")
Back to Journals » Infection and Drug Resistance » Volume 17
Knowledge, Perception, and Self-Confidence of Antibiotic Resistance, Appropriate Antibiotic Therapy, and Antibiotic Stewardship Among Undergraduate Pharmacy Students in Sudan
Authors Abdelkarim OA , Abubakar U , Hussain MA , Abadi AEB, Mohamed AO, Osman W, Sherif AE, Ebrahim SA, Ahmed AH, Ahmed MO, Ashour A
Received 7 November 2023
Accepted for publication 22 February 2024
Published 11 March 2024 Volume 2024:17 Pages 935—949
DOI https://doi.org/10.2147/IDR.S435190
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Omalhassan Amir Abdelkarim,1 Usman Abubakar,2 Mohamed A Hussain,3 Abd Elrahman Babiker Abadi,1 Ahmed Osman Mohamed,3 Wadah Osman,4,5 Asmaa E Sherif,4,6 Sara Altayep Ebrahim,1 Asmaa Hussein Ahmed,1 Marwa Omer Ahmed,1 Ahmed Ashour4,6
1Department of Pharmacy Practice and Clinical Pharmacy, Faculty of Pharmacy, International University of Africa, Khartoum, Sudan; 2Department of Clinical Pharmacy and Practice, College of Pharmacy, QU Health, Qatar University, Doha, Qatar; 3Department of Pharmaceutical Microbiology, Faculty of Pharmacy, International University of Africa, Khartoum, Sudan; 4Department of Pharmacognosy, Faculty of Pharmacy, Prince Sattam Bin Abdulaziz University, Al-KharJ, Saudi Arabia; 5Department of Pharmacognosy, Faculty of Pharmacy, University of Khartoum, Khartoum, Sudan; 6Department of Pharmacognosy, Faculty of Pharmacy, Mansoura University, Mansoura, Egypt
Correspondence: Omalhassan Amir Abdelkarim, Department of Pharmacy Practice and Clinical Pharmacy, Faculty of Pharmacy, International University of Africa, Khartoum, PO Box 2469, Sudan, Email [email protected]
Background: Adequate training in infectious diseases and antibiotic resistance is crucial for pharmacy students to participate in antibiotic stewardship programs and understand microbiology careers.
Aim: The study was carried out to assess the knowledge and self-reported confidence in antibiotic resistance, antibiotic therapy, and antimicrobial stewardship (AMS) among final-year undergraduate pharmacy students in Sudan.
Methods: A cross-sectional study was conducted in three universities using a 57-item online questionnaire between April and May 2022.
Results: A total of 109 students (response rate 36%) participated and showed average knowledge scores of 5.6± 1.7 (out of 10.0) for antibiotic resistance, 4.9± 2.0 (out of 5.0) for appropriate antibiotic therapy, and 3.1± 1.4 (out of 5.0) for AMS. No significant differences were observed among schools. Some students reported poor knowledge about antibiotic therapy and the consequences of resistance. One-third of students lacked confidence in interpreting microbiological results. Knowledge of antibiotic resistance among students’ practice area after graduation was higher (p=0.017) and those interested in ID careers (5.8 vs 4.8) (p=0.037). Male students (5.6 vs 4.5) and those interested in ID careers (4.3 vs 3.4) (p< 0.001) had higher scores of appropriate antibiotic therapy. Students attended antibiotic resistance courses (51.5 vs 45.2), and those interested in ID significantly had higher self-confidence (55.3 vs 45.8) (p=0.008).
Conclusion: Pharmacy students in Sudan have substantial knowledge of AMS and antibiotic resistance with poor knowledge of antibiotic therapy. Adequate training about infectious diseases and related topics is recommended to improve pharmacy students’ understanding of microbiological findings, other competencies, and skills to incorporate in antimicrobial stewardship.
Keywords: antibiotic resistance, antimicrobial stewardship, antimicrobial therapy, Sudan, pharmacy students
Introduction
Antimicrobial resistance (AMR) is considered one of this century’s most severe global public health threats.1 Antimicrobial resistance has developed as one of the significant urgent threats to public health, causing severe issues with the successful prevention and treatment of persistent diseases.2 Moreover, an earlier study has found a correlation between AMR and increased economic costs, morbidity, and mortality in the healthcare sector.3 The improper use of antibiotics in healthcare and agriculture is the leading cause of AMR.2 However, Inappropriate use of antimicrobials is a significant cause of AMR in hospital and community settings.1 Also, bacteria develop resistance through spontaneous evolution, mutation, and horizontal gene transfer of resistance genes.2 The deficiency of new antimicrobials in the development pipeline has augmented the problem of AMR.1
Self-medication and purchasing antimicrobials without a prescription are common issues in community settings. Worldwide, 62% of the antimicrobials in community pharmacies are dispensed without a prescription.4 In some Middle Eastern countries, the percentage of non-prescription of antibiotics has reached 82%.5 In several regions of Sudan, the population purchased most antibiotics from pharmacies.6–8 Moreover, a study conducted in Khartoum State revealed that over 80% of the community practiced self-medication, of which 28.7% were antibiotic users.7
A previous study found that 60.3% of Sudanese medical students used antibiotics frequently,9 while a recent study found that 71.3% of people in Sudan self-medicate with antibiotics.10 Additionally, around 85.5% of community pharmacists in Sudan dispense antibiotics without proper prescriptions.11 These activities contribute to antimicrobial resistance. Hospitals prescribe antibiotics inappropriately in 20% to 50% of cases.12 Current estimates predict that 2050 antibiotic resistance will result in 10 million deaths yearly and a decline in productivity by 2% to 3.5%.13
Antibiotic stewardship is a program that promotes the appropriate use of antibiotics to prohibit antibiotic resistance.1,14 An antibiotic stewardship program aims to improve clinical outcomes and minimize adverse effects.12 A multidisciplinary team with a pharmacist is required to implement antimicrobial stewardship interventions.12,15 According to the Centers for Disease Control and Prevention, having a pharmacist on board is one of the seven critical components of a successful antimicrobial stewardship program.12 The pharmacist’s role in an antibiotic stewardship program includes auditing antibiotic usage, providing feedback, guiding empirical antibiotic treatment, and developing formularies and guidelines.15 Additionally, the pharmacist is responsible for implementing automatic change and stop orders, therapeutic drug monitoring, dose adjustment, optimization, and leading the antibiotic stewardship team.12,14 A pharmacist-led antibiotic stewardship program is beneficial in ensuring the appropriate use of antibiotics, improving clinical outcomes, and reducing antibiotic expenditure.16–18
Training healthcare professionals, especially pharmacists, in antibiotic resistance control strategies is crucial.19 However, the lack of training in infectious disease (ID) and antimicrobial stewardship (AMS) hinders pharmacist participation in stewardship programs.20–22 Studies show pharmacists with postgraduate qualifications have better attitudes towards antibiotic stewardship programs.23 Therefore, undergraduate training in ID and antimicrobial stewardship is necessary to prepare future pharmacists for their duties.
Studies conducted in developed countries have shown that future medical practitioners require more training to enhance their antibiotic prescribing and stewardship skills.24–26 The present study aims to evaluate the readiness of final-year pharmacy students for AMS duties. Furthermore, there needs to be more data on the knowledge of pharmacy undergraduate students in Sudan regarding antibiotic resistance, appropriate antibiotic therapy, and antibiotic stewardship. This study aims to address this gap and identify areas that require further training.
Materials and Methods
Study Design, Settings
A descriptive cross-sectional study was carried out in Khartoum state, Sudan, at three Private Universities, the International University of Africa (IUA), Sudan International University (SIU), and the University of Ibn Sina (UIS), in a period from April 10, 2022, till May 10, 2022.
Study Population
The study was conducted on final-year pharmacy undergraduate students across three universities: IUA, SIU, and UIS. These universities offer a five-year Bachelor of Pharmacy degree program, which includes required pharmacotherapy courses for ID. These courses cover the principles of antimicrobial resistance and therapy.
Study Tool
The study questionnaire was created after reviewing the literature and comprised 57 questions. The questionnaire’s design and validation were adapted from a previous study.27 It consists of five sections: demographic, knowledge of AMR, knowledge of antimicrobial therapy (AMT), knowledge of antimicrobial stewardship, perceptions regarding antimicrobial resistance, self-confidence to accomplish antimicrobial stewardship tasks, and perception towards antimicrobial stewardship. The knowledge of antimicrobial resistance, antimicrobial therapy, and antimicrobial stewardship is assessed using multiple-choice questions with one best answer. Self-confidence to complete antimicrobial stewardship activities and perceptions regarding antimicrobial resistance are evaluated using a 5-point Likert scale.
Data Collection
The survey was conducted during the last semester of the academic session. The data were collected between April and May 2022 in the three universities. The final-year pharmacy undergraduate students from the three universities participated in an electronic survey to evaluate their knowledge of antimicrobial resistance, therapy, and stewardship. The survey link was shared via specific class WhatsApp groups, and students were reminded every three days to complete it. They were instructed to submit the survey only once to avoid duplication.
Data Analysis
The data was analyzed using IBM Statistical Package for Service Solutions (SPSS) version 25. The data was anonymized before analysis. Categorical data was reported as frequencies and percentages, while continuous data was reported as mean with standard deviation (SD). The responses to the knowledge sections were scored using 1 for the correct answers and 0 for incorrect answers. The knowledge score was calculated by adding up correct responses in each section. Self-confidence was also scored on a scale of 1 to 5 (from no confidence at all to extreme confidence, respectively). The association between variables was analyzed through the chi-square test. Student’s t-tests and one-way ANOVA were used to assess the association between student characteristics and scores for AMR, AMT, AMS, and self-confidence, a P-value less than 0.05 was considered statistically significant.
Results
Characteristics of the Students
Table 1 displays the characteristics of pharmacy students who participated in the study. A total of 109 students completed the questionnaire: 56 from IUA, 37 from SIU, and 16 from UIS. The overall response rate was 36%, with 66.1% of respondents being female. The lecture was identified as the most common primary source of information on antimicrobials and AMR across all groups, with percentages of 69.6%, 64.9%, and 62.5% for IUA, SIU, and UIS, respectively. Attendance of a course and workshop on appropriate antimicrobial use was higher among UIS students 13 (81.3%) than SIU and IUA students 23 (62.2%) and 31 (55.4%). After graduation, 36.7% of the students considered pursuing a career as a community pharmacist.
 |
Table 1 Characteristics of the Pharmacy Students Who Participated in the Study (n=109) |
Knowledge and Perception of Antimicrobial Resistance
The study found that more than 70% of the students demonstrated a good knowledge of AMR. They could define it, explain its mechanisms, and identify the factors that caused its emergence.
Moreover, they were familiar with the interventions used to combat it. However, less than 50% of the students could identify the factors responsible for spreading infections resistant to antimicrobial agents. For more details of knowledge and perceptions of AMR, refer to Table 2. More than 50% know the consequences of AMR. The overall mean knowledge score of antibiotic resistance was 5.6±1.7 out of 10. The universities had comparable means at 5.5±1.9, 5.8±1.6, and 5.8±1.6 for IUA, SIU, and ISU, respectively.
 |
Table 2 Knowledge and Perception of Antimicrobial Resistance Among Students (N=109) |
The majority of students, 68 (62.4%), disagreed or strongly disagreed with the notion that antibiotic resistance is not a serious issue and that new antibiotics will be developed to replace resistant ones. In contrast, about 69 (63.3%) students agreed/strongly agreed that they required more training in antibiotic resistance. Moreover, 68% strongly agreed/agreed that comprehensive knowledge of antibiotic resistance is essential in their pharmacy career. The median score for perception of AMR was 18, with a range of 11–25. The details about perception are displayed in Table 2.
Antimicrobial Therapy Knowledge
There was no significant difference in knowledge of upper respiratory tract infections (URTIs) that do not require antimicrobials, antimicrobials used for Clostridium difficile infections, and antimicrobial use during pregnancy among students from the three universities. A higher percentage of students at UIS, 62.5%, were aware of the antibiotics that have the best activity against anaerobes compared to IUA, 58.9%, and SIU, 40.5%. There was no significant difference in knowledge among students at the three universities regarding antimicrobials effective against Methicillin-resistant staphylococcus aureus (MRSA) and those that cross the blood-brain barrier. Overall, the mean knowledge score for appropriate AMT was similar across the three groups, with a mean score of 4.9 ± 2.0 out of a maximum of 9. The details regarding AMT knowledge are presented in Table 3.
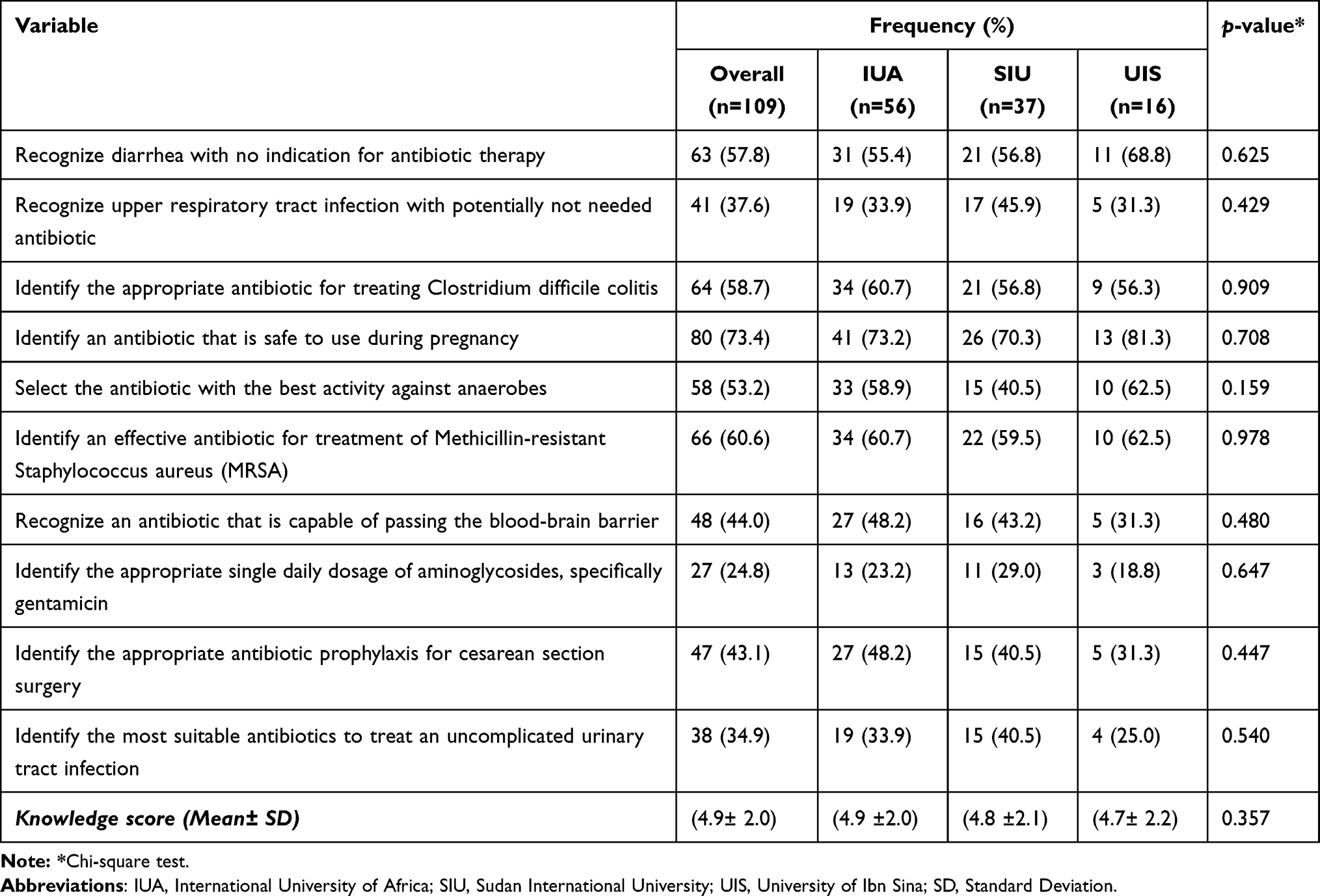 |
Table 3 Pharmacy Students’ Knowledge of Antibiotic Therapy |
Understanding and Perceptions Toward Antimicrobial Stewardship
The knowledge and perceptions of AMS among study students are illustrated in Table 4. Out of the total number of students, only 38.5% had received formal training in AMS, with significant difference (p-value=0.017) in the duration of training. More than 80% of the students expressed the need for additional training about AMT and AMS. The study found no significant difference in the knowledge of the goals of AMS between students in three universities (p=0.369). The maximum score was 5, and the mean knowledge score for AMS was (3.1±1.4).
 |
Table 4 Knowledge and Perception of Antimicrobial Stewardship Among (N=109) Study Students |
Confidence of the Students to Contribute to Antimicrobial Stewardship Activities
Students demonstrated moderate self-confidence in achieving various AMS tasks, including finding reliable sources of information to treat infections 89 (81.7%), choosing the appropriate duration of treatment 87 (78.9%), understanding the basic mechanisms of antibiotic resistance 86 (79.8%), and interpreting therapeutic drug monitoring results and making recommendations 85 (78.0%). However, they showed poor self-confidence in some other AMS skills. Of all the students, only 76 (69.7%) had moderate confidence in interpreting microbiological results. Table 5 shows the distribution of confidence levels of students from different universities towards contributing to AMS activities. The mean score for self-confidence was 49±12.6, with a maximum score of 75.
 |
Table 5 Confidence Levels of the Students to Contribute Antimicrobial Stewardship Activities |
Correlation Between the Characteristics of Students and Knowledge of Antibiotic Resistance, Therapy, Stewardship, and Self-Confidence
Table 6 compares knowledge and self-confidence scores based on various student characteristics. The mean knowledge scores for AMR showed significant differences based on the area of pharmacy chosen after graduation (p-value=0.017) and the student’s interest in ID pharmacy (p-value=0.037). Additionally, appropriate AMT scores demonstrated significant differences based on gender (p-value=0.011) and the student’s interest in ID pharmacy as a career after graduation (p<0.001). The results also showed that self-confidence scores had significant differences based on attendance of workshops, seminars, or courses related to “antibiotic resistance” (p-value=0.011) and the student’s interest in ID pharmacy after graduation (p-value=0.008). However, there were no significant differences in the mean knowledge scores for AMS based on student characteristics.
 |
Table 6 Correlations of Knowledge Scores Concerning Antibiotic Resistance, Therapy, Stewardship, and Self-Confidence Among Students with Different Characteristics |
Discussion
The present study assessed pharmacy students’ knowledge of antimicrobial resistance, therapy, and stewardship and their self-confidence. Despite consistent reminders every three days, the response rate for this study was only 36%, which could be much lower. It’s worth noting that similar studies have also reported lower response rates.28,29 In contrast, a study conducted in Asian countries, including Indonesia, Malaysia, and Pakistan, reported a higher response rate of 77.8%.27,30
In the current study, the majority of students, 67%, relied on lectures as their primary source of information regarding antimicrobials and AMR. In contrast, the results of previous studies reported that lectures as a source of information in 39.3%, 44.8, and 81% of respondents in Asian countries, Malaysia and Nigeria, respectively.27,31 Differences in antibiotic interest may explain the variation between these countries and Sudan. However, the study participants showed good knowledge and positive attitudes toward reducing AMR. This result concurs with those reported in Egypt 2018 among medical students that nearly all had sufficient knowledge of AMR.32 In contrast, in India, medical students lack knowledge about AMR and AMS.33 On the other hand, knowledge of AMR was higher among pharmacy students than medical students in Pakistan.34 This discrepancy may be due to differences in healthcare school curricula and student exposure to experiential learning.
The prevalence of ID pharmacy carriers was 29.4%. In comparison, only 61.5% of our students attended courses/workshops on the appropriate use of antimicrobials, which is lower than in studies from other developing countries.31 Similarly, a high proportion of 45.9% of our study respondents attended ID clerkships compared to Nigerian students.31 This study revealed that pharmacy students in Sudan scored lower than their counterparts in Malaysia. This disparity might be due to differences in the undergraduate pharmacy training curriculum between the two countries. It is possible that the pharmacy training in Sudan is similar to that of Nigerian students.
Our students only received one semester of experiential training in the second semester of their final year. Additionally, the teaching style was primarily theoretical. However, pharmacy students in Malaysia are required to complete at least three semesters of practical learning before graduation.27
Knowledge of Antimicrobial Resistance
This study assessed the knowledge of appropriate antimicrobial therapy, resistance, and stewardship among pharmacy students in Sudan. The majority of students demonstrated moderate knowledge of AMR, which was consistent with an earlier study.27 In contrast, fewer students were aware of AMR in previous studies in Saudi Arabia and Pakistan.30,35 Our study found that student groups had poor knowledge of factors promoting antibiotic resistance and AMR reservoirs. A previous study among final pharmacy students in developing countries supports this finding.31 Our study found that most students accurately identified the definition, mechanisms, and factors contributing to the emergence of antibiotic resistance. Studies conducted in Asian countries, Saudi Arabia, and Pakistan have produced similar findings to this study.27,30,36 However, our results contrast with a survey conducted among master of pharmacy students in the United Kingdom.37 The discrepancy may be attributed to undergraduate pharmacy training curricula content variations between developed and developing countries. The lack of diversity in pharmacy training curricula among the three schools may also explain this variation. It is worth noting that all schools included in the study were private. Training duration varied among students from the three universities in the study. However, all pharmacy students are taught about AMR and AMT. Despite this, some students admitted to not attending these courses, possibly due to different semester offerings, and some could not recall the information they learned.
The current study found significant differences in the mean knowledge scores for AMR based on two factors: the area of pharmacy practice chosen by students after graduation and their interest in ID pharmacy. The differences in knowledge scores were based on the scope of pharmacy practice after graduation. Students who chose to work in a hospital or community pharmacy after graduation had significantly better knowledge of antibiotic resistance than other students. This finding could be supported by a 2022 study in Sudan, which found that more than half of community pharmacists had good knowledge of AMR, which was associated with their years of experience.11 These results agree that a lack of knowledge hindered hospital and community pharmacists’ participation in AMS activities.20,22,27
The study found that students interested in ID pharmacy had significantly higher antibiotic resistance knowledge scores than those without interest. Although students in this study take required courses in infectious disease pharmacotherapy, exposing them to AMR and AMT principles, only about one-third show interest in the subject. This result could be due to the short-term experiential ID clerkship for final pharmacy students in the three schools and the attendance of ID clerkship to improve the knowledge of antimicrobial therapy.27
Perception Toward Antimicrobial Resistance
This study found that 68% of pharmacy students consider having a solid understanding and positive perception of antibiotic resistance crucial for their careers. The study also revealed that 63.3% of students feel they require more training in antibiotic resistance, while 80.7% and 79.8% expressed the need for more training in AMS and AMT, respectively. Final-year pharmacy students showed similar trends in a previous study.27 However, a former study among medical and pharmacy students in developing countries also yielded comparable results.24–26 Future pharmacists require more training on antibiotic resistance to promote appropriate antibiotic use and stewardship teams.
Additionally, the present study showed that 62.4% of the students disagreed or strongly disagreed that antibiotic resistance is not a severe problem. Our finding is lower than the result of 75.8% of a previous study.31 A recent survey conducted in Libya presented a moderate perception of AMR among community pharmacists.38 This disparity is attributed to varying experiential learning exposure and antibiotic knowledge levels among university students.
Knowledge of Antimicrobial Therapy
Experiential, practical training in pharmacy school by attending an ID clerkship may give students more knowledge about AMT.31 The existing study showed moderate knowledge of appropriate antibiotic therapy with a mean score of 4.9 ± 2.0. Similarly, Students in Saudi Arabia have moderate knowledge of appropriate antibiotic therapy, according to a previous study.35 Our findings showed lower knowledge of AMT among pharmacy students in comparison to a previous survey in Malaysia.31 This difference may be attributed to the slighter exposure to ID clerkship among pharmacy students in our study. However, medical students had higher knowledge scores for antibiotic use than non-medical students.39 In contrast, a prior study among undergraduate medical and pharmacy students in East Africa reported a good understanding of antibiotics and antibiotic resistance.40 However, in Nigeria, more than half of the study respondents had good knowledge and practices regarding antimicrobial use.41
Furthermore, in this study, the majority of respondents demonstrated good knowledge of appropriate antibiotics for various conditions, including Methicillin-resistant Staphylococcus aureus (MRSA), Clostridium difficile colitis, during pregnancy, and the lack of indication for antibiotic therapy for diarrhea. Previous studies have revealed that respondents possess a good knowledge of situations where diarrhea does not require antibiotic therapy.26,31,42 This observation was also consistent with the current research. However, most students in the present study needed to improve their knowledge of appropriate antibiotic therapy for surgical prophylaxis during cesarean section, uncomplicated URTI, and UTI. Similar findings were observed in past studies in developed and developing countries.26,27,31 Providing adequate training to pharmacy undergraduate students is crucial in developed and developing countries. The training should impart the skills and knowledge for identifying UTIs that do not require antibiotic therapy, the appropriate use of surgical antimicrobial prophylaxis, and antimicrobials for treating various medical conditions.
Additionally, our study is not supported by a study conducted in East Africa, and only over two-thirds of the students correctly described the appropriate antibiotic for UTI.40 Nevertheless, a survey of community pharmacists in Sudan found that over 50% dispensed antibiotics for UTI without a prescription.11 This widespread overuse of antimicrobials might be one leading cause of antimicrobial resistance, broad-spectrum use when narrow-spectrum is available, and poor patient adherence to prescriptions. On the other hand, AMS aims to address the inappropriate use of antimicrobials for URTI in all hospital and community settings.4,43 A systematic review found that community pharmacies often dispensed antibiotics to patients with symptoms of URTI without a prescription,4 although viruses cause most URTIs and do not require antibiotics. Proper training of pharmacists could reduce the inappropriate use of antibiotics for URTIs.42 The disparity in dispensing practices might be attributed to differences in pharmacy curricula, regulations, and inspection across countries.
Furthermore, the study found that the students lacked sufficient knowledge about the appropriate use of antibiotics that can penetrate the blood-brain barrier. These findings are consistent with a study conducted in several Asian nations.27 On the other hand, they contradict the results of a previous study, which demonstrated that most medical students and doctors accurately identified antibiotics that could cross the blood-brain barrier.42 Therefore, pharmacy students need more training in identifying infections that do not need antimicrobials and prophylaxis and selecting appropriate antimicrobials. Training early career pharmacists is crucial to prevent inappropriate dispensing of antimicrobials.20 Our study found that male students had a significantly better understanding of appropriate antibiotic therapy than female students. The difference in knowledge could be attributed to this study’s unequal distribution of male and female students.
Based on the student’s interest in ID pharmacy after graduation, the differences in their antibiotic therapy knowledge scores could be explained by the variation in pharmacy training curricula. This emphasizes the necessity to standardize pharmacy training curricula across different countries. Previous data supported this observation.26,27 This result strengthens the view that the difference in the AMS training duration was significantly reported in this study. However, knowledge about AMT achievement can be developed by attending practical training by ID clerkship among pharmacy school students.31
Knowledge and Perceptions Toward Antimicrobial Stewardship
Our study found no significant differences in AMS knowledge among students from three universities, including familiarity with AMS goals and formal training. A previous study on antimicrobial training among medical students in the United States (US) had a similar result.44 Furthermore, these findings agree with a study conducted in South Africa.28 Similar to an earlier study conducted in Nigeria, there was no formal training in AMS among more than half of the students.31 The points mentioned earlier highlight the significance of imparting extra training to bridge the gaps in the school curricula of universities, which will boost the knowledge of future pharmacists concerning antibiotic resistance and prepare them to function efficiently as professionals in the appropriate use of antibiotics.
The present study found that only 57.8% of the students were familiar with AMS and its goals. This percentage is noticeably lower than that of previous research studies. For instance, two studies conducted in Pakistan among medical and pharmacy students found that 80.4% and 83.5% of the participants were knowledgeable about AMS.34,45 Similarly, a study conducted in three Asian countries reported that 64.5% of the participants could identify the goals of AMS.27 Our study found a higher percentage of familiarity with AMS among pharmacy students compared to a recent survey conducted in Saudi Arabia, which reported a 50.3% familiarity rate.36 The variation in results can be attributed to differences in curriculum across countries. To improve awareness of responsible antibiotic use, universities should incorporate dedicated modules on AMS and appropriate prescribing practices. This is supported by our study’s finding that there were no significant differences in the mean knowledge scores for AMS based on all student characteristics. This conclusion is reinforced by the fact that students still need to receive training in AMS. A more significant proportion of students have requested further training in AMS to enhance their understanding. Several studies have reported the readiness of students to receive more education on AMS. These studies include research on students of a US medical school, pharmacy students in South Africa, and final-year undergraduate medical students at three universities in East Africa.28,40,44 Therefore, pharmacist training is essential, as a lack of knowledge hinders the participation of community and hospital pharmacists in AMS activities.20,22,27
Students’ Confidence to Contribute to Antimicrobial Stewardship Activities
A confident pharmacist can effectively participate in AMS programs through higher self-confidence, which enables them to convince other healthcare professionals of the appropriate use of antibiotics. Our study found that students reported moderate self-confidence in completing AMS tasks, with moderate confidence observed across all tasks. However, one-third of the current study students need more confidence (not very confident/not confident) to interpret microbiological results. On the contrary, an earlier study documented that Nigerian pharmacy students reported greater confidence in their AMS skills.31
Similarly, there was a gap in understanding microbiology careers among Indian students, according to an earlier study.46 Also, the previous research supported our finding that students needed to be more confident in reporting the microbiological result to influence the choice of appropriate antibiotics.40 Contrary to an earlier study in South Africa, a third of participants express confidence in prescribing antibiotics,47 likely due to adherence to guidelines and consultation with infectious disease specialists. The scarcity of AMS training for pharmacy students explains students’ need for higher confidence. However, proper interpretation of microbiological findings is crucial to avoid misdiagnosis and misuse of antibiotics.48
Students need more preparedness in using microbiology to guide the management of clinical scenarios with antibiotics, which indicates gaps in their understanding of microbiology’s role in AMS. Consequently, including AMS training in the undergraduate curriculum can enhance pharmacists’ skills and confidence, enabling them to contribute to AMS activities. Nevertheless, the previous data reported pharmacists’ vital role in improving and implementing the AMS program.12,14,15 To reduce inappropriate dispensing of antimicrobials, pharmacists must have a confident understanding of microbiological results, enabling them to distinguish between different types of infections that require AMT. which is particularly important in a community pharmacy setting where patients with infections such as URTI have been reported to receive inappropriate dispensing of antimicrobials.4
Our study also found that the self-confidence scores of students to participate in AMS activities varied significantly based on their attendance at an antibiotic resistance workshop, seminar, or course and their interest in ID pharmacy after graduation. The differences in self-confidence scores were due to the diversity of pharmacy training curricula among schools. This study also showed that self-confidence scores varied significantly based on student interest in ID pharmacy after graduation, consistent with previous research in other developing countries.27
Limitation
The study shed light on the knowledge and self-confidence of final-year pharmacy students in Sudan regarding their participation in AMS programs. This is the first study to assess the knowledge and self-confidence of final-year pharmacy students in Sudan regarding antibiotic resistance, therapy, and stewardship. The study emphasizes the need for increased curriculum and experiential learning training to enhance knowledge and self-confidence for future experts in AMS programs. Despite these, some limitations should be considered with caution. Firstly, the research was conducted in private pharmacy schools in Sudan, making it difficult to generalize the results to the entire population. Secondly, convenience sampling was used to select students from three pharmacy schools. Hence, the sample collected does not represent pharmacy students in Sudan. Thirdly, the questions used to evaluate knowledge may only cover some relevant topics, leading to assessment bias. Fourthly, the participants self-reported their confidence levels, which may have been influenced by social desirability bias. Therefore, this can be avoided by using an objective structured clinical examination form in a clinical setting to assess confidence. Fifthly, the questionnaire used in the study contains questions that require students to recall past information, which could increase the risk of recall bias. Sixty, the diversity of pharmacy programs in the participating universities (including differences in training, such as ID clerkships in the final semester and less than fifty percent of students attending ID clerkships) could have affected the study’s outcome. These emphasized limitations should be abridged in future studies.
Conclusion
In Sudan, the final-year pharmacy students possess moderate knowledge and perceptions regarding antimicrobial resistance and stewardship. There needed to be better knowledge of AMT among the students. One-third of students require more confidence to identify microbiological findings accurately. The interest in infectious diseases after graduation significantly affects knowledge and self-confidence scores. The students expressed their requirement for more training regarding antimicrobial resistance, therapy, and stewardship. Therefore, stakeholders in Sudan should consider this study’s findings to strengthen and enforce existing antibiotic use regulations and increase pharmacy students training in antimicrobial therapy, antimicrobial resistance, and antimicrobial stewardship. Consequently, this could improve their knowledge, confidence, and competency toward the rational use of antibiotics and better care for patients. However, it improves their ability to participate in antimicrobial stewardship programs in healthcare settings in their future career. Moreover, it will impact effective healthcare delivery and outcome measures by decreasing antibiotic consumption, compliance with antibiotic policy, and reducing infections. In Sudan, an antimicrobial stewardship program was established following the World Health Organization (WHO) elements and started by developing a National Action Plan to achieve awareness of AMR, surveillance, and research to prevent AMR, improve the use of antimicrobial drugs, and prevent and control infection. Further interventional studies regarding knowledge and attitudes toward antimicrobial resistance and stewardship among community pharmacists are recommended.
Abbreviations
AMR, Antimicrobial resistance; AMS antimicrobial stewardship; AMT, Antimicrobial therapy; ID, Infectious disease; IUA, International University of Africa; MRSA, Methicillin-resistant Staphylococcus aureus; SD, Standard deviation; SIU, Sudan International University; SPSS, Statistical Package for Service Solutions; UIS, University of Ibn Sina; URTI, Upper respiratory tract infection; US, United States; UTI, Urinary tract infection, WHO, World Health Organization.
Data Sharing Statement
The datasets can be accessed upon reasonable request through the corresponding author.
Ethics Approval
Ethical approval was granted by the Research Ethics Committee of the Faculty of Pharmacy at the International University of Africa. Permission to access data from students of two other universities (SIU and ISU) was obtained from the deans of the respective faculties. The questionnaire was sent to the student groups, and their responses were considered as consent to their participation in the study.
Acknowledgments
All authors thank Prince Sattam bin Abdulaziz University for supporting and funding this study.
Author Contributions
All authors had a significant contribution to this work, whether that is in the conception, validation, study design, execution, acquisition of data, software, formal analysis, and interpretation, or other areas such as taking part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study is funded by Prince Sattam bin Abdulaziz University, project number PSAU/2023/R/1445.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization (WHO). Antimicrobial resistance: global report on surveillance; 2014. Available from: https://iris.who.int/bitstream/handle/10665/112642/?sequence=1.
2. Dadgostar P. Antimicrobial Resistance: implications and Costs. Infect Drug Resist. 2019;12:3903–3910. doi:10.2147/IDR.S234610
3. European Centre for Disease Prevention and Control & European Medicines Agency. The bacterial challenge: time to react- a call to narrow the gap between multidrug-resistant bacteria in the EU and the development of new antibacterial agents. ECDC/EMEAJoint Technical report; 2009. Available from: https://www.ecdc.Europa.eu/sites/default/files/media/en/publications/Publications/0909_TER_The_Bacterial_Challenge_Time_to_React.pdf.
4. Auta A, Hadi MA, Oga E, et al. Global access to antibiotics without prescription in community pharmacies: a systematic review and meta-analysis. J Infect. 2019;78(1):8–18. doi:10.1016/j.jinf.2018.07.001
5. Alhomoud F, Aljamea Z, Almahasnah R, Alkhalifah K, Basalelah L, Alhomoud FK. Self-medication and self-prescription with antibiotics in the Middle East- do they really happen? A systematic review of the prevalence, possible reasons, and Outcomes.: IJID: official publication of the International Society for Infectious Diseases. Int J Infect Dis. 2017;57:3–12. doi:10.1016/j.ijid.2017.01.014
6. Ahmed A, Eltayeb I, Eltahir M. Patterns of self-medication with antibiotics in Khartoum State, Sudan. World J Pharm Res. 2014;3:678–692.
7. Awad AI, Eltayeb IB. Self-medication practices with antibiotics and antimalarials among Sudanese undergraduate university students. Ann Pharmacother. 2007;41(7):1249–1255. doi:10.1345/aph.1K068
8. Awad AI, Eltayeb IB, Capps PA. Self-medication practices in Khartoum State, Sudan. Eur J Clin Pharmacol. 2006;62(4):317–324. doi:10.1007/s00228-006-0107-1
9. Elmahi OKO, Musa RAE, Shareef AAH, et al. Perception and practice of self-medication with antibiotics among medical students in Sudanese universities: a cross-sectional study. PLoS One. 2022;17(1):e0263067. doi:10.1371/journal.pone.0263067
10. Hussain MA, Mohamed AO, Abdelkarim OA, et al. Prevalence and predictors of antibiotic self-medication in Sudan: a descriptive cross-sectional study. Antibiotics. 2023;12(3):612. doi:10.3390/antibiotics12030612
11. Abdelrahman Hussain M, Knowledge OMA, Sandel Abkar A, Siddig Mohamed F, Khider Elzubair H. Attitude and practice of community pharmacists in relation to dispensing antibiotics without prescription in Sudan: a cross-sectional study. Integr Pharm Res Pract. 2022;11:107–116. doi:10.2147/IPRP.S363079
12. Centers for Disease Control and Prevention. Core elements of hospital antibiotic stewardship programs. US Department of Health and Human Services; 2014. Available from: https://6.www.cdc.gov/antibiotic-use/healthcare/implementation/core-elements.html.
13. O’Neil J Antimicrobial Resistance: tackling a crisis for the health and wealth of nations; 2014. Available from: https://amr-review.org/sites/default/files/AMR%20Review%20Paper%20-%20Tackling%20a%20crisis%20for%20the%20health%20and%20wealth%20of%20nations_1.pdf.
14. Pollack LA, Srinivasan A. Core elements of hospital antibiotic stewardship programs from the centers for disease control and prevention. an official publication of the infectious Diseases Society of America. Clin Infect Dis. 2014;59(3):S97–S100. doi:10.1093/cid/ciu542
15. Wickens HJ, Farrell S, Ashiru-Oredope DAI, Jacklin A, Holmes A. The increasing role of pharmacists in antimicrobial stewardship in English hospitals. J Antimicrob Chemother. 2013;68(11):2675–2681. doi:10.1093/jac/dkt241
16. Abubakar U, Syed Sulaiman SA, Adesiyun AG, Lo TS. Impact of pharmacist-led antibiotic stewardship interventions on compliance with surgical antibiotic prophylaxis in obstetric and gynecologic surgeries in Nigeria. PLoS One. 2019;14(3):e0213395. doi:10.1371/journal.pone.0213395
17. Brink AJM, Feldman AP, Richards C, et al. Antimicrobial stewardship across 47 South African hospitals: an implementation study. Lancet Infect Dis. 2016;16(9):1017–1025. doi:10.1016/S1473-3099(16)30012-3
18. Wang J, Dong M, Lu Y, Zhao X, Li X, Wen A. Impact of pharmacist interventions on rational prophylactic antibiotic use and cost saving in elective cesarean section. Int J Clin Pharmacol Ther. 2015;53(8):605–615. doi:10.5414/CP202334
19. World Health Organization (WHO). The evolving threat of antimicrobial resistance: options for action; 2012. Available from: http://www.who.int/iris/handle/10665/44812.
20. Abubakar U, Tangiisuran B. Nationwide survey of pharmacists’ involvement in antimicrobial stewardship programs in Nigerian tertiary hospitals. Glob Antimicrob Resist. 2020;21:148–153. doi:10.1016/j.jgar.2019.10.007
21. Rizvi T, Thompson A, Williams M, Zaidi STR. Perceptions and current practices of community pharmacists regarding antimicrobial stewardship in Tasmania. Int J Clin Pharm. 2018;40(5):1380–1387. doi:10.1007/s11096-018-0701-1
22. Weier N, Tebano G, Thilly N, Demoré B, Pulcini C, Zaidi STR. Pharmacist participation in antimicrobial stewardship in Australian and French hospitals: a cross-sectional nationwide survey. J Antimicrob Chemother. 2018;73(3):804–813. doi:10.1093/jac/dkx435
23. Khan MU, Hassali MA, Ahmad A, Elkalmi RM, Zaidi ST, Dhingra S. Perceptions and Practices of Community Pharmacists towards Antimicrobial Stewardship in the State of Selangor, Malaysia. PLoS One. 2016;11(2):e0149623. doi:10.1371/journal.pone.0149623
24. Abbo LM, Cosgrove SE, Pottinger PS, et al. Medical students’ perceptions and knowledge about antimicrobial stewardship: how are we educating our future prescribers? Clin Infect Dis. 2013;57(5):631–638. doi:10.1093/cid/cit370
25. Dyar OJ, Pulcini C, Howard P, Nathwani D. European medical students: a first multicentre study of knowledge, attitudes, and perceptions of antibiotic prescribing and antibiotic resistance. J Antimicrob Chemother. 2014;69(3):842–846. doi:10.1093/jac/dkt440
26. Justo JA, Gauthier TP, Scheetz MH, et al. Knowledge and attitudes of doctor of pharmacy students regarding the appropriate use of antimicrobials. An official publication of the Infectious Diseases Society of America. Clin Infect Dis. 2014;59(Suppl 3):S162–169. doi:10.1093/cid/ciu537
27. Abubakar U, Muhammad HT, Sulaiman SAS, Ramatillah DL, Amir O. Knowledge and self-confidence of antibiotic resistance, appropriate antibiotic therapy, and antibiotic stewardship among pharmacy undergraduate students in three Asian countries. Curr Pharm Teach Learn. 2020;12(3):265–273. doi:10.1016/j.cptl.2019.12.002
28. Burger M, Fourie J, Loots D, et al. Knowledge and perceptions of antimicrobial stewardship concepts among final year pharmacy students in pharmacy schools across South Africa. S Afr J Infect Dis. 2016;31(3):7.
29. Fosnacht K, Sarraf S, Howe E, Peck L. How important are high response rates for college surveys? Rev High Ed. 2017;40(2):245–265. doi:10.1353/rhe.2017.0003
30. Hayat K, Jamshed S, Rosenthal M, et al. Understanding of Pharmacy students towards antibiotic use, resistance and antibiotic stewardship programs: a cross-sectional study from Punjab, Pakistan. Antibiotics. 2021;10(1):66. doi:10.3390/antibiotics10010066
31. Abubakar U, Sha’aban A, Mohammed M, et al. Knowledge and self-reported confidence in antimicrobial stewardship program among final year pharmacy undergraduate students in Malaysia and Nigeria. Pharm Educ. 2021;21:298–305. doi:10.46542/pe.2021.211.298305
32. Assar A, Abdelraoof MI, Abdel-Maboud M, et al. Knowledge, attitudes, and practices of Egypt’s future physicians towards antimicrobial resistance (KAP-AMR study): a multicenter cross-sectional study. Environ Sci Pollut Res Inter. 2020;27(17):21292–21298. doi:10.1007/s11356-020-08534-5
33. Meher BR, Srinivasan A, Vighnesh CS, Padhy BM, Mohanty RR. Factors most influencing antibiotic stewardship program and comparison of prefinal- and final-year undergraduate medical students. Perspect Clin Res. 2020;11(1):18–23. doi:10.4103/picr.PICR_162_18
34. Saleem Z, Hassali MA, Hashmi F, et al. Medical and pharmacy students’ knowledge, attitude, and perception concerning antimicrobial use and resistance in Pakistan. Pharm Educ. 2019;19(1):199–205.
35. Zaidi SF, Alotaibi R, Nagro A, et al. Knowledge and attitude towards antibiotic usage: a questionnaire-based survey among pre-professional students at king Saud bin Abdulaziz University for health sciences on Jeddah Campus, Saudi Arabia. Pharmacy. 2020;8:1. doi:10.3390/pharmacy8010005
36. Tripathi R, Albarraq A, Makeen H, Alqahtani S, Tripathi P, Pancholi S. Knowledge and perceptions of antimicrobial stewardship program among healthcare students in Saudi Arabia. Saudi J for Health Sci. 2020;9(2):122–129. doi:10.4103/sjhs.sjhs_192_19
37. Inácio J, Barnes LM, Jeffs S, et al. Master of Pharmacy students’ knowledge and awareness of antibiotic use, resistance, and stewardship. Curr Pharm Teach Learn. 2017;9(4):551–559. doi:10.1016/j.cptl.2017.03.021
38. Al-Shami HA, Abubakar U, Hussein MSE, Hussin HFA, Al-Shami SA. Awareness, practices and perceptions of community pharmacists towards antimicrobial resistance and antimicrobial stewardship in Libya: a cross-sectional study. J Pharm Policy Pract. 2023;16(1):46. doi:10.1186/s40545-023-00555-y
39. Jairoun A, Hassan N, Ali A, Jairoun O, Shahwan M. Knowledge, attitude and practice of antibiotic use among university students: a cross-sectional study in UAE. BMC Public Health. 2019;19(1):518. doi:10.1186/s12889-019-6878-y
40. Lubwama M, Onyuka J, Ayazika KT. Knowledge, attitudes, and perceptions about antibiotic use and antimicrobial resistance among final year undergraduate medical and pharmacy students at three universities in East Africa. PLoS One. 2021;16(5):e0251301. doi:10.1371/journal.pone.0251301
41. Okedo-Alex I, Madubueze UC, Umeokonkwo CD, Oka OU, Adeke AS, Okeke KC. Knowledge of antibiotic use and resistance among students of a medical school in Nigeria. Malawi Med J. 2019;31(2):133–137. doi:10.4314/mmj.v31i2.5
42. Thriemer K, Katuala Y, Batoko B, et al. Antibiotic prescribing in DR Congo: a knowledge, attitude, and practice survey among medical doctors and students. PLoS One. 2013;8(2):e55495. doi:10.1371/journal.pone.0055495
43. Tham DWJ, Abubakar U, Tangiisuran B. Prevalence and predictors of antibiotic use among children visiting the Emergency Department in a Tertiary Hospital in Malaysia. Eur J Pediatr. 2020;179(5):743–748. doi:10.1007/s00431-019-03560-z
44. Minen MT, Duquaine D, Marx MA, Weiss D. A survey of medical students’ knowledge, attitudes, and beliefs concerning antimicrobial use and resistance. Microb Drug Resist. 2010;16(4):285–289. doi:10.1089/mdr.2010.0009
45. Hussain I, Yousaf N, Haider S, Jalil P, Saleem MU, Imran I. Assessing Knowledge and perception regarding antimicrobial stewardship and antimicrobial resistance in university students of Pakistan: findings and implications. Antibiotics. 2021;10(7):7. doi:10.3390/antibiotics10070866
46. Sawant AP, Patil SA, Vijapurkar J, Bagban NN, Gupta DB. Is the undergraduate microbiology curriculum preparing students for careers in their field?: an assessment of biology majors’ conceptions of growth and control of microorganisms. Inter J Stem Edu. 2018;5(1):42. doi:10.1186/s40594-018-0138-z
47. Wasserman S, Potgieter S, Shoul E, et al. South African medical students’ perceptions and knowledge about antibiotic resistance and appropriate prescribing: are we providing adequate training to future prescribers? S Afr Med J. 2017;107(5):405–410. doi:10.7196/SAMJ.2017.v107i5.12370
48. Pulcini C, Cua E, Lieutier F, Landraud L, Dellamonica P, Roger PM. Antibiotic misuse: a prospective clinical audit in a French university hospital. Diseases: official publication of the European Society of Clinical Microbiology. Eur J Clin Microbiol Infect Dis. 2007;26(4):277–280. doi:10.1007/s10096-007-0277-5
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.