")
Back to Archived Journals » Smart Homecare Technology and TeleHealth » Volume 7
Management of Overweight and Obesity: Technology-Based Interventions Among Generation Y
Authors Marešová P , Hruška J
Received 6 May 2019
Accepted for publication 13 December 2019
Published 6 January 2020 Volume 2020:7 Pages 1—8
DOI https://doi.org/10.2147/SHTT.S214606
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Yelena Yesha
Petra Marešová, Jan Hruška
Department of Economy, Faculty of Informatics and Management, University of Hradec Králové, Hradec Králové, Czech Republic
Correspondence: Petra Marešová
Department of Economy, Faculty of Informatics and Management, University of Hradec Králové, Rokitanského 62, Hradec Králové 500 03, Czech Republic
Tel +420 737929745
Email [email protected]
Background: Obesity is recognized as the most widespread metabolic disease. The growing spread of modern technologies opens new perspectives in treating and caring for people suffering from obesity. The main objective of this paper is to analyze the use of modern technologies among Generation Y (age between 15 and 30) to chart the actual skills of obesity patients.
Methods: The key method used in this paper is a quantitative survey research targeted on generation Y. The two groups “Y” and “non Y” are compared according to numerical and categorical variables. Possible dependences between body mass index and other numerical variables are also analyzed in pairs.
Results: The two groups “Y” and “non Y” do not significantly differ in “hours of physical activities or sports per week” (p>0.33) and in the category of residence size (p>0.10) and they are significantly different in all other variables (p<0.0001). Besides the relatively higher size of sample, the relationships between BMI and three possible numerical variables are not confirmed (p>0.05). Among all respondents, most of them know some obesity-related applications and more than one third uses or used one of them in the past, but only 17.14% of respondents used these applications for active weight loss. Among Generation Y, 41.48% of respondents use an obesity-related application.
Conclusion: Based on the findings of this research, the mobile applications and modern technologies should be considered as a tool with great potential for preventing obesity rather than its treatment.
Keywords: obesity, mobile application, Generation Y, technology
Introduction
Obesity, recognized worldwide as a widespread metabolic illness, reaches in developed as well as in developing countries epidemic dimensions. It affects adults, children and adolescents alike. WHO (World Health Organization) declared obesity a global epidemic and one of the greatest health concerns1 and great socioeconomic consequences.2 Worldwide, the obesity rate from the year 1980 has more than doubled. In 2014, more than 1.9 billion people (older than 18 years) suffered from overweight, and from that number, 600 million suffered from obesity.
The European Commission defines eHealth as follows:
Refers to tools and services using information and communication technologies (ICTs) that can improve prevention, diagnosis, treatment, monitoring and management. It can benefit the entire community by improving access to care and quality of care and by making the health sector more efficient.3
A specific area widely used within eHealth for treatment and care of patients with obesity is telemedicine, defined by the WHO (World Health Organization) as
A cover term for health activities, services and systems operated remotely with information and communication technologies to support global health, prevention and healthcare in health research.4
Contributions of telemedicine consist in monitoring patients at home, shortening the time needed for hospitalization, shortening waiting times, improving the access of consultants and providing overall better options of quality care.5,6
A positive impact of technologies used by people suffering from obesity is demonstrated in a study by Hales et al,7 where using an application for weight loss developed by experts in healthcare focused on self-control and had a clear influence on weight loss.7 Furthermore, Raaijmakers et al8 compared 27 trials in obesity treatment. A total of 13 studies showed significant effects on weight loss compared to controls. Most interventions used a web-based approach (42%). Interventions were screened for five technical key components: self-monitoring, counsellor feedback and communication, group support, use of a structured program and use of an individually tailored program. All interventions that used a combination of all five or four components showed significant losses in weight compared to controls.8
Health-focused mobile applications are proliferating, but before healthcare providers or organizations can recommend an app to the patients they serve, they need to be confident the app will be user-friendly and helpful for the target disease or behavior. The use of mobile technologies to track and improve health outcomes, referred to as mHealth, is a rapidly expanding practice. The advent of smartphone technologies that enable quick and easy access, transfer, and tracking of information, as well as interactive displays and interventions that can be highly engaging, have promoted their adoption. As of June 2019, more than 325,000 health apps existed just in the USA, and the rate of proliferation is nearly exponential. This incredible volume of apps, combined with the rapid evolution of technology and features, makes it difficult for consumers to keep abreast of which apps are available for use by patients.9
What follows from the above mentioned is both the usefulness of technology in obesity treatment and its differing effectivity, determined by the age and skills of users and their BMI. Therefore, the aim of this paper is to analyze the use of selected technologies for preventing and treating obesity with a focus on Generation Y (age between 15 and 30) in the Czech Republic. These dependencies are specifically verified:
-The respondents’ BMI is not related to the number of applications used.
-BMI values are related to the amount of hours per week they spend doing physical activities.
-BMI values are related to the number of hours they spend in front of the TV or computer screen per day.
These relationships are explored across Generation Y and “non Y”.
Methods
Study Population
The source population was defined as all subjects aged between 15 and 30 years, that is, the so-called Generation Y. There are many different sources that describe Generation Y: some sources characterize Generation Y as children born between 1980 and 2000, another study describes it as people born between 1970 and 1990. For the purpose of this study, Generation Y was considered as people who are 15 to 30 years old. For this experiment, Generation Y are persons born around the years 1986 to 2001, which is the corresponding interval in relation to the year of the survey, ie, 2016 (more detailed information on the survey in section Questionnaire design). There is a half-year gap which can create confusion but is explained by the difference between the date when the survey was conducted and the date when this paper was completed. Generation Y is characterized by high digital literacy, which is the reason for our focusing on this group. This characterization, in general, applies to all ranges of birth years mentioned above. The following inclusion criteria were applied: (a) written informed consent; (b) willingness to participate in the questionnaire survey.
Questionnaire Design
Questionnaire design was inspired by the research described in the paper “Exploring the Usability of a Mobile App for Adolescent Obesity Management” by O’Malley et al.10 Questionnaire included 15 questions where the majority of it was a multiple choice. It was divided into four parts and the estimated time for its completion was 5 min. The first part focused on general details, such as gender, age range, weight, height and education. The second part dealt with eating and exercise habits where respondents could write how many hours a week exercise or how many hours a day spend in front of PC or TV screen. The third part was concerned with mobile applications, inquiring which apps the respondents know, which they use, how often they use them and which of the suggested features the apps should offer in order to be more popular. The respondent chose from the following list of applications, which was created by searching the current state of existing solutions for the given year in the given geographical area of the survey conducted. If the respondent used another application, they had the opportunity to write the information (Table 1).
 |
Table 1 List of Applications |
The next part asked for specifications of the apps used by the respondents. These sections were selected to identify how generation Y use apps related to sport and lose weight and how they use them to treat obesity.
A total of 14 questionnaires were filled in incorrectly (missed important questions) and had to be excluded. The final number of respondents was 315 (36.2% male, 63.8% female). The goal of the survey was to target mainly people from Generation Y, so the category between 15 and 30 years is represented by 72.7% (questionnaire was distributed also online so not only individuals from generation Y filled the questionnaire). The sample is not representative of the whole population and therefore should not be used for generalizations. This group was deliberately selected because experts agree on the opinion that this group can have a great influence on future research in many branches, and therefore their opinions and habits can have a significant influence on the whole society.1
The survey was distributed both in the printed version (distributed mostly in schools) and as an online survey (distributed via Facebook) with the help of Google Documents. The survey was in circulation from 8 April 2016 to 17 April 2016. Voluntary completion of the baseline questionnaire implied informed consent. Data were collected anonymously, without reference to the identification of a specific person. The approval of the Ethical Committee of the University of Hradec Kralove is provided.
Statistical Analysis
Statistical analyses of individual respondents were performed using the R Project for Statistical Computing version 3.3.3. MS Excel 2016 was used for data manipulation. A p value of less than 0.05 was considered significant in all cases. The normality of numerical variables and BMI was evaluated using the Chi-square goodness of fit test. It was rejected in all variables, and consequently, median was used to compare the two groups, “Y” and “non-Y”. Specifically, Mood’s Median Test was used to compare medians in the two groups. Three linear models with BMI as dependent variable were tested.
Delphi Method
Delphi method was used to evaluate the feasibility of the results and evaluation of their consequences. A group of experts provided independent opinions on their positions and subsequently analyzed the information. Interviews with experts in this work took place in the week from January 29 to February 2, 2018. Five experts from different fields were involved: software development, medicine, biomedicine, and business economics as those fields fit the topic of the paper.
Results
Sample Characteristics
From a total of 315 respondents, 204 respondents have an optimal BMI ranging between 18.5 and 25 kg/m2. A total of 67 respondents having overweight, with a BMI between 25 and 30 kg/m2. Finally, 20 respondents have obesity, with a BMI higher than 30 kg/m2. The BMI values of the rest of the respondents are lower than 18.5 kg/m2. Underweight respondents were excluded for some tests as the main focus of the paper is on overweight and obese individuals. The most populous age category is that of 15 to 25 years old, accounting for 58.8% of respondents. The second most numerous category is aged from 25 to 30 years, accounting for 12.7%. Finally, the age category under 15 years represents 8.9% of the sample and the age category between 40 and 50 years old accounts for 8.6%.
The gender proportion is made up of 59.5% of women and 40.5% of men. Female respondents with the optimal BMI are represented by 65.7%, but overweight females make up for 55.2% and obese females for 55%. Most respondents live in a city, specifically 55%.
Physical Activity of the Respondents
As to how many hours per day respondents spend in front of the television or computer screen, the most populous category is that of 1 to 3 hrs, represented by 38.1%. The second most populous category is made up of respondents who spend between 3 and 5 hrs a day in front of the screen, accounting for 25.4%. Finally, 19.9% of respondents spend 5 to 10 hrs in front of the screen. With respect to exercise, the most numerous category of respondents, accounting for 35.1%, devotes 1 to 3 hrs per week to physical activities. The second most numerous category, accounting for 18.6%, reports spending 3 to 5 hrs per week exercising. To the question whether they use any app related to sports, weight loss and maintenance or obesity, only 35.1% of respondents answered in the affirmative.
Examined Dependencies in Groups “Y” and “Non-Y”
At the start of statistical analysis, the two groups, “Y” and “non-Y”, were compared (Table 2) to clarify differences between generation Y and others. The following categorical variables were analyzed: sex, education, smartphone use, the question “do you think you have any problem with overweight?” and category of residence. The standard Chi-squared test was used, based on which the two groups differ in the first four variables (p<0.001) but do not differ in the last categorical variable, the category of city (p>0.10).
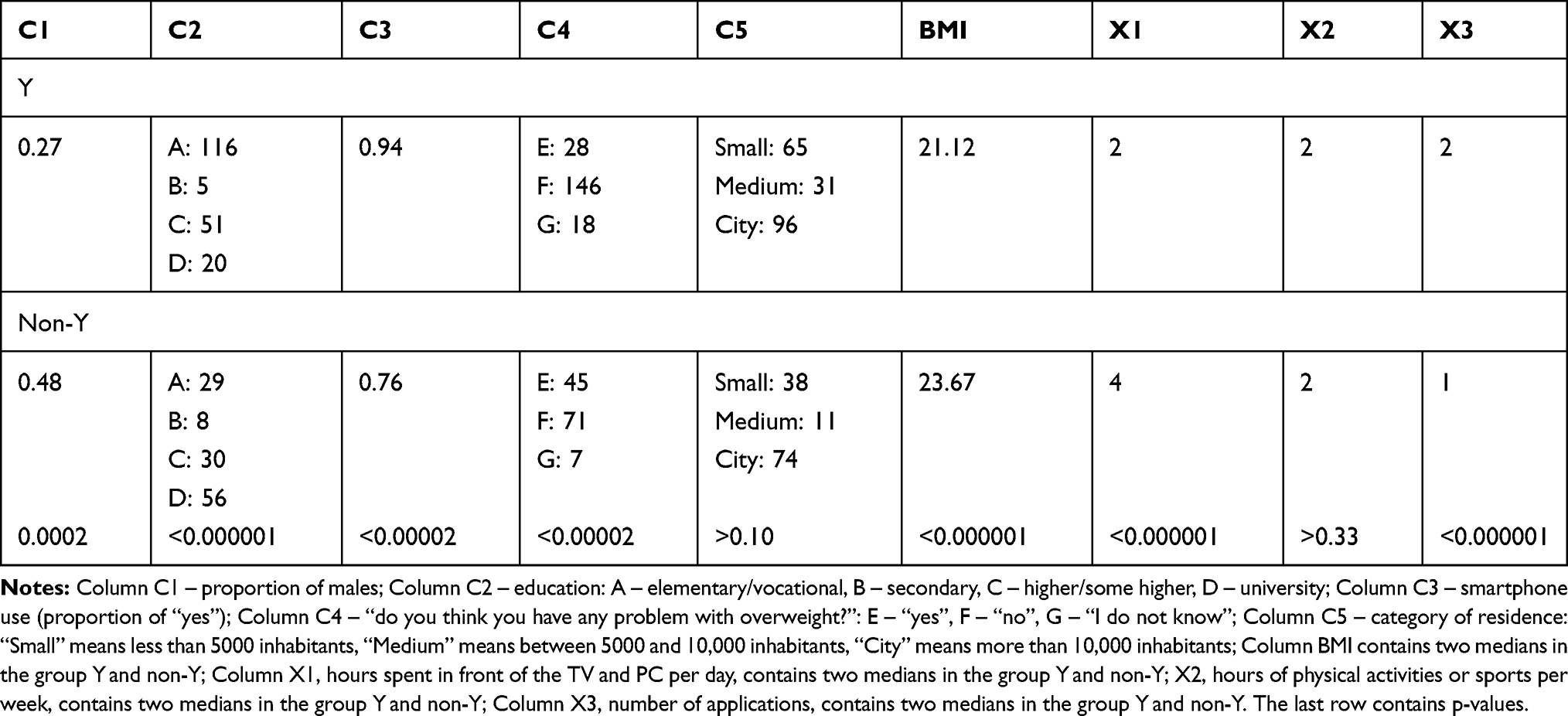 |
Table 2 Result of Statistical Analysis |
Besides that, the following four numerical variables were analyzed: BMI, hours spent in front of the TV and PC per day; hours of physical activities or sports per week and number of applications. Normality was tested in 190 cases in the “Y” group and 123 cases in the “non-Y” group in the four numerical variables.
Normality was rejected in all numerical variables (p<0.0001), and consequently, median was used to compare the two groups. The null hypothesis that medians equal the “Y” and “non-Y” groups was tested using Mood’s test.
Furthermore, BMI was used as a dependent variable in the two linear models with X1, while X2 as an independent variable in each model. X3 was assumed as a dependent variable and BMI as an independent variable in the third linear model. The three models were tested using F-test, and no model is significant (p>0.18; p>0.32; p>0.085). Data used in the three models are shown in Figures 1–3.
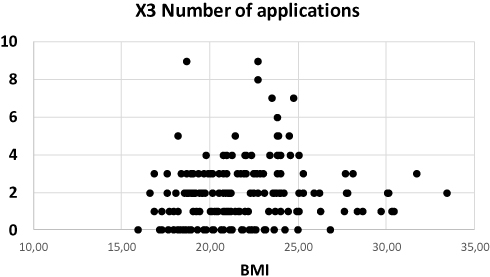 |
Figure 1 Use of applications according to BMI. |
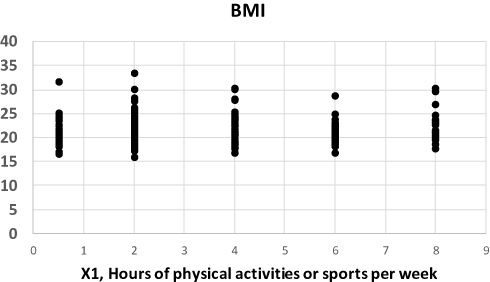 |
Figure 2 Physical activities according to BMI. |
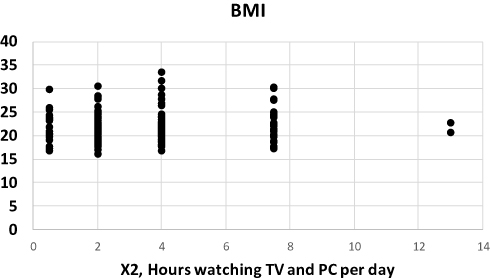 |
Figure 3 Time in front of the screen according to BMI. |
Figures illustrate firstly the number of applications in relation to the X3 variable, shows the BMI of respondents in dependence on the number of applications related to sports, weight loss or obesity they know. The figures illustrate that respondents with a BMI higher than 25, that is, obese respondents, use few apps, mostly 0 to 4. Secondly, BMI in relation to the X1 variable indicates the distribution of the BMI values of respondents according to how many hours per week they spend doing physical activities. And finally, BMI in relation to the X2 variable shows the distribution of respondents according to their BMI and the number of hours they spend in front of the TV or computer screen per day.
Attitudes Towards Use of Technologies and Applications
This section describes the current situation in the field of modern technologies and applications for persons suffering from obesity.
The use of technologies and applications among the respondents is summarized in Table 3. Furthermore, the respondents were asked to consider which functions would induce them to start using weight-control applications. Most respondents checked the answer “Better control of my physical activity” (122 respondents). The respondents also suggested which functionality these applications should have in order to be used by more people. The most frequently selected answer (72%) was “to suggest what and when to eat”. The second most common answer was “to remind me when and how often to exercise” and almost the same number of answers was received by “to evaluate the actual state of my body in detail (for example, statistics, graphs, averages)”. The other suggested answers were: “to support individuals suffering from obesity by important quality information, to support their decision making”, “to increase awareness of these applications, for example, to mediate opinions of doctors and other experts”, “to explain closely step-by-step stories of people who were successfully treated for obesity and their motivation”, “to send information about the condition of the user’s organism directly to doctor”, “to connect better with social media”. All these answers were chosen by less than 30% of the respondents.
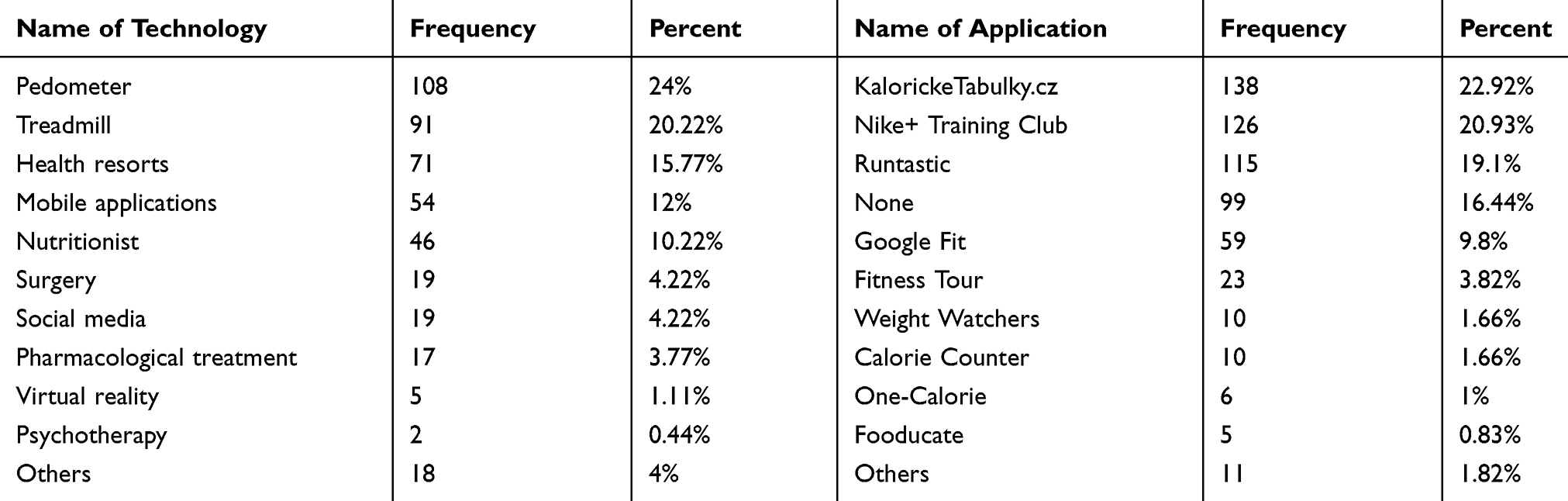 |
Table 3 Frequency of Use of Technologies and Applications |
Expert’s Opinion
The use of technologies and applications from the perspective of future developments was evaluated using the Delphi method. Experts share the same opinion that, due to the proven difference in the use of applications in Y generation and non-Y, generation Y can be considered as an interesting group of customers. It is not considered meaningful to use these applications to target people with obesity, thereby limiting the market potential. There is no evidence that people with obesity are more interested in applications. Due to current IT trends, applications may be perceived as fashionable, with significant potential for sales growth, especially in relation to favorable prices, frequent application updates. In relation to design, it should be a well-visualized application with the possibility of linking to gamification. The application should reflect the elements of a healthy lifestyle linked to promotion in a given culture. The application can also be considered as a tool for communicating with the young generation – millions of mobile phone owners, thus influencing some other aspects of generation Y behaviour. To teach people to use these technologies will be positively reflected in the future in higher use of public electronic systems (mHealth, eGovernment) and brings savings to the public expenditure.
Discussion
The authors of this study were motivated by the connection which is today often made between obesity, behavior of obese people and prevention of obesity with the use of modern technologies and mobile applications.2,6,11–13 Findings of the study indicate that mobile applications are not primarily used for weight loss; for this purpose, the most commonly used tools are pedometers, followed by treadmills. Health resorts rank as the third, while mobile applications rank as the fourth most common method, accounting for less than 50%. Out of a total of 315 respondents, 216 of them know one or more applications in this area (68.57%). From the whole sample, only 113 (35.87%) respondents use such applications. It was proven, as expected, that Generation Y is much more informed and uses more obesity-related mobile applications than other population categories. Among Generation Y, 41.48% of respondents use an obesity-related application. Statically significant differences between the Y and non-Y groups were proven in the use of smartphones (higher in group Y) and the subjective assessment of whether the respondent has an obesity problem or not (higher in group Y).
The assumption that men use weight-control mobile applications more than women was not proved: in both sexes, the number of application users was almost the same (35%). Within Generation Y, another relationship under examination was that between BMI and the number of hours spent in front of a TV or computer screen per day, the number of hours spent exercising per week and the number of applications used. This finding corresponds to studies focused on the use of these tools, which clearly suggest that the most frequently used and most effective tools are those that target not only treating obesity but also preventing it.13–15
Based on the findings of this research, the authors believe that mobile applications and modern technologies should be considered exclusively as a tool for preventing obesity rather than its treatment. This is ultimately confirmed by numerous clinical studies that evaluated the effectiveness of technology-based interventions and explored components of these interventions that are associated with significant BMI outcomes. None of the 14 studies under examination proved a dependence between the use of technology and the successful treatment of obesity.13 In terms of preventing obesity, however, mobile applications hold a great potential because the use of smartphones is still on the rise, and their users are young people8 who can effectively utilize the mobile applications that they install. Weight loss and management applications should be the result of coordinated efforts of developers, nutrition specialists, physicians and the users themselves. Before such applications are introduced to the public, it should be ensured that they are based on the latest research findings and that they include all the functionality required for effective weight management.
The limitations of the current study are related to the structure of the collected data. The non-Y group was not examined in sufficient detail as to the age of the respondents: the maximum age was 50 and above, but it is possible that the results in the different age groups above 50 would show further variations. Regarding the size of the study sample (315 respondents), it was sufficient to prove statistically significant differences between the Y and non-Y groups. Each of these groups included a sufficient number of respondents. On the other hand, the research of dependencies within the Y group did not lead to confirming the assumed differences. In this group, although it was larger than the non-Y group, the number of respondents was not high enough to confirm the expected relationships among the numerical variables. The relatively higher number of cases was compensated by a greater variability, that is, other influencing factors. The above-described study did not capture several significant aspects related to the topic in question, including the doctors’ knowledge of modern technologies and their possibilities. As doctors play a vital role in treating diseases,16 they are extremely important when it comes to disseminating technologies among patients. Doctors can, therefore, be the essential element not only in developing applications but also in their introduction into the market and their more efficient use in qualitative as well as quantitative terms.
Conclusion
The main causes of obesity nowadays are considered poor eating habits together with decreased physical activity. Furthermore, the reduction of physical activity is often associated with a greater use of IT especially in young people for the purpose of leisure. On the other hand, obesity and obesitology is a medical field in which remote communication can be applied. Self-monitoring of obese patients, lifestyle changes, diet regimen and physical activity are critical in weight loss. Professional medical supervision is possible through information and telecommunication technologies, via the Internet or smartphones. The benefit is the possibility of regular communication, both synchronous (in real time) and asynchronous (eg, via e-mail). In this context, modern technologies also have a great potential to succeed and help solve the obesity problem, especially among young people. Child obesity is becoming a much-debated topic in telemedicine as well. Over the past 30 years, the number of obese adolescents has tripled. Recent results of the study show that the potential of IT for treatment is not fully realized. In the context of the Czech Republic, where the research has been realized, it is possible to look for causes not only on the side of the patient but also on the side of doctors, where online communication and sharing this type of data is not common practice. However, for physicians, monitoring of continuous measurement results may mean faster detection of potential health risks of the patient. Nevertheless, with the further development of the eHealth area, it can be expected that this area of patient care will be strengthened. The patient’s side is ready.
Acknowledgments
This study was supported by the project Excellence 2019 (University of Hradec Kralove, Faculty of Informatics and Management) and internal research of Faculty of Informatics and Management, University of Hradec Kralove.
We would like to acknowledge Dr. Dolejs for his help with statistical analysis.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tapscott D. Grown Up Digital: How the Net Generation Is Changing Your World. New York: McGraw-Hill; 2009.
2. Schoffman DE, Turner-McGrievy G, Jones SJ, Wilcox S. Mobile apps for pediatric obesity prevention and treatment, healthy eating, and physical activity promotion: just fun and games? Transl Behav Med. 2013;3(3):320–325. doi:10.1007/s13142-013-0206-3
3. European Commission. Overview | Public Health. Available from: https://ec.europa.eu/health/ehealth/overview_en.
4. WHO Global Observatory for eHealth. MHealth: New Horizons for Health Through Mobile Technologies. Geneva: World Health Organization; 2011.
5. Pelosi P, Gregoretti C. Perioperative management of obese patients. Best Pract Res Clin Anaesthesiol. 2010;24(2):211–225. doi:10.1016/j.bpa.2010.02.001
6. Park HS, Park CY, Oh SW, Yoo HJ. Prevalence of obesity and metabolic syndrome in Korean adults. Obes Rev. 2008;9(2):104–107. doi:10.1111/j.1467-789X.2007.00421.x
7. Hales S, Turner-McGrievy GM, Wilcox S, et al. Social networks for improving healthy weight loss behaviors for overweight and obese adults: a randomized clinical trial of the social pounds off digitally (Social POD) mobile app. Int J Med Inform. 2016;94:81–90. doi:10.1016/j.ijmedinf.2016.07.003
8. Raaijmakers LCH, Pouwels S, Berghuis KA, Nienhuijs SW. Technology-based interventions in the treatment of overweight and obesity: a systematic review. Appetite. 2015;95:138–151. doi:10.1016/j.appet.2015.07.008
9. Boudreaux ED, Waring ME, Hayes RB, Sadasivam RS, Mullen S, Pagoto S. Evaluating and selecting mobile health apps: strategies for healthcare providers and healthcare organizations. Transl Behav Med. 2014;4(4):363–371. doi:10.1007/s13142-014-0293-9
10. O’Malley G, Dowdall G, Burls A, Perry IJ, Curran N. Exploring the usability of a mobile app for adolescent obesity management. JMIR Mhealth Uhealth. 2014;2(2):e29. doi:10.2196/mhealth.3262
11. Yoo J-H. The meaning of information technology (IT) mobile devices to me, the infectious disease physician. Infect Chemother. 2013;45(2):244. doi:10.3947/ic.2013.45.2.244
12. Flores Mateo G, Granado-Font E, Ferré-Grau C, Montaña-Carreras X. Mobile phone apps to promote weight loss and increase physical activity: a systematic review and meta-analysis. J Med Internet Res. 2015;17(11):e253. doi:10.2196/jmir.4836
13. Chen Y. Integrated and intelligent manufacturing: perspectives and enablers. Engineering. 2017;3(5):588–595. doi:10.1016/J.ENG.2017.04.009
14. Zaidan S, Roehrer E. Popular mobile phone apps for diet and weight loss: a content analysis. JMIR Mhealth Uhealth. 2016;4(3):e80. doi:10.2196/mhealth.5406
15. Rivera J, McPherson A, Hamilton J, et al. Mobile apps for weight management: a scoping review. JMIR Mhealth Uhealth. 2016;4(3):e87. doi:10.2196/mhealth.5115
16. Maresova P, Cerna L. Patients’ attitudes to the use of modern technologies in the treatment of diabetes. Patient Prefer Adherence. 2016;10:1869–1879. doi:10.2147/PPA.S118040
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.