")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 14
Krait envenomation in Thailand
Authors Tongpoo A, Sriapha C , Pradoo A , Udomsubpayakul U , Srisuma S , Wananukul W , Trakulsrichai S
Received 28 March 2018
Accepted for publication 30 May 2018
Published 13 September 2018 Volume 2018:14 Pages 1711—1717
DOI https://doi.org/10.2147/TCRM.S169581
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Garry Walsh
Achara Tongpoo,1 Charuwan Sriapha,1 Aimon Pradoo,1 Umaporn Udomsubpayakul,2 Sahaphume Srisuma,1,3 Winai Wananukul,1,3 Satariya Trakulsrichai1,4
1Ramthibodi Poison Center, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand; 2Section for Clinical Epidemiology and Biostatistics, Research Center, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand; 3Department of Medicine, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand; 4Department of Emergency Medicine, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand
Purpose: Three species in the genus Bungarus inhabit Thailand. Among these, Bungarus candidus (Malayan krait) is the most common and deadliest. Currently, the clinical manifestations of patients envenomed by kraits, especially Bungarus fasciatus (banded krait), have not been thoroughly investigated. This study was performed to elucidate the clinical manifestations and outcomes of patients bitten by kraits in Thailand.
Materials and methods: The data of krait envenomation cases that occurred during a 9-year period were obtained from the Ramathibodi Poison Center Toxic Exposure Surveillance System and retrospectively analyzed.
Results: In total, 78 cases of krait envenomation were included. Most patients were male (59.0%) and the median age was 28 years. All had minimal local effects. The median duration from the bite to the onset of neurological manifestations was 3 hours (range, 0.5–8 hours). Besides neurological effects, the patients also developed high blood pressure (67.4%), tachycardia (61.7%), hypokalemia (55.3%), and hyponatremia (17.6%). Severe hyponatremia (<120 mEq/L) was noted in four pediatric patients. Other clinical manifestations were bradycardia, abdominal pain, and rhabdomyolysis. The mortality rate was 6.4%, and all deaths occurred from B. candidus bites. Eighty-six percent of patients received antivenom. Most patients (75.6%) were intubated and underwent assisted ventilation for a median of 6 days (range, 1–37 days). The median length of hospital stay was 7 days. Some patients developed complications during hospitalization; the most common was pneumonia. These in-hospital complications were significantly associated with death.
Conclusion: Although krait bites caused only minimal local effects, the mortality rate was still high, particularly from Malayan krait bites. Besides neurological effects, other clinical manifestations were high blood pressure, tachycardia, hypokalemia, and hyponatremia. Thus, vital signs and electrolytes should be frequently and closely monitored in these patients. Apart from antivenom treatment, adequate supportive care including management of complications might help to decrease the mortality rate.
Keywords: snake bite, Bungarus, Malayan krait, banded krait, clinical manifestation, outcome
Introduction
Snakebite is an important public health problem in tropical and subtropical regions.1 Southeast Asia contains numerous species of elapid snakes, the genus Bungarus or kraits are among these species.2 Three species in the genus Bungarus inhabit Thailand, including Bungarus candidus (Malayan krait), Bungarus fasciatus (banded krait), and Bungarus flaviceps (red-headed krait).2,3 Among these, B. candidus accounts for a large number of bites and is associated with the highest mortality rate.2,4
Krait venom contains neurotoxins that mainly act at both the presynaptic and postsynaptic neuromuscular junction,5–7 resulting in failure of neuromuscular transmission, depletion of synaptic vesicles, and damage to the nerve terminal.8–11 Clinically, neurotoxicity is the most common and significant clinical manifestation of krait envenomation and is frequently characterized by a prolonged period of paralysis.12,13 Extra-neurological manifestations, such as electrolyte abnormalities, rhabdomyolysis, autonomic dysfunction, and cardiovascular effects, have also been reported in envenomed patients.13–20
The mainstay of treatment for krait envenomation is administration of specific antivenom and sufficient supportive care, including efficient ventilation.13,21 In Thailand, the mortality rate associated with the Malayan krait bite was quite high before the availability of the specific antivenom.22 However, Malayan krait monovalent antivenom is currently available nationwide.13,21
Although studies and case reports of many species of krait envenomation are continuously increasing in number, the clinical manifestations and outcomes of patients envenomed by the Malayan krait, banded krait, and red-headed krait have not been well described in Thailand. Additionally, studies of banded krait envenomation are rather scarce and still limited in Southeast Asia. Therefore, this study might provide insight into and support the current clinical data regarding krait envenomation by these three species.
Materials and methods
Study design
We performed a 9-year retrospective study of all cases of krait bites recorded in the Ramathibodi Poison Center (RPC) Toxic Exposure Surveillance System from 2008 to 2016. The primary outcomes of this study were the clinical characteristics and outcomes of all patients.
This study was approved by the Institutional Ethics Committee Board of Ramathibodi Hospital Faculty of Medicine, Mahidol University (ID 04-58-53). Due to the retrospective nature of the study design and because we used the preexisting, confidential poison center database, patient consent was not required by our hospital’s Ethics Committee Board. The results of the study were anonymized before reporting.
Study setting and population
The study setting was the RPC of a tertiary teaching hospital that was involved mostly in consultations by medical personnel from every region in Thailand (~15,000–20,000 consultations/year). All patients with krait bites who consulted with the RPC were included in the study. The type of snake was determined by the snake’s carcass, a description of the snake’s characteristics by the patients, or pictures of snakes that were sent to the RPC’s application line for snake identification. When the snakes were not seen, the diagnosis and type of snake was established by the patient’s history, the area of distribution and habitat of the snakes, and the patient’s local and systemic clinical manifestations.
Study protocol
We collected each patient’s demographic data, medical history, laboratory findings, treatment modalities, follow-up details, final diagnosis, and outcome.
Abnormal vital signs, including bradycardia and hypertension, were defined by the patient’s age range.23 Hypokalemia was defined as a serum potassium concentration of <3.5 mmol/L, and hyponatremia was defined as a serum sodium concentration of <135 mmol/L. Acute kidney injury was diagnosed based on the patient’s clinical history and laboratory data using the Kidney Disease: Improving Global Outcomes (KDIGO) clinical practice guidelines.24 We assumed that all patients without known underlying disease were healthy and had normal kidney function before the snake bite. Rhabdomyolysis was diagnosed when serum creatine phosphokinase level was >1,000 U/L25 or was diagnosed by the attending physicians.
The seasonality of the snakebites was also assessed. The seasons in Thailand are simply classified by three equal 4-month periods: the rainy season (June–September), winter (October–January), and summer (February–May).26
We used PASW Statistics for Windows, Version 18 (SPSS Inc., Chicago, IL, USA) to analyze the data. Mean, median, minimum, maximum, and SD were analyzed for continuous data, and frequency and percentage were analyzed for categorical data. Between-group comparisons were performed by Student’s t-test if the data were normally distributed and by the Mann–Whitney U test otherwise. Differences in categorical variables were evaluated by chi-squared analysis and Fisher’s exact test. A P-value of <0.05 was considered statistically significant.
Results
During the study period, 78 cases of krait envenomation were assessed. Most were Malayan krait bites (n=68), followed by banded krait bites (n=9), and a red-headed krait bite (n=1). Most patients were bitten during the rainy season. With respect to the geographical distribution of krait envenomation, the northeastern region accounted for the largest percentage (70.5%), followed by the central, eastern, and southern regions (9.0% each). One patient was bitten in the northern region and one in the western region. No patients were bitten in Bangkok.
The patients’ demographic data and characteristics are shown in Table 1. Most patients were male, and the median age was 28 years; the youngest patient was only 1 year old. Most patients were bitten outdoors and during the night. Fang marks could not be identified in some patients. The extremities were the most common site of bites (93.6%); among these, 47.4% of all patients were bitten in the upper extremities, whereas 46.2% were bitten in the lower extremities. All patients with obviously visible fang marks had minimal local effects associated with their wounds. The patients did not mention that the bite wound was painful. Sixty-nine patients (88.5%) developed neurological signs and symptoms. All patients were admitted to the hospital.
 | Table 1 Demographic data and characteristics of studied patients |
Apart from neurological effects following krait bites, several other systemic clinical manifestations (extra-neurological effects) were described (Table 2). High blood pressure (67.4%), tachycardia (61.7%), hypokalemia (55.3%), and hyponatremia (17.6%) were the main extra-neurological effects reported in our study. The two other clinical manifestations, bradycardia and abdominal pain, each occurred in <10% of all patients. Rhabdomyolysis occurred in all seven patients who underwent serum creatine phosphokinase measurement. Hypokalemia was more common than hyponatremia, but no patients with banded krait envenomation developed hypokalemia or hyponatremia. High blood pressure and tachycardia (n=3) were the only extra-neurological clinical manifestations in patients with banded krait bites. Severe hyponatremia (≤120 mEq/L) was noted in four pediatric patients (6–9 years of age). Two of these four patients developed seizures after severe hyponatremia. Two patients were siblings and were bitten by the same Malayan krait snake. Both of them had hyponatremia. During investigation of the cause of the hyponatremia, both patients’ urine sodium concentrations were found to be high. The patients’ pediatrician considered syndrome of inappropriate antidiuretic hormone secretion (SIADH), but neither underwent measurement of their ADH level. Of all six patients who developed hyponatremia, five were children.
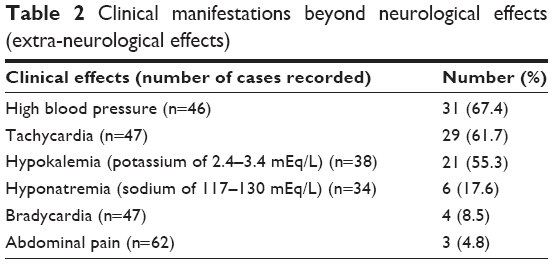 | Table 2 Clinical manifestations beyond neurological effects (extra-neurological effects) |
The clinical courses and treatments of all patients and the patients who were bitten by Malayan kraits and banded kraits are shown in Table 3. The median interval between the snake bite and the onset of neurological signs and symptoms was 3 hours (range, 0.5–8 hours). Nine patients (11.5%) were bitten by kraits but did not develop clinical abnormalities after the bites; these cases were classified as dry bites, and three of them received antivenom. One patient was bitten by a red-headed krait without clinical envenomation, and treatment involved supportive care only. Eighty-six percent of all patients received snake antivenom, and the median amount given was 15 vials (range, 3–50 vials). The median time of the antivenom treatment was 5 hours (30 minutes to 64 hours). The most common type of antivenom administered was a monovalent-specific antivenom (76.1%). Some patients were not treated with antivenom because they did not have motor weakness. Most patients (75.6%) required intubation and ventilator support; the median duration of assisted ventilation was 6 days. Although one patient, who received the specific antivenom, was on assisted ventilation for 37 days because of pneumonia, the patient was finally discharged. The median length of hospital stay was 7 days. No patients developed progressive muscle weakness after antivenom treatment. Some patients developed complications during hospitalization. The most common complications were pneumonia (n=12), acute kidney injury (n=2), cardiac arrest from respiratory failure (n=2), seizure from severe hyponatremia (n=2), and urinary tract infection (n=2). Other complications reported in one patient each were brain anoxia, brain swelling, fetal distress in a pregnant patient, fever, hypoglycemia, respiratory alkalosis, gastrointestinal bleeding, abnormal gait, and sepsis. Dilated cardiomyopathy was reported in one healthy 15-year-old male patient, but whether this condition was associated with krait envenomation could not be determined. One pregnant woman at a gestational age of about 35 weeks developed fetal distress at presentation; however, she and her child survived. Four patients developed allergic reactions to antivenom; symptoms included urticarial rash in all patients and lung wheezing in one patient. All patients received parenteral chlorpheniramine and adrenaline, and their clinical signs and symptoms improved and finally resolved.
 | Table 3 Clinical course and treatment of all patients bitten by MK and BK |
Five patients died, all from Malayan krait envenomation, resulting in an overall mortality rate of 6.4%. All five patients had developed complications, and three of them had rhabdomyolysis during hospitalization. All five patients had also received antivenom and were intubated.
We analyzed the factors during hospital admission that were associated with in-hospital mortality between the patients who died and survived. The clinical manifestations and laboratory findings were compared between the patients in these two groups, as shown in Table 4. The only factor that was significantly different between the patients who died and survived was in-hospital complications. No significant differences were found in age, onset of neurological effects, time to application of antivenom, amount of antivenom, duration of endotracheal intubation, vital signs at presentation (tachycardia, bradycardia, and high blood pressure), or abnormal laboratory findings (hyponatremia and hypokalemia).
 | Table 4 Comparison of clinical manifestations and laboratory findings between patients who survived and those who died |
Discussion
This was one of the largest studies of Malayan krait and banded krait envenomation in Southeast Asia performed to date. We found that the Malayan krait is the most clinically important Bungarus species in Thailand, because it was the most common species involved in krait bites and caused all deaths in this study. The mortality rate of Malayan krait bites was 7.4%. With respect to the epidemiologic distribution, krait bites were discovered in every region of Thailand except Bangkok. Most patients were bitten during the night, and some were bitten inside their houses. These findings support the data from other studies2,13 and are consistent with the known characteristics of kraits; ie, that they are terrestrial, nocturnally active, and often found near human habitats.2 Most patients were bitten during the rainy season in Thailand. The seasonal pattern of krait bites in our study is also consistent with other reports, indicating that krait envenomation mostly occurs during the rainy season.21 These data might assist in the establishment of snakebite prevention and education programs for the general population. In addition, our study supports the findings from other studies and highlights the extra-neurological effects after krait bites,29–31 among which high blood pressure and tachycardia were the most common, accounting for >50% of our cases. These autonomic abnormalities are hypothesized to be caused by decreased parasympathetic activity.19 Electrolyte abnormalities, especially hyponatremia, were also recognized as a clinical manifestation.18,29 Interestingly, hypokalemia was common in our study (55.3%), while hyponatremia was reported less frequently (only 17.6% of all patients). Severe hyponatremia (<120 mEq/L) was only found in the pediatric patients and eventually caused seizures in two patients. The attending pediatrician suspected that the severe hyponatremia was due to SIADH in two patients, but the ADH level was not measured. Therefore, we could not confidently identify the cause of hyponatremia. The pathophysiological explanation for krait bite-associated hyponatremia remains unclear. In one Vietnamese study of Malayan krait bites, the ADH level was found to be low.29 Some researchers have proposed that hyponatremia might be caused by a natriuretic peptide-like toxin, as indicated by the high urinary sodium concentration in patients bitten by the many-banded krait (Bungarus multicinctus) in Vietnam.18,32,33 Therefore, we also emphasize our finding of a high urinary sodium concentration in Malayan krait bite patients with severe hyponatremia in the present study.
In one study, hypokalemia reportedly occurred in 71% of patients with common krait (Bungarus caeruleus) envenomation.34 The authors explained that the hypokalemia might have been caused by a shift of potassium into cells secondary to beta-adrenergic stimulation due to autonomic dysfunction.34 In one case report, a patient who had been bitten by a Sind krait (Bungarus sindanus) developed severe autonomic disturbances and cardiac complications during hospitalization and had hypokalemia (potassium of 3.0 mmol/L) on admission.14 Nonetheless, hypokalemia has not been reported in patients with Malayan krait envenomation. Therefore, the present study indicates that hypokalemia can also be part of the clinical picture of Malayan krait envenomation, although not at a very severe level. Our data did not demonstrate the most appropriate investigation for the pathophysiology of hypokalemia, which was more common than hyponatremia. Thus, the mechanism underlying this electrolyte disturbance needs to be elucidated further.
Interestingly, hypokalemia and hyponatremia were noted only in patients with Malayan krait bites, and neither was present in patients with banded krait bites. However, the number of patients bitten by banded krait was small and might have been inadequate to interpret this clinical parameter.
The onset of neurological signs and symptoms after krait bites was quite rapid (approximately 3 hours), which is similar to the findings of other studies and reports.13,19,27,28 Nevertheless, the longest interval between the bite and the onset of neurological symptoms was 8 hours.
Altogether, our findings indicate that patients who have been bitten by kraits should be observed for clinical features of envenomation for at least 8 hours. Furthermore, frequent and close monitoring of vital signs and electrolyte levels should be performed in all patients with krait bites, especially pediatric patients and those bitten by Malayan kraits.
In a previous case series from Thailand,13 one patient who did not receive antivenom after a Malayan krait bite developed ventricular fibrillation. However, ventricular arrhythmia was not observed in our study regardless of antivenom administration. Thus, our study suggests that ventricular arrhythmia is not a common finding in krait envenomation. In some case reports of Malayan krait bites, some patients who did not receive antivenom were extubated about 1–2 months after the bite.19,28 Most of our patients were intubated and on ventilator support for about 6 days. This might be explained by the efficacy of antivenom administration. The reported incidence of allergic reaction was quite low. Thus, if a patient has indications for antivenom treatment, the antivenom should be given without delay. Bite-related in-hospital complications were significantly associated with death; therefore, besides antivenom treatment, adequate supportive care including management of in-hospital complications might help to lower the mortality rate.
Conclusion
The Malayan krait (B. candidus) was the most common species accounting for krait bites and caused all krait bite fatalities in the present study in Thailand. Krait bites caused clinical neurological features with only minimal local effects. The onset of neurological manifestations after bites was quite rapid (0.5–8 hours). Therefore, patients should be observed for at least 8 hours. The most common extra-neurologic signs and symptoms found in our study included high blood pressure, tachycardia, hypokalemia, and hyponatremia. Thus, frequent and close monitoring of vital signs and electrolytes is needed in these patients, especially pediatric patients and those bitten by Malayan kraits. Bite-related in-hospital complications were significantly associated with deaths. Thus, besides antivenom treatment, adequate supportive care including management of complications might help to reduce the mortality rate.
Limitations
This study was limited by its retrospective design, which might have resulted in incomplete data. Additionally, the patients provided their histories to the doctors or nurses, from whom we obtained the information for this study; therefore, the information might not have been clear or completely accurate in all cases. Finally, no definitive laboratory test was performed to confirm the diagnosis of krait bites.
Disclosure
The authors report no conflicts of interest in this work.
References
No authors listed. Snake bite – the neglected tropical disease. Lancet. 2015;386(9999):1110. | ||
Chanhome L, Cox M, Vasaruchapong T, Chaiyabutr N, Sitprija V. Characterization of venomous snakes of Thailand. Asian Biomedicine. 2011;5(3):311–328. | ||
Sibunruang SS, Sitprija V. Manual of Practical Management of Snake-bites and Animal Toxin Injury. Bangkok: Queen Saovabha Memorial Institute, The Thai Red Cross Society; 2013. | ||
Warrell DA. Guidelines for the Management of Snake-bites. New Delhi: World Health Organization, Regional Office for South-East Asia; 2010. Available from: http://apps.searo.who.int/PDS_DOCS/B4508.pdf. Accessed January 18, 2018. | ||
Tan NH, Poh CH, Tan CS. The lethal and biochemical properties of Bungarus candidus (Malayan krait) venom and venom fractions. Toxicon. 1989;27(9):1065–1070. | ||
Khow O, Chanhome L, Omori-Satoh T, et al. Isolation, toxicity and amino terminal sequences of three major neurotoxins in the venom of Malayan krait (Bungarus candidus) from Thailand. J Biochem. 2003;134(6):799–804. | ||
Kuch U, Molles BE, Omori-Satoh T, Chanhome L, Samejima Y, Mebs D. Identification of alpha-bungarotoxin (A31) as the major postsynaptic neurotoxin, and complete nucleotide identity of a genomic DNA of Bungarus candidus from Java with exons of the Bungarus multicinctus alpha-bungarotoxin (A31) gene. Toxicon. 2003;42(4):381–390. | ||
Chang CC, Lee CY. Isolation of neurotoxins from the venom of bungarus multicinctus and their modes of neuromuscular blocking action. Arch Int Pharmacodyn Ther. 1963;144:241–257. | ||
Dixon RW, Harris JB. Nerve terminal damage by beta-bungarotoxin: its clinical significance. Am J Pathol. 1999;154(2):447–455. | ||
Prasarnpun S, Walsh J, Harris JB. Beta-bungarotoxin-induced depletion of synaptic vesicles at the mammalian neuromuscular junction. Neuropharmacology. 2004;47(2):304–314. | ||
Chen IL, Lee CY. Ultrastructural changes in the motor nerve terminals caused by β-bungarotoxin. Virchows Archiv B. 1970;6(1):318–325. | ||
Warrell DA, Looareesuwan S, White NJ, et al. Severe neurotoxic envenoming by the Malayan krait Bungarus candidus (Linnaeus): response to antivenom and anticholinesterase. Br Med J. 1983;286(6366):678–680. | ||
Leeprasert W, Kaojarern S. Specific antivenom for Bungarus candidus. J Med Assoc Thai. 2007;90(7):1467–1476. | ||
Pillai LV, Ambike D, Husainy S, Khaire A, Captain A, Kuch U. Severe neurotoxic envenoming and cardiac complications after the bite of a ‘Sind Krait’ (Bungarus cf. sindanus) in Maharashtra, India. Trop Med Health. 2012;40(3):103–108. | ||
Faiz A, Ghose A, Ahsan F, et al. The greater black krait (Bungarus niger), a newly recognized cause of neuro-myotoxic snake bite envenoming in Bangladesh. Brain. 2010;133(11):3181–3193. | ||
Kaushik JS, Chakrabarty B, Gulati S, et al. Unusual late neurological complication in a child after an Indian krait bite. Pediatr Neurol. 2014;51(1):130–132. | ||
Agarwal R, Aggarwal AN, Gupta D. Elapid snakebite as a cause of severe hypertension. J Emerg Med. 2006;30(3):319–320. | ||
Höjer J, Tran Hung H, Warrell D. Life-threatening hyponatremia after krait bite envenoming – a new syndrome. Clin Toxicol. 2010;48(9):956–957. | ||
Laothong C, Sitprija V. Decreased parasympathetic activities in Malayan krait (Bungarus candidus) envenoming. Toxicon. 2001;39(9):1353–1357. | ||
Kularatne SA. Common krait (Bungarus caeruleus) bite in Anuradhapura, Sri Lanka: a prospective clinical study, 1996–1998. Postgrad Med J. 2002;78(919):276–280. | ||
Regional Office for South-East Asia, World Health Organization. Guidelines for the Management of Snakebites, 2nd ed. WHO Regional Office for South-East Asia. Available from: http://apps.searo.who.int/PDS_DOCS/B5255.pdf?ua=1. Accessed January 18, 2018. | ||
Looareesuwan S, Viravan C, Warrell DA. Factors contributing to fatal snake bite in the rural tropics: analysis of 46 cases in Thailand. Trans R Soc Trop Med Hyg. 1988;82(6):930–934. | ||
Hoffman R, Howland MA, Lewin N, Nelson L, Goldfrank L. Initial evaluation of the patient: vital signs and toxic syndromes. In: Hoffman RS, Howland MA, Lewin NA, Nelson LS, Goldfrank LR, Flomenbaum NE, editors. Goldfrank’s Toxicologic Emergencies. 10th ed. New York: McGraw Hill Education; 2015:26–29. | ||
Kidney Disease: Improving Global Outcomes (KDIGO) CKD-MBD Work Group. KDIGO clinical practice guideline for the diagnosis, evaluation, prevention, and treatment of Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD). Kidney Int Suppl. 2009;113:S1–S130. | ||
Counselman FL, Lo BM. Rhabdomyolysis. In: Judith E, Tintinalli J, Stapczynski S, et al, editors. Tintinalli’s Emergency Medicine. 8 ed. New York: McGraw Hill Education; 2016:581–584. | ||
Thai Meteorological Department. Climate of Thailand; 2014. Available from: https://www.tmd.go.th/info/info.php?FileID=53. Accessed February 8, 2018. | ||
Pochanugool C, Wilde H, Jitapunkul S, Limthongkul S. Spontaneous recovery from severe neurotoxic envenoming by a Malayan krait Bungarus candidus (Linnaeus) in Thailand. Wilderness Environ Med. 1997;8(4):223–225. | ||
Chaosirikul S. Severe neurotoxic envenoming by Malayan krait: a case report. Med J Srisaket Burirum Hospitals. 1993;8:230–236. | ||
Trinh KX, Khac QL, Trinh LX, Warrell DA. Hyponatraemia, rhabdomyolysis, alterations in blood pressure and persistent mydriasis in patients envenomed by Malayan kraits (Bungarus candidus) in southern Viet Nam. Toxicon. 2010;56(6):1070–1075. | ||
Chaisakul J, Rusmili MR, Hodgson WC, et al. A Pharmacological Examination of the Cardiovascular Effects of Malayan Krait (Bungarus candidus) Venoms. Toxins. 2017;9(4):122. | ||
Chaiyabutr N, Chanholme L, Sitprija V. Observations on General Circulation and Renal Hemodynamics in the Rabbit Given Venom of Bungarus candidus. Oral Presentation 040 Presented at 8th IST Asia-Pacific Meeting on Animal, Plant, and Microbial Toxins; 2–6 December 2008. Vietnam: Hanoi & Halong Bay; 2008. | ||
Siang AS, Doley R, Vonk FJ, Kini RM. Transcriptomic analysis of the venom gland of the red-headed krait (Bungarus flaviceps) using expressed sequence tags. BMC Mol Biol. 2010;11:24. | ||
Akashi YJ, Springer J, Lainscak M, Anker SD. Atrial natriuretic peptide and related peptides. Clin Chem Lab Med. 2007;45(10):1259–1267. | ||
Namal Rathnayaka RM, Kularatne SA, Kumarasinghe KD, Jeganadan K, Ranathunga PE. Two rare case reports of confirmed Ceylon krait (Bungarus ceylonicus) envenoming in Sri Lanka. Toxicon. 2017;127:44–48. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.