")
Back to Journals » Open Access Rheumatology: Research and Reviews » Volume 14
Metabolic Abnormalities, Cardiovascular Disease, and Metabolic Syndrome in Adult Rheumatoid Arthritis Patients: Current Perspectives and Clinical Implications
Authors Santos-Moreno P , Rodríguez-Vargas GS, Martínez S, Ibatá L, Rojas-Villarraga A
Received 8 August 2022
Accepted for publication 12 October 2022
Published 4 November 2022 Volume 2022:14 Pages 255—267
DOI https://doi.org/10.2147/OARRR.S285407
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Chuan-Ju Liu
Pedro Santos-Moreno,1 Gabriel-Santiago Rodríguez-Vargas,1 Susan Martínez,2 Linda Ibatá,2 Adriana Rojas-Villarraga3
1Rheumatology, Biomab IPS, Bogotá, Colombia; 2Epidemiology, Epithink Health Consulting, Bogotá, Colombia; 3Research Institute, Fundación Universitaria de Ciencias de la Salud–FUCS, Bogotá, Colombia
Correspondence: Pedro Santos-Moreno, Rheumatology, Biomab IPS, Calle 48 # 13-86, Bogotá, Colombia, Tel +57 320 8094232, Email [email protected]
Aim: Rheumatoid arthritis is a prevalent worldwide disease, associated with an increased risk of multiple metabolic abnormalities that generate a higher disease burden.
Objective: To gather the available evidence on the epidemiology, pathophysiology, current perspectives, clinical implications and prognosis of metabolic abnormalities in patients with rheumatoid arthritis.
Methods: This is a narrative literature review. Search was conducted in PubMed, OVID, and Taylor & Francis databases, using the following MeSH terms: “Arthritis Rheumatoid”, “Metabolic Diseases”, and “Metabolic Syndrome”.
Results: This study describes the main metabolic manifestations of rheumatoid arthritis. Research has recognized that rheumatoid arthritis and metabolic abnormalities share pathophysiological mechanisms with an additive effect that increases cardiovascular risk. In that context, appropriate antirheumatic treatment can also impact on cardiovascular risk.
Conclusion: There are metabolic abnormalities in rheumatoid arthritis patients that increase cardiovascular risk. Therefore, it is crucial to evaluate cardiovascular risk to provide appropriate comprehensive management to reduce morbidity and mortality in patients with this disease.
Keywords: rheumatoid arthritis, metabolic diseases, cardiovascular diseases, metabolic syndrome
Introduction
Rheumatoid arthritis (RA) is a systemic autoimmune disease—affecting 5 out of every 1000 peopl—with a female predominance and an increased incidence in people over 60 years old.1 This disease is characterized by arthralgia—which is disabling in some cases—morning stiffness, and joint swelling.2 Also, there is extra-articular involvement in other systems such as cardiovascular, respiratory, renal, and ophthalmic.3 Besides the disease burden, these patients have an increased risk of developing metabolic abnormalities, such as diabetes mellitus (DM), arterial hypertension (AH), osteoporosis (OP), and arteriosclerosis. These alterations lead to a significant increase in cardiovascular risk (CVR),4 mortality, and disability.5 Although there is an increase in last decades regarding research in this topic, there is still a gap to close in order to impact CVR and to analyze the metabolic pathways abnormalities present in RA patients.6 This review aims to gather the available evidence on the epidemiology, pathophysiology, current perspectives, clinical implications and prognosis of metabolic abnormalities in patients with rheumatoid arthritis.
Methods
This is narrative literature review. Search for documents was conducted in the following databases: PubMed, OVID, and Taylor & Francis, using the following MeSH terms: “Arthritis Rheumatoid”, “Metabolic Diseases”, and “Metabolic Syndrome.” Additional studies were sought from the reference list of certain primary studies and different reviews. We select the studies that were more relevant for the aim of the review.
Epidemiology
In 2010, the Global Burden of Disease study found that RA had a global prevalence of 0.25%, discriminated by sex with 0.35% for women and 0.13% for men. Besides, it was ranked as the 42nd cause of global disability,7 demonstrating the high impact of RA on the disease burden worldwide. Additionally, economic studies reflect the increased financial burden of RA: this disease generates costs of approximately $ 2408 to $ 83,845 per patient each year, including direct and indirect costs, such as medicines, hospitalization, and workplace absenteeism.8
Regarding metabolic alterations, patients with RA have a high prevalence of this type of comorbidities. For example, a cross-sectional and multicenter study conducted in 2014 by Dougados et al, which included 3920 patients from 17 countries, evaluated the prevalence of comorbidities in people with RA, and it found that 40.4% of the patients had AH, 31.7% had hypercholesterolemia, and 15% had DM.9 In another study conducted in Spain, patients with RA had a high prevalence of metabolic comorbidities. The most common were hypercholesterolemia in 45% of the population, AH in 41%, and DM in 12%.10 Thus, these metabolic comorbidities in RA patients present an increase in the burden of the disease, and in addition in CVR. The most common metabolic comorbidities in patients with RA are summarized in Table 1.
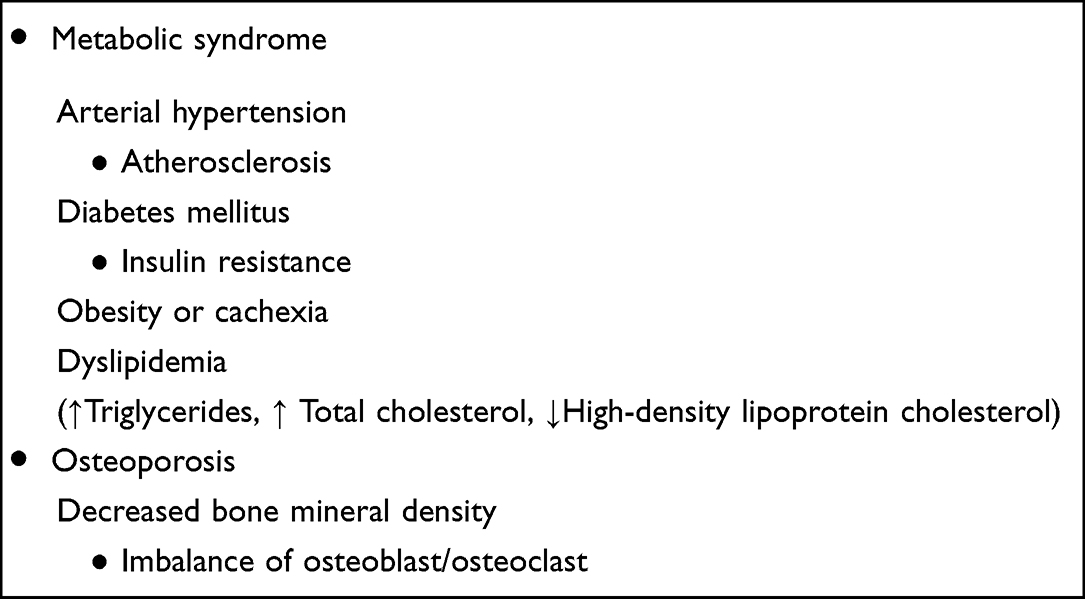 |
Table 1 Frequent Metabolic Abnormalities in Rheumatoid Arthritis |
Pathophysiology of Rheumatoid Arthritis
Alterations in the inflammatory response occur long before the symptom development. This period is known as pre-RA, where epigenetic and genetic interactions generate citrullination process.11 The organism's inability to recognize these new citrullinated products causes the activation of dendritic cells, triggering a co-stimulation between CD4+ and T cells. All this process ends with the production of autoantibodies: rheumatoid factor and anti-citrullinated protein antibody (ACPA) are the most common.12
Environmental factors, for instance pollution, generate reactive oxygen species that activate pro-inflammatory factors, such as nuclear factor kappa B (NF-kB). This activation produces inflammatory cascades where tumor necrosis factor (TNF), IL-1, and IL-6 play a fundamental role promoting joint swelling and bone erosion.13 This joint damage is caused by synovial macrophages and fibroblast-like synoviocytes activated by receptor activator ligand for NF-kB (RANKL), which are stimulated by IL-17, another pro-inflammatory interleukin present in this complex dysregulation of the immune system.14 Besides the osteoclastic activity generated by the immune system, other molecules, such as adipokines, exert a direct action by modifying the function of cells, such as fibroblasts and chondrocytes,15,16 and increasing IL-6 levels. Studies have shown adipokines are increased in RA patients; therefore, they have been proposed as a marker of the disease.17
Common Risk Factors
It has been observed that RA and metabolic alterations share risk factors that could lead to metabolic syndrome (AH, DM, hypertriglyceridemia, central obesity) or OP. In addition, environmental factors such as exposure to tobacco,11 obesity, high sodium intake, and pollution have been remarked as possible causes of RA and metabolic abnormalities.18 These shared factors lead to positive feedback between metabolic alterations and RA, where inflammation is the principal factor. It is known that obesity, DM, and AH are pathologies that generate pro-inflammatory states, leading to the activation of metabolic and immune pathways, accelerating RA.19
Pathophysiological Pathways Present in Rheumatoid Arthritis and Metabolic Alterations
RA and metabolic alterations, such as OP and insulin resistance, have shown common pathophysiological pathways that converge in a CVR increase.20 The insulin resistance in patients with RA has an estimated prevalence of 51% for recently diagnosed RA and 58% for long-standing RA. These figures are higher than the 19% presented in the general population.21 The main factors involved in the pathophysiological process of insulin resistance are TNF, IL-1, and IL-6.22 These cytokines interfere with insulin since decreasing the tyrosine phosphorylation that leads to produce negative feedback on this hormone.21 Leptin increases cardiovascular risk in RA patients due to its pro-inflammatory cytokine function.23 A study in 77 patients with RA showed a significant relationship between high leptin values and disease activity (p=0.047), obesity (p=0.038), positive rheumatoid factor (p=0.009), tobacco (p=0.009), and metabolic syndrome (p=0.001). A remarkable finding was the low levels of leptin were related to the consumption of hydroxychloroquine (p=0.023),24 because it opens the door to new research about the anti-inflammatory effect of hydroxychloroquine.
Another factor that contributes to increased CVR in RA is a process known as “inflammaging”, this term was introduced in the year 2000 as a chronic inflammation that develops with age,25 which leads to alterations in DNA repair and elimination of cellular debris, and translates into endothelial dysfunction and loss of elasticity in the arterial walls.26 It is important to note that microvascular dysfunction, aging, and metabolic disorders, together with inflammation and oxidative stress,27 occur as a consequence of inflammaging and the chronic inflammation exposure.
In addition, immunosenescence, defined as an increase in inflammation and a deterioration in the immune system, leads to tissue dysfunction and an increased risk of metabolic disease,28 processes that also occur with the inflammatory pattern of RA, which is similar to “inflammaging”. It has also been described that aged adipose tissue, similar to tissue undergoing persistent chronic inflammation as occurs in RA, suffers changes in many subsets of innate and adaptive immune cells, revealing a complex interplay that contributes to inflammation, increased senescence, impaired catecholamine-induced lipolysis, and altered insulin sensitivity.28
The development of atherosclerosis has been demonstrated in metabolic syndrome and RA, where chronic inflammation leads to the oxidation of low-density lipoproteins. So, when this process is associated with low levels of antioxidant enzymes, such as paraoxonase-1, it causes a propensity for atheromas.29 A remarkable event after initiating anti-inflammatory treatment is a rise in cholesterol levels, called the “lipid paradox”. However, this phenomenon has not been related to increased mortality rates.30
On the other hand, the alteration of bone structure has two components, local and systemic bone loss31; in both, factors such as TNF, IL-6, IL-1, and RANKL decrease osteoblastogenesis and increase osteoclastogenesis.32 The cortical bone suffers a more significant alteration than the trabecular bone, being the distal radius and femoral neck the most affected.33 Also, ACPA developed during the disease process stimulates osteoclasts, leading to increased inflammation and bone structure loss. Therefore, these antibodies have been defined as a marker of severe disease.34
Finally, another important event that converges between RA and metabolic syndrome is obesity. The development of hormones, such as adipokines, especially adiponectin,15 has activity over cartilage, immune cells, and the synovial membrane in patients with obesity35 (Figure 1).
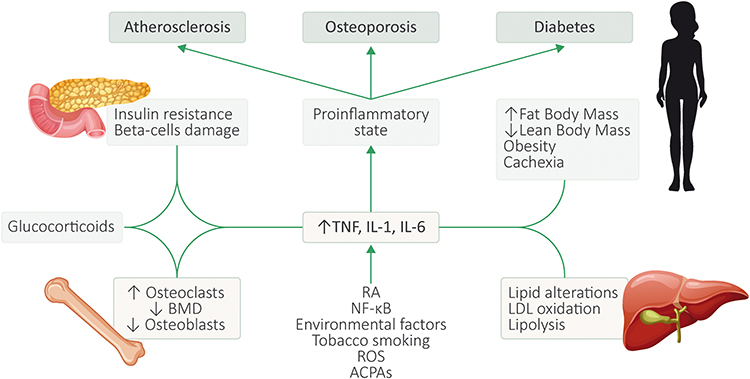 |
Figure 1 Common pathophysiological pathways between rheumatoid arthritis and metabolic disorders. Abbreviations: Source, self-made; TNF, tumor necrosis factor; IL-1, interleukin 1; IL-6, interleukin 6; BMD, bone mineral density; RA, rheumatoid arthritis; NF-kB, nuclear factor kappa B; ROS, reactive oxygen species; ACPAs, anti-citrullinated protein autoantibodies; LDL, low-density lipoproteins. |
Rheumatoid Arthritis and Metabolic Syndrome
Metabolic syndrome is a group of clinical findings including abdominal obesity, high blood glucose, triglycerides, decreased low-density lipoproteins, and AH.36,37 Its prevalence in 2009 was almost 30% in the general population. Also, the Framingham study found that patients diagnosed with metabolic syndrome had an age-adjusted relative risk (RR) of cardiovascular disease (CVD) of 2.88 for men and 2.25 for women.38
As mentioned above, all these factors generate an additive effect that causes RA patients to have a higher incidence and prevalence of metabolic syndrome. Some studies suggest that the incidence of metabolic syndrome in RA, is up to 13%.37 Another study found that the prevalence was 32% in patients with RA and 14% in patients without RA. Also, women were more affected than men, and, between these two groups, it found significant differences in body mass index (p=0.039), pain, rheumatoid factor positivity, high C-reactive protein and erythrocyte sedimentation rate.39
CVD is one of the leading causes of disability worldwide, contributing 24% of the total number of years lived with disability of all chronic noncommunicable diseases.5 Unhealthy lifestyle habits, such as high sodium and unsaturated fats intake and sedentariness, explain this result.40 Furthermore, patients with RA have an increased risk of developing metabolic alterations and CVD as the disease progresses,41 related to the inflammatory pathways that generate a prone state to inflammation added to unhealthy lifestyles that turn out to be a risk factor for both pathologies.42
Patients diagnosed with RA and CVD have an increased risk of death,43 since the excess risk of morbidity and mortality due to CVD is 48% and 60%, respectively.44 The metabolic profile is atypical in these patients and depends on the stage of the disease. In the beginning, there are characteristic findings of metabolic syndrome, but over time, there are changes such as the “lipid paradox” and rheumatoid cachexia.4
The metabolic syndrome’s main alterations responsible for increasing CVR in patients with RA will be reviewed below.
- Diabetes Mellitus: This comorbidity is a fundamental part of the increase in CVR. The estimated prevalence of DM in these patients is between 15% and 19%.45 In fact, patients with RA have a relative risk of 1.43 developing DM (95% CI: 1.38–1.47).46 Adding DM as a CVR factor to patients already suffering from RA generates an increased risk of CVD (RR 1.94, 95% CI: 1.58, 2.30) compared to those without DM.44 The pathophysiological pathways shared by DM and RA are explained by the chronic inflammatory state, the use of medications such as steroids, and unhealthy lifestyle habits.45
- Changes in Body Mass Composition: Muscle, subcutaneous fat and visceral fat proportion are closely related to the stage and disease compromise. For example, high TNF, IL-6 levels and ACPA exist in highly active and therapy-resistant RA. These levels lead to rheumatoid cachexia, where there is an increase in fat content and a decrease in lean body mass.37 These changes have been paradoxically associated with an increased risk of mortality from cardiovascular etiology4 (Table 2).
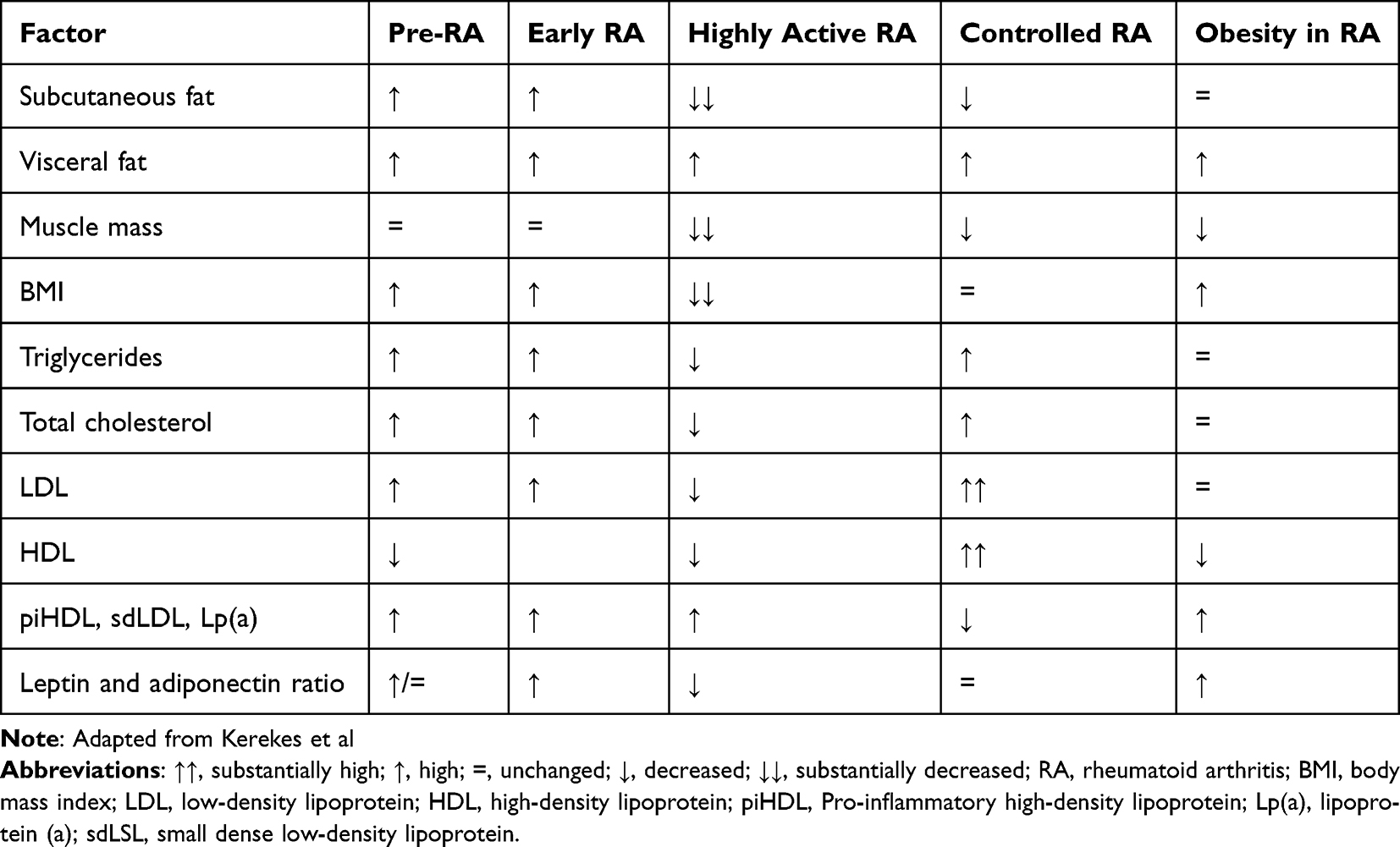 |
Table 2 Metabolic Profiles in Different Stages of Rheumatoid Arthritis |
Cardiovascular Risk
Despite that mortality figures from RA have improved, they are not entirely encouraging. A report carried out in 1953 showed excess mortality of 29% in patients with RA.47 In 2021, these data were still worrying and showed a higher mortality rate in RA patients than in the general population,48 and this mortality increase is due to CVR factors.49
The pathophysiological pathways in RA cause changes in the patient’s metabolism, and CVR increases when adding an unhealthy lifestyle. This risk is higher in patients with RA than in the general population, and it produces major events, such as ischemic heart disease, heart failure, cerebrovascular events, and peripheral artery diseases.10 Therefore, specialists (rheumatologists, cardiologists, endocrinologists) and general practitioners should implement interventions to reduce CVR in these patients, such as promoting a healthy lifestyle, choosing medicines with a dual effect (to impact RA and metabolic alterations), and performing a proper follow-up.50
Regarding lifestyle changes, a group of randomized clinical trials called “Plants for Joints” are being developed in patients diagnosed with RA, based on the fact that the type of diet and obesity may contribute to the disease. In these studies, researchers propose to study the effects of change in lifestyle in patients with RA or at risk of RA through a program based on guided exercise, stress management, and better nutrition.51 These studies are promising and will bring more evidence to justify a healthier lifestyle in RA patients.
Risk Stratification
An important part of the approach to patients with RA and metabolic disorders is the stratification of CVR, since this is used to make decisions on management and follow-up.52 As seen, RA is an independent risk factor for cardiovascular events, so these patients are a particular population when stratifying CVR. The most recent EULAR recommendations of 2016 continue the line of recommendations of 2009, by advising to multiply the result of the Systematic Coronary Risk Evaluation (SCORE) scale stratification by 1.5, in people with positive antibodies such as Rheumatoid Factor or ACPA, disease duration greater than 10 years or extra-articular manifestations,53 since, in some cases, the real risk presented by RA patients may be underestimated. In addition, for those patients with a moderate CVR, the use of non-invasive tools such as carotid ultrasound, which analyzes the thickness of the intima-media or ankle-arm index, looking for subclinical atherosclerosis, is recommended.54 In fact, disease activity has been significantly associated with high CVR in RA patients when reclassification was made by SCORE risk charts and carotid ultrasound.55 Ferraz-Amaro et al showed that in RA patients followed by 6 years, the moderate and severe disease activity levels were related to the early appearance of atherosclerotic plaque, measured by carotid ultrasound, evidencing subclinical endothelial injury depending on patients’ proinflammatory state.56 Although most guidelines do not contemplate the evaluation of the coronary artery calcium score in the search for subclinical atherosclerosis, recent studies show its benefit in patients with RA as a stratification tool.57 Regarding the control of metabolic comorbidities in these patients, the recommendations arise from studies done in the general population; therefore, the EULAR guidelines suggest focusing and managing CVR in these patients in the same way as is done in the population without RA53,58 and emphasis should be placed on the practice of physical exercise depending on the functional capacity of the person.59 Table 3 compiles the most important recommendations on CVR management involving the EULAR guidelines and additional scientific evidence.52
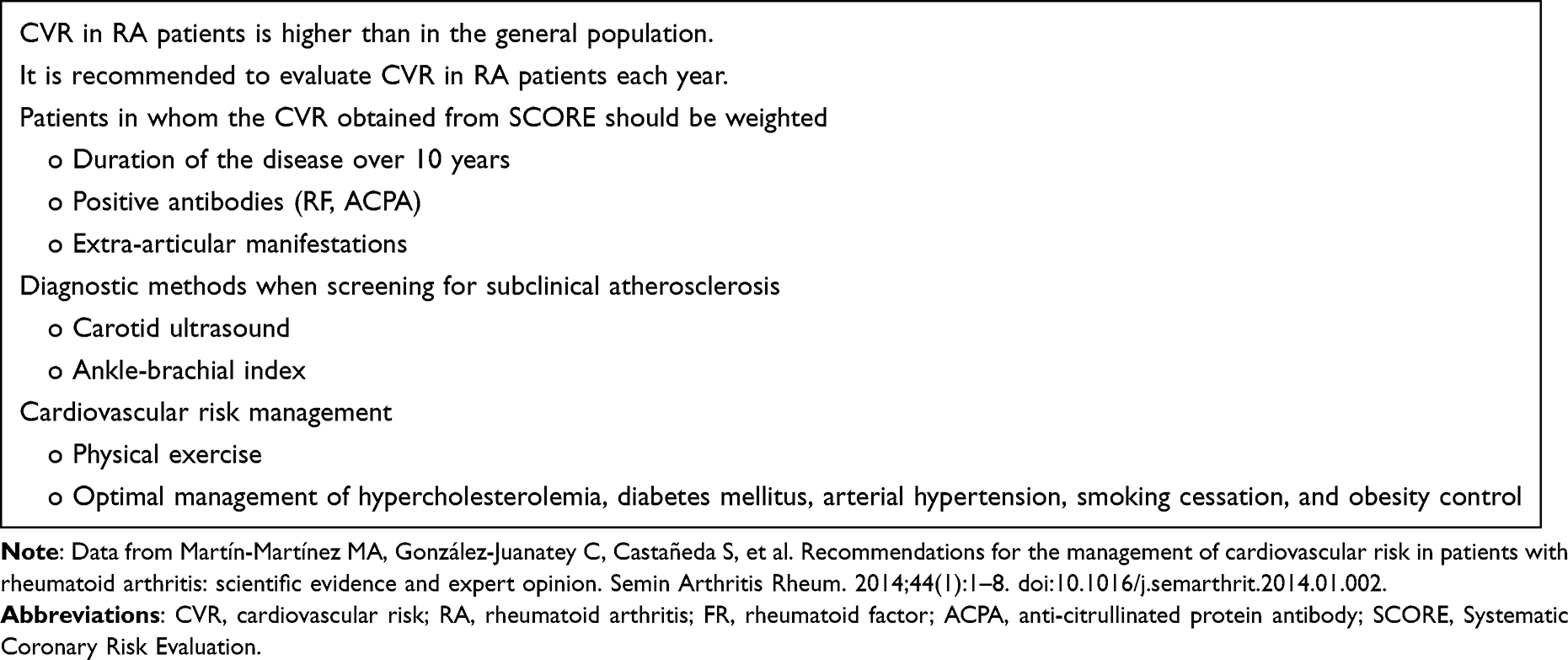 |
Table 3 Cardiovascular Risk Management in Rheumatoid Arthritis Patients |
Rheumatoid Arthritis and Osteoporosis
Alterations in bone composition have been strongly associated with RA,60 and research has shown that the development of OP in RA patients is partly caused by the pro-inflammatory state related to RA and the chronic use of some medications.61 These factors lead to an imbalance between the action of osteoblasts and osteoclasts that damages the bone structure.61 Therefore, RA patients who develop OP have an increased risk of fragility fractures and increased mortality.62
Many RA patients will develop OP throughout the disease.31 A study found that OP had a prevalence of 38.6%,63 and another study showed a prevalence of almost 30%. The incidence partly depended on the medication used; for instance, patients who took glucocorticoids had an incidence of 7.5 cases per 1000 person-years.31
Several risk factors for developing OP and fractures are recognized, and they can be classified them as disease and treatment factors. These are described below:
- ACPA: These antibodies have been proposed as active factors in bone degeneration, mainly in early RA.64 This hypothesis has not been confirmed conclusively because some studies have found that, although there is more significant compromise in bone mineral density (BMD) in patients with positive antibodies in early RA, there are no long-term differences in bone involvement compared to patients who have negative antibodies.65
- Activity of the Disease: The degree of RA activity is associated with more significant inflammatory alteration, producing high levels of inflammatory cytokines. For example, TNF and IL-6 share an osteoclast-activating effect, like ACPA.66 Likewise, several investigations have found an association between high levels of cytokines and lower BMD.67 The progression of bone loss could decrease by inhibiting these cytokines’ activity. This hypothesis has been tested in different studies, where biological therapies block TNF and IL-6 action and reduce bone loss, directly impacting the development of fractures.68
- Glucocorticoids: These medicines were crucial in managing RA before disease-modifying antirheumatic drugs (csDMARDs) and biological disease-modifying antirheumatic drugs (bDMARDs). Glucocorticoids alter bone structure by promoting osteoclastic activity associated with low BMD.69
Fractures in RA Patients
There is an increased risk of fractures in RA patients, which is even higher in patients under glucocorticoid treatment; this condition is known as glucocorticoid-induced OP.69 A meta-analysis explored the effects of systemic glucocorticoid therapy on bone health in RA patients. 46,711 glucocorticoid-treated RA subjects and 857 healthy controls were included. Lumbar BMD (− 0.038 g/cm2; [95% CI, −0.052, − 0.024]) and femoral neck BMD (− 0.017 g/cm2; [− 0.030, − 0.003]; 43.90%) was lower in patients receiving glucocorticoid management compared to patients without this medicine. The BMD-lowering effect was also associated with the daily dose administered, because patients receiving a dose of 5–10 mg had lower BMD than those receiving less than 5 mg. Additionally, vertebral fracture in this group of patients had a prevalence of 13.0% in RA patients treated with glucocorticoids.63
In another study, the incidence of general and fragility fractures in RA patients was 33.00 (95% CI: 18.39 to 59.21) and 15.31 (95% CI: 10.43 to 22.47) per 1000 person-years, respectively.70 Besides, it was reported that patients with RA had an increased risk of general (RR 1.52, 95% CI: 1.07–2.14) and fragility fractures (RR 1.61, 95% CI: 1.44–1.79). Fractures directly impact RA patients’ mortality since these patients have more years lived with disability, less physiological reserve, fragility, and immobility syndrome.71
Medicines Commonly Used in Rheumatoid Arthritis and Their Impact on Metabolic Comorbidities
At the beginning of the pharmacological management of RA, two essential premises must be considered: 1) csDMARD or bDMARDs management impacts the disease’s activity and reduces CVR. 2) The use of medicines that increase CVR should be avoided. The following is a short review of medicines indicated for patients with RA. We will see that some have dual effects that benefit the disease and comorbidities.72 However, some have beneficial effects on the disease but detrimental effects on metabolic abnormalities.73
Non-Steroidal Anti-Inflammatory Drugs
These medicines are used as adjuvants in acute episodes in RA patients’ pain management and have been related to an increase in CVR.73 Several studies have demonstrated their direct relationship with increased CVR,74 mainly due to AH and the development of thrombotic events, since cyclooxygenase inhibition increases coronary events mediated by thrombotic phenomena.75
Glucocorticoids
Although widely used in patients with RA, glucocorticoids have multiple side effects in the long term, including insulin resistance, because they increase hepatic gluconeogenesis and decrease insulin sensitivity in the muscle and liver.75,76 In some cases, they can lead to DM.74 Therefore, using the lowest effective doses in the shortest time possible is recommended. Metabolic effects, including dyslipidemia and AH, are linked to the use of doses higher than 7 mg. Although this dosage should be administered in RA for acute control of inflammatory status, assessing metabolic risk is critical when used chronically.74
Antimalarial Drugs, Conventional Synthetic DMARDs, and Small Molecules
Hydroxychloroquine
Hydroxychloroquine improves insulin resistance. In addition, regarding the risk of developing DM, a long-term study with a large sample of patients found a reduction in the development of DM (HR: 0.62; CI 95%: 0.42–0.92) with a dose–response effect.77 Furthermore, the RA patients’ follow-up has shown that these drugs significantly reduce glycated hemoglobin levels by more than 50%.78 Besides, it impacts fat metabolism, improving the lipid panel, specifically total cholesterol and low-density lipoprotein levels.77
Methotrexate
It seems methotrexate positively affects CVR by reducing metabolic syndrome risk and blood glucose levels. A study found it is a protective factor in reducing blood sugar in RA patients (OR: 0.517; 95% CI: 0.33–0.81; P=0.004).79 A meta-analysis found methotrexate is a protective factor (RR 0.48) for developing DM in RA patients under this treatment when compared with patients that did not take this medicine.44 In addition, this medicine decreases the development of CVD by more than 20%.80 A recently published study found that patients on methotrexate treatment had a lower vascular age than those who were not receiving this treatment.81 These results suggest benefits in reducing cardiovascular risk in these patients. Furthermore, a recent meta-analysis showed that methotrexate significantly reduced mortality in RA patients (HR: 0.59, 95% CI: 0.50–0.71, P < 0.001). Also, its use was independently associated with a decrease in CVD mortality (HR: 0.72, 95% CI: 0.53–0.97, P = 0.031).82
Leflunomide
Safety data about leflunomide are inconclusive. Some guidelines do not recommend it as a first line in patients with coexisting AH because it could cause a decrease in artery distensibility with the consequent blood pressure increase.83 Remarkably, some studies are contradictory. For instance, the study by Rho et al showed that although leflunomide does not significantly impact CVR reduction in patients with RA, it decreases glucose levels.84 On the other hand, the study by Naranjo et al showed that prolonged exposure to leflunomide (HR: 0.59; 95% CI: 0.43–0.79) was associated with a reduced risk of cardiovascular morbidity. Also, the potential benefit of decreasing CVR in patients receiving this medicine along with TNF-α inhibitors has been mentioned.85
Sulfasalazine
It works as an inhibitor of NF-kB, leading to suppression in the production of TNF-α.86 A decrease in CVR has been observed when using this drug in the long term, unrelated to AH, DM, and hypercholesterolemia. These effects are the same when used with other drugs.83
Janus Kinase Inhibitors
They act on JAK-1, which activates pro-inflammatory cytokines, such as IL-6.87 It has been observed that this pharmacological group alters the lipid profile; however, no long-term studies assess if these alterations increase CVR.88 Besides, it has been suggested that its action can generate weight gain in people receiving these medicines. Nevertheless, it has also been considered potential management for obesity. However, the information is not conclusive.87
However, a recent clinical trial compared outcomes in RA patients receiving combined doses of tofacitinib with patients under a TNF-α inhibitor in a population with high CVR. Thus, it found that the risks of major adverse cardiovascular events and cancer were higher with tofacitinib and did not meet the non-inferiority criteria. As a result, FDA (Food and Drug Administration) issued a safety statement, saying that patients receiving this treatment should be adequately stratified.89
Biologic DMARDs (bDMARDs)
Substantial evidence was found about the possible beneficial effects of bDMARDs in patients with autoimmune rheumatic diseases, specifically RA. It seems that bDMARDs, some more than others, alter the lipid profile in RA patients but do not negatively affect, in most cases, the total cholesterol/HDL ratio. Additionally, favorable effects on arterial stiffness and endothelial function were observed. These effects are related to a lower risk of cardiovascular events, which can be seen in observational studies of RA patients treated with bDMARDs. Noteworthy, more data is available about TNF-α inhibitors than other bDMARDs, such as tocilizumab, abatacept, and rituximab.90
Tocilizumab (Anti-IL-6)
Its mechanism of action focuses on the inhibition of IL-6. Initially, some trials found alteration in the lipid profile, mainly an increase in LDL cholesterol91; however, the IL-6 pathway is strongly implicated with the development of atherogenesis, so meta-analyses of randomized controlled trials have shown a decrease in major cardiovascular events in patients in whom tocilizumab is administered.92 Indeed, in a recent network meta-analysis, tocilizumab was shown to have safe cardiovascular outcomes compared with other bDMARDs.93 Moreover, although the mentioned increase in LDL cholesterol has been demonstrated, an increase in HDL cholesterol efflux capacity, as well as a reduction in lipoprotein (Lp)(a) serum concentration levels, has been found in RA patients under long-term treatment with tocilizumab.94
Anti-TNF Biologics
Research has shown that using these drugs in refractory diseases decreases overall and cardiovascular mortality because they appear to halt the progression of atherosclerosis by impacting endothelial function. In addition, recent studies have shown beneficial effects on the development of insulin resistance and DM.21
Remarkably, TNF-α inhibitors can inhibit receptors like TNFR2 more than TNFR1. TNFR2 is primarily a cardioprotective receptor and its increased inhibition results in cardiovascular morbidity associated with TNF-α inhibitors. That is why they have been involved in deteriorating patients with heart failure.95 However, other studies have shown that anti-TNF therapy reduces subclinical myocardial inflammation and improves cardiovascular function in patients with rheumatic diseases, including RA.96 Additionally, it has been demonstrated that TNF-α blocking agents may be related to reduced risk of cardiovascular events compared to non-biological DMARDs.97
Abatacept
It is a selective modulator of co-stimulation (selective CD80 and CD86 ligand) that interferes with the immune activity of T cells. Regarding glucose metabolism, recently, it has been reviewed the preclinical evidence supporting a possible role of T lymphocytes in insulin resistance in RA and how abatacept might improve glucose metabolism by suppressing infiltrating cells from adipose tissue.98 From a cardiovascular point of view, a study evaluated the incidence of CVD from 1998 to 2017, involving 18,754 patients with RA. It is shown that the use of abatacept and anti-TNF was related to a decrease in CVR compared to csDMARDs.72
On the other hand, a cohort in Taiwan evaluated 1584 RA patients who did not respond to anti-TNF, and it showed that those who received second-line tocilizumab or abatacept had better results in preventing cardiovascular events compared to those who received rituximab.99 Additionally, another study evaluated more than 10,000 RA patients from a North American registry, and it was found that abatacept contributed to a 20% risk reduction of CVD compared to anti-TNF.100 Furthermore, a study sought to assess the impact of BMI and the efficacy and retention of abatacept during 6 months in RA patients who had not received any biological treatment. It was found that BMI does not affect clinical response or abatacept retention.101
Rituximab
Rituximab is a monoclonal antibody that binds to the CD20 antigen to interfere with B lymphocyte function. A study evaluated RA patients treated with rituximab showed a significant increase in the outflow capacity of high-density lipoprotein cholesterol at 52 follow-up weeks.102 Another study evaluated 55 women with RA, reporting that rituximab treatment potently suppresses systemic inflammation, improves the lipid profile and atherogenicity index of plasma, decreases carotid intima-media thickening, and improves the elastic properties of arteries in RA patients without cardiovascular disease.103 Additionally, another study evaluated 20 RA patients after 6 months of receiving rituximab treatment, and it found an improvement in macrovascular and microvascular endothelial function and a reduction of systemic inflammation. However, there was a modest but significant increase in lipids (cholesterol and triglycerides).104 On the contrary, some published clinical cases showed that rituximab could induce cardiovascular events (which can be severe), usually in the first infusion but also in subsequent infusions. Although myocardial infarction remains a rare complication after rituximab infusion and often occurs in people with previous cardiovascular disease, it has been suggested that patients presenting clinical symptoms of ischemic heart disease should be closely analyzed to avoid such complications.105
Conclusion
Patients with RA have an increased risk of developing metabolic disorders, which represents an increased risk of both developing and dying from CVD. Research has recognized that both RA and metabolic disorders share pathophysiological mechanisms that have an additive effect that increases CVR. Additionally, some drugs used in the treatment of RA also increase the risk of CVD. In contrast, there are other drugs that could have a protective effect. There is evidence of some gaps in the staging of CVR in these patients, so new research is needed to clarify how to approach this risk and thus have a direct impact on mortality.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
PSM has received fees for conferences, counseling, advisory boards, and also travel to academic meetings expenses and research grants in last 5 years from AbbVie, Biopas-UCB, Bristol, Janssen, Lilly, Pfizer, Roche and Sanofi. The other authors declare that they have no known competing commercial, financial interests or personal relationships that could have appeared to influence the work reported in this manuscript.
References
1. Aletaha D, Smolen JS. Diagnosis and management of rheumatoid arthritis: a review. JAMA. 2018;320(13):1360–1372. doi:10.1001/jama.2018.13103
2. Sharif K, Sharif A, Jumah F, Oskouian R, Tubbs RS. Rheumatoid arthritis in review: clinical, anatomical, cellular and molecular points of view. Clin Anat. 2018;31(2):216–223. doi:10.1002/ca.22980
3. Sparks JA. Rheumatoid Arthritis. Ann Intern Med. 2019;170(1):ITC1–ITC16. doi:10.7326/AITC201901010
4. Kerekes G, Nurmohamed MT, González-Gay MA, et al. Rheumatoid arthritis and metabolic syndrome. Nat Rev Rheumatol. 2014;10(11):691–696. doi:10.1038/nrrheum.2014.121
5. Gheorghe A, Griffiths U, Murphy A, Legido-Quigley H, Lamptey P, Perel P. The economic burden of cardiovascular disease and hypertension in low- and middle-income countries: a systematic review. BMC Public Health. 2018;18(1):1–11. doi:10.1186/s12889-018-5806-x
6. Ladak K, Hashim J, Clifford-Rashotte M, Tandon V, Matsos M, Patel A. Cardiovascular risk management in rheumatoid arthritis: a large gap to close. Musculoskelet Care. 2018;16(1):152–157. doi:10.1002/msc.1196
7. Cross M, Smith E, Hoy D, et al. The global burden of rheumatoid arthritis: estimates from the Global Burden of Disease 2010 study. Ann Rheum Dis. 2014;73(7):1316–1322. doi:10.1136/annrheumdis-2013-204627
8. Hsieh PH, Wu O, Geue C, McIntosh E, McInnes IB, Siebert S. Economic burden of rheumatoid arthritis: a systematic review of literature in biologic era. Ann Rheum Dis. 2020;79(6):771–777. doi:10.1136/annrheumdis-2019-216243
9. Dougados M, Soubrier M, Antunez A, et al. Prevalence of comorbidities in rheumatoid arthritis and evaluation of their monitoring: results of an international, cross-sectional study (COMORA). Ann Rheum Dis. 2014;73(1):62–68. doi:10.1136/annrheumdis-2013-204223
10. Balsa A, Lojo-Oliveira L, Alperi-López M, et al. Prevalence of comorbidities in rheumatoid arthritis and evaluation of their monitoring in clinical practice: the Spanish cohort of the COMORA study. Reumatol Clin. 2019;15(2):102–108. doi:10.1016/j.reuma.2017.06.002
11. Radu AF, Bungau SG. Management of rheumatoid arthritis: an overview. Cells. 2021;10(11):2857. doi:10.3390/cells10112857
12. Scherer HU, Häupl T, Burmester GR. The etiology of rheumatoid arthritis. J Autoimmun. 2020;110:102400. doi:10.1016/j.jaut.2019.102400
13. Essouma M, Noubiap JJN. Is air pollution a risk factor for rheumatoid arthritis? J Inflamm. 2015;12(1). doi:10.1186/s12950-015-0092-1
14. Lundy SK, Sarkar S, Tesmer LA, Fox DA. Cells of the synovium in rheumatoid arthritis T lymphocytes. Arthritis Res Therapy. 2007;9(1):1–11. doi:10.1186/ar2104
15. Chen X, Lu J, Bao J, Guo J, Shi J, Wang Y. Adiponectin: a biomarker for rheumatoid arthritis? Cytokine Growth Factor Rev. 2013;24(1):83–89. doi:10.1016/j.cytogfr.2012.07.004
16. Lago R, Gomez R, Otero M, et al. A new player in cartilage homeostasis: adiponectin induces nitric oxide synthase type II and pro-inflammatory cytokines in chondrocytes. Osteoarthr Cartil. 2008;16(9):1101–1109. doi:10.1016/j.joca.2007.12.008
17. Young HR, Solus J, Sokka T, et al. Adipocytokines are associated with radiographic joint damage in rheumatoid arthritis. Arthritis Rheum. 2009;60(7):1906–1914. doi:10.1002/art.24626
18. Deane KD, Demoruelle MK, Kelmenson LB, Kuhn KA, Norris JM, Holers VM. Genetic and environmental risk factors for rheumatoid arthritis. Best Pract Res Clin Rheumatol. 2017;31(1):3–18. doi:10.1016/j.berh.2017.08.003
19. Liao KP. Cardiovascular disease in patients with rheumatoid arthritis. Trends Cardiovasc Med. 2017;27(2):136. doi:10.1016/j.tcm.2016.07.006
20. Lebovitz HE. Insulin resistance: definition and consequences. Experiment Clin Endocrinol Diabetes. 2001;109(SUPPL. 2):S135–S148.
21. Nicolau J, Lequerré T, Bacquet H, Vittecoq O. Rheumatoid arthritis, insulin resistance, and diabetes. Joint Bone Spine. 2017;84(4):411–416. doi:10.1016/j.jbspin.2016.09.001
22. Masuko K. Angiopoietin-like 4: a molecular link between insulin resistance and rheumatoid arthritis. J Orthop Res. 2017;35(5):939–943. doi:10.1002/jor.23507
23. Vadacca M, Margiotta DPE, Navarini L, Afeltra A. Leptin in immuno-rheumatological diseases. Cell Mol Immunol. 2011;8(3):203–212. doi:10.1038/cmi.2010.75
24. Batún-Garrido JADJ, Salas-Magaña M, Juárez-Rojop IE. Association between leptin and IL-6 concentrations with cardiovascular risk in patients with rheumatoid arthritis. Clin Rheumatol. 2017;37(3):631–637. doi:10.1007/s10067-017-3897-x
25. Franceschi C, Garagnani P, Parini P, Giuliani C, Santoro A. Inflammaging: a new immune–metabolic viewpoint for age-related diseases. Nat Rev Endocrinol. 2018;14(10):576–590. doi:10.1038/s41574-018-0059-4
26. Santos-Moreno P, Burgos-Angulo G, Martinez-Ceballos MA, et al. Review: inflammaging as a link between autoimmunity and cardiovascular disease: the case of rheumatoid arthritis. RMD Open. 2021;7(1):1470.
27. Mengozzi A, Pugliese NR, Chiriacò M, Masi S, Virdis A, Taddei S. Microvascular ageing links metabolic disease to age-related disorders: the role of oxidative stress and inflammation in promoting microvascular dysfunction. J Cardiovasc Pharmacol. 2021;78:S78–87. doi:10.1097/FJC.0000000000001109
28. Dahlquist KJV, Camell CD. Aging leukocytes and the inflammatory microenvironment of the adipose tissue. Diabetes. 2022;71(1):23–30. doi:10.2337/dbi21-0013
29. Charles-Schoeman C, Lee YY, Grijalva V, et al. Cholesterol efflux by high density lipoproteins is impaired in patients with active rheumatoid arthritis. Ann Rheum Dis. 2012;71(7):1157–1162. doi:10.1136/annrheumdis-2011-200493
30. González-Gay MA, González-Juanatey C. Inflammation and lipid profile in rheumatoid arthritis: bridging an apparent paradox. Ann Rheum Dis. 2014;73(7):1281–1284. doi:10.1136/annrheumdis-2013-204933
31. Adami G, Saag KG. Osteoporosis pathophysiology, epidemiology, and screening in rheumatoid arthritis. Curr Rheumatol Rep. 2019;21(7). doi:10.1007/s11926-019-0836-7
32. Takayanagi H. New developments in osteoimmunology. Nat Rev Rheumatol. 2012;8(11):684–689. doi:10.1038/nrrheum.2012.167
33. Haugeberg G, Uhlig T, Falch JA, Halse JI, Kvien TK. Bone mineral density and frequency of osteoporosis in female patients with rheumatoid arthritis. Results from 394 patients in the Oslo County Rheumatoid Arthritis Register. Arthritis Rheum. 2000;43(3):522–530. doi:10.1002/1529-0131(200003)43:3<522::AID-ANR7>3.0.CO;2-Y
34. Hauser B, Riches PL, Wilson JF, Horne AE, Ralston SH. Prevalence and clinical prediction of osteoporosis in a contemporary cohort of patients with rheumatoid arthritis. Rheumatology. 2014;53(10):1759–1766. doi:10.1093/rheumatology/keu162
35. Gómez R, Conde J, Scotece M, Gómez-Reino JJ, Lago F, Gualillo O. What’s new in our understanding of the role of adipokines in rheumatic diseases? Nat Rev Rheumatol. 2011;7(9):528–536. doi:10.1038/nrrheum.2011.107
36. Samson SL, Garber AJ. Metabolic Syndrome. Endocrinol Metab Clin North Am. 2014;43(1):1–23. doi:10.1016/j.ecl.2013.09.009
37. Ferraz-Amaro I, González-Juanatey C, López-Mejias R, Riancho-Zarrabeitia L, González-Gay MA. Metabolic syndrome in rheumatoid arthritis. Mediators Inflamm. 2013;2013:e710928. doi:10.1155/2013/710928
38. Wilson PWF, D’Agostino RB, Parise H, Sullivan L, Meigs JB. Metabolic syndrome as a precursor of cardiovascular disease and type 2 diabetes mellitus. Circulation. 2005;112(20):3066–3072. doi:10.1161/CIRCULATIONAHA.105.539528
39. Burli AP, Dave M. Demographic profile and prevalence of metabolic syndrome among patients with rheumatoid arthritis and its correlation with disease activity. J Assoc Physicians India. 2022;70(4):11–12.
40. Francula-Zaninovic S, Nola IA. Management of measurable variable cardiovascular disease’ risk factors. Curr Cardiol Rev. 2018;14(3):153–163. doi:10.2174/1573403X14666180222102312
41. Romano S, Salustri E, Ruscitti P, Carubbi F, Penco M, Giacomelli R. Cardiovascular and metabolic comorbidities in rheumatoid arthritis. Curr Rheumatol Rep. 2018;20(12). doi:10.1007/s11926-018-0790-9
42. Gremese E, Ferraccioli G. The metabolic syndrome: the crossroads between rheumatoid arthritis and cardiovascular risk. Autoimmun Rev. 2011;10(10):582–589. doi:10.1016/j.autrev.2011.04.018
43. Kašperová S, Tarabčáková L, Kašperová B, Šteňová EK. Rheumatoid arthritis and metabolic disorders. Vnitr Lek. 2021;67(E–2):18–24. doi:10.36290/vnl.2021.029
44. Baghdadi LR. Correction: effect of methotrexate use on the development of type 2 diabetes in rheumatoid arthritis patients: a systematic review and meta-analysis. PLoS One. 2020;15(12):e0243960–e0243960. doi:10.1371/journal.pone.0243960
45. Liu XZ, Gao Y, Fan J, et al. Metabolic abnormalities in rheumatoid arthritis patients with comorbid diabetes mellitus. Clin Rheumatol. 2017;37(1):219–226. doi:10.1007/s10067-017-3847-7
46. Jiang P, Li H, Li X. Diabetes mellitus risk factors in rheumatoid arthritis: a systematic review and meta-analysis. Clin Exp Rheumatol. 2015;33(1):115–121.
47. Cobb S, Anderson F, Bauer W. Length of life and cause of death in rheumatoid arthritis. N Engl J Med. 1953;249(14):553–556. doi:10.1056/NEJM195310012491402
48. Lee YK, Ahn GY, Lee J, et al. Excess mortality persists in patients with rheumatoid arthritis. Int J Rheum Dis. 2021;24(3):364–372. doi:10.1111/1756-185X.14058
49. Gabriel SE. Cardiovascular morbidity and mortality in rheumatoid arthritis. Am J Med. 2008;121(10):S9–S14. doi:10.1016/j.amjmed.2008.06.011
50. Bartels CM, Saucier JM, Thorpe CT, et al. Monitoring diabetes in patients with and without rheumatoid arthritis: a Medicare study. Arthritis Res Ther. 2012;14(4):R166. doi:10.1186/ar3915
51. Walrabenstein W, van der Leeden M, Weijs P, et al. The effect of a multidisciplinary lifestyle program for patients with rheumatoid arthritis, an increased risk for rheumatoid arthritis or with metabolic syndrome-associated osteoarthritis: the “Plants for Joints” randomized controlled trial protocol. Trials. 2021;22(1):1–11. doi:10.1186/s13063-021-05682-y
52. Martín-Martínez MA, González-Juanatey C, Castañeda S, et al. Recommendations for the management of cardiovascular risk in patients with rheumatoid arthritis: scientific evidence and expert opinion. Semin Arthritis Rheum. 2014;44(1):1–8. doi:10.1016/j.semarthrit.2014.01.002
53. Agca R, Heslinga SC, Rollefstad S, et al. EULAR recommendations for cardiovascular disease risk management in patients with rheumatoid arthritis and other forms of inflammatory joint disorders: 2015/2016 update. Ann Rheum Dis. 2017;76(1):17–28. doi:10.1136/annrheumdis-2016-209775
54. Smolen JS, Landewé RB, Bijlsma JW, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2019 update. Ann Rheum Dis. 2020;79(6):685–699. doi:10.1136/annrheumdis-2019-216655
55. Ferraz-Amaro I, Corrales A, Quevedo-Abeledo JC, et al. Disease activity influences the reclassification of rheumatoid arthritis into very high cardiovascular risk. Arthritis Res Ther. 2021;23(1):162. doi:10.1186/s13075-021-02542-7
56. Ferraz-Amaro I, Corrales A, Atienza-Mateo B, et al. Moderate and high disease activity predicts the development of carotid plaque in rheumatoid arthritis patients without classic cardiovascular risk factors: six years follow-up study. J Clin Med. 2021;10(21):4975. doi:10.3390/jcm10214975
57. Martínez-Ceballos MA, Sinning Rey JC, Alzate-Granados JP, et al. Coronary calcium in autoimmune diseases: a systematic literature review and meta-analysis. Atherosclerosis. 2021;335:68–76. doi:10.1016/j.atherosclerosis.2021.09.017
58. Perk J, De Backer G, Gohlke H, et al. European Guidelines on cardiovascular disease prevention in clinical practice (version 2012) The Fifth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of nine societies and by invited experts) Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur Heart J. 2012;33(13):1635–1701. doi:10.1093/eurheartj/ehs092
59. Metsios GS, Stavropoulos-Kalinoglou A, van Zanten JJCSV, et al. Rheumatoid arthritis, cardiovascular disease and physical exercise: a systematic review. Rheumatology. 2008;47(3):239–248. doi:10.1093/rheumatology/kem260
60. Raterman HG, Bultink IE, Lems WF. Osteoporosis in patients with rheumatoid arthritis: an update in epidemiology, pathogenesis, and fracture prevention. Expert Opin Pharmacother. 2020;21(14):1725–1737. doi:10.1080/14656566.2020.1787381
61. Hu Z, Zhang L, Lin Z, et al. Prevalence and risk factors for bone loss in rheumatoid arthritis patients from South China: modeled by three methods. BMC Musculoskelet Disord. 2021;22(1):1–9. doi:10.1186/s12891-021-04403-5
62. Wysham KD, Baker JF, Shoback DM. Osteoporosis and fractures in rheumatoid arthritis. Curr Opin Rheumatol. 2021;33(3):270–276. doi:10.1097/BOR.0000000000000789
63. Wang Y, Zhao R, Gu Z, Dong C, Guo G, Li L. Effects of glucocorticoids on osteoporosis in rheumatoid arthritis: a systematic review and meta-analysis. Osteoporos Int. 2020;31(8):1401–1409. doi:10.1007/s00198-020-05360-w
64. Harre U, Georgess D, Bang H, et al. Induction of osteoclastogenesis and bone loss by human autoantibodies against citrullinated vimentin. J Clin Invest. 2012;122(5):1791–1802. doi:10.1172/JCI60975
65. Amkreutz JAMP, de Moel EC, Theander L, et al. Association between bone mineral density and autoantibodies in patients with rheumatoid arthritis. Arthritis Rheumatol. 2021;73(6):921–930. doi:10.1002/art.41623
66. Auréal M, Machuca-Gayet I, Coury F. Rheumatoid arthritis in the view of osteoimmunology. Biomolecules. 2020;11(1):1–18. doi:10.3390/biom11010048
67. Book C, Karlsson M, Åkesson K, Jacobsson L. Disease activity and disability but probably not glucocorticoid treatment predicts loss in bone mineral density in women with early rheumatoid arthritis. Scand J Rheumatol. 2008;37(4):248–254. doi:10.1080/03009740801998747
68. Zerbini CAF, Clark P, Mendez-Sanchez L, et al. Biologic therapies and bone loss in rheumatoid arthritis. Osteoporos Int. 2017;28(2):429–446. doi:10.1007/s00198-016-3769-2
69. Adami G, Saag KG. Glucocorticoid-induced osteoporosis update. Curr Opin Rheumatol. 2019;31(4):388–393. doi:10.1097/BOR.0000000000000608
70. Jin S, Hsieh E, Peng L, et al. Incidence of fractures among patients with rheumatoid arthritis: a systematic review and meta-analysis. Osteoporos Int. 2018;29(6):1263–1275. doi:10.1007/s00198-018-4473-1
71. Lin YC, Li YH, Chang CH, et al. Rheumatoid arthritis patients with Hip fracture: a nationwide study. Osteoporos Int. 2014;26(2):811–817. doi:10.1007/s00198-014-2968-y
72. Ozen G, Pedro S, Michaud K. The risk of cardiovascular events associated with disease-modifying antirheumatic drugs in rheumatoid arthritis. J Rheumatol. 2020;48(5):648–655. doi:10.3899/jrheum.200265
73. Braun J, Baraliakos X, Westhoff T. Nonsteroidal anti-inflammatory drugs and cardiovascular risk - a matter of indication. Semin Arthritis Rheum. 2020;50(2):285–288. doi:10.1016/j.semarthrit.2019.07.012
74. Atzeni F, Rodríguez-Carrio J, Popa CD, Nurmohamed MT, Szűcs G, Szekanecz Z. Cardiovascular effects of approved drugs for rheumatoid arthritis. Nat Rev Rheumatol. 2021;17(5):270–290. doi:10.1038/s41584-021-00593-3
75. Halacoglu J, Shea LA. Cardiovascular risk assessment and therapeutic implications in rheumatoid arthritis. J Cardiovasc Transl Res. 2020;13(5):878–890. doi:10.1007/s12265-020-09964-9
76. Dessein PH, Joffe BI, Stanwix AE, Christian BF, Veller M. Glucocorticoids and insulin sensitivity in rheumatoid arthritis. J Rheumatol. 2004;31(5):867–874.
77. Solomon DH, Garg R, Lu B, et al. Effect of hydroxychloroquine on insulin sensitivity and lipid parameters in rheumatoid arthritis patients without diabetes mellitus: a randomized, blinded crossover trial. Arthritis Care Res. 2014;66(8):1246–1251. doi:10.1002/acr.22285
78. Rekedal LR, Massarotti E, Garg R, et al. Changes in glycosylated hemoglobin after initiation of hydroxychloroquine or methotrexate treatment in diabetes patients with rheumatic diseases. Arthritis Care Res. 2010;62(12):3569–3573. doi:10.1002/art.27703
79. Toms TE, Panoulas VF, John H, Douglas KMJ, Kitas GD. Methotrexate therapy associates with reduced prevalence of the metabolic syndrome in rheumatoid arthritis patients over the age of 60- more than just an anti-inflammatory effect? A cross sectional study. Arthritis Res Ther. 2009;11(4):1–10. doi:10.1186/ar2765
80. Micha R, Imamura F, Wyler Von Ballmoos M, et al. Systematic review and meta-analysis of methotrexate use and risk of cardiovascular disease. Am J Cardiol. 2011;108(9):1362–1370. doi:10.1016/j.amjcard.2011.06.054
81. Rodríguez-Vargas GS, Santos-Moreno P, Rubio-Rubio JA, et al. Vascular age, metabolic panel, cardiovascular risk and inflammaging in patients with rheumatoid arthritis compared with patients with osteoarthritis. Front Cardiovasc Med. 2022;9:1707.
82. Xu J, Xiao L, Zhu J, Qin Q, Fang Y, Zhang J. Methotrexate use reduces mortality risk in rheumatoid arthritis: a systematic review and meta-analysis of cohort studies. Semin Arthritis Rheum. 2022;55:152031. doi:10.1016/j.semarthrit.2022.152031
83. Giollo A, Bissell LA, Buch MH. Cardiovascular outcomes of patients with rheumatoid arthritis prescribed disease modifying anti-rheumatic drugs: a review. Expert Opin Drug Saf. 2018;17(7):697–708. doi:10.1080/14740338.2018.1483331
84. Rho YH, Oeser A, Chung CP, Milne GL, Stein CM. Drugs used in the treatment of rheumatoid arthritis: relationship between current use and cardiovascular risk factors. Arch Drug Inf. 2009;2(2):34–40. doi:10.1111/j.1753-5174.2009.00019.x
85. Murdaca G, Spanò F, Puppo F. Use of leflunomide plus TNF-α inhibitors in rheumatoid arthritis. Expert Opinion Drug Safety. 2013;12(6):801–804. doi:10.1517/14740338.2013.823947
86. Wahl C, Liptay S, Adler G, Schmid RM. Sulfasalazine: a potent and specific inhibitor of nuclear factor kappa B. J Clin Invest. 1998;101(5):1163. doi:10.1172/JCI992
87. Harrington R, Al Nokhatha SA, Conway R. JAK inhibitors in rheumatoid arthritis: an evidence-based review on the emerging clinical data. J Inflamm Res. 2020;13:519. doi:10.2147/JIR.S219586
88. Clarke B, Yates M, Adas M, Bechman K, Galloway J. The safety of JAK-1 inhibitors. Rheumatology. 2021;60(Suppl2):ii24–ii24. doi:10.1093/rheumatology/keaa895
89. Ytterberg SR, Bhatt DL, Mikuls TR, et al. Cardiovascular and cancer risk with tofacitinib in rheumatoid arthritis. N Engl J Med. 2022;386(4):316–326. doi:10.1056/NEJMoa2109927
90. Fragoulis GE, Soulaidopoulos S, Sfikakis PP, Dimitroulas T, Kitas GD. Effect of biologics on cardiovascular inflammation: mechanistic insights and risk reduction. J Inflamm Res. 2021;14:1915. doi:10.2147/JIR.S282691
91. Schiff MH, Kremer JM, Jahreis A, Vernon E, Isaacs JD, van Vollenhoven RF. Integrated safety in tocilizumab clinical trials. Arthritis Res Ther. 2011;13(5):R141. doi:10.1186/ar3455
92. Singh S, Fumery M, Singh AG, et al. Comparative risk of cardiovascular events with biologic and synthetic disease-modifying antirheumatic drugs in patients with rheumatoid arthritis: a systematic review and meta-analysis. Arthritis Care Res. 2020;72:561. doi:10.1002/acr.23875
93. Castagné B, Viprey M, Martin J, Schott AM, Cucherat M, Soubrier M. Cardiovascular safety of tocilizumab: a systematic review and network meta-analysis. PLoS One. 2019;14(8):e0220178–e0220178. doi:10.1371/journal.pone.0220178
94. Ferraz-Amaro I, Hernández-Hernández MV, Tejera-Segura B, et al. Effect of IL-6 receptor blockade on proprotein convertase Subtilisin/Kexin type-9 and cholesterol efflux capacity in rheumatoid arthritis patients. Horm Metab Res. 2019;51(3):200–209. doi:10.1055/a-0833-4627
95. Hussain A, Tarahomi T, Singh L, Bollampally M, Heydari-Kamjani M, Kesselman MM. Cardiovascular risk associated with TNF alpha inhibitor use in patients with rheumatoid arthritis. Cureus. 2021;13(9):e17938.
96. Ntusi NAB, Francis JM, Sever E, et al. Anti-TNF modulation reduces myocardial inflammation and improves cardiovascular function in systemic rheumatic diseases. Int J Cardiol. 2018;270:253–259. doi:10.1016/j.ijcard.2018.06.099
97. Solomon DH, Curtis JR, Saag KG, et al. Cardiovascular risk in rheumatoid arthritis: comparing TNF-α blockade with nonbiologic DMARDs. Am J Med. 2013;126(8):730.e9–730.e17. doi:10.1016/j.amjmed.2013.02.016
98. Ursini F, Mauro D, Naty S, Gagliardi D, Grembiale RD. Improvement in insulin resistance after short-term treatment with Abatacept: case report and short review. Clin Rheumatol. 2012;31(9):1401–1402. doi:10.1007/s10067-012-2034-0
99. Hsieh MJ, Lee CH, Tsai ML, et al. Biologic agents reduce cardiovascular events in rheumatoid arthritis not responsive to tumour necrosis factor inhibitors: a national cohort study. Can J Cardiol. 2020;36(11):1739–1746. doi:10.1016/j.cjca.2020.01.003
100. Jin Y, Kang EH, Brill G, Desai RJ, Kim SC. Cardiovascular (CV) risk after initiation of abatacept versus TNF inhibitors in rheumatoid arthritis patients with and without baseline CV disease. J Rheumatol. 2018;45(9):1240–1248. doi:10.3899/jrheum.170926
101. Mariette X, Alten R, Nüßlein HG, et al. The effect of body mass index on clinical response to Abatacept as a first-line biologic for rheumatoid arthritis: 6-month results from the 2-year, observational, prospective ACTION study. Joint Bone Spine. 2017;84(5):571–576. doi:10.1016/j.jbspin.2016.10.011
102. Cacciapaglia F, Perniola S, Venerito V, et al. The impact of biologic drugs on high-density lipoprotein cholesterol efflux capacity in rheumatoid arthritis patients. J Clin Rheumatol. 2022;28(1):E145–E149. doi:10.1097/RHU.0000000000001657
103. Novikova DS, Popkova TV, Lukina GV, et al. The effects of rituximab on lipids, arterial stiffness and carotid intima-media thickness in rheumatoid arthritis. J Korean Med Sci. 2016;31(2):202. doi:10.3346/jkms.2016.31.2.202
104. Hsue PY, Scherzer R, Grunfeld C, et al. Depletion of B-cells with rituximab improves endothelial function and reduces inflammation among individuals with rheumatoid arthritis. J Am Heart Assoc. 2014;3(5). doi:10.1161/JAHA.114.001267
105. Sharif K, Watad A, Bragazzi NL, et al. Anterior ST-elevation myocardial infarction induced by rituximab infusion: a case report and review of the literature. J Clin Pharm Ther. 2017;42(3):356–362. doi:10.1111/jcpt.12522
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.