")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Long Term Survival Benefits of Different Conduits Used in Coronary Artery Bypass Graft Surgery- A Single Institutional Practice Over 20 Years
Authors Momin A, Ranjan R , Valencia O, Jacques A, Lim P, Fluck D, Chua TP, Chandrasekaran V
Received 21 February 2024
Accepted for publication 3 April 2024
Published 8 April 2024 Volume 2024:17 Pages 1505—1512
DOI https://doi.org/10.2147/JMDH.S461567
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Aziz Momin,1 Redoy Ranjan,1,2 Oswaldo Valencia,1 Adam Jacques,3 Pitt Lim,4 David Fluck,3 Tuan P Chua,5 Venkatachalam Chandrasekaran1
1Department of Cardiac Surgery, St George’s University Hospitals NHS Foundation Trust, London, UK; 2Department of Cardiac Surgery, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh; 3Department of Cardiology, Ashford and St Peter’s Hospitals NHS Foundation Trust, London, UK; 4Department of Cardiology, St George’s University Hospitals NHS Foundation Trust, London, UK; 5Department of Cardiology, Royal Surrey NHS Foundation Trust, London, UK
Correspondence: Aziz Momin, Consultant Cardiac Surgeon, St George’s University Hospitals NHS Foundation Trust, London, SW17 0QT, United Kingdom, Tel +447956336739, Email [email protected]
Objective: This study determined hazard factors and long-term survival rate of total arterial coronary artery bypass graft surgery over 20 years in an extensively large, population-based cohort.
Methods: A total of 2979 patients who underwent isolated CABG from April 1999 to March 2020 were studied in 4 groups- Group-A (bilateral internal mammary artery ± radial artery), Group-B (single internal mammary artery + radial artery ± saphenous vein), Group-C (single internal mammary artery ± saphenous vein; no radial artery), and Group-D (radial artery ± saphenous vein; no internal mammary artery). The study endpoints analysed the correlation between the number and types of grafts with the survival time following isolated CABG surgery.
Results: The total arterial revascularization (Group A) group had an admirable mean long-term survival of ~19 years, compared to 18.6 years (Group B), 15.86 years (Group C), and 10.99 years (Group D). A Kaplan-Meier curve demonstrated confidence interval (CI) for study groups- (95% CI 18.33– 19.94), (95% CI 18.14– 19.06), (95% CI 15.40– 16.32), and (95% CI 9.61– 12.38) in Group A, B, C, D respectively. In the Holm-Sidak method analysis, significant associations existed between the number of arterial grafts and the long-term outcome. A statistically significant (P≤ 0.05) long-term survival advantage for arterial grafting was demonstrated, especially total arterial revascularisation over all other combinations except single internal mammary artery + radial artery grafting.
Conclusion: In this series, over 20 years, total arterial CABG use has excellent long-term survival, achieving complete myocardial revascularisation. There is no significant difference between the BIMA group and SIMA with radial artery. However, there is a reduced survival with decreased use of arterial conduits.
Keywords: coronary artery bypass graft, CABG, bilateral internal mammary artery, total arterial CABG, long term outcome, multiple arterial graft, mortality, survival benefits
Introduction
Coronary artery bypass graft (CABG) surgery is the preferred revascularisation strategy for multivessel coronary artery disease (CAD).1,2 However, there is significant evidence in the literature that the type of conduits is directly related to graft patency rate and potentially influences the long-term surgical outcome.2,3 Graft failure or loss of graft patency is not directly linked to early postoperative mortality but is associated with recurrent angina, reoperation, and poor health-related quality of life.2–5 Recently published research articles and meta-analyses demonstrated that CABG with total arterial revascularisation (TAR), especially bilateral mammary and radial grafts, have better longevity and superior postoperative outcomes than venous grafts. A total arterial revascularisation strategy reduces postoperative morbidity, particularly in early graft failure rate, recurrent angina, and redo-CABG surgery.3–6
The left internal mammary artery (LIMA) has a superior long-term graft patency rate and has been well-established over the last 25 years.4–8 However, bilateral internal mammary artery (BIMA) graft in CABG is still under evaluation, especially regarding long-term graft patency and survival benefits. Only about 10% of European patients are revascularized with BIMA grafts. The Arterial Revascularisation Trial (ART), a multicentre RCT study, compared survival benefits between a bilateral internal mammary artery (BIMA) versus a single internal mammary artery (SIMA) and failed to demonstrate the superiority of BIMA after ten years of follow-up.9 However, the ART investigators concluded that radial graft to the left coronary system and optimized medical management in conjunction with SIMA graft to the LAD territory had similar outcomes to BIMA grafts, and surgeons could avoid certain complications like sternal wound infections.9
There is limited published data and evidence on the outcome of TAR-CABG and utilising at least one SVG (non-TAR) CABG surgery. However, a recently published meta-analysis using propensity-match scoring demonstrated superior survival benefits and long-term outcomes for multi-arterial CABG surgery.10 This superiority is based on the graft patency rates of ≥90% for BIMA and 25% for venous graft, respectively, for ten years of follow-up. Only a few RCTs observed short-term outcomes limited to small samples or survival, and most of the extensive observational studies have only described in-hospital TAR-CABG surgery outcomes.11–15
Few studies, including RCTs, observe long-term results following TAR-CABG surgery. The potential risk benefits of TAR-CABG surgery for left main CAD are due to the expectation of better graft patency and improved postoperative quality of life with total arterial revascularisation. This study evaluated the long-term survival benefits of myocardial revascularisation with multiple arterial coronary artery bypass graft surgery over 20 years in the United Kingdom.
Patients and Methods
A total of 2979 consecutive patients who underwent isolated CABG at St George’s Hospital NHS Foundation Trust from 1999 to 2020 were prospectively studied, and the last day of the census was 05 May 2021. Perioperative data were collected prospectively and validated by the data quality team. This study complies with the Declaration of Helsinki. The institutional review board clearance was waived as the audit department approved this retrospective analysis of prospectively collected data under the adult NICOR (National Institute for Cardiovascular Outcomes Research) UK database. All patients provided written informed consent, and the data collected was encrypted to ensure confidentiality and security.
Study Procedure
This study included isolated CABG patients with or without a previous history of cardiac surgery. The study excluded patients who had concomitant valvular and congenital heart diseases. This study ensured complete myocardial revascularisation with CABG surgery, and none of the patients in the study cohort was under-revascularized. Nevertheless, this study protocol was TAR for all patients <65 years and mixed conduits for ≥65 years, as in the UK, 65 years of age has been considered the start of older age. Each patient appears only once in the series, and this study population was divided into four groups:
- Group A (431 patients had total arterial revascularisation with BIMA ± Radial artery).
- Group B (823 patients had SIMA + Radial artery ± Saphenous vein graft).
- Group C (1565 patients had SIMA ± Saphenous vein: no Radial artery graft).
- Group D (160 patients had Radial artery ± saphenous vein graft; no Internal mammary artery graft).
The data quality team of the information department completed all-cause mortality and validation of NHS Numbers using the adult NICOR database. St George’s Hospital NHS Foundation Trust regularly receives notifications of death from general practitioners or other hospitals, and the data quality team is in charge of validating the patient’s NHS numbers. When patients were considered too old, we collected the last date they were known to be alive. The study endpoints analysed the correlation between the number and types of grafts with the survival time following isolated CABG surgery. The secondary study outcome evaluated the efficacy of the number of conduits and grafts in terms of survival time following CABG surgery. Dates of all-cause mortality were obtained from the hospital registry.
Statistical Analysis
A SPSS (statistical package for the social sciences) v28.0 software was utilised to analyse the data, and data were analysed for the survivors versus the deceased population. Univariate analyses determine the risk pattern in the datasets using the chi-square, Fisher’s exact test and Mann–Whitney U-tests, as appropriate. The normality of continuous variables was evaluated with the Shapiro–Wilk test, and the Kruskal-Walli’s test was utilised to compare the significance of four study groups. Multivariate logistic regression analysis utilised all independent variables with a P value of ≤0.05 to identify independent predictors of long-term mortality. Kaplan-Meier survival analysis was performed with previously found significant (P≤0.05) or clinically relevant groups. Using the Cox regression model, hazard ratios (HR) with 95% confidence intervals (CI) were observed as the independent predictors of death over the period. Furthermore, proportional hazard was assessed by the log minus log function. Significance was obtained with the Gehan-Breslow test, and the Holm-Sidak method was utilized for multiple pairwise comparisons. A P-value ≤0.05 is considered statistically significant.
Results
We observed that males are predominant, about 90.7%, 81.2%, 78.5%, and 76.3% (P<0.001), and the median (IQR: interquartile range) age was 61 (55–68), 63 (57–69), 72 (65–77), and 71 (65–77) years (P<0.001) in BIMAs, SIMA+R, SIMA-R, and Radial ± Vein groups, respectively (Table 1). Potential risk factors evaluation observed a significant difference between study groups, specifically diabetes (P=0.023), previous MI (P<0.001), hypertension (P<0.001), smoking (P=0.002), chronic pulmonary disease (P=0.05), neurological disease (P<0.001), extracardiac arteriopathy (P<0.001), preoperative AF (P<0.001), multi-vessel (≥3 vessels) CAD (P<0.001), IABP (P<0.001), previous heart surgery except for CABG (P<0.001), and NYHA Class III & IV (P<0.001) between the study groups. Approximately 60% of cases were performed electively in all study groups, and about two-thirds of the study population had good LV function (≥50% EF) except the Radial ± Vein group, where only 61.3% population had ≥50% EF, which was statistically significantly (P<0.001).
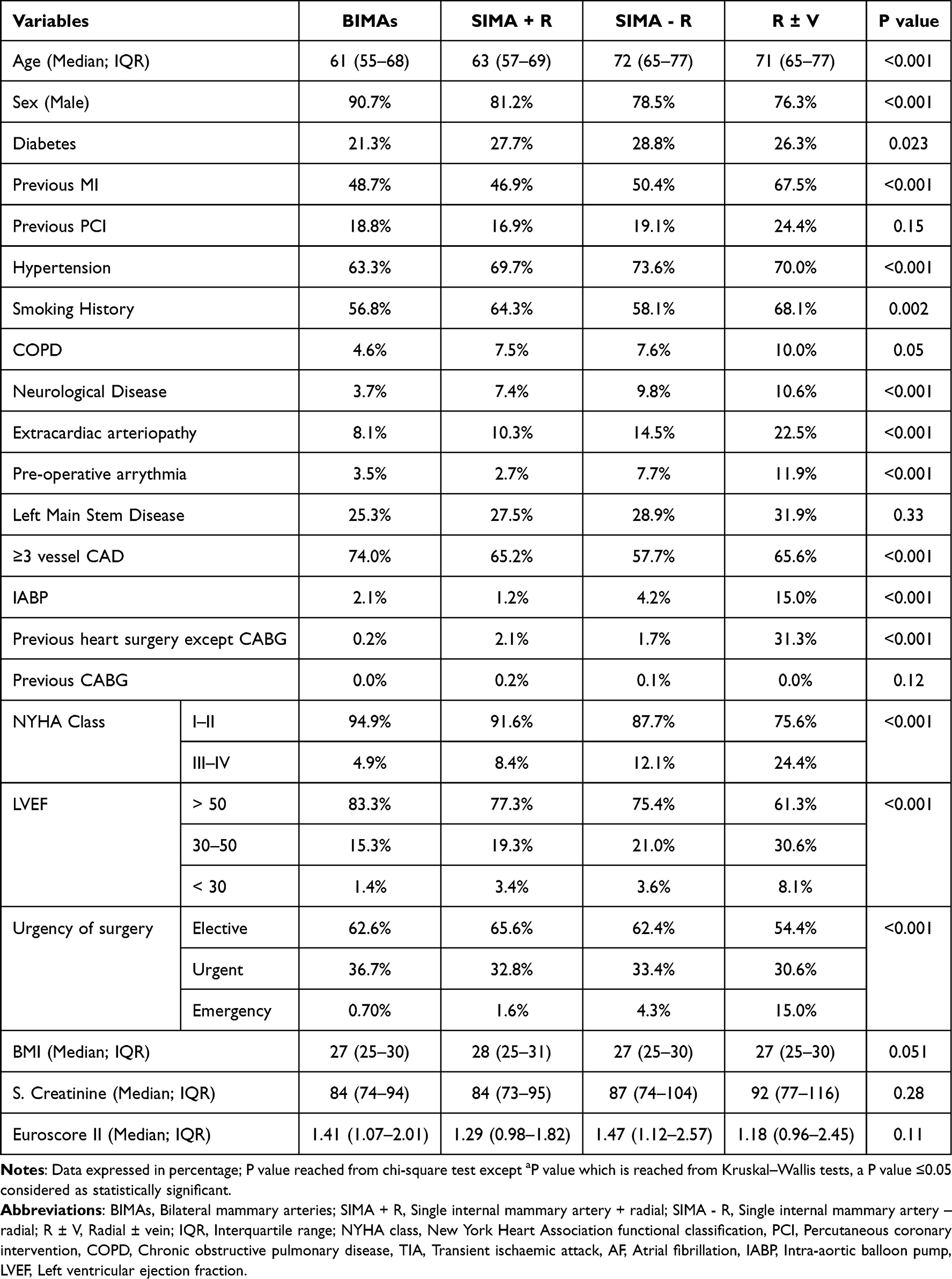 |
Table 1 Sociodemographic Variables of Study Population |
The number of used grafts was significantly higher in the BIMAs population; about 59% had ≥4 grafts in the BIMAs group, whereas only 43.5%, 41.4%, and 28.1% had ≥4 grafts in SIMA+R, SIMA-R, and Radial ± Vein group, respectively (Table 2). Chest re-exploration due to postoperative bleeding complications was higher among the Radial ± Vein group (P= 0.006). The actual age versus survival time graph observed approximately 20 years survival rate for the <60 years age group population. Moreover, the population age group 60–69, 70–79 and >80 years had a survival time of about 17.71 (95% CI 17.23–18.19), 14.98 (95% CI 14.41–15.54) and 8.86 (95% CI 7.83–9.88) years respectively (Table S1). However, a Kaplan-Meier survival analysis curve demonstrated a mean survival time of 16.9 years with a 95% CI of 16.6 −17.2 (Figure-S1). Cox proportional hazards regression model (Table 3) evaluated potential predictors of the survivability of the study population and found age (HR 1.08; 95% CI 1.07–1.09), hypertension (HR 1.31; 95% CI 1.10–1.57), diabetes on insulin (HR 1.38; 95% CI 1.08–1.77), multi-vessel CAD (HR 1.43; 95% CI 1.22–1.69), recent MI (HR 1.54; 95% CI 1.22–1.93), NYHA class III–IV (HR 1.57; 95% CI 1.29–1.92), extracardiac arteriopathy (HR 1.61; 95% CI 1.34–1.93), chest re-exploration (HR 2.14; 95% CI 1.52–3.03), and redo surgery (HR 3.04; 95% CI 2.13–4.35) are significantly associated with increase mortality of study population (P ≤0.05).
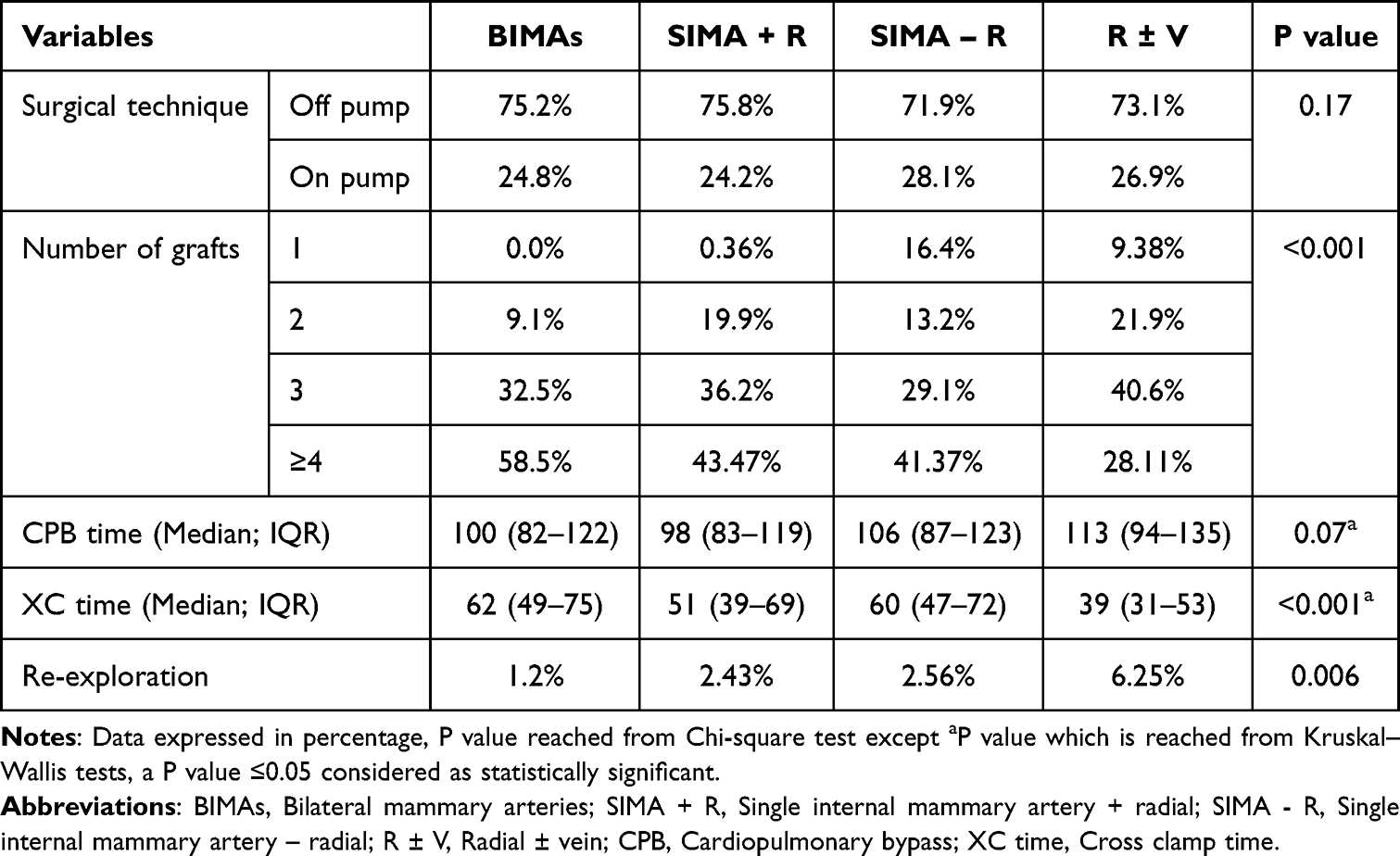 |
Table 2 Operative Variables of Study Population |
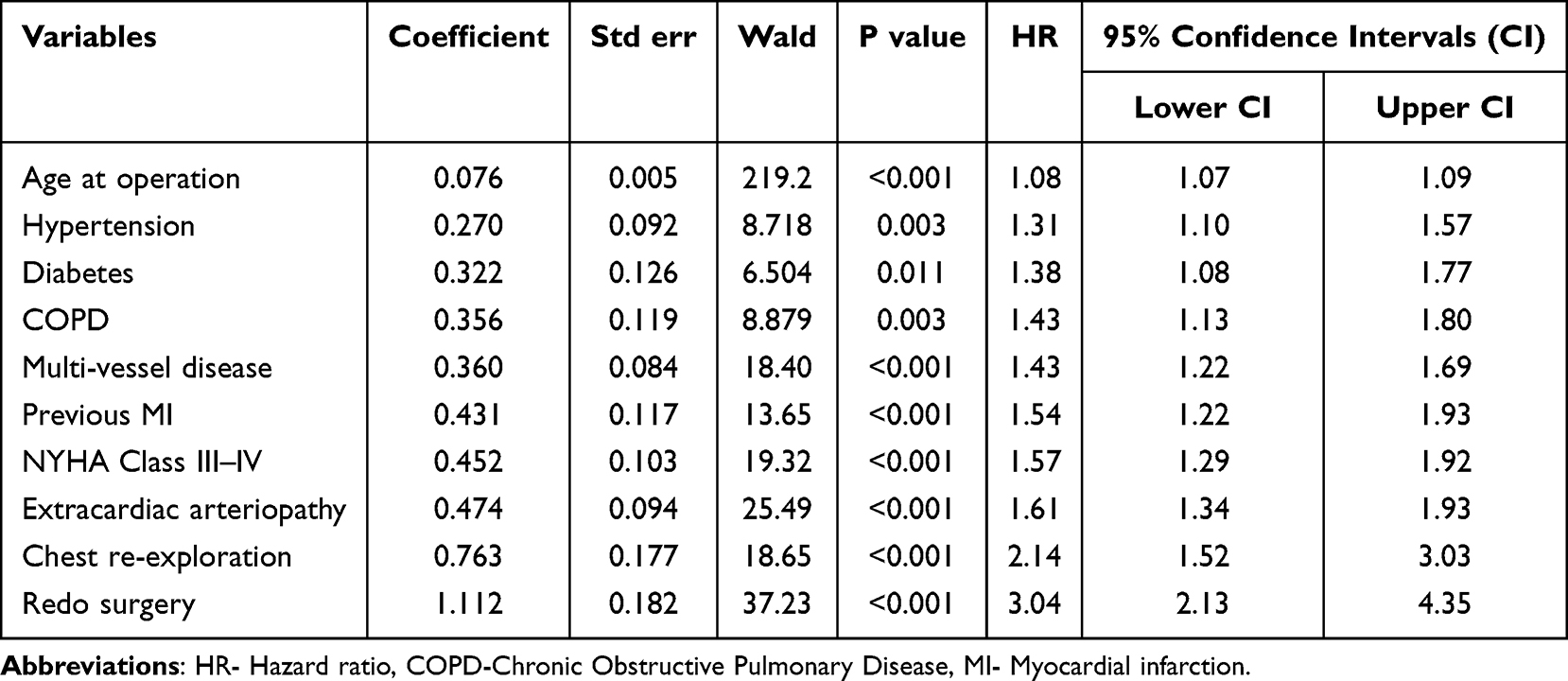 |
Table 3 Cox Regression-Proportional Hazards Model Observed Predictors of Mortality Among the Study Population |
In this study, survival time for total arterial revascularization with BIMA and radial (19.14 years, 95% CI 18.33–19.94), BIMA without radial 17.30 years, 95% CI 15.93–18.67), SIMA and radial (18.60 years, 95% CI 18.14–19.06), and SIMA without radial (15.86 years, 95% CI 15.40–16.32), was significantly higher (P<0.001) to radial ± vein without IMA (10.99 years, 95% CI 9.61–12.38) grafts (Figure-S2). Furthermore, the Holm-Sidak method analysis also demonstrated a statistical difference between the outcome of total arterial and mixed arterio-venous CABG surgery (Tables S2 and S3).
Discussion
This study observed that total arterial revascularisation (TAR) utilising BIMA and radial artery has a significantly superior long-term survival rate over 20 years in a single institution covering two adult cardiac surgeons’ practices. The TAR-CABG population had better long-term survival at 18.65 years, and the poorest outcome was in the group (Radial ± Vein) with no IMA graft at 10.99 years. Nevertheless, the Holm-Sidak method of multiple comparison analysis demonstrated statistically significant comparisons between the number of arterial grafting and the long-term postoperative outcome. The better long-term survival rate with total arterial revascularisation confirms the established prognostic benefits of LIMA to LAD graft, which has been known since the landmark paper published by Loop and coworkers in 1986.2
In multi-vessel coronary artery disease, surgical myocardial revascularisation with CABG surgery is frequently associated with several adverse events, especially graft failure.5,8–11 Recently published articles observed early graft failure commonly encountered in saphenous venous grafts, leading to recurrent angina, poor quality of life and increased reintervention rate.7–9,12–14 Further, the radial artery is usually disease-free with a good calibre and length, which is relatively resistant to atherosclerosis and has a good muscle layer that accommodates arterial pressure well and facilitates graft anastomosis. For those reasons, total arterial coronary artery bypass graft surgery utilising bilateral mammary and radial arteries has increasingly gained attention among cardiothoracic surgeons and researchers over the last few decades.2–8,11–15 However, several aspects require consideration, specifically the severity of proximal coronary artery lesions and technical challenges associated with radial artery harvesting, including vasospasm and nerve injury. Also, sternal wound infection among BIMA graft patients impedes cardiac surgeons from endorsing it as a regular conduit.8,12–16
Several published literature hypothesised that using multiple arterial grafts during myocardial revascularisation may provide better survival benefits than mixed arterial and venous grafts in CABG surgery.5–11 In a randomised controlled trial (RCTs) of 1036 CABG patients, Gaudino and coworkers found radial-artery grafts have a lower adverse cardiac event and better graft patency rate over five years of follow-up, similar to our study results.17 Furthermore, after a comprehensive analysis of 20,076 CABG patients, Pu and coworkers18 concluded that multi-arterial grafts CABG were associated with better early as well as long-term survival benefits, which concord with other study findings.19–21
A randomised controlled trial in the United Kingdom pioneered by Professor Taggart et al9 observed similar all-cause mortality between bilateral versus single IMA grafts over ten years of follow-up, comparable to other published articles.6–10,14 Moreover, Taggart and coworkers9 utilised a significant number of radial artery grafts instead of vein grafts, about 23% of grafts to the left coronary territory system. However, they advocated further studies to evaluate the graft patency rates, especially venous conduits, and quality of life in a larger population and over the long term with comprehensive follow-up. In a recent and comprehensive follow-up study to evaluate the feasibility of the LIMA and radial “Y” graft in total arterial CABG surgery, Royse et al found that the “Y” graft is a highly efficient, reliable, and flexible technique for the achievement of total arterial revascularisation.22 In another extensive retrospective cohort analysis, Rocha et al evaluated a total of 50,230 consecutive isolated CABG patients in Canada, with better long-term life expectancy and freedom from MACCEs (major adverse cardiac and cerebrovascular events) and better quality of life, similar to the current study results.23
In a recent study, Rayol et al24 observed the long-term benefits of total arterial revascularisation among the CABG population and encouraged the utilisation of arterial conduits, which concord with existing published results.16–22 Similarly, a meta-analysis comparing survival benefits among bilateral and single internal mammary artery (BIMA versus SIMA) CABG patients by Yi and coworkers observed that BIMA has a higher survival rate with up to 10 years of follow-up, and long-term survival benefits seem to have a higher survival rate to continue in the second decade of post-CABG.25 Nevertheless, Lüscher et al26 and Otsuka et al27 demonstrated that the preservation of graft patency rate is influenced by vascular endothelial nitric oxide (NO), which helps to maintain vascular tone by preventing platelet aggregation, thrombus formation, and smooth muscle cell proliferation. Additionally, arterial conduits exhibit superior endothelium‐dependent relaxation and remodelling under increased stress. In contrast, venous grafts show a decrease in the biological effects of NO, leading to vascular smooth muscle cell proliferation and acceleration of atherosclerosis and degenerative process, which results in a poor graft patency rate.26,27
Strengths and Limitations
Our study adds to this wealth of data and is unique in the findings that over 20 years, no significant long-term adverse outcomes were associated with utilising BIMAs grafts. Further, the total arterial myocardial revascularisation with CABG surgery positively impacts long-term survival benefits over 20 years.28–30 This study also advocates surgeons’ routine use of multiple arterial grafts to achieve total arterial myocardial revascularisation technique, especially in younger patients, supporting previously published papers.29–32 Albeit this is the most extensive United Kingdom-based National Health Service (NHS) cohort observing the long-term outcome of TAR-CABG, it has some limitations. This retrospective observational study is limited to all-cause mortality and is based primarily on the population from England, which is why the study findings may not be generalised elsewhere. This study analysed data from a contemporary period utilising a standard datasheet from a surgeon in the NHS Foundation Trust, UK and used propensity score matching analysis to mitigate the selection bias. Although treatment strategies, especially the choice of conduits, have evolved over the years, the NHS always maintains standard patient care that minimises the risk of outcome bias. Although the study sample was based on a heterogeneous group, the survival rate in each study group and the independent predictors from a propensity score-matched sample with similar EuroSCORE II risk profiles are topics of high interest.
Conclusion
Myocardial revascularisation with total or multi-arterial CABG surgery is safe, feasible, and associated with excellent clinical outcomes and survival benefits at 20-year follow-up compared to the mixed arterio-venous CABG population. To validate this study’s findings globally, we recommended further randomised controlled trials and prospective studies.
Data Sharing Statement
Datasets are available on reasonable request from the corresponding author.
Ethical Approval and Consent of Participants
The institutional review board clearance was waived as the St George’s Hospital audit department approved this retrospective analysis of prospectively collected data in the adult NICOR (National Institute for Cardiovascular Outcomes Research) UK database. Moreover, informed written consent was obtained from the patients, and the data were encrypted.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Marasco S. Total arterial revascularization. Oper Tech Thorac Cardiovasc Surg. 2016;21(1):20–30. doi:10.1053/j.optechstcvs.2016.08.002
2. Loop FD, Lytle BW, Cosgrove DM, et al. Influence of the internal-mammary-artery graft on 10-year survival and other cardiac events. N Engl J Med. 1986;314(1):1–6. doi:10.1056/NEJM198601023140101
3. Kumar A, Ranjan R, Adhikary AB. Postoperative atrial fibrillation following off-pump coronary artery bypass graft surgery: elderly versus young patients. Cureus. 2023;15(5):e39232. doi:10.7759/cureus.39232
4. Momin A, Ranjan R, Valencia O, et al. Survival and independent predictors of mortality following coronary artery bypass graft surgery in a single-unit practice in the United Kingdom over 20 years. Cureus. 2023;15(5):e38413. doi:10.7759/cureus.38413
5. Ranjan R, Adhikary AB. SYNTAX score and coronary artery bypass graft surgery in Bangladesh. Asian Cardiovasc Thorac Ann. 2019;27(7):542–547. doi:10.1177/0218492319869787
6. Farkouh ME, Domanski M, Dangas GD, et al. FREEDOM follow-on study investigators. Long-term survival following multivessel revascularization in patients with diabetes: the FREEDOM follow-on study. J Am Coll Cardiol. 2019;73(6):629–638. doi:10.1016/j.jacc.2018.11.001
7. Goldman S, Zadina K, Moritz T, et al. Long-term patency of saphenous vein and left internal mammary artery grafts after coronary artery bypass surgery: results from a department of veterans affairs cooperative study. J Am Coll Cardiol. 2004;44(11):2149–2156. doi:10.1016/j.jacc.2004.08.064
8. Tinica G, Chistol RO, Enache M, Leon Constantin MM, Ciocoiu M, Furnica C. Long-term graft patency after coronary artery bypass grafting: effects of morphological and pathophysiological factors. Anatol J Cardiol. 2018;20(5):275–282. doi:10.14744/AnatolJCardiol.2018.51447
9. Taggart DP, Benedetto U, Gerry S, et al. Arterial revascularization trial investigators. Bilateral versus single internal-thoracic-artery grafts at 10 years. N Engl J Med. 2019;380(5):437–446. doi:10.1056/NEJMoa1808783
10. Gaudino M, Puskas JD, Di Franco A, et al. Three arterial grafts improve late survival: a meta-analysis of propensity-matched studies. Circulation. 2017;135(11):1036–1044. doi:10.1161/CIRCULATIONAHA.116.025453
11. Head SJ, Kappetein AP. Coronary bypass surgery: an ART for dedicated surgeons. N Engl J Med. 2019;380(5):489–491. doi:10.1056/NEJMe1814681
12. Yanagawa B, Verma S, Mazine A, et al. Impact of total arterial revascularization on long term survival: a systematic review and meta-analysis of 130,305 patients. Int J Cardiol. 2017;233:29–36. doi:10.1016/j.ijcard.2017.02.010
13. Dimitrova KR, Hoffman DM, Geller CM, Dincheva G, Ko W, Tranbaugh RF. Arterial grafts protect the native coronary vessels from atherosclerotic disease progression. Ann Thorac Surg. 2012;94(2):475–481. doi:10.1016/j.athoracsur.2012.04.035
14. Aldea GS, Bakaeen FG, Pal J, et al. Society of thoracic surgeons. The society of thoracic surgeons clinical practice guidelines on arterial conduits for coronary artery bypass grafting. Ann Thorac Surg. 2016;101(2):801–809. doi:10.1016/j.athoracsur.2015.09.100
15. Mohammadi S, Dagenais F, Voisine P, et al. Impact of the radial artery as an additional arterial conduit during in-situ bilateral internal mammary artery grafting: a propensity score-matched study. Ann Thorac Surg. 2016;101(3):913–918. doi:10.1016/j.athoracsur.2015.08.054
16. Raja SG, Benedetto U, Ilsley CD, Amrani M; Harefield Cardiac Outcomes Research Group. Multiple arterial grafting confers survival advantage compared to percutaneous intervention with drug-eluting stents in multivessel coronary artery disease: a propensity score adjusted analysis. Int J Cardiol. 2015;189:153–158. doi:10.1016/j.ijcard.2015.04.059
17. Gaudino M, Benedetto U, Fremes S, et al. RADIAL investigators. Radial-artery or saphenous-vein grafts in coronary-artery bypass surgery. N Engl J Med. 2018;378(22):2069–2077. doi:10.1056/NEJMoa1716026
18. Pu A, Ding L, Shin J, et al. Long-term outcomes of multiple arterial coronary arteries bypass grafting: a population-based study of patients in British Columbia, Canada. JAMA Cardiol. 2017;2(11):1187–1196. doi:10.1001/jamacardio.2017.3705
19. Takagi H, Goto SN, Watanabe T, Mizuno Y, Kawai N, Umemoto T. A meta-analysis of adjusted hazard ratios from 20 observational studies of bilateral versus single internal thoracic artery coronary artery bypass grafting. J Thorac Cardiovasc Surg. 2014;148(4):1282–1290. doi:10.1016/j.jtcvs.2014.01.010
20. Shi WY, Tatoulis J, Newcomb AE, Rosalion A, Fuller JA, Buxton BF. Is a third arterial conduit necessary? Comparison of the radial artery and saphenous vein in patients receiving bilateral internal thoracic arteries for triple vessel coronary disease. Eur J Cardiothorac Surg. 2016;50(1):53–60. doi:10.1093/ejcts/ezv467
21. Locker C, Schaff HV, Dearani JA, et al. Multiple arterial grafts improve late survival of patients undergoing coronary artery bypass graft surgery: analysis of 8622 patients with multivessel disease. Circulation. 2012;126(9):1023–1030. doi:10.1161/CIRCULATIONAHA.111.084624
22. Royse A, Pawanis Z, Canty D, et al. The effect on survival from the use of a saphenous vein graft during coronary bypass surgery: a large cohort study. Eur J Cardiothorac Surg. 2018;54(6):1093–1100. doi:10.1093/ejcts/ezy213
23. Rocha RV, Tam DY, Karkhanis R, et al. Long-term outcomes associated with total arterial revascularization vs non–total arterial revascularization. JAMA Cardiol. 2020;5(5):507–514. doi:10.1001/jamacardio.2019.6104
24. Rayol SC, Van den Eynde J, Cavalcanti LRP, et al. Total arterial coronary bypass graft surgery is associated with better long-term survival in patients with multivessel coronary artery disease: a systematic review with meta-analysis. Braz J Cardiovasc Surg. 2021;36(1):78–85. doi:10.21470/1678-9741-2020-0653
25. Yi G, Shine B, Rehman SM, Altman DG, Taggart DP. Effect of bilateral internal mammary artery grafts on long-term survival: a meta-analysis approach. Circulation. 2014;130(7):539–545. doi:10.1161/CIRCULATIONAHA.113.004255
26. Lüscher TF, Diederich D, Siebenmann R, et al. Difference between endothelium‐dependent relaxation in arterial and venous coronary bypass grafts. N Engl J Med. 1988;319(8):
27. Otsuka F, Yahagi K, Sakakura K, Virmani R. Why is the mammary artery so special, and what protects it from atherosclerosis? Ann Cardiothorac Surg. 2013;2(4):
28. Suzuki T, Asai T, Nota H, Kinoshita T, Fujino S. Impact of total arterial reconstruction on long-term mortality and morbidity: off-pump total arterial reconstruction versus non-total arterial reconstruction. Ann Thorac Surg. 2015;100(6):2244–2249. doi:10.1016/j.athoracsur.2015.05.034
29. Dewantoro D, Nenna A, Satriano U, Chello M, Spadaccio C. Advantages and disadvantages of total arterial coronary artery bypass graft as compared to venous coronary artery bypass graft. Vessel Plus. 2018;2(8):20. doi:10.20517/2574-1209.2018.50
30. Ranjan R, Adhikary AB. Outcome of coronary artery bypass graft surgery with coronary endarterectomy. Bangladesh Med Res Counc Bull. 2018;44(2):124–131. doi:10.3329/bmrcb.v44i3.39935
31. Tranbaugh RF, Dimitrova KR, Lucido DJ, et al. The second-best arterial graft: a propensity analysis of the radial artery versus the free right internal thoracic artery to bypass the circumflex coronary artery. J Thorac Cardiovasc Surg. 2014;147(1):133–140. doi:10.1016/j.jtcvs.2013.08.040
32. Momin A, Ranjan R, Chandrasekaran V. Is complete myocardial revascularisation with total arterial coronary artery bypass graft a dream or reality? Health Sci Rep. 2023;6(8):e1532. doi:10.1002/hsr2.1532
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.