")
Back to Journals » Orthopedic Research and Reviews » Volume 14
Management of Displaced Midshaft Clavicle Fractures in Pediatrics and Adolescents: Operative vs Nonoperative Treatment
Authors Markes AR, Garcia-Lopez E, Halvorson RT , Swarup I
Received 16 August 2022
Accepted for publication 17 October 2022
Published 1 November 2022 Volume 2022:14 Pages 373—381
DOI https://doi.org/10.2147/ORR.S340538
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Clark Hung
Alexander R Markes, Edgar Garcia-Lopez, Ryan T Halvorson, Ishaan Swarup
Department of Orthopaedic Surgery, University of California-San Francisco, San Francisco, CA, USA
Correspondence: Ishaan Swarup, Email [email protected]
Abstract: The purpose of the current review is to describe the management of displaced midshaft clavicle fractures in pediatric and adolescent patients. Midshaft clavicle fractures are relatively common in pediatric and adolescent patients. They most commonly occur from direct trauma and are often related to sports participation in adolescents. Recent literature in the management of adult midshaft clavicle fractures has supported operative management due to improved functional outcomes, decreased time to union, leading to early return to activity. A similar trend of increasing frequency in operative management has been seen in pediatric and adolescent patients with no consensus in the literature on optimal management. Nonoperative treatment consists of with a brief period of sling immobilization followed by range of motion. Operative management may be considered for open fractures, fractures with significant neurovascular compromise and soft tissue complications. Studies have shown comparable mid- to long-term functional and patient-reported outcomes after operative and nonoperative management of midshaft clavicle fractures in pediatric patients.
Keywords: pediatric clavicle fracture, adolescent clavicle fracture, midshaft clavicle fracture
Introduction
Clavicle fractures account for 8–15% of all skeletal injuries in the pediatric and adolescent population.1–4 The vast majority of these fractures predominantly affect males and occur during sports as a result of direct impact to the shoulder.1 The majority of clavicle fractures occur at the middle third and have a tendency to be displaced and shortened.1,2,5 Although midshaft clavicle fractures are very common in adolescents, management recommendations tend to follow adult literature. However, there are several recent studies focusing on this population.
Historically, pediatric midshaft clavicle fractures have been managed nonoperatively. Prospective studies analyzing nonoperative management in pediatric and adolescent patients have shown good radiographic and functional outcomes.6–9 However, recent randomized controlled trials in the management of adult midshaft clavicle fractures have supported operative management for increasing indications due to improved functional outcomes, decreased time to union, leading to early return to activity. Similar trends without the same level of supportive data have been seen in pediatric and adolescent patients, leading to an increased interest in operative management of pediatric and adolescent clavicle fractures; though exact operative indications are controversial.10–12 Thus, the purpose of the current review is to describe the management of displaced midshaft clavicle fractures in pediatric and adolescent patients.
Anatomy, Epidemiology, and Classification
Anatomy
The clavicle is an S-shaped bone whose medial end is connected to the axial skeleton via the sternoclavicular joint and the lateral end is connected to the scapula via the acromioclavicular joint. Ossification happens within the seventh week of gestation and the thick periosteum in the developing clavicle may offer a protective advantage by preventing complete displacement.1,3,13 The muscles and ligaments that attach to the clavicle include the deltoid, trapezius, subclavius, pectoralis major, and sternocleidomastoid (SCM) with the coracoclavicular (trapezoid and conoid), costoclavicular, and sternoclavicular ligaments (Figure 1).14,15 The SCM acts as a deforming force pulling the medial fragment cranially and while the lateral fragment is pulled inferiorly and rotated anteriorly by the weight of the shoulder (Figure 1).14,15 The area between the outer and middle third of the clavicle is the thinnest part of the bone and is the only area with no muscle or ligamentous attachments.2,14 These features make the clavicle prone to fracture.
 |
Figure 1 Deforming forces acting on the clavicle after midshaft fracture. The blue arrows on the radiograph demonstrate the dominant vectors of displacement for the two fracture fragments. The SCM pulls the medial fragment cranially and posteriorally and the weight of the arm pulls the medial fragment inferior and anterior. Notes: Left image is used with permission of Elsevier, from Skeletal Trauma of the Upper Extremity, 1st Edition. Johnson P, McKee M. Midshaft Clavicle Fractures. In: Garrigues GE, Richard MJ, Gage MJ, eds. 28–35, copyright 2022; permission conveyed through Copyright Clearance Center, Inc.59 |
Clavicle fractures account for between 5–15% of all pediatric and adolescent fractures, with up to 90% occurring midshaft.3,16–19 The population incidence of clavicle fractures is highest in the second decade of life and has been increasing over recent years.20,21 A multi-institution group was formed in 2013 to investigate adolescent clavicle fracture treatments (Function after Adolescent Clavicle Trauma and Surgery [FACTS]) drawing patients from 8 geographically diverse, tertiary pediatric hospitals of different sizes and payer mixes to form their cohort.1 This cohort found that 79% occurred in males, 88% in athletes, and 56% on the non-dominant side.1 The most common mechanism of injury is trauma, usually via direct blow to the shoulder or upper arm, with most injuries occurring during sports participation (most commonly football), followed by horseplay, biking, falling, or motor vehicle collisions.1,22
Less common etiologies include birth trauma (2.7 to 5.7 per 1000 live births), especially in the setting of macrosomia, vacuum assisted delivery, as well as infectious, metabolic, or pathologic conditions for which limited data are available among pediatric patients.23,24 Neonatal clavicle fractures from birth are particularly concerning as, although they are rare, they present with higher prevalence of brachial plexus injury. Ergün et al reviewed 55 perinatal clavicle fractures diagnosed over 6 years at their institution and found that 23 (41.8%) had a brachial plexus injury. The study also found a statistically significant correlation between spiral and oblique clavicle fracture morphology and development of brachial plexus injury.25
Classifications
Clavicle fractures are commonly reported using several classification systems, including anatomic location, the Neer classification, the Allman classification, and the AO/OTA classification. Anatomically, the clavicle can be divided into the proximal, middle, and distal thirds. Correspondingly, Allman classified fractures into group I (middle third), group II (distal third), and group III (proximal third).26
Similarly, as seen in Table 1, the AO/OTA classifies according to segment as well as articular involvement for medial fractures, pattern for diaphyseal fractures, and displacement and coracoclavicular ligament disruption for lateral fractures.27 In the AO classification, “15” refers to the clavicle and the number following the decimal is either a 1, 2, or 3, referring, respectively, to the proximal, middle, and distal clavicle. 15.1 fractures (proximal clavicle) and 15.3 fractures (distal clavicle) are further subdivided into A, B, or C, referring to extra-articular, partial articular, or complete articular fractures, respectively. 15.2 fractures (middle clavicle) are further subdivided into A, B, or C referring to simple fractures (spiral, oblique or transverse patterns), wedge fractures, or comminuted fractures, respectively.
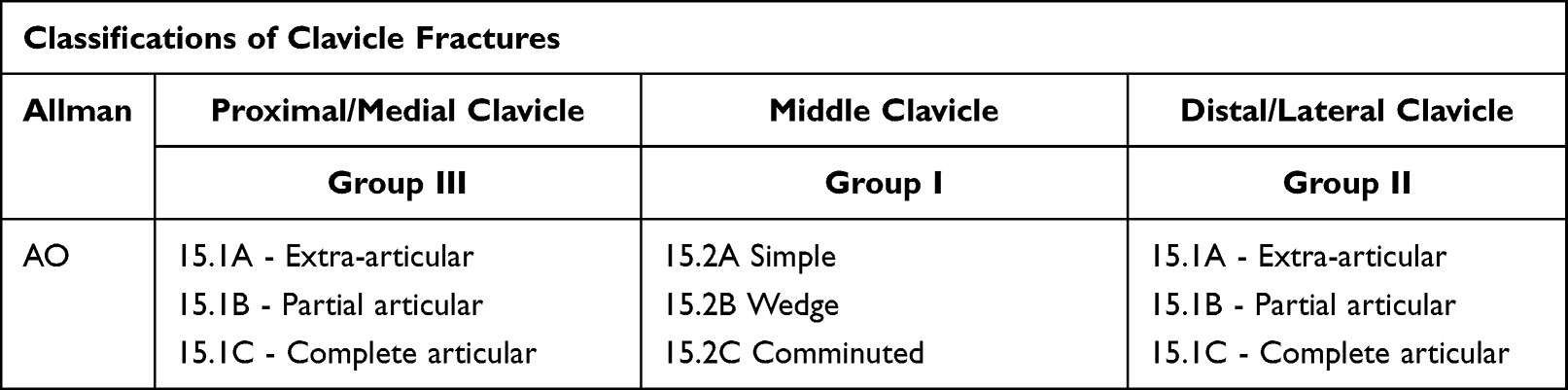 |
Table 1 Classifications of Clavicle Fractures |
Diagnosis
Clinical Evaluation
During initial evaluation, a thorough history and physical examination exam should be performed. In the setting of trauma, abrasions or ecchymosis may be seen on the shoulder with a direct blow or midline seen in seat belt shoulder strap injuries. Palpation will reveal tenderness, and crepitus may be felt with gentle manipulation. Displaced fractures that pierce through the trapezial fascia can result in skin that is blanched and no longer mobile over the fracture fragment. These characteristic findings are commonly referred to as “tenting” of the skin (Figure 2) and signify threatened skin at subsequent risk of progressing to open skin.
 |
Figure 2 Depiction of skin tenting seen in a displaced clavicle fracture. Notes: Reproduced from Antabak A, Matković N, Stanić L et al. Results of Clavicle Fracture Treatment in Children. Acta Clin Croat. 2015;54(3):6. Open Access.60 |
Due to the proximity of the brachial plexus and subclavian vessels, it is important to perform a complete neurovascular exam. Skin discoloration or decreased distal pulses may be present with a subclavian vessel injury. Focal neurologic deficits distally along the arm may represent a brachial plexus injury, with the ulnar nerve being at highest risk given its location adjacent to the middle third of the clavicle.2 A complete lung examination with appropriate chest radiographs, pulse oximetry, and auscultation should be performed, particularly in the setting of subjective dyspnea, as there may be an injury to the lung apex resulting in a hemothorax or pneumothorax. Injuries associated with the ipsilateral upper extremity must also be evaluated, such as associated rib or scapula fractures. An associated ipsilateral proximal humerus fracture is indicative of a floating shoulder, a relative indication of fixation. Patients with poly-trauma may also benefit from fixation to facilitate earlier mobilization and upper extremity (UE) weight-bearing.
Radiographic Evaluation
Shortening is important in determining management; however, there is considerable variability in the techniques used to measure shortening. Shortening may be measured on a standardized 15° tilted radiograph of the clavicle, a 15° uptilted AP panorama radiograph of the shoulder girdle, a standardized PA thorax radiograph,28 an abduction lordosis view,29 or clinically with a simple tape measure.15,30 In a comparison analysis, Smekal et al found that PA thorax radiographs with the patient standing erect had the highest agreement with CT measurement.31 Additionally, the measurement of shortening in the literature can vary with some using an end-to-end technique described as measuring the distance between the most lateral tip of the major medial fragment and the most medial tip of the major lateral fragment.32 More readily used is a cortex-to-corresponding-cortex measurement described as “true” shortening, which is the distance from the fracture tip of the major medial fragment to the corresponding defect, or lucency, on the major lateral fragment, or vice versa.1
The role of advanced imaging in adolescent clavicle fractures is unclear. CT allows for three-dimensional reconstruction of the clavicle, which is important in determining the true total length of the clavicle, the fracture pattern and also in assessing comminuted fractures.31 Pandya et al advocated for routine use of CT to evaluate total length, shortening, and comminution fractures requiring surgical fixation.15 Drawbacks of the use of routine CT include cost and radiation exposure, with the latter being of particular concern in the pediatric and adolescent population given their greater radiosensitivity.33 There is currently no consensus on which clavicle fractures require advanced imaging, though in the setting of complex fracture patterns they may be useful for surgical planning.
Management
Nonoperative Treatment
Historically, pediatric clavicle fractures have been universally treated nonoperatively. This approach was championed by classic studies, such as that by Neer at al., which found a 0.1% non-union rate in over 2000 middle-third adult clavicle fractures, and by Wilkes et al, who in 1987 similarly documented adequate remodeling up to 90° and 4 cm overlap in 35 children with displaced midshaft clavicle fractures.34–36 As seen in Table 2, indications for nonoperative treatment include all acute non-displaced fractures.
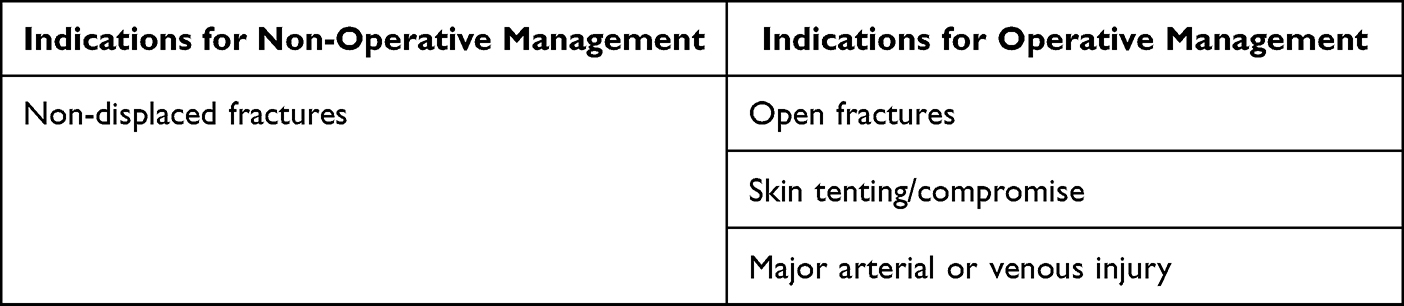 |
Table 2 Indications for Non-Operative and Operative Management |
Common options for nonoperative treatment include observation without immobilization, sling or shoulder immobilization, or figure-of-eight brace immobilization.15,35 The duration of immobilization is generally 2 to 4 weeks, followed by progressive range of motion. Questions remain regarding optimal immobilization. In a Cochrane review analyzing different methods for nonoperative treatment for acute middle-third clavicle fractures, Lenza et al assessed two trials comparing figure-of-eight brace with arm sling.37 The only statistically significant difference in clinical outcomes was that the patients treated with figure-of-eight bracing had significantly higher pain scores at 15-day follow-up in one trial.37 Additionally, they found that in one study 9 of 34 patients (26%) were dissatisfied with the figure-of-eight brace compared with only 2 of 27 patients (7%) with arm slings. The authors postulated that the difference was associated with discomfort caused by the figure-of-eight brace, including agility impairments, difficulty with personal care, arm edema, sleep disturbance, and paresthesias.15,37 Other considerations commented on in the literature are that a sling is more visible, thus alerting others to the child’s injury, and more readily available in primary and urgent care settings; however, it does not allow use of the hand, wrist, or elbow, potentially leading to stiffness.35 This is compared to the figure-of-eight brace, which will allow free use of both hands and can be hidden under normal clothing; however, it also crosses over at the fracture site, causing discomfort, and is considerably more expensive than a sling.35 Currently, there is insufficient evidence to definitively favor one versus the other; however, given many of the above discussed benefits, we prefer the use of a sling when nonsurgical management is indicated.
After a period of immobilization and progressive range of motion, return to sport is usually between 8–12 weeks, depending on activity level. A review of 36 nonoperatively managed adolescents with clavicle fractures demonstrated a return to sport in 61 ± 38 days, with fracture displacement, greater comminution, and angulation all being risk factors for a slower return to sport.38
Indications for Operative Treatment
Absolute indications for operative treatment of pediatric and adolescent clavicle fractures are listed in Table 2, including open fractures, skin tenting/compromise, and major arterial or venous injury. Refracture and nonunions are also common indications for fixation. However, with the expansion of surgical indications for operative treatment of clavicle fractures in adults has come a discussion of likewise expanding indications in adolescents. One of the landmark studies in adults that has been used to advocate for these expanding indications is the multicenter study performed by the Canadian Orthopedic Trauma Society, prospectively comparing nonsurgical management with plate fixation for displaced midshaft clavicle fractures. They found that surgically managed fractures had improved Disability of the Arm, Shoulder, and Hand (DASH) scores, faster time to radiographic union (16.4 weeks versus 28.4 weeks), decreased rate of nonunion and malunion and improved patient satisfaction.39 Of note, this study included patients aged 16 and older and therefore it is not applicable to all adolescents.
Understanding the basis for the expansion of indications in adults is critical to the discussion of how these may be relevant in our pediatric population. Pandya et al, in a review of adolescent clavicle fractures, argues that we should consider whether indications used for adult fractures, such as presence of >15mm of shortening, 100% displacement and/or significant comminution, should be used for the subset of pediatric patients participating in higher-demand activities for which adult-type demands are placed on the shoulder girdle, resulting in fracture patterns resembling high-energy adult trauma. Despite this, exact indications for operative treatment besides those listed in Table 2 are controversial.
Operative Techniques
Open reduction and internal fixation can be performed using plates and screws or elastic stable intramedullary nailing (ESIN) in supine or beach chair position, on a radiolucent table, with the head and neck tilted away from the operative side. A bump should be placed behind the scapula to bring the shoulder girdle forward, aiding in reduction. The arm is prepped in the field to allow for manipulation and traction. Traditionally, an incision is made directly over the clavicle following Langer’s lines. However, some advocate for a more anteroinferior skin incision with subsequent mobilization of the skin and clavipectoral fascia superiorly to allow for visualization of the clavicle. Once the plate is applied, the skin is released and the incision will not be directly over the plate, theoretically limiting wound complications.40
A 3.5 mm dynamic compression plate or plate of similar strength should be used with at least six cortices on each side.2 Semi-tubular plates are not adequately rigid and should not be used for definitive fixation.41,42 Both reconstruction plates and pre-contoured plates have been successfully utilized, with the pre-contoured offering the advantage of ease of placement without significant manipulation of the plate.2 Locked plates offer no significant advantage to conventional plating for pediatric midshaft clavicle fractures and cost considerably more, so are generally avoided.
Placement of the plate is another factor one must consider. Definitive plate fixation can be achieved with position of the plate either anteriorly or superiorly on the clavicle. Early mechanical analysis demonstrated that superior plate placement exhibited significantly greater biomechanical stability in axial and torsional stiffness than those plated at the anterior aspect.43 Subsequent analysis by Favre demonstrated that superior plating is less likely to fail in axial compression while anteroinferior plating was less likely to fail in cantilever bending.44 Nourian demonstrated via meta-analysis that there was no significant difference between anteroinferior plating and superior plating with regard to DASH scores, union rates, or implant failures. Patients who received superior plating had a higher probability of symptomatic hardware and higher rates of implant removal.45
Dual plating of both the anteroinferior and superior surfaces can also be performed. Cadaveric studies in adult clavicles have demonstrated dual plate constructs with a superior 2.4-mm and anterior 2.7-mm plate to be stiffer with axial loading than single plate constructs. However, dual plate constructs had similar torsional and bending stiffness to anterior single plate constructs.46 Though we can extrapolate some data from adult populations, none of these studies were specifically performed in the adolescent or pediatric population and differences between plating position in this population remain an open question. Despite increased biomechanical stability, there are no studies in a pediatric population to suggest that dual plate constructs improve clinical outcomes. It is the author’s opinion that, for the majority of clavicle fractures, single plate constructs, either anteroinferior or superior, will be sufficient.
Use of ESIN for internal fixation of midshaft clavicle fractures has also been described. Patient positioning can be supine or beach chair. The fracture can be closed or open. A small incision is made over the medial clavicle and start site is achieved fluoroscopically to be in line with the intramedullary canal. After reaming, the nail is advanced across the fracture site and fixed to both segments. Similarly, threaded K-wire fixation without reaming can be used for operative fixation, although there is limited information in the pediatric and adolescent literature on this technique. Prinz et al reported on the use of K-wire (n=2) and ESIN (n=8) fixation for pediatric clavicle fractures and found that all achieved good functional and cosmetic results.47 Fuglesang randomized 123 adult patients to either plate fixation or ESIN and found that plate fixation resulted in a faster functional recovery in the first six months, with no differences at one year.48 However, the recovery after ESIN was noted to be slower in those with increasing fracture comminution.48 Smekal et al similarly found that for midshaft clavicle fractures with comminution they were unable to restore clavicular length, resulting in nonunion and telescoping of the implant.49 In addition, intramedullary nailing of clavicular midshaft fractures is technically demanding, with risk of high fluoroscopy and surgical times, cortical perforations, nail breakage, and hardware irritation.15,50 For these reasons, we do not generally recommend nailing for pediatric clavicle fractures.
Postoperatively, for both plate fixation and ESIN, unrestricted shoulder motion is allowed in a progressive fashion. For ESIN, when rotational stability is a concern, some advocate for restrictions in forward elevation to 90° and abduction to 90° for the first 4 weeks.2 Return to full sports participation generally occurs between 8–12 weeks.
Outcomes from Nonoperative and Operative Treatment
Nonunion and Malunion
In the pediatric and adolescent population, clavicular nonunions are very rare complications. A systematic review in 2018 found only 20 cases of reported clavicle fracture nonunions in patients between the ages of 4–17 across 13 articles.51 No denominator of total cases were given so we were unable to determine true incidence of clavicular nonunion. Management of plate and screw surgical fixation for 16 of 20 cases achieved good functional outcomes . Similarly, a separate retrospective analysis conducted over an 11-year period across 9 institutions only found 25 nonunion cases.52 In their review, no patients were younger than 10 years old, although demographic factors, such as age and gender, and radiographic factors, such as fracture displacement, AO classification, shortening, and comminution, were not found to be associated with clavicle nonunions. One-hundred percent of nonunion cases underwent surgical management (92% plate fixation and 8% intramedullary compression screw), with 24/25 patients showing healing of nonunion clavicles at an average of 12.4±5.6 weeks.52 Overall, nonunion rates are very low and exceedingly infrequent in those younger than 10, though management can be successful with surgical fixation.
Regarding malunion, Heyworth et al found the frequency of clavicular malunion to be 3.8% after surgical treatment and 4.6% after nonoperative treatment.53 While management of malunion in adults is more frequently operative, the mainstay of treatment for clavicular malunion in the pediatric and adolescent population is nonoperative. Bae et al looked at 16 children and adolescents with clavicular malunion following nonoperative treatment of clavicle fracture with displacement of >2cm. At a mean 27.2 months after injury, all displaced fractures achieved union with continued nonoperative treatment with no clinically meaningful loss of shoulder motion or abduction/adduction strength.6
Hardware Prominence and Refracture
A common complication in the adult literature, hardware prominence is likewise an issue for adolescents undergoing surgical fixation. Li et al looked at 36 patients, age 10–18, with displaced midshaft clavicle fractures who underwent surgical fixation and found an overall complication rate of 86% (32/37), of which 59% (22/37) was from implant prominence or irritation. Of 37 patients, 15 (40%) underwent a second surgery for implant removal secondary to pain and prominence.54 Namdari et al reported an implant removal rate of 28.6% in their analysis of 14 adolescent patients with displaced midshaft clavicle fractures.55 Some surgeons even advocate for routine elective removal of hardware, as seen in Mehlman et al, in which all 24 of their adolescent patients who underwent plate fixation had their hardware removed.56
Though a rare phenomenon, refracture can also occur after operative treatment. Li et al, in 2018, described above, also reported that 1 patient sustained a refracture 3 weeks after plate removal while snowboarding.54 Swarup et al in 2021 also noted that 2 out of 43 (5%) operatively treated midshaft clavicle fractures in adolescents sustained refracture.
Functional Outcomes
Nonoperative treatment, which has historically been the mainstay of treatment for these fractures, continues to demonstrate good functional outcomes. Recently, Schulz et al performed maximal and endurance strength and range of motion testing in 16 patients, 10 to 18 years old, with isolated, completely displaced, shortened, midshaft clavicle fractures treated nonoperatively. Compared with the uninjured limb and measured 2 years from injury, no differences were noted in range of motion or strength, except for an 8% decrease in maximal shoulder external rotation strength (p=0.04) and an 11% loss of shoulder abduction endurance strength (p=0.04). Additionally, SANE (Single Assessment Numeric Evaluation), QuickDASH (shortened version of the Disabilities of the Arm, Shoulder and Hand questionnaire), and Constant scores were similar between sides. Interestingly, they also noted a 100% union rate but with significant shortening compared to the uninjured clavicle, which, as demonstrated, did not affect patients’ functional outcome.9 Parry et al, in a smaller study, similarly evaluated 8 operatively treated and 8 nonoperatively treated displaced clavicle fractures with >15-mm shortening and a minimum of 9-month follow-up and found no difference in range of motion, strength, or endurance between groups. However, operatively treated patients had a 3% decreased abduction endurance rate compared with the uninjured side.57 Of note, this difference is likely clinically insignificant.
Patient Outcomes
Studies directly comparing functional outcomes of adolescents treated nonoperatively and operatively show overall good functional recovery regardless of treatment. Swarup et al, in their prospective analysis, looked at 43 operatively treated and 36 nonoperatively treated displaced midshaft clavicle fractures with a median 3.8-year follow-up. They found no difference in QuickDash, University of California Los Angeles (UCLA) Activity Scale, or Patient-Reported Outcomes Measurement Information System (PROMIS) scores between groups, even for patients at or near skeletal maturity and those with shortening of >15 mm or >100% translation.58 This is similar to 2-year results from the FACTS study, which showed that, while greater percentages of operative than nonoperative patients reported suboptimal satisfaction scores (ASES: 15% vs. 5%, QuickDASH 11% vs 5%, satisfaction 11% vs 5%), these differences did not reach significance.53
Summary
A common injury seen from direct trauma or sports participation, pediatric and adolescent midshaft clavicle fractures can generally be treated nonoperatively with a brief period of sling immobilization followed by range of motion. Operative treatment is more heavily considered in the setting of open injury, neurovascular compromise, and soft tissue complications. Outcomes after nonoperative treatment of midshaft clavicle fractures are comparable to operative treatment at both mid- and long-term follow-up in pediatric and adolescent patients.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ellis HB, Li Y, Bae DS, et al. Descriptive epidemiology of adolescent clavicle fractures: results from the FACTS (function after adolescent clavicle trauma and surgery) prospective, multicenter cohort study. Orthop J Sports Med. 2020;8(5):2325967120921344. doi:10.1177/2325967120921344
2. Jeray KJ. Acute midshaft clavicular fracture. J Am Acad Orthop Surg. 2007;15(4):239–248. doi:10.5435/00124635-200704000-00007
3. Postacchini F, Gumina S, De Santis P, Albo F. Epidemiology of clavicle fractures. J Shoulder Elbow Surg. 2002;11(5):452–456. doi:10.1067/mse.2002.126613
4. Ropars M, Thomazeau H, Huten D. Clavicle fractures. Orthop Traumatol Surg Res. 2017;103(1S):S53–S59. doi:10.1016/j.otsr.2016.11.007
5. Shultz R, Kedgley AE, Jenkyn TR. Quantifying skin motion artifact error of the hindfoot and forefoot marker clusters with the optical tracking of a multi-segment foot model using single-plane fluoroscopy. Gait Posture. 2011;34(1):44–48. doi:10.1016/j.gaitpost.2011.03.008
6. Bae DS, Shah AS, Kalish LA, Kwon JY, Waters PM. Shoulder motion, strength, and functional outcomes in children with established malunion of the clavicle. J Pediatr Orthop. 2013;33(5):544–550. doi:10.1097/BPO.0b013e3182857d9e
7. Pennock AT, Heyworth BE, Bastrom T, et al. Changes in superior displacement, angulation, and shortening in the early phase of healing for completely displaced midshaft clavicle fractures in adolescents: results from a prospective, multicenter study. J Shoulder Elbow Surg. 2021;30(12):2729–2737. doi:10.1016/j.jse.2021.05.006
8. Robinson L, Gargoum R, Auer R, Nyland J, Chan G. Sports participation and radiographic findings of adolescents treated nonoperatively for displaced clavicle fractures. Injury. 2015;46(7):1372–1376. doi:10.1016/j.injury.2015.04.019
9. Schulz J, Moor M, Roocroft J, Bastrom TP, Pennock AT. Functional and radiographic outcomes of nonoperative treatment of displaced adolescent clavicle fractures. J Bone Joint Surg Am. 2013;95(13):1159–1165. doi:10.2106/JBJS.L.01390
10. Hagstrom LS, Ferrick M, Galpin R. Outcomes of operative versus nonoperative treatment of displaced pediatric clavicle fractures. Orthopedics. 2015;38(2):e135–e138. doi:10.3928/01477447-20150204-62
11. Riiser MO, Molund M. Long-term functional outcomes and complications in operative versus nonoperative treatment for displaced midshaft clavicle fractures in adolescents: a retrospective comparative study. J Pediatr Orthop. 2021;41(5):279–283. doi:10.1097/BPO.0000000000001768
12. Scott ML, Baldwin KD, Mistovich RJ. Operative versus nonoperative treatment of pediatric and adolescent clavicular fractures: a systematic review and critical analysis. JBJS Rev. 2019;7(3):e5. doi:10.2106/JBJS.RVW.18.00043
13. Ogata S, Uhthoff HK. The early development and ossification of the human clavicle--an embryologic study. Acta Orthop Scand. 1990;61(4):330–334. doi:10.3109/17453679008993529
14. Burnham JM, Kim DC, Kamineni S. Midshaft clavicle fractures: a critical review. Orthopedics. 2016;39(5):e814–821. doi:10.3928/01477447-20160517-06
15. Pandya NK, Namdari S, Hosalkar HS. Displaced clavicle fractures in adolescents: facts, controversies, and current trends. JAAOS. 2012;20(8):498–505. doi:10.5435/JAAOS-20-08-498
16. Landin LA. Fracture patterns in children. Analysis of 8682 fractures with special reference to incidence, etiology and secular changes in a Swedish urban population 1950–1979. Acta Orthop Scand Suppl. 1983;202:1–109.
17. Nordqvist A, Petersson C. The incidence of fractures of the clavicle. Clin Orthop Relat Res. 1994;300:127–132. doi:10.1097/00003086-199403000-00016
18. Rennie L, Court-Brown CM, Mok JYQ, Beattie TF. The epidemiology of fractures in children. Injury. 2007;38(8):913–922. doi:10.1016/j.injury.2007.01.036
19. van der Meijden OA, Gaskill TR, Millett PJ. Treatment of clavicle fractures: current concepts review. J Shoulder Elbow Surg. 2012;21(3):423–429. doi:10.1016/j.jse.2011.08.053
20. Robinson CM. Fractures of the clavicle in the adult: epidemiology and classification. J Bone Joint Surg Am. 1998;80-B(3):476–484. doi:10.1302/0301-620X.80B3.0800476
21. Suppan CA, Bae DS, Donohue KS, Miller PE, Kocher MS, Heyworth BE. Trends in the volume of operative treatment of midshaft clavicle fractures in children and adolescents: a retrospective, 12-year, single-institution analysis. J Pediatr Orthop B. 2016;25(4):305–309. doi:10.1097/BPB.0000000000000301
22. Luo TD, Ashraf A, Larson AN, Stans AA, Shaughnessy WJ, McIntosh AL. Complications in the treatment of adolescent clavicle fractures. Orthopedics. 2015;38(4). doi:10.3928/01477447-20150402-56
23. Perlow JH, Wigton T, Hart J, Strassner HT, Nageotte MP, Wolk BM. Birth trauma. A five-year review of incidence and associated perinatal factors. J Reprod Med. 1996;41(10):754–760.
24. Hughes CA, Harley EH, Milmoe G, Bala R, Martorella A. Birth trauma in the head and neck. Arch Otolaryngol Head Neck Surg. 1999;125(2):193–199. doi:10.1001/archotol.125.2.193
25. Ergün T, Sarikaya S. Newborn clavicle fractures: does clavicle fracture morphology affect brachial plexus injury? J Pediatr Orthop. 2022;42(4):e373. doi:10.1097/BPO.0000000000002071
26. Allman FL. Fractures and ligamentous injuries of the clavicle and its articulation. J Bone Joint Surg Am. 1967;49(4):774–784. doi:10.2106/00004623-196749040-00024
27. Meinberg EG, Agel J, Roberts CS, Karam MD, Kellam JF. Fracture and Dislocation Classification Compendium-2018. J Orthop Trauma. 2018;32(Suppl 1):S1–S170. doi:10.1097/BOT.0000000000001063
28. Lazarides S, Zafiropoulos G. Conservative treatment of fractures at the middle third of the clavicle: the relevance of shortening and clinical outcome. J Shoulder Elbow Surg. 2006;15(2):191–194. doi:10.1016/j.jse.2005.08.007
29. Riemer BL, Butterfield SL, Daffner RH, O’Keeffe RM. The abduction lordotic view of the clavicle: a new technique for radiographic visualization. J Orthop Trauma. 1991;5(4):392–394. doi:10.1097/00005131-199112000-00002
30. McKee MD, Wild LM, Schemitsch EH. Midshaft malunions of the clavicle. Surgical technique. J Bone Joint Surg Am. 2004;86-A(Suppl 1):37–43. doi:10.2106/00004623-200403001-00006
31. Smekal V, Deml C, Irenberger A, et al. Length determination in midshaft clavicle fractures: validation of measurement. J Orthop Trauma. 2008;22(7):458–462. doi:10.1097/BOT.0b013e318178d97d
32. Silva SR, Fox J, Speers M, et al. Reliability of measurements of clavicle shaft fracture shortening in adolescents. J Pediatr Orthop. 2013;33(3):e19–e22. doi:10.1097/BPO.0b013e318287f73f
33. Brenner DJ, Hall EJ. Computed tomography--an increasing source of radiation exposure. N Engl J Med. 2007;357(22):2277–2284. doi:10.1056/NEJMra072149
34. Neer CS. NONUNION OF THE CLAVICLE. JAMA. 1960;172(10):1006. doi:10.1001/jama.1960.03020100014003
35. Schlechter JA. Clavicle fractures in children and adolescents; 2010.
36. Wilkes JA, Hoffer MM. Clavicle fractures in head-injured children. J Orthop Trauma. 1987;1(1):55–58. doi:10.1097/00005131-198701010-00008
37. Lenza M, Belloti JC, Andriolo RB, Faloppa F. Conservative interventions for treating middle third clavicle fractures in adolescents and adults. Cochrane Database Syst Rev. 2014;(5):CD007121. doi:10.1002/14651858.CD007121.pub3
38. Ahearn BM, Shanley E, Thigpen CA, Pill SG, Kissenberth MJ. Factors influencing time to return to sport following clavicular fractures in adolescent athletes. J Shoulder Elbow Surg. 2021;30(7):S140–S144. doi:10.1016/j.jse.2021.04.006
39. Canadian Orthopaedic Trauma Society. Nonoperative treatment compared with plate fixation of displaced midshaft clavicular fractures. A multicenter, randomized clinical trial. J Bone Joint Surg Am. 2007;89(1):1–10. doi:10.2106/JBJS.F.00020
40. Coupe BD, Wimhurst JA, Indar R, Calder DA, Patel AD. A new approach for plate fixation of midshaft clavicular fractures. Injury. 2005;36(10):1166–1171. doi:10.1016/j.injury.2005.03.007
41. Böstman O, Manninen M, Pihlajamäki H. Complications of plate fixation in fresh displaced midclavicular fractures. J Trauma. 1997;43(5):778–783. doi:10.1097/00005373-199711000-00008
42. Poigenfürst J, Rappold G, Fischer W. Plating of fresh clavicular fractures: results of 122 operations. Injury. 1992;23(4):237–241. doi:10.1016/s0020-1383(05)80006-3
43. Iannotti MR, Crosby LA, Stafford P, Grayson G, Goulet R. Effects of plate location and selection on the stability of midshaft clavicle osteotomies: a biomechanical study. J Shoulder Elbow Surg. 2002;11(5):457–462. doi:10.1067/mse.2002.125805
44. Favre P, Kloen P, Helfet DL, Werner CML. Superior versus anteroinferior plating of the clavicle: a finite element study. J Orthop Trauma. 2011;25(11):661–665. doi:10.1097/BOT.0b013e3182143e06
45. Nourian A, Dhaliwal S, Vangala S, Vezeridis PS. Midshaft fractures of the clavicle: a meta-analysis comparing surgical fixation using anteroinferior plating versus superior plating. J Orthop Trauma. 2017;31(9):461–467. doi:10.1097/BOT.0000000000000936
46. Kitzen J, Paulson K, Korley R, Duffy P, Martin CR, Schneider PS. Biomechanical evaluation of different plate configurations for midshaft clavicle fracture fixation: single plating compared with dual mini-fragment plating. JB JS Open Access. 2022;7(1):
47. Prinz KS, Rapp M, Kraus R, Wessel LM, Kaiser MM. Dislozierte Klavikulafrakturen im Kindes-und Jugendalter: Wer profitiert von einer Operation? [Dislocated midclavicular fractures in children and adolescents: who benefits from operative treatment?]. Z Orthop Unfall. 2010;148(1):60–65. German. doi:10.1055/s-0029-1186155
48. Fuglesang HFS, Flugsrud GB, Randsborg PH, Oord P, Jš B, Utvåg SE. Plate fixation versus intramedullary nailing of completely displaced midshaft fractures of the clavicle: a prospective randomised controlled trial. Bone Joint J. 2017;99-B(8):1095–1101. doi:10.1302/0301-620X.99B8.BJJ-2016-1318.R1
49. Smekal V, Irenberger A, Attal RE, Oberladstaetter J, Krappinger D, Kralinger F. Elastic stable intramedullary nailing is best for mid-shaft clavicular fractures without comminution: results in 60 patients. Injury. 2011;42(4):324–329. doi:10.1016/j.injury.2010.02.033
50. Vander Have KL, Perdue AM, Caird MS, Farley FA. Operative versus nonoperative treatment of midshaft clavicle fractures in adolescents. J Pediatr Orthop. 2010;30(4):307–312. doi:10.1097/BPO.0b013e3181db3227
51. Hughes K, Kimpton J, Wei R, et al. Clavicle fracture nonunion in the paediatric population: a systematic review of the literature. J Child Orthop. 2018;12(1):2–8. doi:10.1302/1863-2548.12.170155
52. Pennock AT, Edmonds EW, Bae DS, et al. Adolescent clavicle nonunions: potential risk factors and surgical management. J Shoulder Elbow Surg. 2018;27(1):29–35. doi:10.1016/j.jse.2017.06.040
53. Heyworth BE, Pennock AT, Li GY, et al. Two-year functional outcomes of operative vs. non-operative treatment of completely displaced midshaft clavicle fractures in adolescents: results from a prospective, multicenter, level 2 study. Orthop J Sports Med. 2019;7(7_suppl5):2325967119S0042. doi:10.1177/2325967119S00428
54. Li Y, Helvie P, Farley FA, Abbott MD, Caird MS. Complications after plate fixation of displaced pediatric midshaft clavicle fractures. J Pediatr Orthop. 2018;38(7):350–353. doi:10.1097/BPO.0000000000000832
55. Namdari S, Ganley TJ, Baldwin K, et al. Fixation of displaced midshaft clavicle fractures in skeletally immature patients. J Pediatr Orthop. 2011;31(5):507–511. doi:10.1097/BPO.0b013e318220ba48
56. Mehlman CT, Yihua G, Bochang C, Zhigang W. Operative treatment of completely displaced clavicle shaft fractures in children. J Pediatr Orthop. 2009;29(8):851–855. doi:10.1097/BPO.0b013e3181c29c9c
57. Parry JA, Van Straaten M, Luo TD, et al. Is there a deficit after nonoperative versus operative treatment of shortened midshaft clavicular fractures in adolescents? J Pediatr Orthop. 2017;37(4):227–233. doi:10.1097/BPO.0000000000000627
58. Swarup I, Maheshwer B, Orr S, Kehoe C, Zhang Y, Dodwell E. Intermediate-term outcomes following operative and nonoperative management of midshaft clavicle fractures in children and adolescents: internal fixation may improve outcomes. JB JS Open Access. 2021;6(1):
59. Johnson P, McKee M. 6 - midshaft clavicle fractures. In: Garrigues GE, Richard MJ, Gage MJ editors. Skeletal Trauma of the Upper Extremity. Elsevier; 2022:28–35. doi:10.1016/B978-0-323-76180-2.00006-4
60. Antabak A, Matković N, Stanić L, et al. Results of clavicle fracture treatment in children. Acta Clin Croat. 2015;54(3):6.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.