")
Back to Journals » Journal of Healthcare Leadership » Volume 15
Leadership Development Strategies in Interprofessional Healthcare Collaboration: A Rapid Review
Received 26 January 2023
Accepted for publication 19 July 2023
Published 23 August 2023 Volume 2023:15 Pages 175—192
DOI https://doi.org/10.2147/JHL.S405983
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Russell Taichman
Juan Bornman,1 Brenda Louw1,2
1Centre for Augmentative and Alternative Communication, University of Pretoria, Pretoria, Gauteng, South Africa; 2Department Audiology and Speech-Language Pathology, East Tennessee State University, Johnson City, TN, USA
Correspondence: Juan Bornman, Email [email protected]
Background: Contemporary healthcare practitioners require leadership skills for a variety of professional roles related to improved patient/client outcomes, heightened personal and professional development, as well as strengthened interprofessional collaboration and teamwork.
Objective/Aim: The aim of this study is to systematically catalogue literature on leadership in healthcare practice and education to highlight the leadership characteristics and skills required by healthcare practitioners for collaborative interprofessional service delivery and the leadership development strategies found to be effective.
Methods/Design: A rapid review was conducted. The Preferred Reporting Items for Systematic Reviews and Meta Analyses (PRISMA) diagram shows that the 11 databases, yielded 465 records. A total of 147 records were removed during the initial screening phase. The remaining 318 records were uploaded onto Rayyan, an online collaborative review platform. Following abstract level screening, a further 236 records were removed with 82 records meeting the eligibility criteria at full text level, of which 42 were included in the data extraction. The Mixed Methods Appraisal Tool (MMAT) was used for quality appraisal.
Results: Results showed variability in methodologies used, representing various healthcare disciplines with a range in population size (n = 6 to n = 537). Almost half of the results reported on new programs, with interprofessional collaboration and teamwork being the most frequently mentioned strategies. The training content, strategies used as well as the length of training varied. There were five outcomes which showed positive change, namely skills, knowledge, confidence, attitudes, and satisfaction.
Conclusion: This rapid review provided an evidence-base, highlighted by qualitative, quantitative, and mixed methods research, which presents distinct opportunities for curriculum development by focusing on both content and the methods needed for leadership programs. Anchoring this evidence-base within a systematic search of the extant literature provides increased precision for curriculum development.
Keywords: collaboration, healthcare practitioners, interprofessional healthcare, leadership development, strategies
Introduction
Changes in healthcare worldwide have led to an emphasis on leadership development in healthcare professions, which include medical, dental, public health, nursing, and allied health providers (eg, audiology, nutrition, occupational therapy, physical therapy, pharmacy, respiratory therapy, radiography, speech-language therapy) to meet current healthcare needs.1–3 These changes have been brought about by factors, such as advances in information technology, automation, human interconnectivity, cross-sector mergers, advances in precision medicine, community involvement, providing services during periods of financial instability, and more recently the global COVID-19 pandemic.1,4,5
As a result, effective leadership is now needed at all levels of healthcare for safety assurance, to drive service development, to ensure good clinical outcomes,6 to foster engagement of healthcare practitioners (HCP),2 to advocate for their patients/clients, to be self-aware and prioritize personal and professional development, to become innovative thinkers and to practice ethically.7,8
Importantly, leadership skills enhance HCPs willingness to participate in team care and facilitates the long-term sustainability of team care.5 Internationally, clinical leadership has been emphasized to ensure quality of care, job satisfaction and retention of HCP.9
Global changes in healthcare necessitated new strategies and ways of working in HCP. Currently, there is widespread international recognition that bridging the boundaries of professional disciplines is required to address the challenges posed by changes in healthcare,1,10 validating the World Health Organization’s11 call to meet the complex service needs of the future through interprofessional collaboration (IPC).
In the IPC approach, members work collaboratively to complete an activity collectively.12 IPC is defined by a diversity of skills, roles, and perspectives, bringing practitioners who have divergent expertise together with the purpose of combining their skills and insights to realize a shared goal that could not otherwise be achieved through the reliance on a single skill set of one disciplinary group. Leadership is essential for interprofessional collaboration.13 A scoping review14 (n = 114) examined how leadership is referred to and used in IPC and found that most papers did not refer to a specific leadership approach, nor did they identify, define, describe, or theorize leadership capabilities. A more critical examination of interprofessional leadership and the capabilities required to lead the necessary changes in both education and practice settings is needed.
As leadership is now valued by HCP at all levels, new models of leadership have emerged as important contributions to HCPs who work collaboratively, including, but not limited to collaborative leadership,3,13 transformational leadership,15,16 systemic leadership,17 ethical leadership,18,19 and recently remote leadership.20 Collaborative leadership models feature largely in Interprofessional Education (IPE)13 and includes shared and team leadership with an emphasis on a common vision. As such, shared leadership involves the distribution of leadership influence in the team across multiple team members. Shared leadership has been shown to enhance processes, effectiveness, and performances in interprofessional teams21 while increasing HCP satisfaction and reducing burnout.22 Similarly, in team leadership different professions share influence and there is a thoughtful allocation of responsibilities. Central control is shifted from a leader to the team. Team members are independent and coordinate their activities to reach the shared team goal.3
Transformational leadership is a contemporary form of leadership, and the underlying tenets are to inspire individuals and to form teams to inspire goals through idealized influence, inspirational motivation, individualized consideration, and intellectual stimulation.3 Transformational leadership is important to retaining HCP and to achieve overall patient satisfaction.16
Leadership beliefs of clinicians and how it differs between professions has been explored in the research.5 The link found between group identification and leadership beliefs, suggests that strategies which promote strong identification in both professional and interprofessional teams are likely to be conducive to clinicians supporting principles of shared leadership. HCPs benefit from developing not only leadership skills and characteristics, but also followership skills as leaders and followers co-produce the leadership that is needed in teamwork.23 A pervasive leadership myth is that leadership is lodged in positional power in a specific organization. This type of thinking is false and flawed. HCPs at many levels and with many different roles daily display leadership, eg, leading an item on a case discussion, or leading a discussion with family members or with students.19 This points to the requirement of HCPs to be adaptable and able to switch effortlessly between leadership and followership roles as it is beneficial to advance patient care.
HCPs are highly qualified and skilled professionals who work in range of health care settings. HCP providers require knowledge, clinical skills and competency, efficiency and productivity, and positive relationships with clients/patients.24 In addition, HCPs require leadership skills to ensure the quality of care, to improve patient/client outcomes, to advocate for their patients/clients, to be self-aware and prioritize personal and professional development, to become innovative thinkers and to practice ethically.7,25,26 Importantly, leadership skills enhance HCPs willingness to participate in team care and facilitates the long-term sustainability of team care, which relies on shared leadership.5 However, the skills needed to be an effective HCP are different to those required to be an effective leader.27 Training in HCP prepares individuals for leadership in a multitude of ways, for example, by taking care of patients, interacting with interdisciplinary team members, guiding groups, writing grant proposals with colleagues and emulating mentors or professors.28 It is commonly acknowledged that although formal training in the multifaceted components of leadership has become accepted as highly desirable for healthcare leaders,29 clinical HCPs have generally not been prepared for their expected role as effective health care leaders.9,27 Furthermore, there are also gaps in leadership development practices in higher education settings of HCP.1,30
Leadership development in HCP is an emerging research field and has been studied in various contexts by using a variety of methodologies, such as bibliometric analysis,31 survey research,5 qualitative research,10,30 systematic reviews,6 scoping reviews,32 rapid reviews17 and theoretical papers.3,33 However, despite the broad diversity of the research there are limitations and a lack of consensus regarding the theoretical and conceptual frameworks applied, leadership models promoted, competencies required, training approach and strategies used to leadership development of HCP.1,32 It was proposed that a universally applicable framework for leadership development in HCP will support leadership development programs aimed at multiple disciplines, both in professional training and in continuing education. Such a universal model can also lead to greater efficiency in developing new leadership development programs.1
A new type of leader is emerging in healthcare, namely one who focuses on teamwork, improving patient outcomes and models the balance between autonomy and accountability.3 Leadership development programs need to prepare and equip HCPs to fulfill this role expectation.
The aim of this study is to systematically catalogue literature on leadership in healthcare practice and education, in an unbiased manner, using a rapid review methodology by highlighting the leadership characteristics and skills required by HCPs for collaborative interprofessional service delivery and the leadership development strategies found to be effective.
Method
A rapid review was undertaken due to its potential for producing timely and relevant research.17,34 Rapid reviews are also attracting interest as a research method in the discipline of speech-language pathology (SLP). For example, Bolton et al35 conducted a rapid review on aerosol generating procedures, dysphagia assessment and COVID-19 in response to urgent clinical needs, while Malandraki and colleagues36 conducted a rapid systematized review of telehealth for dysphagia across the life span.
While there is no standardized procedure for conducting rapid reviews, several approaches have been suggested and used.37 This rapid review used systematic review methodology and follows the Preferred Reporting Items for Systematic Reviews and Meta Analyses (PRISMA) statement.38,39
Identifying the Research Question
To ensure that the rapid review included information relevant to the main aim, the review question was formulated in a PIO-format (Population-Intervention-Outcome): What are the leadership characteristics, skills, and strategies (Outcomes) required by HCPs (Population) in IPC and IPE (Intervention)?
Search Strategy and Study Selection
A systematic search of 11 relevant databases was conducted to capture a wide variety of potential papers that may be indexed across different databases.40 A librarian assisted in identifying the relevant databases and interfaces as well as in refining search terms. Search terms using keywords were generated through the PIO method that categorizes the population, intervention, and outcome to identify search terms (see Table 1). The keywords included Boolean operators AND and OR to link the population to the intervention and outcomes in the search as well as truncation. No hand searches were performed due to restrictions brought on by the global COVID-19 pandemic.
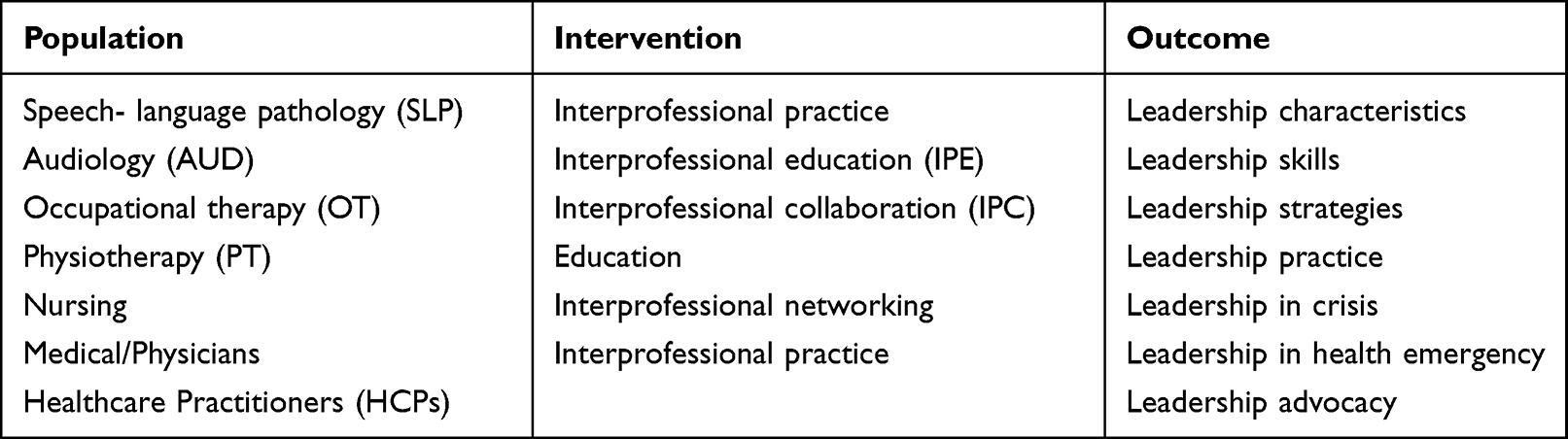 |
Table 1 PIO-Format |
The following four criteria were applied in the searches: (1) Only material published between January 2000 and December 2022; (2) any study design (ie, qualitative studies, quantitative studies or mixed-method research designs); (3) studies published in English; and (4) no grey literature (eg, reports, fact sheets, conference proceedings, chapters of academic textbooks, websites, newspapers and policy documents) as preliminary searches of the grey literature yielded limited information relevant to the pre-determined inclusion criteria of this review.41
The 11 databases yielded a total of 465 records when employing the search terms, namely PubMed (n = 86), EBSCO (n = 71), Academic Search Complete (n = 58), CINAHL (n = 58), Web of Science (n =56), Health Source – Nursing Academic Edition (n = 55), PsychInfo (n = 42), Scopus (n = 18), PsychArticles (n = 9), Taylor and Francis (n = 7) and AccessMedicine (n = 5). An independent librarian versed in systematic reviews reviewed the search strategy and recommended databases related to health sciences and based on the topic.42 Using multiple databases increased the depth of the search.
Initial Screening
As mentioned earlier, of the 465 records, a total of 95 duplicates were identified and removed (n = 370 remained). The 370 remaining records were uploaded onto Rayyan, an online platform where researchers can perform collaborative systematic reviews.43 The Rayyan platform was beneficial as it increased the objectivity of study selection and aided in improving the interrater agreement. The remaining 370 records were screened on title level of which 52 were excluded as the focus of these records was not on the topic of the current rapid review.
The remaining 318 abstracts were reviewed independently by two reviewers. The reviewers agreed on 291 abstracts, resulting in a 91.5% interrater agreement. The remaining 27 abstracts were discussed with two additional reviewers until 100% consensus was reached.38 Studies were excluded on abstract level due to the non-target population, non-target outcome, or non-target focus of the study. The same process was followed to determine eligibility on the full text level of the remaining 82 records using the a priori inclusion and exclusion criteria by two reviewers. The initial interrater agreement for this stage was also high (88.9%). Table 2 shows the inclusion- and exclusion criteria that was used for the screening and eligibility phases.
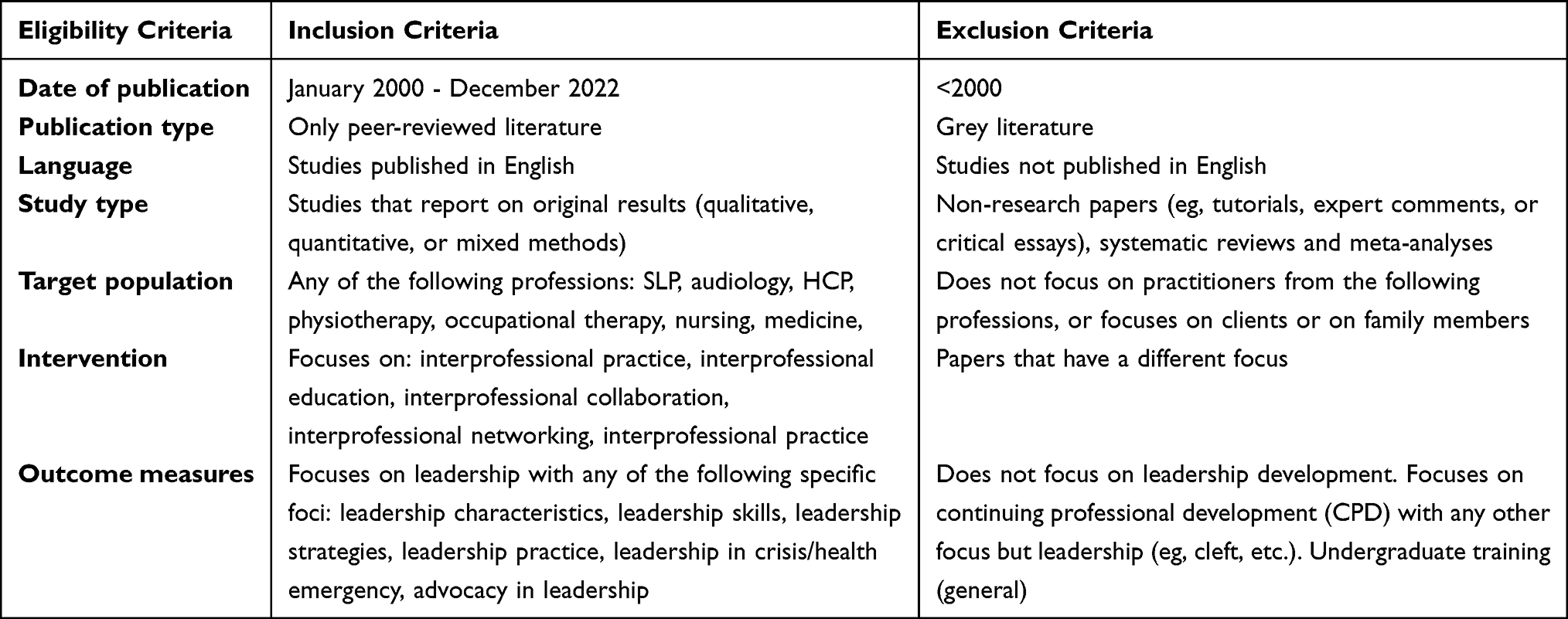 |
Table 2 Screening – Eligibility Criteria: Title and Abstract Level |
After the screening at abstract level, 318 records remained. The remaining 82 records were read at full text level and assessed for eligibility by two reviewers. The initial interrater agreement was 89.0% (reviewers agreed on 73 of the 82 records), which is regarded as a high agreement.44 Disagreements were discussed with two additional members of the research team until 100% consensus was reached for every study record. A total of 42 studies were selected for full-text inclusion, based on the criteria in Table 1.
The PRISMA diagram is shown in Figure 1.
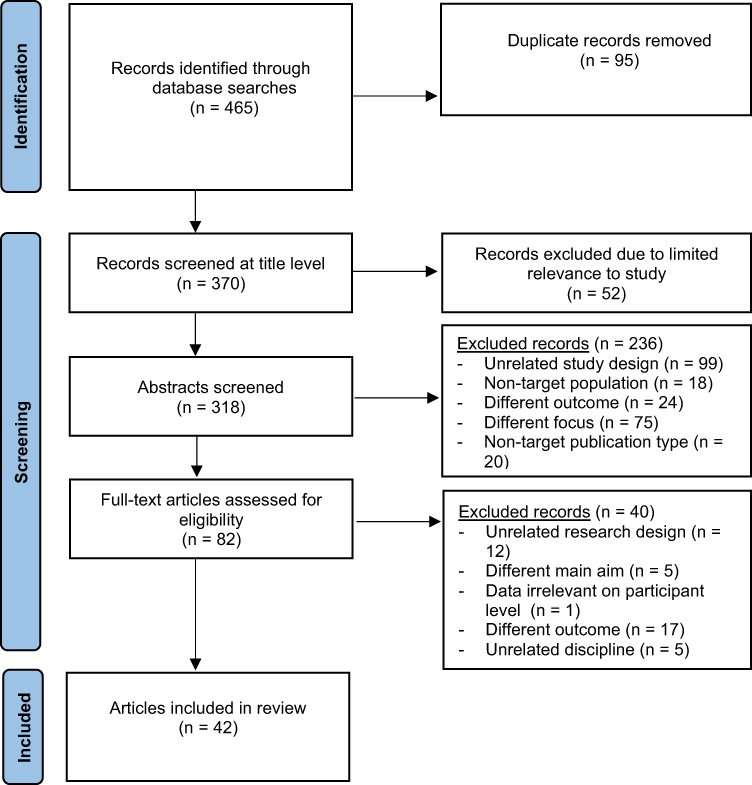 |
Figure 1 PRISMA diagram for scoping review process. Notes: Adapted from Moher D, Liberati A, Tetzlaff J, Altman, DG, and The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009;6(7):1–6. Creative Commons.39 |
Data Extraction and Analysis
A data extraction tool was developed to compile consistent and independent data reports. It included general information (ie, authors, year of publication and publication type), descriptive information (ie, the discipline involved, country of publication and design used), as well as information related to the specific population (ie, the specific discipline, the number of participants and their experience), the intervention (ie, whether a specific course/module on leadership is described and if so, the type of course) and the outcomes (ie, leadership characteristics, skills, etc.). All data were extracted independently by at least two reviewers. As was the case for the initial screening, disagreements were resolved through consensus meetings and upon full consensus, the extracted data were transferred from the data extraction tool to a synthesized Excel spreadsheet.
Critical Appraisal
Following the data extraction, the quality of the included studies was appraised using the MMAT45 to systematically check each article for biases. The MMAT firstly considers if there is a clear research question and if the collected data address the research questions before looking at specific questions depending on the study method. The MMAT overall quality score used descriptors such as numbers ranging from 1 (indicating 20% quality criteria) to 5 (indicating 100% quality criteria met). Two raters initially scored each of the 42 papers, but the interrater reliability was unacceptably low (64.3%). Hence, an additional two raters with more experience were added and the agreement level increased to 97.6%.46 The consensus MMAT scores for the 42 studies included are shown in Table 3.
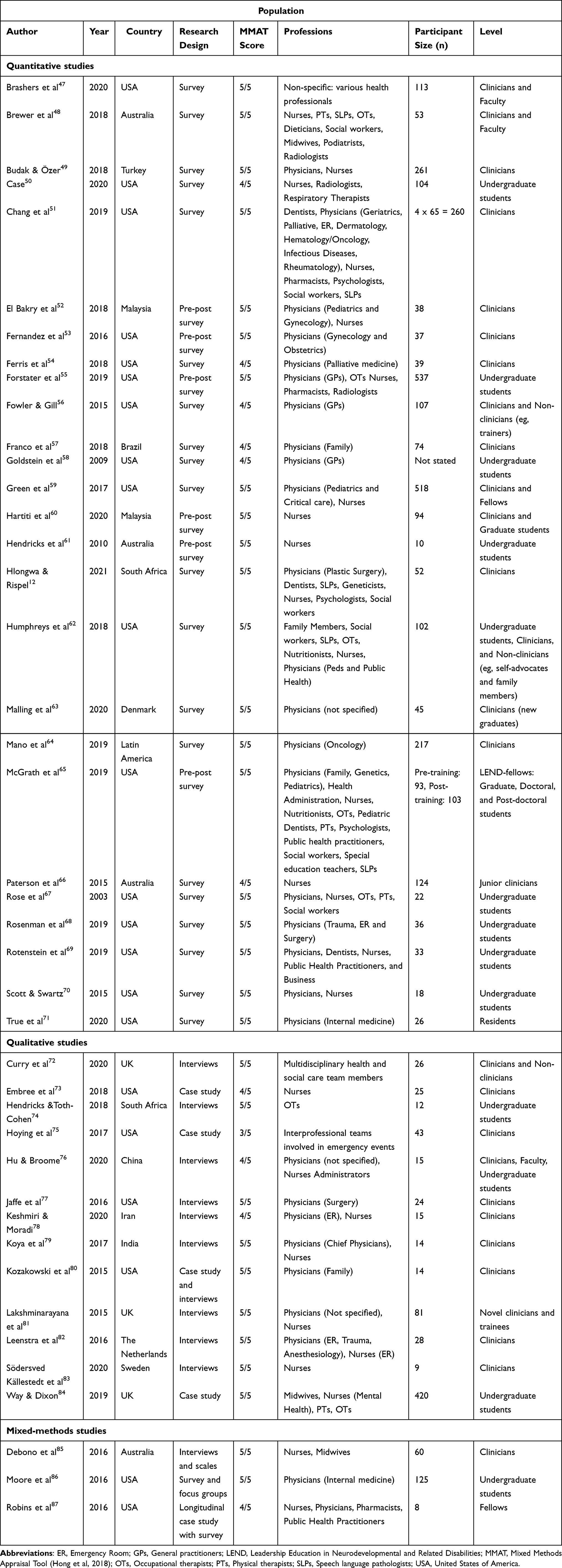 |
Table 3 Descriptive Information and Population (N = 42) |
Results
The results of the rapid review are presented as descriptive information related to the 42 included studies (authors, year of publication, country, research design) and the study population (discipline, number of participants and their level) (see Table 3). First, the quantitative studies are shown, followed by the qualitative and mixed methods studies. This is followed by an analysis of the intervention that was used, as well as the outcomes of the intervention described in the various studies included (see Table 4).
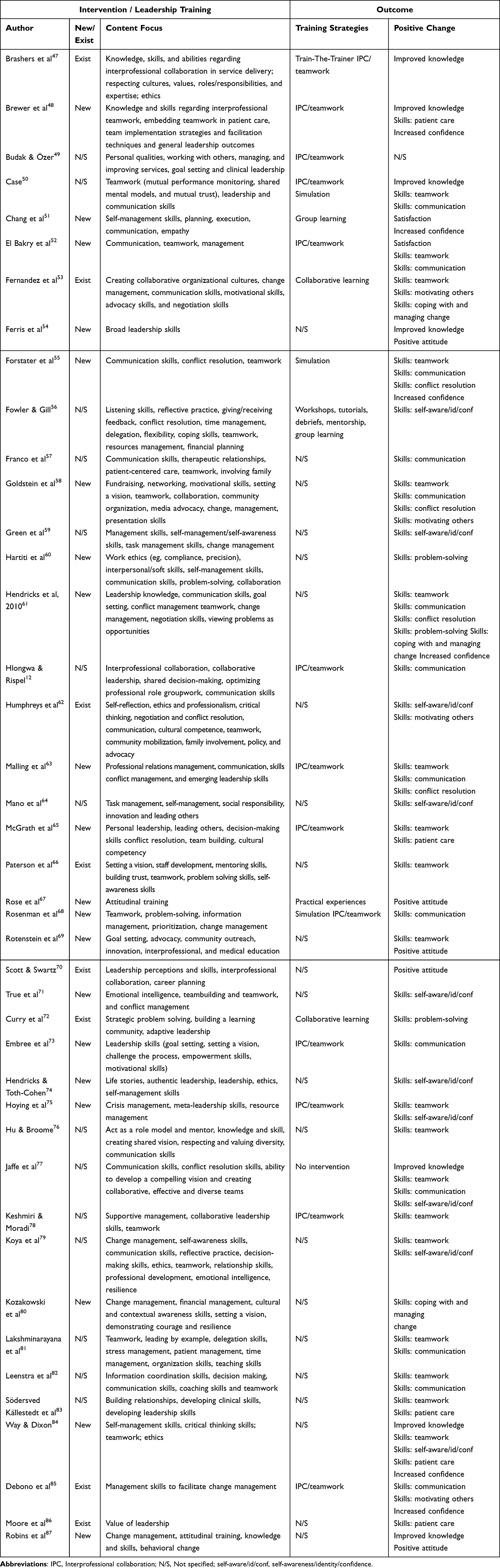 |
Table 4 Intervention Applied and Outcomes Achieved (N = 42) |
Descriptive Information on Included Studies
It is evident that there has been a steady increase in the number of studies published on the topic of leadership with only three studies published in the period 2000–2012 (7%) fulfilling the criteria set for the current review; five studies in the period 2013–2015 (12%), 17 studies between 2016 and 2018 (40%), and 17 studies between 2019 up to December 2022 (40%).
The methodologies used in the 42 studies included 26 surveys (62%) of which six (14%) specifically mentioned being offered pre- and post-training; 13 were qualitative studies (31%) of which four were case studies and nine were interviews; and three mixed-methods studies (7%) and one study (2%) was longitudinal in nature.
Geographically, half of the studies (n = 20) were conducted in the USA. The other half were split between the United Kingdom (n = 4), Australia (n = 4); Malaysia (n = 2); South Africa (n = 3) and one each from Sweden, Denmark, the Netherlands, Turkey, Iran, India, China, Brazil, and Latin America (n = 9).
Regarding the quality appraisal, the one study that met 60% of the quality indicators (score of 3/5) was a qualitative case study. The 10 studies that met 80% of the quality indicators (score of 4/5) consisted of seven studies that employed surveys of which one study was longitudinal in nature, although none of the pre- and post-surveys fell into this category, as well as two qualitative studies which made use of interviews (one study used an in-depth interview and the other study used a semi-structured interview) and one case study. Most of the studies (n = 31) obtained a score of 5 which indicated 100% descriptive quality.
Population: Healthcare Practitioners
The number of participants ranged from six81 to 537.55 Slightly more than a quarter of the studies (11/42 = 26%) reported on more than 100 participants, while 10 studies (24%) reported on 20 or less participants. The remaining 50% of papers (21) reported on between 21 and 99 participants. One study58 did not report on the number of participants.
Of the specific disciplines that were included, three studies47,72,75 did not specify the disciplines which were included, but simply mentioned “multi-disciplinary teams”. Figure 2 shows the distribution of the professions which were included.
In the 29 studies that mentioned physicians, and the 24 studies that mentioned nurses, some differentiated the type of medicine (oncology, emergency medicine, surgery, pediatrics, family medicine and public health) as shown in Table 3. HCPs in the applied professions included SLPs (five studies); occupational therapists (OTs) (seven studies), physiotherapists (PTs) (four studies) and nutritionists (three studies). Other HCPs included midwives, dentists, pharmacists, and podiatrists.
Regarding the level at which these practitioners were functioning, it is evident that most studies (26/42 = 62%) reported on clinicians (ie, practicing professionals), although four of these studies reported on both clinicians and students while two studies reported on both clinicians and the academic faculty. A total of 16 students at different levels of their studies participated (ranging from under-graduate to master’s level).
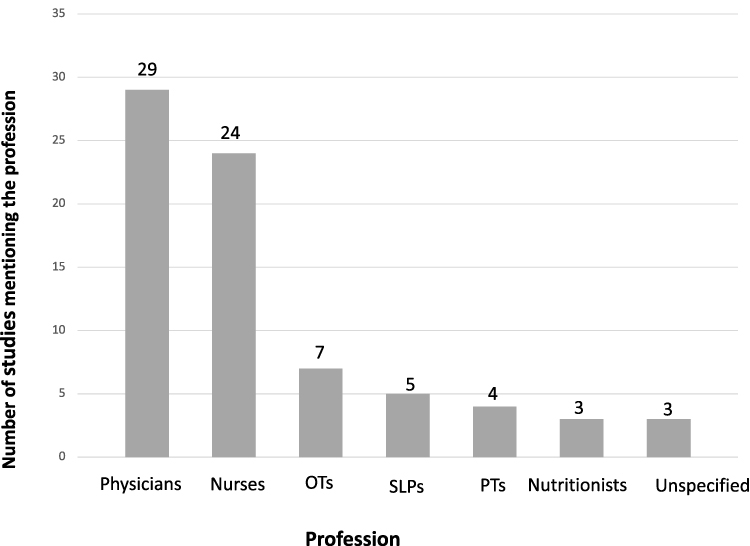 |
Figure 2 Distribution of professions. |
Interventions Employed to Train/Enhance Leadership Development
Table 4 reports on the specific interventions that were described in the different programs. Nearly half of the studies (20/42) reported on new training programs, while eight studies reported on existing programs.47,53,66,70,72,76,85,86 In total, 14 studies did not specify whether the research reported on a new or on an existing program.7,12,49,50,56,57,59,76,78,81–83,88 Most of the studies did not report on the length of training, although there appeared to be variability ranging from intensive-three and a half day courses53 to courses spanning over two years.54 Different training strategies were used, of which interprofessional teamwork (ie, working in teams across disciplinary boundaries) was the most prominent, and was mentioned in 13 of the 42 studies.12,47–50,52,63,65,68,73,75,78,85 Three studies mentioned the use of group or collaborative learning,51,53,72 while the use of simulation activities as a means of knowledge application was also mentioned in three studies.50,55,68 Practical experiences was mentioned in the study by Rose and colleagues67 and the use of the “train-the-trainer” method in the Brashers et al47 study as forms of hands-on learning. In total, 23 studies did not mention what type of training strategy was used.
Regarding the content on which the training focused, it appeared that aspects related to the importance of teamwork (including a variety of teamwork elements, as well as collaboration across disciplines) received high priority in 25 of the 42 studies.12,47–50,52–54,56–58,62,65,66,68,71,73,76–79,81,82,84,88 This was an expected finding given the focus on leadership, as leadership often involves teamwork. The aspects related to teamwork included conflict resolution, communication skills in teams, problem-solving, setting a joint vision and motivating others towards such a vision, roles and responsibilities of team members, time management and resource management. The important roles of the family as team members were also highlighted.
Another aspect that received attention was self-management, which also included demonstrating courage and resilience, empathy, reflection, and self-awareness.51,60,65,66,71,74,76,79,80,84 A number of the studies specifically highlighted the importance of managing change and assisting others in this regard53,58,59,61,67,68,79,80,85 as well as practicing in an ethically responsive manner.47,60,62,74,79,84 Some studies did not specify the leadership skills, but merely reported on broad or general leadership skills,50,54,61,63,64,70,73,75,83,86 while other studies were more specific and mentioned, for example, clinical leadership,49 adaptive leadership,72 authentic leadership,74 collaborative leadership,12,78 personal leadership,65 or in some cases, not leadership skills but management skills.59,60,63,64,68,78–81,87
Outcomes Achieved by the Specific Interventions Employed
Table 4 also shows the main outcomes (ie, positive change) that could be directly attributed to the interventions described in the various studies. There were five main types of outcomes achieved. The majority of the 42 studies focused on increasing specific skills with seven studies each reporting on an increase in knowledge47,48,50,54,77,84,87 and in confidence,48,51,55,60,61,84,85 while more positive attitudes were reported in four studies54,67,70,87 and satisfaction with the leadership training program in two studies.51,52 The nature of the skills which were addressed in the different studies varied greatly and hence resulted in different types of skills such as IPC or teamwork skills that improved in 18 studies,50,52,53,55,58,60,61,65,75–79,81–84 followed by 15 studies that emphasized communication skills,12,50,52,55,57,58,60,61,63,68,73,77,81,82,85 and increased self-awareness/self-identity and self-confidence in 10 studies.59,60,62,64,71,74,75,77,79,84 Four studies each reported back on improved skills related to conflict resolution,55,58,61,63 patient care,48,65,83,84 and motivating others,53,58,62,85 while three studies each reported on skills related to coping with change,53,61,80 and problem-solving.61,72,85 From Table 4, it is possible to see that any combination of outcomes was possiblefor example, improving both knowledge and skills, or improving skills and facilitating a positive attitude. Furthermore, some studies only reported on one skill improving,68 while some reported on multiple skills (eg, Jaffe77).
Discussion
The aim of the present rapid review is to investigate literature on leadership in health and education practice to highlight the leadership characteristics, skills and strategies of HCPs required for collaborative interprofessional service delivery. Leadership literature dated between 2010 and 2022 was studied, using a number of criteria. The main findings of this review are discussed below.
Leadership in Healthcare Professions
Leadership is viewed as a core role and responsibility of HCPs across a variety of care disciplines to ensure improved service delivery and patient care. A trend of more published research in leadership in HCPs was noted from the year 2010. Although studies from around the globe were included, the USA appears to lead the research in the current study. This trend was also noted by Brewer and colleagues14 who mentioned that most empirical studies included in their review were undertaken by researchers based in North America. This may be attributed to the vast healthcare system in the USA and requirements for evidence-based practice that permeates all healthcare professions. In contrast to early intervention and early childhood special education where Movahedazarhouligh89 reported a paucity of research on leadership research, this topic is well studied in the healthcare profession.
Evidence Base
This review identified a variety of methodologies employed, which can be attributed to the different types of training programs reported on. Survey research was the predominant methodology (60%) employed to study the outcomes of leadership training. Qualitative research, including case studies and interviews, mixed-methods research and a longitudinal study were included in the 42 articles included and analyzed in this review. Complying with quality indicators of research design is essential to the development of an evidence base of leadership within healthcare.90 The different disciplines within the healthcare profession were widely represented in the populations studied, although three studies did not specify which disciplines were studied. This variation points to the strength of the research evidence which can be used to inform the development of future quality training programs within the healthcare profession.
Similar to the review by Brewer et al,14 most articles in the present review also did not refer to, or operationalize any specific leadership approaches or models. Bahreini et al91 emphasize the importance of developing and adhering to a framework for training leadership in HCPs, especially one that can be adapted for use in local situations. Therefore, the extracted components of the current rapid review can be viewed as a first step in developing an evidence base, building on a comprehensive overview of leadership in HCPs.
Elements of Leadership Training
Leadership is viewed to be an inherent quality and characteristic of HCPs.90 However, the complex and dynamic nature of leadership in HCPs precludes the unanimously accepted description of the characteristics required to perform an effective leadership role. Smith et al92 conclude that effective interprofessional health and social care team leadership requires a unique blend of understanding and skills that support innovation and improvement. Some of the ways through which leadership is often evidenced is through advocacy (ie, to promote the self-advocacy of the clients with whom HCPs work), training of families and other role players, mentoring (eg, of less experienced colleagues), supervision, continuing education, and research. It is thus self-explanatory that leadership necessitates a complex set of knowledge, skills and attitudes which require formal education, either at a pre-professional or professional level.7 Despite this acknowledgement of the importance of leadership, formal training for the development of skill sets and abilities is generally lacking to better prepare future HCPs and in continuing education for practicing HCPs. In rare cases where leadership is included in curricula, the emphasis is on aspects, such as leadership for healthcare systems, advancing careers, etc., rather than on, for example advocacy.7
The current review reveals some gaps in reporting on the specific nature of the training programs, for example gaps related to the length and intensity of programs, which is important in evaluating the training outcomes. Regarding training strategies, an interprofessional teamwork approach was followed by 31% of the programs and three studies followed a collaborative learning approach. These approaches reflect the recent trends in healthcare service delivery.13 There is, however, a need for research to clearly justify and describe the training strategies employed, as 55% of the studies did not describe this in their methods. The content of the training programs was focused on different elements of leadership including interprofessional collaboration and teamwork and the specific skills required to lead in that context, personal leadership skills such as self-management, strategies for managing change and ethical responsibilities of leaders. Furthermore, not all programs identified their approach to leadership, which is the framework for selecting the knowledge and skills to be trained. Although the studies had sound research methodologies, the training program development could be more rigorous, which would allow for the replication of training programs. Rao et al93 point to the importance of course design when developing quality improvement educational leadership programs.
Leadership Training Outcomes
Although all the articles reported positive changes which were attributed to the training programs, the question remains how to ensure retention, as only a few studies included post-surveys and long-term training. Since leadership is a desired outcome of HCPs training programs, whether on a pre-professional or professional level, it should instill a process of lifelong reflection and development.88 By identifying specific leadership competencies relating to knowledge and skill development, defined objectives can be formulated. Curriculum mapping on the pre-professional level can be implemented to determine the overage of leadership-related competencies across the curriculum.88,94
Lastly, the global COVID-19 pandemic added urgency and importance to leadership skills in the healthcare profession internationally. Difficulties in accessing services due to COVID-19 restrictions led to telehealth. However, the use of technology is challenging and could be limiting in managing complex situations. HCPs were further challenged in a variety of ways such as applying universal precautions and accessing personal protection equipment, to name but a few. The COVID-19 health emergency called for crisis leadership with specific competencies such as signal detection, prevention and preparation, containment and damages and learning and reflection.95
Limitations and Suggestions for Future Research
This rapid review includes strengths with its size, method, and scope, but also has limitations. Firstly, it is possible that the identified search terms did not identify all possible papers as only 11 databases were searched, and no hand-searching of papers was included. The present review focused only on papers published in English and only from the year 2000 onwards. One study met the 60% MMAT quality appraisal score with many studies reflecting “missing data” (eg, did not specify the sample size; did not specify the methods used for leadership training; did not specify the length of training).
The international scope of this rapid review presents distinct challenges for research conducted across varying disciplines and the methods used in the different contexts. Papers covered a range of HCP disciplines which may not result in the same implications across disciplines. However, it is expected that it would contribute to the existing body of literature and assist HCPs when developing leadership curricula for their specific discipline.
Future research could build on the current data and focus on a more critical examination of interprofessional leadership, and the capabilities required to lead the changes required in both education and practice settings.14 To further support the emerging trend of including leadership development programs in HCP curricula, sustainability of the outcomes of leadership development programs in different contexts can be explored.
Conclusion
This rapid review was designed to systematically catalogue literature on leadership in healthcare practice and education in an unbiased manner to highlight the leadership characteristics and skills required by HCPs for collaborative interprofessional service delivery. It also described the leadership development strategies that had been found to be effective. As the change in healthcare leadership continues to evolve, leadership development programs need to attend to the needs of HCP on all levels. The review revealed that a paucity exists in the description of leadership approaches and models used. Moreover, a dearth of information was found on retention and long-term impact of leadership development programs. The evidence-based highlighted by qualitative, quantitative, and mixed methods research presents distinct opportunities for curriculum development by focusing on both content and the methods needed for leadership programs. Anchoring this evidence-base within a systematic search of the extant literature provides increased precision for curriculum development.
Acknowledgments
The Carnegie African Diaspora Fellowship (ADF) Program (PS00174859 and PS00157223) and the University of Pretoria’s Research Office are gratefully acknowledged for sponsoring this research project. The authors also wish to thank Gabrielle Saliba and Mary Catherine Smith who assisted with the search, screening, and data extraction as well as with the technical editing of the manuscript.
Disclosure
We have no known conflicts of interest to disclose.
References
(All studies included in the review are marked with an asterisk*)
1. Garman AN, Standish MP, Wainio JA. Bridging worldviews: toward a common model of leadership across the health professions. Health Care Manage Rev. 2020;45(4):E45–E55. doi:10.1097/HMR.0000000000000243
2. McGowan E, Hale J, Bezner J, Harwood K, Green-Wilson J, Stokes E. Leadership development of health and social care professionals: a systematic review. Leader. 2020;4(4):231–238. doi:10.1136/leader-2020-000211
3. van Diggele C, Burgess A, Roberts C, Mellis C. Leadership in healthcare education. BMC Med Educ. 2020;20(S2):456. doi:10.1186/s12909-020-02288-x
4. Papadakos T, Gospodarowicz M, Giuliani M. Why leadership? The Intersectionality of leadership and health equity. Int J Radiation Oncology Biol Physics. 2022;113(1):37–39. doi:10.1016/j.ijrobp.2022.01.051
5. Forsyth C, Mason B. Shared leadership and group identification in healthcare: the leadership beliefs of clinicians working in interprofessional teams. J Interprof Care. 2017;31(3):291–299. doi:10.1080/13561820.2017.1280005
6. Cleary M, Kornhaber R, Thapa DK, West S, Visentin D. A systematic review of behavioral outcomes for leadership interventions among health professionals. J Nurs Res. 2020;28(5):e118. doi:10.1097/jnr.0000000000000397
7. Carozza LS. Leadership in Speech-Language. Pathology. Plural Publishing Inc; 2019.
8. Rath T, Conchie B. Strength based leadership. NHRD Network J. 2008;2(5):146–147. doi:10.1177/0974173920090531
9. Mianda S, Voce A. Developing and evaluating clinical leadership interventions for frontline healthcare providers: a review of the literature. BMC Health Serv Res. 2018;18(1):747. doi:10.1186/s12913-018-3561-4
10. Folkman AK, Tveit B, Sverdrup S. Leadership in interprofessional collaboration in health care. J Multidiscip Healthc. 2019;12:97–107. doi:10.2147/JMDH.S189199
11. World Health Organization. Framework for action on interprofessional education and collaborative practice. World Health Organization; 2010. Available from: https://www.who.int/publications/i/item/framework-for-action-on-interprofessional-education-collaborative-practice.
12. *Hlongwa P, Rispel LC. Interprofessional collaboration among health professionals in cleft lip and palate treatment and care in the public health sector of South Africa. Hum Resour Health. 2021;19(1):25. doi:10.1186/s12960-021-00566-3
13. Iachini AL, DeHart DD, Browne T, Dunn BL, Blake EW, Blake C. Examining collaborative leadership through interprofessional education: findings from a mixed methods study. J Interprof Care. 2019;33(2):235–242. doi:10.1080/13561820.2018.1516635
14. Brewer ML, Flavell HL, Trede F, Smith M. A scoping review to understand “leadership” in interprofessional education and practice. J Interprof Care. 2016;30(4):408–415. doi:10.3109/13561820.2016.1150260
15. Curado C, Santos R. Transformational leadership and work performance in health care: the mediating role of job satisfaction. Leadersh Health Serv. 2021;ahead-of-print. PMID: 34767323. doi:10.1108/LHS-06-2021-0051
16. Robbins B, Davidhizar R. Transformational leadership in health care today. Health Care Manag. 2020;39(3):117–121. doi:10.1097/HCM.0000000000000296
17. Kaehne A, Feather J, Chambers N, et al. Rapid Review on System Leadership in Health Care: System Leadership: What Do We Know and What Do We Need to Find Out? Edge Hill University; 2022.
18. Franczukowska AA, Krczal E, Knapp C, Baumgartner M. Examining ethical leadership in health care organizations and its impacts on employee work attitudes: an empirical analysis from Austria. Leadersh Health Serv. 2021;34:229–247. PMID: 34085804; PMCID: PMC8939467. doi:10.1108/LHS-06-2020-0034
19. McKimm J, Redvers N, Omrani OE, Parkes MW, Elf M, Woollard R. Education for sustainable healthcare: leadership to get from here to there. Med Teach. 2020;42(10):1123–1127. doi:10.1080/0142159X.2020.1795104
20. Terkamo-Moisio A, Karki S, Kangasniemi M, Lammintakanen J, Häggman-Laitila A. Towards remote leadership in health care: lessons learned from an integrative review. J Adv Nurs. 2022;78:595–608. doi:10.1111/jan.15028
21. Ong YH, Koh MHY, Lim WS. Shared leadership in interprofessional teams: beyond team characteristics to team conditions. J Interprof Care. 2020;34(4):444–452. doi:10.1080/13561820.2019.1653834
22. Dyrbye LN, West CP, Hunderfund AL, et al. Relationship between burnout, professional behaviors, and cost-conscious attitudes among US physicians. J Gen Intern Med. 2020;35(5):1465–1476. doi:10.1007/s11606-019-05376-x
23. Varpio L, Teunissen P. Leadership in interprofessional healthcare teams: empowering knotworking with followership. Med Teach. 2021;43(1):32–37. doi:10.1080/0142159X.2020.1791318
24. Page MD. The quadrat of performance: a leadership tool for professional growth. Perspect ASHA Spec Interest Groups. 2020;5(6):1564–1576. doi:10.1044/2020_PERSP-20-00167
25. Allwood D, Koka S, Armbruster R, Montori V. Leadership for careful and kind care. BMJ Leader. 2022;6:125–129. doi:10.1136/leader-2021-000451
26. Sakr CJ, Rahme D, Fakih L, et al. Anxiety among healthcare workers during COVID-19 pandemic in Lebanon: the importance of the work environment and personal resilience. Psychol Res Behav Manag. 2022;15:811–821. doi:10.2147/PRBM.S350125
27. Perez J. Leadership in healthcare: transitioning from clinical professional to healthcare leader. J of Healthc Managem. 2021;66(4):280–302. doi:10.1097/JHM-D-20-00057
28. Stoll BJ. Reflections on leadership: seizing and embracing opportunities-holding up half the sky. JAMA. 2020;323(17):1728–1729. doi:10.1001/jama.2020.3097
29. Sonnino RE. Health care leadership development and training: progress and pitfalls. J Health Leadership. 2016;8:19–29. doi:10.2147/JHL.S68068
30. Brame JL, Price J, Taylor PM. Academic Leadership development for health professions programs. J Allied Health. 2022;51(4):e105–e111.
31. Bhulani N, Miao TL, Norbash A, Castillo M, Khosa F. Leadership in healthcare: a bibliometric analysis of 100 most influential publications. BMJ Leader. 2021;5:65–68. doi:10.1136/leader-2019-000207
32. Johnson O, Begg K, Kelly AH, Sevdalis N. Interventions to strengthen the leadership capabilities of health professionals in Sub-Saharan Africa: a scoping review. Health Policy Plan. 2021;36(1):117–133. doi:10.1093/heapol/czaa078
33. Nightingale A. Implementing collective leadership in healthcare organisations. Nurs Stand. 2020;35(5):53–57. doi:10.7748/ns.2020.e11448
34. Haby MM, Chapman E, Clark R, Barreto J, Reveiz L, Lavis JN. What are the best methodologies for rapid reviews of the research evidence for evidence-informed decision making in health policy and practice: a rapid review. Health Res Policy Sys. 2016;14(1):83. doi:10.1186/s12961-016-0155-7
35. Bolton L, Mills C, Wallace S, Brady MC; Royal College of Speech and Language Therapists (RCSLT) COVID‐19 Advisory Group. Aerosol generating procedures, dysphagia assessment and COVID‐19: a rapid review. Int J of Lang Comm Disor. 2020;55(4):629–636. doi:10.1111/1460-6984.12544
36. Malandraki GA, Arkenberg RH, Mitchell SS, Malandraki JB. Telehealth for dysphagia across the life span: using contemporary evidence and expertise to guide clinical practice during and after COVID-19. Am J Speech Lang Pathol. 2021;30(2):532–550. doi:10.1044/2020_AJSLP-20-00252
37. Bell V, Wade D. Mental health of clinical staff working in high-risk epidemic and pandemic health emergencies a rapid review of the evidence and living meta-analysis. Soc Psychiatr Epidemiol. 2021;56(1):1–11. doi:10.1007/s00127-020-01990-x
38. Blanco D, Altman D, Moher D, Boutron I, Kirkham JJ, Cobo E. Scoping review on interventions to improve adherence to reporting guidelines in health research. BMJ Open. 2019;9(5):e026589. doi:10.1136/bmjopen-2018-026589
39. Moher D, Liberati A, Tetzlaff J, Altman DG; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):1–6. doi:10.1371/journal.pmed.1000097
40. Khalil H, Peters M, Godfrey CM, McInerney P, Soares CB, Parker D. An evidence-based approach to scoping reviews: EBP approach to scoping reviews. Worldviews on Evidence-Based. Nurs. 2016;13(2):118–123. doi:10.1111/wvn.12144
41. Godin K, Stapleton J, Kirkpatrick SI, Hanning RM, Leatherdale ST. Applying systematic review search methods to the grey literature: a case study examining guidelines for school-based breakfast programs in Canada. Syst Rev. 2015;4(1):138. doi:10.1186/s13643-015-0125-0
42. Harari MB, Parola HR, Hartwell CJ, Riegelman A. Literature searches in systematic reviews and meta-analyses: a review, evaluation, and recommendations. J Voc Beh. 2020;118:103377. doi:10.1016/j.jvb.2020.103377
43. Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan - A web and mobile app for systematic reviews. Syst Rev. 2016;5(1):210. doi:10.1186/s13643-016-0384-4
44. Graham M, Milanowski A, Miller J. Measuring and Promoting Inter-Rater Agreement of Teacher and Principal Performance Ratings Wisconsin: Center for Educator Compensation Reform; 2012. Available from: https://eric.ed.gov/?id=ED532068.
45. Hong QN, Pluye P, Fàbregues S, et al. Improving the content validity of the mixed methods appraisal tool: a modified e-Delphi study. J Clinic Epidem. 2019;111:49–59. doi:10.1016/j.jclinepi.2019.03.008
46. Sattler DN, McKnight PE, Naney L, Mathis R. Grant peer review: improving inter-rater reliability with training. PLoS One. 2015;10(6):e0130450. doi:10.1371/journal.pone.0130450
47. *Brashers V, Haizlip J, Owen JA. The ASPIRE Model: grounding the IPEC core competencies for interprofessional collaborative practice within a foundational framework. J Interprof Care. 2020;34(1):128–132. doi:10.1080/13561820.2019.1624513
48. *Brewer ML, Flavell H, Trede F, Smith M. Creating change agents for interprofessional education and practice: a leadership programme for academic staff and health practitioners. Inter J of Leadership Educ. 2017;21(5):1–13. doi:10.1080/13603124.2017.1279349
49. *Budak F, Özer Ö. Exploring the impacts of personal factors on clinical leadership in a University Hospital. J Res Nurs. 2018;23(8):711–724. doi:10.1177/1744987118788716
50. *Case RD. The effectiveness of interprofessional simulation experiences used in health science education. Resp Care Educ Annual. 2020;29:3–12.
51. *Chang A, Lundebjerg NE, Abrams J, et al. Leadership, inside and out: the tideswell‐AGS‐ADGAP emerging leaders in aging program. J Am Geriatr Soc. 2019;67(3):437–442. doi:10.1111/jgs.15702
52. *El Bakry AAN, Farghaly A, Shehata MH, Matter A, Hosny S. Evaluation of an interprofessional course on leadership and management for medical and nursing pre-registration house officers. EIMJ. 2018;10(1):41–52. doi:10.21315/eimj2018.10.1.6
53. *Fernandez CSP, Noble CC, Jensen ET, Chapin J. Improving leadership skills in physicians: a 6-Month retrospective study. J Ldrship Studies. 2016;9(4):6–19. doi:10.1002/jls.21420
54. *Ferris FD, Moore SY, Callaway MV, Foley KM. Leadership development initiative: growing global leaders… Advancing palliative care. J Pain and Sympt Managemt. 2018;55(2):S146–S156. doi:10.1016/j.jpainsymman.2017.05.011
55. *Forstater A, Sicks S, Collins L, Schmidt E. Team SAFE: a large-scale interprofessional simulation-based TeamSTEPPS® curriculum. J of Interprof Educ Prac. 2019;16:100221. doi:10.1016/j.xjep.2018.12.002
56. *Fowler I, Gill A. Leadership skills teaching in Yorkshire & the Humber – a survey: uncovering, sharing, developing, embedding. Educ for Prim Care. 2015;26(5):311–316. doi:10.1080/14739879.2015.1079022
57. *Franco CA, Franco RS, Lopes JMC, Severo M, Ferreira MA. Clinical communication skills and professionalism education are required from the beginning of medical training - A point of view of family physicians. BMC Med Educ. 2018;18(1):43. doi:10.1186/s12909-018-1141-2
58. *Goldstein AO, Calleson D, Bearman R, Steiner BD, Frasier PY, Slatt L. Teaching Advanced Leadership Skills in Community Service (ALSCS) to medical students. Acad Med. 2009;84(6):754–764. doi:10.1097/ACM.0b013e3181a40660
59. *Green ML, Winkler M, Mink R, et al. Defining leadership competencies for pediatric critical care fellows: results of a national needs assessment. Med Teacher. 2017;39(5):486–493. doi:10.1080/0142159X.2017.1297527
60. *Hartiti T, Poddar S, Bhaumik A. Development transformational leadership model to improve nurses’ soft skills. Malaysian J of Med and Health Sciences. 2020;16(Supp 10):113–118.
61. *Hendricks JM, Cope VC, Harris M. A leadership program in an undergraduate nursing course in Western Australia: building leaders in our midst. Nurse Educ Today. 2010;30(3):252–257. doi:10.1016/j.nedt.2009.12.007
62. *Humphreys BP, Kurtz AJ, Portrie C, Couse LJ, Hajnaghizadeh F. Advancing leadership skills: a multiyear examination of LEND trainee self-efficacy growth. Matern Child Health J. 2018;22(10):1377–1383. doi:10.1007/s10995-018-2582-2
63. *Malling B, de Lasson L, Just E, Stegeager N. How group coaching contributes to organisational understanding among newly graduated doctors. BMC Med Educ. 2020;20(1):193. doi:10.1186/s12909-020-02102-8
64. *Mano MS, Gomes R, Werutsky G, et al. Cross-cultural validity study of medical education leadership competencies instrument in Latin American physicians: a multinational study. J Glob Oncol. 2019;(5):1–9. doi:10.1200/JGO.19.00243
65. *McGrath ER, Bacso DR, Andrews JG, Rice SA. Intentional interprofessional leadership in maternal and child health. Leadersh Health Serv. 2019;32(2):212–225. doi:10.1108/LHS-04-2018-0026
66. *Paterson K, Henderson A, Burmeister E. The impact of a leadership development programme on nurses’ self‐perceived leadership capability. J Nurs Manag. 2015;23(8):1086–1093. doi:10.1111/jonm.12257
67. *Rose MA, Lyons KJ, Miller KS, Cornman-Levy D. The effect of an interdisciplinary community health project on student attitudes toward community health, people who are indigent and homeless, and team leadership skill development. J Allied Health. 2003;32(2):122–125.
68. *Rosenman ED, Vrablik MC, Brolliar SM, Chipman AK, Fernandez R. Targeted simulation-based leadership training for trauma team leaders. West J Emerg Med. 2019;20(3):520–526. doi:10.5811/westjem.2019.2.41405
69. *Rotenstein L, Perez K, Wohler D, et al. Preparing health professions students to lead change. Leadersh Health Serv. 2019;32(2):182–194. doi:10.1108/LHS-02-2018-0011
70. *Scott EA, Swartz MK. Interprofessional student experiences on the HAVEN free clinic leadership board. J Interprof Care. 2015;29(1):68–70. doi:10.3109/13561820.2014.934339
71. *True MW, Folaron I, Colburn JA, Wardian JL, Hawley-Molloy JS, Hartzell JD. Leadership training in graduate medical education: time for a requirement? Mil Med. 2020;185(1/2):e11–e16. doi:10.1093/milmed/usz140
72. *Curry LA, Ayedun AA, Cherlin EJ, Allen NH, Linnander EL. Leadership development in complex health systems: a qualitative study. BMJ Open. 2020;10(4):e035797. doi:10.1136/bmjopen-2019-035797
73. *Embree JL, Wagnes L, Hendricks S, LaMothe J, Halstead J, Wright L. Empowering nurses to lead interprofessional collaborative practice environments through a nurse leadership institute. J Contin Educ Nurs. 2018;49(2):61–71. doi:10.3928/00220124-20180116-05
74. *Hendricks F, Toth-Cohen S. Perceptions about authentic leadership development: south African occupational therapy students’ camp experience. Occ Ther Inter. 2018;2018:1–9. doi:10.1155/2018/1587906
75. *Hoying C, Farra S, Mainous R, Baute R, Gneuhs M. Collaboration between academia and practice: interprofessional crises leadership and disaster management. JONA. 2017;47(2):123–128. doi:10.1097/NNA.0000000000000451
76. *Hu Y, Broome M. Leadership characteristics for interprofessional collaboration in China. J Prof Nurs. 2020;36(5):356–363. doi:10.1016/j.profnurs.2020.02.008
77. *Jaffe GA, Pradarelli JC, Lemak CH, Mulholland MW, Dimick JB. Designing a leadership development program for surgeons. J Surg Res. 2016;200(1):53–58. doi:10.1016/j.jss.2015.08.002
78. *Keshmiri F, Moradi K. Perceptions of Iranian emergency department directors of interprofessional leadership: an interview study. J Interprof Care. 2020;34(6):747–755. doi:10.1080/13561820.2019.1672632
79. *Koya K, Anderson J, Sice P. The embodied nurse: interdisciplinary knowledge exchange between compassionate nursing and recent developments in embodied leadership studies. J Adv Nurs. 2017;73(12):3028–3040. doi:10.1111/jan.13363
80. *Kozakowski SM, Eiff MP, Green LA, et al. Five key leadership actions needed to redesign family medicine residencies. J Grad Med Educ. 2015;7(2):187–191. doi:10.4300/JGME-D-14-00214.1
81. *Lakshminarayana I, Wall D, Bindal T, Goodyear HM. A multisource feedback tool to assess ward round leadership skills of senior paediatric trainees: (1) Development of tool. Postgrad Med J. 2015;91(1075):262–267. doi:10.1136/postgradmedj-2014-132692
82. *Leenstra NF, Jung OC, Johnson A, Wendt KW, Tulleken JE. Taxonomy of trauma leadership skills: a framework for leadership training and assessment. Acad Med. 2016;91(2):272–281. doi:10.1097/ACM.0000000000000890
83. *Södersved Källestedt M, Asp M, Letterstål A, Widarsson M. Perceptions of managers regarding prerequisites for the development of professional competence of newly graduated nurses: a qualitative study. J Clin Nurs. 2020;29(23):4784–4794. doi:10.1111/jocn.15522
84. *Way S, Dixon L-A. Applying interprofessional education to the practice setting. BR J Nurs. 2019;28(17):1144–1147. doi:10.12968/bjon.2019.28.17.1144
85. *Debono D, Travaglia JF, Dunn AG, et al. Strengthening the capacity of nursing leaders through multifaceted professional development initiatives: a mixed method evaluation of the ‘Take the Lead’ program. Collegian. 2016;23(1):19–28. doi:10.1016/j.colegn.2014.09.005
86. *Moore JM, Wininger DA, Martin B. Leadership for all: an internal medicine residency leadership development program. J Grad Med Educ. 2016;8(4):587–591. doi:10.4300/JGME-D-15-00615.1
87. *Robins L, Murphy N, Zierler B. Leveraging a faculty fellowship programme to develop leaders in interprofessional education. J Interprof Care. 2016;30(4):520–522. doi:10.3109/13561820.2016.1150258
88. Janke KK, Nelson MH, Bzowyckyj AS, Fuentes DG, Rosenberg E, DiCenzo R. Deliberate integration of student leadership development in Doctor of Pharmacy programs. AJPE. 2016;80(1):2. doi:10.5688/ajpe8012
89. Movahedazarhouligh S. A scoping review of the knowledge base, landscape, and trends in leadership literature in early intervention, early childhood and early childhood special education. Infants and Young Child. 2021;34(3):159–177. doi:10.1097/IYC.0000000000000196
90. Ledlow GR, Stephens JH. Leadership for Health Professionals: Theory, Skills, and Applications.
91. Bahreini R, Gholizadeh M, Gedik FG, Yousefi M, Janati A. Components of contributing conditions to strengthen health system management and leadership capacity building: a systematic review and decision-making framework. LHS. 2021;34(4):527–545. doi:10.1108/LHS-01-2021-0006
92. Smith T, Fowler-Davis S, Nancarrow S, Ariss SMB, Enderby P. Leadership in interprofessional health and social care teams: a literature review. Leadersh Health Serv. 2018;31(4):452–467. doi:10.1108/LHS-06-2016-0026
93. Rao SK, Carballo V, Cummings BM, Millham F, Jacobson JO. Developing an interdisciplinary, team-based quality improvement leadership training program for clinicians: the partners clinical process improvement leadership program. Am J Med Qual. 2017;32(3):271–277. doi:10.1177/1062860616648773
94. Tucci M, Tong K, Chia K, DiVall M. Curricular and co-curricular coverage of leadership competencies and the influence of extracurricular engagement on leadership development. Am J Pharm Educ. 2019;83(2):238–248. doi:10.5688/ajpe6535
95. Sosik JJ. Leadership in times of crisis: competencies, coping mechanisms, and charisma. Penn State Great Valley webinar; 2020. Available from: https://psgv.secure.force.com/events/targetX_eventsb__events#/esr?eid=a124T000000PfHJQA0.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.