")
Back to Journals » Local and Regional Anesthesia » Volume 17
Knowledge, Attitudes and Practices Regarding Use of Local Anaesthetics Among Non-Anaesthesia Healthcare Professionals at Mulago National Referral Hospital
Authors Abdi IA, Kasumba JM, Wabule A, Nabukenya MT, Kayongo J, Kyoheirwe B , Sheikdon AA , Osman KD
Received 22 August 2023
Accepted for publication 19 December 2023
Published 8 March 2024 Volume 2024:17 Pages 29—37
DOI https://doi.org/10.2147/LRA.S428661
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Stefan Wirz
Intisar Ahmed Abdi,1 John Mark Kasumba,1 Agnes Wabule,1 Mary T Nabukenya,1 Joseph Kayongo,1 Bernadette Kyoheirwe,1 Abdirizak Abdullahi Sheikdon,2 Kamaludin D Osman3
1Department of Anaesthesia and Critical Care, Makerere University, Kampala, Uganda; 2Department of Orthopedics, Royal Hospital, Mogadishu, Somalia; 3Department of General Surgery, Royal Hospital, Mogadishu, Somalia
Correspondence: Intisar Ahmed Abdi, Department of Anaesthesia and Critical Care, Makerere University, Kampala, Uganda, Tel +256762635165, Email [email protected]
Introduction: Local anaesthetics (LA) are commonly used in dental and surgical emergency wards by both anaesthesia professionals and non-anaesthesia professionals. Anecdotal evidence shows that non-anaesthesia health-care professionals do not monitor vital signs during the use of local anaesthesia, and there are no standard hospital guidelines on the use of LA and management of LA toxicity by non-anaesthesia professionals.
Purpose: This study sought to assess the knowledge, attitudes and practices regarding local anaesthetic use among non-anaesthesia health-care professionals at Mulago National Referral Hospital.
Patients and Methods: This was a cross-sectional study that utilized a quantitative research approach. The sample size of the study was 43 non-anaesthesia healthcare professionals from the casualty and surgical outpatient wards and Mulago dental ward. Data was collected using a questionnaire and analyzed using STATA 15.
Results: Overall, 66.67% of the Specialist, 76.47% of the senior house officers, 100% of medical officers, and 80% of the clinical orthopedic house officers had unsatisfactory levels of knowledge in Mulago casualty and surgical outpatient wards. 20% of the specialist and 16.67% of the senior house officers had unsatisfactory levels of knowledge in Mulago dental ward. 87.5% of the non-anaesthesia health-care professionals do not give a test dose on a routine basis in Mulago casualty and surgical outpatient wards. A total of 63.64% of the non-anaesthesia healthcare professionals in Mulago dental ward do not sterilize the site of injection.
Conclusion: Non-anaesthesia health-care professionals had unsatisfactory levels of knowledge, somewhat good practices, and negative attitudes toward LA use.
Keywords: local anesthetics, LA toxicity, non-anaesthesia healthcare professionals, knowledge, attitude, practices
Introduction
Local anaesthetics are used the world over by anaesthesia and non-anaesthesia professionals in medical practice to achieve a loss of sensation to pain for invasive procedures like cannulation, debridement, surgical toilet and suture, episiotomy, circumcision, and dental procedures, among others.1 A key trend observed in the market is a significant rise in demand for post-operative pain relief options. Local anesthetics function by blocking the generation and the conduction of nerve impulses2
The global growth of day case surgeries, the prevailing global trends of private office-based surgeries, the increasing demand for chair side dental procedures, and the introduction of new and effective local anesthetic drugs with lesser side effects compared to general anesthetics are some of the motivators propelling the unmonitored use of local anesthetics by both non-anaesthesia and anaesthesia health-care professionals. In spite of records of safety set by using these drugs, there is evidence of adverse reactions to local anaesthesia ranging from 2.5% to 11%. Most of the reactions originate from the autonomic nervous system. Total perioperative mortality decreased progressively over the decades, from 10,603 per million before the 1970s, to 4533 per million in the 1970s-80s, and 1176 per million in the 1990s-2000s.3
In developing countries, there always exists a big gap between the growing population and their health-care needs. This becomes even more important to utilize the limited resources with the greatest efficiency and judiciously, at the same time. However, there is still a long way to go for developing countries to improve and implement safe anaesthesia services for all patients. Local anaesthesia-related morbidity and mortality are largely preventable in low- and middle-income countries. Several contributory factors relate to human resources, technical resources, education/teaching system, and other utilities all of which require further attention in the poor income group countries.
Developing countries like Uganda, with a history of conflicts, have a critical shortagehealthcare workers and medical resources.4 As an important part of medical services, anaesthesia services are particularly susceptible to the level of socio-economic development.5 The lack of proper education in anaesthesia in most of developing countries remains an area of great concern. The non-availability and shortage of teaching staff adversely affect the training of residents, medical students and nurses.6 Therefore, without proper knowledge and monitoring during the practice of providing LA, complications occur7 and the risk of LA toxicity remains a high concern for most clinicians. Local anesthetic systemic toxicity (LAST) is a life-threatening adverse event associated with the increasingly prevalent utilization of local anesthetic (LA) techniques throughout various healthcare settings (Mulago hospital inclusive), with an incidence estimated to be 0.03%, or 0.27 episodes per 1000 peripheral nerve blocks.8
Although LA is being used in different hospital settings, it has severalside effects and possibilities of rare but serious complications. LAs have the possibility to produce various toxic effects in many tissues, especially heart and brain. All LAs have similar toxicity to some extent. However, the intensity of the toxicity varies among LAs, according to the chemical structure.9 Toxicity may result from inadequate administration in cases of high doses and inappropriate site of administration.10 Acute neurotoxicity and cardiac toxicity are derived from unexpectedly high serum concentration. Allergic reactions are also observed in some cases, especially following the use of ester structure drugs. Chronic toxicity is provoked when nerve fibers are exposed to local anesthetics at a high concentration for a long duration.11
Nonetheless, there are limited data on knowledge, attitudes and practices regarding local anesthetic use among non-anaesthesia health-care professionals both globally and locally. Therefore, this study aimed to determine the knowledge, attitudes and practices regarding local anaesthetic use among non-anaesthesia health-care professionals at Mulago National Referral Hospital.
Materials and Methods
This study used a cross-sectional research design and a quantitative research approach. The sample size was 43 (determined using Yamane’s (1967) formula) non-anaesthesia health-care professionals (11 from Mulago dental ward and 32 from casualty and surgical outpatient ward). Simple random sampling was used to select participants. Data was collected using a questionnaire. Data was analyzed using STATA 15 through the use of descriptive statistics. This study was approved by the Research Ethics Committee. Informed consent was obtained from each study participant.
Results
Questionnaires were administered to all the 43 non-anaesthesia health-care professionals. The response rate of the study was 100%. The non-anaesthesia health-care professionals in Mulago casualty and surgical outpatient ward were 3 specialists, 17 senior house officers, 7 medical officers and 5 clinical orthopedic house officers. The mean age was 32±4.55 years. Majority of the non-anaesthesia health-care professionals were male (87.50%) (Table 1). The non-anaesthesia health-care professionals in Mulago dental ward were 5 specialists and 6 senior house officers. Majority (63.64%) were males. 64.63% of the non-anaesthesia health-care professionals had experience in administering LA of 20 years and above. The mean age of the non-anaesthesia health-care professionals was 44 ±11.23 years (Table 2). Table 3 shows that regarding the toxic dose of Lidocaine, 46.88% were knowledgeable while 53.13% were not knowledgeable. Similarly, while 21.88% were knowledgeable about the toxic dose for bupivacaine, 78.13% of the non-anaesthesia health-care professionals were not knowledgeable. Table 4 shows that 72.73% were knowledgeable of toxic dose of Lidocaine, while 27.27% were not knowledgeable. Similarly, while 18.18% were knowledgeable about the toxic dose for bupivacaine. Figure 1 shows that with regard to the level of knowledge, 66.67% (2) of the specialists had an unsatisfactory level of knowledge, 76.47% (13) of the senior house officers had an unsatisfactory level of knowledge, 100% (7) of the medical officers had an unsatisfactory level of knowledge and 80% (4) of the clinical orthopedic house officers had an unsatisfactory level of knowledge. Figure 2 shows that with regard to the level of knowledge, 20% (1) of the specialist had an unsatisfactory level of knowledge, 16.67% (1) of the senior house officers had an unsatisfactory level of knowledge. On the other hand, 80% (4) of the specialist had very satisfactory knowledge and 33.33% (2) of the senior house officers had very satisfactory knowledge.
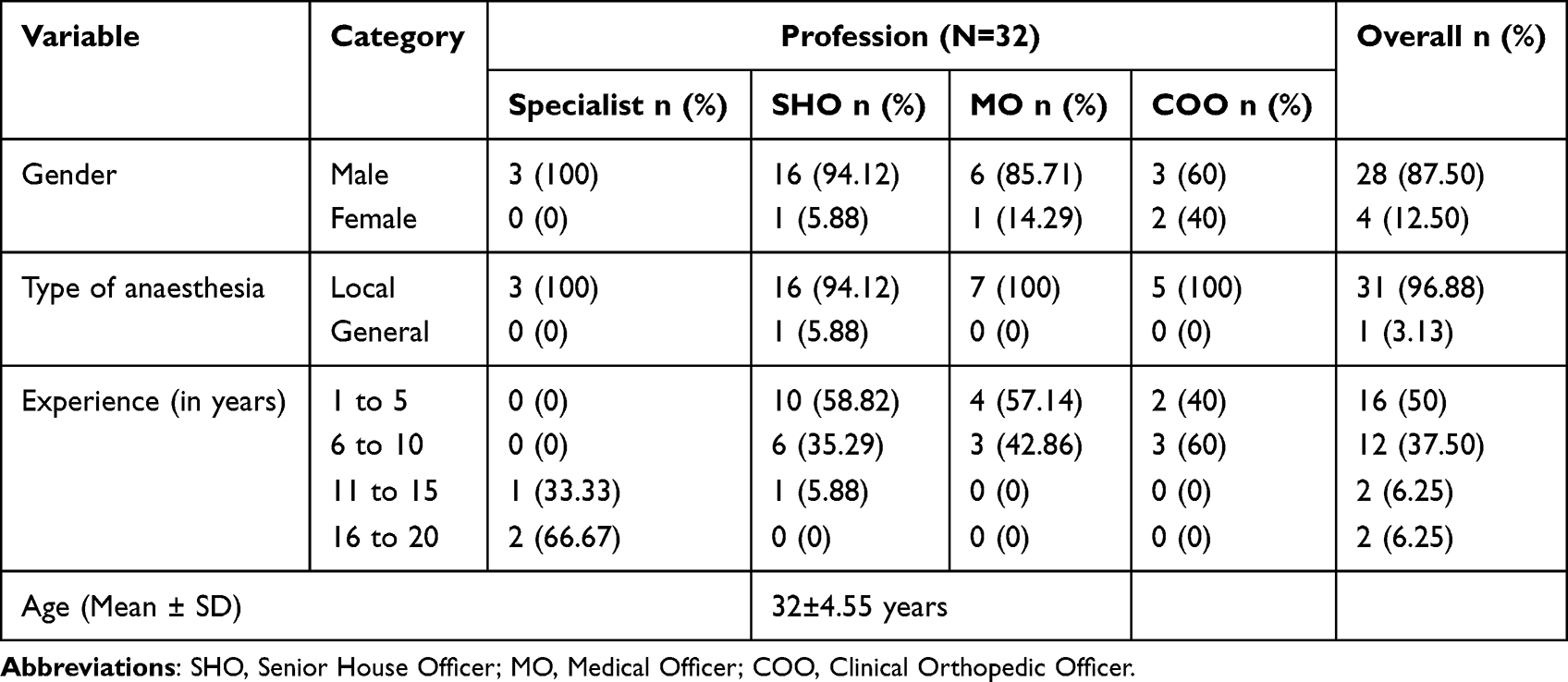 |
Table 1 Details of Non-Anaesthesia Healthcare Professionals in Mulago Casualty and Surgical Outpatient Wards |
 |
Table 2 Details of Non-Anaesthesia Healthcare Professionals in Mulago Dental Ward |
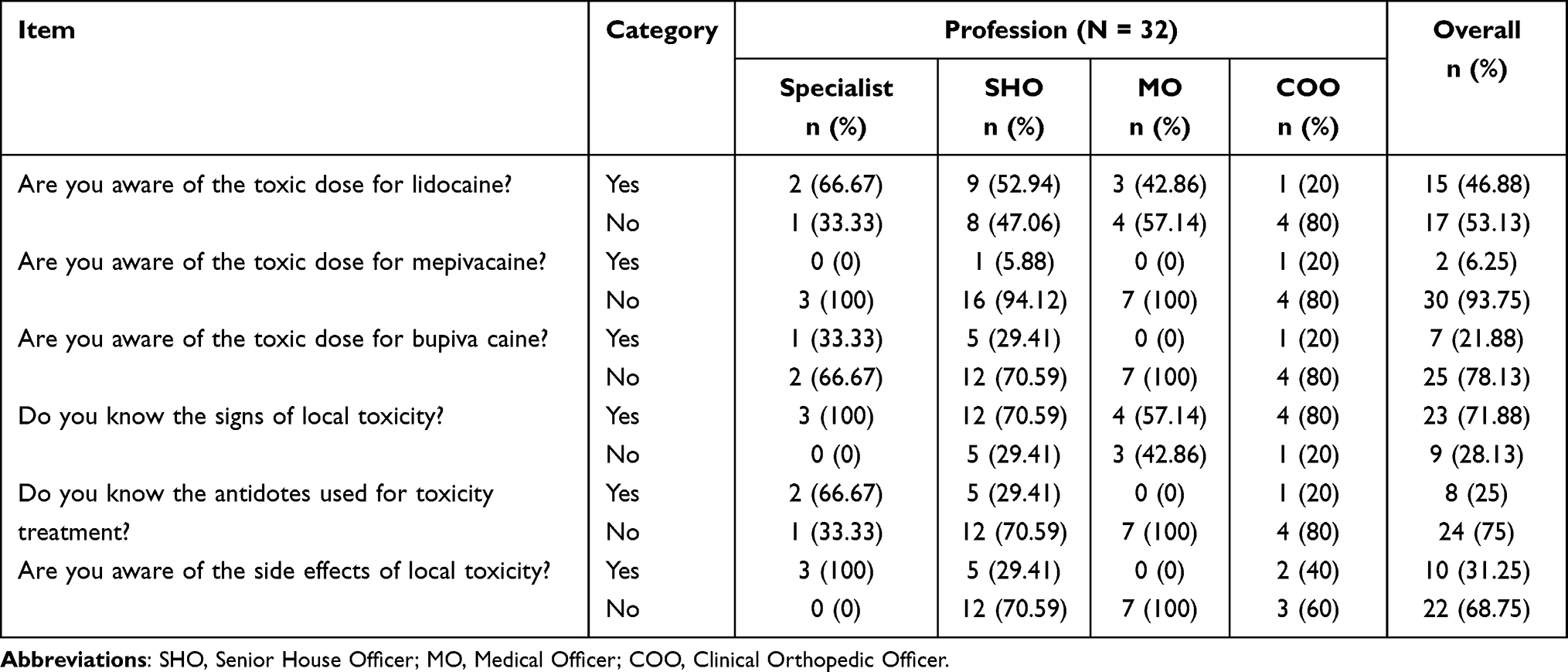 |
Table 3 Knowledge About Local Anesthetic Use Among Non-Anaesthesia Health Professionals at Mulago Casualty and Surgical Outpatient Wards |
 |
Table 4 Knowledge About Local Anesthetic Use Among Non-Anaesthesia Health Professionals at Mulago Dental Ward |
 |
Figure 1 Level of Knowledge of non-anesthesia health care professionals at Mulago casualty and surgical outpatient wards. |
 |
Figure 2 Level of knowledge of non-anesthesia healthcare professionals in Mulago dental ward. |
Table 5 shows that 71.88% of non-anaesthesia health-care professionals do not administer LA to all patients in the same way. A total of 87.5% of the non-anaesthesia health-care professionals opined that there are no guidelines availed on how to administer LA in their department (100% of the specialist, 82.35% of the senior house officers, 85.71% of the medical house officers and 100% of the C.O.H.O). Table 6 shows that a total of 81.82% of non-anaesthesia health-care professionals do not administer LA to all patients in the same way (80% of the specialists, 83.33% of the senior house officers). Similarly, 72.73% of the non-anaesthesia health-care professionals do not test for LA allergy before injecting LA to patients (80% of the specialists and 66.67% of the senior house officers). Figures 3 and 4 show a total of 84.38% (27) of the non-anaesthesia health-care professionals sterilize the site of injection (100% (3) of the specialists, 82.35% (14) of the senior house officers, 85.71% (6) of the medical officers, and 80% (4) of the clinical orthopedic officers). In addition, 93.75% (30) of the non-anaesthesia health-care professionals aspirate while administering LA (100% (3) of the specialists, 94.12% (16) of the senior house officers, 85.71% (6) of the medical officers, and 100% (5) of the clinical orthopedic officers). Figures 5 and 6 show a total of 63.64% (7) of the non-anaesthesia health-care professionals (83.33% (5) of the senior house officers and 40% (2) of the specialists) in the Mulago dental ward do not sterilize the site of injection. On the other hand, 90.91% (10) of the non-anaesthesia health-care professionals in the Mulago dental ward (100% (5) of the specialists and 83.33% (5) of the senior house officers) aspirate while administering LA.
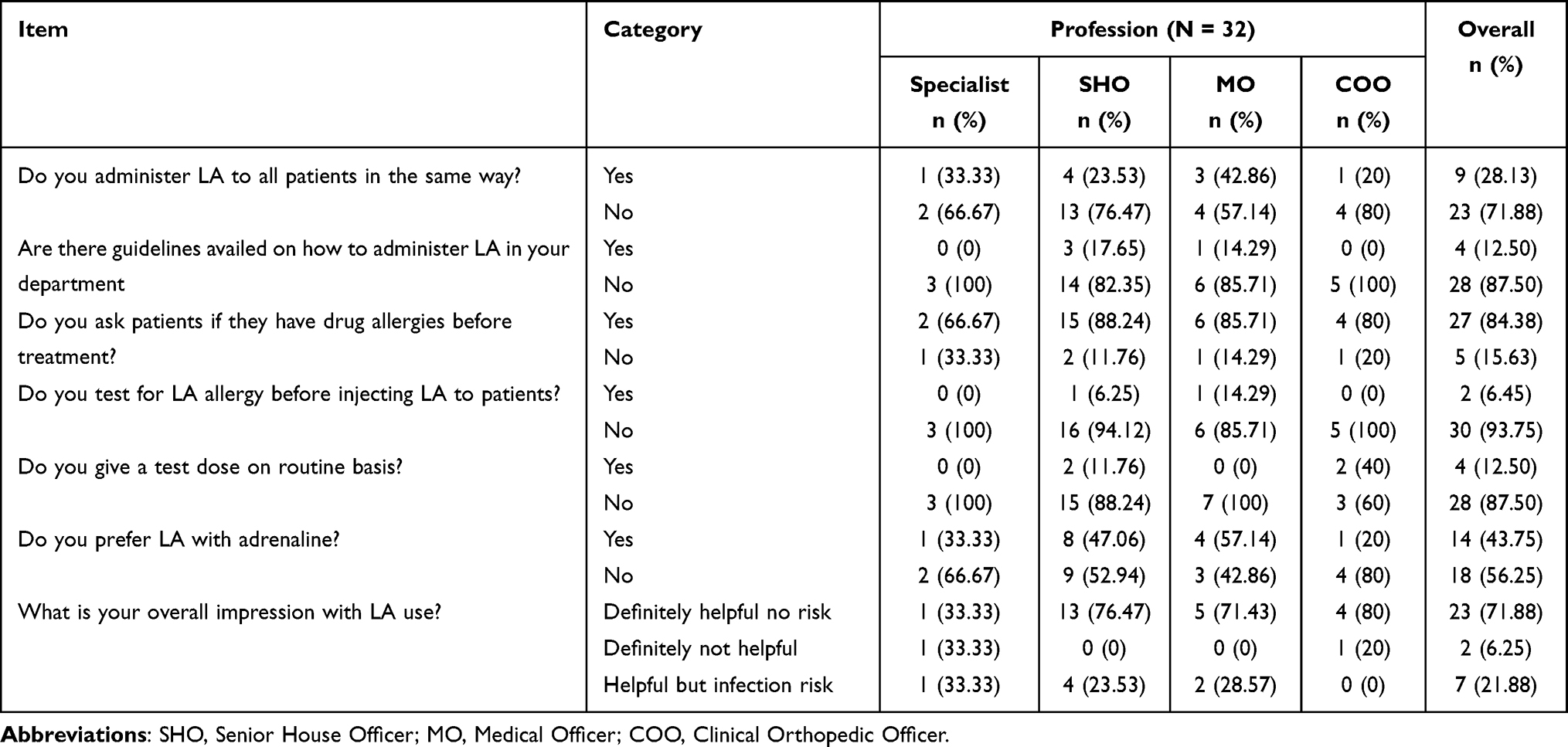 |
Table 5 Attitude About Local Aesthetic Use Among Non-Anaesthesia Health-Care Professionals at Mulago Casualty and Surgical Outpatient Wards |
 |
Table 6 Attitude About Local Aesthetic Use Among Non-Anaesthesia Health-Care Professionals at Mulago Dental Ward |
 |
Figure 3 Sterilization of injection site non anaesthesia healthcare professional at Mulago catualty and surgical outpatient. |
 |
Figure 4 Aspiration while administering LA non anaesthesia healthcare professional at Mulago catualty and surgical outpatient. |
 |
Figure 5 Sterilization of injection site non anaesthesia healcare professional at Mulago dental word. |
 |
Figure 6 Aspiration while administering LA non anaesthesia healthcare professional at Mulago dental word. |
Discussion
The study's finding of 46.88%, non-anaesthesia health-care professionals in Mulago casualty and surgical outpatient wards knowledgeable about the toxic dose for lidocaine, is two times the findings of Lopez et al where it was reported that toxic dose for lidocaine was only known by 21% of respondents (36.6% anaesthesiologists; 5% surgeons). The study findings that 21.88% of the non-anaesthesia health-care professionals in Mulago casualty and surgical outpatient ward and 18.18% of the non-anaesthesia health-care professionals in Mulago dental ward being knowledgeable of the toxic dose for Bupivacaine are much lower than the findings of Lopez et al where 46.9% (85.4% anaesthesiologists, 7.5% surgeons) had knowledge of the toxic dose of Bupivacaine. The study findings regarding knowledge about toxic doses of Lidocaine and Bupivacaine in our setting are a clear representation of choice of local anaesthetic familiarity. In like manner, the findings regarding knowledge about the toxic dose of Mepivacaine in this study, 6.25%, clearly demonstrate the lack of access to this drug in our setting when compared to the findings in the study by Lopez et al where it was revealed that the toxic dose for mepivacaine was known by 19.8% (36.6% anaesthesiologists; 2.5% surgeons). This study found that antidote toxicity treatment was known by 25% of the non-anaesthesia health-care professionals in Mulago casualty and surgical outpatient ward disagrees with the findings of Lopez et al where the researchers reported that toxicity treatment was known by 59.3% (87.8% anaesthesiologists; 30% surgeons). However, this study result which shows that 90.91% of the non-anaesthesia health-care professionals in Mulago dental ward are in line with the findings of Lopez et al.
This study’s findings show that 43.75% of the non-anaesthesia health-care professionals in Mulago casualty and surgical outpatient and 90.91% of the non-anaesthesia health-care professionals in Mulago dental ward prefer LA with adrenaline corroborates with the results of a study carried out by Krishnamurthy et al where it was reported that 98% of the dentists preferred local anesthetic with adrenaline. This study results which revealed that 72.73% of the non-anaesthesia health-care professionals in Mulago dental ward and 93.75% of the non-anaesthesia health-care professionals in Mulago casualty and surgical outpatient do not test for LA allergy before injecting LA to patients disagrees with the findings of Das et al where it was established that 85.5% of the clinicians admitted testing for LA allergy before injecting LA to the patient. However, this study's findings also confirm the results of a study carried out amongst dentists by Krishnamurthy et al where it was reported that only 3% admitted that they give test dose on a routine basis, implying that majority of the participants do not give test dose on a routine basis. This study’s finding which shows that 93.75% of the non-anaesthesia health-care professionals in Mulago casualty and surgical outpatient ward and 90.91% of the non-anaesthesia health-care professionals in Mulago dental ward aspirate while administering LA is in stark contrast with the findings of a study carried out by Khalil (2014) that only 4% of the participants performed injection aspiration in all LA injection techniques.12 This finding also diverges from the findings of a study carried out by Kaira and Dabral (2014) which indicated that a total of 49% of general dental practitioners and specialists do not perform aspiration when injecting local anesthetics.
Conclusion
Non-anaesthesia health-care professionals in Mulago casualty, surgical outpatient and Mulago dental (46.88% and 21.88%, respectively) are more knowledgeable about the toxic dose and signs of local anaesthetic toxicity for Lidocaine than Bupivacaine. Non-anaesthesia health-care professionals lack knowledge about the toxic dose of Mepivacaine (93.75%). Non-anaesthesia health-care professionals in Mulago prefer LA with adrenaline. More than 70% of non-anaesthesia health-care professionals do not test for LA allergy before injecting LA into patients. More than 84% of non-anaesthesia health-care professionals will ask their patients whether they have drug allergies before administering local anaesthetics. 90.91% of the non-anaesthesia health-care professionals in Mulago aspirate while administering LA.
Acknowledgments
The Author would like to thank with gratitude the assistance, patience, help, guidance, support and advice from Dr John Mark Kasumba, Dr Agnes Wabule and Dr Mary T Nabukenya.
Disclosure
No conflict of interests have been declared by the authors.
References
1. Becker DE, Reed KL. Essentials of local anesthetic pharmacology. AnaesthesiaProgress. 2006;53(3):98. doi:10.2344/0003-3006(2006)53[98:EOLAP]2.0.CO;2
2. EA Health. Mulago National Referral Hospital. EA Health; 2020. Available from: www.eahealth.org.
3. Bainbridge D, Martin J, Arango M, Cheng D; Evidence-based Peri-operative Clinical Outcomes Research (EPiCOR) Group. Perioperative and anaesthetic-related mortality in developed and developing countries: a systematic review and meta-analysis. Lancet. 2012;380:1075–1081. doi:10.1016/S0140-6736(12)60990-8
4. Liverani M, Nguon C, Sok R. Improving access to health care amongst vulnerable populations: a qualitative study of village malaria workers in Kampot, Cambodia. BMC Health Serv Res. 2017;17(1):335. doi:10.1186/s12913-017-2282-4
5. Nyberger K, Jumbam DT, Dahm J. The situation of safe surgery and anaesthesia in Tanzania: a systematic review. World J Surg. 2019;43(1):24–35. doi:10.1007/s00268-018-4767-7
6. McQueen KA, Malviya S, Gathuya ZN, Tyler DC. International advocacy for education and safety. Paediatr Anaesth. 2012;22:962–968. doi:10.1111/pan.12008
7. Weiniger CF, Golovanevski L, Domb AJ, Ickowicz D. Extended release formulations for local anaesthetic agents. Anaesthesia. 2012;67(8):906–916. doi:10.1111/j.1365-2044.2012.07168.x
8. El‐Boghdadly K, Pawa A. The erector spinae plane block: plane and simple. Anaesthesia. 2017;72(4):434–438. doi:10.1111/anae.13830
9. Anesthetics L. R H Hoffman, Goldfrank’s Toxicologic Emergencies (10 Ed). McGraw‐Hill Education; 2015.
10. Veering BT. Complications and local anaesthetic toxicity in regional anaesthesia. Curr Opin Anaesthesiol. 2003;16(5):455–459. doi:10.1097/00001503-200310000-00004
11. Sekimoto K, Tobe M, Saito S. Local anesthetic toxicity: acute and chronic management. Local Anesth Acute Med Surg. 2017;4(2):152–160.
12. Khalil H. Local anesthetics dosage still a problem for most dentists: a survey of current knowledge and awareness. Saudi J Dent Res. 2014;5(1):49–53. doi:10.1016/j.ksujds.2013.08.002
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.