")
Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 16
Knowledge, Attitude and Practice of Toothbrush Contamination and Disinfection Among Undergraduate Students in Selected Universities in Somalia
Authors Hussein SA , Hussein AA, Nur AM, Ali AN, Mohamed YG , Ali AJA
Received 8 November 2023
Accepted for publication 17 February 2024
Published 22 February 2024 Volume 2024:16 Pages 33—40
DOI https://doi.org/10.2147/CCIDE.S448793
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Christopher E. Okunseri
Saadaq Adan Hussein,1 Abdirahman Aden Hussein,2 Ahmed Mohamed Nur,3 Ayan Nor Ali,4 Yahye Garad Mohamed,4 Abdul Jalil Abdullahi Ali3
1Department of Tropical and Infectious Diseases, Benadir University, Mogadishu, Somalia; 2Department Public Health, Ministry of Livestock, Forestry & Range, Mogadishu, Somalia; 3Department of M&E Statistic, Benadir University, Mogadishu, Somalia; 4Department Radiology, Mogadishu Somali Türkiye Training and Research Hospital, Mogadishu, Somalia
Correspondence: Saadaq Adan Hussein, Department of Tropical and Infectious Diseases, Benadir University, Bundada Street, Wabari District, Mogadishu, Somalia, Tel +252612223224, Email [email protected]
Background: Oral health is crucial for overall well-being and systemic health and Humans are exposed to several bacteria after birth and will causes systemic illnesses like septicemia, respiratory, gastrointestinal, and renal issues. This study aimed to evaluate undergraduate students’ knowledge, attitudes, and practices regarding toothbrush contamination and disinfection.
Methods: A descriptive cross-sectional study was carried out with undergraduates from seven selected universities, including public and private universities. A closed-ended questionnaire containing 24 items was distributed to A total of 490 undergraduate students.
Results: The study showed that (28.6%, n=140) had knowledge about toothbrush cleaning and disinfection. A total of (350, n=71.4%) needed to gain knowledge about toothbrush cleaning and disinfection. Fifty-two percent of the students feel that bacteria are the primary mode of toothbrush contamination. Many of the students had different ways of disinfecting toothbrushes, including, boiling a small pot of normal water (51.4%, n=252), chemical agent (31.8%, n=156), ultraviolet sanitizer (0.2%, n=4), and microwave radiation (0.2%, n=1) does not know (16.1%, n=79). Most students (76.9%, n=377) felt that toothbrush disinfection was necessary.
Conclusion: Fewer students have sufficient knowledge about toothbrush contamination and practice disinfection methods, whereas most students need to be made aware of the contamination of toothbrushes and the use of disinfectant methods.
Keywords: knowledge, practice, toothbrush, infection, contamination
Background
Dental caries and periodontitis are both gum diseases that have been prevalent worldwide for the past three decades.1 They are also the two most common oral diseases.2 The most serious oral cavity cancer, squamous cell carcinoma (SCC), originates from the mucosal epithelium and accounts for over 90% of cases.3 Oral health is crucial for overall well-being and systemic health.4 After birth, humans are exposed to several bacteria.5 and for various ages, they use toothbrushes to clean their mouths.6 Globally, squamous cell carcinoma is the sixth most common oral cancer.7,8 Oral diseases affect 3.5 billion people, including 514 million children and 2 billion adults.9 More than 50% of the population, mostly adults, is affected by gum disease.10 Despite being preventable and inexpensive to treat, oral disorders have received little attention from the medical community,11 Millions of germs are found in the oral cavity12 and in a 1920 paper, Cobb was the first to address this issue.13 There are hundreds of bacterial species, fungi, viruses, and transient microorganisms in the oral cavity.14 Toothbrushes can be contaminated with germs, body fluids, and toothpaste when used to clean off soft debris like plaque from teeth.12 Therefore, brush disinfection is crucial to remove harmful bacteria.15 Factors such as an unhealthy, high-sugar diet, excessive tobacco use, and problematic alcohol consumption can contribute to poor dental health.16 This, in turn, can lead to various illnesses, including endocarditis, cardiovascular disease, pregnancy and childbirth complications, pneumonia, osteoporosis, and Alzheimer’s disease,17 as well as systemic illnesses like septicemia, respiratory, gastrointestinal, and renal issues.18 It is crucial to thoroughly clean toothbrushes to prevent infections, particularly in susceptible individuals like young children, the elderly, and those with compromised immune systems.19 Despite its importance, oral health remains a low priority, greatly burdening families, and individuals, increasing the risk of disability, decreasing quality of life, and creating social isolation and socioeconomic disparity.20 The African continent has 47 countries,20 and oral cancer is most prevalent in developing nations,7,8 In Africa, 480 million people, or 43.7% of the total population, face oral diseases.20 Most sub-Saharan African countries, about 70%, spend less than $1 per person annually on dental treatment,21 and face inadequate health workforce capabilities,22 despite having the highest population growth rate globally of 2.8%.23 Antimicrobial rinses and sprays, or covering toothbrush bristles with toothpaste or antimicrobial gel, have been studied as ways to disinfect toothbrushes.24 Therefore, our study aims to determine the knowledge, attitudes, and practices of undergraduate students at select Somali universities regarding toothbrush contamination and disinfection. Despite the importance of this topic, there is a lack of readily available studies in Somalia. Hence, this study will attempt to fill this gap and provide valuable insights for future research and healthcare interventions.
Methodology
A descriptive cross-sectional study was conducted with undergraduate students from seven selected universities, both public and private, after obtaining ethical approval from the Ethics Committee of the Ministry of Health and Human Services, Federal Government of Somalia. From November 15, 2022, to April 15, 2023, a total of 490 undergraduate students between the ages of 18 and 30 were enrolled and obtained written, informed consent from all participants. All of the universities included in the study have been accredited by the Ministry of Education, Culture, and Higher Education of Somalia. There is one public university and six private universities. The public university, Somali National University, the private universities included in the study are Zamzam University of Science and Technology, Al Hayat Medical University (AMU), Salaam University (SU), Somali International University, SIMAD University, Horseed International University (HIU), and they are all located in Mogadishu. A modified version of previously published research25 was used to create a closed-ended questionnaire with 24 items, which were administered through individual interviews conducted at the participants’ convenience. The survey included crucial questions about participants’ knowledge, attitudes, and practices regarding toothbrush contamination and disinfection, covering four main areas: 1) Demographics, such as gender, age, marital status, academic year, and faculty of study. 2) Knowledge about cleaning and disinfecting toothbrushes and which microorganisms can cause contamination. 3) Attitudes, including the standard way of transmitting infections through a toothbrush and improving oral hygiene. 4) Practices such as disinfecting and storing toothbrushes All eligible participants were directly interviewed in person to complete the questionnaire, which included both open-ended and closed-ended questions. For the knowledge assessment, each positive answer was scored as 1, while a negative answer was scored as 0. Overall knowledge scores ranged from 0 to 8, with scores of 0 to 3 classified as poor knowledge and scores above 3 considered good knowledge. Toothbrush contamination and disinfection practices were assessed using a 6-point questionnaire, with scores between 0 and 3 indicating poor practice and scores between 4 and 6 indicating good practice. A pilot study26 was conducted before data collection, and final changes were made to the questionnaire after discarding items that did not yield useful information. The data was collected, processed, coded, and entered into Kobo Collect, and then statistical analysis and the chi-square test were used to examine the results using SPSS Statistics, Version 25.0. Armonk, NY: IBM Corp. Using Cronbach’s internal consistency measure, the questionnaire’s Differences with a p-value of less than 0.05 were considered statistically significant Interviews were conducted on university campuses based on the studies of the participants, with each interview lasting approximately 15–25 minutes. This approach allowed for the collection of valuable insights from undergraduate students from seven selected universities, both public and private, in Mogadishu, Somalia.
Results
The survey was responded to by 490 students in total, of whom 41.4% (203) were male and 287 (58.5%) were female. Students’ ages ranged from 18 to 30 (mean age ± standard deviation: 21.1–0. ± 0.3 years). Study participants were laboratory students (112–22.9%), medical students (79–16.1%), midwife students (36–7.3%), nurse students (139–28.4%), public health students (108–22.0%), and others (16–3.3%) [Table 1]. Overall, 71.4% (350) had no knowledge about toothbrush contamination. The sources of information about toothbrush contamination and disinfection were medical (45.1%; 221), social media platforms (43.9%; 215), and unknown (11.0%; 54). This difference between information sources was found to be statistically significant (P<0.05). Most students felt that toothbrush disinfection was necessary (76.9%, 377); and 70.8% (347) of students believed that disinfection was necessary for everyone (29.2%, 143). In special patient groups such as immunocompromised individuals, hospital patients, and children, a statistically significant difference (<0.05*) was observed between students who felt they needed to disinfect their toothbrushes and those who felt disinfection was not necessary. Approximately 33.5% (164) of students felt like sharing toothpaste with other people, and other students did not feel like sharing toothpaste with other people, 66.5% (326), a statistically significant difference between the two groups (P value < 0.05*). Approximately 76.9% (377) of students believed that contact between toothbrushes was the primary concern, and 23.1% (113) believed it was not necessary. A statistically significant difference was observed (P < 0.05). Many students thought that the microorganisms causing toothbrush contamination were bacteria (52%; 255), fungi (13.5%; 66), viruses (7.3%; 133), or they did not know (27.1%). Student perceptions of toothbrush contamination and its impact on systemic disease were 80% (392), 19.9% (97) unrelated, and 0.1%.1 The student believed that the main causes of toothbrush contamination were contact with other toothbrushes (62.0%), the external environment (31.8%), the oral cavity (3.5%), and I do not know (2.7%) [Table 2]. Ninety percent (441) of students believed that a dirty toothbrush could cause oral disease, while 10% (49) believed it. Statistically significant differences were found (P value <0.05*). The primary method of infection transmission through a toothbrush was sharing the same toothbrush holder (14.1%, 69). The primary method of toothbrush infection transmission was sharing the same toothbrush holder (14.1%, 69), toothbrush sharing 68.2% (334), and toothpaste sharing 17.8% (87). The majority of students, 34.5% (169), rated their oral hygiene as excellent, 62.2% (305) as good, and 3.3%16 as poor. The difference in self-assessment of oral hygiene between the students was also statistically significant (P 0.05) [Table 3]. Approximately 42.9% (210) of students used disinfectant on their toothbrushes, while 57.1% (280) did not. Many students reported that 4.5%22 shared their toothbrushes with others, and 95.5% (468) kept them separate from others. The majority of students, 93.7% (459), brushed their teeth twice a day, 2.7%13 brushed their teeth more than three times, and 3.7%18 brushed their teeth one day. Many students change their toothbrushes every two months (33.1% of 162), monthly (64.9% of 318), every three months (1.2% of 6), and every three months or more often (0.8% of 4). The majority of students use various methods to disinfect toothbrushes. Boil a small pot of normal water: 51.4% (252), chemical agent 31.8% (156), UV disinfectant 0.2%,4 microwave radiation 0.2%,1 and, I know not, 16.1% of 79. Most of them the students reported that they kept their toothbrushes in open contact with the environment in the bathroom (8.6% of 42), in a closed cabinet in the bathroom (5.7% of 28), outside the bathroom in a closed cupboard (67.1% of 329), and outside the bathroom in open contact with the environment (18.6% of 91) [Table 4].
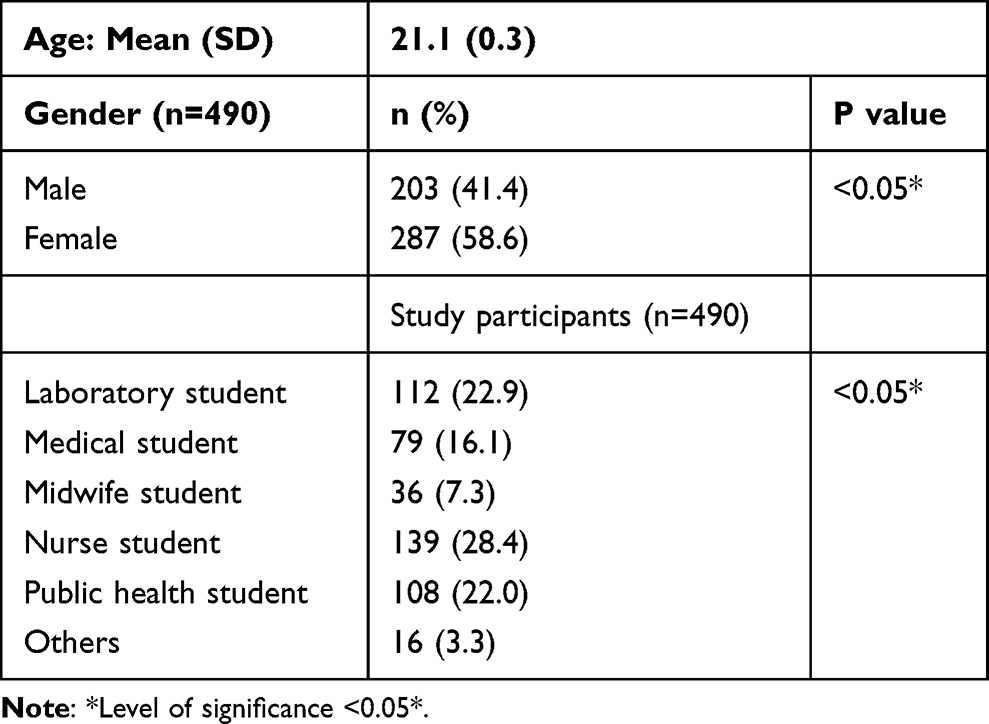 |
Table 1 Distribution of Study Participants Based on Age, Gender, and Study Participants |
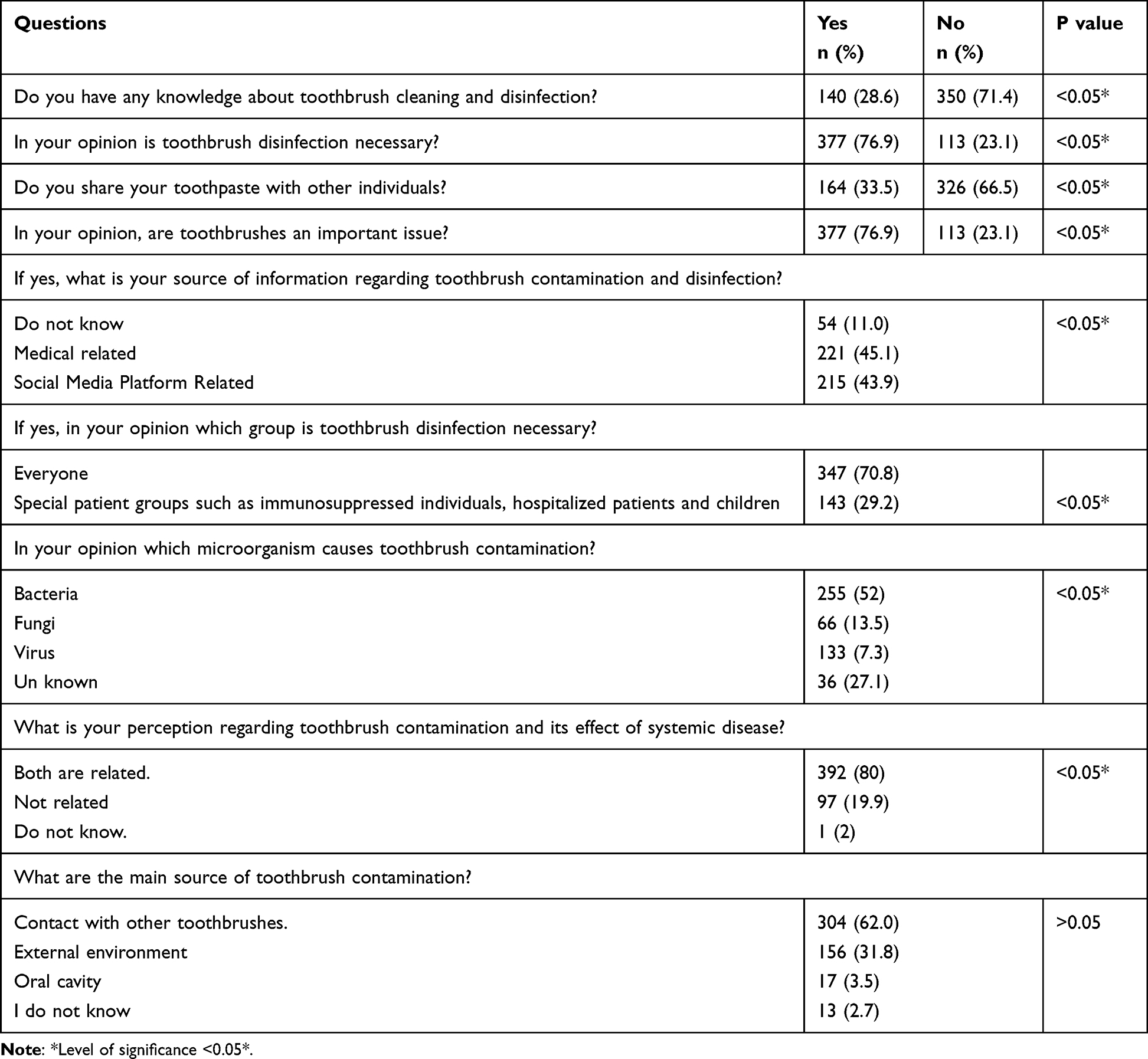 |
Table 2 Knowledge Regarding Toothbrush Contamination and Disinfection Among Study Participants |
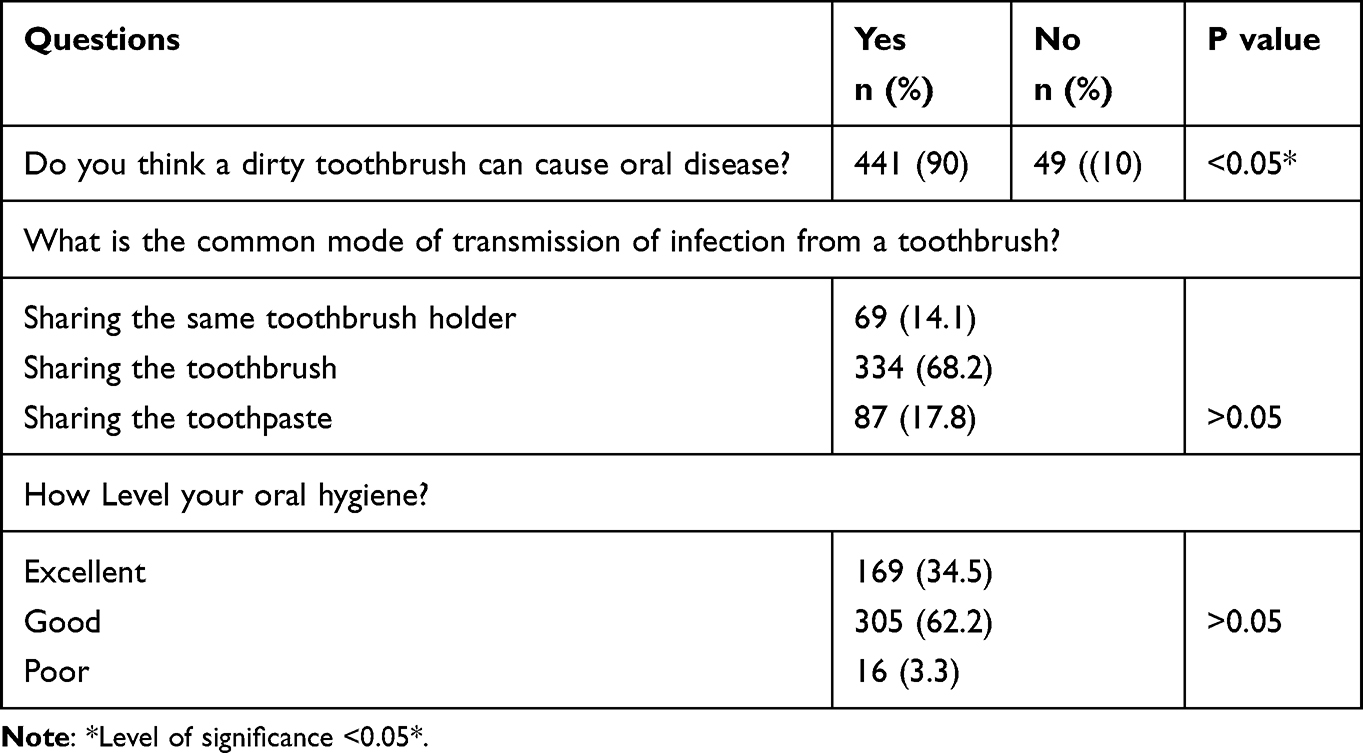 |
Table 3 Attitudes Regarding Toothbrush Contamination and Disinfection Among Study Participants |
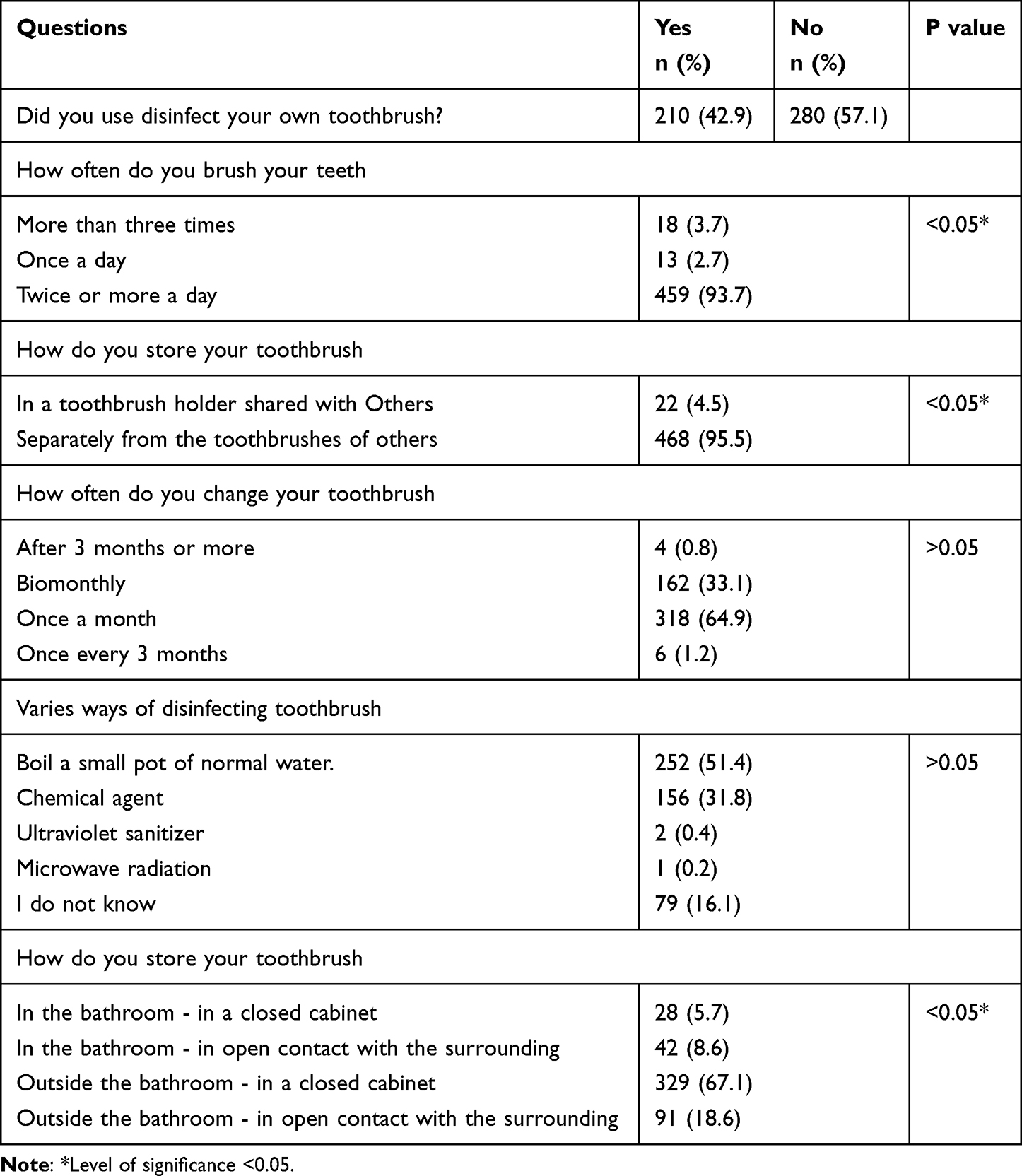 |
Table 4 Practices Regarding Toothbrush Contamination and Disinfection Among Study Participants |
Discussion
The survey assessed undergraduate students’ knowledge, attitudes, and practices regarding toothbrush contamination and disinfection. Toothbrushes have become a crucial tool for maintaining oral hygiene and preventing diseases due to their significant role in preventative dental care.25 There was a statistically significant difference between students who knew about toothbrush disinfection and those who did not, similar to study of Knowledge and behavior of undergraduate students in a dental school regarding toothbrush disinfection which showed that, approximately 50% and 47% of participants did not have any knowledge of toothbrush disinfection and did not disinfect their own toothbrushes, respectively.1 In 70.8% of cases, disinfection was required for everyone. Approximately 66.5% do not share toothpaste individually with others. The results of this study are similar to previous study which reported 86.32% of the students felt that sharing the toothbrushes was the usual mode of infection transmission from a toothbrush and 78.92% felt that bacteria were capable of causing toothbrush contamination.2 Nearly 76.9% of students felt that contact between toothbrushes was the greatest concern. According to 52% of students, bacteria are the most common microorganism that causes toothbrush contamination. Several studies have shown that bacteria are the main cause of contaminated toothbrushes.3–5 In 70.8% of cases, disinfection was required for everyone. Approximately 66.5% do not share toothpaste individually with others. Almost 76.9% of students felt that contact between toothbrushes was the greatest concern. According to 52% of students, bacteria are the most common microorganism that causes toothbrush contamination. The research results are consistent with those of other studies. Several studies have found that bacteria are the main cause of contaminated toothbrushes.27 Eighty percent of students’ perceptions of toothbrush contamination and its impact on systemic diseases are related. A total of 62.0% (304) believed that the main cause of toothbrush contamination was contact with other toothbrushes, and 90% (441) believed that a dirty toothbrush can cause oral diseases. Sharing toothbrushes (68.2%) was found to be the most common type of infection transmission through a toothbrush in the current study. Many students (34.5%) rated their oral hygiene as excellent, 62.2% as good and 3.3% as poor. The difference in self-assessment of oral hygiene between students was also statistically significant (P < 0.05). Approximately 42.9% (210) of students used disinfectant on their own toothbrushes, while 57.1% (280) did not. In this study, 95.5% (468) of students reported that they stored their toothbrushes in a toothbrush holder separate from other people’s toothbrushes. Several research studies that examined the oral health attitudes and habits of students in different countries found that many students brushed their teeth at least twice a day.28 In the present study, many students (93.7% of 459) brushed their teeth twice daily and often changed their toothbrush once a month (64.9% of 318).25 Brushes can become contaminated by bacteria from the oral cavity or the surrounding air if they are stored in a damp place without disinfection after use29 Most students disinfecting toothbrushes boil them in a small pot of normal water (51.4%). Most students reported storing their toothbrushes outside the bathroom in a closed cabinet (67.1%). A few of the limitations of this study were: using a convenient sample method may have limited the generalizability of our study’s results; and the cross-sectional survey design restricted our ability to demonstrate a causal association between study variables.
Conclusion
A survey revealed that a significant number of students lack knowledge about toothbrushes and do not disinfect them, indicating a lack of awareness about oral hygiene practices. This highlights the need for increased education on toothbrush disinfection and good oral hygiene. Dentists can help address this issue by raising awareness through campaigns, workshops, seminars, collaborations with educational institutions, distribution of information materials, and community events. By taking proactive measures, dentists can educate individuals about toothbrush disinfection and encourage good oral hygiene habits, ultimately contributing to better overall oral health and preventing long-term dental problems.
Data Sharing Statement
The data that support the findings of this study are will be made available from the corresponding author upon reasonable request.
Ethical Statement
This study subjects were conducted in accordance with the Declaration of Helsinki guidelines. Ethical approval was obtained from the institutional Ethics committee of Ministry of health and human Services Federal Government of Somalia, with the reference number (115/23).
Consent
Informed consent was obtained from all participants involved in the study. Participants were briefed about the nature of the study, potential risks, benefits, and their rights, and written consent was obtained prior to their participation. The confidentiality and anonymity of human subjects were rigorously maintained throughout the study. Identifying information has been appropriately anonymized to protect the privacy of participants.
Acknowledgment
The authors would like to express their appreciation for the support and resources that contributed to the completion of this study. While there are no specific individuals to acknowledge, we are grateful for universities that facilitated our work.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study received no specific grant from any funding agency, and there is no funding support to this study.
Disclosure
The authors declare no conflicts of interest related to the study, including financial, personal, or other relationships that may influence the study or its interpretation.
References
1. Kumar A, Grover V, Satpathy A, et al. ISP good clinical practice recommendations for gum care. J Indian Soc Periodontol. 2023;27(1):4. doi:10.4103/jisp.jisp_561_22
2. (PDF) awareness of tooth brushing techniques and proper oral hygiene among school children [Internet]; 2023. Available from: https://www.researchgate.net/publication/281765868_Awareness_of_tooth_brushing_techniques_and_proper_oral_hygiene_among_school_children.
3. Gupta N, Gupta R, Acharya AK, et al. Changing trends in oral cancer - a global scenario. Nepal J Epidemiol. 2016;6(4):613. doi:10.3126/nje.v6i4.17255
4. 3 num [Internet]; 2023. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4535112/pdf/JFMPC-4-444.pdf.
5. Raiyani CM, Arora R, Bhayya DP, Dogra S, Katageri AA, Singh V. Assessment of microbial contamination on twice a day used toothbrush head after 1-month and 3 months: an in vitro study. J Nat Sci Biol Med. 2015;6(Suppl 1):S44. doi:10.4103/0976-9668.166072
6. Naik R, Mujib BRA, Telagi N, Anil BS, Spoorthi BR. Contaminated tooth brushes–potential threat to oral and general health. J Family Med Prim Care. 2015;4(3):444. doi:10.4103/2249-4863.161350
7. Korir A, Okerosi N, Ronoh V, Mutuma G, Parkin M. Incidence of cancer in Nairobi, Kenya (2004–2008). Int J Cancer. 2015;137(9):2053–2059. doi:10.1002/ijc.29674
8. Gakunga R, Parkin DM. Cancer registries in Africa 2014: a survey of operational features and uses in cancer control planning. Int J Cancer. 2015;137(9):2045–2052. doi:10.1002/ijc.29668
9. The global status report on oral health 2022 [Internet]; 2023. Available from: https://www.who.int/team/noncommunicable-diseases/global-status-report-on-oral-health-2022.
10. Herrera D, Sanz M, Kebschull M, et al. Treatment of stage IV periodontitis: the EFP S3 level clinical practice guideline. J Clin Periodontol. 2022;49(S24):4–71. doi:10.1111/jcpe.13639
11. WHO highlights oral health neglect affecting nearly half of the world’s population [Internet]; 2023. Available from: https://www.who.int/news/item/18-11-2022-who-highlights-oral-health-neglect-affecting-nearly-half-of-the-world-s-population.
12. Use & handling of toothbrushes | FAQs | infection control | division of oral health | CDC; 2023. Available from: https://www.cdc.gov/oralhealth/infectioncontrol/faqs/toothbrush-handling.html.
13. Cobb CM. Toothbrushes as a cause of repeated infections of the mouth. Boston Med Surg J. 1920;183:263–264. doi:10.1056/NEJM192008261830905
14. Paster BJ, Boches SK, Galvin JL, et al. Bacterial diversity in human subgingival plaque. J Bacteriol. 2001;183(12):3770. doi:10.1128/JB.183.12.3770-3783.2001
15. Basman A, Peker I, Akca G, Alkurt MT, Sarikir C, Celik I. Evaluation of toothbrush disinfection via different methods. Braz Oral Res. 2015;30(1). doi:10.1590/1807-3107BOR-2016.vol30.0006
16. Petersen PE, Bourgeois D, Ogawa H, Estupinan-Day S, Ndiaye C. Policy and practice the global burden of oral diseases and risks to oral health. Bull World Health Organ. 2005;83(9):1.
17. Lee YH, Chung SW, Auh QS, et al. Progress in oral microbiome related to oral and systemic diseases: an update. Diagnostics. 2021;11(7). doi:10.3390/diagnostics11071283
18. Vandana K, Raju SH, Kumar DR, Babu JN. Knowledge, perceptions and practices about tooth brush sterilization among dental students and faculty in Andhra Pradesh, South India – a Cross sectional study. J Indian Assoc Public Health Dent. 2020;18(4):296. doi:10.4103/jiaphd.jiaphd_123_19
19. Nascimento AP, Watanabe E, Ito IY. Toothbrush contamination by Candida spp. and efficacy of mouthrinse spray for their disinfection. Mycopathologia. 2010;169(2):133–138. doi:10.1007/s11046-009-9239-z
20. Oral health [Internet]; 2023. Available from: https://www.who.int/health-topics/oral-health#tab=tab_1.
21. Africa burdened with largest global increase of oral diseases | WHO | regional office for Africa; 2023. Available from: https://www.afro.who.int/news/africa-burdened-largest-global-increase-oral-diseases.
22. The African regional framework for the implementation of the global strategy on human resources for health: workforce 2030: report of the Secretariat; 2023. Available from: https://iris.who.int/handle/10665/260238.
23. World population prospects 2022: summary of results | population division; 2023. Available from: https://www.un.org/development/desa/pd/content/World-Population-Prospects-2022.
24. Boylan R, Simeonova L, Sherwin G, et al. Reduction in bacterial contamination of toothbrushes using the Violight ultraviolet light activated toothbrush sanitizer. American journal of dentistry. 2008;21(5):313.
25. Bettanapalya Venkatesh S, Kamath V, Shetty S, Shetty SS. Knowledge, attitude and practice of undergraduate students regarding toothbrush contamination and disinfection. Indian J Forensic Med Toxicol. 2020;14(4):1.
26. In J. Introduction of a pilot study. Korean J Anesthesiol. 2017;70(6):601. doi:10.4097/kjae.2017.70.6.601
27. Sowmya K, Puranik M, James J, Sabbarwal B. Perceptions about toothbrush contamination and disinfection among dental students in Bengaluru City: a cross-sectional study. Indian J Dent Res. 2017;28(6):646. doi:10.4103/ijdr.IJDR_301_17
28. Wagle M, Trovik TA, Basnet P, Acharya G. Do dentists have better oral health compared to general population: a study on oral health status and oral health behavior in Kathmandu, Nepal. BMC Oral Health. 2014;14(1):1–8. doi:10.1186/1472-6831-14-23
29. (PDF) knowledge and behavior of undergraduate students in a dental school regarding toothbrush disinfection; 2023. Available from: https://www.researchgate.net/publication/336870129_Knowledge_and_behavior_of_undergraduate_students_in_a_dental_school_regarding_toothbrush_disinfection.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.