")
Back to Journals » Infection and Drug Resistance » Volume 14
Microbial Repercussion on Hemodialysis Catheter-Related Bloodstream Infection Outcome: A 2-Year Retrospective Study
Authors Abd El-Hamid El-Kady R, Waggas D, AkL A
Received 9 August 2021
Accepted for publication 21 September 2021
Published 1 October 2021 Volume 2021:14 Pages 4067—4075
DOI https://doi.org/10.2147/IDR.S333438
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Rania Abd El-Hamid El-Kady, 1, 2 Dania Waggas, 2 Ahmed AkL 3, 4
1Department of Medical Microbiology and Immunology, Faculty of Medicine, Mansoura University, Mansoura, Egypt; 2Department of Pathological Sciences, Fakeeh College for Medical Sciences, Jeddah, Kingdom of Saudi Arabia; 3Department of Nephrology, Urology and Nephrology Center, Mansoura University, Mansoura, Egypt; 4Department of Internal Medicine/Adult Nephrology, Dr. Soliman Fakeeh Hospital, Jeddah, Kingdom of Saudi Arabia
Correspondence: Rania Abd El-Hamid El-Kady
Department of Pathological Sciences, Fakeeh College for Medical Sciences, Jeddah, 2537, Kingdom of Saudi Arabia
Tel +966 569849897
Email [email protected]
Background: Albeit growing technical advances in the design of hemodialysis catheters, intravascular catheter-related bloodstream infection (CRBSI) still represents an utmost clinical challenge to the health-care workers (HCWs). Data regarding the influence of the culprit organism on the scenario of CRBSI in the literature are extremely lacking. Thereby, this research was carried out.
Methods: We undertook a retrospective cohort study over an interval of 2 years, involving patients who underwent regular hemodialysis via catheters in the Renal Dialysis Unit (RDU) of Dr. Soliman Fakeeh Hospital (DSFH), Jeddah, Kingdom of Saudi Arabia (KSA). The study enrolled 139 patients (56.8% females and 43.2% males), with mean age of 60.79 ± 11.45 years.
Results: The aggregate rate of CRBSI was 5.1/1000 catheter days. Amongst the 139 study candidates confirmed of having CRBSI, while 69.8% of CRBSIs were ascribed to Gram-positive cocci, about one-third of the infectious episodes were secondary to Gram-negative bacilli. Interestingly, fever was the most common presentation of S. aureus CRBSI compared to CoNS and Gram-negative bacilli CRBSIs (20.9% versus 12.9% versus 6.5%, p= 0.0001), whereas CRBSIs due to CoNS were presented mainly with rigors (19.4%). Of note, CRBSIs caused by Gram-negative bacilli had a tendency to manifest with unusual symptoms such as vomiting or hypotension. Besides, they were more prone to involve hospitalization or ICU admission. In this study, no mortality was attributed to CRBSIs.
Conclusion: Our study disclosed that the illicit organism has a repercussion on the clinical presentation as well as the fate of CRBSI among hemodialysis patients. This highlights the worth of identifying the infected cases in a periodic manner, to avoid the occurrence of devastating complications. A large body of work from various hemodialysis centers should take place in the near future so as to provide more insight in this perspective.
Keywords: hemodialysis, catheter, ESRD, CRBSI, susceptibility
A Letter to the Editor has been published for this article.
Introduction
The rising rate of end-stage renal disease (ESRD) around the world, and the requirement for hemodialysis as a treatment thereof, is a crucial indication for the use of central venous catheters (CVCs).1 According to the annals of the United States Renal Data System, about 80% of the incident and 20% of the prevalent hemodialysis patients require CVCs as their initial vascular route.2 Nonetheless, hemodialysis catheter insertion may be complicated by hemodialysis catheter-related bloodstream infection (HD-CRBSI) which is a noteworthy confront for the health-care sector owing to increased patient morbidity, mortality, and economic load.3 Recently, it is estimated that CRBSIs occur at a rate of 5.37 to 6.5/1000 catheter days.4
Patients undergoing hemodialysis are liable to infection cited for several predisposing issues, including compromised immune status, recurrent exposure to hospital instruments, as well as microbial colonization of the hemodialysis catheter during hemodialysis sessions.5 It is proposed that microbial bloodstream invasion and subsequent CRBSI can occur by one of 2 routes. An extraluminal pathway, in which the microorganisms are transferred from the skin insertion site to the catheter tip and then invade the blood stream.6 Alternatively, the intraluminal pathway involves adventitious contamination of the catheter hub and subsequent microbial colonization of the lumen secondary to improper aseptic precautions during catheter manipulation by the health-care personnel.7
Regardless of the pathway of infection, whenever the pathogen is introduced into the bloodstream, it may adhere to the catheter surface or become embedded within a fibrin layer.8 Being an inanimate medical device, microbial attachment to the catheter surface stimulates biofilm formation which is an orchestrated community of microorganisms living within an exopolysaccharide matrix.9 CRBSIs are frequently caused by Gram-positive bacteria, particularly coagulase-negative staphylococci (CoNS) and Staphylococcus aureus.10 Currently, Gram-negative bacteria are condemned to be etiologic agents for CRBSIs.11
Hitherto, limited data are existing concerning the influence of the infectious agent on the clinical presentation and prognosis of CRBSIs. In view of that, this retrospective cohort study was conducted to (i) determine the incidence of CRBSIs during a 2-year study period among hemodialysis patients who underwent hemodialysis in the Renal Dialysis Unit (RDU) of Dr. Soliman Fakeeh Hospital (DSFH), (ii) figure out the microbiological spectrum of CRBSIs and the antimicrobial susceptibility pattern of the recovered isolates, and (iii) investigate the impact of the infecting organism on the patients’ clinical characteristics as well as the outcome of CRBSI.
Patients and Methods
Study Design, Population, and Setting
This retrospective cohort study enrolled 139 consecutive adult (>18 years) ESRD patients diagnosed with HD-CRBSI (single episode/patient) throughout a duration of 2 years (January 2019 to December 2020). The study cohort was selected from patients who underwent hemodialysis through CVCs at the RDU under the care of the Nephrology Department of DSFH (a private, tertiary-care hospital), Jeddah, Saudi Arabia. The RDU of DSFH is a 17-bedded facility that provides inpatient and outpatient services for the dwellers of Saudi Arabia (natives and citizens).
Study Participants’ Data Collection
Patients’ medical record numbers (MRN) were used to electronically extract the data related to the study group including (a) demographic characteristics, (b) primary cause of ESRD, (c) any associated comorbidity, (d) clinical presentation of CRBSI such as fever, rigors, hypotension, or vomiting, and (e) site of hemodialysis catheter insertion.
Data indicating a complicated-CRBSI were also retrieved including (a) need to hospitalization and its duration, (b) admission to the ICU, (c) metastatic infection diagnosed by clinical presentation as well as imaging techniques, and (d) death.
Criteria for Diagnosis of CRBSI
The engaged patients were confirmed to have CRBSI according to the 2009 Infectious Diseases Society of America (IDSA) diagnostic criteria.12 Data on blood culture results as well as catheter segment or tip culture results from the recruited patients during the study period, including the causative microorganisms as well as the antimicrobial susceptibility profiles were captured from the electronic database of the Microbiology Laboratory of DSFH.
The specimens were processed in keeping with the standard policies of the hospital laboratory with VITEK TWO (bioMérieux, Brazil) automated system used for the identification and susceptibility testing of the recovered isolates. Antibiotic sensitivity results were interpreted as per the published criteria of the Clinical and Laboratory Standards Institute (CLSI),13,14 whereas tigecycline susceptibility results were interpreted on the basis of the European Committee on Antimicrobial Susceptibility Testing (EUCAST) breakpoints.15
Exclusion Criteria
Hemodialysis patients who presented with other source of infection, and patients <18 years old were excluded from our study.
Statistical Analysis
All data were collected, processed, and analyzed using IBM®SPSS® Statistics program version 26.0 for Windows (SPSS Inc., Chicago, IL, USA). The number of catheter days was calculated as the number of days from catheter insertion to removal, and the CRBSI rate was calculated as the number of CRBSI episodes/1000 catheter days (episodes of CRBSI/total sum of catheter days × 1000).16
Categorical variables were described as numbers and percentages with Pearsons Chi-Square (χ2) test used for comparison; meanwhile, Fischer’s Exact test was used as a correction for χ2 test when >25% of cells have count <5 in 2×2 tables. Continuous variables were described as means ± standard deviation (SD) for parametric data after testing normality using Kolmogorov-Smirnov test. The difference was considered statistically significant at p values ≤0.05.
Results
Demographics and Baseline Features of the Study Population
A total of 139 hemodialysis patients with a mean age of 60.79 ± 11.45 years were proven to have a CRBSI (a single isolate/patient) based on the 2009 IDSA diagnostic criteria. The study cohort included 56.8% females and 43.2% males (p= 0.1). About two-thirds of our cohort were Saudi nationals. Diabetic nephropathy was the most predominant cause for ESRD accounting for 45.3%, whereas the most relevant comorbid condition was cardiovascular disease (17.3%).
Serologic testing disclosed that 19 (13.7%) patients had hepatitis B, 12 (8.6%) were infected with human immunodeficiency virus (HIV), and 7 (5%) had hepatitis C. Approximately 6% of our cohort were suffering from malignant conditions along with ESRD (3.6% hepatocellular carcinoma, 1.4% chronic myeloid leukemia, and 1% multiple myeloma). Likewise, patients with underlying lupus nephritis (13.7%) and immune thrombocytopenic purpura (6.5%) were receiving immunosuppressive therapy (Table 1).
 |
Table 1 Demographic Characteristics of the Study Participants |
Criteria of the Used CVCs
In our cluster of patients, hemodialysis was accomplished via tunneled hemodialysis catheters (THCs). The mean duration of CVC insertion was 49.54 ± 10.84 days. The most common site for catheter insertion was the right jugular vein (43.9%) followed by the left jugular vein (19.4%). On the other hand, the left femoral vein was the least frequently used vascular access for catheter insertion amongst our cohort (1.4%). Overall, the incidence rate of CRBSI was 5.1 episodes/1000 catheter days.
Microbiology of CRBSIs
In the present work, Gram-positive cocci were the most commonly retrieved isolates with CoNS and S. aureus constituting 39.6% and 30.2%, respectively, of the total strains. On the other hand, Gram-negative bacilli represented approximately one-third of the isolates (30.2%). No fungal isolates were recovered during the study period. Also, no polymicrobial episodes of CRBSIs had been recorded (Table 2).
 |
Table 2 Spectrum of the Pathogens Associated with CRBSI Among the Study Subjects |
Antibiotic Sensitivity Patterns of Gram-Positive Cocci Causing CRBSIs
None of the retrieved Gram-positive cocci (CoNS and S. aureus isolates) showed resistance to vancomycin, teicoplanin, or tigecycline. Only one S. aureus isolate was resistant to linezolid (LRSA). Based on cefoxitin sensitivity testing,17 methicillin-resistant S. epidermidis (MRSE) and methicillin-resistant S. aureus (MRSA) comprised 47.4% and 33.3% of the total S. epidermidis and S. aureus isolates, respectively. None of the isolated strains demonstrated sensitivity to penicillin.
Antibiotic Sensitivity Patterns of Gram-Negative Bacilli Associated with CRBSIs
Out of 30 tested Gram-negative isolates against tigecycline, only one Acinetobacter baumannii strain was resistant. Unanticipatedly, almost half of the investigated Gram-negative isolates were proven to be extended spectrum β-lactamase (ESBL)-producers. On top of that, 19% of the isolates were carbapenem-resistant, whereas 16.7% were multidrug-resistant (Table 3).
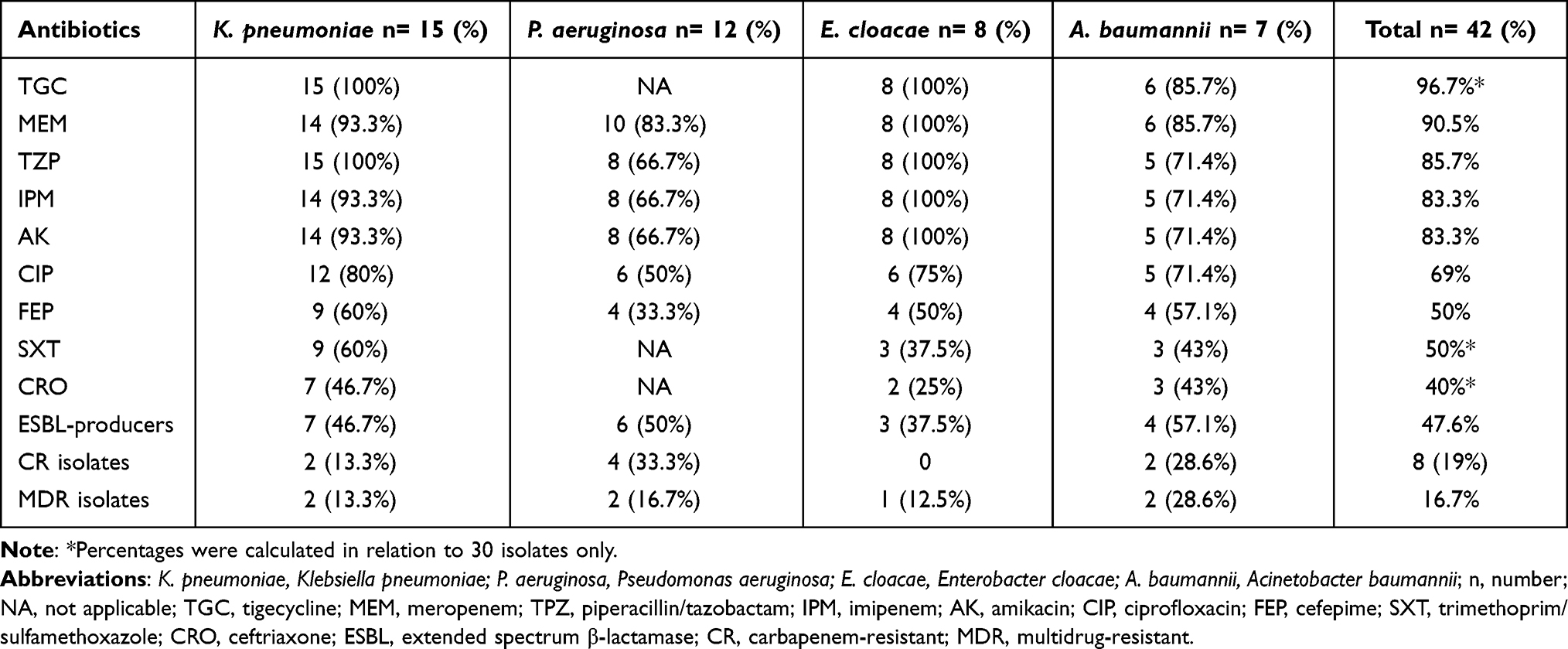 |
Table 3 Antibiotic Susceptibility Profiles of Gram-Negative Bacilli Causing CRBSIs |
Correlation Between the Clinical Presentation of CRBSI and the Causative Organism
In the current study, out of 139 infected cases, the primary clinical presentation of CRBSI was fever (40.3%) followed by rigors (30.2%). Only 15.1% and 14.4% of the study cohort experienced vomiting and hypotension as the chief presenting symptom, respectively.
Table 4 illustrates the distribution of different clinical manifestations of CRBSI according to the causative organism. Notably, fever was the most frequent presentation of S. aureus CRBSI in relation to that of CoNS and Gram-negative bacilli (p= 0.0001). Nevertheless, rigors were more recurrent in infections caused by CoNS (p= 0.0001). For Gram-negative CRBSI, vomiting and hypotension were more commonly recorded compared to S. aureus- and CoNS-attributed CRBSI with a statistically significant difference (p= 0.014, and 0.033, respectively).
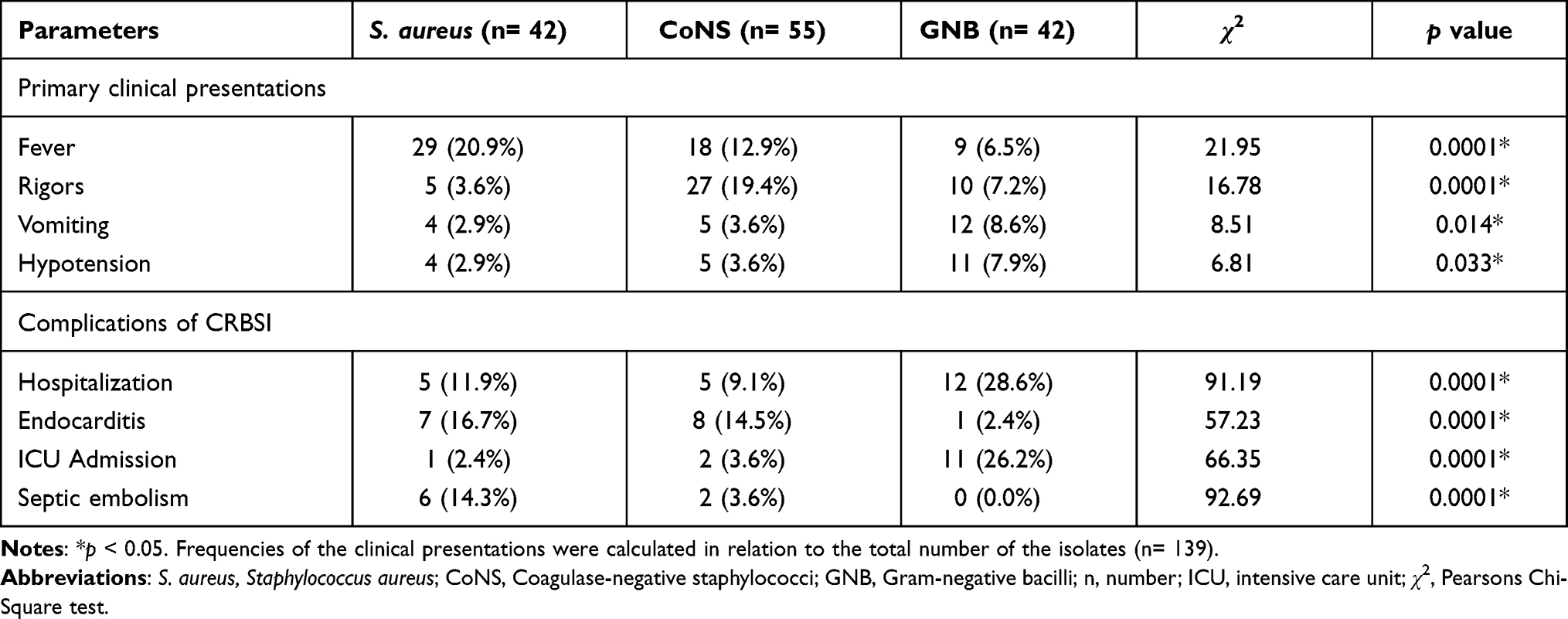 |
Table 4 Primary Clinical Presentations and Complications of CRBSIs in Relation to the Causative Organism |
Correlation Between the Complications of CRBSI and the Causative Organism
Of 139 patients, 60 (43.2%) cases experienced complications secondary to CRBSI. Hospital admission to the Adult Nephrology Department (DSFH) was the most common complication (15.8%) followed by endocarditis (11.5%). In addition, 10.1% of our series required an admission to the ICU, while 5.8% developed septic embolism.
Table 4 summarizes different complications of CRBSI structured along with the etiologic agents. Approximately 29% of the patients that acquired Gram-negative CRBSIs (12 out of 42) required hospitalization, in contrast to 12% and 9% of those caused by S. aureus and CoNS, respectively (p= 0.0001). The mean hospital stay for Gram-negative CRBSIs was 7.75 ± 2.42 versus 4.6 ± 1.52 and 4.4 ± 1.14 days for that caused by CoNS and S. aureus, respectively (p= 0.005). Moreover, Gram-negative CRBSIs were more commonly associated with admission to the ICU of DSFH (26.2%). On the other hand, endocarditis and septic embolism were more generally observed in S. aureus CRBSIs (16.7% and 14.3%, respectively).
Discussion
No doubt that the use of CVCs to initiate hemodialysis saved the lives of patients requiring renal replacement therapy. However, CRBSI is a conspicuous barrier for the use of these catheters. CRBSI ranks the second leading cause of mortality in patients undergoing hemodialysis.18 In patients with ESRD, increased infection rate is assigned to uremia which contributes to defective cell-mediated immunity (CMI), neutrophil dysfunction, as well as complement activation disorders.19
In this retrospective cohort study that enrolled 139 participants over a period of 2 years, CRBSI had occurred at a cumulative rate of 5.1 episodes/1000 days of use of hemodialysis catheters, which comes close to rates reported by other investigators.20 A recent Indian paper published by Viswanath and his associates declared an even higher infection rate up to 12.5 episodes/1000 catheter days.21 On the flip side, considerably lower rates were declared by Thompson et al from one Canadian study (0.19/1000 catheter days)22 and Smyth et al from another study held in Australia and New Zealand (0.39–1.2/1000 catheter days).23 It seems that the incidence of CRBSI varies from country to country and from one medical center to another. The dissimilar rates could be explained by different geographic locations with unalike adherence to infection control measures among the hemodialysis centers as well as incongruent demographic profiles of patients undergoing hemodialysis.
In the present work, the microbiological outline of CRBSIs showed that Gram-positive bacteria were incriminated into two-thirds of these infections, with 39.6% and 30.2% of the episodes, not amazingly, caused by CoNS and S. aureus, respectively. Rather, Klebsiella pneumoniae was the most predominant organism among Gram-negative isolates contributing to 10.8% of CRBSIs. Our findings have been echoed in analogous series where S. epidermidis, a normal skin flora, together with other CoNS, have been repeatedly recorded in many studies to be the most common cause of CRBSI. It is postulated that the movement of the bacterial flora lengthwise to the insertion site of the catheter into the skin, paves the way for bacterial contamination of the catheter hub, and consequent intraluminal infection by Gram-positive organisms, especially CoNS.24
In keeping with our findings, Hadian et al concluded that CoNS were the most preponderant cause of CRBSI (44%) followed by S. aureus (28.6%) and Gram-negative bacilli.25 In addition, Mohamed et al found that the most dominant culprits among their cohort of Irish hemodialysis patients were CoNS (61%) and S. aureus (23%), though Gram-negative isolates were identified in less than 5% of the specimens.26
Unexpectedly, a similar study conducted in Saudi Arabia at the Regional Kidney Center at King Abdul Aziz Specialist Hospital, Taif, concluded that S. aureus was the most prevalent organism among the isolated Gram-positive cocci.27 Definitely, nasal carriage of S. aureus is a major promoting factor for developing a HD-CRBSI, because contaminated hands facilitate the transmission of these bacteria to the catheter insertion site. Accordingly, decolonization procedures in the hemodialysis settings involving intranasal mupirocin prophylaxis should be considered to lessen the incidence of infectious episodes, and subsequently the health-care expenses proportionate to treating CRBSIs once they ensue.28
Quite the reverse of our ascertained microbial pattern, a comparable study conducted in Brazil,29 another one in Jeddah, KSA,30 and a third one in Hofuf, KSA31 had proven a paramountcy of Gram-negative bacteria, accounting for 50%, 54.6%, and 61.5% of CRBSIs, respectively. A high infection rate with Gram-negative bacilli in health-care settings raises concern about the possibility of inadequate hand hygiene and poor compliance to catheter maintenance precautions by the health-care staff of the affiliated hemodialysis center, which should be taken into account while implementing infection control and prevention policies.
Awareness of the pertinent antibiotic sensitivity profiles of the bacterial isolates in hemodialysis units is highly indicated in order to select the ideal antibiotics together with tailoring empiric therapy. Unfortunately, the frequent prescription of antibiotic regimens owing to repeated hospital admissions of hemodialysis patients culminated into infections with antimicrobial-resistant bugs.32 In the contemporary analysis, whereas about half of our S. epidermidis isolates were methicillin-resistant, around one-third of S. aureus strains demonstrated methicillin resistance. Fram and his associates reported that while 38.5% of their S. aureus isolates were methicillin-resistant, all the recovered CoNS were resistant to this antimicrobial.33 Interestingly, none of the recovered isolates from our sequence of patients displayed resistance to vancomycin, or teicoplanin. Similar conclusions were also drawn by other investigators.34 Outstandingly, none of the test isolates showed sensitivity to penicillin, signifying the injudicious outpatient use of this antibiotic.
Of the Gram-negative organisms, 14% and 19% were resistant to piperacillin/tazobactam and carbapenems, respectively. One impressive finding was the production of ESBLs in almost half of our Gram-negative isolates. Other than that, 16.7% of the recovered isolates were multidrug-resistant (MDR). These unpredictably high rates of antimicrobial resistance highlight the need for stringent infection-control measures and intervention strategies, including antibiotic recycling to diminish additional emergence and propagation of these serious bugs.
Of clinical note, fever was the most common manifestation of sepsis among our cohort (40.3%), followed by rigors (30.2%). Furthermore, vomiting and hypotension were the main pointing alarms to CRBSI in 15.1% and 14.4% of the study population, respectively. It is worth mentioning that, in our study, fever was the most frequent presenting symptom of CRBSIs attributed to S. aureus (20.9%), in comparison to those caused by CoNS (12.9%) and Gram-negative bacilli (6.5%) with a statistically significant difference (p= 0.0001). On the other side, CoNS-triggered CRBSIs were predominantly presented with rigors (19.4%). A substantial proportion of Gram-negative CRBSIs were presented with non-specific symptoms such as vomiting and hypotension as well. The endotoxins present in the outer membrane of Gram-negative bacteria may in part subscribe to hypotension.35 Our data are in accord with those of an earlier work issued by Al-Solaiman et al.36
Undesirably, CRBSIs are associated with sequelae farther the initial incident in some hemodialysis patients. In the current work, 43.2% of the infected patients got ancillary complications such as hospitalization to the Adult Nephrology Department (15.8%), endocarditis (11.5%), admission to the ICU (10.1%), and septic embolism (5.8%). It should be noted that hospitalizations with lengthy hospital stays recurred more often in patients suffering from Gram-negative CRBSIs as compared to those with S. aureus or CoNS (almost 29% versus 12% versus 9%, respectively), with a remarkably significant difference (p= 0.0001). On top of that, admission to the ICU was mandatory in 26.2% of Gram-negative CRBSIs as opposed to 3.6% of CoNS- and 2.4% of S. aureus- associated CRBSIs (p= 0.0001). Conversely, Al-Solaiman et al36 and Farrington and Allon37 noticed that the likelihood of hospitalization and ICU admission was highest with S. aureus, moderate with S. epidermidis, and least with Gram-negative CRBSIs.
In the present study, metastatic infections such as endocarditis (33.6%) and septic embolism (17.9%) had developed in our set of patients. Strikingly, the incidence of these 2 complications inclined to be more common with S. aureus rather than CoNS or Gram-negative CRBSIs, with a statistically significant difference (p= 0.0001). Our observations are in conformity with the results of former studies.37,38
It is important to address the fact that all of our infected patients received empiric systemic antibiotic therapy in the outpatient settings while waiting culture and sensitivity results (intravenous vancomycin and ceftazidime). When culture results returned back, their treatment was tailored to the reported sensitivity patterns. Interestingly, 79 patients (56.8%) responded to a 4-week antibiotic regimen (uncomplicated CRBSIs). On the other hand, the remaining patients that developed complicated CRBSIs did not respond to the prescribed antibiotics, which necessitated catheter replacement as well as longer course of antibiotics (6–8 weeks).
While it has been lately reported by Quinn et al, in one Canadian study, that CRBSIs culminated into death of 2.3% of their cohort,39 Farrington and Allon affirmed that only 1% of the recorded mortality between their catheter-reliant hemodialysis patients was ascribed to CRBSI.37 Recently, a substantively higher mortality rate up to 5% was specified by Martin et al.40 In contrast, although 2.16% of our hemodialysis patients died during the 2 years-study period, mortality could not be allocated directly to CRBSI, denoting that the use of hemodialysis catheters was not a leading cause of death per se amongst our cohort.
Indeed, our study has some limitations that are worth mentioning. First, the retrospective design of the study makes it amenable to selection bias of the study cohort. Second, the study mirrors a single-center experience, so globalization of our results may not be compatible with other hemodialysis centers. Finally, our cohort included only adult patients, making relevance of these findings to children undergoing hemodialysis unrealistic.
Conclusion
Our study showed that the causative organism has a fingerprint on the clinical presentation as well as the consequence of CRBSI among hemodialysis patients. Therefore, it is crucial for each hemodialysis center to early recognize and treat infected patients, so as to achieve optimal treatment outcomes. What is more, data regarding the antibiotic susceptibility patterns of the causative organisms as well as their periodic monitoring in the hemodialysis settings is of utmost importance to allow for the best choice of antimicrobials along with re-evaluating empiric therapy.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Ethics Approval and Informed Consent
The study was conducted in accordance with the Declaration of Helsinki. The study protocol was approved by the institutional review board (IRB) of DSFH (183/IRB/2021), and the need for informed consent was waived since all data were anonymized before analysis. Patients’ data privacy and confidentiality were respected in all levels of the study.
Disclosure
The authors have no conflicts of interest to declare.
References
1. Böhlke M, Uliano G, Barcellos FC. Hemodialysis catheter-related infection: prophylaxis, diagnosis and treatment. J Vasc Access. 2015;16(5):347–355. doi:10.5301/jva.5000368
2. United States Renal Data System. Annual data report; 2018.
3. El Nekidy WS, Soong D, Kadri A, Tabbara O, Ibrahim A, Ghazi IM. Salvage of hemodialysis catheter in staphylococcal bacteremia: case series, revisiting the literature, and the role of the pharmacist. Case Rep Nephrol Dial. 2018;8(2):121–129. doi:10.1159/000489923
4. Shah S, Singhal T, Naik R, Thakkar P. Incidence and etiology of hemodialysis catheter related blood stream infections at a tertiary care hospital in Mumbai: a 5 year review. Indian J Nephrol. 2020;30(2):132–133. doi:10.4103/ijn.IJN_127_19
5. Zhang J, Burr RA, Sheth HS, Piraino B. Organism-specific bacteremia by hemodialysis access. Clin Nephrol. 2016;86(9):141–146. doi:10.5414/CN108633
6. Mermel LA. What is the evidence for intraluminal colonization of hemodialysis catheters? Kidney Int. 2014;86(1):28–33. doi:10.1038/ki.2013.527
7. Lock CE. Management of a patient with catheter-related bloodstream infection. Clin J Am Soc Nephrol. 2017;12(11):1873–1877. doi:10.2215/CJN.01210217
8. Veerachamy S, Yarlagadda T, Manivasagam G, Yarlagadda PK. Bacterial adherence and biofilm formation on medical implants: a review. Proc Inst Mech Eng H. 2014;228(10):1083–1099. doi:10.1177/0954411914556137
9. Zatorska B, Groger M, Moser D, Diab-Elschahawi M, Lusignani LS, Presterl E. Does extracellular DNA production vary in staphylococcal biofilms isolated from infected implants versus controls? Clin Orthop Relat Res. 2017;475(8):2105–2113. doi:10.1007/s11999-017-5266-0
10. Sahli F, Feidjel R, Laalaoui R. Hemodialysis catheter-related infection: rates, risk factors and pathogens. J Infect Public Health. 2017;10(4):403–408. doi:10.1016/j.jiph.2016.06.008
11. Wright MO, Decker SG, Allen-Bridson K, Hebden JN, Leaptrot D. Healthcare-associated infections studies project: an American Journal of Infection Control and National Healthcare Safety Network data quality collaboration: location mapping. Am J Infect Control. 2018;46(5):577–578. doi:10.1016/j.ajic.2017.12.012
12. Mermel LA, Allon M, Bouza E, et al. Clinical practice guidelines for the diagnosis and management of intravascular catheter-related infection: 2009 update by the Infectious Diseases Society of America. Clin Infect Dis. 2009;49(1):1–45.
13. Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing.
14. Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing.
15. European Committee on Antimicrobial Susceptibility Testing. Breakpoint tables for interpretation of MICs and zone diameters. Version 9.0; 2018. Available from: http://www.eucast.org.
16. Sun Y, Bao Z, Guo Y, Yuan X. Positive effect of care bundles on patients with central venous catheter insertions at a tertiary hospital in Beijing, China. J Int Med Res. 2020;48(7):030006052094211. doi:10.1177/0300060520942113
17. Skov R, Larsen AR, Kearns A, et al. Phenotypic detection of mecC-MRSA: cefoxitin is more reliable than oxacillin. J Antimicrob Chemother. 2014;69(1):133–135. doi:10.1093/jac/dkt341
18. Laurin LP, Harrak H, Elftouh N, Ouimet D, Vallée M, Lafrance JP. Outcomes of infection-related hospitalization according to dialysis modality. Clin J Am Soc Nephrol. 2015;10(5):817–824. doi:10.2215/CJN.09210914
19. Nguyen DB, Arduino MJ, Patel PR. Hemodialysis-associated infections. In: Chronic Kidney Disease, Dialysis, and Transplantation; 2019:389–410. e8.
20. Chandra A, Das A, Sen M, Srivastava D. Haemodialysis catheter-related blood stream infection in ESRD patients: incidence, outcome and antibiogram of the isolated organisms. Int J Adv Med. 2016;3(4):912–919. doi:10.18203/2349-3933.ijam20163723
21. Viswanath MV, Sadineni R, Rao VP, Kolla PK. Clinical profile of hemodialysis catheter related bloodstream infections. EJMCM. 2021;8(2):919–933.
22. Thompson S, Wiebe N, Klarenbach S, et al.; Alberta Kidney Disease Network. Catheter-related blood stream infections in hemodialysis patients: a prospective cohort study. BMC Nephrol. 2017;18(1):357. doi:10.1186/s12882-017-0773-5
23. Smyth B, Kotwal S, Gallagher M, Gray NA, Polkinghorne K; REDUCCTION Partnership Project. Dialysis catheter management practices in Australia and New Zealand. Nephrology. 2019;24(8):827–834. doi:10.1111/nep.13507
24. Gahlot R, Nigam C, Kumar V, Yadav G, Anupurba S. Catheter-related bloodstream infections. Int J Crit Illn Inj Sci. 2014;4(2):162–167. doi:10.4103/2229-5151.134184
25. Hadian B, Zafarmohtashami A, Razani M. Catheter-related blood stream infections in hemodialysis patients. J Renal Inj Prev. 2020;9(4):e34. doi:10.34172/jrip.2020.34
26. Mohamed H, Ali A, Browne LD, et al. Determinants and outcomes of access-related blood-stream infections among Irish haemodialysis patients; a cohort study. BMC Nephrol. 2019;20(1):68. doi:10.1186/s12882-019-1253-x
27. Masoodi I, Alharth FR, Irshad S, et al. Hemodialysis catheter-related infections: results of a tertiary care center study in Saudi Arabia. Int J Med Sci Public Health. 2019;8(4):319–325. doi:10.5455/ijmsph.2019.0203107032019
28. Fisher M, Golestaneh L, Allon M, Abreo K, Mokrzycki MH. Prevention of bloodstream infections in patients undergoing hemodialysis. Clin J Am Soc Nephrol. 2020;15(1):132–151. doi:10.2215/CJN.06820619
29. Menegueti MG, Betoni NC, Bellissimo-Rodrigues F, Romão EA. Central venous catheter-related infections in patients receiving short-term hemodialysis therapy: incidence, associated factors, and microbiological aspects. Rev Soc Bras Med Trop. 2017;50(6):783–787. doi:10.1590/0037-8682-0438-2017
30. Alhazmi SM, Noor SO, Alshamrani MM, Farahat FM. Bloodstream infection at hemodialysis facilities in Jeddah: a medical record review. Ann Saudi Med. 2019;39(4):258–264. doi:10.5144/0256-4947.2019.258
31. Mohsin B. Pattern of causative micro-organisms in catheter related blood stream infections in dialysis patients: experience from Saudi Arabia. J Ayub Med Coll Abbottabad. 2017;29(4):635–640.
32. Wang TZ, Kodiyanplakkal RPL, Calfee DP. Antimicrobial resistance in nephrology. Nat Rev Nephrol. 2019;15(8):463–481. doi:10.1038/s41581-019-0150-7
33. Fram D, Okuno MF, Taminato M, et al. Risk factors for bloodstream infection in patients at a Brazilian hemodialysis center: a case-control study. BMC Infect Dis. 2015;15(1):158. doi:10.1186/s12879-015-0907-y
34. Agrawal V, Valson AT, Mohapatra A, et al. Fast and furious: a retrospective study of catheter-associated bloodstream infections with internal jugular nontunneled hemodialysis catheters at a tropical center. Clin Kidney J. 2019;12(5):737–744. doi:10.1093/ckj/sfy138
35. Ehrentraut S, Frede S, Stapel H, et al. Antagonism of lipopolysaccharide-induced blood pressure attenuation and vascular contractility. Arterioscler Thromb Vasc Biol. 2007;27(10):2170–2176. doi:10.1161/ATVBAHA.107.146100
36. Al-Solaiman Y, Estrada E, Allon M. The spectrum of infections in catheter-dependent hemodialysis patients. Clin J Am Soc Nephrol. 2011;6(9):2247–2252. doi:10.2215/CJN.03900411
37. Farrington CA, Allon M. Complications of hemodialysis catheter bloodstream infections: impact of infecting organism. Am J Nephrol. 2019;50(2):126–132. doi:10.1159/000501357
38. Maya ID, Carlton D, Estrada E, Allon M. Treatment of dialysis catheter-related Staphylococcus aureus bacteremia with an antibiotic lock: a quality improvement report. Am J Kidney Dis. 2007;50(2):289–295. doi:10.1053/j.ajkd.2007.04.014
39. Quinn RR, Oliver MJ, Devoe D, et al. The effect of predialysis fistula attempt on risk of all-cause and access-related death. J Am Soc Nephrol. 2017;28(2):613–620. doi:10.1681/ASN.2016020151
40. Martin K, Lorenzo YSP, Leung PYM, et al. Clinical outcomes and risk factors for tunneled hemodialysis catheter-related bloodstream infections. Open Forum Infect Dis. 2020;7(6):ofaa117. doi:10.1093/ofid/ofaa117
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.