")
Back to Journals » Patient Preference and Adherence » Volume 18
Learned Helplessness and Associated Factors Among Patients with Lung Cancer
Authors Huang F , Shi Y, Ding L, Huang J, Zhang Z
Received 3 November 2023
Accepted for publication 11 January 2024
Published 22 February 2024 Volume 2024:18 Pages 467—474
DOI https://doi.org/10.2147/PPA.S446523
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Fengmei Huang,1,* Yumei Shi,1,* Li Ding,2 Jingui Huang,1 Zhaoli Zhang2
1Department of Medical Oncology, Chongqing University Cancer Hospital, Chongqing, 400030, People’s Republic of China; 2Nursing Department, Chongqing University Cancer Hospital, Chongqing, 400030, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhaoli Zhang, Nursing Department, Chongqing University Cancer Hospital, No. 181 Hanyu Road, Shapingba District, Chongqing, People’s Republic of China, Tel +86-23-65079129, Email [email protected]
Purpose: Learned helplessness (LH) is the psychological state in which an individual experiences multiple failures and setbacks and experiences a sense of loss when facing the current situation. It is a significant burden for lung cancer patients that can impair quality of life and lead to physical, social, and psychological difficulties. Thus, this study aimed to determine the level of LH among patients with lung cancer and identify factors associated with LH.
Patients and Methods: From August 2022 to March 2023, 237 patients with lung cancer from Chongqing University Cancer Hospital were selected for this study. A general information questionnaire, the LH scale, the Brief Illness Perception questionnaire, the Strategies Used by People to Promote Health questionnaire, the Medical Coping Modes questionnaire, and the Self-esteem scale were used for the investigation. Multiple linear regression was employed to identify influencing factors for LH in patients with lung cancer.
Results: The total LH score of patients with lung cancer was 52.19± 11.20. Multiple linear regression analysis showed that illness perception (β=0.249, P=0.001), self-efficacy (β=− 0.194, P=0.017), and resignation coping mode (β=0.267, P< 0.001) were the main influencing factors of LH (P< 0.05), which explained 42.0% of the total variance.
Conclusion: The score of LH in patients with lung cancer was at a moderate level in this study. Illness perception, self-efficacy, and resignation coping mode have been found to impact LH among patients with lung cancer. Healthcare professionals should implement effective interventions, such as promoting self-efficacy, encouraging positive coping, and reducing illness perception, to alleviate LH.
Keywords: lung cancer, learned helplessness, risk factors, psychology
Introduction
In 2020, there were 2.2 million new lung cancer cases and 1.8 million deaths worldwide, of which the incidence rate is 11.4% and the mortality rate is 18%. The 2020 China Cancer Report’s most recent statistics show that China has 820,000 new lung cancer cases and 710,000 lung cancer deaths.1,2 Lung cancer is the primary cause of cancer-related death worldwide, and the 5-year survival rate is only 19.7% in China. Patients with lung cancer experience significant physical symptom burden, social challenges, fear of death, psychological distress, and so on.3
Learned helplessness(LH) originated from Seligman’s research on animal behavior and further demonstrated the existence of this phenomenon through dog experiments, referring to the psychological state in which an individual experiences multiple failures and setbacks and experiences a sense of loss when facing the current situation.4 LH theory suggests that when people face unpredictable and uncontrollable negative events, they constantly feel powerless, lose confidence, and fall into a state of helplessness.5,6 A reformulation of LH theory in terms of attribution theory has thought that individuals with LH attribute their failures to a personal, pervasive, and persistent lack of abilities and their successes to luck.7 Existing research explored LH in patients with stroke, systemic lupus erythematosus, inflammatory polyarthritis, chronic lower back pain, and maintenance hemodialysis. Studies showed that LH is a common psychological phenomenon experienced by most individuals with chronic diseases.8–11
Patients with lung cancer are subject to LH due to the physical symptoms, intensive treatments, and poor prognoses that accompany the condition. LH not only affects the patient’s compliance with treatment but may also cause serious psychological disorders. A study revealed that individuals who experienced intense feelings of anxiety, helplessness, and despair had a diminished sense of life satisfaction and a poorer quality of life.12 LH is associated with depression, suicidal ideation, and personal behavior in patients, whereby timely identification and intervention of their LH may be effective in preventing or delaying more serious outcomes.13 Some studies explored that risk factors for LH with chronic patients were age, educational level, income, pain, uncertainty in illness, and so on.8,9 There are no reports regarding the level and risk factors for LH in patients with lung cancer.
Therefore, this study aimed to identify the level and risk factors for LH in patients with lung cancer and provide the basis for effective intervention for improving LH in lung cancer patients.
Material and Methods
Participants
Using a convenience sampling method, patients with lung cancer hospitalized at Chongqing University Cancer Hospital between August 2022 to March 2023 were chosen as the study population. Inclusion criteria: (1) meet lung cancer diagnostic criteria (including small cell lung cancer and non-small cell lung cancer); (2) ≥ 18 years old; (3) clarify one’s condition and cancer diagnosis; (4) have clear consciousness and ability; and (5) informed consent is required to participate in this study. Exclusion criteria: (1) previous or current mental illness and disorders of consciousness; (2) complicated with other serious life-threatening diseases; (3) having other extrapulmonary metastatic cancers. This study was conducted strictly with national laws and the Declaration of Helsinki. All study participants provided informed consent. Ethical approval was obtained from the Institutional Review Board at the hospital where the study was performed (CZLS2022022-A).
Measurements
General Information Survey Questionnaire
A self-compiled general information questionnaire obtained demographic information and disease information, including age, gender, marital status, education level, annual income, occupation, residence, genetic history, course of disease, pathological type, pathological stage, tumor metastasis, and so on.
Learned Helplessness Scale (LHS)
LHS was developed by Chinese scholar Wu Xiao-Yan and comprises two dimensions: helplessness (13 items) and hopelessness (5 items), for a total of 18 items. Using the Likert 5-level scoring method for evaluation, each item is scored 1–5 points, from “completely non-compliant” to “completely compliant”, for a total score of 18–90 points. The higher the score, the more severe the sense of LH. The split-half reliability of 0.901 and the retest reliability of 0.898.14 In this study, Cronbach’s α coefficient was 0.891, indicating good reliability.
Strategies Used by People to Promote Health Questionnaire (SUPPH)
Lev and Owen developed SUPPH, which Qian Hui-juan translated into Chinese version.15 This scale is used to assess self-efficacy. With a total of 28 items, this scale has three dimensions: self-decompression, self-decision-making, and positive attitude. A 5-level rating system is employed, with 1 point denoting no confidence and 5 points denoting very confidence. The total score is 28–140 points, and the amount of self-efficacy increases as the overall score rises. In this study, Cronbach’s α coefficient was 0.990.
Brief Illness Perception Questionnaire (BIPQ)
BIPQ was developed by Broadbent et al and includes 9 items.16 Except for the cause of disease, each item adopts a 0–10 level scoring method (with reverse scoring for items 3, 4, and 7), with a total score of 0–80 points. The higher the score, the more severe the patient’s disease perception. The Chinese version of BIPQ has good psychological measurement characteristics. In this study, Cronbach’s α coefficient was 0.817.
Medical Coping Modes Questionnaire (MCMQ)
The MCMQ was developed by Feifel et al and Shen Xiao-hong et al translated it into Chinese. This scale includes subscales for three coping modes: “confrontation”, “avoidance”, and “resignation”. Among them, “confrontation” consists of 8 items, avoidance “consists of 7 items”, and “resignation” consists of 5 items. Each item is scored on a scale of 1–4, with 12 items being scored positively and 8 items being scored backward. The scoring range of the three subscales is 8–32 points, 7–28 points, and 5–20 points, respectively. The higher the score on the subscale, the more the patient uses this coping mode.17,18 In this study, the Cronbach’s α coefficient for the three dimensions in this study were 0.732, 0.745, and 0.762, respectively.
Rosenberg Self-Esteem Scale (RSES)
RSES is used to assess self-esteem, which was developed by Rosenberg and Ji Yi-fu et al translated it into Chinese, It consists of 10 questions that must be answered on a scale of 1 to 4, with 1 being strongly agree and 4 being strongly disagree.19 Questions 1, 2, 4, 6, and 7 belong to positive statement questions; Questions 3, 5, 8, 9, and 10 are reverse statement questions and are graded at four levels, with a total score range of 10–40. Overall, a high score indicates more self-esteem. In this study, Cronbach’s α coefficient was 0.875.
Information Collection
This study adopts a questionnaire survey method, with oncology nurses who have received unified training responsible for data collection. On the day of admission, explain the purpose and methods of this study to patients who meet the standards, following the principles of voluntary and informed consent. Before filling in the form, the researchers will use unified guidance language to explain. Fill it out anonymously and promise to keep the information provided by the patient strictly confidential. After completing the form, the researcher will verify it on the spot. If there are any omissions, the patient is requested to promptly supplement and complete them.
Data Analysis
Data were analyzed using SPSS Statistics Version 26.0®. Counting data is described as cases, while measurement data is described as mean ± standard deviation. Univariate analysis was conducted using independent sample t-tests and one-way ANOVA tests. Pearson correlation analysis was used to explore the relationship between LH score and SUPPH score, BIPQ score, MCMQ score, and RSES score. Using multiple linear regression equations to analyze the influencing factors of LH, using a bilateral test, with P<0.05 indicating a statistically significant difference.
Results
General Data Description of Patients with LH
In this study, 244 patients were initially enrolled; 7 of those cases were later removed due to missing fundamental data, leaving 237 patients for the final data analysis. The results showed statistically significant differences (P<0.05) by residence, employment status, and tumor metastases, as shown in Table 1.
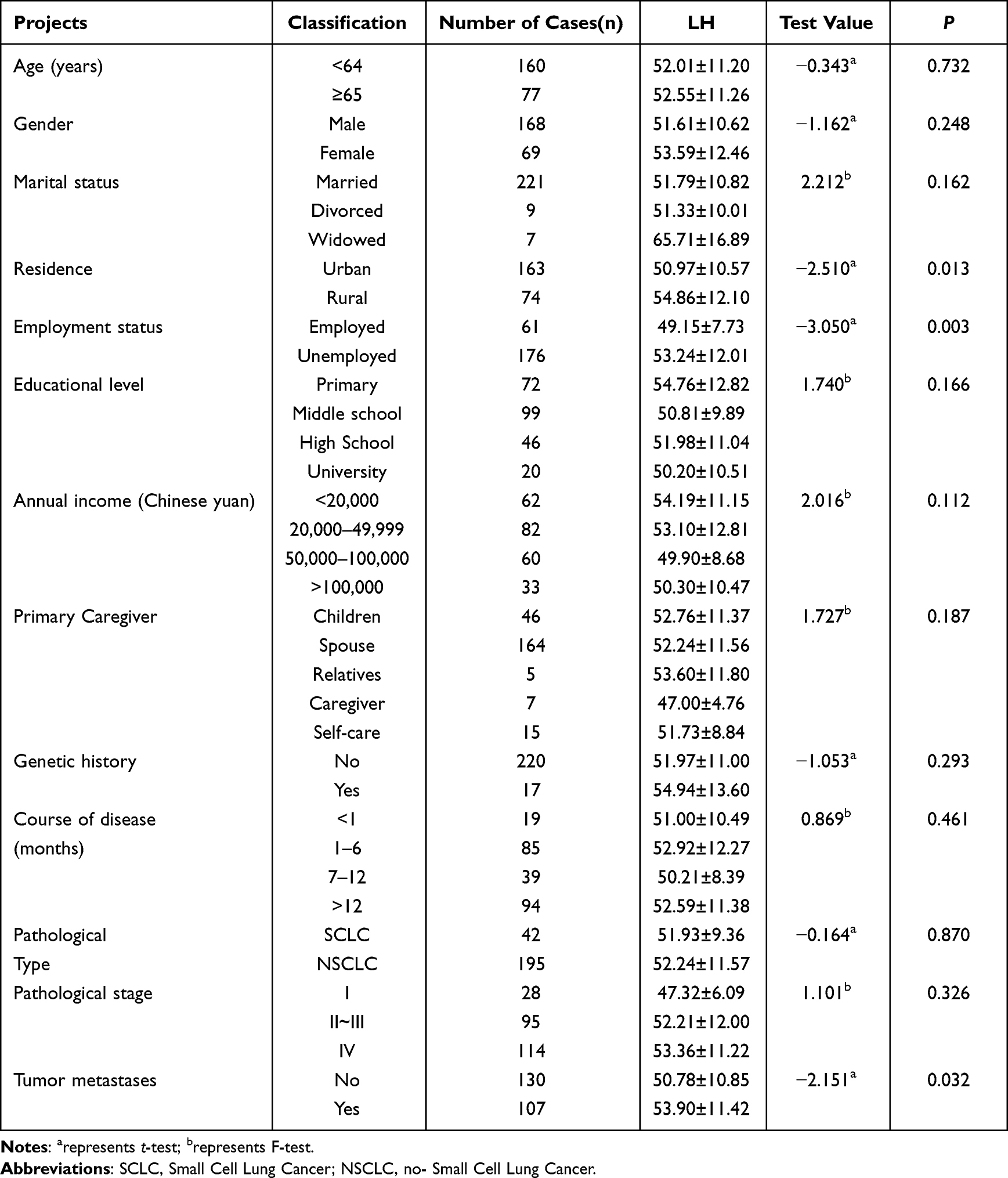 |
Table 1 Description of General Data of Patients with Lung Cancer (N=237) |
LH, BIPQ, SUPPH, MCMQ, and RSES Scores of Patients with Lung Cancer
The results of the study showed that the LH score of patients with lung cancer is 52.19±11.20, with 12.49±2.82 for hopelessness and 39.69±8.95 for helplessness. BIPQ, SUPPH, MCMQ, and RSES scores are shown in Table 2.
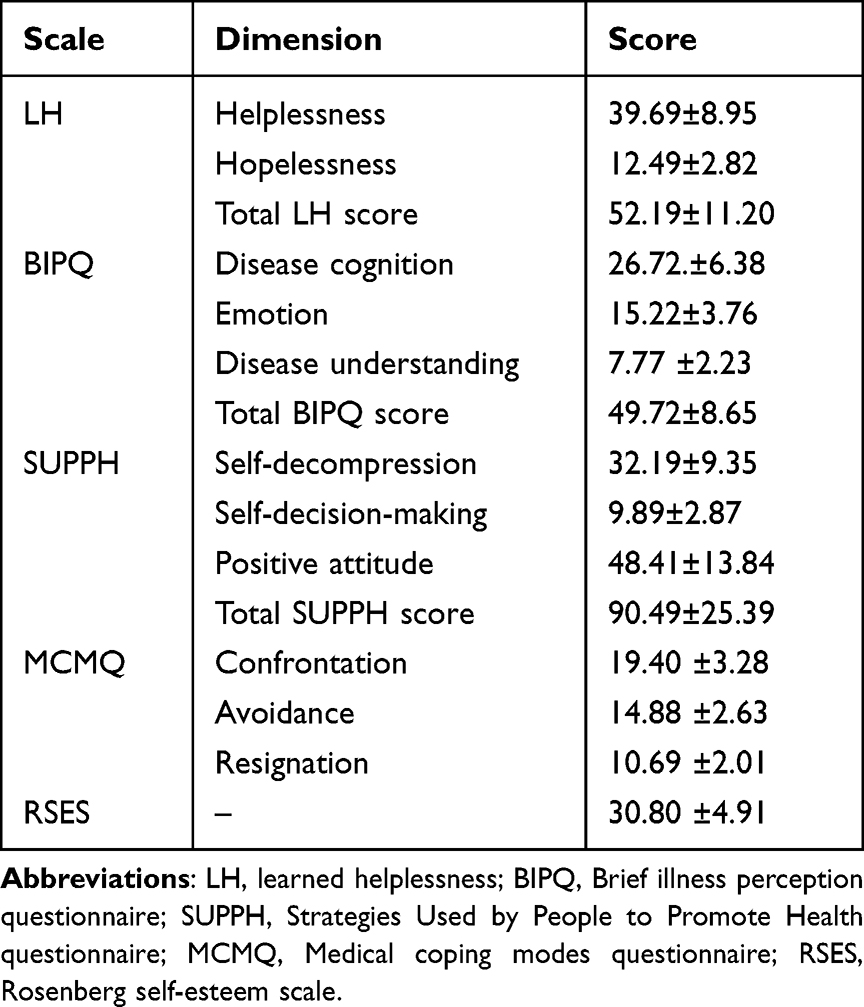 |
Table 2 Scores on Each Scale (N=237) |
Correlation Analysis of LH with the BIPQ and SUPPH and MCMQ and RSES
Pearson correlation analysis showed that LH is negatively correlated with the SUPPH and RSES. LH is positively correlated with BIPQ, avoidance coping mode, and resignation coping mode, with statistically significant differences (P<0.05), as shown in Table 3.
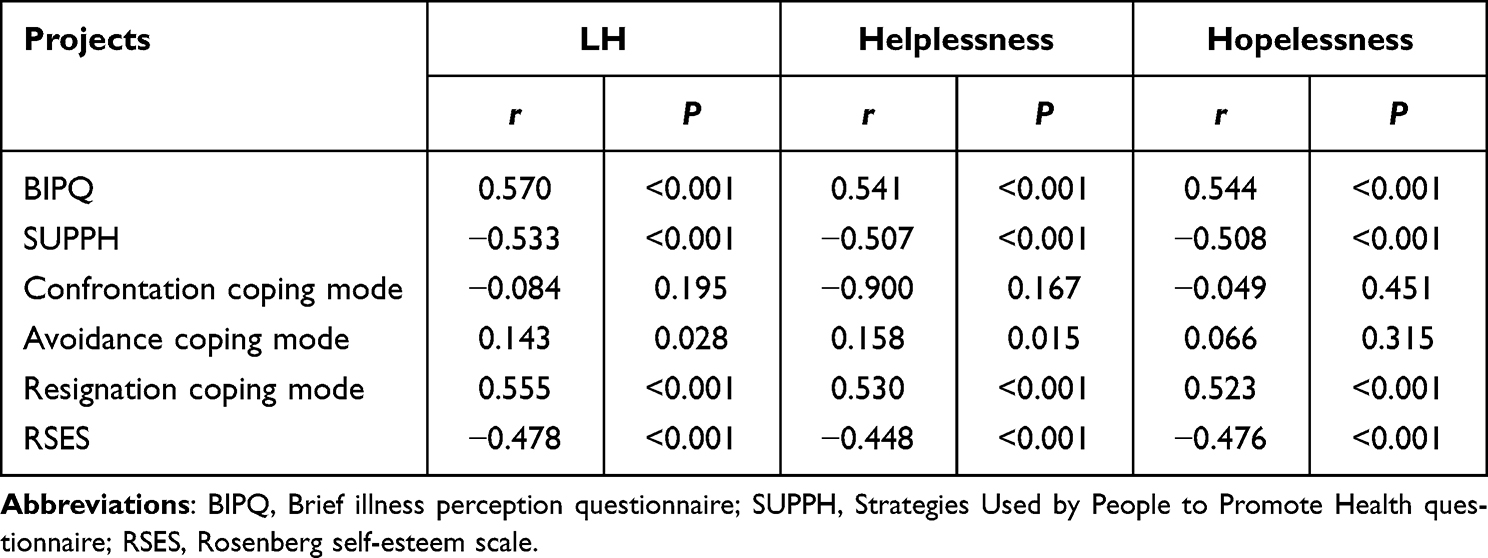 |
Table 3 Correlation of LH with BIPQ and SUPPH and MCMQ and RSES (N=237) |
Multiple Linear Regression Analysis of the Factors Influencing LH
LH score for lung cancer patients was used as the dependent variable, and statistically significant data (employment status, residence, and tumor metastases), BIPQ score, SUPPH score, RSES score, avoidance coping mode score, and resignation coping mode score were used as independent variables in a multiple linear regression analysis. The linear regression results showed that the BIPQ score (β=0.249, P=0.001), SUPPH score (β=−0.194, P=0.017), and resignation coping mode score (β=0.267, P<0.001) were independent influences on the level of LH. The model was well fitted (R2 = 0.420), meaning that the variables together explained 42.0% of the total variation in LH in patients with lung cancer, as shown in Table 4.
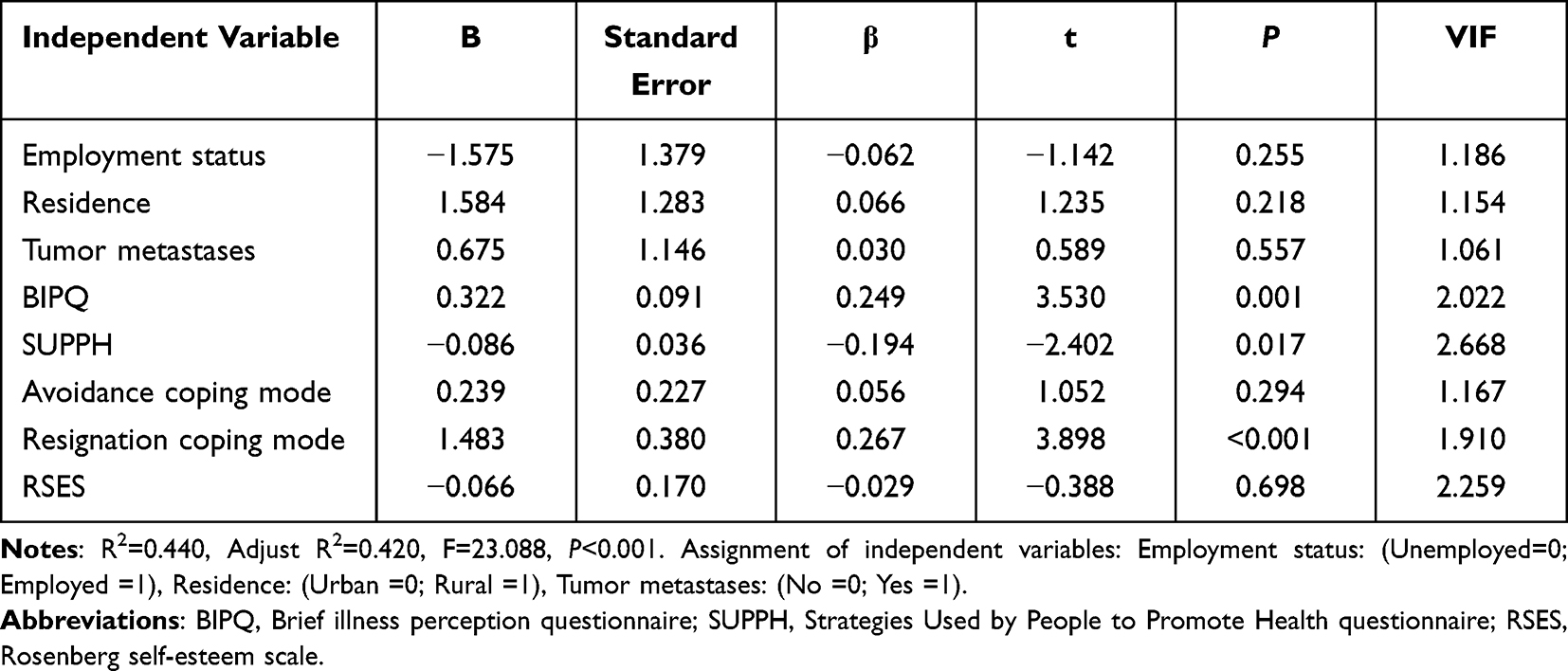 |
Table 4 Multiple Linear Regression Analysis of Factors Influencing LH (N=237) |
Discussion
Status of LH in Patients with Lung Cancer
The present study assessed the LH of patients with lung cancer and subsequently explored the influence factors of LH. In the study, the LH score of patients with lung cancer was (52.19±11.20), which was at a moderate level. There are no studies on LH among patients with lung cancer. At present, the research population of LH is mostly concentrated in students, maintenance hemodialysis patients, and stroke patient.20,21 The assessment scales used are different, thus, the results of the studies are not comparable. Patients with lung cancer will inevitably experience various failures and setbacks in the course of disease, diagnosis, and treatment, which may result in negative cognition that their behavior cannot control the disease progress and improve the therapeutic effect, resulting in LH.22,23
Factors Influencing LH in Patients with Lung Cancer
Illness perception is the cognitive response of patients to diseases when their health is threatened, which can affect their emotional and behavioral responses.24 Illness perception was identified as a factor influencing LH in patients with lung cancer in this study, which showed that the higher the level of BIPQ score, the higher the level of LH in patients with lung cancer (β=0.249, P=0.001). High levels of illness perception can exacerbate negative emotions and reduce patients’ confidence in coping with stressful events. The higher the level of illness perception in patients with lung cancer, the more negative emotions such as stigma and negative experience are generated, and the heavier the psychological pressure burden and the higher-level LH.25 Additionally, due to the subtlety and lack of specificity of the early clinical manifestations of lung cancer, most patients are already in the middle to late stages of diagnosis. The 5-year survival rate of lung cancer in China has been only 19.7% in the past 20 years, low survival rates greatly reduce patients’ psychological endurance and often cause them to fear disease progression, which in turn leads to LH.26,27 In the clinical nursing process, healthcare professionals should emphasis evaluating patients’ illness perception. By implementing group health education, and psychological counseling, and using cognitive behavioral interventions guide patients to correctly understand their own disease conditions to help patients improve their disease perception, positive cognition should be strengthened, and emotional distress should be alleviated.
Self-efficacy refers to a person’s belief in their ability to successfully complete specific tasks or behaviors related to their own health in a variety of situations.28 Studies have indicated that individuals with a strong sense of self-efficacy are more confident when facing adversity and fighting their disease.29 In this study, self-efficacy was negatively correlated with the level of LH in lung cancer patients (β=−0.194, P=0.017). This finding aligns with the results of Lyu’s research, which suggested that high self-efficacy predicts more positive emotional performance in cancer patients.30 Self-efficacy is the core of self-management of cancer patients, and patients with high self-efficacy can increase their ability to self-manage their diseases, reduce risk events and unpleasant responses associated with treatment, boost recovery, and contribute to their psychological well-being.31 Therefore, healthcare professionals should assess the patient’s awareness of diseases, and improve their self-efficacy through health education and encouraging patient participation in decision-making, in order to mobilize potential coping and abilities to solve problem, thereby improving the patient’s psychological condition and reducing LH.
Coping modes are the methods and means that individuals use to cope with specific stressful situations and associated emotional distress, including negative coping modes and positive coping modes.32 A proper coping mode can reduce psychological stress and maintain mental health. Resignation coping mode was identified as a factor influencing LH in lung cancer patients in this study. The results indicated that lung cancer patients with higher levels of LH were more inclined to adopt a resignation coping mode which is a negative coping mode (β=0.267, P<0.001). Considered to be related to the patient’s fear of disease progression and a negative attitude towards the disease, leading to a decrease in confidence in the treatment of the disease and an increase in the level of LH.33 Consistent with the findings of the present study, Shimizu et al found that a negative coping mode was correlated with significant depression.34 The level of LH was higher when patients adopted resignation coping mode. Resignation is a negative coping mode for patients with lung cancer. When patients yield to the disease, their compliance behavior declines, resulting in adverse outcomes and ultimately leading to LH. Therefore, healthcare professionals should pay attention to the moderating role of coping styles, provide psychological counseling and health education to patients in time, and guide patients to adopt positive coping mode, avoid resignation coping mode, and reduce the LH of patients.
Limitations
The limitations of this study are the small sample size and its cross-sectional nature. The present study was performed only on lung cancer patients residing in our hospital, and it was not performed on patients at other hospitals. Future studies should increase the sample size and conduct multi-center cross-sectional investigations and longitudinal studies.
Conclusion
The research results showed that LH among lung cancer patients is at a moderate level. The independent influencing factors of LH include illness perception, self-efficacy, and resignation coping mode. Therefore, healthcare professionals should offer formulating intervention strategies based on these influencing factors, such as promoting self-efficacy, encouraging positive coping, and reducing illness perception, to prevent the occurrence and development of LH.
Acknowledgments
This research was sponsored by the Natural Science Foundation of Chongqing, China (cstc2021jcyj-msxmX1094). The authors express their gratitude to all contributors for their diligent work on this study and all participants who voluntarily participated in the research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Siegel RL, Miller KD, Fuchs HE, Cancer Statistics JA 2021. Ca a Cancer J Clinicians. 2021;71(1):7–33. doi:10.3322/caac.21654
2. Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015. Ca a Cancer J Clinicians. 2016;66(2):115–132. doi:10.3322/caac.21338
3. Osborne J, Kerr H. Role of the clinical nurse specialist as a non-medical prescriber in managing the palliative care needs of individuals with advanced lung cancer. Int j Palli Nur. 2021;27(4):205–212. doi:10.12968/ijpn.2021.27.4.205
4. Overmier JB, Seligman ME. Effects of inescapable shock upon subsequent escape and avoidance responding. J Comp Physiol Psychol. 1967;63(1):28–33. doi:10.1037/h0024166
5. Maier SF, Seligman ME. Learned helplessness at fifty: insights from neuroscience. Psychol Rev. 2016;123(4):349–367. doi:10.1037/rev0000033
6. Pryce CR, Azzinnari D, Spinelli S, Seifritz E, Tegethoff M, Helplessness MG. A systematic translational review of theory and evidence for its relevance to understanding and treating depression. Pharmacol Ther. 2011;132(3):242–267. doi:10.1016/j.pharmthera.2011.06.006
7. Abramson LY, Seligman ME, Teasdale JD. Learned helplessness in humans: critique and reformulation. J Abnorm Psychol. 1978;87(1):49–74. doi:10.1037/0021-843X.87.1.49
8. Xie C, Li L, Li Y. Trajectories of learned helplessness in maintenance haemodialysis patients and their predictive effects on self-management: a latent growth mixture modeling approach. Psychol Res Behav Manag. 2023;16:351–361. doi:10.2147/PRBM.S401380
9. Moyano S, Scolnik M, Vergara F, et al. Evaluation of learned helplessness, perceived self-efficacy, and functional capacity in patients with fibromyalgia and rheumatoid arthritis. J Clin Rheumatol. 2019;25(2):65–68. doi:10.1097/RHU.0000000000000769
10. Thumboo J, Strand V. Health-related quality of life in patients with systemic lupus erythematosus: an update. Annals Acad Med. 2007;36(2):115–122. doi:10.47102/annals-acadmedsg.V36N2p115
11. Chapman SL, Brena SF. Learned helplessness and responses to nerve blocks in chronic low back pain patients. Pain. 1982;14(4):355–364. doi:10.1016/0304-3959(82)90144-0
12. Polański J, Chabowski M, Świątoniowska-Lonc N, Jankowska-Polańska B, Mazur G. Can life satisfaction be considered a predictor of quality of life in patients with lung cancer? Eur Rev Med Pharmacol Sci. 2020;24(21):11128–11138. doi:10.26355/eurrev_202011_23600
13. Xie C, Li L, Li Y. Learned helplessness in renal dialysis patients: concept analysis with an evolutionary approach. Patient Prefer Adherence. 2022;16:2301–2312. doi:10.2147/PPA.S373134
14. Wu XY, Zeng H, Ma SH, et al. Development of learned helplessness scale and its relationship with personality. Journal of Sun Yat-sen University. 2009;30(3):357–360 doi:10.3321/j.issn:1672-3554.2009.03.026
15. Lev EL, Owen SV. A measure of self-care self-efficacy. Res Nurs Health. 1996;19(5):421–429. doi:10.1002/(SICI)1098-240X(199610)19:5<421:AID-NUR6>3.0.CO;2-S
16. Broadbent E, Wilkes C, Koschwanez H, Weinman J, Norton S, Petrie KJ. A systematic review and meta-analysis of the brief illness perception questionnaire. Psychol Health. 2015;30(11):1361–1385. doi:10.1080/08870446.2015.1070851
17. Feifel H, Strack S, Nagy VT, et al. Coping strategies and associated features of medically ill patients. Psychosom Med. 1987;49(6):616–625. doi:10.1097/00006842-198711000-00007
18. Sun H, Zhang J, Fu X. Psychological status, coping, and social support of people living with HIV/AIDS in central China. Public Health Nur. 2007;24(2):132–140. doi:10.1111/j.1525-1446.2007.00617.x
19. Rosenberg M. Society and the Adolescent Self-Image. Social Forces. 1965;44 2 :255 doi:10.2307/2575639
20. Xie C, Li L, Zhou L, Sun C, Zhang Y, Li Y. Mediating role of learned helplessness’ components in the association between health literacy/social support and self-management among maintenance haemodialysis patients in Changsha, China: a cross-sectional study. BMJ Open. 2023;13(8):e068601. doi:10.1136/bmjopen-2022-068601
21. Raufelder D, Kulakow S. The role of social belonging and exclusion at school and the teacher-student relationship for the development of learned helplessness in adolescents. Br J Educ Psychol. 2022;92(1):59–81. doi:10.1111/bjep.12438
22. Trindade IA, Mendes AL, Ferreira NB. The moderating effect of psychological flexibility on the link between learned helplessness and depression symptomatology: a preliminary study. J Con Behav Sci. 2020;15:68–72. doi:10.1016/j.jcbs.2019.12.001
23. Conwill J. Understanding and combating helplessness. Rehabil Nurs. 1993;18(6):388–394. doi:10.1002/j.2048-7940.1993.tb00795.x
24. Richardson EM, Schüz N, Sanderson K, Scott JL, Schüz B. Illness representations, coping, and illness outcomes in people with cancer: a systematic review and meta-analysis. Psychooncology. 2017;26(6):724–737. doi:10.1002/pon.4213
25. Ośmiałowska E, Staś J, Chabowski M, Illness Perception J-PB. Quality of Life in Patients with breast cancer. Cancers. 2022;14(5):1214. doi:10.3390/cancers14051214
26. Zeng H, Chen W, Zheng R, et al. Changing cancer survival in China during 2003–15: a pooled analysis of 17 population-based cancer registries. Lancet Glob Health. 2018;6(5):e555–e567. doi:10.1016/S2214-109X(18)30127-X
27. Hopman P, Rijken M. Illness perceptions of cancer patients: relationships with illness characteristics and coping. Psycho‐Oncology. 2015;24(1):11–18. doi:10.1002/pon.3591
28. Foster C, Brown J, Killen M, The BS. NCRI cancer experiences collaborative: defining self management. Eur J Oncol Nurs. 2007;11(4):295–297. doi:10.1016/j.ejon.2007.08.002
29. Somasundaram RO, Devamani KA. Study on resilience, perceived social support and hopelessness among cancer patients treated with curative and palliative care. Indian J Palliat Care. 2016;22(2):135–140. doi:10.4103/0973-1075.179606
30. Lyu MM, Chiew-Jiat RS, Cheng KKF. The effects of physical symptoms, self-efficacy and social constraints on fear of cancer recurrence in breast cancer survivorsExamining the mediating role of illness representations. Psychooncology. 2023. doi:10.1002/pon.6264
31. He J, Xia J. Effect of a wechat-based perioperative nursing intervention on risk events and self-management efficacy in patients with thyroid cancer. Am J Transl Res. 2021;13(7):8270–8277.
32. Chen S, Mei R, Tan C, Li X, Zhong C, Ye M. Psychological resilience and related influencing factors in postoperative non-small cell lung cancer patients: a cross-sectional study. Psychooncology. 2020;29(11):1815–1822. doi:10.1002/pon.5485
33. Chabowski M, Jankowska-Polańska B, Lomper K, Janczak D. The effect of coping strategy on quality of life in patients with NSCLC. Cancer Manag Res. 2018;10:4085–4093. doi:10.2147/CMAR.S175210
34. Shimizu K, Nakaya N, Saito-Nakaya K, et al. Personality traits and coping styles explain anxiety in lung cancer patients to a greater extent than other factors. Jap j Clinical Oncol. 2015;45(5):456–463. doi:10.1093/jjco/hyv024
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.