")
Back to Journals » Journal of Healthcare Leadership » Volume 16
Leadership Commitment and the Quality of Adolescent-Friendly Sexual Reproductive Health Services in Public Health Facilities Among Pastoral Districts of Guji Zone, Ethiopia
Authors Boku GG, Abeya SG, Ayers N, Abera M
Received 3 October 2023
Accepted for publication 6 February 2024
Published 12 February 2024 Volume 2024:16 Pages 53—66
DOI https://doi.org/10.2147/JHL.S441951
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Zhanming Liang
Gobena Godana Boku,1,2 Sileshi Garoma Abeya,3 Nicola Ayers,2 Muluembet Abera1
1Department of Population and Family Health, Faculty of Public Health, Jimma University, Jimma, Ethiopia; 2Department of Nursing, BPP University, London, UK; 3Department Public Health, Adama Hospital Medical College, Adama, Ethiopia
Correspondence: Gobena Godana Boku, Tel +251911545441 ; +25178451885, Email [email protected]
Background: Accessible and high-quality sexual and reproductive health services are essential for adolescents. However, there is a need for more knowledge about the role of leadership and the quality of these services in Ethiopia, where a significant proportion of the population consists of adolescents. Inadequate quality of friendly health services may lead to underutilization and higher rates of unintended pregnancies and sexually transmitted infections. This study aimed to evaluate the leadership role and quality of friendly health services in the pastoral community of East Guji Zone, Ethiopia.
Methods: We implemented in-depth interviews and focus group discussions with eight key informants and fifty participants. Study design: We used a programmatic qualitative research design. Data were collected using 22 semi-structured questions and analyzed using ATLAS.ti7.
Results: The findings indicate significantly less commitment to health sector leadership and substandard quality of adolescent-friendly sexual and reproductive health services. Inadequate achievement of the quality of care frameworks, including accessibility, equitability, availability, acceptability, and appropriateness, contributed to the insufficient quality of friendly health services.
Conclusions and Recommendations: Poor commitment of health facility leaders influenced the quality of adolescent-friendly sexual and reproductive health services in the pastoral community of the East Guji Zone, according to the study. We recommend enhancing organizational and provider readiness, ensuring equitability, and redesigning services through improving leadership commitment, which is crucial to improving the quality of adolescent-friendly health services. The Ministry of Health Ethiopia and relevant stakeholders should consider these recommendations to improve the quality of friendly health services for adolescents in Ethiopia.
Keywords: leadership commitment, adolescent, sexual and reproductive health, health services quality, health facilities, pastoral community
Introduction
Scientific evidence emphasizes the importance of higher-quality sexual and reproductive healthcare for adolescents.1 One of the Sustainable Development Goals (SDG) quality health care includes the imperative to “achieve universal health coverage, including access to quality essential healthcare services and access to safe, effective, quality and affordable essential medicines for all”..2,3 According to the healthcare quality improvement projects, Effectiveness, Safety, and Patient-centeredness/responsiveness are the three core dimensions of healthcare quality; other attributes, including appropriateness, continuity, timeliness, and acceptability, might easily be accommodated within these three dimensions.4 However, among these dimensions of healthcare quality, this study focused on patient-centered and effectiveness as core dimensions and equitability, acceptability, and satisfaction sub-dimension of healthcare quality, and key success factors of health quality improvement, which are leadership and their commitment.4,5
Adolescent-friendly health services aim to provide accessible care without barriers related to structures, sociocultural factors, or individual characteristics. Quality-friendly healthcare is one of the WHO service standards for all adolescents irrespective of their ability to pay, sex, age, marital status, education level, ethnic origin, sexual orientation, or other characteristics.6 However, challenges persist in the quality of sexual and reproductive health services globally, even after implementing the International Conference on Population & Development.7 The latest Ethiopian mini demographic and health surveys (EDHS 2019) identified that adolescents comprise 26.9% of Ethiopia’s population. Even though adolescents comprise a significant portion of the population, the quality of adolescent-friendly health services is low across different dimensions: 58.8%, 46.4%, and 47.2%, respectively.8–10
Conversely, The global trends show that only a few healthcare units provide high-quality reproductive health services to adolescents.1 Research evidence suggests that friendly health services should be accessible, acceptable, equitable, appropriate, and effective.11 In addition, Sexual and reproductive health services should adhere to human rights norms, medical ethics, and technical standards, encompassing availability, accessibility, acceptability, and quality of care. Every human being has a right and deserves to have the highest attainable standard of the four human right-based attributes of health services, including availability, accessibility, acceptability, and quality of care.7 High-quality adolescent-friendly sexual and reproductive health services contribute to client safety, increased utilization, trustworthiness, and reduced risks of sexual and reproductive problems. Public Health Facilities can only attract adolescents if they provide high-quality, friendly health services. However, middle and low-income countries, including Ethiopia, need to improve the quality of friendly health services.1,12,13 For Example, a study conducted in South Africa found that the district health facilities needed to meet the minimum standards required for Adolescent Friendly Health Services. Therefore, health facilities must recognize the unique needs of adolescents and be committed to providing high-quality services.14 However, without the excellent commitment of health sector leadership at different levels, achieving the quality of friendly health services in public health facilities is impossible. In addition, allocating the budget, creating attractive facilities, and ensuring the accessibility and availability of supplies, drugs, and relevant equipment are not possible without the decision-making role of health sector leadership on materials and human resources.
The Ethiopian health system is an administrative structure that includes the Ministry of Health, Regional Health Bureau, zonal Health department, and Wodera Health Office. Ethiopia’s health system comprises three-tier systems: primary healthcare units, general hospitals, and specialized hospitals. The primary healthcare unit (PHCU) comprises health posts staffed by health extension workers, clinics, and health centers, which are staffed with frontiers, healthcare providers, and primary hospitals. The primary health care unit (PHCU) provides most adolescent-friendly health services. As per the study conducted in Southern Ethiopia, the quality of youth-friendly services at public health facilities is poorly coordinated and uneven due to the lack of commitment of health facility leaders.
Moreover, this study also showed the need for more evidence on youth-friendly service quality in South Ethiopia.15 Similarly, the Ethiopian government has made considerable investments in health system infrastructure and health workforce development to expand primary healthcare units, general hospitals, and tertiary-level health facilities in the last 20 years. However, there are still wide disparities in equity and quality of healthcare delivery across and within the region.13
This study focuses on two primary healthcare units, precisely type “A” and type “B” health centers (Wadara & Harekelo), respectively. Cost-effective interventions for reducing SRH problems, including STIs/HIV, unsafe sex, unintended pregnancies, unsafe abortions, pregnancy-related illnesses, and complications, have identified adolescent-friendly health services. Ethiopia is one of sub-Saharan Africa where adolescent’ and youth deaths are the highest in the world.16 The unacceptably high burden of adolescent morbidity and mortality in Ethiopia is due to poor utilization of SRH services. One of the reasons for Poor adolescent-friendly SRH services utilization in Ethiopia is the poor quality of SRH services.17 Therefore, this study aims to examine the quality of adolescent-friendly health intervention and the role of leadership in the pastoral community of the east Guji zone in Ethiopia. Therefore, the findings confidently help interested researchers as scientific literature and mainly provide access to essential information on the quality of adolescent-friendly health services among public health facilities in pastoral communities in Ethiopia. Furthermore, we hope the results could significantly help policymakers and stakeholders by providing pertinent information that could guide them to improve the quality of adolescent-friendly health services.
Research question: Does the leadership commitment influence the quality of adolescent-friendly sexual and reproductive Health Services within public Health facilities among pastoral districts of Guji Zone?
Methods and Materials
Study Settings and Participants
Focus Group Discussions
We purposefully selected two pastoral communities’ districts for the study. We chose Gorodola and Wadara districts because they are among the districts with poor utilization of adolescent-friendly sexual and reproductive health (AFSRH) services in the East Guji Zone. Moreover, the high proportion of the Adolescent population in these two districts is due to the high catchment area population in both Districts. We selected adolescents who had used friendly health services at health centers for at least six months as members of the focus group discussions (FGDs). Youth center representatives within the catchment area also participated in the FGDs. Each FGD had 8 to 12 participants.
In-Depth Interviews
We conducted in-depth interviews (IDIs) with informants who had direct experiences with adolescent-friendly health services, either as experts at different spans of health sector levels or as health care providers at health facilities. Higher-level IDI expertise and coordinators actively developed adolescent and youth health strategy documents and implemented the program. Moreover, they could provide pertinent information about the quality of adolescent-friendly sexual and reproductive health services. We recruited IDI participants from the Federal Ministry of Health (FMoH), Oromia Regional Health Bureau (ORHB), Zonal Health Department (ZHD), HC heads, and healthcare providers (HCPs) who had worked in FHS units for at least one year.
Study Design
The study employed a programmatic qualitative research design, utilizing IDIs and FGDs to assess the influence of leadership commitment on the quality of adolescent-friendly sexual and reproductive health services in the East Guji Zone, Ethiopia’s pastoral community. We selected both IDIs and FGD to assess pertinent information from both sides as policymakers or service providers (IDIs) and friendly sexual and reproductive health services users in public health facilities (Adolescents and youths).
Sampling and Recruitment
Sampling and recruitment involved a stratified purposive sampling technique. The study team included seven IDI informants, comprising FHS coordinators at the MoH, the FHS focal point at ORHB, the FHS focal point at GZHD, head of water HCs, head of Harekello HCs, and one healthcare provider (HCP) from each Wadara and Harekello. IDI recruitment aimed to encompass FHS program coordinators and experts at all levels of the healthcare sector in Ethiopia. They have direct experiences with adolescent-friendly health services either as experts in different spans of the health sector or practiced as health care providers at health facilities. For instance, the higher-level IDI coordinators directly exercised the development of adolescent and youth health strategy documents and program implementation. Six FGD sessions were organized separately for males, females, and mixed-gender adolescents aged 15–24. Participants for both IDIs and FGDs were selected based on their prior experience with the FHS program and their satisfaction with the inclusion criteria. We used a stratified purposive sampling technique to select IDI and FGD participants. Table 1 provides detailed information on the inclusion and exclusion criteria for the study.
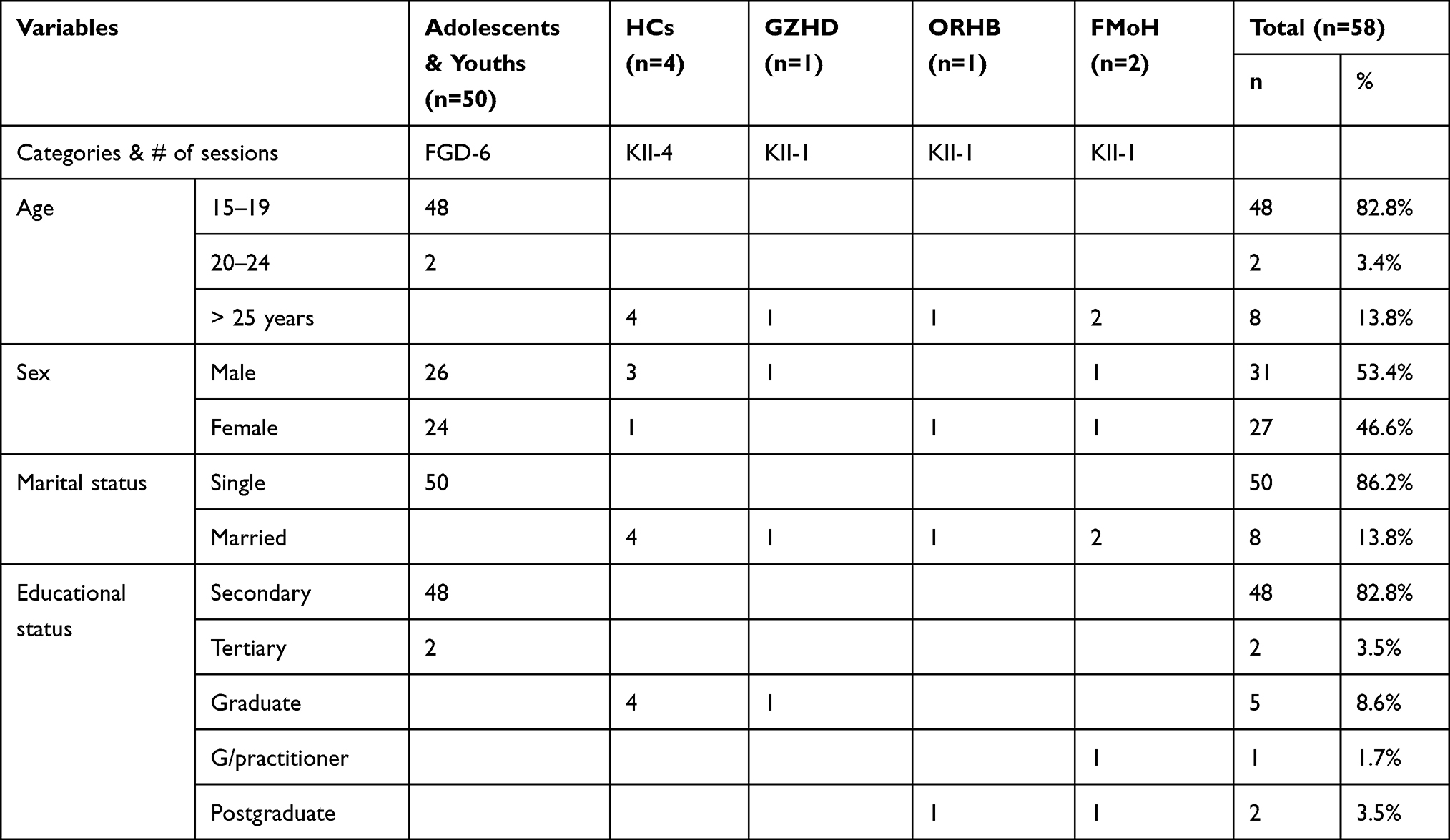 |
Table 1 Socio-Demographic Characteristics of Adolescents’ Friendly Health Services Quality, FGD & KII Participants, MoH, ORHB, GZHD & HCs, East Guji Zone, Ethiopia. Nov. 2021 |
Fieldwork Team Recruitment and Training
We recruited two qualitative research assistants and three facilitators. We recruited them based on their experience and skills in conducting qualitative research interviews. Two held a BA degree in social science, two had a BSc degree in natural sciences, and one facilitator was a first-year university student majoring in social science. The research assistants had substantial experience conducting qualitative research interviews and were proficient in the local language (Oromiifa).
We had an experienced supervisor with an MPH degree to oversee the research assistants and fieldwork activities. All research assistants attended a four-day training session covering the study’s background information, guidance tools, consent forms, and effective data collection methods through interviews. The principal investigator provided training to both the data collectors and facilitators.
IDI and FGD Guide
Open-ended semi-structured questionnaires with probes guided the key informants through in-depth interviews and focus group discussions (FGDs). We designed the question to prompt participants to respond directly or encourage them to offer related comments (eg, concerning provider attitudes toward adolescent FHS). We employed a set of 22 qualitative research guide questions centered on five critical areas of WHO quality of FHS care preference factors (availability, accessibility, acceptability, equitability, and appropriateness).18
Coding Book and Measurement
The study utilized Donabedian’s structure, process, and outcome model to guide the assessment of the quality of AFSRH services. We hypothesized that healthcare quality results from the interrelated effects of structure, process, and outcome.19 We applied this model to evaluate the Quality of adolescent FHS in the pastoral community of the Guji Zone. We considered five key areas of adolescent FHS quality: accessibility, equitability, acceptability, appropriateness, and effectiveness. We analyzed and measured the preference factors that influenced the Quality of adolescent FHS. The responses obtained from in-depth interviews and FGDs at all levels determined the level of FHS quality.
Structure
Structure is a broad category encompassing family codes such as accessibility, equitability, and organizational readiness. In essence, the structure represents the capacity of the healthcare sector, including health facilities and healthcare providers, to meet the needs for high-quality adolescent FHS. It involves establishing program support structures (leadership) at all levels of the healthcare sector, including directorates, case teams, focal persons, functioning FHS with established standards and resources, and equitable FHS provision.
Process
Process is another broad category that includes family codes such as availability, appropriateness, effectiveness, and provider readiness. It primarily addresses the various aspects of adolescents’ sexual and reproductive health service needs. It includes ensuring the availability of appropriate policies, effective planning, budgeting, reporting, monitoring, and evaluation, as well as evidence-based research and involving customers in the decision-making process. It also involves proper training, enhancing providers’ skills, delivering services tailored to specific needs, respecting medical ethics, and maintaining confidentiality.
Outcome
Outcome is a comprehensive category that encompasses family codes like acceptability. In general, outcome pertains to the observed effects of friendly health system activities, including changes in physical settings and adolescents’ functional and psychosocial status. It also considers factors such as trust and customer satisfaction. (See Figure 1)
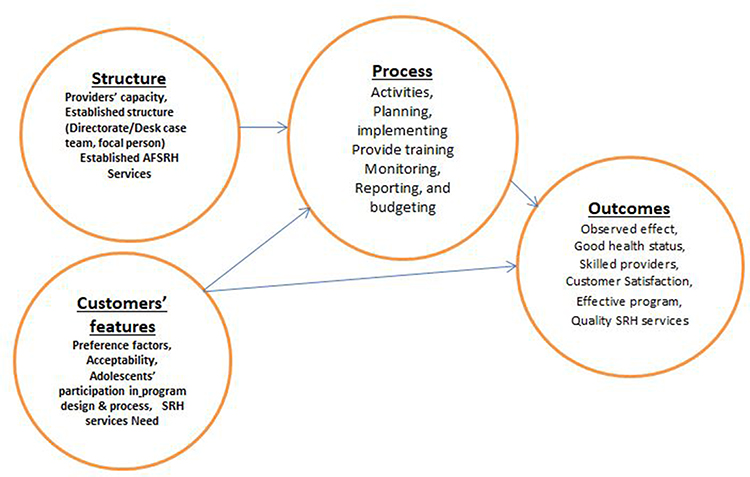 |
Figure 1 Sexual and reproductive health services quality Model adapted from Donabedian’s structure, process, and outcomes model. Wadara and Harekello Health centers, Guji zone, Ethiopia. November 2021. |
Site of Figure One
Data Collection and Management
The study tools were translated into the local language (Oromiiffa) and underwent pretesting to assess validity, reliability, clarity, sequence, consistency, and understandability during the data collection in October 2020. We conducted the pretest in Shakiso town and refined the tools based on the feedback received from the pretest assessment before proceeding with data collection.
To ensure transparency and informed participation, the team used recruitment scripts to explain the study’s purpose, procedures, and the rights of participants. We obtained oral consent from each IDI participant before conducting the interviews. We completed informed consent forms for adolescents aged 18–19 and mature minors. We obtained parental permission and assent for adolescents aged 15–17.
We collected data through IDIs and FGDs in a conducive environment. Organizers facilitated each FGD session, while interviewers led the IDIs and key informant interviews (KIIs). We took audio recordings and field notes during the data collection process. Supervisors communicated continuously with the research assistants (RAs) throughout the fieldwork activities.
Data Analysis
All research guide tools were developed in English and translated into the local language. They conducted all FGDs and IDIs in Oromifa, except for the IDIs at FMoH Ethiopia, in English. Audio files from IDIs and FGDs were transcribed directly from the data files of the language they had recorded. All the transcriptions in Oromiifa were re-checked to ensure the original meaning was maintained. We also used handwritten notes to supplement evidence gaps from the audio-recorded transcripts. We analyzed all 13 transcripts using Atlas.ti7 software for identifying, naming, conceptually categorizing, labeling, and describing the data. We analyzed the data in six thematic phases: 1) read and reread to become familiar with the data; 2) generate primary codes and group coded data; 3) probe for themes by organizing recorded codes into themes and assembly relevant codes to each theme; 4) review themes and create a map of the analyze; 5) define and name elegant themes; and 6) finally produced an analyze report as quoted in (Braun et al, 2006),20 we have established 30 primary codes through these processes and finalized 18 refined codes. The study subcategorized the refined codes into six sub-thematic areas. Finally, we analyzed six sub-thematic areas into three major thematic areas.
Results
Characteristics of Study Participants
We recruited 58 participants: the study recruited 25 FGD participants from Harekello and 25 from Wadara. The age of FGD participants ranged from 15 to 24, and they were all unmarried youths. Similarly, the age of all IDIs was greater than 25 years. Thus, 8 KII participated from MoH, ORHB, GZHD, Harekello, and Wadara Health Centers. Gender participants: Nearly 53% were male, and 47% were female. About 86.2% of participants were high school and university students, and 13.8% were graduate and postgraduate experts. Public health facilities within pastoral communities of the east Guji zone, South Ethiopia, organize these results. (See Table 1)
Major Findings
We conducted a total of 8 key informants’ in-depth interviews and six FGDs and presented the results based on the six key thematic areas that developed from QDA findings: 1) Organizational readiness, 2) Provider readiness, 3) Equitability; 4) leadership commitment; 5) Evidence-based services and 6) Acceptability of services by adolescents’ customers.
Organizational Readiness
The findings revealed that the quality of AFSRH services in East Guji Zone pastoral districts is substandard. Inaccessible surroundings describe customers needing to be more trusted due to poor confidentiality and less availability of supplies and goods. Likewise, most FGD Participant adolescents believe that friendly health services are unattractive and less accessible.
The Quality of the FHS system in the Oromia region is unsatisfactory. However, despite all the challenges, the customers who purposely visit health facilities were utilizing the service. We recommend providing it as an integrated setting rather than a separate one. (ORHB KII 2 Focal person)
Adolescents’ FHS performance in the beginning phase is excellent. However, due to lack of budget, poor follow up, and monitoring and feedback system, the status of current AYH at Guji zonal health department is the week (GZHD, KII Focal person)
An adolescent FHS in Harekello HC depends on partners. Whenever partners provide aid, we witness significant movement. However, after phasing out the project, FHS became distorted. We think MoH and ORHB should allocate budget line to achieve sustainable improvement of FHS (Harekello HC Head KII)
Previously, we have provided FHS; however, two years ago, we stopped separate FHS due to a lack of trained experts. We advertise and publicize FHS through different posters and banners in the HC… but we were not advertising outside of HC (Wadara HC Head KII)
I cannot claim that services for adolescents’ friendly reproductive health had delivered pleasantly. From observation, the program needed attention from the HC head and other authorities. Whether we submit activities report or not nobody had asked (Wadara HC, KII HCP-1)
As you see, the size of HC is minimal. Providers have mixed all services, shaming adolescents into using the services with the assumption that parents may see them (FGD-1, 3, male & female)
FHS is ideal and theoretical, rather than practical because nothing is tangible in our health center. However, we need real FHS for apt utilization of the services. (FGD 2&6 female & male)
The findings indicate that service standards were not adhered to in providing adolescents’ FHS. Furthermore, some providers have yet to learn the availability of FHS standards. On the other hand, we noticed that FHS standards still needed to be updated for 15 years.
As MoH Ethiopia, we had adopted eight youth FHS standards from the (WHO) and added one more standard convenient for our settings. (MoH/MCH Expert KII 1)
Adolescents and youth’s FHS standard is very explanatory, and can make it easier to run the programs. However, none of our health facilities have provided FHS as per the standards (ORHB Focal person KII)
According to adolescents & youth FHS criteria, services units could have at least two rooms, and those rooms should have a television and examination room. However, our HC could not fulfill any of these criteria. (Harekelo HC & HCP)
The study argued that FHS goods have no regular supplies and programmatic materials support from MoH, ORHB, or the Zonal Health Department. FHS is out of a run unless partners provide supplies and programmatic materials.
To tell you the truth, we did not receive regular supplies and programmatic material from MoH and did not provide for ZHD and HFs. Previously, some partners supported this program with specific supplies and materials. However, currently, we have not seen partners come with the related project (ORHB Focal person KII)
We have not provided supplies and programmatic materials for the FHS program for health facilities, as we did not have a specific budget for this program. (GZHD, KII Focal person)
We have not received any direct materials support from any sources. The health center has no specific budget for the program. Hence, we provided other programs condoms for FHS unit (Wdara and Harekello HC HCPs)
Although providers routinely prescribed supplies and drugs at FHS, nobody took them. So adolescents do not get the condoms when they need it (Harekello FGD 5 male)
The health sector needs to establish an adequate structure for all levels of adolescents and youth FHS programs. Thus, inadequate FHS program structure still leaves 42% of adolescents and youths in Ethiopia.
Previously, only the focal person had been assigned as an adolescent and youth FHS officer. The MOH has upgraded the FHS support structure to a case team. However, the case team can not satisfy the vast needs of nearly 42% of the adolescents and youth.8 So upgrading to an adolescent and youth-friendly health services directorate is better. (AYFHSD), (MoH/MCH Expert KII 1)
Only one focal person has been assigned to support the FHS program in ORHB. As we know, Oromia is the biggest region in Ethiopia. A focal person is not enough to facilitate FHS among all regional HFs. As to we, at least we have to have an FHS case team (ORHB Focal person KII)
I am not sure one focal person is enough to coordinate GZHD, as many HFs need our support … surely it is impossible to coordinate FHS at all HFs (GZHD, KII Focal person)
Providers’ Readiness
Almost all FGD participants agreed that they need to utilize adolescents’ and youths’ FHS, but providers are not ready to provide the services, as there is no accountability system.
If health care providers respect FHS customers, I am sure many adolescents would utilize FHS., But we are not provided service as per their needs (Wadara & Harekello HC HCPs)
As a user of these services, let me share with you my experiences. Healthcare providers are not ready to welcome customers in the right way. Even there are times when adolescents are troubled, as they joke on them (FGD 2&6 female & male)
Federal MoH Ethiopia claimed they had provided ToT training for most health facilities, ZHD, and RHBs. However, they determine if trained staff are on similar duties. Besides, some health center heads are not committed to coordinating the program.
Most HCPs who trained on FHS transferred to another position. So newly assigned experts to have need training. (GZHD, KII Focal person)
I know at the beginning of the program, focal persons and other staff had trained, but they shifted to other departments. We cannot assign staff to the FHS unit since no one has applied to the FHS unit. It is the staff’s right to shift to another work unit (Wadara KII HC Head)
Skilled HCPs have welcomed the customers and created trust among FHS utilizers. We, providers, should understand their psychology and keep it secret. However, we lack apt FHS skills. (Wadara HC KII HCP)
Most adolescents are interested in using FHS if skilled Health care providers provide it. But we are not lucky (FGD 4 & 6 female & male)
Most adolescent participants in FGDs mentioned that health workers have their own beliefs and values. However, they must respect their professional ethics and properly provide FHS regardless of their values. However, people do not respect HCPs for their professional morals.
I know HCPs have their beliefs and value system, but they have to respect professional morals & hence properly provide FHS despite of their values (Wadara FGD-6 male)
In my opinion, HCPs are not working according to the professional obligation. Most of the time, customers get angry and sad due to their poor handling (Harekello FGD-1 female)
The study’s outcome identified that adolescents needed restricted confidentiality while utilizing SRH services. However, the FHS setting environment could not be conducive to an acceptable level of privacy.
Adolescents want to do vis-à-vis sexuality secretly….and come to the health center in the late evening to request for condoms and emergency pills (Harekello HC KII HCP)
I think adolescents want to keep their secret…. For me, it is impossible in this HC since there was only one room for the services (Harekello FGD-3 male & female)
Equitable
The study results showed that adolescent and youth Friendly Health Services are not equitable among regions, zones, and health facilities, nor the male and female customers.
The readiness for FHS among regions and City administration is inequitable For instance, Addis Abeba and Dire Dawa achieved >85% staff training. Yet Oromia and Somali regions have achieved only 30% to 35 % (MoH/MCH Expert KII 1)
Some zones have special support from partners, and others are not. So, service readiness, staff training, and achievement among FHS are not uniform (ORHB KII Focal)
I do not think the unmarried adolescent girl has visited FHS as male…. Since HCPs negative attitudes have shamed her. Thus she visits illegal private HFs (Wadara FGD-2 female)
Leadership Commitment
Evidence has shown that MoH has been given reasonable attention to strengthening friendly health services at the policy level. However, the leadership commitment at the Oromia Regional Health Bureau, Guji Zonal Health Department, and Wadara and Harekello Health Centers heads has influenced the quality of adolescent-friendly sexual and reproductive Health Services within public Health facilities among pastoral districts of Guji Zone. Moreover, there is no accountability system at all levels of the health sector.
As you know, as a health leadership commitment, Ethiopia has launched a youth FHS national strategy. As part of this, we also developed a national adolescents and youth strategy for 2016-2020. Additionally, MoH had developed a guideline for health extension workers (MoH/MCH Expert KII 1)
Some interested HCPs were going the extra mile to improve FHS, but there is no reward system for encouragement for the excellent performers. Thus, the MoH and Oromia Regional Health Bureau leadership has to establish a rewards and accountability system. (GZHD, KII Focal person)
The finding identified that there were no harmonized plans for youths-friendly health services programs except for adolescents and youth FHS case team and individual plans at MoH
Yes, as an expert of the FHS case team, I have an individual annual plan, but we do not have an appropriate plan at the Regional and Zonal health departments. (MoH/MCH Expert KII 1.
We have RH annual plan, but not have separate youths FHS plan (ORHB KII Focal)
We have no specific plan for adolescents FHS, except the PHCU plan that is not specific to most FHS activities. (GZHD, KII, Harekello & Wadara HC heads)
Adolescent and youth FHS programs have severe budget deficits; thus, they can only be implemented if the budget supports interested partners’ FHS program activities. One of the significant health sector leadership roles has assigned an adequate budget for adolescent-friendly sexual and reproductive health services activities. However, almost all IDIs claimed that the leadership at all levels did not allocate an adequate budget for friendly health service programs.
As I said, budget is the biggest problem every time. While we get a small amount of budget from SDG, it is too small, about 20% of the needed budget (MoH/MCH Expert KII 1)
No, I mean adolescents and youth FHS have not any budget, so we cannot even provide an orientation to health extensions workers (ORHB KII Focal)
We have seen FHS program have good movement when partners come with projects but shut down immediately when the NGO project has phase-out (GZHD KII Focal-1)
The government has not allocated budget for FHS, except staff salary. We used other program budgets & supplies for FHS (Wadara & Harekello HC Heads)
Federal MoH had targeted supervision at RHB, Woreda, youth centers, and industrial parks. However, ORHB did not conduct either supervision or a Monitoring and Evaluation program, as they have no specific budget for the FHS program.
We do have targeted supervision, to check FHS services against the standards…. we visit regions, zones, youth center, and industrial park. (MoH/MCH Expert KII 1)
We do not have supervised zones and health facilities due to lack of budget…. we simply communicate ZHD via telephone (ORHB KII Focal)
We identified that there needed to be an organized system for collecting adolescent FHS reports. MoH, ORHB, and GZHD have collected a few activity reports on adolescents’ ages. Most facilities have not reported adolescent and youth health (AYH) services. A system shall create a reporting system for FHS activities.
We have not received direct FHS reports from Regions; instead, we gather data elements from DHIC and send them to another program for adolescent age groups. The DHIC data element did not include the report for adolescents’ FHS. (MoH/MCH Expert KII 1)
There is not a regular submission of FHS performance report. To improve the program, MoH should include FHS Activities report in DHIC (ORHB KII Focal)
We are not submitting regular FHS-specific reports. An accountability and feedback system must ensure the submission of the report. However, some responsible health facilities submitted the report. (GZHD KII Focal-1)
Our health center did not submit regular reports to GZHD, as they do not ask for FHS Performance reports. (Wadara HC Head KII-1)
Evidence-Based Services
Experts at the national level believe that young people have participated in designing adolescent and youth FHS programs. However, participants from the youth center in the FGD claimed that neither Guji Zonal Health Department nor Health centers had invited them to Friendly Health Services for program design or planning activities.
We invited youths on FHS national programs……they had participated in the program design, and provided feedback in the ongoing program (MoH/MCH Expert KII-1)
The invitations have been expected either from GZHD or health center. However, as a youth center, we have not had such information almost for the last two years. (Wadara FGD 4 Female and male)
Adolescents and youth FHS in Ethiopia have considerable evidence gaps, particularly in service quality, demand, and gaps. Evidence data will be needed to improve the program.
As program coordinators, we need evidence to develop strategic planning or improve the program, but there is no adequate evidence on FHS. So if interested researchers will conduct specific research on FHS in Ethiopia. (MoH/MCH Expert KII 2)
Acceptability of Friendly Health Services
Adolescents and youth are not trusted FHS providers; they must welcome them when they visit health centers for service utilization. Moreover, Adolescents do not trust healthcare providers due to the uncertainty of confidentiality.
I experienced that when your approach is friendly adolescents want to know everything, about sexuality and RH issues. But HCPs are not welcoming them (Wadara HCP, KII-1)
I do not think a married woman would come to visit FHS in this health center….as they have poor trust in health care providers for their privacy issues (Wadara FGD-2 female)
The finding assured that SRH service utilizers were mainly unsatisfied due to poor hospitality at FHS units. They choose illegal private health facilities rather than friendly health services.
No, let alone satisfied by FHS, adolescents get angry and stop using FHS at HC and shift to visit dishonest private health facilities. (Harekello FGD 3 male & female)
I think the way HCPs give you the service has not given you a comfort…. I do not think they are giving the service as their professional morals, rather they did as an obligation to have their salary (Wadara FGD-5 male)
Discussion
This research aimed to discover the influence of leadership commitment on the quality of adolescent-friendly sexual and reproductive health services among health facilities in the pastoral community of the east Guji zone. We found barriers at all six vital thematic areas facilitating factors: 1) Organizational readiness, 2) Provider readiness, 3) Equitability, 4) leadership commitment, 5) Evidence-based services, and 6) service acceptability. Our findings indicated that the quality of adolescent-friendly health services and leadership commitment in pastoral communities of the east Guji Zone was substandard—these outcomes concomitant with Homer et al (2018) and Chandra-Mouli et al. Tanzania (2013) and Olijira L. Ethiopia (2016), which discussed adolescents’ healthcare quality, were undermined due to lack of availability, accessibility, poor infrastructure, and inadequate regulation.12,21,22 However, this finding differed from Hoopoes et al ‘s India (2016) Pilgrim et al USA (2019), and a study in Mexico showed improvement in service quality as 86.1% of adolescents had received medium to high-quality adolescent FHS.1,23,24
The critical barriers to organizational readiness thematic area identified that FHS in the east Guji zone was inaccessible to adolescents due to a lack of supplies and goods, poor knowledge of service standards, and lack of adequate leadership structure for FHS programs at all levels of the health sector. These outcomes are associated with Ngwenya S. Zimbabwe (2016) and Mazur et al systematic review (2018), which discussed difficulties of accessing contraception and other FHS, unspecific services to adolescents’ needs and often reflected basic FHS standards.25–27 However, this finding was not related to Bukenya et al Uganda (2018) and Andersen et al Nepal (2015) reported sufficient supplies and good accessibility of essential RH services among health facilities.28,29
The critical barriers in the provider’s readiness thematic area identified that HCPs were not ready for the FHS due to a lack of training or shift of trained staff to other positions, poor confidentiality, and being highly influenced by their beliefs and values systems rather than respecting professional morals. These outcomes are associated with Godia et al Kenya (2013), Jonas et al Sub-Saharan Africa (2017), and Jonas et al. South Africa (2018), Kennedy et al Vanuatu (2013) discussed that HCPs have a lack of training, negative attitudes, and being torn between personal feelings, cultural, religious values, and beliefs.13,30–33 However, this finding is not in line with Z Esseck et al. KwaZulu-Natal. SA (2016) discussed that many providers felt they could uphold their professional rather than personal outlooks.34
The critical barriers to service equitability thematic area identified that adolescents and youth FHS provision were inequitable among regions, zones, health facilities, and male and female customers. This finding is in line with Godia et al. Kenya (2014), India (2015), Thin Zaw et al. Myanmar (2013) and IPPF & UNFPA (2017) reported no equitability of FHS programs among rural and urban males and females. Similarly, FHS programs are designed for women and children and are often not seen as male and adolescent girls.35–38
The key barriers of leadership commitment thematic area identified that FHS needed to be properly available for adolescents as there were no harmonized plans at the facility level due to a lack of budget and unavailability of regular reporting and program evaluation, except for few activities at MoH/MCHD level that demonstrated fairly good commitment to strengthening the FHS program, which includes conducted targeted supervision. They collected reports from adolescents’ age groups sent for other purposes. The finding was in line with ODO et al. Nigeria (2018) and C Sivagurunathan et al. Inda (2015) revealed severe limitations in healthcare services for adolescents.39,40 However, the findings differ from Rebecca S. Geary et al, South Africa (2015) and Huaynoca et al. Colombia (2015) discussed that solid M & E of SRHS could enable HCPs to address adolescents’ needs.41–43
We found critical barriers to evidence-based services. The thematic area identified that adolescent FHS could have been more appropriate and effective as there were no evidence-based services due to inadequate research on FHS quality in Ethiopia. Moreover, youth participated in the design of FHS programs at the national level. Mulugeta et al in Ethiopia (2019) reported that a lack of research evidence prevented the discovery of youth-friendly service quality in southern Ethiopia. Thus, more research and documentation for involving youth in SRH programs are needed.15,44
We also found critical barriers to services in the acceptability thematic area and identified that adolescents did not trust/accept FHS providers, as providers did not welcome the customers. Consequently, adolescents are not satisfied with FHS units. These outcomes are related to Godia et al. Kenya (2014) stated that male adolescents feel uncomfortable seeking FHS.45 On the other hand, our finding was not in line with Tangut D et al ‘s. Ethiopia (2015), Pilgrim et al. Atlanta GA (2018), and Schmidt et al. Germany (2016) discussed that the majority of adolescents were delighted with the timely care of FHS.10,24,46
In summary, we conclude that poor commitment to leadership inhibits the quality of adolescents’ friendly sexual and reproductive health services among public health facilities in the pastoral community of Guji zone, south Ethiopia. Therefore, the study has clear policy implications. Thus, Ethiopia is one of the sub-Saharan African countries among the leading causes of adolescent mortality in the world.47 The National Adolescents and Youth Health Strategy (2016–2020) also includes minimum health goals to be achieved by 2020 for reducing mortality and morbidity by 50%, Reducing pregnancy-related deaths by 50%, and Reducing HIV incidence by 75% as a top priority.47,48 These goals need more leadership commitment to maximize the accessibility of quality sexual and reproductive health services. According to the recent Adolescent and youth health strategy and the SDG-3 target 3.7, Ethiopia continues to reduce adolescent morbidity and mortality by providing high-quality and equitable adolescent and youth-friendly health services.45,49 The minimum Adolescent and youth Health strategy Goals and SDG targets indicate that extra work needs to be done to improve adolescent services utilization. Hence, improving the quality of friendly health services in public health facilities is critical for improving adolescent service utilization. We hope this article has potential policy implications that contribute to improving the quality of friendly health services within public health facilities.
Strength and Limitations
Our study had several strengths. We gained detailed information from in-depth insights into the practices of critical informants among MoH, ORHB, GZHD, HCs, and the head of expertise in the adolescents and youths FHS program. Moreover, a mixture of several respondents provided critical information on the Quality of AFSRH services. In addition, we selected Harekello and Wadara health centers because both health centers have implemented adolescents’ and youths’ FHS and have a high catchment area of the adolescent population in the pastoral districts of Guji Zone.
On the other hand, the study has some limitations, including the selection criteria for study participants being purposeful and FGD participants not having rich information about the FHS in the health facilities. Both factors may have contributed to information bias.
Conclusions and Recommendations
The quality of adolescent and youth-friendly SRH services among public health facilities in pastoral areas of the east Guji Zone was substandard. The quality of adolescent-friendly services was poor due to a lack of commitment to the health sector’s leadership role in ensuring service quality. All other thematic areas contributed to the poor quality of friendly health services within public health facilities among pastoral communities, directly or indirectly associated with poor leadership commitment. Therefore, we firmly believe four significant recommendations will improve the quality of adolescents-friendly health services in pastoral communities: First, ensure accessibility through improving organizational and provider readiness. Second, ensure availability via demonstrating leadership commitment through allocating an adequate budget and strengthening the M&E system. Third, implement the FHS program in all Regions, Zones, and Health Facilities to ensure equity. Fourth, we strongly suggest redesigning adolescents’ FHS as an integrated approach setting called “Maternal, Children, and Adolescence FHS.” Hence, MoH, RHB, interested researchers, and health facilities could consider these recommendations to improve the quality of adolescent-friendly health services in pastoral communities of Ethiopia.
Abbreviation
AAA, Availability, Accessibility, Acceptability, and Quality of care; AFHS, Adolescent Friendly Health Services; AFSRH, Adolescent Friendly Sexual and Reproductive Health; AYFH, Adolescent and Youth Friendly Health; DHIS, District health information system; EDHS, Ethiopian Demographic and Health Survey; FGD, Focus Group Discussion; FHS, Friendly Health Services; GZHD, Guji Zonal Health Department; HC, Health Center; HCP, Health Care Providers; HEW, Health Extension Workers; ICPD, International Conference on Population Development; IDI, In-Depth Interview; KII, Key Informant Interview; MCHD, Maternal and Child Health Directorate; MoH, Ministry of Health; PHCU, primary health care unit; QDA, Qualitative data analysis; RHB, Regional Health Bureau; RA Research assistance; ZHD, Zonal Health Department.
Data Sharing Statement
Original transcripts of the study are available (in Oromiiffa and English) from the corresponding author upon request.
Ethical Consideration
We obtained ethical clearance from Jimma University (Ref.No IHRPCA/721/202, date 17/08/2020) and the Bureau of Regional Health, Oromia (Lakk/Ref No BEFO/MBTF/2081, date 27/01/2013, ETC. or 07/10/2020). Earlier in the in-depth interview and FGD, all study participants gave verbal informed consent. We completed the qualitative data collection in November 2020. We confirmed that our study complies with the Declaration of Helsinki, and participants’ and parents’ informed consent included the publication of the anonymized responses.
Acknowledgment
As authors, we would like to thank the Population and Family Health Department, and faculty of public health, Jimma University, as well as the MoH of Ethiopia, for sponsoring our expenses and data collectors costs and last but not least, lovely family members for their particular assistance to the progress of the manuscript.
Funding
The research received only minimal Ph.D. students’ funds from Jimma University for data collection and related costs.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Villalobos A, Rojas-Martínez R, De Castro F, et al. Quality of reproductive healthcare for adolescents: a nationally representative survey of providers in Mexico. PLoS One. 2017;12(3):e0173342. doi:10.1371/journal.pone.0173342
2. The O, Sustainable T, Goals D, Nqps T. National Quality Policy And Strategy: driving Change For Stronger Health Systems And Improved Health Outcomes. 2018.
3. UN. The 2030 Agenda and the Sustainable Development Goals: An Opportunity for Latin America and the Caribbean. Thank You for Your Interest in This ECLAC Publication; 2018.
4. WHO. Quality Improvement in Primary Health Care; 2004.
5. Upadhyai R, Jain AK, Studies E, Roy H, Studies E. A Review of Healthcare Service Quality Dimensions and their AReview of Healthcare Service Quality Dimensions and their Measurement. Journal of Health Management. 2019;21(1):102–127. doi:10.1177/0972063418822583
6. Brief P. POLICY BRIEF A standards-driven approach to improve the quality of healthcare services for adolescents. 2015;1–4.
7. Germain BA ICPD Beyond 2014.
8. MoH. Mini Demographic and Health Survey, Ethiopia; 2019.
9. Gebrie M, Asrade G, Tsehay CT, Yazachew L, Id ED. Quality of AdolescentAdolescent and youth-friendly health services in Dehana district public health facilities, northeast Ethiopia: using the Donabedian quality framework. PLoS One. 2021;1–19.
10. Dagnew T, Tessema F, Hiko D. Original Article Health And Reported Satisfaction Among Adolescents In Dejen District, Ethiopia: a Cross-Sectional Study. Ethiopian Journal of Health Sciences. 2015;25(1):17–28. doi:10.4314/ejhs.v25i1.4
11. WHO. Making Health Services Adolescent-Friendly; 2012.
12. Chandra-mouli V, Mapella E, John T, et al. Standardizing and scaling up quality adolescent-friendly health services in Tanzania. BMC Public Health. 2013;13(1):1. doi:10.1186/1471-2458-13-579
13. Godia PM, Olenja JM, Lavussa JA, Quinney D, Hofman JJ, Van Den Broek N. Sexual reproductive health service provision to young people in Kenya; Health service providers’ experiences. BMC Health Serv Res. 2013;13(1). doi:10.1186/1472-6963-13-476
14. James S, Pisa PT, Imrie J, et al. Assessment of adolescent and youth-friendly services in primary healthcare facilities in two provinces in South Africa. BMC Health Serv Res. 2018;18(1):1–10. doi:10.1186/s12913-018-3623-7
15. Mulugeta B, Girma M, Kejela G, Meskel FG, Andarge E, Zerihun E. Assessment of Youth-Friendly Service Quality and Associated Factors at Public Health Facilities in Southern Ethiopia: a Facility-Based Cross-Sectional Study. BioMed Research International. 2019;2019. doi:10.1155/2019/9696278
16. Yonas FB, Chernet AA. Sexual and reproductive health service utilization and associated factors among high school learners in the Dawuro zone, Southwest Ethiopia Study area and period. African Journal of Reproductive Health. 2022;26(September):48–54. doi:10.29063/ajrh2022/v26i9.5
17. Zenebe GA, Ewunie TM, Belay MM, Abose AM. Quality of AdolescentAdolescent and youth-friendly sexual and reproductive health services and associated factors in Ethiopia: a systematic review and. Front Public Health. 2023;11:1191676.
18. World Bank, WHO, OECD. Delivering Quality Health Services: A Global Emprative for Universal Health Coverage. 2018.
19. NHS. A Model for Measuring Quality Care; 2005.
20. Francis T. Qualitative data analysis. London: Taylor and Francis; 2005.
21. Homer CSE, Lopes SC, Nove A, et al. Barriers to and strategies for addressing the availability, accessibility, acceptability, and quality of the sexual, reproductive, maternal, newborn and adolescent health workforce: addressing the post-2015 agenda. BMC. 2018;1–11.
22. Oljira L. National Adolescent and Youth Health Strategy (2016-2020) Federal Democratic Republic of Ethiopia Health Ministry. 2020.
23. Hoopes AJ, Agarwal P, Bull S, Chandra-Mouli V. Measuring adolescent-friendly health services in India: a scoping review of evaluations. Reprod Health. 2016;13(1):1–8. doi:10.1186/s12978-016-0251-8
24. Pilgrim N, Jennings JM, Sanders R. Understanding Quality of Care and Satisfaction with Sexual and Reproductive Health Care among Young Men. J Healthcare Quality. 2019;40(6):354–365.
25. Mazur A, Brindis CD, Decker MJ. Assessing youth-friendly sexual and reproductive health services: a systematic review. BMC Health Serv Res. 2018;18(1):1–12. doi:10.1186/s12913-018-2982-4
26. Care A. STI Services for Adolescents and Youth in Low and Middle-Income Countries: perceived and Experienced Barriers to Accessing Care. J Adolesc Health. 2017;59(1):7–16.
27. Ngwenya S. Communication of reproductive health information to the rural girl child in Filabusi. Zimbabwe. 2016;16(2):451–461.
28. Andersen KL, Khanal RC, Teixeira A, et al. Marital status and abortion among young women in Rupandehi. Nepal. 2015;1–9.
29. Bukenya JN, Mulogo E, Kibira SPS, Muhumuza C, Atuyambe LM. Health facilities’ readiness to provide friendly reproductive health services to young people aged 10-24 years in Wakiso district. Uganda. 2018;2(3):56.
30. Jonas K, Crutzen R, Borne B, Van D, Reddy P. Healthcare workers’ behaviors and personal determinants associated with providing adequate sexual and reproductive healthcare services in sub-Saharan Africa: a systematic review, BMC Pregnancy Childbirth. 2017;1–19.
31. Jonas K, Crutzen R, Krumeich A, et al. Healthcare workers ‘beliefs, motivations and behaviors affecting adequate provision of sexual and reproductive healthcare services to adolescents in Cape Town, South Africa: a qualitative study. BMC Health Services Res. 2018;1–13.
32. Mulaudzi M, Dlamini BN, Coetzee J, Sikkema K, Gray G, Dietrich JJ. Perceptions of counselors and youth-serving professionals about sexual and reproductive health services for adolescents in Soweto. South Africa. 2018;1–9.
33. Kennedy EC, Bulu S, Harris J, Humphreys D, Malverus J, Gray NJ. “Be kind to young people so they feel at home”: a qualitative study of adolescents’ and service providers’ perceptions of youth-friendly sexual and reproductive health services in Vanuatu. BMC Health Serv Res. 2013;13(1):1. doi:10.1186/1472-6963-13-455
34. Essack Z, Toohey J, Strode A. Reflecting on adolescents ‘evolving sexual and reproductive health rights: canvassing the opinion of social workers in KwaZulu-Natal, South Africa rights: canvassing the opinion of social workers in KwaZulu-Natal. RHM. 2016;24(47):195–204. doi:10.1016/j.rhm.2016.06.005
35. Godia PM, Olenja JM, Hofman JJ, Van Den Broek N. Young people’s perception of sexual and reproductive health services in Kenya. BMC Health Serv Res. 2014;14(1). doi:10.1186/1472-6963-14-172
36. Gupta M, Bhatnagar N, Bahugana P. Inequity in awareness and utilization of adolescent reproductive and sexual health services in the union territory, Chandigarh, North India. Indian J Public Health. 2015;59(1):9. doi:10.4103/0019-557X.152846
37. I& UNFPA. Global Sexual and Reproductive Health Service Package for male and Adolescent boys; 2017.
38. Phyu P, Zaw T, Liabsuetrakul T, Mcneil E, Htay TT. Gender differences in exposure to SRH information and risky sexual debut among poor Myanmar youths. BMC Public Health. 2013;1–9.
39. Odo AN, Samuel ES, Nwagu EN, Nnamani PO, Atama CS. Sexual and reproductive health services (SRHS) for adolescents in Enugu state, Nigeria: a mixed methods approach. BMC Health Services Res. 2018;1–12.
40. Article R, Sivagurunathan C, Umadevi R, Rama R, Gopalakrishnan S. Adolescent Health: present Status and Its Related Programmes in India. Are We in the Right Direction. 2015;9(3):565.
41. Mchome Z, Richards E, Nnko S, Dusabe J, Mapella E, Obasi A. A “mystery client” evaluation of adolescent sexual and reproductive health services in health facilities from two regions in Tanzania. PLoS One. 2015;10(3):1–11. doi:10.1371/journal.pone.0120822
42. Geary RS, Webb EL, Clarke L, Norris SA. Evaluating youth-friendly health services: young people’s perspectives from a simulated client study in urban South Africa. BMC Health Services Res. 2015;1:1–9.
43. Huaynoca S, Svanemyr J, Chandra-mouli VC, Jeaneth D, Lopez M. Documenting good practices: scaling up the youth-friendly health service model in Colombia. Reprod Health. 2015;12:1–13. doi:10.1186/1742-4755-12-1
44. Villa-torres L, H MSP, Svanemyr J, Ph D. Ensuring Youth’s Right to Participation and Promotion of Youth Leadership in the Development of Sexual and Reproductive Health Policies and Programs. J Adolesc Heal. 2015;56(1):S51–S57. doi:10.1016/j.jadohealth.2014.07.022
45. Godia PM, Olenja JM, Hofman JJ, Van Den BN. Young people’s perception of sexual and reproductive health services in Kenya. BMC Health Services Research. 2014;14(1):56.
46. Schmidt S, Thyen U, Herrmann-garitz C, Bomba F, Muehlan H. The Youth Health Care Measure- satisfaction, utilization, and Needs (YHC- SUN) -is developing a self-report version of Child Health Care (CHC-SUN). BMC Health Serv Res. 2016;16:1–12. doi:10.1186/s12913-015-1254-9
47. Bill F, Foundation MG. Global, regional, and national mortality among young people aged 10 – 24, 1950 – 2019: a systematic analysis for the Global Burden of Disease Study 2019. BMC Health Services Res. 2021;1593–1618.
48. MoHE. National Adolescent and Youth Health Strategy (2016-2020); 2020.
49. FMoH. National Adolescent and Youth Health Strategy; 2016.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.