")
Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 15
Mandibular Second Molars and Their Pathologies Related to the Position of the Mandibular Third Molar: A Radiographic Study
Authors Skitioui M , Jaoui D, Haj Khalaf L, Touré B
Received 20 June 2023
Accepted for publication 30 August 2023
Published 16 October 2023 Volume 2023:15 Pages 215—223
DOI https://doi.org/10.2147/CCIDE.S420765
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Mohamed Skitioui, Dounia Jaoui, Lauzan Haj Khalaf, Babacar Touré
Department of Conservative Dentistry and Endodontics, Faculty of Dental Medicine, College of Health Sciences, International University of Rabat, Rabat, Morocco
Correspondence: Mohamed Skitioui, Department of Conservative Dentistry and Endodontics, Faculty of Dental Medicine, College of Health Sciences, International University of Rabat, Rabat, Morocco, Email [email protected]
Objective: The aim of this study was to determine the prevalence of mandibular third molar malposition and its impact in relation to the lower second molar using panoramic radiography.
Methods and Materials: This was a cross-sectional descriptive study of 353 panoramic images of patients who visited the Dental Clinic of the International University of Rabat. Panoramic images were analyzed in order to determine the number of second molar pathologies associated with the positions of third molars. The following radiographic lesions on the second molar were recorded: caries, root resorption and distal alveolysis. The Chi-square test was used to assess the association between different variables.
Results: Of these 353 radiographies, 169 were males, ie, 48%, and 184 were females, ie, 52%. The age range was from 18 to 63 years. The prevalence of the impacted position of the lower third molar was noted in 60%. Distal caries on the second mandibular molar was present in 47.5% of instances having an impacted third molar. Caries was present in 65.5% of wisdom teeth in a normal position and was also present in 79.6% of the impacted teeth. This difference was statistically significant with p = 0.01. The angulation of the third molar is a factor of caries of the second molar: 58.56% of them were carious. Of all the teeth in association with an angulation, 72.03% showed distal alveolysis in the second molar. In addition, root resorption was found in 20.4% of second molars linked to a wisdom tooth in all angulation occurrences.
Conclusion: It has been noted that among the pathologies seen on the mandibular second molar, distal alveolysis accounts for the majority of cases (58%), followed by caries (47.5%) and root resorption (13.3%). This study illustrated the importance of performing Orthopantomogram X-rays at each new consultation in patients over the age of 18.
Keywords: impacted, partially-erupted, panoramic radiography, mandibular third molar, root resorption, caries, alveolysis, prevalence
Introduction
The mandibular third molar can undergo several accidents during its evolution, dominated by infectious accidents. Its pathological position creates both local and regional complications.1 By its pathological position and by the accidents of evolution, the third mandibular molar is the cause of the appearance of several pathologies at the level of the adjacent teeth. The second mandibular molar then experiences the onset of pathologies such as caries at the distal level, distal periodontal bone lysis as well as root resorption. The occurrence of these pathologies at the level of the lower second molar led us to want to carry out a study which would demonstrate their frequency by being associated with partially impacted or erupted wisdom teeth. To date, several studies have been conducted on the development of pathologies associated with mandibular third molars in different populations.2–4 One of the most common pathologies is the distal caries of the second molar, Chen et al conducted a study where they find an overall prevalence of 31.6% when it is related to the position of the mandibular third molar. In fact, distal caries was more severe when the mesial angulation of the third molar was between 16° and 75°.5 In Syed et al study, a total of 979 patients had impacted third molars. A prevalence of 39% of patients with impacted third molars had distal cervical caries in the second molar. Mesioangular impaction was the most important type.6 Another study was made by Dias et al to assess and compare second molar bone loss adjacent to impacted mandibular third molar and the outcomes showed that mesioangular and horizontal third molars had a statistically significant association with bone loss of the adjacent second molars (p < 0.05).7 In the other hand, Smailienė et al study showed that mesioangular and horizontal positions of third molars had the strongest association with external root resorption (50% and 84.2%, respectively). Nonetheless, impacted third molars in vertical and distoangular positions also tended to cause external root resorption (23.6% and 6.9%, respectively).8 However, few investigations have been carried out on the Moroccan population. The objective of this radiographic study was to evaluate the prevalence of second molar pathologies and their association to the position of the mandibular third molar.
Materials and Methods
This descriptive study was conducted cross-sectionally on panoramic radiographs of Moroccan subjects. Patients signed consent forms stating that their radiographs could only be used for educational and research purposes and that their identities would be kept anonymous. The International Faculty of Dental Medicine of Rabat – International University of Rabat’s Research Ethics Board gave its approval to the study, which was carried out in accordance with the Declaration of Helsinki (CUMD/FIMD 003/20/22/Approval/2019). The X-ray images were obtained at the dental clinic of the International University of Rabat. The image quality of the panoramic digital X-rays and traditional X-rays at the site supported the selection. The patients’ ages and sexes are listed in the radiographic record. The radiographs were carried out in accordance with radiography guidelines in accordance with the ICRP’s (the International Commission on Radiological Protection) recommendations, taking into account the safety of the subjects and the radiographic operators. An X-ray machine made by the company KAVO was used to take panoramic images. An experienced radiology technician followed the manufacturer’s instructions when taking the radiographs. Digital Imaging and Communications in Medicine, or DICOM format, was used to export the images. RADIANT®, a DICOM image reading software, was used to read the images and perform the morphometric analysis on a computer.
In this study, the inclusion criteria were as follows: Moroccan patients over the age of 18. The selected panoramic radiographies had to be of good quality and show mature lower third molars, ie, with complete root development. The patient’s date of birth and sex had to be recorded on the subject’s X-ray or on the patient’s chart. This information was noted and saved to an EXCEL file. Selected panoramic radiographies had to include both lower second and lower third molars. The left side was the preferred side, otherwise the right side. All images presenting artefacts of movements, anatomical and metallic superpositions incompatible with the reading of anatomical structures were not retained. Low-quality panoramic radiographies as well as those showing mandibular third molars with incomplete root formation were excluded from the study. The analysis of OPGs x-ray (Orthopantomograms x-ray) was to determinate prevalence of malpositions of the 3rd mandibular molar, the tilt angle of the 38 or 48 compared to 37 or 47, respectively, the pathologies associated with the 37 or 47 (cavities, radicular resorption, alveolysis) and to identify the pathologies of the 38 or 48.
The third molar was defined as partially impacted or partially erupted when it has partially broken through the gum tissue but still partially underlying. When an impacted tooth is clinically visible, which means partially erupted, its long axis is almost always angulated when compared with that of the neighboring teeth.9 Primarily, impacted mandibular third molars were identified in the OPG. Subsequently, the following radiographic lesions were recorded on the OPGs: caries in the impacted and the adjacent tooth, periodontal bone loss on the distal side of the mandibular second molar, and resorption of the root of the adjacent tooth.
The diagnosis of pathologies linked to partially impacted third molars in the mandible was made as follows: dental caries manifests as radiolucency that causes the enamel to lose its normal homogeneity, and as the lesion moves closer to the dentino-enamel junction (DEJ), the DEJ line loses continuity in the area. On the OPG, root resorption of the tooth next to the impacted third molar was clearly seen as a loss of material in the second molar’s root as a result of direct contact between the teeth. From the enamel-cement junction to the marginal bone level, a distance of over 5mm was used to quantify the periodontal bone loss of the second molar’s distal portion.
Two examiners analyzed the radiographies. To avoid any intra-examiner variability, calibration was first performed on 30 random x-rays. Reproducibility was calculated by reassessment of 15 selected panoramic radiographies out of 30 radiographies over a 10-day interval. Cohen’s kappa was calculated for the degree of inter-examiner and intra-examiner agreement. The computer tools of the RADIANT DICOM reader software Version 2021.1 evaluated the inclination angles of the third molar.
The factors looked at were the third molar’s computed angle of inclination with respect to the second molar, as well as its normal, impacted, or partially erupted anatomical position. Using the WINTER categorization,10 the angulation between the long axes of the neighboring second molar and the mandibular third molar was measured to determine the inclination angle as follows:
- Vertical position: 0° to 10°
- Mesioangular position: 11° to 79°
- Horizontal position: 80° to 100°
- Distoangular position: −11° to −79°
- Other: 111° to −80°
- Buccolingual position
The classification of unusual angulations such as “mesio-inverted”, “distortion-inverted” and “distortion-horizontal” were combined and designated as “other”.
OPG revealed cavities in either the third molar or the adjacent second. The distal alveolysis of the second molar was indicated by the presence of a radiolucent image replacing the lamina dura, initially radiopaque. Root resorption was objectified by the presence of a radiolucent image on the distal root of the second molar in relation to the crown of the embedded or impacted third molar.
Statistical Analysis
Software called JAMOVI was used to do the statistical analysis. Results for the quantitative variables were presented as means ± with standard deviation, while those for the qualitative variables were presented as counts and percentages. To evaluate the relationship between qualitative variables, the Chi-square test was applied. In order for the findings to be deemed statistically significant, the p-value had to be less than 5% (p < 0.05). Strong inter-examiner agreement was found, as evidenced by a 0.86 Cohen’s kappa coefficient. The reproducibility of examiner number 1 was almost perfect as well as that of the second examiner (pending thesis) with Kappa Cohen values of 0.9 and 0.85, respectively.
Results
A total of 353 panoramic radiographs of 184 (52%) women and 169 (48%) men were retained. The average age was 32.2 ± 9.87 years old. The minimum age was 18, and the maximum was 63. The most present age group was that of 26–35 years (38.5%, n = 134), then 18–25 years (31.5%, n = 112), followed 36–45-year old (18.1%, n = 64), then 46–55-year old (8.5%, n = 30) and finally 56–65-year old (3.7%, n = 13). According to the status of the mandibular third molar, 40% (n = 142) showed a normal position and 60% (n = 211) an impacted position. The impacted position of the mandibular third molar was as equal in women (n = 110) as in men (n = 101). There is no significant difference p = 0.99.
The mesio-angulation position was the most present (38.5%, n = 71) in the female sex, followed by the vertical position (32%, n = 59) then the disto-angulation (18.5%, n = 34), finally the horizontal position (11%, n = 20). In the other hand, the mesio-angulated position prevailed (46%, n = 78), then the vertical position (29%, n = 49), after the horizontal and disto-angulated position presenting the same percentage (12.5%, n = 21) (Table 1). There was no statistically significant difference between the relationship between angulation and patient sex p = 0.33.
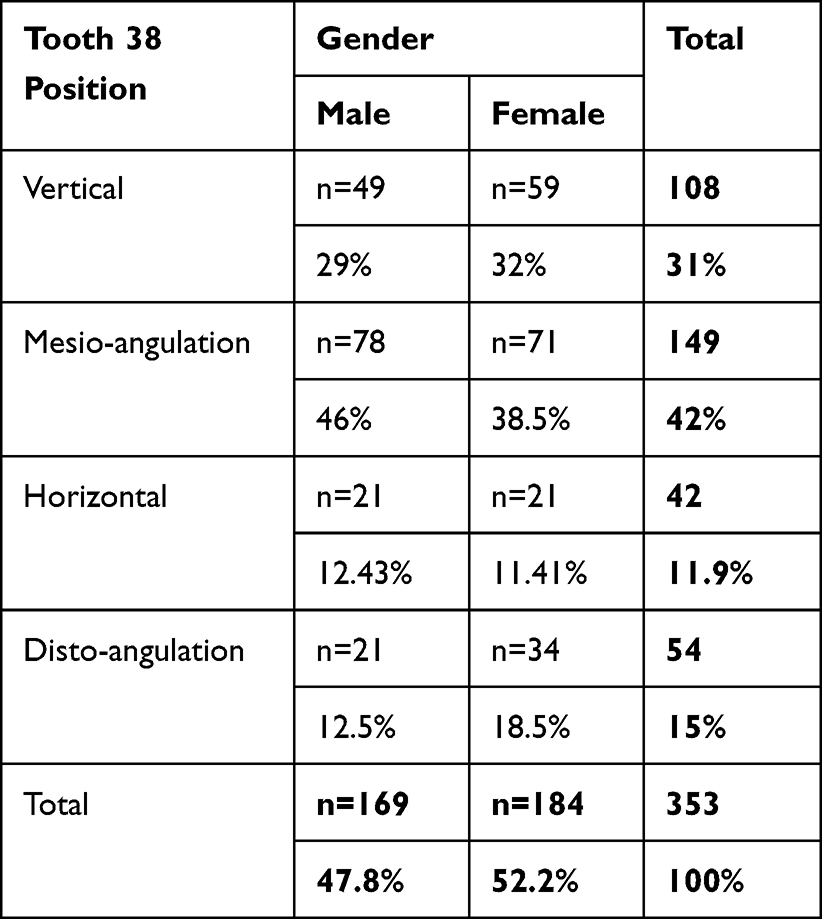 |
Table 1 Distribution of the Third Mandibular Molar Position According to Gender |
Caries on tooth 37 were more frequent if tooth 38 was in a partially impacted position compared to the normal position. Caries was present in 65.5% (n = 93) of all wisdom teeth in a normal position (n = 142) and was present in 79.6% (n = 168) of the 211 impacted teeth. This difference was statistically significant with p = 0.01. The presence of bone loss was associated with the position of the mandibular third molar. Alveolysis was more noted when the third molar was impacted in 97% of cases (n = 205), than when it presented a normal position in 37% of cases (n = 53). The difference was statistically significant with p < 0.01. Distal root resorption in the second mandibular molar was more important at the level of the partially impacted teeth with 20.37% of cases (n = 43) unlike teeth associated with a wisdom tooth in normal position with 2.8% (n = 4). The statistical difference was significant with p < 0.01 (Table 2).
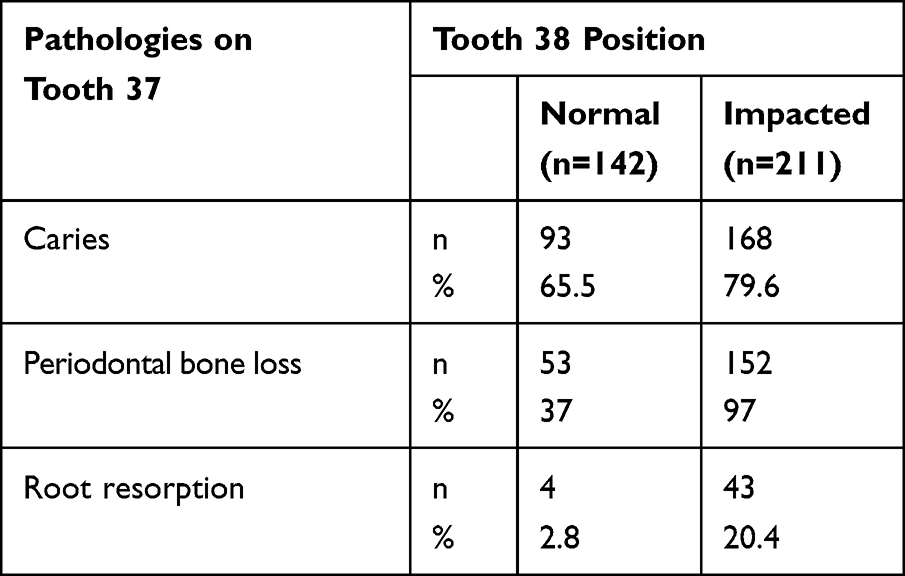 |
Table 2 Pathologies of the Mandibular Second Molar |
The presence of caries was detectable in all age groups: beyond 25 years, more than a third of the teeth were decayed. The highest caries percentage was in the age groups 26–35 years (62.5%) and 46–55 years (56.66%). Regarding bone lysis, a gradient according to age was observed. The older the patient, the higher the prevalence. It was 46.26% for 18–25-year old and 76.69% for 56–65-year old. For root resorption, analysis with age did not reveal any particularities. However, it was more frequent in younger patients (Table 3).
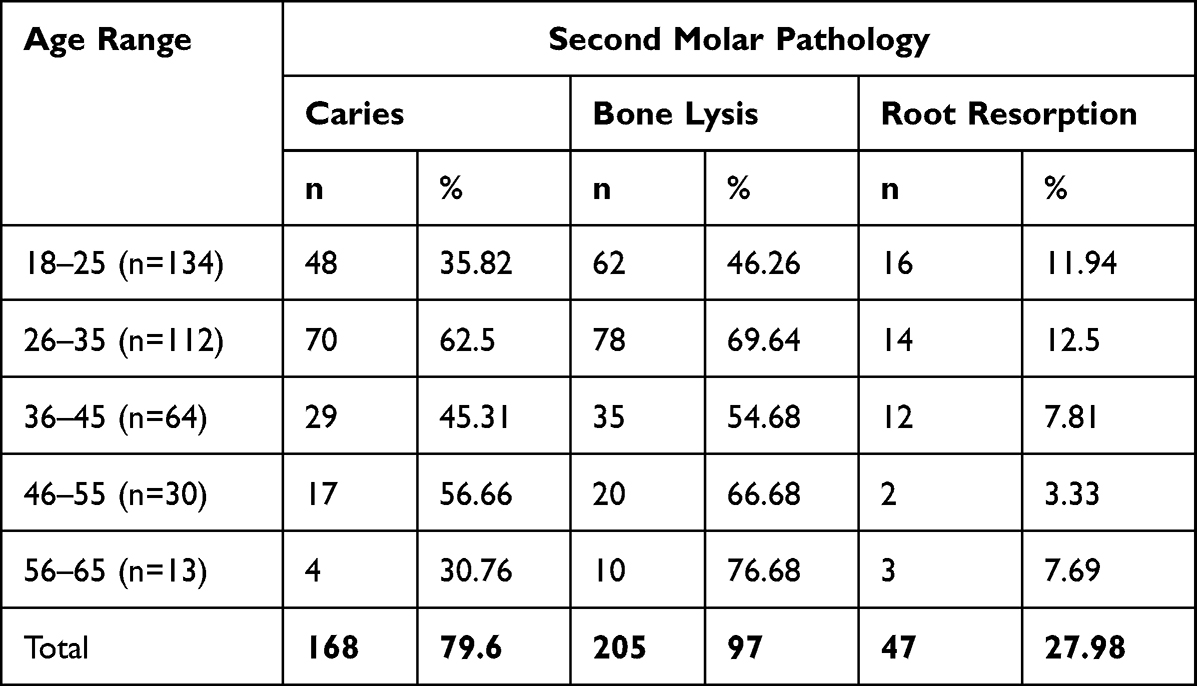 |
Table 3 The Distribution of Pathologies According to Age Groups |
Caries pathology was detected in 168 second molar: 90 in men (53.6%) and 78 in women (46.4%). Among the 168 decayed teeth, 100 are related to an impacted wisdom tooth and 68 are not related to it. Cavities in the mandibular second molar were most prevalent when it comes to teeth associated with a mesio-angulated third molar position: 58.5% (n = 65) of (n = 111), followed by those associated with teeth in a vertical position with 44.45% (n = 8) of cases (n = 18), then those in a horizontal position with 39% (n = 16) and finally those in disto-angulation with 26.82% (n = 11) of cases n = 41 (Table 4).
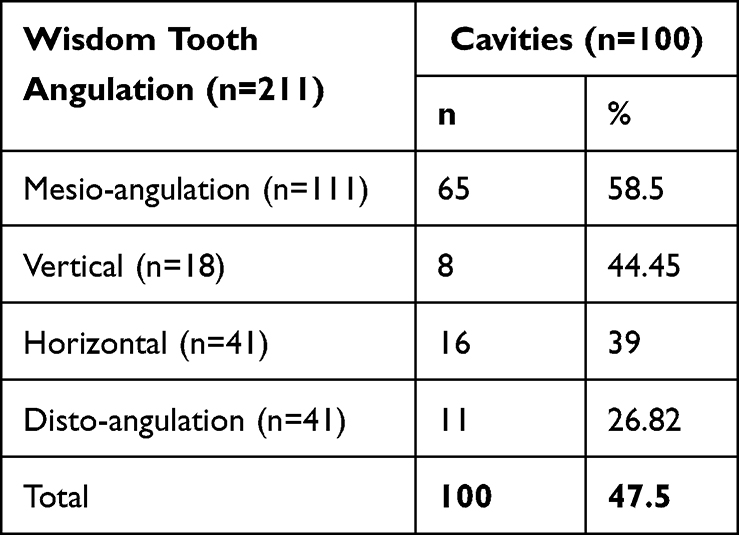 |
Table 4 Angulation of 38 and Presence of Caries on the Second Molar 37/47 |
Concerning distal alveolysis of the second mandibular molar, it was found in 58% (n = 205) of the entire sample (353): 49.8% (n = 102) were men and 50.2% (n = 103) women. This is the most important pathology among all the three studied. Alveolar bone lysis distal to 37 was noted in 72% (n = 152) of cases associated with the impacted third molar with a significant association p = 0.01. Mesio-angulation was strongly associated with distal alveolysis of second molars, with a p = 0.001. Teeth associated with a horizontal mandibular third molar presented the highest rate of distal periodontal alveolysis (87.8%), followed by the mesio angulated (85.6%) of the cases (n = 111) then the position vertical (55.5%) and finally the disto-angulated (26.8%) (Table 5).
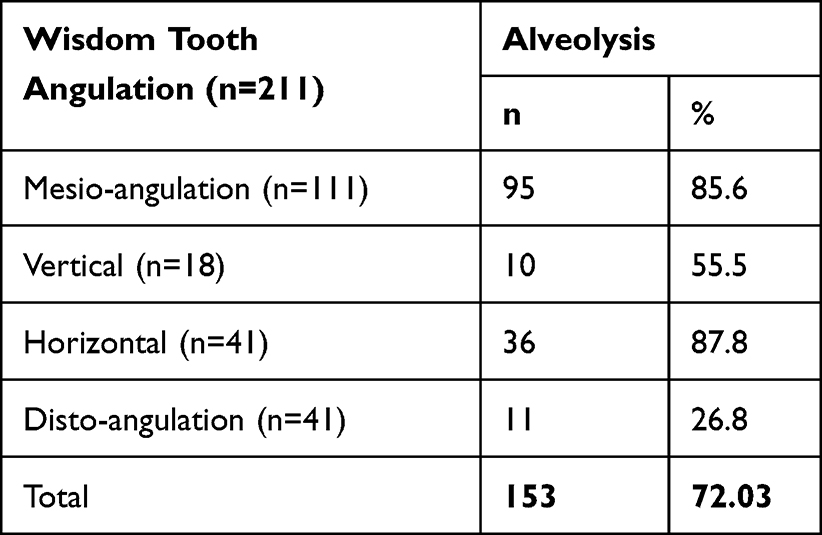 |
Table 5 Association Between the Angulation of 38 and Distal Bone Alveolysis of 37/47 |
Regarding root resorption of the second mandibular molar, it was found in 13% (n = 47 radiographs) of the entire sample (353), including 51% (n = 24) of men and 49% (n = 23) of women. This is the least common pathology in the second mandibular molars. Resorption was most observed in teeth with a horizontal position (36.5%), then teeth in the mesio angulation position (24.3%) and finally those in disto angulation (2.43%) (Table 6).
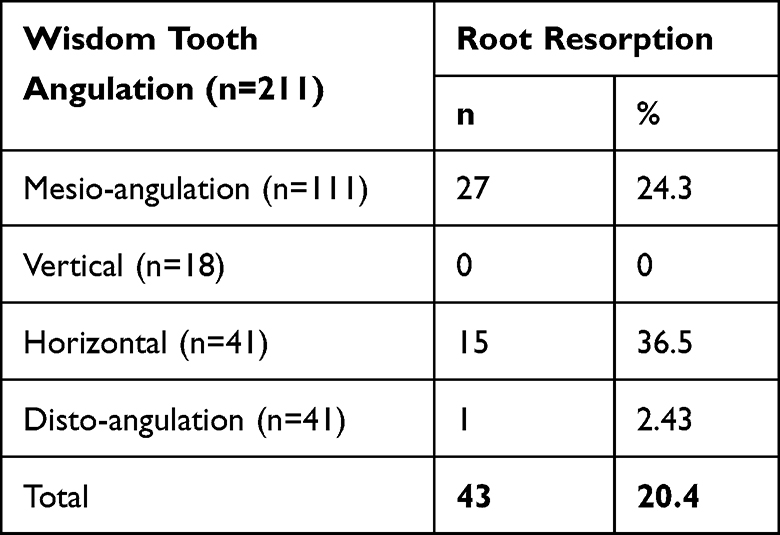 |
Table 6 Association Between the Angulation of 38 and the Presence of Root Resorption of 37/47 |
The most present pathological profile of the third mandibular molar was caries with 24% (n = 86) followed by cystic pathologies with 11% (n = 40 affected teeth) and finally tumor images in only 2 teeth or 0.5% (Table 7).
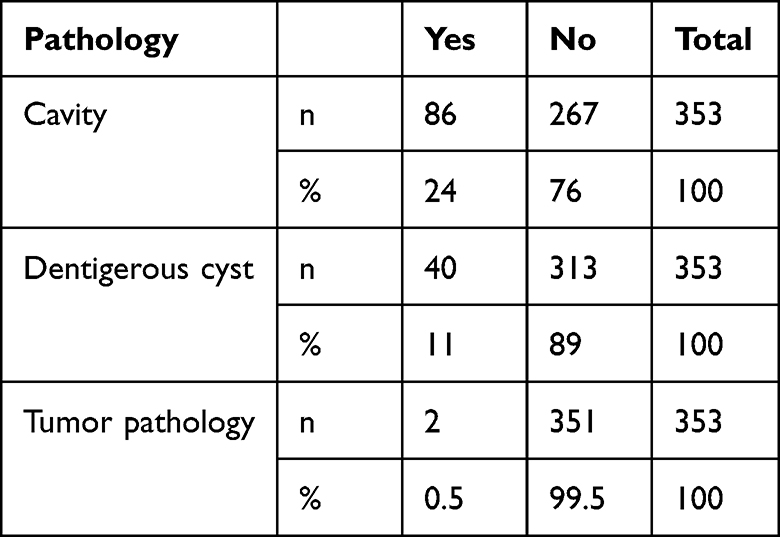 |
Table 7 Pathological Profile of the Mandibular Third Molar |
Discussion
This study demonstrated that the prevalence of partially impacted mandibular third molar was 60%. Impaction was as equal for both sexes. However, in Bjôrk et al study, they determined the prevalence of mandibular third molars in inclusion, enclavement (partially erupted) or non-evolution cases: The study was carried out on 237 Swedish male dental students with complete dental arches and ranging in age from 19 to 30 years old. The study showed that the frequency of impacted, retained or enclaved (partially erupted) mandibular third molars would be around 15 to 25% compared to all mandibular third molars as well as among all impacted, enclaved or retained teeth, the third mandibular molars represented between 55 and 60% of the cases.11
The study of the angulation of impacted or enclaved third molars according to the Winter scale showed that the mesio-angulated position was the most present with 46% of cases. According to Kaka et al,12 in mesio-angulation, the ectopic third molar is the most frequently encountered. This would be due to the eruption trajectory of the mandibular third molars. The wisdom tooth is slightly tilted mesially, due to the thickness of the bone distally and the straightening curve, this predominance of mesio-angulation can also be justified by a delay in development and maturation and the lack of space in old age.13 The results of this study were similar to data obtained from studies conducted in some countries as United States,14 China,15 Thailand and Spain,16 where the most common type was also mesio-angulation.
In this present study, 47.5% of radiographs showed caries in the distal of the mandibular second molar in cases associated with an impacted third molar. The angulation of the latter is also an aggravating factor of caries of the second molar: on 111 teeth in mesio-angulation, 65 were decayed. Moreover, in previous studies, the prevalence rate of distal caries on the second molar adjacent to an impacted mandibular third molar has been shown to range from 6% to 55%.2 In Chen et al study, the prevalence of distal caries in the adjacent second molar associated with the third molar was 31.6%,5 which was higher than that in some previous studies.17–20 This variability can be linked to cultural and socio-economic factors, but also to the age of the patient. Tooth angulation can also play a role in ratio differences. According to Altan et al,2 it was shown that 31.7% of the second molars were carious in the presence of a third molar in mesio angulation contrary to the vertical position of the third molar which represented only 5% of the totality. Based on Pepper et al study,21 The distal surfaces of 59/1414 (4.2%) mandibular second molars were carious. This was 4% greater when they were connected to a mandibular third molar that was partially erupted as opposed to one that was fully erupted or missing (29/414 (7%) vs 30/1000 (3%); p = 0.001). 22/133 mandibular second molars (16.5%) that were close to a mesioangularly impacted third molar had carious lesions in the distal side. Additionally, the third molar can be extracted to lower the incidence of caries in second molars that are accompanied by a partially erupted mesioangular mandibular third molar.21
The presence of mandibular wisdom teeth is a risk factor of alveolysis in the distal side of the second molar, this risk is much higher when it is angulated in a mesio position. Thus, we found 72.03% (n = 152) of mandibular second molars had distal alveolysis when it comes to a partially erupted third adjacent molar. The study by Blakey et al22 revealed that 25% of those with asymptomatic third molars have severe periodontal disease in the area of the third molars connected to the distal of second molars. According to Qu et al,23 whatever the conditions, the presence of the mandibular third molar is a risk factor for the appearance of periodontal pathologies in the second molar.
The recent studies revealed that in the case of third molar impaction, in more than 90% of cases, there was a contact between the crown of the impacted third molar and the adjacent second molar, and consequently, this may result in root resorption of the second molar.8 In this study, the impaction of the third molar caused root resorption in 13% of all cases. It was detected in 20.4% of mandibular second molars associated with a partially erupted wisdom tooth. This pathology was the most present in the second molars associated with the mandibular third molars in a mesio-angulated position. A study carried out at the Dental University of Kosovo showed that out of all the cases studied including maxillary and mandibular radiographic analysis, 23.7% of the cases, of which 18.4% at the mandibular level, presented a distal root resorption in the adjacent tooth. The results were much higher than the majority of other studies but are almost in line with the results we obtained.24 Besides, the study carried out by Chu et al in Hong Kong reported a percentage of 0.4% resorption present in all 3000 cases analyzed.25 Another study by van Der Linden et al reporting a prevalence of 0.9% of 2872 impacted third molars.26 Furthermore, in another study by Ahlqwits et al, among the 121 impacted molars studied, only one case of root resorption was observed.27 The variability of the results concerning the pathology analyzed can be explained by the diversity of the denomination given to the term bone resorption. In some studies, this has been defined as discontinuity and irregularity of the root surface while in others it has been more defined as a clear loss of root substance from the root.
Study Limitations
Low sensitivity of panoramic images to detect caries pathologies, root resorption and bone lysis were a real limitation during the study. The selection of X-rays was based on the use of digital panoramic radiographs instead of analog ones. That choice was supported by an almost 60% shorter exposure time when taking photos X-rays, as well as the possibility for the computer to save images. The storage of analog panoramic radiographs and the image quality, which is dependent on the chemical treatment of the film, had a great impact on the analysis of the radiographs and could affect the reproducibility of the results. Moreover, the absence of clinical information such as visual clinical examination, periodontal probing as well as the absence of clinical symptomatology formed a bias on the reliability of the data.
Conclusion
Assessing the prevalence of pathologies linked to partially erupted or impacted wisdom tooth in a specified population makes it possible to establish a model to compare various regions and populations of the world, thus facilitating procedures for the prevention and anticipation of such cases as well as accomplishing effective treatment.
By this study, it was able to highlight the pathologies of the mandibular second molar caused by the pathological position of the third molar as well as the importance of the panoramic radiographs in the detection of these and in the study of the relationship between the two adjacent molars.
Ethics Approval
The study was conducted following the Declaration of Helsinki and approved by the Research Ethics Board of the International Faculty of Dental Medicine of Rabat – International University of Rabat (Ref: CUMD/FIMD 003/20/22/Approval/2019).
Consent to Participate
Informed consent was obtained from each author.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Disclosure
The authors deny any conflicts of interest.
References
1. Peron JM. Accidents D’évolution Des Dents de Sagesse [Accidents of evolution of Wisdom Teeth]. Elsevier; 2004:147.
2. Altan A, Akbulut N. Does the angulation of an impacted mandibular third molar affect the prevalence of preoperative pathoses? J Dent. 2019;20(1):48–52. doi:10.30476/DENTJODS.2019.44563
3. Seigneuric JB, Denhez F, Andreani JF, Cantaloube D. Extraction des dents incluses: dents de sagesse. Med Chir. 1999;1999:1.
4. Vandeplas C, Vranckx M, Hekner D, Politis C, Jacobs R. Does retaining third molars result in the development of pathology over time? A systematic review. J Oral Maxillofac Surg. 2020;78(11):1892–1908. doi:10.1016/j.joms.2020.06.014
5. Chen Y, Zheng J, Li D, et al. Three-dimensional position of mandibular third molars and its association with distal caries in mandibular second molars: a cone beam computed tomographic study. Clin Oral Investig. 2020;24(9):3265–3273. doi:10.1007/s00784-020-03203-w
6. Syed KB, Alshahrani FS, Alabsi WS, et al. Prevalence of distal caries in mandibular second molar due to impacted third molar. J Clin Diagn Res. 2017;11(3):ZC28–ZC30. doi:10.7860/JCDR/2017/18582.9509
7. Dias MJ, Franco A, Junqueira JL, Fayad FT, Pereira PH, Oenning AC. Marginal bone loss in the second molar related to impacted mandibular third molars: comparison between panoramic images and cone beam computed tomography. Med Oral Patol Oral Cir Bucal. 2020;25(3):e395–e402. doi:10.4317/medoral.23443
8. Smailienė D, Trakinienė G, Beinorienė A, Tutlienė U. Relationship between the position of impacted third molars and external root resorption of adjacent second molars: a retrospective CBCT study. Medicina. 2019;55(6):305. doi:10.3390/medicina55060305
9. Peterson LJ, Miloro M. Peterson’s Principles of Oral and Maxillofacial Surgery. Springer; 2004.
10. Winter G. Impacted Mandibular Third Molars. St Louis: American Medical Book Co.; 1926.
11. Bjork A, Jensen E, Palling M. Mandibular growth and third molar impaction. Acta Odontol Scand. 1956;14:231–272.
12. Kaka L. Impacted mandibular third molar and the inferior alveolar canal in Iraqis (a radiographical study). Iraq. 2008;5(4):403.
13. Hashemipour MA, Tahmashi-Arashlow M, Fahimi-Hanzaaei F. Incidence of impacted mandibular and maxillary third molars: a radiographic study in a Southeast Iran population. Med Oral Pathol Oral Chir Buc. 2013;18(1):140–145. doi:10.4317/medoral.18028
14. Bui CH, Seldin EB, Dodson TB. Types, frequencies, and risk factors for complications after third molar extraction. J Oral Maxillofac Surg. 2003;61(12):1379–1389. doi:10.1016/j.joms.2003.04.001
15. Quek SL, Tay CK, Tay KH, Toh SL, Lim KC. Pattern of third molar impaction in a Singapore Chinese population: a retrospective radiographic survey. Int J Oral Maxillofac Surg. 2003;32(5):548–552. doi:10.1016/S0901-5027(03)90413-9
16. Chaparro-Avendaño AV, Pérez-García S, Valmaseda-Castellón E, Berini-Aytés L, Gay-Escoda C. Morbidity of third molar extraction in patients between 12 and 18 years of age. Med Oral Patol Oral Cir Bucal. 2005;10(5):422–431.
17. Chang SW, Shin SY, Kum KY, Hong J. Correlation study between distal caries in the mandibular second molar and the eruption status of the mandibular third molar in the Korean population. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108(6):838–843. doi:10.1016/j.tripleo.2009.07.025
18. Ozeç I, Hergüner Siso S, Taşdemir U, Ezirganli S, Göktolga G. Prevalence and factors affecting the formation of second molar distal caries in a Turkish population. Int J Oral Maxillofac Surg. 2009;38(12):1279–1282. doi:10.1016/j.ijom.2009.07.007
19. Falci SG, de Castro CR, Santos RC, et al. Association between the presence of a partially erupted mandibular third molar and the existence of caries in the distal of the second molars. Int J Oral Maxillofac Surg. 2012;41(10):1270–1274. doi:10.1016/j.ijom.2012.03.003
20. Marques J, Montserrat-Bosch M, Figueiredo R, Vilchez-Pérez M, Valmaseda-Castellón E, Gay-Escoda C. Impacted lower third molars and distal caries in the mandibular second molar. Is prophylactic removal of lower third molars justified? J Clin Exp Dent. 2017;9(6):e794–ee79. doi:10.4317/jced.53919
21. Pepper T, Grimshaw P, Konarzewski T, Combes J. Retrospective analysis of the prevalence and incidence of caries in the distal surface of mandibular second molars in British military personnel. Br J Oral Maxillofac Surg. 2017;55(2):160–163. doi:10.1016/j.bjoms.2016.10.009
22. Blakey GH, Marciani RD, Haug RH, et al. Periodontal pathology associated with asymptomatic third molars. J Oral Maxillofac Surg. 2002;60(11):1227–1233. doi:10.1053/joms.2002.35717
23. Qu HL, Tian BM, Li K, Zhou LN, Li ZB, Chen FM. Effect of asymptomatic visible third molars on periodontal health of adjacent second molars: a cross-sectional study. J Oral Maxillofac Surg. 2017;75(10):2048–2057. doi:10.1016/j.joms.2017.04.006
24. Sejfia Z, Koçani F, Macan D. Prevalence of pathologies associated with impacted third molars in Kosovo population: an orthopantomographic study. Acta Stomatal Croat. 2019;53(1):72–81. doi:10.15644/asc53/1/8
25. Chu F, Li T, Lui V, Newsome P, Chow R, Cheung L. Prevalence of impacted teeth and associated pathologies-A radiographic study of the Hong Kong Chinese population. Hong Kong Med J. 2003;9(3):158–163.
26. Van der Linden W, Cleaton-Jones P, Lownie M. Diseases and le- sions associated with third molars: review of 1001 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995;79(2):142–145.
27. Ahlqwits M, Grôndahl HG. Prevalence of impacted teeth and associated pathology in middle aged and older Swedish population. Community Dent Oral Epidemiol. 1991;19(2):116–119. doi:10.1111/j.1600-0528.1991.tb00124.x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.