")
Back to Journals » Orthopedic Research and Reviews » Volume 16
Management of Garden-I and II Femoral Neck Fractures: Perspectives on Primary Arthroplasty
Authors Olansen J , Ibrahim Z , Aaron RK
Received 11 August 2023
Accepted for publication 22 December 2023
Published 3 January 2024 Volume 2024:16 Pages 1—20
DOI https://doi.org/10.2147/ORR.S340535
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Clark Hung
Jon Olansen, Zainab Ibrahim, Roy K Aaron
Department of Orthopedic Surgery, Warren Alpert Medical School of Brown University, Providence, RI, USA
Correspondence: Roy K Aaron, University Orthopedics Inc., 2 Dudley Street, Ste. 200, Providence, RI, 02906, USA, Tel +1-401-274-9660, Fax +1-401-270-1560, Email [email protected]
Abstract: This review compares internal fixation versus arthroplasty in the treatment of nondisplaced femoral neck fractures (FNFs) calling attention to evolving areas of consensus that influence clinical decision-making. The Garden classification system, typically dichotomized into nondisplaced (types I and II) and displaced (types III and IV) fractures, has been used as a guide for surgical decision-making. Conventionally, treatment of nondisplaced FNF in the elderly has been with internal fixation, and treatment of a displaced FNF has been hemi-, or more recently total hip, arthroplasty. Studies over the last decade have raised concern over the appropriate treatment of nondisplaced FNFs due to high rates of reoperation of nondisplaced FNFs treated with internal fixation. Avascular necrosis (AVN), failure of internal fixation, secondary malunion, and pin/nail penetration through the femoral head have all been observed. Several studies have attributed fixation failure to a degree of femoral neck tilt ≥ 20°, either posteriorly or anteriorly as seen on the lateral X-ray. Because of these observations of fixation failures, the suggestion has been made that arthroplasty be used when the degree of posterior tilt exceeds a threshold of ≥ 20° tilt with the expectation of diminishing failure of fixation, decreasing the risk of reoperation and preserving function without increasing mortality rate. Frustrating additional analyses are uncertainties over the mechanisms of failure of internal fixation with ≥ 20° tilt and the persistently substantial 1-year mortality rate after FNF, which has not been influenced by fixation or replacement type. Due to the lack of consensus regarding the determination of the appropriate surgical intervention for nondisplaced FNFs, an improved algorithm for surgical decision-making for these fractures may prove useful.
Keywords: nondisplaced, internal fixation, hip arthroplasty, posterior tilt, mortality, reoperation
Introduction
Surgical treatment of femoral neck fractures (FNFs) has varied over the years. Constructs have included screw and pin fixation, static and dynamic hip screws, hemiarthroplasty, and total hip arthroplasty. The treatment of FNFs reflects progress not only in our understanding of the vasculature and biomechanics of the femoral head and neck but also in the development of orthopedic implants and devices. Traditionally, nondisplaced FNFs have been treated with in situ stabilization, while displaced fractures have been treated with replacement arthroplasty. These fractures often occur in elderly and, very frequently, fragile individuals. Less invasive procedures have been preferred in this demographic to minimize surgical trauma including blood loss, muscle dissection, and anesthesia time. However, this treatment algorithm has been questioned because of relatively high failure rates which then necessitate reoperation.
The epidemiology of FNFs is significant for several reasons. With an aging population and the increased prevalence of osteoporosis globally, the incidence of hip fractures is increasing along with associated mortality. As reported by the World Health Organization, the global population aged ≥85 will increase 4.5-fold from 2010 to 2050 and, concurrently, the global incidence of FNFs is estimated to rise to 2.6 million annually by 2025 and at least 4.5 million by 2050.1–3 As these numbers rise, further investigation into reasons for treatment failures is imperative to ensure optimum surgical management and mortality mitigation.
While several studies report that treatment of FNFs via internal fixation is not satisfactory due to a high rate of complication, many other studies still advocate internal fixation because of its advantage as a minimally invasive method with less blood loss and surgical trauma, and shorter operation time as compared to arthroplasty.4–7 Comparative studies of internal fixation and arthroplasty for the treatment of FNFs are difficult to do because limited access to the medical history of the pre-injured patient may create unmatched cohorts and introduce inadvertent bias. Additionally, the complications of internal fixation and arthroplasty are distinct from one another. Although the revision rates of arthroplasty tend to be lower than internal fixation, the potential complications are, on average, much greater. Both, however, are characterized by substantial and essentially equivalent mortality rates. Randomized clinical trials (RCT) have been done infrequently and with small cohort sizes. It may be that larger RCT cohorts are needed to balance these confounding factors. Although several RCTs have been published, only one identified study has substantial sample size. Additional RCTs are warranted to compare these two treatment methods.
This review presents seminal reports of observations, methods of measurement, and outcomes of the treatment of nondisplaced (Garden I and II) FNFs to examine if a current treatment consensus can be reached. We consider outcomes in the categories of mortality, postoperative function, perioperative complications, and reoperation. Finally, we explore several unresolved issues, particularly regarding mechanisms of failure and impacts on function, so that further refined treatment indications may be agreed upon.
The Garden Classification
Classification systems can serve numerous functions, including prediction or prognosis, evaluation of stability, or simply description. In 1961, R.S. Garden proposed a classification system for intracapsular FNFs that provided prognostic information about outcomes of surgical treatment and has strongly influenced surgical decision-making.8 The system is simple and is based upon the nature and extent of angular deformity and displacement of the femoral neck on AP radiographs, with prognostic implications for healing of the FNF and survival of the femoral head.
The Garden classification was foundationally based exclusively on anteroposterior radiographs with no consideration of alignment on lateral X-rays. Garden types I and II are nondisplaced fractures, with Garden I indicating a valgus-impacted incomplete fracture and Garden II indicating a complete but nondisplaced fracture. Conversely, Garden types III and IV are both displaced. Garden III is a complete fracture with partial displacement and Garden IV is a complete fracture with complete displacement as indicated by parallel orientation of the trabeculae (Figure 1).8
 |
Figure 1 Garden classification system of femoral neck fractures. (A) Garden Type I. (B) Garden Type II. (C) Garden Type III. (D) Garden Type IV. Notes: Reproduced with permission from Kazley JM, Banerjee S, Abousayed MM, Rosenbaum AJ. Classifications in Brief: Garden Classification of Femoral Neck Fractures. Clin Orthop Relat Res. 2018;476(2):441–445.9 |
Internal Fixation
To determine the appropriate role of arthroplasty, an understanding of the failure rates of internal fixation is beneficial. Until recently, the clinical consensus suggested that internal fixation should be the treatment of choice for nondisplaced (Garden I or II) FNFs.10 In patients with displaced fractures (Garden III or IV), a decision would have to be made whether to reduce and internally fix the fracture or to perform an arthroplasty.10 Shah et al developed a flowchart in 2002 to describe the appropriate intervention for FNFs. This decision-making tool indicated, simply, that the appropriate treatment for nondisplaced fractures was cannulated screw fixation.11 Many patients with nondisplaced FNFs are elderly and frail, and much of the appeal of internal fixation in this group is that it allows for shorter surgical time, less blood loss, and reduced surgical trauma. The treatment algorithm for nondisplaced FNFs began to unravel with the recognition that surgical failure and reoperation rates of internally fixed FNFs ranged from 8% to 21%, whereas arthroplasty maintains a less frequent rate of reoperation ranging from 2% to 7%.12,13
Several different strategies exist for internal fixation of FNFs, including dynamic hip screws and cancellous screws. The robust 2017 “Fixation using Alternative Implants for the Treatment of Hip fractures” (FAITH) trial determined the efficacy of sliding hip screws (n=557) as compared to cancellous screws (n=551) in terms of risk of reoperation and other, patient reported, outcomes.14 Patients who had experienced low-energy FNFs, the majority of which were nondisplaced, were randomly assigned to one of the two cohorts. Many demographic characteristics were similar between the cohorts, including age, sex, ethnicity, pharmaceutical use, BMI, smoking history, laterality, mechanism of fracture, and additional injuries. The study included FNFs at various levels in the neck and all four Garden types. The study determined that an age ≥80 years was associated with increased risk of reoperation as compared to those in a younger demographic (15.3% [35 of 229]; HR, 3.88; 95% CI, 1.16 to 12.90; P = 0.03). Also noted, when considering patients with all 3 of the risk factors with observed trends (ie, posterior tilt ≥20°, age ≥80 years, and being of the female sex), the failure rate was 42.9% (6 of 14).15 Risk factors such as these must be considered in the surgical decision-making process because of their impact on perioperative and intraoperative complications.
Although poor bone quality is commonly cited as a reason for failure of internal fixation, a study by Viberg et al did not find any association with fixation failure and low bone mineral density (BMD; T-score below 2.5 standard deviations from the reference) in a series of 140 patients treated with multiple cancellous screws who had DEXA scans postoperatively.16 In another prospective study comparing outcomes in patients with displaced FNFs, DEXA scans found similar BMD in osteoporotic and osteopenic patients with fixation failure. The rate of failure was also insignificantly different when comparing osteoporotic to osteopenic patients (42% vs 41%, P=0.87).17 However, factors that influence the hip BMD measurement must also be considered. BMD of the hip is not constant and declines in the elderly population by approximately 0.5% per year, which may partially be attributed to declines in activity. The few studies that address the question of BMD in relation to outcomes of nondisplaced FNF treatment either lack adjustment for confounding variables or do not report critical information such as reduction quality or preoperative displacement. As such, further detailed studies are needed to determine the relationship between BMD and risk of FNF fixation failure.
The role of posterior tilt, or apex anterior fracture angulation, has also been cited as a reason for construct failure. A method of measuring posterior tilt on lateral X-rays was described by Palm et al as the angle between the mid-femoral neck and the head-neck segment on either side of the fracture (Figure 2). The posterior tilt measured according to their method combines posterior angulation and displacement between the femoral head and neck, both of which may influence the stability of the fracture and the vessels passing the fracture area.18
 |
Figure 2 AP (left) and lateral (right) radiographs of a Garden II femoral neck fracture demonstrating posterior tilt (a) measured as the angle between the mid-column (neck) line (MCL) and the radius column (neck) line (RCL), drawn from the center of the femoral head (C) to the point at which the femoral head and MCL cross. Notes: Reproduced with permission from Palm H, Gosvig K, Krasheninnikoff M, Jacobsen S, Gebuhr P. A new measurement for posterior tilt predicts reoperation in undisplaced femoral neck fractures: 113 consecutive patients treated by internal fixation and followed for 1 year. Acta Orthop. 2009;80(3):303–307.18 |
However, a lack of consensus regarding the role of posterior tilt in surgical failure persists. Conn and Parker evaluated a cohort of 3444 patients with nondisplaced FNFs and found that, generally, the presence of posterior tilt was a statistically significant predictor of nonunion, but not of subsequent AVN.19 To clarify this, Palm et al assessed reoperations due surgical failures according to specific degrees of preoperative posterior tilt.18 Of the study cohort of 113 patients, 26 (23%) required reoperation because of surgical failure caused by nonunion, AVN, infection, additional fracture, or device penetration through the femoral head. An additional 5 patients had reoperations for implant irritation or infection. To assess the threshold at which tilt becomes clinically significant, the degree of posterior tilt was stratified as being <20° or ≥20°. 14/25 (56%) patients with preoperative, posterior tilt of ≥20° required reoperation compared to 12/88 (14%) with <20° (p<0.001) (Figure 3). Of the many clinical factors analyzed by logistic regression, posterior tilt of ≥20° was the only predictor of reoperation. 21/113 (19%) of the patients died within the first postoperative year.18 The authors concluded that, postoperatively, neither the positioning of the implants nor the fracture reduction influenced the reoperation rate. Rather, they suggested that reoperation may instead be associated with preoperative posterior tilt, which may cause injury to the retinacular vessels resulting in AVN or may create a more unstable fracture pattern.18
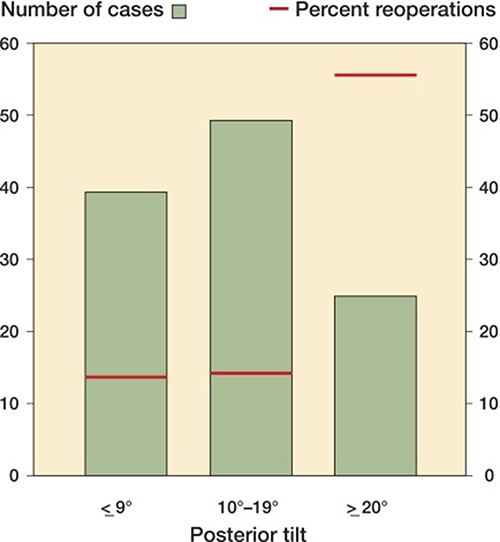 |
Figure 3 Distribution of posterior tilt and rates of reoperation in the 113 patients who were operated on with internal fixation for a Garden I or II femoral neck fracture. Bar graphs represent the total number of cases and red lines represent the percent of the group that underwent reoperation, shown to be disproportionately greater in patients with a posterior tilt >20°. Notes: Reproduced with permission from Palm H, Gosvig K, Krasheninnikoff M, Jacobsen S, Gebuhr P. A new measurement for posterior tilt predicts reoperation in undisplaced femoral neck fractures: 113 consecutive patients treated by internal fixation and followed for 1 year. Acta Orthop. 2009;80(3):303–307.18 |
In response to this new method of measurement proposed by Palm et al, a 2012 cohort study aimed to validate the claim that posterior tilt was indeed a preoperative risk factor influencing reoperation rate after internal fixation of Garden type I and II FNFs. The participants were divided into three groups by degree of posterior tilt identified on lateral radiograph: 0–9° (n=170), 10–19° (n=139), and ≥20° (n=73). Among the three groups, there were no significant differences in rate of reoperation (P = 0.3) and no significant differences in mortality.20 These observations questioned the clinical significance of the measurements of Palm et al and Conn and Parker, which claimed posterior tilt should be identified as a preoperative risk factor and guide surgical decision-making. Palm acknowledged that leg rotation could detract from the accuracy of the measurements made using his method and an element of standardization may need to be adopted in taking the lateral film.
The clinical data are very compelling and point to 20° as a decision point for surgery (Table 1). However, common radiographic experience reveals that angulation can appear quite differently depending upon how the bone is rotated relative to the X-ray beam (Figure 4). Studies pointing out the importance of femoral neck tilt in surgical decision-making did not report consistent beam positioning relative to the femoral neck. As it would be difficult to do, in any event, in the fracture patient, it is worth considering if there is any influence of proximal femoral positioning on the perception of femoral neck tilt. As Palm suggests in his rebuttal to the observations made in Lapidus et al, positioning of the femoral head and neck is critical for proper evaluation. As seen in the image below, simple rotation of the femur can result in variability in the perceived femoral neck angle. This is also true for lateral radiographs. Therefore, formulation of a standardizing procedure when obtaining radiographs, such as through manipulation to achieve anatomical position or the use of stirrups, may prove useful.12
 |
Figure 4 Example with a proximal femur model within a fixed direction X-ray beam demonstrates that rotation of the bone within the beam produces varying perceptions of femoral neck angle. (1) femoral neck angle measured to be 130°, (2) measured to be 134°, (3) measured to be 149°, and (4) measured to be 142°. |
 |
Table 1 Reoperation Rates in Studies of Nondisplaced FNF Repair Comparing Preoperative Tilt |
Two contemporary, retrospective studies using the Swedish registry data revisited this method of measurement of nondisplaced FNFs, supplementing with an evaluation of anterior tilt as well. In agreement with Palm’s observations, the overall reoperation rate of internal fixation in one study was 69/417 (17%). This revealed a relative risk (RR) of treatment failure of 5.5 (95% CI, 2.8 to 11) in patients with a preoperative anterior tilt of ≥10° and 2.2 (95% CI, 1.2 to 3.8) in those with a posterior tilt of ≥20°.21 In addition, the hazard ratio was identified to be significant in patients with an anterior tilt of ≥10° and a posterior tilt of ≥20°.
The concurrent consideration of anterior tilt with posterior tilt was a novel development at the time and, therefore, required additional confirmation with greater numbers. To do so, Sjoholm et al used the Swedish registry once more to confirm these observations in a group with a mean age of 81, finding again an overall internal fixation reoperation rate of 17% (Figure 5). In this reexamination, the reoperation rates of fractures with a posterior tilt ≥20° and anterior tilt ≥10° (22% and 35%, respectively) were disproportionately higher than in those with posterior tilt <20° (15%).22 This is suggestive that arthroplasty as an initial intervention for a subgroup of elderly fracture patients with a posterior tilt ≥20° may prove beneficial, as this may avoid complications such as AVN or nonunion, and subsequent reoperation. The outcomes of arthroplasty in elderly patients with FNF would need to be determined and this is presented, to the extent known, in subsequent sections.
 |
Figure 5 Graph showing the risk of treatment failure (Hazard Ratio) as a function of tilt in degrees. Anterior tilt corresponds with negative values on the x-axis. Posterior tilt corresponds with positive values on the x-axis. Vertical blue lines represent the significant hazard ratios. The values are adjusted for sex, American Society of Anesthesiologists (ASA) classification, sheltered housing, implant inclination, cognitive impairment, and postoperative fracture tilt. The light blue area corresponds to the 95% CI. Notes: Modified from Sjöholm P, Sundkvist J, Wolf O, Sköldenberg O, Gordon M, Mukka S. Preoperative Anterior and Posterior Tilt of Garden I–II Femoral Neck Fractures Predict Treatment Failure and Need for Reoperation in Patients Over 60 Years. JB JS Open Access. 2021;6(4):e21.00045. Creative Commons.22 |
A more recent systematic review and meta-analysis of cohort studies examined the contribution of posterior tilt in nondisplaced FNFs to fixation failure.23 Studies included in this review were comprised of patients who had been treated with internal fixation and did not consider the outcomes of arthroplasty. Thirteen high-quality trials were included, which resulted in a pooled cohort of 4818 patients. Of these patients, 698 had a posterior tilt of ≥20°, 3578 had a posterior tilt of <20°, 483 had a posterior tilt of ≥10°, and 496 patients had a posterior tilt of <10°. Treatment failures were observed in 170/698 (24%) of patients with posterior tilt ≥20° and 392/3578 (11%) of patients with posterior tilt <20° (RR 2.73). Four of the included studies also evaluated 10° of posterior tilt as a threshold of difference in the way the fractures behave. Within these studies, a tilt ≥10° was not associated with an increased risk of failure of fixation compared to a tilt <10°, indicating that a degree of tilt ≥10 is not a valid threshold to utilize as a risk factor for treatment failure.23 Thus, Garden I and II FNFs with a significant preoperative posterior tilt (≥20°) appear to behave like unstable fractures and have a four times higher risk of failure.24 This behavior has suggested to some observers that this potential failure may be indicative of the role that arthroplasty can play in surgical decision-making.
Song et al reported that, of 308 patients with nondisplaced FNF treated with internal fixation, 32 (10.3%) experienced failed treatment. Complications included biomechanical failure (3.2%) and AVN (7.1%). The three factors noted to have an association with failure were an initial valgus tilt ≥15° (p = 0.001), an initial posterior tilt ≥15° (p < 0.001), and the distance of the sliding of the implanted screw (p < 0.001).24 It was suggested that a posterior tilt greater than 15° causes fractures to become unstable by widening the fracture gap, potentially causing vascular disruption, which could predispose subsequent treatment to fail.
With new understanding of the impact of posterior tilt on these potentially unstable fractures, Kamara et al proposed a treatment algorithm specifically designed to address the issue of posterior tilt, adding to the previous algorithm proposed by Shah et al. These algorithms suggested dichotomously that if a Garden I or II fracture’s posterior tilt is found to be ≥20° in a patient over 65 years of age without severe medical comorbidities, arthroplasty is the intervention of choice.25 This is consistent with the findings of Palm, Song, and several of the studies included in the meta-analysis conducted by Wang et al, based upon the observations that primary arthroplasty has been shown to minimize revision surgery rates without significantly increasing mortality rates. However, the treatment algorithm contained an arbitrary age threshold, an ambiguous use of “severe medical comorbidities” as an indicator for non-operative treatment, and a reliance on Palm’s method of measuring posterior tilt which may benefit from amendment.
Mechanisms of Failure
Although substantial literature is available supporting the management of nondisplaced FNFs with internal fixation, complication rates are still unacceptably high, reinforcing the case that arthroplasty may be the more suitable technique to treat these fractures. While a considerable number of studies have described biomechanical failure of the bone-implant construct, little is known about the contribution of bone to the mode of failure. Opportunities for bone failure could include femoral neck comminution and osteoporosis while surgical contributions could include inappropriate hardware placement.
Vascular and biomechanical factors might have critical influence upon the surgical decision-making process in the hip fracture population. One of the best studies investigating the failure mechanisms of internal fixation reflects injury to the ascending retinacular vessels along the femoral neck with consequent under-perfusion of the femoral head and segmental ischemia leading to AVN. Tenuous blood supply to the femoral head and neck is believed to be the primary etiologic factor for the vascular complications following surgery, ie AVN.26 The retinacular system of vessels branches off the circumflex arteries, traverses along the femoral neck, and penetrates the femoral capsule. The superior and inferior retinacular arteries are implicated as significant arterial suppliers of the femoral head, as demonstrated by several MRI studies.27 Vascular trauma as a result of an FNF could result in the disruption of these retinacular vessels that perfuse the area, creating regional ischemia and possibly creating a tamponade effect of hematoma within the intracapsular space.28 In a nondisplaced FNF, the compression side is often comminuted; a vascular insult could be caused by either compression or tension. Disruption of femoral head and subchondral bone perfusion is believed to result in the subsequent development of AVN.29 Liu et al showed that the rate of AVN after a femoral neck fracture was directly linked to the number of vessels crossing the fracture line, resulting in impaired perfusion and ischemia of bone cells, which is followed by cell death.30,31 Necrosis of bone cells and the subsequent stages of repair, particularly the resorption process, results in significant structural changes and loss of integrity at the fracture site.32 Therefore, quality reduction, stable internal fixation, and preservation of the intact blood supply to the fracture site are critical if one is to avoid AVN or subsequent reoperation.
Several different modalities have been used to better understand the specifics of fracture-induced ischemia. At the macroscopic scale, Dyke et al used dynamic contrast MRI analysis to examine blood supply to the femoral head following a displaced FNF. Quadrant specific analysis found statistically significant decreases in arterial perfusion and venous outflow in the femoral heads of patients with displaced FNFs. These parallel processes together have a synergistic effect in compromising the viability of osteocytes leading to structural compromise of the femoral head.26
Radionuclide scintigraphy has also been used to examine blood supply, and it has been noted that an area of decreased tracer uptake indicating perfusion deficit (a so-called “cold deficit”) can be an early scintigraphic sign of AVN of the femoral head.33 Han et al performed a study of internal fixation of Garden I and II that fractures examined radiotracer uptake patterns of the femoral head on postoperative bone SPECT/CT and subsequent AVN. In patients with Garden I and II fractures, 15/39 showed normal femoral head uptake and 24/39 showed cold defects on immediate postoperative SPECT/CTs but did not go on to develop AVN.33 However, cold defects at 2–5 months follow-up were associated with the development of AVN. Figure 6 shows a similar perioperative cold defect in a femoral head that does go on to develop AVN in the superolateral quadrant. Normal uptake on SPECT/CT indicates intact vascularity, which is necessary for healing of FNFs following fixation.34 It is important to recognize that patients with nondisplaced FNFs may experience a greater vascular insult than what has previously been believed.
 |
Figure 6 A preoperative radiograph of a 72-year-old male with right Hip pain shows a right femoral neck fracture (Garden stage III) (a). The immediate postoperative bone SPECT (b) and SPECT/CT fusion (c) images at 3 days show a cold defect of the right femoral head. The follow-up bone SPECT (d) and SPECT/CT fusion (e) images at 3 months show partially normalized uptake with the remaining defect in the superior portion of the right femoral head. Postoperative radiograph (f) at 15 months shows avascular necrosis of Ficat stage III with subchondral collapse of the right femoral head. Arrows represent ischemic region. Notes: Reproduced with permission from Han S, Oh M, Yoon S et al. Risk Stratification for Avascular Necrosis of the Femoral Head After Internal Fixation of Femoral Neck Fractures by Post-Operative Bone SPECT/CT. Nucl Med Mol Imaging. 2017;51(1):49–57. Springer Nature.33 |
For example, another outcome of significance between the two methods of internal fixation in the FAITH study was the frequency with which avascular necrosis (AVN) developed when using a sliding hip screw compared to cancellous screws. Interestingly, this study affirms the efficacy and lower reoperation rate of cancellous screws for most patients, while suggesting sliding hip screws may be more effective in those with displaced fractures, basicervical fractures, and fractures sustained by active smokers. AVN developed in 50/557 (9%) of sliding hip screw patients compared to 28/551 (5%) of cancellous screw patients (hazard ratio [HR] 1.91, 1.06–3.44; p=0.032). The primary outcome, reoperation rate, did not differ between the two groups (HR 0.83, 95% CI 0.63–1.09; p=0.18). However, while reoperation rates were not significantly different, they remained high for both types of internal fixation (21% overall) as compared to the reoperation rates observed in arthroplasty.14
Although Garden I and II fractures are less likely to go on to AVN following fixation compared to Garden III and IV fractures, the fact that any number of them do suggests that some degree of injury to the blood supply is occurring. The close relationship of the retinacular vessels to the femoral neck makes them particularly susceptible to damage (Figure 7). Several studies have shown that isolated vascular insult is almost always dependent upon the retinacular arteries, so it may also be considered that the process of performing internal fixation of the femoral neck itself can further exacerbate vascular insult and cause subsequent AVN if the retinacular vessels are compromised.35–37
 |
Figure 7 Anatomical dissection demonstrating the metaphyseal retinacular vessels as they traverse the femoral neck and supply the femoral head. Fracture of the femoral neck can cause rupture or shearing of the vessels, subsequently leading to AVN and mechanical failure. |
Although often mentioned briefly in many studies, there has been little investigation into the contribution of fracture stability and comminution to the success of internal fixation. Some point to comminution and impaction as the stabilizing factor in a nondisplaced FNF, while others suggest that subsequent reoperation may be dependent upon the quality and stability of the reduction. While discussion has been quite robust regarding the association of preoperative tilt with reoperation and mortality rate, there have been fewer considerations concerning the role of successful or unsuccessful reduction of postoperative tilt seen in nondisplaced FNFs. A retrospective study of 96 patients suggested that fracture reduction is crucial to the success of internal fixation. On average, the preoperative posterior tilt was 28°, and the preoperative valgus tilt was 11° on CT. The postoperative posterior tilt, however, was corrected to an average of 3° and the valgus displacement to 5°. Upon follow-up, the authors explain that significant closure of the posterior gap on the lateral view radiographs and the CT scans was consistent with unchanged, stable, long-term postoperative near-physiologic position. It was concluded that most of the complications found in surgeries can be avoided by appropriate reduction of the posterior tilt (Figure 8).38 Recent three-dimensional analysis of Garden type I fractures support this sentiment. These fractures were observed to have deceivingly large measurements of displacement, calling into question the decision for nonsurgical treatment of nondisplaced FNFs.39 This is contrary to the discussion in Palm et al who suggested that only the degree of preoperative tilt is a strong indicator for reoperation. The potential impact of posterior tilt on the success of internal fixation of nondisplaced FNFs should be cause for evaluation of postoperative reduction as a predictor of subsequent failure. Future investigations with larger cohorts and updated procedures may elucidate the role preoperative tilt and postoperative reduction play in subsequent development of complications and reoperation.
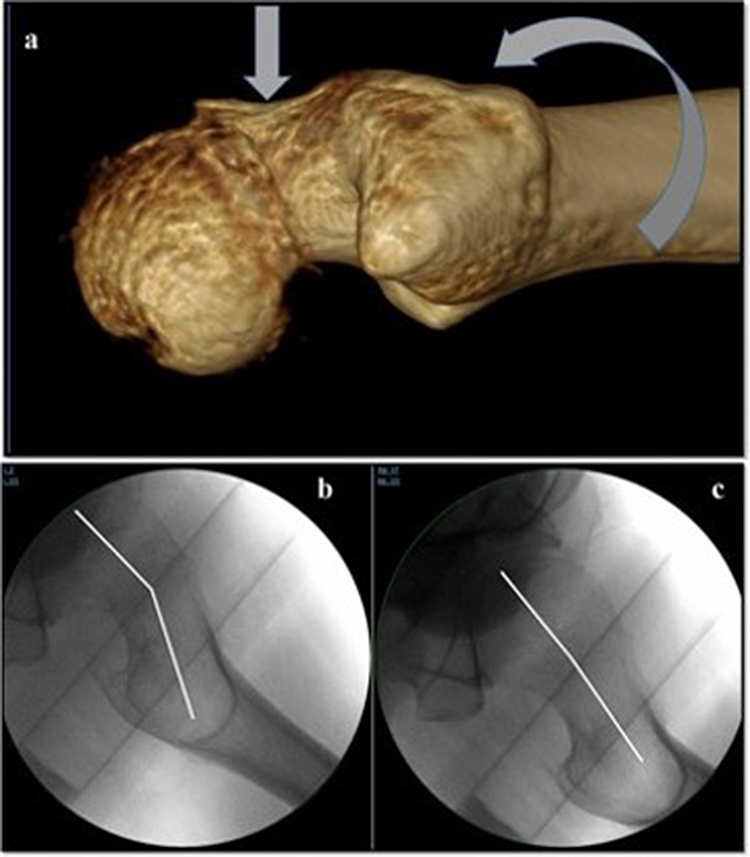 |
Figure 8 Pre- and post-reduction of femoral neck fracture angulation. (a) shows fracture reduction method performed on a fracture table by internal rotation and traction with gentle application of anteroposterior pressure on the femoral neck if needed, (b) shows prereduction tilt on plain film, (c) shows postoperative correction of the tilt achieved by the procedure described. Notes: Reproduced with permission from Steinberg EL, Albagli A, Snir N et al. Addressing posterior tilt displacement during surgery to lower failure risk of sub-capital Garden types 1 and 2 femoral fractures. Arch Orthop Trauma Surg. 2022;142(8):1885–1893.38 |
Summarizing these observations from previous studies, the consensus suggests that a posterior tilt greater than 20° causes fractures to become unstable by widening the fracture gap, potentially causing vascular disruption, which could predispose subsequent treatment to fail. Taken altogether, this degree of tilt about the femoral neck may be sufficiently disruptive to the blood supply such that AVN may result after fixation. Thus, femoral neck fractures with posterior tilt can be considered unstable even when they are classified as Garden I or II fractures on AP radiographs, stimulating consideration that functionally unstable fractures may benefit from arthroplasty as a primary treatment.
The Role of Arthroplasty: Observational Comparative Studies, and Randomized Clinical Trials
Having considered the treatment failures of internal fixation for nondisplaced FNFs, the alternatives, namely one type or another of arthroplasty, should be considered. The outcomes of primary arthroplasty need to be compared with outcomes of both internal fixation and secondary arthroplasty after fixation failures should be evaluated.
Meta-Analyses
In 2003, a meta-analysis of RCTs comparing treatment options for displaced FNFs, namely internal fixation versus arthroplasty, illuminated the potential risk reduction of revision surgery after failed fixation.40 Although reporting results of displaced (Garden III and IV) rather than nondisplaced fractures (Garden I and II), surgical techniques that are 20–25 years old, implants that are no longer in use, and obsolete anesthesia techniques, the observations are of interest because they describe the consequences of the various types of surgical intervention that may be relevant to surgical decisions treating nondisplaced hip fractures. Trends in the treatment of displaced FNF suggested that arthroplasties maintained high mortality rates at 4 months and 1 year postoperatively. Arthroplasty also reduced the risk of revision surgery by 77% compared to internal fixation (Relative Risk (RR): 0.23, P = <0.001). Despite advancements in many techniques and devices, the outcome measures of reoperation and mortality have not substantially improved.
Three recent meta-analyses gathered results from previous RCTs and comparative observational studies to evaluate three primary outcome domains, including perioperative complications, reoperations, and postoperative function by Harris Hip Score (HHS). Specifically, Ma et al reported revision surgery rates, mortality rates at 1 month and 1 year, HHS at one- and two-years post-op, length of hospital stay, and duration of surgery for both internal fixation and arthroplasty. They found that arthroplasty was associated with a lower revision surgery rate than internal fixation (Odds Ratio: 4.5; 95% Confidence Interval [CI], 2.0–9.9). No significant difference was noted in postoperative mortality rates or HHS at 1 year, but patients treated with internal fixation had shorter lengths of stay and surgical time.41 Although the comparison of papers within the meta-analysis is of value, the study reflects only three papers with relatively small cohort sizes, indicating the need for additional, powerful randomized control trials to determine the best course of action when treating FNFs.
As the body of literature regarding nondisplaced FNFs is limited in scope, another meta-analysis conducted by Richards et al analyzing patients older than 65 utilized the same studies seen in the analysis by Ma et al with the addition of one additional observational study conducted by Kang. This meta-analysis confirmed that patients treated with arthroplasty had a significantly lower risk of reoperation when compared with those treated with internal fixation [RR: 0.30 (95% CI, 0.16–0.55, P = 0.01)]. There was no significant difference detected in 1-year mortality risk between the two treatment groups.13
Most recently, a meta-analysis was able to include an additional RCT conducted by Wei et al in 2020. This in-depth meta-analysis evaluated outcome domains consistent with the categories we have presented, including perioperative complications and reoperation. Like previous reports, the pooled studies showed that patients who underwent internal fixation had a higher risk of reoperation [20.1% vs 6.0%, RR = 3.30 (1.79, 6.08), P = <0.001] and lower intraoperative blood loss (mL) [mean difference (MD) = −138.88 (−209.58, −68.18), P = 0.001]. The authors also suggest that, although complications with arthroplasty may be rarer, they may carry with them greater severity. This has implications for the frail, elderly population in which these types of fractures are common as arthroplasty carries with it a higher physiologic burden, especially if it subsequently requires reoperation. Further, there was no statistical significance between the two modalities in terms of function measured by the HHS [MD = −2.73 (−6.26, 0.79), P = 0.13] or mortality [23.4% vs 20.6%, RR = 1.13 (0.75, 1.71), P = 0.48], at 12 months.42
These data collectively indicate that, despite a higher risk of reoperation, internal fixation may serve as an equivalent intervention as compared to arthroplasty in terms of function and mortality. Arthroplasty continues to be tolerated similarly to internal fixation by the elderly population and offers a function profile like that of internal fixation. Hip fracture related mortality rates continue to be high despite advances in treatment.13,40–42
Comparative Observational Studies
Several quality observational studies have been done comparing results of internal fixation with those of primary arthroplasty for FNFs. There is consistency among the studies reviewed in terms of reoperation rate. In a retrospective analysis comparing management of both displaced and nondisplaced FNFs treated with either internal fixation (n=70) or arthroplasty (n=70), those treated with arthroplasty were associated with a lower risk of reoperation (P = 0.016), as expected. Functionally, the HHS of the arthroplasty cohort was significantly higher at 3- (internal fixation (IF): 77.3, hemiarthroplasty (HA): 79.2; P = 0.028), 6- (IF: 82.7, HA: 83.6; P = 0.034), and the 12-month follow-up (IF: 91.8, HA: 84.7; P = 0.045), respectively, at each follow-up evaluation); however, the differences were no longer significant at the 24-month evaluation (P = 0.087).43 In contrast, there are notable risks associated with undergoing arthroplasty. For example, the mean blood loss associated with internal fixation was significantly lower (mean 1.6 blood units; 95% CI 1.48–1.72) compared to that of arthroplasty (mean 2.8 blood units; 95% CI 2.66–2.94) [P = 0.034]. There is also an increased risk of infection and operative time with arthroplasty compared to internal fixation.43,44
A retrospective study of the Norwegian hip fracture registry revealed that the outcomes of revision of displaced FNFs with arthroplasty were even better than the revision of nondisplaced fractures with internal fixation.45 This registry consists of a large data set in which nondisplaced, displaced FNFs, intertrochanteric, and basicervical fractures were compared to identify the trends in surgical intervention. It was observed that nondisplaced fractures were increasingly treated with arthroplasty, however the incidence only rose from 2.1% to 9.7% over a decade. With the support of the methods introduced by those like Palm et al and Kamara et al, this increase likely reflects that the incidence of fractures presenting with posterior tilt, previously unnoticed, were now being identified.45 Several studies still confirmed a more satisfactory outcome in terms of reoperation rate as well as an insignificant difference in mortality when nondisplaced FNFs were managed with arthroplasty. The forest plot (Figure 9) provides visual representation of reoperation rates favoring arthroplasty, and mortality rates favoring internal fixation, although with a modest risk ratio. In the comparative studies analyzed, reoperation rates are diminished using primary arthroplasty. However, observed mortality rates tend to vary greatly and the difference in mortality rate between the two interventions has consistently lacked statistical significance. The gravity of both mortality rate and reoperation rate gives cause to the need for further understanding of the unclear discrepancy between internal fixation and arthroplasty.
 |
Figure 9 Forest plot of the relative risk of reoperation and 1-year mortality in the included studies. Notes: Reproduced with permission from Richards JT, Overmann AL, O’Hara NN, D’Alleyrand JC, Slobogean GP. Internal Fixation Versus Arthroplasty for the Treatment of Nondisplaced Femoral Neck Fractures in the Elderly: A Systematic Review and Meta-Analysis. J Orthop Trauma. 2020;34(1):42–48.13 |
The newest comparative study out of the UK analyzing patients between 2015 and 2020 supported many of the findings that preceded it, eg observations of revision rates, mortality, perioperative complications, and functionality as measured by weight-bearing ability.46 Patients were observed in three different cohorts: cannulated hip fixation, dynamic hip screw, and hemiarthroplasty. The pooled revision rate for internal fixation was 58/581 (9.8%) with the most common reasons for revision being failed fixation (n = 26) and AVN (n = 16). The revision rate for arthroplasty was 8/692 (1.2%) with the reasons for revision being either dislocation (n = 4) or periprosthetic fracture (n = 4). Mortality rates were comparable in both cohorts, as has been consistently observed. Weight-bearing ability was used to represent functional status. When comparing patients who were full weight bearing or partial weight bearing, functional status was a statistically significant indicator of revision within the cannulated hip screw group [Χ2 test, P = 0.003] and the arthroplasty group [Χ2 test, P = 0.02].46 Several other studies also showed lack of statistical significance when comparing internal fixation and arthroplasty in the domain of mortality (Table 2).47–50 Most of the comparative studies to date, however, do not report a reliable method of measuring functional outcomes, if at all. Functional capabilities of patients postoperatively can have profound impacts on their quality of life and, subsequently, morbidity and mortality. Therefore, great care should be used when determining an appropriate plan for weight-bearing postoperatively, especially in the elderly and those who are at risk for complications.
 |
Table 2 Mortality Rates in Studies of Nondisplaced FNF Repair |
These large, national registries enable researchers to conduct quality comparative analyses with substantial power. It is important, though, to bear in mind the relationship between clinical significance and large bodies of data, especially when evaluating patient reported outcomes, as the sample size may obscure the clinical significance. Therefore, the support for an outcome’s clinical application may not be as strong because the presence of P-value indicating statistical significance does not automatically imply clinical significance. Large registries may provide insight into potential best clinical practices, however, as many have analyzed neither functional outcomes nor comparisons of many pertinent comorbidities, more comprehensive comparisons are still necessary.
Randomized Clinical Trials
Several groups have conducted RCTs to reduce selection bias and better understand the benefits and detriments of both internal fixation and arthroplasty as intervention techniques for nondisplaced FNFs. The need for these studies is clear as consensus has yet to be reached regarding which intervention is most appropriate in certain patient populations. Improvements in surgical techniques of internal fixation and arthroplasty have decreased complication rates, but mortality rates continue to be comparable when treating nondisplaced FNFs. In a multicenter RCT conducted by Dolatowski et al, 219 patients ≥70 years of age with a nondisplaced FNF (Garden I or II) were randomly allocated to internal fixation or hemiarthroplasty.44 The baseline characteristics of patients who met the inclusion criteria but were not included in the trial did not differ from those of the patients who were included in the trial. Patient functionality, reoperation, and mortality were recorded. Functionality and quality of life were observed through many validated measures, including the HHS, Timed Up-and-Go (TUG) test, Pain Intensity (PI-NRS), EuroQol-5 (EQ-5D), and the Mini-Mental State Exam. There were no significant differences in hip pain, quality of life measures, and cognition between the two treatment groups at any time point. Of note, patients allocated to receive hemiarthroplasty demonstrated increased mobility by measure of the TUG compared to internal fixation, but no significant difference was found in reestablishing hip function by the HHS (24-month adjusted between-group mean difference = −2 [95% CI = 26 to 3]; P = 0.499). Internal fixation performed in 22/110 (20%) patients was found to be a risk factor for major reoperation in comparison to hemiarthroplasty in which reoperation was performed in 5/108 (5%) patients (relative risk reduction [RRR] = 3.3 [95% CI = 0.7 to 10.0]; P = 0.002).42 This is consistent with the observation that internal fixation is a significant indicator for increased surgical complications, such as nonunion and osteonecrosis, which occurred significantly more often in patients allocated to internal fixation (RRR = 1.8 [95% CI = 0.4 to 4.8]; P = 0.004). As in other studies, and importantly, there were no significant differences in mortality between the two groups. At 24 months, the internal fixation cohort experienced a mortality of 36% while the arthroplasty cohort experienced a mortality of 26% (RRR = 0.4 [95% CI = −0.1 to 1.1]; P = 0.110).44 While these figures do not demonstrate statistical significance, some clinicians might feel that a 10% difference in mortality is clinically significant and must be considered when deciding upon the appropriate surgical intervention.
Similar findings by Lu et al have shown that, while the reoperation rate is significantly lower in the case of arthroplasty, to be expected, the perioperative factors that potentially have prognostic implications are improved in the case of internal fixation.51 Intraoperative outcomes measured included incision length (3.8 cm ± 0.53 for fixation vs 12.3 cm ± 2.57 for arthroplasty), operation time in minutes (43.80 ± 6.47 for fixation vs 64.03 ± 8.76 for arthroplasty), and blood loss (28.66 mL ± 6.41 for fixation vs 175.08 mL ± 25.60 for arthroplasty), all of which demonstrated significant differences between the two interventions. These differences in surgery-related indicators may be important to consider if they affect operative outcomes. The average HHS for both cohorts was above 75 (on a scale of 100) when reported during follow-up visits ranging from 6 months to 5 years. Upon statistical analysis, measurement of post-operative functionality using the HHS did not reveal significant differences between the two treatment options. The 12-month HHS was 77.25 ± 9.4 (n=28) in the internal fixation cohort and 81.07 ± 12.3 (n=30) in the hemiarthroplasty cohort. However, the excellent and good rating in the hemiarthroplasty group was significantly higher than that in the internal fixation group (P < 0.05), indicating that there may be early benefits to complete replacement of the joint in elderly patients.51
These comparisons indicated that there is no significant difference in functionality, quantified using HHS, at the 12-month mark when comparing internal fixation and arthroplasty (Table 3).44,51–53 Altogether, the four studies comparing patient hip functionality after internal fixation or arthroplasty reported that arthroplasty was not found to be superior to internal fixation when assessing function (HHS) as the primary outcome. However, the rate of reoperation and patient mobility did demonstrate statistical significance, in addition to the earlier achievement of function and pain control by arthroplasty. These data indicate that further trials are needed to assess the difference in patient outcomes between internal fixation and arthroplasty, especially in the cases of the elderly and those with comorbidities as outcomes may be different in these populations and they may benefit from one treatment over another.
 |
Table 3 Functional Scores Measured Postoperatively in Studies of Nondisplaced FNF Repair |
A recent 2020 RCT included three cohorts for comparison: nonoperative treatment, internal fixation, and hemiarthroplasty. The primary outcome of the study was hip function, with secondary aims of quality of life, mortality, hip pain, complications, and reoperation rates. Randomizing patients >75 years old in equal ratios (nonoperative treatment n = 51, IF n = 51, HA n = 52), showed similar findings to those of the preceding Dolatowski et al and Lu et al studies. Hip function, as measured by HHS, was significantly higher in the arthroplasty group as compared to the internal fixation during the early postoperative months (P < 0.05) but lost its significance at the 12-month follow-up (P = 0.371). Quality of life, hip pain, and mortality all lacked statistical significance beyond the 12-month follow-up as well. Nonoperative treatment compared to internal fixation did not show any significant difference in outcomes which maintains its value as an intervention for younger patients with valgus impacted fractures. Compared to arthroplasty, however, nonoperative treatment demonstrated lower HHS and Quality of Life in the early recovery period. In contrast to previous studies, the arthroplasty group had a shorter duration of stay in the hospital postoperatively (P < 0.05). In addition, no significant difference was found in reoperation rate among the three groups. Of note, however, the fractures reported in this study were all impacted which, the authors suggested, may create a more stable fracture and more favorable conditions for union.53 This was sternly contradicted in a more recent retrospective study that showed a staggering 62% rate of secondary surgery after nonoperative management in a population with a mean age of 81.54 This is in agreement with the findings of several other aforementioned studies suggesting surgical intervention for elderly patients. Among all the RCTs mentioned, none were conducted as blind studies, always difficult in surgery. Comorbidities and causes of death were also not evaluated in these studies; thus, mortality could not be linked to surgery, comorbidities, or other confounders (see Table 2 and Table 3).
Conclusions: Extant Issues Influencing Surgical Thinking
Currently, the consensus appears to distinguish treatment options between nondisplaced and displaced FNFs. However, due to many additional factors such as patient fragility, osteoporosis, and nutritional and hydration status, the decision to repair a nondisplaced FNF via internal fixation or arthroplasty requires individual patient assessment. Nonoperative care is a viable option in younger patients with Garden 1 or 2 valgus-impacted fractures with no posterior tilt after physical exam shows no pain on hip ROM. The decisional paradigm, excluding those who are younger and determined to be candidates for nonoperative care, has appeared to shift in favor of arthroplasty primarily to avoid perioperative complications and subsequent reoperation in the elderly population. Internal fixation provides the benefits of simplicity, reduced cost, and a lower physiological burden. Arthroplasty improves reoperation rates and early functional capabilities. However, mortality does not appear to differ between the two. Further understanding of whether arthroplasty serves as a better primary intervention for elderly patients may clarify the decision-making process when considering these factors. Here, we summarize the factors that may be changing the paradigm and the extant issues that influence surgical decision-making as the paradigm shifts towards arthroplasty.
With increased tilt about the femoral neck, whether it be posteriorly or anteriorly, there is believed to be decreased stability and increased injury to the surrounding vasculature. Demonstrated in several examples to have a threshold of ≥20°, the degree of posterior tilt may serve as a proxy for determining which method of intervention is most appropriate, although this has been contested. Many retrospective studies observed a relationship between preoperative posterior tilt and subsequent reoperation rates; however, one substantial study did not make the same observations. As mentioned in Palm’s invited commentary, the ability of patients to ambulate early based upon their perceived pain, institutional variation of when to reoperate, and inconsistency of standardized imaging procedures may be causes for the conflicting findings.55
The Garden classification of FNFs is descriptive of the fracture configuration with no inclusion of patient qualities or comorbidities that can influence surgical treatment, including age, gender, intercurrent illnesses, polypharmacy, mental status, and bone quality/density. Due to the significant bone loss that occurs with aging, complications of surgery in such a fragile population are to be expected. If there is construct failure or AVN following internal fixation of FNFs, hip arthroplasty is the salvage procedure of choice. The necessity of salvage is a significant complication in older patients. Lagergren et al used the results from a Swedish Register Cohort to examine conversion to arthroplasty after internal fixation of nondisplaced femoral neck fractures. They found that 1 in 10 patients had a conversion to arthroplasty within 5 years, over 50% of which occurred within the first year. Conversions were highest in women and in patients between 70 and 79 years old.56 The conversion rate in the literature ranges from 8% to 16%.7 This is significant as these patients experience inferior outcomes compared to patients with primary arthroplasty in addition to a prolonged period of pain and impaired mobilization.56 Therefore, it is suggested that arthroplasty be selected as the primary treatment in certain instances to allow faster mobilization and potentially decreased morbidity and mortality.57
We have discussed the major outcome domains of previous studies that we believe contribute to the difficulty finding consensus regarding appropriate FNF treatment, including mortality, perioperative complications, functionality, and reoperation. Mortality rates of hip fractures have remained stubbornly high over the years, with 12-month mortality hovering near 20%, irrespective of the form of intervention.58 Several contemporary studies have continued to observe this trend. In Table 2, aside from one study which was conducted two decades ago, none demonstrate statistical significance in the domain of postoperative mortality when comparing internal fixation to arthroplasty. The prevention of reoperation could decrease this mortality rate. While it may be intuitive that arthroplasty would effectively prevent reoperation, excluding extenuating circumstances, it is important to note that internal fixation and arthroplasty maintain distinct perioperative complications that complicate their comparison. Thus, the observations of mortality presented above highlight that surgical decision-making is multi-component, emphasizing the need for a better-defined standard of care for nondisplaced FNFs.
Nondisplaced Garden type I and II femoral neck fractures are surprisingly difficult to treat in patients with a poor biologic milieu resulting in significant reoperation rates. Most frequently, postoperative complications consist of nonunion, AVN, and infection. One of the major reasons for complication is the disruption of the tenuous blood supply about the femoral neck. Displacement or tilt of the fracture damages the surrounding retinacular vessels that perfuse the proximal femur. Studies have demonstrated significant microscopic and structural changes that occur because of lack of perfusion, leading to AVN and structural femoral head failure. Although by choosing arthroplasty over internal fixation the surgeon effectively eliminates the risks of non-union, malunion, and AVN of the femoral head, a new set of perioperative complications may be introduced including infection, longer surgery times, and significantly increased blood loss. The equivalence of mortality rates between internal fixation and arthroplasty remains troubling and raises questions of fracture-related mortality versus all-cause mortality.
Functional outcomes are beneficial to the recovery process as they have been shown to be correlated with an improved quality of life, often as measured by the EQ-5D. Across the major studies reviewed here, postoperative functional ability consistently lacked significance when comparing the internal fixation and arthroplasty after approximately two years of recovery. A proposed RCT out of Denmark may provide more insight into this as one of its primary outcomes will be hip function as represented by the New Mobility Score, defined by Parker in 1993 and shown to have good correlation to gait function by Kristensen.59,60 This evaluative tool, in conjunction with the HHS and the TUG test, could be incorporated into future comparative studies more readily to evaluate patient outcomes postoperatively, though our observations suggest that functional status may not be a decisive factor when determining which intervention to implement.61
In determining which surgical intervention to pursue for the treatment of nondisplaced Garden types I & II fractures, a multivariate algorithm may prove useful in the mitigation of reoperation. Some studies have reported that the reoperation rates of internal fixation range from 8% to 23%,19,47,62 and that occurrence of major complications may reach 34.6%.63 Strides have been made in the literature to guide clinical decision-making, including the Garden and Pauwels classifications as well as the method for measuring posterior tilt introduced by Palm. However, a powerful algorithm that results in decreased reoperation, predictably good postoperative function, and acceptable mortality rate remains undefined and the reason for this lack of definition is multifactorial. The failure to develop a treatment consensus may be related to the inconsistent recommendations in many contemporary studies comparing internal fixation to arthroplasty in the context of nondisplaced FNFs. Such a large reoperation rate of internal fixation, as it carries with it an additional surgical burden and its associated morbidity, is cause for reevaluation.
Given the observations presented, further evaluation of bone biology, associated comorbidities (the health status of fragile individuals), and posterior tilt in the fracture setting may be of value when determining which surgical intervention to pursue. Therefore, we recommend additional studies, namely RCTs with substantial power, to further interrogate the impacts of comorbid conditions that may affect outcomes as well as the cost–benefit analysis of performing arthroplasty rather than internal fixation on elderly patients who have suffered a nondisplaced hip fracture, especially if the fracture does not exceed the threshold of 20° posterior tilt in the lateral plane. It is our hope that what would emerge from these studies is a well-defined, comprehensive algorithm to be used in the surgical decision-making process, like the one designed and implemented at the Hvidovre Hospital in Denmark by Palm et al.12 In clinical reality with patient heterogeneity, it may not be feasible to simply rely on a flowchart or algorithm to decide which intervention would be most appropriate based on group characteristics. For example, we must still consider that the young hip fracture patient with valgus impaction, no posterior tilt, and no pain on physical exam ROM could be a potential candidate for nonoperative care rather than THA. Instead, an informed, patient-centered approach supported by said framework should be used. Successful management of a nondisplaced FNF requires that the surgeon balance the potential risks and healthcare costs with the benefits associated with intervention. While the treatment of femoral neck fractures is typically considered a simple and easily manageable task, this paper highlights the need to critically examine nondisplaced FNF treatment considering the ambiguity in the literature.
Funding
This work was funded by a research grant from The Miriam Hospital.
Disclosure
Each author certifies that neither he nor she, nor any member of his or her immediate family, have funding or commercial associations that might pose a conflict of interest in connection with the submitted article.
References
1. Sing CW, Lin TC, Bartholomew S, et al. Global epidemiology of hip fractures: secular trends in incidence rate, post-fracture treatment, and all-cause mortality [published online ahead of print, 2023 Apr 29]. J Bone Miner Res. 2023. doi:10.1002/jbmr.4821
2. Gullberg B, Johnell O, Kanis JA. World-wide projections for Hip fracture. Osteoporos Int. 1997;7(5):407–413. doi:10.1007/pl00004148
3. Johnell O, Kanis JA. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int. 2006;17(12):1726–1733. doi:10.1007/s00198-006-0172-4
4. Haubruck P, Heller RA, Tanner MC. Femoral neck fractures: current evidence, controversies and arising challenges. Orthop Traumatol Surg Res. 2020;106(4):597–600. doi:10.1016/j.otsr.2020.03.006
5. Bjorgul K, Reikeras O. Outcome of undisplaced and moderately displaced femoral neck fractures. Acta Orthop. 2007;78(4):498–504. doi:10.1080/17453670710014149
6. Eisler J, Cornwall R, Strauss E, Koval K, Siu A, Gilbert M. Outcomes of elderly patients with nondisplaced femoral neck fractures. Clin Orthop Relat Res. 2002;399:52–58. doi:10.1097/00003086-200206000-00008
7. Onativia IJ, Slullitel PA, Diaz Dilernia F, et al. Outcomes of nondisplaced intracapsular femoral neck fractures with internal screw fixation in elderly patients: a systematic review. Hip Int. 2018;28(1):18–28. doi:10.5301/hipint.5000532
8. Garden RS. Low-angle fixation in fractures of the femoral neck. J Bone Joint Surg Br. 1961;43(4):647–663. doi:10.1302/0301-620X.43B4.647
9. Kazley JM, Banerjee S, Abousayed MM, Rosenbaum AJ. Classifications in brief: garden classification of femoral neck fractures. Clin Orthop Relat Res. 2018;476(2):441–445. doi:10.1007/s11999.0000000000000066
10. NICE. Guideline - Hip fracture: management; 2011. Available from: https://www.nice.org.uk/guidance/cg124/chapter/Recommendations#surgical-procedures.
11. Shah AK, Eissler J, Radomisli T. Algorithms for the treatment of femoral neck fractures. Clin Orthop Relat Res. 2002;399:28–34. doi:10.1097/00003086-200206000-00005
12. Palm H, Krasheninnikoff M, Holck K, et al. A new algorithm for Hip fracture surgery. Reoperation rate reduced from 18 % to 12 % in 2000 consecutive patients followed for 1 year. Acta Orthop. 2012;83(1):26–30. doi:10.3109/17453674.2011.652887
13. Richards JT, Overmann AL, O’Hara NN, D’Alleyrand JC, Slobogean GP. Internal fixation versus arthroplasty for the treatment of nondisplaced femoral neck fractures in the elderly: a systematic review and meta-analysis. J Orthop Trauma. 2020;34(1):42–48. doi:10.1097/BOT.0000000000001656
14. Nauth A, Creek AT, Zellar A. Fixation using Alternative Implants for the Treatment of Hip fractures (FAITH) Investigators. Fracture fixation in the operative management of Hip fractures (FAITH): an international, multicentre, randomised controlled trial. Lancet. 2017;389(10078):1519–1527. doi:10.1016/S0140-6736(17)30066-1
15. Okike K, Udogwu UN, Isaac M, et al. Not all garden-I and II femoral neck fractures in the elderly should be fixed: effect of posterior tilt on rates of Subsequent arthroplasty. J Bone Joint Surg Am. 2019;101(20):1852–1859. doi:10.2106/JBJS.18.01256
16. Viberg B, Frøslev T, Overgaard S, Pedersen AB. Mortality and revision risk after femoral neck fracture: comparison of internal fixation for undisplaced fracture with arthroplasty for displaced fracture: a population-based study from Danish National Registries. Acta Orthop. 2021;92(2):163–169. doi:10.1080/17453674.2020.1850940
17. Heetveld MJ, Raaymakers EL, van Eck-Smit BL, van Walsum AD, Luitse JS. Internal fixation for displaced fractures of the femoral neck. Does bone density affect clinical outcome? J Bone Joint Surg Br. 2005;87(3):367–373. doi:10.1302/0301-620x.87b3.15715
18. Palm H, Gosvig K, Krasheninnikoff M, Jacobsen S, Gebuhr P. A new measurement for posterior tilt predicts reoperation in undisplaced femoral neck fractures: 113 consecutive patients treated by internal fixation and followed for 1 year. Acta Orthop. 2009;80(3):303–307. doi:10.3109/17453670902967281
19. Conn KS, Parker MJ. Undisplaced intracapsular Hip fractures: results of internal fixation in 375 patients. Clin Orthop Relat Res. 2004;421:249–254. doi:10.1097/01.blo.0000119459.00792.c1
20. Lapidus LJ, Charalampidis A, Rundgren J, Enocson A. Internal fixation of garden I and II femoral neck fractures: posterior tilt did not influence the reoperation rate in 382 consecutive hips followed for a minimum of 5 years. J Orthop Trauma. 2013;27(7):386–391. doi:10.1097/BOT.0b013e318281da6e
21. Sjöholm P, Otten V, Wolf O, et al. Posterior and anterior tilt increases the risk of failure after internal fixation of Garden I and II femoral neck fracture. Acta Orthop. 2019;90(6):537–541. doi:10.1080/17453674.2019.1637469
22. Sjöholm P, Sundkvist J, Wolf O, Sköldenberg O, Gordon M, Mukka S. Preoperative anterior and posterior tilt of garden I-II femoral neck fractures predict treatment failure and need for reoperation in patients over 60 years. JB JS Open Access. 2021;6(4):
23. Wang W, Huang Z, Peng J, Fan J, Long X. Preoperative posterior tilt can be a risk factor of fixation failure in nondisplaced femoral neck fracture: a systematic review and meta-analysis [published online ahead of print, 2023 Mar 22]. Eur J Orthop Surg Traumatol. 2023;33(7):3197–3205. doi:10.1007/s00590-023-03518-w
24. Song HK, Choi HJ, Yang KH. Risk factors of avascular necrosis of the femoral head and fixation failure in patients with valgus angulated femoral neck fractures over the age of 50 years. Injury. 2016;47(12):2743–2748. doi:10.1016/j.injury.2016.10.022
25. Kamara E, Zvi YS, Vail TP. Treatment of valgus-impacted and nondisplaced femoral neck fragility fractures in the elderly. J Am Acad Orthop Surg. 2021;29(11):470–477. doi:10.5435/JAAOS-D-19-00866
26. Dyke JP, Lazaro LE, Hettrich CM, Hentel KD, Helfet DL, Lorich DG. Regional analysis of femoral head perfusion following displaced fractures of the femoral neck. J Magn Reson Imaging. 2015;41(2):550–554. doi:10.1002/jmri.24524
27. Aaron RK, Lorich DG, Lazaro LE. Fractures and Bone Repair. In: Skeletal Circulation in Clinical Practice. World Scientific; 2016:185–208. doi:10.1142/9789814713764_0009
28. Ogden JA. Changing patterns of proximal femoral vascularity. J Bone Joint Surg Am. 1974;56(5):941–950. doi:10.2106/00004623-197456050-00007
29. Gautier E, Ganz K, Krügel N, Gill T, Ganz R. Anatomy of the medial femoral circumflex artery and its surgical implications. J Bone Joint Surg Br. 2000;82(5):679–683. doi:10.1302/0301-620X.82B5.0820679
30. Liu Y, Li M, Zhang M, et al. Femoral neck fractures: prognosis based on a new classification after superselective angiography. J Orthop Sci. 2013;18(3):443–450. doi:10.1007/s00776-013-0367-4
31. Sen RK, Tripathy SK, Gill SS, Verma N, Singh P, Radotra BD. Prediction of posttraumatic femoral head osteonecrosis by quantitative intraosseous aspirate and core biopsy analysis: a prospective study. Acta Orthop Belg. 2010;76(4):486–492.
32. Shah KN, Racine J, Jones LC, Aaron RK. Pathophysiology and risk factors for osteonecrosis. Curr Rev Musculoskelet Med. 2015;8(3):201–209. doi:10.1007/s12178-015-9277-8
33. Han S, Oh M, Yoon S, et al. Risk stratification for avascular necrosis of the femoral head after internal fixation of femoral neck fractures by post-operative bone SPECT/CT. Nucl Med Mol Imaging. 2017;51(1):49–57. doi:10.1007/s13139-016-0443-8
34. Ehlinger M, Moser T, Adam P, et al. Early prediction of femoral head avascular necrosis following neck fracture. Orthop Traumatol Surg Res. 2011;97(1):79–88. doi:10.1016/j.otsr.2010.06.014
35. Arnoldi CC, Lemperg RK. (1977) fracture of the femoral neck. Clin Orthopaedics Related Res. 1977;129:217–222. doi:10.1097/00003086-197711000-00029
36. Gill TJ, Sledge JB, Ekkernkamp A, Ganz R. Intraoperative assessment of femoral head vascularity after femoral neck fracture. J of Orthop Trauma. 1998;12(7):474–478. doi:10.1097/00005131-199809000-00008
37. Zhao D, Wang Z, Cheng L, et al. The significance of evaluating the femoral head blood supply after femoral neck fracture. OrthopaedicSurgery. 2022;14(4):742–749. doi:10.1111/os.13241
38. Steinberg EL, Albagli A, Snir N, et al. Addressing posterior tilt displacement during surgery to lower failure risk of sub-capital Garden types 1 and 2 femoral fractures. Arch Orthop Trauma Surg. 2022;142(8):1885–1893. doi:10.1007/s00402-021-03900-5
39. Wang Y, Ma J, Bai H, et al. A three-dimensional measurement study of fracture displacement in Garden I femoral neck fracture: a retrospective study. BMC Musculoskelet Disord. 2023;24(1):623. doi:10.1186/s12891-023-06737-8
40. Bhandari M, Devereaux PJ, Swiontkowski MF, et al. Internal fixation compared with arthroplasty for displaced fractures of the femoral neck. A meta-analysis. J Bone Joint Surg Am. 2003;85(9):1673–1681. doi:10.2106/00004623-200309000-00004
41. Ma HH, Chou TA, Tsai SW, Chen CF, Wu PK, Chen WM. Outcomes of internal fixation versus hemiarthroplasty for elderly patients with an undisplaced femoral neck fracture: a systematic review and meta-analysis. J Orthop Surg Res. 2019;14(1):320. doi:10.1186/s13018-019-1377-5
42. Sattari SA, Guilbault R, MacMahon A, Salem HS, Khanuja HS. Internal fixation versus hemiarthroplasty for nondisplaced femoral neck fractures: a systematic review and meta-analysis. J Orthop Trauma. 2023;37(5):e219–e226. doi:10.1097/BOT.0000000000002558
43. Nicolaides V, Galanakos S, Mavrogenis AF, et al. Arthroplasty versus internal fixation for femoral neck fractures in the elderly. Strategies Trauma Limb Reconstr. 2011;6(1):7–12. doi:10.1007/s11751-010-0099-3
44. Dolatowski FC, Frihagen F, Bartels S, et al. Screw fixation versus hemiarthroplasty for nondisplaced femoral neck fractures in elderly patients: a multicenter randomized controlled trial. J Bone Joint Surg Am. 2019;101(2):136–144. doi:10.2106/JBJS.18.00316
45. Gjertsen JE, Dybvik E, Furnes O, et al. Improved outcome after Hip fracture surgery in Norway. Acta Orthop. 2017;88(5):505–511. doi:10.1080/17453674.2017.1344456
46. Ahmed M, Tirimanna R, Ahmed U, et al. A comparison of internal fixation and hemiarthroplasty in the management of un- or minimally displaced Hip fractures in patients over 60 years old. Injury. 2023;54(4):1180–1185. doi:10.1016/j.injury.2022.11.065
47. Chen JY, She GR, Luo SM, et al. Hemiarthroplasty compared with internal fixation for treatment of nondisplaced femoral neck fractures in elderly patients: a retrospective study. Injury. 2020;51(4):1021–1024. doi:10.1016/j.injury.2020.02.098
48. Laubach M, Bläsius FM, Volland R, et al. Internal fixation versus Hip arthroplasty in patients with nondisplaced femoral neck fractures: short-term results from a geriatric trauma registry. Eur J Trauma Emerg Surg. 2022;48(3):1851–1859. doi:10.1007/s00068-021-01801-1
49. Kang JS, Jeon YS, Ahn CH, Roh TH. Osteosynthesis versus endoprosthesis for the treatment of femoral neck fracture in Asian elderly patients. BMC Musculoskelet Disord. 2016;17:264. doi:10.1186/s12891-016-1123-7
50. Sikand M, Wenn R, Moran CG. Mortality following surgery for undisplaced intracapsular Hip fractures. Injury. 2004;35(10):1015–1019. doi:10.1016/j.injury.2004.01.004
51. Lu Q, Tang G, Zhao X, Guo S, Cai B, Li Q. Hemiarthroplasty versus internal fixation in super-aged patients with undisplaced femoral neck fractures: a 5-year follow-up of randomized controlled trial. Arch Orthop Trauma Surg. 2017;137(1):27–35. doi:10.1007/s00402-016-2591-9
52. Mukka S, Sjöholm P, Aziz A, et al. A cohort study comparing internal fixation for undisplaced versus Hip arthroplasty for displaced femoral neck fracture in the elderly: a pilot study for a clinical trial. Pilot Feasibility Stud. 2020;6(1):98. doi:10.1186/s40814-020-00642-w
53. Wei P, Xu Y, Gu Y, Geng D, Yao Q, Wang L. Conservative vs surgical treatment of impacted femoral neck fracture in patients 75 years and older. J Am Geriatr Soc. 2020;68(10):2214–2221. doi:10.1111/jgs.16535
54. Erivan R, Soleihavoup M, Villatte G, Perez Prieto D, Descamps S, Boisgard S. Poor results of functional treatment of Garden-1 femoral neck fracture in dependent patients. Orthop Traumatol Surg Res. 2020;106(4):601–605. doi:10.1016/j.otsr.2019.09.027
55. Palm H. Invited Commentary. J of Orthop Trauma. 2013;27(7):390–391. doi:10.1097/BOT.0b013e318281db75
56. Lagergren J, Mukka S, Wolf O, Nauclér E, Möller M, Rogmark C. Conversion to arthroplasty after internal fixation of nondisplaced femoral neck fractures: results from a Swedish register cohort of 5428 Individuals 60 years of age or older. J Bone Jt Surg. 2023;105(5):389–396. doi:10.2106/JBJS.22.01035
57. Kristensen PK, Thillemann TM, Søballe K, Johnsen SP. Are process performance measures associated with clinical outcomes among patients with Hip fractures? A population-based cohort study. Int J Qual Health Care. 2016;28(6):698–708. doi:10.1093/intqhc/mzw093
58. Downey C, Kelly M, Quinlan JF. Changing trends in the mortality rate at 1-year post Hip fracture - a systematic review. World J Orthop. 2019;10(3):166–175. PMID: 30918799; PMCID: PMC6428998. doi:10.5312/wjo.v10.i3.166
59. Parker M, Palmer C. A new mobility score for predicting mortality after Hip fracture. J Bone Joint Surg Br. 1993;75(5):797–798. doi:10.1302/0301-620X.75B5.8376443
60. Kristensen MT, Foss NB, Kehlet H. Timed up and go and new mobility score as predictors of function six months after hip fracture. Ugeskr Laeger. 2005;167(35):3297–3300.
61. Viberg B, Kold S, Brink O, et al. Is arthroplasty better than internal N al fixation for undisplaced S placed femoral neck E ck fracture? A national pragmatic RCT: the SENSE trial. BMJ Open. 2020;10(10):e038442. doi:10.1136/bmjopen-2020-038442
62. Kim SJ, Park HS, Lee DW. Complications after internal screw fixation of nondisplaced femoral neck fractures in elderly patients: a systematic review. Acta Orthop Traumatol Turc. 2020;54(3):337–343. doi:10.5152/j.aott.2020.03.113
63. Han SK, Song HS, Kim R, et al. Clinical results of treatment of garden type 1 and 2 femoral neck fractures in patients over 70-year old. Eur J Trauma Emerg Surg. 2016;42(2):191–196. doi:10.1093/intqhc/mzw093
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.