")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 20
Minimally Invasive Treatment of Chyle Leak After Thyroidectomy and Cervical Lymph Node Dissection in Patients with Thyroid Carcinoma: Results of a Study Involving 36 Patients
Authors Cuong NN , Hoan L , Tra My TT , Luu DT, Tuan Linh L, Canh PH, Tinh TQ, Khanh Chi TN, Trung NQ, Hoa TQ
Received 9 November 2023
Accepted for publication 1 February 2024
Published 9 February 2024 Volume 2024:20 Pages 75—82
DOI https://doi.org/10.2147/TCRM.S446113
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Deyun Wang
Nguyen Ngoc Cuong,1,* Le Hoan,2,* Thieu Thi Tra My,3 Doan Tien Luu,1 Le Tuan Linh,1 Pham Hong Canh,1 Trieu Quoc Tinh,1 Tran Nguyen Khanh Chi,1 Nguyen Quang Trung,1 Tran Quoc Hoa4
1Diagnostic Imaging and Interventional Center, Hanoi Medical University Hospital, Ha Noi, Viet Nam; 2Respiratory Department, Hanoi Medical University Hospital, Ha Noi, Viet Nam; 3Diagnostic Imaging and Nuclear Medicine Department, Vinmec Times City International Hospital, Ha Noi, Viet Nam; 4Urology Surgery department, Hanoi Medical university, Ha Noi, Viet Nam
*These authors contributed equally to this work
Correspondence: Nguyen Ngoc Cuong, Diagnostic Imaging and Interventional Center, Hanoi Medical University Hospital, No. 1, Ton That Tung, Dong Da, Ha Noi, Viet Nam, Email [email protected]
Objective: Chyle leak (CL) after head and neck surgery is a rare but well-known complication. In patients with high-output leakage, the treatment can be complicated. This study aims to report on a recent innovation in lymphatic intervention for treating such patients.
Materials and Methods: A retrospective review of 36 patients with chyle leak after neck surgery for thyroid cancer was conducted to assess the efficacy of percutaneous lymphatic embolization and thoracic duct (TD) disruption.
Results: Antegrade catheterization of the thoracic duct was achieved in 31 of 36 patients (86.1%). Therefore, embolization of the thoracic duct and thoracic duct branches was performed in 26 and 5 patients, respectively. In 5 cases of unsuccessful antegrade catheterization into the thoracic duct, transcervical access embolization was performed in 2 patients, and TD disruption (TDD) was performed in 3 patients. The pooled overall technical success rate of lymphatic embolization was 33/36 patients (91.7%). One patient who underwent thoracic duct embolization (TDE) with technical success (1/33 patients) but clinical failure had additional treatment directly sclerosing the TD under computed tomography scan. Cervical fluid collection sclerotherapy was done in 7 patients as an additional treatment. Resolution of the chyle leak after procedures was observed in all patients (100%). The mean time to resolution was 3 days (1– 7 days). There was no complication intra and after procedures.
Conclusion: TDE, selective TD branches embolization and TDD are safe and effective minimally invasive treatments for CL post-surgery for thyroid carcinoma. Sclerosing cervical fluid collection contributes to clinical success.
Keywords: thyroid cancer, thyroidectomy, chyle leak, thoracic duct embolization, thoracic duct disruption, sclerotherapy
Introduction
Chyle leak is a rare but serious complication of thyroidectomy. It is reported that the incidence is 0.5–1.4% of thyroidectomies and the risk increases when thyroidectomy is associated with neck dissection, up to 8.3%.1–3 Chyle leak may be identified intraoperatively, postoperatively immediately or several days after surgery when enteral feeding is started.4 Prolonged high-volume loss of chyle leads to nutritional failure and immunosuppression, which may even be life-threatening. The output volumes and color of the drainage depend on diet and injury site of the thoracic duct or its branches.
Currently, there are no guidelines for management of chyle leak post-thyroidectomy. The treatment options for post-thyroidectomy chyle leak depend on drain output and patient comorbidities. Management usually starts with conservative measures. Conservative treatments such as nutritional management, pressure dressings, negative pressure suction dressing, somatostatin and octreotide may be effective in patients with low output.4 Patients who had persistent high output or failure of conservative measures required other management approaches such as surgery, thoracic duct embolization, or sclerotherapy.5,6 Lymphatic embolization has been reported as an effective method of managing patients with chylous ascites and chylothorax.7,8 There are some sporadic reports about TDE in management of CL post-thyroidectomy when conservative management is ineffective.9,10 The purpose of this study was to evaluate the technical success and clinical outcomes of minimal invasive intervention in management of CL following cervical lymph node dissection in thyroid carcinoma patients.
Materials and Methods
Patient Characteristics
The retrospective study included 36 patients with chyle leak after thyroidectomy and cervical lymph node dissection in patients with thyroid carcinoma. This was a review of all patients who underwent TDE or TDD for the management of CL at Hanoi Medical University Hospital from June 2019 to July 2023. All subjects had confirmed CL based on drain fluid triglyceride levels greater than 110mg/dL. Conservative therapy has failed to stop chylous leakage in these patients, which included a low-fat diet or total parenteral nutrition and octreotide, and reoperation. Our retrospective study was in accordance with the ethical guidelines of the Declaration of Helsinki. This retrospective study was approved by the institutional review board of the Department of Science and Technology of Hanoi and Hanoi Medical University Hospital (Ref: 139/QĐ-SKHCN dated 24 February 2023) and all patients provided written informed consent.
Data was obtained from patient records including age, sex, surgical procedure, clinical symptoms, volume of drainage output (high-output ≥500 mL/day, low-output <500 mL/day), lymphangiography findings, variant anatomy of thoracic duct, TDE/TDD technical approach, material used to perform the procedure, subsequent interventions, complications, and hospital stay. The amount and duration of chyle drainage output volume per 24 hours before and after the procedure were recorded.
Techniques
Thoracic duct embolization (TDE) and TDD were used.
Transabdominal Antegrade Access
Ultrasound of the bilateral inguinal lymph node was performed to identify lymph nodes. Then, a needle accessed the inguinal node under ultrasound guidance. A total of 10 mL oiled contrast agent was slowly injected into the bilateral inguinal lymph node under fluoroscopic guidance. After the cisterna chyli and the thoracic duct became visible, a 21-gauge Chiba accessed the cisterna chyli via the transabdominal approach. A guidewire was advanced through the needle into the cisterna chyli. Then, a microcatheter was advanced over guide wire into the TD. Contrast was injected through the microcatheter to confirm the site of leakage and evaluate the anatomy of the thoracic duct. TDE was then performed using different embolization materials.
Transcervical Retrograde Access
Transcervical access was performed after a failed antegrade access attempt. A 21-gauge Chiba was directly punctured to the distal of the TD near its insertion at the venous angle under fluoroscopic guidance. Then, a microcatheter was advanced over a guide wire into the TD. Lymphatic embolization was then performed.
Thoracic Duct Disruption (TDD)
TDD was performed as described by Cope et al.11 In patients whose thoracic duct cannulation was unsuccessful, TDD was performed by puncturing the TD, the tissue next to the TD multiple times with a fine needle, and injection of a mixture of Histoacryl and Lipiodol at a 1:3 ratio or saline in the space surrounding the TD under fluoroscopy. This may reduce or interrupt the lymphatic flow by leaking the sclerosing agents into the TD via scratching or compression of the thoracic duct, allowing the leak to heal spontaneously.
Outcome
The technical success of lymphatic embolization was defined as cannulation of the TD via transabdominal antegrade or cervical retrograde access and delivery of embolic material, if indicated, to treat a chyle leak. The clinical success of the procedure was defined as the drain output being resolved within 1 week after procedures.
Statistical Analyses
Demographic and operative data, location of the chyle leaks, drain output data, management approach, embolization materials, technical success (the ability to access the TD and subsequent embolization of the TD), and clinical success (resolution of the presenting chyle leak) were retrospectively collected. These data were analyzed using standard statistical techniques, including medians and ranges for continuous data and counts and percentages for categorical data. Follow-up data were obtained until patients’ discharge and at re-examination one month later.
Results
The study included 36 patients (30 females and 6 males), with a mean age of 49.8 years (range: 21 to 77 years). Of the total 36 patients, 31 had experienced a thyroidectomy with cervical node dissection and 5 patients had undergone only cervical node dissection, with no history of thyroidectomy. Most patients (29) presented with creamy or milky drain output, 7 patients presented with neck palpable fluid collection, and 3 patients had dyspnea. Most patients developed a leak on the left side (34 patients, 94.4%) and 2 patients had left cervical and thoracic leaks. All patients were switched to a fasting or low-fat diet. Four patients experienced repeat surgery for ligated or stitched thoracic duct; one patient was reoperated on twice. Patient demographics and clinical presentations are summarized in Table 1.
 |
Table 1 Characteristics of Patients with Chyle Leak |
The maximum drain volumes ranged from 100 to 1500 mL per 24 hours (mean 342 ± 338 mL), and the duration of leakage prior to intervention ranged from 7 to 52 days (mean 18.5 ± 11 days). The duration of leakage after intervention ranged from 1 to 7 days (mean 3 ± 1.7 days). After the procedure, the output drainage decreased (mean 20 ± 19 mL; range 10–75 mL). The characteristics of chyle leak are summarized in Table 2.
 |
Table 2 Characteristics of Chyle Leak |
On lymphangiography, most patients had an injury of the terminal thoracic duct (27 patients, 75%) and 9 patients had CL due to injury of a thoracic duct branch. Six patients had an anatomical variance: the cisterna chyli was not visualized in 3 patients, 2 patients had a plexiform thoracic duct in the mediastinum, and 1 patient had a double thoracic duct with bilateral terminations to the left and right subclavian veins.
Catheterization of the TD was technically successful in 31 patients (31/36). Transabdominal embolization was performed in these patients: 26 underwent thoracic duct embolization and 5 experienced thoracic duct branch embolization. The reasons for failed TD access were small or absent cisterna chyli. Five patients experienced failed TDE: two of them underwent transcervical TD access (1 patient with TD branch embolization and 1 patient with TDE) and 3 others had TDD. For patients with neck fluid collection, an additional sclerotherapy treatment for fluid collection with absolute ethanol was performed (in total, 7 patients: 6 with TDE and 1 with TDD). The materials used in the embolization procedures were n-BCA glue in 14 patients, and coils combined with n-BCA glue in 19 patients. The characteristics of the procedures are summarized in Table 3.
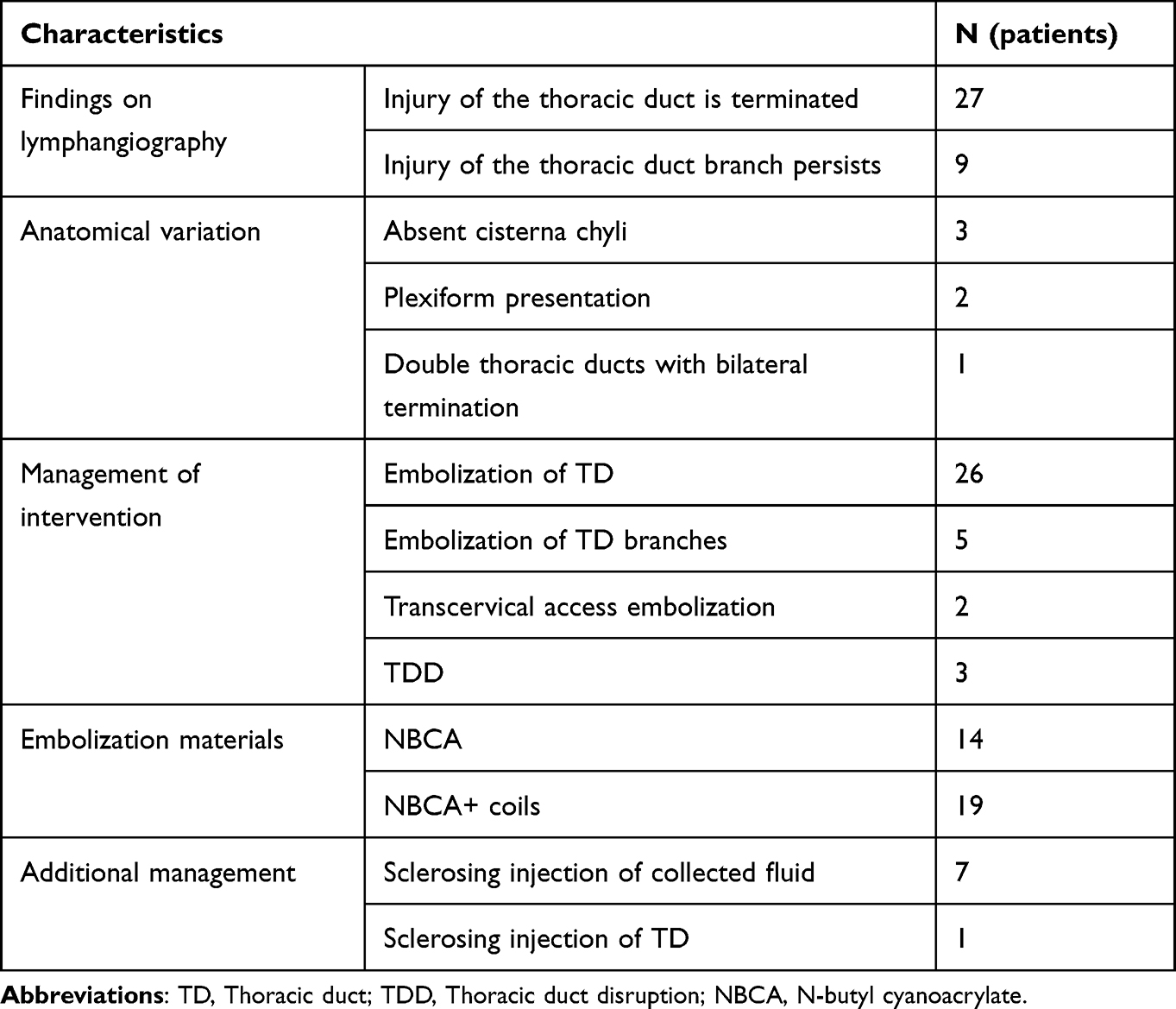 |
Table 3 Procedure Characteristics |
The combined technical and clinical outcomes of intervention are summarized in Figure 1. The technical success rate of transabdominal embolization was 86.1% (31/36 patients); both transcervical access (2/2) and TDD (3/3) were 100% successful. The overall technical success rate of lymphatic embolization was 91.7% (33/36). Following transabdominal embolization, 30 of 31 patients experienced resolution and 1 patient did not. This patient underwent a second procedure: sclerosing injection to the thoracic duct under computed tomography guidance on the 23rd day after TDE. Then, this patient received total parenteral nutrition and octreotide. The causes of failure were inadequate filling and washout of the glue in the lumen of the thoracic duct when the patient was discharged and returned to a normal diet. There was no complication intra and after all procedures.
 |
Figure 1 Flowchart of the technical and clinical outcomes of 36 patients. One patient underwent 2 procedures. |
The clinical success rate after successful transabdominal retrograde access lymphatic embolization was 30/31 patients (96.8%), and after TDD was 3/3 patients (100%). Two patients experienced successful resolution of CL after undergoing transcervical embolization. Clinical success after the initial procedure was found in 35/36 patients. In one patient who underwent a second procedure after initial clinical failure, clinical success was also achieved. Overall, clinical success was achieved in 100% of patients. The hospital stay after intervention was from 3–15 days (median 5 days). Follow-up was performed after 1 month of discharge no one has experienced persistent or recurrent CL.
Discussion
Chyle leak develops as a result of injury to the lymphatic duct after head and neck surgery. It may present as cervical or thoracic leaks. Incidence is significantly higher on the lefthand side because of the anatomy of the TD,10,12 as was the case in our study. One patient presented with a chyle leak on the right side of the neck because of thoracic duct anatomical variance (double thoracic duct with bilateral termination). In our series, we found various leakage points resulting from differences in thoracic duct anatomy (Figure 2). There is no consensus on the need for reoperation or lymphatic embolization as defined by chyle volume loss or timing. Indications for non-conservative treatment vary widely among studies, ranging from 100 mL to 1.1 L per day and/or a persistent chyle leak after 2 to 14 days of conservative management.13,14 Reisenauer et al15 recommended that chyle drainage of ≥1100 mL in 24 hours postoperatively should be considered the threshold for intervention. Others suggest that lymphatic embolization is indicated when the drainage output is >1000 mL in 24 h or >100–300 mL/24 h for over 1 week.14,16
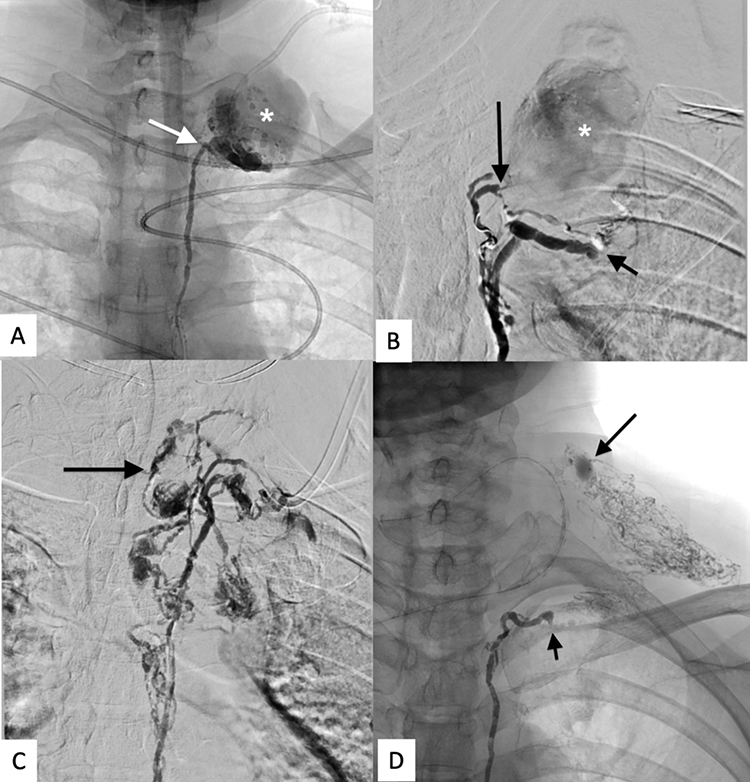 |
Figure 2 Typical features of thoracic duct lesion. (A) Laceration of the proximal part of the TD (arrow) causing extravasation of contrast in fluid collection (star). (B) Laceration of the TD branch (long arrow) causing extravasation of contrast (star) while the normal terminal part of the TD was intact (short arrow). (C) Anatomic change of the TD with the branches; one of these branches was ruptured after lymph node resection (arrow). (D) TD occlusion (short arrow) and laceration of collateral lymphatic vessels (long arrow). |
In our study, transabdominal access was performed in all patients but success was achieved in 86.1% (31/36). Transcervical access and TDD were performed and successful in 2 and 3 patients, respectively. The overall technical success rate of lymphatic embolization was 91.7% (33/36). This rate is lower than that reported by Nadolski et al17 (98%) but higher than the 62.9% reported following the meta-analysis conducted by Kim et al,18 the 67% found by Itkin et al,19 and the 79% reported by Pamarthi et al.20 Crawford et al21 reported an overall TDE success rate of 68%; TDE with transabdominal antegrade access had a 44% success rate; and TDE with transcervical retrograde access had a 77% success rate. There are very few reports about using lymphatic embolization or TDD in management of chyle leak from neck surgery; almost all are sporadic case reports or case series.10,14 Moussa et al10 reported 6 cases undergoing a total of seven TDE procedures; resolution was achieved in all patients. The technical failures of transabdominal access in this study were due to unsuccessful cannulation of the cisterna chyli or thoracic duct. The reasons were small cisterna chyli or inability to visualize them or anatomic variations of the TD (eg, plexiform presentation, double TD). The study of Crawford et al21 showed that most patients who failed TD access had small cisterna chyli; other reasons were TD occlusion and slow progression of the contrast agent to the cisterna chyli. Pamarthi et al20 reported that unsuccessful cannulation was caused by no visualization of the cisterna chyli, inadequate pedal lymphatic vessels for cannulation, left paraaortic cisterna, oversedation, and power injector malfunction. In addition to TDE, we tried to access and embolize the injury branch of TD in order to preserve the thoracic duct; technical and clinical success was achieved in 6 patients. This method has not been commonly mentioned in the literature describing treatment of chyle leak. Kim et al14 reported a study of 8 patients who were successfully treated with lymphatic embolization to manage chyle leak after neck surgery; selective embolization of the TD branches (5 patients) was more highly prioritized than embolization of the terminal thoracic duct (2 patients). Selective embolization with preservation of the thoracic duct has potential because it maximizes preservation of the lymph flow. Moreover, percutaneous ethanol injection of the collected cervical fluid causes fibrosis of the connective tissue around the fistula, which contributes to healing the leak.
The overall clinical success rate of procedures in treatment of chyle leak in this study was 100% for all subjects. This finding is higher than those of Pamarthi et al (64%),20 Itkin et al (71%)19 and Yannes et al (71%).22 A meta-analysis conducted by Kim et al18 showed that the clinical success rates of TDE, TDD and overall were 79.5%, 60.8% and 60.1%, respectively. A systematic review showed median clinical success rates for TDE of 74.6% (range: 57–98%) and TDD of 72% (range: 41.7–100%).13 The use of multiple techniques as assistance or alternative methods when transabdominal access fails could reduce the clinical failure rate. According to Kim et al14 and Moussa et al,10 chyle leak resolved in all patients from 1 to 5 days after intervention. Another study demonstrated that the median time to resolution of chyle leak in patients with TDE was 3 days, and in patients with TDD was 7 days.22
There were no minor or major complications in our study. The rate of complications related to TDE and TDD ranged from 0% to 6.7% and most were minor complications.10,14,19,20 These included non-target glue embolization to the lung, non-target glue embolization to the portal vein, retained guide wire fragment in the retroperitoneum, transient apnea caused by oversedation, perihepatic hematoma at the percutaneous access site, bile leak, further chyle leak, leg edema, and inconsequential coil misplacement.13,14,20 Other possible complications of TDD reported are a hematoma between the aorta and vertebral body and a guide wire fracture.22
There are some limitations to this study. First, we used a retrospective design and there is a lack of long-term follow-up. The patients were followed for only 1 month after the procedure, so no data on long-term complications of TD embolization were collected. Second, the sample size was relatively small and involved a single center; it may thus not be representative of other centers. Third, most of the patients came from other hospitals and had received treatment over a long period of time; thus the previous approaches and surgical ligation techniques experienced by them are unknown and varied. Despite these limitations, this study may provide useful information for the management and treatment of chyle leak following thyroidectomy.
Conclusion
Lymphatic embolization and TDD is a safe and effective procedure that results in resolution of chyle leak after surgery for thyroid cancer. Sclerosing therapy is an adjuvant therapy that contributes to reducing the clinical failure rate. Lymphatic intervention should be the initial treatment of choice for high-output chyle leak or failure of conservative management. A long-term study should be conducted to assess the impact of thoracic duct embolization.
Data Sharing Statement
The datasets generated or analyzed during this study are available from the corresponding author on reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors have no potential conflicts of interest to disclose for this work.
References
1. Lorenz K, Abuazab M, Sekulla C, Nguyen-Thanh P, Brauckhoff M, Dralle H. Management of lymph fistulas in thyroid surgery. Langenbecks Arch Surg. 2010;395(7):911–917. doi:10.1007/s00423-010-0686-2
2. Roh JL, Yoon YH, Park CI. Chyle leakage in patients undergoing thyroidectomy plus central neck dissection for differentiated papillary thyroid carcinoma. Ann Surg Oncol. 2008;15(9):2576–2580. doi:10.1245/s10434-008-0017-9
3. Roh JL, Kim DH, Park CI. Prospective identification of chyle leakage in patients undergoing lateral neck dissection for metastatic thyroid cancer. Ann Surg Oncol. 2008;15(2):424–429. doi:10.1245/s10434-007-9692-1
4. Delaney SW, Shi H, Shokrani A, Sinha UK. Management of chyle leak after head and neck surgery: review of current treatment strategies. Internat J Otolaryngol. 2017;2017:1–12. doi:10.1155/2017/8362874
5. Merki V, Pichler J, Giger R, Mantokoudis G. Chylothorax in thyroid surgery: a very rare case and systematic review of the literature. J of Otolaryngol. 2016;45(1):52. doi:10.1186/s40463-016-0166-y
6. Cuong NN, Hoan L, Linh LT, Tan PH, My TTT, Duc NM. Percutaneous sclerosing injection to the thoracic duct under CT guidance for cervical chylous leakage post thyroidectomy: a case report. Radiol Case Rep. 2021;16(9):2687–2691. doi:10.1016/j.radcr.2021.06.054
7. Chen E, Itkin M. Thoracic duct embolization for chylous leaks. Semin intervent Radiol. 2011;28(01):063–074. doi:10.1055/s-0031-1273941
8. Morikawa K, Takenaga S, Hasumi J, et al. Retrograde transvenous lymphatic embolization for postoperative chylous ascites: a report of three cases and literature review. Radiol Case Rep. 2020;15(9):1623–1628. doi:10.1016/j.radcr.2020.06.052
9. Lee I, Kim HK, Lee J, Soh EY, Kim J. Thoracic duct embolization for chyle leakage after thyroid surgery. Int J Thyroidol. 2020;13(1):47–50. doi:10.11106/ijt.2020.13.1.47
10. Moussa AM, Maybody M, Gonzalez-Aguirre AJ, Buicko JL, Shaha AR, Santos E. Thoracic duct embolization in post-neck dissection chylous leakage: a case series of six patients and review of the literature. Cardiovasc Intervent Radiol. 2020;43(6):931–937. doi:10.1007/s00270-020-02475-9
11. Cope C, Kaiser LR. Management of unremitting chylothorax by percutaneous embolization and blockage of retroperitoneal lymphatic vessels in 42 patients. J Vasc Interv Radiol. 2002;13(11):1139–1148. doi:10.1016/S1051-0443(07)61956-3
12. Lee J, Bae IE, Yoon J, et al. Postoperative chylothorax after modified radical neck dissection for thyroid carcinoma: a missable rare complication of thyroid surgery. Medicina. 2020;56(9):481. doi:10.3390/medicina56090481
13. Power R, Smyth P, Donlon NE, Nugent T, Donohoe CL, Reynolds JV. Management of chyle leaks following esophageal resection: a systematic review. Dis Esophagus. 2021;34(11):doab012. doi:10.1093/dote/doab012
14. Kim J, Bang DH, Choi TW, Won JH, Kwon Y. Lymphangiography and lymphatic embolisation for the treatment of chyle leaks after neck surgery: assessment of lymphangiography findings and embolisation techniques. BJR. 2023;96:20220831. doi:10.1259/bjr.20220831
15. Reisenauer JS, Puig CA, Reisenauer CJ, et al. Treatment of Postsurgical Chylothorax. Ann Thorac Surg. 2018;105(1):254–262. doi:10.1016/j.athoracsur.2017.07.021
16. Wang X, Wang S, Li C, et al. Lymph or chyle leak after neck dissection in patients with thyroid carcinoma: results of a study on 1724 patients. Am Surg. 2022;88(1):109–114. doi:10.1177/0003134820981723
17. Nadolski GJ, Itkin M. Lymphangiography and thoracic duct embolization following unsuccessful thoracic duct ligation: imaging findings and outcomes. J Thoracic Cardiovasc Surg. 2018;156(2):838–843. doi:10.1016/j.jtcvs.2018.02.109
18. Kim PH, Tsauo J, Shin JH. Lymphatic Interventions for chylothorax: a systematic review and meta-analysis. J Vasc Interv Radiol. 2018;29(2):194–202.e4. doi:10.1016/j.jvir.2017.10.006
19. Itkin M, Kucharczuk JC, Kwak A, Trerotola SO, Kaiser LR. Nonoperative thoracic duct embolization for traumatic thoracic duct leak: experience in 109 patients. J Thoracic Cardiovasc Surg. 2010;139(3):584–590. doi:10.1016/j.jtcvs.2009.11.025
20. Pamarthi V, Stecker MS, Schenker MP, et al. Thoracic duct embolization and disruption for treatment of chylous effusions: experience with 105 patients. J Vasc Interv Radiol. 2014;25(9):1398–1404. doi:10.1016/j.jvir.2014.03.027
21. Crawford D, Guevara CJ, Kim SK. Thoracic duct embolization using transabdominal antegrade and transcervical retrograde accesses. J Vasc Interv Radiol. 2022;33(12):1536–1541. doi:10.1016/j.jvir.2022.08.022
22. Yannes M, Shin D, McCluskey K, Varma R, Santos E. Comparative analysis of intranodal lymphangiography with percutaneous intervention for postsurgical chylous effusions. J Vasc Interv Radiol. 2017;28(5):704–711. doi:10.1016/j.jvir.2016.12.1209
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.