")
Back to Journals » Substance Abuse and Rehabilitation » Volume 15
Managing Opioid Withdrawal Symptoms During the Fentanyl Crisis: A Review
Authors Weber AN , Trebach J , Brenner MA , Thomas MM, Bormann NL
Received 7 February 2024
Accepted for publication 5 April 2024
Published 10 April 2024 Volume 2024:15 Pages 59—71
DOI https://doi.org/10.2147/SAR.S433358
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rajendra D. Badgaiyan
Andrea Nicole Weber,1 Joshua Trebach,2 Marielle A Brenner,2 Mary Margaret Thomas,3 Nicholas L Bormann4
1Department of Psychiatry, University of Iowa, Iowa City, IA, USA; 2Department of Emergency Medicine, University of Iowa, Iowa City, IA, USA; 3Hardin Library for the Health Sciences, University of Iowa, Iowa City, IA, USA; 4Department of Psychiatry and Psychology, Mayo Clinic, Rochester, MN, USA
Correspondence: Andrea Nicole Weber, Department of Psychiatry, University of Iowa, 500 Newton Road, 1-308 MEB, Iowa City, IA, 52242, USA, Tel +1-319-335-6980, Fax +1-319-384-7467, Email [email protected]
Abstract: Illicitly manufactured fentanyl (IMF) is a significant contributor to the increasing rates of overdose-related deaths. Its high potency and lipophilicity can complicate opioid withdrawal syndromes (OWS) and the subsequent management of opioid use disorder (OUD). This scoping review aimed to collate the current OWS management of study populations seeking treatment for OWS and/or OUD directly from an unregulated opioid supply, such as IMF. Therefore, the focus was on therapeutic interventions published between January 2010 and November 2023, overlapping with the period of increasing IMF exposure. A health science librarian conducted a systematic search on November 13, 2023. A total of 426 studies were screened, and 173 studies were reviewed at the full-text level. Forty-nine studies met the inclusion criteria. Buprenorphine and naltrexone were included in most studies with the goal of transitioning to a long-acting injectable version. Various augmenting agents were tested (buspirone, memantine, suvorexant, gabapentin, and pregabalin); however, the liberal use of adjunctive medication and shortened timelines to initiation had the most consistently positive results. Outside of FDA-approved medications for OUD, lofexidine, gabapentin, and suvorexant have limited evidence for augmenting opioid agonist initiation. Trials often have low retention rates, particularly when opioid agonist washout is required. Neurostimulation strategies were promising; however, they were developed and studied early. Precipitated withdrawal is a concern; however, the rates were low and adequately mitigated or managed with low- or high-dose buprenorphine induction. Maintenance treatment continues to be superior to detoxification without continued management. Shorter induction protocols allow patients to initiate evidence-based treatment more quickly, reducing the use of illicit or non-prescribed substances.
Keywords: synthetic opioids, treatment, diagnosis, prevention, addiction medicine
Introduction
Despite policy changes targeting improved access and availability of opioid use disorder (OUD) treatment, opioid-related overdose deaths continue to increase in the United States. Between June 2022 and 2023, the Center for Disease Control and Prevention reported 106,661 drug overdose deaths, a 2.3% increase from the 12-months prior.1 Beginning around 2013, opioid overdose deaths previously associated with prescription opioids and heroin were superseded by deaths associated with non-methadone synthetic opioids, including illicitly manufactured fentanyl (IMF) and its analogues.2 IMF exposure can be unintentional at both the individual and systemic levels. Individuals may use stimulants or other opioids that unknowingly contain IMF.3 At a systemic level, contamination during the manufacturing or distribution process can increase exposure risk over large geographic areas.3 Fentanyl’s high potency and lipophilicity can complicate opioid withdrawal syndromes (OWS) and OUD management, which increases the urgency for more effective and accessible OWS treatments.4
Current State of Opioid Withdrawal
The endogenous opioid receptor system consists of four primary G-protein coupled receptors, including mu, delta, kappa, and opioid receptor-like 1.5 Opioid receptors exist throughout the nervous system and are expressed by most major organs.6 Both endogenous and exogenous ligands interact with these receptors. The effect of receptor agonism is a function of ligand, receptor type, and location.7 The opioid system is required for normal reward- and aversion-based learning. When compromised, the integration of reward and pain aversion information is impaired, as observed in OUD.
Exogenous opioid potency has been positively correlated with mu-opioid receptor desensitization and cyclic adenosine monophosphate upregulation. These changes are hypothesized to mediate increased OWS severity secondary to IMF exposure.8,9
Identifying Opioid Withdrawal
OWS occur following the cessation or significant decrease in opioid receptor activity after weeks to months of agonism.10 Opioid tolerance, physical dependence, and/or withdrawal do not equate with OUD, but many with OUD experience these physiologic adaptations.11 OWS include physical and psychological symptoms, including chills, body aches, emesis, diarrhea, dysphoria, irritability, and anxiety.12 Several validated tools exist to facilitate diagnosing and rating OWS severity. The Clinical Opiate Withdrawal Scale (COWS), published in 1999, is widely used in clinical care and research. Symptoms were categorized by severity or intensity (eg, reported nausea being of low severity and observable emesis being of high severity). Total score correlates with OWS severity and is categorized into severity groups.13 The Subjective Opiate Withdrawal Scale (SOWS) and Objective Opiate Withdrawal Scale (OOWS) also exist for use.14 The SOWS is distinct as patients rate 16 items from a score of “not at all” to “extremely” (0 to 4). Items include “I feel anxious” and “My muscles twitch.” In contrast, OOWS is observer-rated, noting the presence and/or frequency of 13 signs of opioid withdrawal including yawning, mydriasis, and restlessness.
Opioid Withdrawal Treatment
Efficient OWS identification, assessment, and treatment are crucial. Symptom resolution, by either treatment or return to use, is an important motivator in OUD.12 Fear of opioid withdrawal, particularly its undertreatment in the healthcare setting, has been a frequently reported reason for individuals delaying OUD treatment.15 Individuals with OUD may discontinue hospitalization or medical care following inadequately treated withdrawal and pain.16,17 For example, approximately 1 in 6 people hospitalized for drug use-associated infective endocarditis leave the hospital prematurely due to undertreated withdrawal.18,19
The use of methadone, buprenorphine, and other full-agonist opioids to treat OWS is the standard of care.20 Both buprenorphine and methadone as maintenance medications are effective in treatment retention and reducing illicit opioid use; this has continued support in the fentanyl era.21,22 Yet, growing evidence suggests OWS following IMF does not respond as well to non-opioid medications, buprenorphine, introductory doses of methadone, or standard doses of slow-release oral morphine.23–25 Given the risk of returning to opioid use and overdose death when these medications are only utilized for short-term withdrawal management, published guidelines highlight the importance of maintenance of MOUD.26
Aim
We reviewed current practices in OWS management and presented therapeutic interventions that have been studied and published between January 2010 and November 2023, focusing on research that may inform OWS management while increasing IMF exposure. This review focuses specifically on study populations seeking treatment for OWS and/or OUD directly from an unregulated opioid supply such as IMF.
Methods
The search strategies were developed in collaboration with a health science librarian (MT). Searches focused on identifying citations of opioid withdrawal concepts.
Systematic search strategies were created for PubMed and PsycINFO (EBSCOhost) databases. The search terms included controlled vocabulary, synonyms, and concepts related to opiates, opioid withdrawal, and opioid withdrawal management. The final database search was conducted on November 13, 2023, with all results exported to a citation manager the same day. Date of publication was limited to between January 2010 and November 2023. The January 2010 start date was considered a conservative time estimate for when IMF was entering the drug supply, but prior to the surge in IMF-related overdose deaths.27
In addition to date filters in both databases, PubMed’s clinical study filter and PsycINFO’s age and academic journal filters were used. Inclusion criteria were adults (18 years old and older) most recently utilizing an illicit, unregulated drug supply prior to the identification and/or treatment of opioid withdrawal. Exclusion criteria included studies on neonatal withdrawal syndromes or transitioning from a regulated and/or prescription opioid supply.
After deduplication, 426 studies were included. Article titles and abstracts were screened by AW and NB, using the inclusion and exclusion criteria described above. AW, JT, MB, and NB reviewed the full text of the articles and 173 studies. Uncertainty was resolved by discussion of AW, JT, MB, and NB as needed. Figure 1 summarizes the PRISMA flowchart for study inclusion.
Results
Buprenorphine
Buprenorphine is a partial agonist of the mu-opioid receptor with high receptor affinity.28 This characteristic allows for the displacement of full agonists by buprenorphine, causing buprenorphine-precipitated opioid withdrawal (BPOW). BPOW typically develops within 10–15 minutes following buprenorphine administration, lasts 8–24 hours and has been objectively defined by some as an increase of >6 on the COWS29,30 Notably, chronic IMF use carries a greater risk of BPOW.31 Prior to the rise of IMF, BPOW was estimated to occur in 9% of buprenorphine initiations.30 This risk has subsequently increased with traditional initiation models, likely secondary to fentanyl’s rapid onset of action and high lipophilicity4,31,32 For a standard buprenorphine induction in those chronically exposed to fentanyl, some guidelines suggest that waiting until the COWS is >13 (moderate severity range).33 However, low-dose and high-dose initiations are alternative options.
Review results indicate that buprenorphine continues to be effective for OWS treatment.34 Notably, buprenorphine maintenance treatment remains superior to detoxification alone in reducing illicit opioid use and increasing treatment retention.22 Therefore, it is of high importance to have effective approaches to initiate buprenorphine in the fentanyl era. One method is low-dose initiation (ie, microinduction), which provides increased flexibility as it can be initiated at any COWS level but requires access to full-agonist opioids throughout the titration.35 It is premised on slowly increasing the buprenorphine dose and frequency over several days, while a full-agonist opioid is maintained. This avoids prolonged moderate-to-severe OWS while minimizing clinically significant BPOW risk.36 Low-dose initiations can be adapted for various formulations of buprenorphine, including intravenous, transdermal, and buccal versions.37,38 An example of a low-dose buprenorphine initiation using a full-agonist opioid to bridge is included in Table 1. Other studies have also examined low-dose buprenorphine initiation protocols that may not require full agonist–opioid bridging. For example, a 20 mcg/h transdermal patch can be used for the initial 24–48 hours, with 8 and 16 mg sublingual buprenorphine administered at the 24 and 48 h mark, respectively. On day 3, the transdermal patch was removed and followed by sublingual buprenorphine titration. Most patients evaluated retrospectively with this method were reported to tolerate it fairly well.37 This protocol is summarized in Table 2.
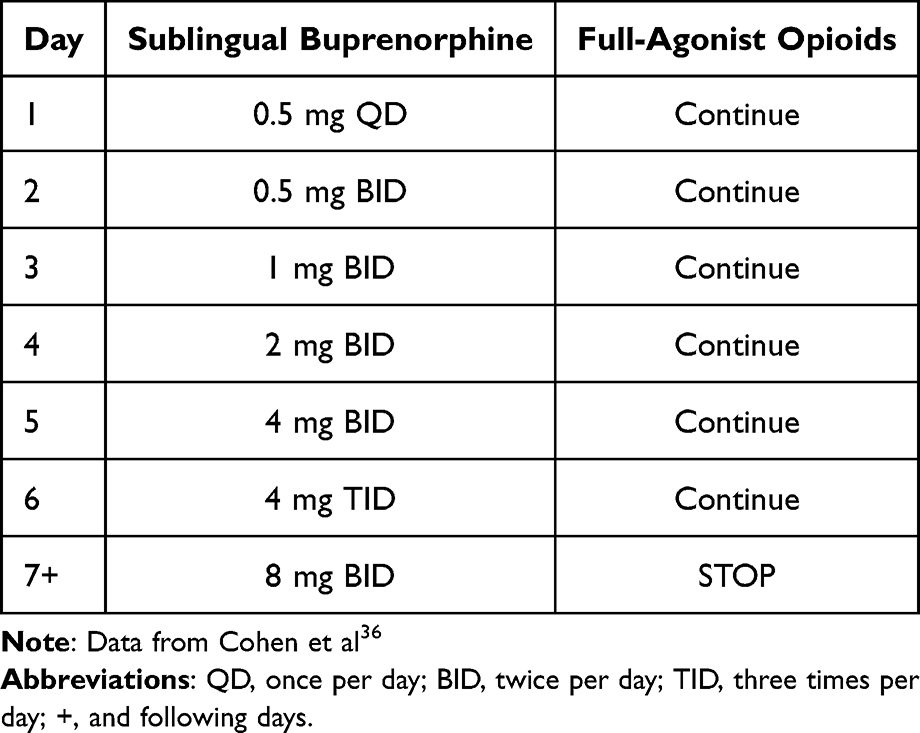 |
Table 1 Low-Dose Buprenorphine Initiation Using Sublingual Buprenorphine |
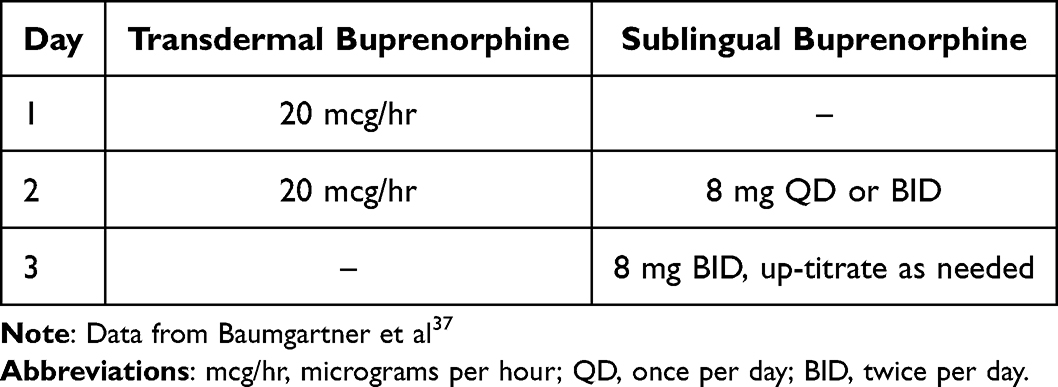 |
Table 2 Low-Dose Buprenorphine Initiation Using Transdermal Buprenorphine Without Concurrent Full-Agonist Opioid |
The initiation of high-dose buprenorphine therapy is another treatment strategy. It is predicated on rapidly reaching therapeutic buprenorphine levels by repeatedly dosing 8–24 mg of buprenorphine every 30–60 minutes until OWS has resolved followed by subsequent daily maintenance of buprenorphine.39 This technique was primarily developed and studied in emergency department settings, where rapid stabilization and discharge are a priority.39 Extended release buprenorphine (BUP-XR) formulations (ie, injectables) have been similarly utilized in the emergency department without precipitating opioid withdrawal.40 An observational cohort of 1200 people with fentanyl-positive urine receiving emergency department-initiated buprenorphine reported only 9 episodes of precipitated withdrawal. These were equally distributed between sublingual and BUP-XR formulations.41
High-dose regimens, along with adjunctive medication, are increasingly used for BPOW treatment.33,39 A case documented BPOW (COWS 16 increased to 33) after the administration of buprenorphine 8 mg following 29 h of no illicit substance use. Escalated doses of buprenorphine 4–16 mg every 2–3 hours were administered over the next 24 hours, reducing the COWS to a 5.28 A similar case of BPOW used repeated 16 mg dosing of buprenorphine, totaling 148 mg over the first 48 hours, to adequately treat symptoms.32 Additionally, higher buprenorphine doses may provide greater reductions in COWS and cravings.42 This data emphasizes the need for dosing flexibility when managing OWS, particularly BPOW.
Strategies also exist to accelerate the transition from illicit opioids to BUP-XR. Mariani et al transitioned 5 patients from high-potency opioids to BUP-XR after only 2–3 days of sublingual buprenorphine. This was 4–5 days faster than that of the package insert. The induction COWS ranged between 10 and 16, with a day 1 sublingual buprenorphine dose range of 10–24 mg. In all cases, the COWS score was significantly reduced immediately and 24 h after treatment with 300 mg of BUP-XR. The authors concluded that tolerance to 16 mg sublingual buprenorphine over two days conferred successful transition to BUP-XR and that further delay was unnecessary.43 Another strategy involved one dose of 4 mg sublingual buprenorphine followed an hour later by BUP-XR 300 mg if COWS did not increase by 6 or more following the sublingual dose. BPOW did not occur following any sublingual buprenorphine and only occurred in 2 (8.3%) cases following BUP-XR. Notably, both patients had the highest urine fentanyl and norfentanyl levels at the time of admission. The authors reported widespread use of adjuvant medications (ondansetron, clonidine, ibuprofen, and trazodone) in these patients.40
Methadone
Methadone, a long-acting synthetic opioid with a full mu-opioid receptor agonist effect, has drawn increasing attention as a treatment for OWS and MOUD in the fentanyl era. Unlike buprenorphine, there is no risk of precipitating opioid withdrawal, increasing usability across settings.44 Methadone serum concentrations have been inversely correlated with subjective OWS during initiation and maintenance phase, supporting dose adjustments based on patient reported cravings and withdrawal symptoms.45 Methadone’s full agonist mechanism may provide additional benefit in cases where buprenorphine is unable to manage OWS.46 In efforts to increase access to methadone, clinics are leveraging the “72 hour rule” under the current federal law, 21 CFR 1306.07, to more rapidly initiate methadone by non-opioid treatment program (OTP) providers and facilitate entry into OTPs. A transitional clinic in the Northeast United States working with a primarily fentanyl-exposed population (85%) successfully linked most individuals to an OTP (n = 138, 87%), with the majority (58%) still undergoing treatment at 1-month follow-up.47
Methadone deregulation of OUD treatment in the United States to a community pharmacy-based distribution model resembling Canada and Australia has potential for increasing treatment retention and cost-effectiveness when compared to take-home flexible dosing buprenorphine.48,49 The United States Congress is considering the Modernizing Opioid Treatment Access Act, which would allow physicians board-certified in addiction medicine or addiction psychiatry to prescribe methadone for OUD outside of OTP settings.50 Critics raise concerns that this law could increase diversion and overdose risk while decreasing treatment retention.51,52 Supporters note the lack of OTP access in the United States and the significant burden OTP requirements place on patients.53 Methadone take-home dosing relaxation during the COVID-19 pandemic was not associated with an increase in diversion or methadone-related overdose.54,55 Given the increases in patient satisfaction and treatment engagement without significantly worsening outcomes, the above legislation continues to gain bipartisan support as opioid-related fatalities increase nationwide.56
Other Opioid Agonist Treatments
Other full agonist opioids may be options for OUD treatment initiation and maintenance in the fentanyl era. A group in Vancouver, Canada, is studying sustained-release oral morphine (SROM) versus methadone in decreasing unregulated opioid use and improving treatment retention, safety, overdose risk, patient satisfaction, and quality of life.57 This may add to the existing literature suggesting SROM has similar efficacy to methadone in increasing drug-free time.58 In Iran, a study reviewing tramadol 600 mg daily vs methadone 60 mg daily to manage OWS over 3 days resulted in similar OOWS scores and drop-out rates.59 Of note, conversion of tramadol to its highly potent active metabolite, O-desmethyltramadol, is dependent on CYP2D6 enzyme activity. The prevalence of CYP2D6 ultra-metabolizers (who create higher levels of O-desmethyltramadol) varies worldwide and is higher in Middle East populations.60 Therefore, the use of tramadol for OWS management may not be generalizable.
Of note, the use of short-acting opioids to manage OWS in the United States during the fentanyl era has been limited to the hospital setting, given federal law restricting the use of full-agonist opioids to treat OUD outside of a federally certified OTP.61,62
Naltrexone/Naloxone
Naltrexone, an antagonist of the mu-opioid receptor, is an FDA-approved daily maintenance treatment for OUD. A once-monthly extended-release naltrexone (XR-NTX) intramuscular version is also available. A barrier to naltrexone initiation is the package insert requirement of 7–10 days being opioid free before initiation to avoid precipitated withdrawal. As discussed above, IMF’s properties heighten this concern.4 Safe and comfortable inductions onto XR-NTX are particularly relevant as when looking at 24-week outcomes between initiation on either buprenorphine or XR-NTX, individuals have greater success starting buprenorphine; however, those who successfully start XR-NTX may do equally well at follow-up.63
Several strategies have been developed to assist in initiation. All identified trials included liberal use of adjunctive medications (including clonidine, trazodone, acetaminophen, loperamide, clonazepam, zolpidem, or simply stating “and other adjuvant medications”). Rudolf et al highlighted how non-opioid-based withdrawal management (scheduled tizanidine, gabapentin, and hydroxyzine over four days) can be effective for some attempting to initiate XR-NTX.64 However, the utilization of short-course buprenorphine was most common in the included literature.
Mannelli et al conducted two open-label trials to transition outpatients from illicit opioids to XR-NTX. In their initial trial, 20 patients using opioids (majority heroin) were started on 0.25 mg of naltrexone on day 1 along with 4 mg of buprenorphine. Naltrexone was titrated daily for 7 days to a final mean dose of 31.3 (SD = 8.14, range = 13–50); buprenorphine was decreased to 2 mg on days 2 and 3 and then discontinued. Fifteen of the 20 patients completed this phase. Fourteen patients received XR-NTX on day 8. The COWS peaked at baseline, decreased, and remained low throughout the 4-week follow-up period. Of interest, they note that increasing doses of naltrexone following discontinuation of buprenorphine had no significant changes on COWS.65 Their second trial used the same buprenorphine 3-day taper and naltrexone escalation in a group of 35 patients, showing similar results.66 Table 3 summarizes protocols by Rudolf et al and Mannelli et al
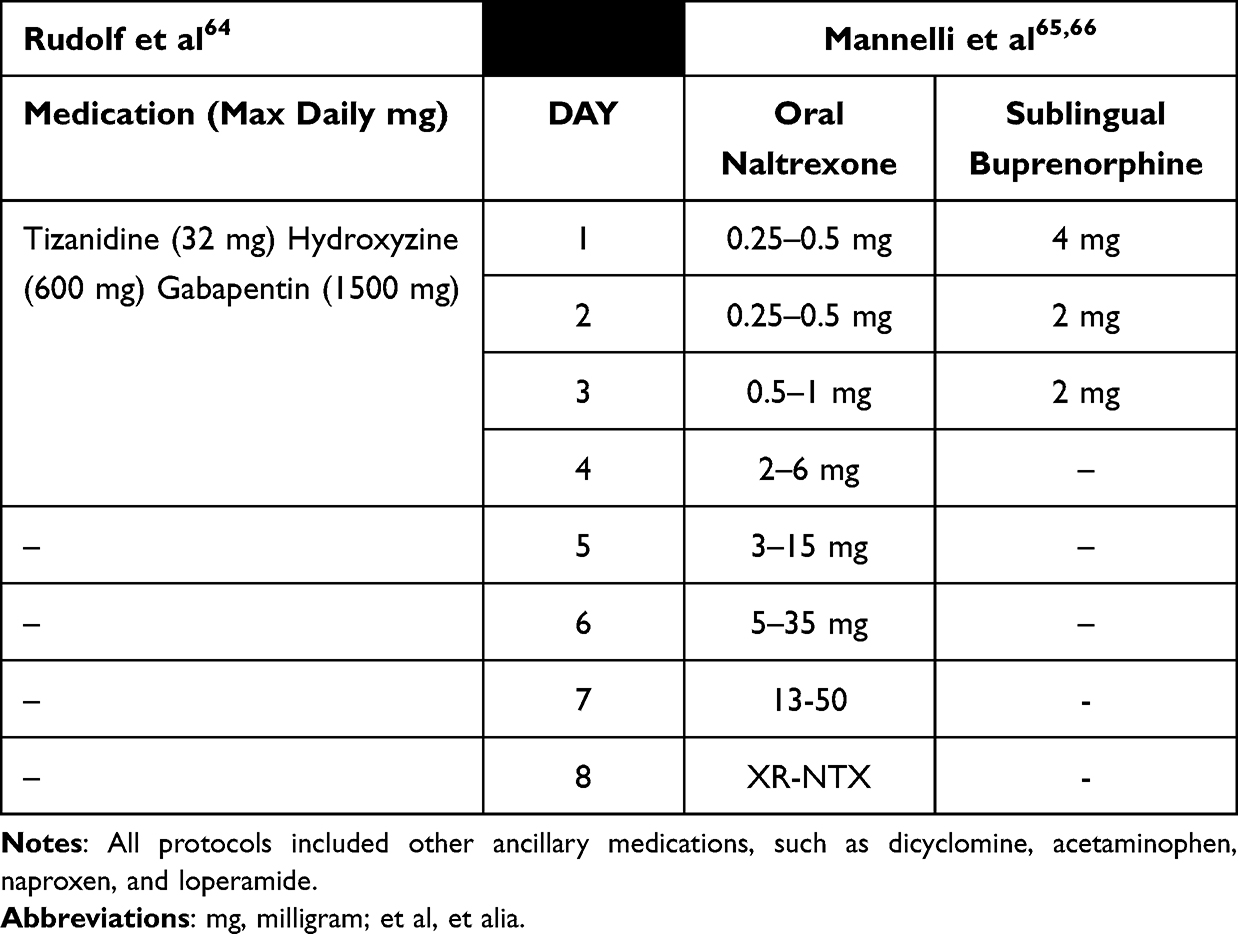 |
Table 3 Comparison of Published Protocols Using Various Medications to Transition to Extended-Release Naltrexone (XR-NTX) |
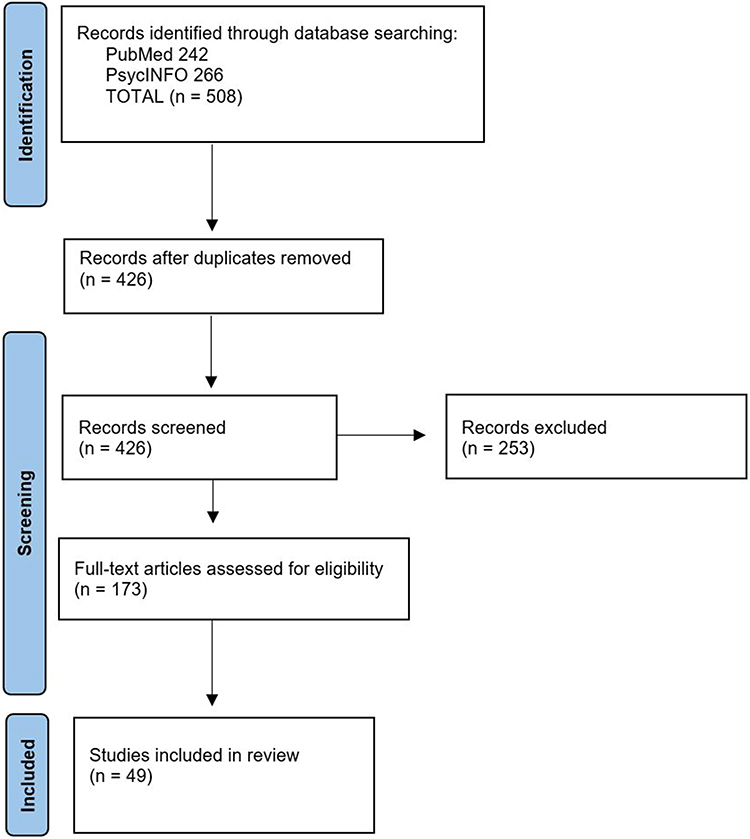 |
Figure 1 Prisma Flow Diagram. |
Two trials compared naltrexone with naltrexone plus buprenorphine targeting XR-NTX initiation. Sullivan et al enrolled 150 patients with OUD who received adjunctive medications on day 1 and up to 8 mg buprenorphine on day 2. The study then diverged to either a washout day followed by increasing naltrexone doses (1 mg to 25 mg) on days 4–7 followed by XR-NTX on day 8 or a buprenorphine taper from 6 mg on day 3 to 1 mg on day 7, followed by a 7-day wash-out and XR-NTX on day 15. The OWS was comparable across groups; however, most participants complained of protracted OWS over the first 21 days. The naltrexone arm was significantly more likely to start XR-NTX (56.1% vs 32.7%) and receive a second injection (50.0% vs 26.9%). The authors concluded that the naltrexone arm benefited from shorter time-to-initiation.67
Bisaga et al enrolled 378 patients with OUD with the goal of starting XR-NTX, randomized to 3 arms: naltrexone with buprenorphine, naltrexone with placebo buprenorphine, and placebo naltrexone with placebo buprenorphine. Naltrexone dosing began on day 1 at 0.25 mg and increased to 15 mg by day 7; buprenorphine dosing started at 4–6 mg on day 1, followed by 2 mg on days 2–3, and then wash-out. The COWS scores decreased similarly across the groups. Notably, SOWS was significantly lower in the naltrexone with buprenorphine arm after the day 8 XR-NTX injection than in the other arms. There was no difference between the groups in starting XR-NTX, with all arms below 50%.68
Methods that eliminate multiple-day tapers include ultra-rapid opioid detoxification. However, little research has been conducted in this area. A review found one prospective study of 173 participants with physiological opioid dependence who underwent the ultra-rapid procedure.69 Participants were premedicated with clonidine and midazolam, intubated using propofol and atracurium, and mechanically ventilated. Opioid detoxification occurred following 50 mg of naltrexone via a nasogastric tube, followed by intravenous naloxone for 6 h. The patient was then brought out of anesthesia. The mean OOWS was 1.52 before the procedure and peaked at 3.89 one hour after the end of anesthesia. They noted that participants experienced a high rate of withdrawal from the queried symptoms. No major adverse events were reported.
Bisaga et al conducted two trials with memantine augmentation of a buprenorphine taper onto naltrexone and XR-NTX.70,71 Memantine is a glutamate antagonist at the N-methyl-d-aspartate (NMDA) receptor, with preclinical evidence that it ameliorates OWS. However, neither trial was found to be effective. Similarly, dronabinol, an oral synthetic molecule of delta-9-tetrahydrocannabinol, and lorcaserin, a high-affinity 5-HT2C receptor agonist, were investigated for the augmentation of buprenorphine tapers to start XR-NTX. Both trials yielded negative results.
Non-Opioid Pharmaceutical Treatments
Lofexidine is an alpha-2-adrenergic receptor agonist FDA-approved for management of OWS. In a pivotal trial, patients with OUD were randomized to receive 3.2 mg lofexidine daily for 5 days (n = 134) or placebo (n = 130). Overall retention was low, with 50 and 35 patients in the lofexidine and placebo groups, respectively, completing the 7-day inpatient detoxification period. The day 3 SOWS (primary endpoint) was significantly lower in the lofexidine group than in the placebo (6.32 vs 8.67, p = 0.021). Additionally, non-completers stayed in the trial longer if they received lofexidine.72 Two different daily doses of lofexidine (2.16 mg and 2.88 mg) were compared against placebo in a trial of 603 patients with OUD over 7 days. Retention was low, at 27.8% for placebo, 41.5% for low-dose lofexidine, and 39.6% for high-dose lofexidine. However, both groups’ SOWS were significantly lower than placebo, and few discontinuations were reported to be due to adverse side effects.73 In a trial comparing lofexidine with diazepam, no differences were seen in OOWS or SOWS on days 3 and 4 (peak withdrawal).74
Gabapentin and pregabalin, both N-type calcium channel blockers, have been studied for opioid withdrawal, typically as augmentation of opioid agonists. In a small placebo-controlled study, gabapentin augmentation (1600 mg daily) during buprenorphine detoxification did not result in significant differences in OWS compared to buprenorphine only but was associated with decreased opioid-positive urine results at follow-up.75 Similarly, 450 mg daily pregabalin augmentation of buprenorphine detoxification was not significantly different in SOWS between intervention and placebo augmentation.76 A third small trial compared 1600 mg of gabapentin versus 450 mg of pregabalin and placebo. Again, no significant differences were observed in the SOWS.77
Suvorexant, an orexin antagonist used to treat insomnia, has been studied in buprenorphine detoxification tapers. The study doses (20 mg and 40 mg) did not differ from the placebo in the SOWS measurement of OWS. However, suvorexant significantly improved sleep duration, exceeding the American Academy of Sleep Medicine threshold for clinically relevant sleep improvements.78
Dextromethorphan (d-3-methoxy-N-methylmorphine) is a commonly used cough-suppressant. Dextromethorphan exhibits NMDA receptor antagonism, which is similar to memantine listed above, and may help attenuate OWS. In patients receiving clonidine to ameliorate OWS from heroin, dextromethorphan 60 mg (compared with placebo) showed improvements in OOWS scores during the later phase (days 3–6) of withdrawal. However, this was only revealed during a post-hoc analysis, with no significant difference from the placebo OOWS scores overall.79
Intramuscular olanzapine 10 mg (33 patients), a second-generation antipsychotic, was compared with oral clonidine 0.3 mg (30 patients) in the treatment of OWS in the emergency department. Olanzapine-treated patients received fewer rescue medications and showed greater improvement in COWS; however, no statistical tests were reported. This may be of value when treating OWS in emergency departments that do not have the ability to administer buprenorphine or opioid agonists, or if co-occurring significant agitation is present.80
The role and application of medicinal plants in OWS treatment has also been investigated. One specific plant, Sophora alopecuroides, is traditionally used in Iranian folk medicine to treat pain and addiction. The seed extract of Sophora alopecuroides (three 400 mg capsules once a day) was found to decrease COWS scores (versus placebo) on days 3 and 8 in patients undergoing opioid withdrawal.81 In another study on patients undergoing heroin withdrawal, the seed extract (same dose as above) led to a significant decrease in COWS scores on days 3 and 8 compared to placebo.82 The seed extracts also demonstrated a good safety profile.
Buspirone, a 5-HT1a agonist with D2 antagonist properties and memantine have been investigated to augment buprenorphine tapers for the treatment of OWS. Buspirone 45 mg daily significantly decreased SOWS in combination with buprenorphine versus buprenorphine alone over two weeks of residential treatment for OUD. Buspirone was also associated with improved sleep during the buprenorphine taper.83 Memantine at 20 mg dosing, which is lower than other studies investigating the medication, saw no differences in SOWS when combined with buprenorphine and clonidine versus those two medications alone.84
The corticotropin-releasing factor receptor (CRF1) increases the hypothalamus-pituitary axis activity during OWS, and its modulation has been investigated for acute OWS treatment. Pexacerfont, a CRF1 antagonist, was studied for 3 weeks via burst and taper (300 mg, 200 mg, and 100 mg, each daily for 1 week). Cravings and craving-related metrics (eg, temptation severity) were improved with active treatment versus placebo; however, COWS was similar between the groups across the measured time-points.85
Scopolamine is a muscarinic antagonist that is used to treat nausea and vomiting associated with motion sickness. Inpatients with OUD were randomized to receive a methadone taper versus light anesthesia with 0.03–0.05 mg/kg of scopolamine hydrobromide and 0.6–1.0 mg/kg of chlorpromazine hydrochloride for 3–4 days. SOWS was largely stable in the scopolamine group versus an acute 2–3-day spike in SOWS that was seen in the methadone taper (after the conclusion of dosing). More patients who received scopolamine therapy remained abstinent and in outpatient treatment for 8 weeks compared to those in the methadone taper group. The scopolamine group had significant adverse effects, including respiratory distress, aspiration pneumonia, and pulmonary edema, some of which were life-threatening events.86
Neurostimulation Interventions
Neurostimulation in addiction treatment is being extensively studied, primarily for the maintenance of OUD treatment. For OWS management, the most established neurostimulation techniques are mediated by the vagus nerve, either cervically or at the ear, with transcutaneous or percutaneous electrical stimulation. Although the underlying mechanism remains unclear, a plausible pathway exists. Autonomic changes are a hallmark of OWS. The locus coeruleus is the brain’s principal norepinephrine-producing region and is important in the autonomic nervous system.87 In acute opioid withdrawal, locus coeruleus firing rates increase and are associated with OWS.88 The locus coeruleus receives input from the vagus nerve via the solitary nucleus.89,90 Through use of these neurostimulation devices, there is potential for balance to be regained between the sympathetic and parasympathetic nervous systems.
While further research is needed to elucidate the underlying treatment mechanisms, the FDA has granted approval for two percutaneous electrical nerve field stimulators (PENFS) for OWS.91,92 Both devices require transillumination of the ear to place needle electrodes for periodic stimulation delivery and can be worn for up to five days. A pivotal study by Miranda et al in 2018 led to approval of the BridgeTM device. This was an open-label (ie, no sham-control) retrospective study that evaluated 73 outpatients with mild (n = 4) or moderate-to-moderately severe (n = 69) opioid withdrawal. The COWS was assessed up to three times in the initial hour following device placement and again at the 5-day follow-up. At baseline, the mean COWS was 20.1 (SD = 6.1). At 1 h of device use, the mean COWS was 3.1 (SD = 3.4), and 57 (78.1%) individuals with COWS < 4. Thirty-three of 73 (45.2%) individuals were seen at follow-up, with mean COWS of 0.6 (SD not reported). The stated goal was an eventual transition to MOUD, noting that 64 of 73 (88.8%) patients started MOUD; however, the breakdown of MOUD was not presented. They noted that 33 individuals started naltrexone after using the device; however, the number of days following either 1) final opioid use or 2) the final day of the BridgeTM device use before naltrexone initiation was not reported. This prevents any hypothesis formation on if this device may reduce precipitated withdrawal symptoms.92 Regarding the DyAnsys Drug ReliefTM device, there was no readily identifiable data in the literature nor mention within the FDA approval memo regarding specific data that led to FDA device approval.91
A retrospective 5 case series by Buono et al also reported auricular delivery of PENFS for over 5 days. The data presented are sparse; however, only reporting improvements in COWS across study days, alongside daily blood pressure and heart rate. No statistical tests were performed. These cases also existed within a 52-week structured treatment program.93 Tirado et al prospectively studied auricular treatment of opioid withdrawal using noninvasive transcutaneous auricular neurostim (tAN). Thirty-one individuals were randomized to receive either 30 minutes of active tAN (n = 16) or 30 minutes of sham treatment (n = 15). There was a more significant reduction in the COWS of the active tAN group than that in the sham group after 30 min of stimulation (reduced by 6.3 compared to 3.7, p = 0.036).94
Two other trials evaluated alternative anatomical locations. Gazi et al investigated transcutaneous cervical vagus nerve stimulation (tcVNS) in individuals with OUD whose last opioid use was at least 8 hours prior. Over two hours, the participants received either four 2-minute active stimulation sessions (n = 10) or four 2-minute sham stimulation sessions (n = 11). The study evaluators considered six scales along with COWS decomposition. While the active group did have significantly improved self-report of subjective cravings, withdrawal, and overall distress, the COWS itself was not significantly different between groups at the 2-hour endpoint.95 Meade et al investigated transcutaneous electric acupoint stimulation (TEAS) at acupoints hegu and neiguan as an adjunctive treatment for opioid detoxification with buprenorphine. Anatomically, electrodes were placed between the first and second metacarpal bones (dorsal and palmar surfaces) of one hand, whereas the other upper limbs had electrodes placed on the median nerve at the forearm (dorsal and palmar surfaces). All the participants received buprenorphine. Twenty-six participants received thrice-daily 30-minute TEAS treatments for four days, while 29 received thrice-daily sham stimulation over four days. Two weeks after discharge, the active TEAS group was less likely to have reported any drug use as compared to the sham group (35% vs 77%, p < 0.05). However, no differences in OWS were observed.96
No studies have used transcranial magnetic stimulation or direct current stimulation for opioid withdrawal. As there is evidence that these interventions combined with MOUD may be beneficial in SUD-related outcomes in maintenance treatment, future research exploring their potential utility in withdrawal management may be warranted.97
Discussion
Fentanyl exposure has been associated with a reduced likelihood of treatment initiation, worse treatment retention, and increased OWS severity.98,99 This review highlights that although IMF has affected the initiation and maintenance of MOUD, many core principles of OWS treatment remain the same. Buprenorphine can be safely and effectively initiated in both observed and unobserved settings, increasing patient autonomy and creating flexibility around timing.100 Novel strategies have improved the successful initiation of buprenorphine by reducing the risk of BPOW. A BPOW rate of 1% utilizing newer protocols in fentanyl-positive participants is reassuring, increasing their applicability in the fentanyl era.41 As injectable buprenorphine XR becomes more available, more research into accelerated initiation protocols is needed and may help increase successful transition from IMF to buprenorphine. Methadone, an effective treatment for OWS and OUD, has gained momentum in the fentanyl era, given its ease of use and lack of precipitated withdrawal. The deregulation of methadone during the COVID-19 pandemic has improved many patient-centered aspects of MOUD care without increasing methadone-related diversion or overdose deaths. Policies that uncouple methadone treatment from restrictive OTP standards may improve care for OWS and OUD in the fentanyl era. Our review also included quicker and more supportive protocols to transition people with OUD to XR-NTX, allowing practitioners to utilize expedited plans for those most interested in nonopioid strategies. Outside FDA-approved medications for OUD, newer studies on non-opioid pharmacology, such as lofexidine, gabapentin, and suvorexant, have been most helpful in augmenting the initiation of opioid agonists; however, their evidence is limited. Neurostimulation interventions are currently in development, with a few studies showing mild improvement in withdrawal symptoms. Although more research is needed on monotherapy for acute OWS, these devices may be beneficial for patients who choose to transition away from buprenorphine and methadone after establishing OUD remission.
Conclusion
There is an urgent need to identify, research, and implement adequate treatments for OWS and OUD in the era of high-potency synthetic opioids such as fentanyl. Buprenorphine and methadone, with or without adjunctive medications, have been used to successfully treat OWS. Research shows that combination treatment and pharmacokinetically informed protocols may reduce OWS severity while reducing the time required for a successful transition to MOUD. Shorter induction protocols allow patients to initiate evidence-based treatment more quickly, reducing the use of illicit or non-prescribed substances.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ahmad FBCJ, Rossen LM, Sutton P. Provisional drug overdose death counts. National Center for Health Statistics. 2023.
2. Gladden RM, Martinez P, Seth P. Fentanyl Law Enforcement Submissions and Increases in Synthetic Opioid-Involved Overdose Deaths - 27 States, 2013-2014. MMWR Morb Mortal Wkly Rep. 2016;65(33):837–843. doi:10.15585/mmwr.mm6533a2
3. Jones CM, Bekheet F, Park JN, Alexander GC. The Evolving Overdose Epidemic: synthetic Opioids and Rising Stimulant-Related Harms. Epidemiol Rev. 2020;42(1):154–166. doi:10.1093/epirev/mxaa011
4. Jannetto PJ, Helander A, Garg U, Janis GC, Goldberger B, Ketha H. The Fentanyl Epidemic and Evolution of Fentanyl Analogs in the United States and the European Union. Clin Chem. 2019;65(2):242–253. doi:10.1373/clinchem.2017.281626
5. Higginbotham JA, Markovic T, Massaly N, Moron JA. Endogenous opioid systems alterations in pain and opioid use disorder. Front Syst Neurosci. 2022;16:1014768. doi:10.3389/fnsys.2022.1014768
6. Peng J, Sarkar S, Chang SL. Opioid receptor expression in human brain and peripheral tissues using absolute quantitative real-time RT-PCR. Drug Alcohol Depend. 2012;124(3):223–228. doi:10.1016/j.drugalcdep.2012.01.013
7. Trescot AM, Datta S, Lee M, Hansen H. Opioid pharmacology. Pain Physician. 2008;11(2 Suppl):675.
8. Morgan MM, Christie MJ. Analysis of opioid efficacy, tolerance, addiction and dependence from cell culture to human. Br J Pharmacol. 2011;164(4):1322–1334. doi:10.1111/j.1476-5381.2011.01335.x
9. Williams JT, Ingram SL, Henderson G, et al. Regulation of mu-opioid receptors: desensitization, phosphorylation, internalization, and tolerance. Pharmacol Rev. 2013;65(1):223–254. doi:10.1124/pr.112.005942
10. Pergolizzi JV Jr, Raffa RB, Rosenblatt MH. Opioid withdrawal symptoms, a consequence of chronic opioid use and opioid use disorder: current understanding and approaches to management. J Clin Pharm Ther. 2020;45(5):892–903. doi:10.1111/jcpt.13114
11. Volkow ND, McLellan AT. Opioid Abuse in Chronic Pain--Misconceptions and Mitigation Strategies. N Engl J Med. 2016;374(13):1253–1263. doi:10.1056/NEJMra1507771
12. Koob GF. Anhedonia, Hyperkatifeia, and Negative Reinforcement in Substance Use Disorders. Curr Top Behav Neurosci. 2022;58:147–165. doi:10.1007/7854_2021_288
13. Wesson DR, Ling W. The Clinical Opiate Withdrawal Scale (COWS). J Psychoactive Drugs. 2003;35(2):253–259. doi:10.1080/02791072.2003.10400007
14. Handelsman L, Cochrane KJ, Aronson MJ, Ness R, Rubinstein KJ, Kanof PD. Two new rating scales for opiate withdrawal. Am J Drug Alcohol Abuse. 1987;13(3):293–308. doi:10.3109/00952998709001515
15. Hall OT, Entrup P, Farabee K, et al. The Perceived Role of Withdrawal in Maintaining Opioid Addiction among Adults with Untreated Opioid Use Disorder: a Survey of Syringe Exchange Program Participants. Subst Use Misuse. 2024;59(2):312–315. doi:10.1080/10826084.2023.2269571
16. Alrawashdeh M, Rhee C, Klompas M, et al. Association of Early Opioid Withdrawal Treatment Strategy and Patient-Directed Discharge Among Hospitalized Patients with Opioid Use Disorder. J Gen Intern Med. 2023;38(10):2289–2297. doi:10.1007/s11606-023-08059-w
17. Harris M. Normalised pain and severe health care delay among people who inject drugs in London: adapting cultural safety principles to promote care. Soc Sci Med. 2020;260:113183. doi:10.1016/j.socscimed.2020.113183
18. Kimmel SD, Kim JH, Kalesan B, Samet JH, Walley AY, Larochelle MR. Against Medical Advice Discharges in Injection and Non-injection Drug Use-associated Infective Endocarditis: a Nationwide Cohort Study. Clin Infect Dis. 2021;73(9):e2484–e2492. doi:10.1093/cid/ciaa1126
19. Simon R, Snow R, Wakeman S. Understanding why patients with substance use disorders leave the hospital against medical advice: a qualitative study. Subst Abus. 2020;41(4):519–525. doi:10.1080/08897077.2019.1671942
20. Wakeman SE, Larochelle MR, Ameli O, et al. Comparative Effectiveness of Different Treatment Pathways for Opioid Use Disorder. JAMA Network Open. 2020;3(2):e1920622. doi:10.1001/jamanetworkopen.2019.20622
21. Mattick RP, Breen C, Kimber J, Davoli M. Buprenorphine maintenance versus placebo or methadone maintenance for opioid dependence. Cochrane Database Syst Rev. 2014;2014(2):CD002207. doi:10.1002/14651858.CD002207.pub4
22. Stein M, Herman D, Conti M, Anderson B, Bailey G. Initiating buprenorphine treatment for opioid use disorder during short-term in-patient ‘detoxification’: a randomized clinical trial. Addiction. 2020;115(1):82–94. doi:10.1111/add.14737
23. Neimark G, Tjoa C. Treating Fentanyl Withdrawal. J Behav Health Serv Res. 2020;47(4):614–615. doi:10.1007/s11414-020-09710-8
24. Sue KL, Cohen S, Tilley J, Yocheved A. A Plea From People Who Use Drugs to Clinicians: new Ways to Initiate Buprenorphine Are Urgently Needed in the Fentanyl Era. J Addict Med. 2022;16(4):389–391. doi:10.1097/ADM.0000000000000952
25. Bromley LKM, Regenstreif L, Srivastava A, Wyman J. Methadone Treatment for People Who Use Fentanyl: Recommendations. META: PHI, editor. Toronto, ON; 2021.
26. Calcaterra SL, Bottner R, Martin M, et al. Management of opioid use disorder, opioid withdrawal, and opioid overdose prevention in hospitalized adults: a systematic review of existing guidelines. J Hosp Med. 2022;17(9):679–692. doi:10.1002/jhm.12908
27. Ciccarone D. The triple wave epidemic: supply and demand drivers of the US opioid overdose crisis. Int J Drug Policy. 2019;71:183–188. doi:10.1016/j.drugpo.2019.01.010
28. Oakley B, Wilson H, Hayes V, Lintzeris N. Managing opioid withdrawal precipitated by buprenorphine with buprenorphine. Drug Alcohol Rev. 2021;40(4):567–571. doi:10.1111/dar.13228
29. Cisewski DH, Santos C, Koyfman A, Long B. Approach to buprenorphine use for opioid withdrawal treatment in the emergency setting. Am J Emerg Med. 2019;37(1):143–150. doi:10.1016/j.ajem.2018.10.013
30. Whitley SD, Sohler NL, Kunins HV, et al. Factors associated with complicated buprenorphine inductions. J Subst Abuse Treat. 2010;39(1):51–57. doi:10.1016/j.jsat.2010.04.001
31. Varshneya NB, Thakrar AP, Hobelmann JG, Dunn KE, Huhn AS. Evidence of Buprenorphine-precipitated Withdrawal in Persons Who Use Fentanyl. J Addict Med. 2022;16(4):e265–e268. doi:10.1097/ADM.0000000000000922
32. Bormann NL, Gout A, Kijewski V, Lynch A. Case Report: buprenorphine-precipitated fentanyl withdrawal treated with high-dose buprenorphine. F1000Res. 2022;11:487. doi:10.12688/f1000research.120821.2
33. Spadaro A, Long B, Koyfman A, Perrone J. Buprenorphine precipitated opioid withdrawal: prevention and management in the ED setting. Am J Emerg Med. 2022;58:22–26. doi:10.1016/j.ajem.2022.05.013
34. Nemlekar SS, Mehta R, Dave KR, Chaudhari F. Opioid withdrawal and its stabilization on sublingual buprenorphine in intravenous drug users: a South Gujarat Perspective. j Arch Psychiatry Psychother. 2020;22(1):63–69. doi:10.12740/app/109265
35. Hammig R, Kemter A, Strasser J, et al. Use of microdoses for induction of buprenorphine treatment with overlapping full opioid agonist use: the Bernese method. Subst Abuse Rehabil. 2016;7:99–105. doi:10.2147/SAR.S109919
36. Cohen SM, Weimer MB, Levander XA, Peckham AM, Tetrault JM, Morford KL. Low Dose Initiation of Buprenorphine: a Narrative Review and Practical Approach. J Addict Med. 2022;16(4):399–406. doi:10.1097/ADM.0000000000000945
37. Baumgartner K, Salmo E, Liss D, et al. Transdermal buprenorphine for in-hospital transition from full agonist opioids to sublingual buprenorphine: a retrospective observational cohort study. Clin Toxicol. 2022;60(6):688–693. doi:10.1080/15563650.2022.2028802
38. Webster L, Hjelmstrom P, Sumner M, Gunderson EW. Efficacy and safety of a sublingual buprenorphine/naloxone rapidly dissolving tablet for the treatment of adults with opioid dependence: a randomized trial. J Addict Dis. 2016;35(4):325–338. doi:10.1080/10550887.2016.1195608
39. Herring AA, Vosooghi AA, Luftig J, et al. High-Dose Buprenorphine Induction in the Emergency Department for Treatment of Opioid Use Disorder. JAMA Network Open. 2021;4(7):e2117128. doi:10.1001/jamanetworkopen.2021.17128
40. Hassman H, Strafford S, Shinde SN, Heath A, Boyett B, Dobbins RL. Open-label, rapid initiation pilot study for extended-release buprenorphine subcutaneous injection. Am J Drug Alcohol Abuse. 2023;49(1):43–52. doi:10.1080/00952990.2022.2106574
41. D’Onofrio G, Hawk KF, Perrone J, et al. Incidence of Precipitated Withdrawal During a Multisite Emergency Department-Initiated Buprenorphine Clinical Trial in the Era of Fentanyl. JAMA Network Open. 2023;6(3):e236108. doi:10.1001/jamanetworkopen.2023.6108
42. Ahmadi J, Jahromi MS, Ghahremani D, London ED. Single high-dose buprenorphine for opioid craving during withdrawal. Trials. 2018;19(1):675. doi:10.1186/s13063-018-3055-z
43. Mariani JJ, Mahony A, Iqbal MN, Luo SX, Naqvi NH, Levin FR. Case Series: rapid Induction Onto Long Acting Buprenorphine Injection for High Potency Synthetic Opioid Users. Am J Addict. 2020;29(4):345–348. doi:10.1111/ajad.13018
44. Su MK, Lopez JH, Crossa A, Hoffman RS. Low dose intramuscular methadone for acute mild to moderate opioid withdrawal syndrome. Am J Emerg Med. 2018;36(11):1951–1956. doi:10.1016/j.ajem.2018.02.019
45. Chalabianloo F, Fadnes LT, Hoiseth G, et al. Subjective symptoms and serum methadone concentrations: what should guide dose adjustments in methadone maintenance treatment? A naturalistic cohort study from Norway. Subst Abuse Treat Prev Policy. 2021;16(1):39. doi:10.1186/s13011-021-00367-w
46. Laks J, Kehoe J, Farrell NM, et al. Methadone initiation in a bridge clinic for opioid withdrawal and opioid treatment program linkage: a case report applying the 72-hour rule. Addict Sci Clin Pract. 2021;16(1):73. doi:10.1186/s13722-021-00279-x
47. Taylor JL, Laks J, Christine PJ, et al. Bridge clinic implementation of “72-hour rule” methadone for opioid withdrawal management: impact on opioid treatment program linkage and retention in care. Drug Alcohol Depend. 2022;236:109497. doi:10.1016/j.drugalcdep.2022.109497
48. Enns B, Krebs E, Whitehurst DGT, et al. Cost-effectiveness of flexible take-home buprenorphine-naloxone versus methadone for treatment of prescription-type opioid use disorder. Drug Alcohol Depend. 2023;247:109893. doi:10.1016/j.drugalcdep.2023.109893
49. Panwala V, Joudrey P, Kowalski M, Bach P, Amram O. Changes to methadone maintenance therapy in the United States, Canada, and Australia during the COVID-19 pandemic: a narrative review. J Subst Use Addict Treat. 2023;152:209086. doi:10.1016/j.josat.2023.209086
50. GovTrack. S. 644: modernizing Opioid Treatment Access Act. Available from: https://www.govtrack.us/congress/bills/118/s644.
51. Gauthier G, Eibl JK, Marsh DC. Improved treatment-retention for patients receiving methadone dosing within the clinic providing physician and other health services (onsite) versus dosing at community (offsite) pharmacies. Drug Alcohol Depend. 2018;191:1–5. doi:10.1016/j.drugalcdep.2018.04.029
52. Strang J, Hall W, Hickman M, Bird SM. Impact of supervision of methadone consumption on deaths related to methadone overdose (1993-2008): analyses using OD4 index in England and Scotland. BMJ. 2010;341:c4851. doi:10.1136/bmj.c4851
53. Simon C, Vincent L, Coulter A, et al. The Methadone Manifesto: treatment Experiences and Policy Recommendations From Methadone Patient Activists. Am J Public Health. 2022;112(S2):S117–S122. doi:10.2105/AJPH.2021.306665
54. Jones CM, Compton WM, Han B, Baldwin G, Volkow ND. Methadone-Involved Overdose Deaths in the US Before and After Federal Policy Changes Expanding Take-Home Methadone Doses From Opioid Treatment Programs. JAMA Psychiatry. 2022;79(9):932–934. doi:10.1001/jamapsychiatry.2022.1776
55. Administration SAa MHS. Methadone take-home flexibilities extension guidance. 2021. Available from: https://www.samhsa.gov/medication-assisted-treatment/statutes-regulations-guidelines/methadone-guidance.
56. Krawczyk N, Rivera BD, Levin E, Dooling BCE. Synthesising evidence of the effects of COVID-19 regulatory changes on methadone treatment for opioid use disorder: implications for policy. Lancet Public Health. 2023;8(3):e238–e246. doi:10.1016/S2468-2667(23)00023-3
57. Socias ME, Wood E, Dong H, et al. Slow release oral morphine versus methadone for opioid use disorder in the fentanyl era (pRESTO): protocol for a non-inferiority randomized clinical trial. Contemp Clin Trials. 2020;91:105993. doi:10.1016/j.cct.2020.105993
58. Ferri M, Minozzi S, Bo A, Amato L. Slow-release oral morphine as maintenance therapy for opioid dependence. Cochrane Database Syst Rev. 2013;2(6):CD009879. doi:10.1002/14651858.CD009879.pub2
59. Zarghami M, Masoum B, Shiran MR. Tramadol versus methadone for treatment of opiate withdrawal: a double-blind, randomized, clinical trial. J Addict Dis. 2012;31(2):112–117. doi:10.1080/10550887.2012.665728
60. Dean L, Kane M, et al. Tramadol Therapy and CYP2D6 Genotype. In: Pratt V, Scott SA, Pirmohamed M, editors. Medical Genetics Summaries [Internet]. National Center for Biotechnology Information; 2021.
61. Kleinman RA, Wakeman SE. Treating Opioid Withdrawal in the Hospital: a Role for Short-Acting Opioids. Ann Intern Med. 2022;175(2):283–284. doi:10.7326/M21-3968
62. Thakrar AP. Short-Acting Opioids for Hospitalized Patients With Opioid Use Disorder. JAMA Intern Med. 2022;182(3):247–248. doi:10.1001/jamainternmed.2021.8111
63. Lee JD, Nunes EV Jr, Novo P, et al. Comparative effectiveness of extended-release naltrexone versus buprenorphine-naloxone for opioid relapse prevention (X:BOT): a multicentre, open-label, randomised controlled trial. Lancet. 2018;391(10118):309–318. doi:10.1016/S0140-6736(17)32812-X
64. Rudolf G, Walsh J, Plawman A, et al. A novel non-opioid protocol for medically supervised opioid withdrawal and transition to antagonist treatment. Am J Drug Alcohol Abuse. 2018;44(3):302–309. doi:10.1080/00952990.2017.1334209
65. Mannelli P, Wu LT, Peindl KS, Swartz MS, Woody GE. Extended release naltrexone injection is performed in the majority of opioid dependent patients receiving outpatient induction: a very low dose naltrexone and buprenorphine open label trial. Drug Alcohol Depend. 2014;138:83–88. doi:10.1016/j.drugalcdep.2014.02.002
66. Mannelli P, Swartz M, Wu LT. Withdrawal severity and early response to treatment in the outpatient transition from opioid use to extended release naltrexone. Am J Addict. 2018;27(6):471–476. doi:10.1111/ajad.12763
67. Sullivan M, Bisaga A, Pavlicova M, et al. Long-Acting Injectable Naltrexone Induction: a Randomized Trial of Outpatient Opioid Detoxification With Naltrexone Versus Buprenorphine. Am J Psychiatry. 2017;174(5):459–467. doi:10.1176/appi.ajp.2016.16050548
68. Bisaga A, Mannelli P, Yu M, et al. Outpatient transition to extended-release injectable naltrexone for patients with opioid use disorder: a Phase 3 randomized trial. Drug Alcohol Depend. 2018;187:171–178. doi:10.1016/j.drugalcdep.2018.02.023
69. Safari F, Mottaghi K, Malek S, Salimi A. Effect of ultra-rapid opiate detoxification on withdrawal syndrome. J Addict Dis. 2010;29(4):449–454. doi:10.1080/10550887.2010.509278
70. Bisaga A, Sullivan MA, Cheng WY, et al. A placebo controlled trial of memantine as an adjunct to oral naltrexone for opioid dependence. Drug Alcohol Depend. 2011;119(1–2):e23–9. doi:10.1016/j.drugalcdep.2011.05.019
71. Bisaga A, Sullivan MA, Glass A, et al. A placebo-controlled trial of memantine as an adjunct to injectable extended-release naltrexone for opioid dependence. J Subst Abuse Treat. 2014;46(5):546–552. doi:10.1016/j.jsat.2014.01.005
72. Gorodetzky CW, Walsh SL, Martin PR, Saxon AJ, Gullo KL, Biswas K. A Phase III, randomized, multi-center, double blind, placebo controlled study of safety and efficacy of lofexidine for relief of symptoms in individuals undergoing inpatient opioid withdrawal. Drug Alcohol Depend. 2017;176:79–88. doi:10.1016/j.drugalcdep.2017.02.020
73. Fishman M, Tirado C, Alam D, et al. Safety and Efficacy of Lofexidine for Medically Managed Opioid Withdrawal: a Randomized Controlled Clinical Trial. J Addict Med. 2019;13(3):169–176. doi:10.1097/ADM.0000000000000474
74. Guo S, Manning V, Yang Y, et al. Lofexidine versus diazepam for the treatment of opioid withdrawal syndrome: a double-blind randomized clinical trial in Singapore. J Subst Abuse Treat. 2018;91:1–11. doi:10.1016/j.jsat.2018.04.012
75. Sanders NC, Mancino MJ, Gentry WB, et al. Randomized, placebo-controlled pilot trial of gabapentin during an outpatient, buprenorphine-assisted detoxification procedure. Exp Clin Psychopharmacol. 2013;21(4):294–302. doi:10.1037/a0033724
76. Kheirabadi GR, Moazeni S, Salehi M, Mahaki B. Pregabalin Does Not Reduce Opioid Withdrawal Symptoms: a Randomized Controlled Trial. Addictive Disorders Their Treatment. 2019;18(4):205–211. doi:10.1097/adt.0000000000000166
77. Kheirabadi GR, Salehi M, Bahrami M, Maracy MR. Gabapentin, Pregabalin, and Placebo in Reducing Opioid Withdrawal Symptoms in Opioid-dependent Individuals: a Randomized-controlled Trial. Addictive Disorders Their Treatment. 2018;17(2):55–64. doi:10.1097/adt.0000000000000127
78. Huhn AS, Finan PH, Gamaldo CE, et al. Suvorexant ameliorated sleep disturbance, opioid withdrawal, and craving during a buprenorphine taper. Sci Transl Med. 2022;14(650):eabn8238. doi:10.1126/scitranslmed.abn8238
79. Lin SK, Pan CH, Chen CH. A double-blind, placebo-controlled trial of dextromethorphan combined with clonidine in the treatment of heroin withdrawal. J Clin Psychopharmacol. 2014;34(4):508–512. doi:10.1097/JCP.0000000000000144
80. Klein LR, Cole JB, Driver BE, et al. An open-label randomized trial of intramuscular olanzapine versus oral clonidine for symptomatic treatment of opioid withdrawal in the emergency department. Clin Toxicol. 2019;57(8):697–702. doi:10.1080/15563650.2018.1547828
81. Kianbakht S, Hajiaghaee R, Akhondzadeh S. Efficacy and safety of Sophora alopecuroides var. alopecuroides seed extract for opioid detoxification: a randomized, double-blind, and placebo-controlled clinical trial. Phytother Res. 2020;34(5):1108–1113. doi:10.1002/ptr.6578
82. Hashem-Dabaghian F, Kianbakht S. A randomized controlled trial on the seeds of Sophora alopecuroides var. alopecuroides for the treatment of acute heroin withdrawal syndrome. Complement Ther Clin Pract. 2023;51:101740. doi:10.1016/j.ctcp.2023.101740
83. Bergeria CL, Tan H, Antoine D, et al. A double-blind, randomized, placebo-controlled, pilot clinical trial examining buspirone as an adjunctive medication during buprenorphine-assisted supervised opioid withdrawal. Exp Clin Psychopharmacol. 2023;31(1):194–203. doi:10.1037/pha0000550
84. Kheirabadi G, Najafian N, Khodadadi F. The Effect of Adding Memantine to Clonidine in Reducing Withdrawal Symptoms in Opioid-Dependent Patients: a Double-Blind Randomized Controlled Trial. J Clin Psychopharmacol. 2021;41(6):644–649. doi:10.1097/JCP.0000000000001466
85. Morabbi MJ, Razaghi E, Moazen-Zadeh E, et al. Pexacerfont as a CRF1 antagonist for the treatment of withdrawal symptoms in men with heroin/methamphetamine dependence: a randomized, double-blind, placebo-controlled clinical trial. Int Clin Psychopharmacol. 2018;33(2):111–119. doi:10.1097/YIC.0000000000000200
86. Liu S, Li L, Shen W, Shen X, Yang G, Zhou W. Scopolamine detoxification technique for heroin dependence: a randomized trial. CNS Drugs. 2013;27(12):1093–1102. doi:10.1007/s40263-013-0111-9
87. Samuels ER, Szabadi E. Functional neuroanatomy of the noradrenergic locus coeruleus: its roles in the regulation of arousal and autonomic function part I: principles of functional organisation. Curr Neuropharmacol. 2008;6(3):235–253. doi:10.2174/157015908785777229
88. Rasmussen K. The role of the locus coeruleus and N-methyl-D-aspartic acid (NMDA) and AMPA receptors in opiate withdrawal. Neuropsychopharmacology. 1995;13(4):295–300. doi:10.1016/0893-133X(95)00082-O
89. Farrand A, Jacquemet V, Verner R, Owens M, Beaumont E. Vagus nerve stimulation parameters evoke differential neuronal responses in the locus coeruleus. Physiological Reports. 2023;11(5):e15633. doi:10.14814/phy2.15633
90. Fornai F, Ruffoli R, Giorgi FS, Paparelli A. The role of locus coeruleus in the antiepileptic activity induced by vagus nerve stimulation. Eur J Neurosci. 2011;33(12):2169–2178. doi:10.1111/j.1460-9568.2011.07707.x
91. U.S. Food & Drug Administration, Drug Relief - Percutaneous Nerve Stimulator for Opioid Withdrawal https://www.accessdata.fda.gov/cdrh_docs/pdf17/K173861.pdf 2018
92. Miranda A, Taca A. Neuromodulation with percutaneous electrical nerve field stimulation is associated with reduction in signs and symptoms of opioid withdrawal: a multisite, retrospective assessment. Am J Drug Alcohol Abuse. 2018;44(1):56–63. doi:10.1080/00952990.2017.1295459
93. Buono FD, Pickering R, Berlepsch R, Halligan S. Percutaneous electrical nerve field stimulation to reduce clinical opiate withdrawal: a case series. J Subst Use. 2022;27(5):501–504. doi:10.1080/14659891.2021.1961894
94. Tirado CF, Washburn SN, Covalin A, et al. Delivering transcutaneous auricular neurostimulation (tAN) to improve symptoms associated with opioid withdrawal: results from a prospective clinical trial. Bioelectronic Medicine. 2022;8(1):12. doi:10.1186/s42234-022-00095-x
95. Gazi AH, Harrison AB, Lambert TP, et al. Transcutaneous cervical vagus nerve stimulation reduces behavioral and physiological manifestations of withdrawal in patients with opioid use disorder: a double-blind, randomized, sham-controlled pilot study. Brain Stimul. 2022;15(5):1206–1214. doi:10.1016/j.brs.2022.08.017
96. Meade CS, Lukas SE, McDonald LJ, et al. A randomized trial of transcutaneous electric acupoint stimulation as adjunctive treatment for opioid detoxification. J Subst Abuse Treat. 2010;38(1):12–21. doi:10.1016/j.jsat.2009.05.010
97. Bormann NL, Oesterle TS, Arndt S, Karpyak VM, Croarkin PE. Systematic review and meta-analysis: combining transcranial magnetic stimulation or direct current stimulation with pharmacotherapy for treatment of substance use disorders. Am J Addict. 2024. doi:10.1111/ajad.13517
98. Socias ME, Wood E, Le Foll B, et al. Impact of fentanyl use on initiation and discontinuation of methadone and buprenorphine/naloxone among people with prescription-type opioid use disorder: secondary analysis of a Canadian treatment trial. Addiction. 2022;117(10):2662–2672. doi:10.1111/add.15954
99. Thakrar AP, Faude S, Perrone J, et al. Association of Urine Fentanyl Concentration With Severity of Opioid Withdrawal Among Patients Presenting to the Emergency Department. J Addict Med. 2023;17(4):447–453. doi:10.1097/ADM.0000000000001155
100. Amass L, Pukeleviciene V, Subata E, et al. A prospective, randomized, multicenter acceptability and safety study of direct buprenorphine/naloxone induction in heroin-dependent individuals. Addiction. 2012;107(1):142–151. doi:10.1111/j.1360-0443.2011.03577.x
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.