renal clearance in a population of critically ill patients. J Intensive Care Med. 2020;35(10):1044–1052. doi:10.1177/0885066618809688
12. Mikami R, Hayakawa M, Imai S, Sugawara M, Takekuma Y. Onset timing and duration of augmented renal clearance in a mixed intensive care unit. J Intensive Care. 2023;11(1):13. doi:10.1186/s40560-023-00660-9
13. Egea A, Dupuis C, de Montmollin E, et al. Augmented renal clearance in the ICU: estimation, incidence, risk factors and consequences-a retrospective observational study. Ann Intensive Care. 2022;12(1):88. doi:10.1186/s13613-022-01058-w
14. Perez-Blanco JS, Lanao JM. Model-Informed Precision Dosing (MIPD). Pharmaceutics. 2022;14(12):2731. doi:10.3390/pharmaceutics14122731
15. Mahmoud SH, Shen C. Augmented renal clearance in critical illness: an important consideration in drug dosing. Pharmaceutics. 2017;9(3):36. doi:10.3390/pharmaceutics9030036
16. Sutter R, Ruegg S, Tschudin-Sutter S. Seizures as adverse events of antibiotic drugs: a systematic review. Neurology. 2015;85(15):1332–1341. doi:10.1212/WNL.0000000000002023
17. Schwartz GJ, Munoz A, Schneider MF, et al. New equations to estimate GFR in children with CKD. J Am Soc Nephrol. 2009;20(3):629–637. doi:10.1681/ASN.2008030287
18. Craig WA. State-of-the-art clinical article: pharmacokinetic/pharmacodynamic parameters: rationale for antibacterial dosing of mice and men. Clin Infect Dis. 1998;26(1):1–10, 11–12. doi:10.1086/516284
19. Huang Y, Xu K, Zhan Y, et al. Comparable effect of two-step versus extended infusions on the pharmacokinetics of imipenem in patients with sepsis and septic shock. Adv Ther. 2020;37(5):2246–2255. doi:10.1007/s12325-020-01339-5
20. Dinh TD, Nguyen HN, Le BH, Nguyen T, Nguyen H. Population-based pharmacokinetics and dose optimization of imipenem in Vietnamese critically-ill patients. Infect Drug Resist. 2022;15:4575–4583. doi:10.2147/IDR.S373348
21. Fratoni AJ, Mah JW, Nicolau DP, Kuti JL. Imipenem/cilastatin/relebactam pharmacokinetics in critically ill patients with augmented renal clearance. J Antimicrob Chemother. 2022;77(11):2992–2999. doi:10.1093/jac/dkac261
22. Dong L, Zhai XY, Yang YL, et al. Population pharmacokinetics and dosing optimization of imipenem in children with hematological malignancies. Antimicrob Agents Chemother. 2019;63(6):e6–e19. doi:10.1128/AAC.00006-19
23. Bai J, Wen A, Li Z, Li X, Duan M. Population pharmacokinetics and dosing optimisation of imipenem in critically ill patients. Eur J Hosp Pharm. 2023;ejhpharm-2022–003403. doi:10.1136/ejhpharm-2022-003403
24. Jaruratanasirikul S, Boonpeng A, Nawakitrangsan M, Samaeng M. NONMEM population pharmacokinetics and Monte Carlo dosing simulations of imipenem in critically ill patients with life-threatening severe infections during support with or without extracorporeal membrane oxygenation in an intensive care unit. Pharmacotherapy. 2021;41(7):572–597. doi:10.1002/phar.2597
25. Marquet P, Destere A, Monchaud C, et al. Clinical pharmacokinetics and bayesian estimators for the individual dose adjustment of a generic formulation of tacrolimus in adult kidney transplant recipients. Clin Pharmacokinet. 2021;60(5):611–622. doi:10.1007/s40262-020-00959-y
26. Greppmair S, Brinkmann A, Roehr A, et al. Towards model-informed precision dosing of piperacillin: multicenter systematic external evaluation of pharmacokinetic models in critically ill adults with a focus on Bayesian forecasting. Intensive Care Med. 2023;49(8):966–976. doi:10.1007/s00134-023-07154-0
27. Cheng Y, Wang CY, Li ZR, Pan Y, Liu MB, Jiao Z. Can population pharmacokinetics of antibiotics be extrapolated? Implications of external evaluations. Clin Pharmacokinet. 2021;60(1):53–68. doi:10.1007/s40262-020-00937-4
28. Donagher J, Martin JH, Barras MA. Individualised medicine: why we need Bayesian dosing. Intern Med J. 2017;47(5):593–600. doi:10.1111/imj.13412
29. Udy AA, De Waele JJ, Lipman J. Augmented renal clearance and therapeutic monitoring of beta-lactams. Int J Antimicrob Agents. 2015;45(4):331–333. doi:10.1016/j.ijantimicag.2014.12.020
30. Bricheux A, Lenggenhager L, Hughes S, Karmime A, Lescuyer P, Huttner A. Therapeutic drug monitoring of imipenem and the incidence of toxicity and failure in hospitalized patients: a retrospective cohort study. Clin Microbiol Infect. 2019;25(3):381–383. doi:10.1016/j.cmi.2018.11.020
31. Bakdach D, Elajez R, Bakdach AR, Awaisu A, De Pascale G, Ait HA. Pharmacokinetics, pharmacodynamics, and dosing considerations of novel beta-lactams and beta-lactam/beta-lactamase inhibitors in critically ill adult patients: focus on obesity, augmented renal clearance, renal replacement therapies, and extracorporeal membrane oxygenation. J Clin Med. 2022;11(23):6898. doi:10.3390/jcm11236898
32. Polasek TM, Rayner CR, Peck RW, Rowland A, Kimko H, Rostami-Hodjegan A. Toward dynamic prescribing information: codevelopment of companion model-informed precision dosing tools in drug development. Clin Pharmacol Drug Dev. 2019;8(4):418–425. doi:10.1002/cpdd.638
33. Darwich AS, Polasek TM, Aronson JK, et al. Model-informed precision dosing: background, requirements, validation, implementation, and forward trajectory of individualizing drug therapy. Annu Rev Pharmacol Toxicol. 2021;61:225–245. doi:10.1146/annurev-pharmtox-033020-113257
34. Yoshizawa K, Ikawa K, Ikeda K, Kumon H, Ohge H, Morikawa N. Optimisation of imipenem regimens in patients with impaired renal function by pharmacokinetic-pharmacodynamic target attainment analysis of plasma and urinary concentration data. Int J Antimicrob Agents. 2012;40(5):427–433. doi:10.1016/j.ijantimicag.2012.06.011
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.