")
Back to Journals » Patient Preference and Adherence » Volume 18
International Survey to Evaluate Current Options for Subcutaneous Injection of Methotrexate (MTX) and a New Button-Free MTX Autoinjector
Authors Müller-Ladner U , Edwards CJ, Erkens A
Received 3 November 2023
Accepted for publication 13 February 2024
Published 6 March 2024 Volume 2024:18 Pages 579—590
DOI https://doi.org/10.2147/PPA.S440818
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Johnny Chen
Ulf Müller-Ladner,1 Christopher J Edwards,2 Andreas Erkens3
1Department of Rheumatology and Clinical Immunology, Justus-Liebig-University Giessen, Campus Kerckhoff, Bad Nauheim, Germany; 2Musculoskeletal Research Unit, NIHR Southampton Clinical Research Facility, University Hospital Southampton, Southampton, UK; 3Aurum Research GmbH, Lauf a.d., Pegnitz, Germany
Correspondence: Ulf Müller-Ladner, Department of Rheumatology and Clinical Immunology, Justus-Liebig-University Giessen, Benekestrasse 2-8, D-61231 Bad Nauheim, Germany, Fax +49 6032-996 2104, Email [email protected]
Purpose: Prefilled syringes (PFS) and various types of pens are available for subcutaneous injection of methotrexate (MTX) in patients with rheumatoid arthritis or moderate to severe psoriasis. A new MTX pen with modernized button-free autoinjection technology was developed as a successor to a button-activated pen (metoject®/metex® PEN). To assess the needs of users and the relevance of features of the new MTX autoinjector an international online survey was performed.
Methods: A structured questionnaire was distributed to physicians, nurses and patients in Germany, France, and the United Kingdom. Participants received illustrations and information about features of the new MTX autoinjector.
Results: In total, 189 rheumatologists, 111 dermatologists, 90 nurses, and 180 patients answered the questions. Specific reasons for a preference for the use of MTX pens over PFS could predominantly be assigned to the categories “dosing/administration” and “ease of use”. The first impression of the new MTX autoinjector was positive in 82% of physicians, 87% of nurses, and 76% of patients, respectively. The four most important features of the new MTX autoinjector were 2-step autoinjector mechanism (receiving a mean 14.1 to 18.1 chips of a total of 100 chips), small injection volume (9.7 to 11.7 chips), 10 different doses for dose flexibility (8.0 to 13.2 chips), and short injection time below 5 seconds (8.5 to 11.1 chips).
Conclusion: Arguments for the use of MTX pens as opposed to PFS predominantly refer to dosing/administration and ease of use. The new button-free MTX autoinjector combines a number of advantageous features identified by the international survey.
Plain Language Summary: Subcutaneous injection of methotrexate (MTX) is an option to treat patients with specific inflammatory diseases. A new MTX autoinjector with button-free activation of the injection and no need to build a skin fold was developed to address some of the reasons for non-adherence. The importance of specific needs of users as well as the relevance of features of the new MTX autoinjector are unknown. Therefore, a structured questionnaire was distributed to physicians, nurses and patients in Germany, France, and the United Kingdom. Illustrations and information about features of the new MTX autoinjector were distributed to the participants. The results of the study show that arguments for the use of MTX pens as opposed to prefilled syringes predominantly affect the categories dosing/administration and ease of use followed by safety/side effects. In addition, the study identified four main advantageous features of the new MTX autoinjector, ie simplicity due to the 2-step button-free autoinjector mechanism, the small injection volume, 10 different doses for dose flexibility, and the short injection time below 5 seconds.
Keywords: autoinjector, methotrexate, pen, psoriasis, rheumatoid arthritis, syringe
Introduction
The antimetabolite methotrexate (MTX) is a folic acid antagonist which inhibits DNA synthesis through a competitive inhibition of the enzyme dihydrofolate reductase. Due to its immunomodulatory, anti-inflammatory and antirheumatic properties MTX is used to treat patients with a number of chronic inflammatory diseases including active rheumatoid arthritis (RA), moderate to severe psoriasis vulgaris as well as severe psoriatic arthritis (hereinafter summarized as follows: moderate to severe psoriasis), juvenile idiopathic arthritis, and Crohn’s disease.1–3 In patients with RA MTX is administered either orally, subcutaneously or very rarely intramuscularly.4 At higher doses of MTX parenteral administration improves bioavailability5,6 as well as clinical efficacy4,6–8 versus oral administration. In addition, the subcutaneous route has been suggested to be advantageous with respect to gastrointestinal safety,6–8 adherence,7 and persistence.9
Efficacy of disease-modifying antirheumatic drugs (DMARDs) such as MTX depends on persistence and patient adherence,10–13 which were highly variable in clinical studies investigating MTX in RA.11,14 In a retrospective German cohort study 26% of 7146 patients with RA receiving MTX therapy were non-adherent during 12-month follow-up.15 The non-adherence rate for MTX in Italian patients with psoriatic arthritis was 38% (1108 of 2952 patients) with a twofold increase in non-adherence for oral versus parenteral MTX.16 In part, this may be due to more gastrointestinal events with oral versus subcutaneous MTX.2 Concerns about side effects may result in an active avoidance of taking the medication, also named as conscious non-adherence, whereas unconscious, non-intentional poor adherence can be caused by insufficient patient motivation, drug regimen misunderstanding, forgetfulness, needle phobia, and problems with drug administration due to reduced hand capabilities or complex handling.17 In a French prospective observational study, the switch from oral to subcutaneous route improved adherence to MTX, mainly due to a reduction of intentional non-adherence whereas non-intentional non-adherence remained almost unchanged.18
To improve the acceptability of subcutaneous treatment with MTX or biologic drugs in patients with RA or other chronic inflammatory diseases different pens were developed and compared to prefilled syringes (PFS). For example, a randomized controlled trial in patients with RA yielded favorable acceptability scores for a MTX autoinjector versus PFS concerning satisfaction, ease of use, pleasantness, treatment-related burden, motivation for further utilization and reassuring.19 However, percentages of patients with local adverse events at injection site were similar between groups (7% versus 3%), and non-inferiority of MTX autoinjector concerning the two coprimary endpoints percentage of good compliers (90% versus 95%) as well as the percentage change of functional capacity measured by the Health Assessment Questionnaire (HAQ) score could not be demonstrated.19 In a retrospective analysis the use of a pen was favorable with respect to adherence and persistence if compared to syringes in patients with Crohn´s disease treated with adalimumab.20 There are several studies showing reductions of pain at injection site with pens for MTX or biologic drugs if compared to PFS,21–24 whereas one study revealed individual differences favoring PFS with respect to pain over the autoinjector in 17 of 46 RA patients (37%) treated with an adalimumab biosimilar.25 Autoinjector devices for subcutaneous self-administration of MTX may be useful to improve patient satisfaction, preference, and potentially adherence.26
Examples for targets of further developments are decreased risk of accidental needle injury, reduced needle phobia as well as the perception of injection pain, and facilitating injection especially in patients with disabilities such as functional limitations.27 With this in mind, a new pre-filled MTX pen with modernized autoinjection technology was developed, hereinafter also referred to as “new MTX autoinjector”, as a successor of a button-activated pre-filled MTX autoinjector which was introduced in 2013, hereinafter also referred to as “former MTX autoinjector” (brand names for both MTX autoinjectors: metoject® PEN or metex® PEN, medac GmbH, Wedel, Germany). Besides other new features the new MTX autoinjector allows for a button-free activation of the injection with no need to build a skin fold which reduces the 3-step autoinjection to a 2-step autoinjection. A reduced number of application steps was one reason for patients’ preference for a 2-step autoinjector in acute migraine treatment compared with a 3-step device and a multi-step device.28 An international online survey was conducted to determine the importance of specific needs of users as well as the relevance of features of the new 2-step button-free MTX autoinjector.
Materials and Methods
Between April and May 2022, a structured quantitative online questionnaire for evaluation and analysis of findings gained in a preceding qualitative phase was distributed to physicians, nurses and patients in Germany, France, and the United Kingdom (UK). Participants were contacted through a market research invitation email through an online panel called M3 Global Research community which can, among others, be joined by consumers and patients who “are interested in giving their opinion about goods, services, medication, etc. in the healthcare industry”.29 Criteria for participation in the survey were defined for the three relevant target groups as follows: (1) Rheumatologists and dermatologists had at least 3 years of experience in the medical field of specialization, worked full time with at least 50% of their time given to patient care and were therapy decision makers, who initiate and actively prescribe at least four MTX pens (former MTX autoinjector in France and Germany) per quarter for RA-patients and/or two MTX pens (former MTX autoinjector in Germany and the UK) per quarter for patients with moderate to severe psoriasis. (2) Nurses had at least 2 years of experience in the field of RA and train patients (mainly adults) on MTX pens, ie at least four (UK) or two (France and Germany) patients with RA who have been trained on the former MTX autoinjector in the last 3 months. (3) Patients with RA or moderate/severe psoriasis were at least 18 years old and had more than 6 months (RA) or more than 3 months (psoriasis) experience with a MTX pen.
Participants received illustrations of three MTX devices currently available on the market (metoject®/metex® PEN, medac, GmbH Germany; Nordimet® pre-filled pen, Nordic Group B.V., The Netherlands; Methofill® pre-filled injector, Accord Healthcare Ireland Ltd., Ireland), and were informed about design (photo, description), function, handling, and features of the new MTX autoinjector (Figure 1, Table 1). The two steps to start the injection with this autoinjector were described as follows: (1) removal of the cap and (2) placement on skin and pushing firmly. With the former MTX autoinjector three steps were required for autoinjection: (1) pulling the cap straight off, (2) building a skin fold and pushing the pen firmly into the skin, (3) pushing the button.
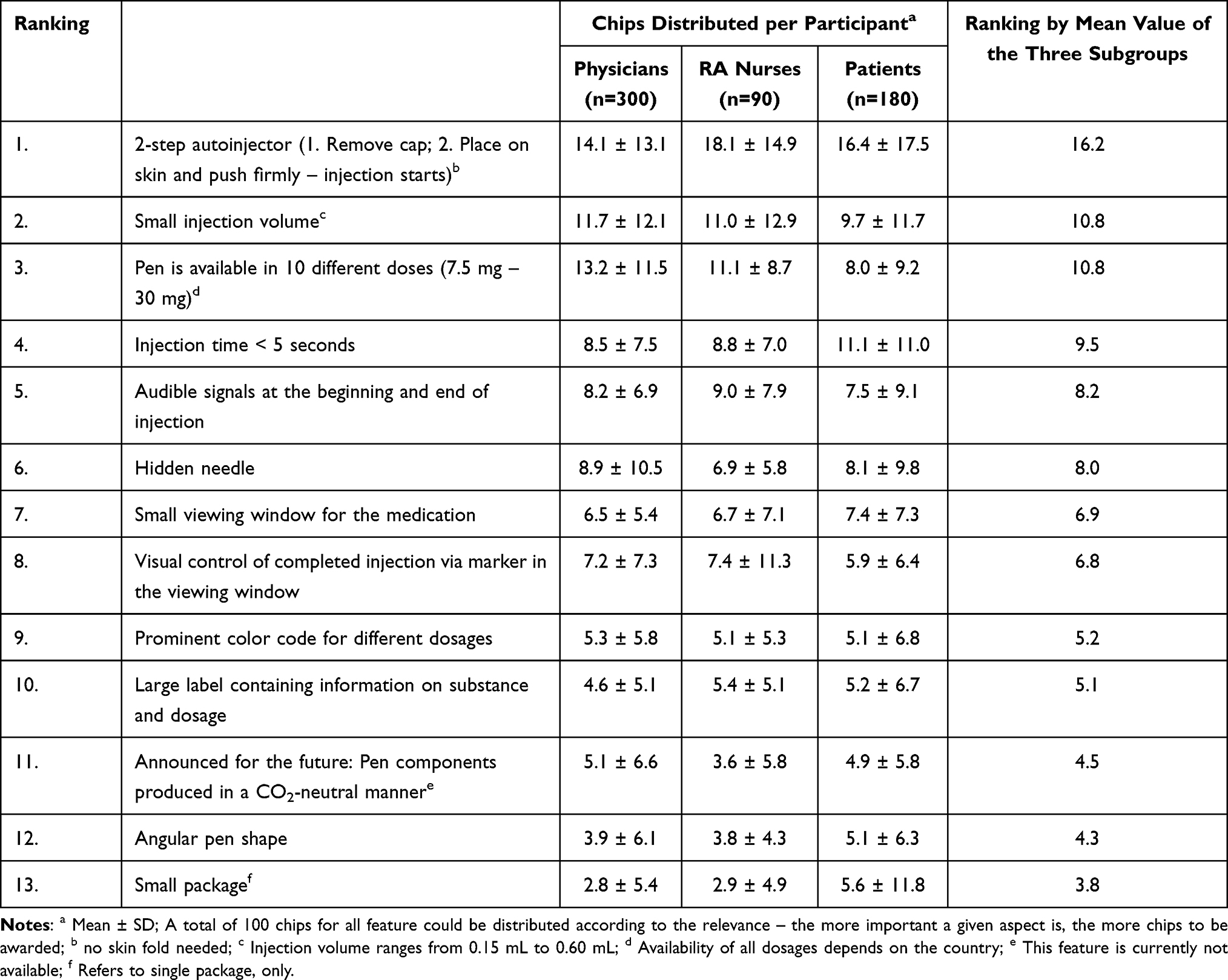 |
Table 1 Features of the New Button-Free MTX Autoinjector and Their Importance Rated by Distribution of a Total of 100 Chips per Participant |
 |
Figure 1 Design, function and handling of the new MTX autoinjector. Note: *This illustration was not shown to the respondents. |
Satisfaction with the pens which are currently available on the market (physicians, nurses) or used (patients) was assessed by using a scale ranging from 1 “not at all satisfied” to 10 “very satisfied” (Table S1). The physicians and nurses were asked to list specific medical arguments which might favor the use of a MTX pen as opposed to PFS (Table S1).
Out of 11 closed questions and one open question answered by the respondents five closed questions were used to analyze features and benefits of the new MTX autoinjector (Table S1). To rate the relevance of features the respondents could distribute a total of 100 ‘chips’ among 13 prespecified features of the new MTX autoinjector (Table 1). Respondents were asked to select up to three major benefits out of up to eight benefits listed for each feature of the new MTX autoinjector.
The data were analyzed descriptively with groups of physicians, nurses and patients expressed as numbers and percentages. For the other variables, mean values ± standard deviation (SD) were calculated. P-values were not calculated as no formal hypothesis was defined in advance.
Results
In total, 570 participants answered the questions of the survey. Rheumatologists (n=189) treated 323 ± 293 patients with RA. Dermatologists (n=111) took care of 227 ± 283 patients with moderate or severe psoriasis (Table 2). Forty-five of 90 nurses (50%) had trained at least 25 patients, and another 38% of nurses 10 to 24 patients. Most patients participating in the survey (n=180) were younger than 40 years (38%) or 40 to 59 years (44%) old (Table 3). Only 18% of patients were 60 years or older. Patients injected themselves always (79%) or mostly (21%), respectively.
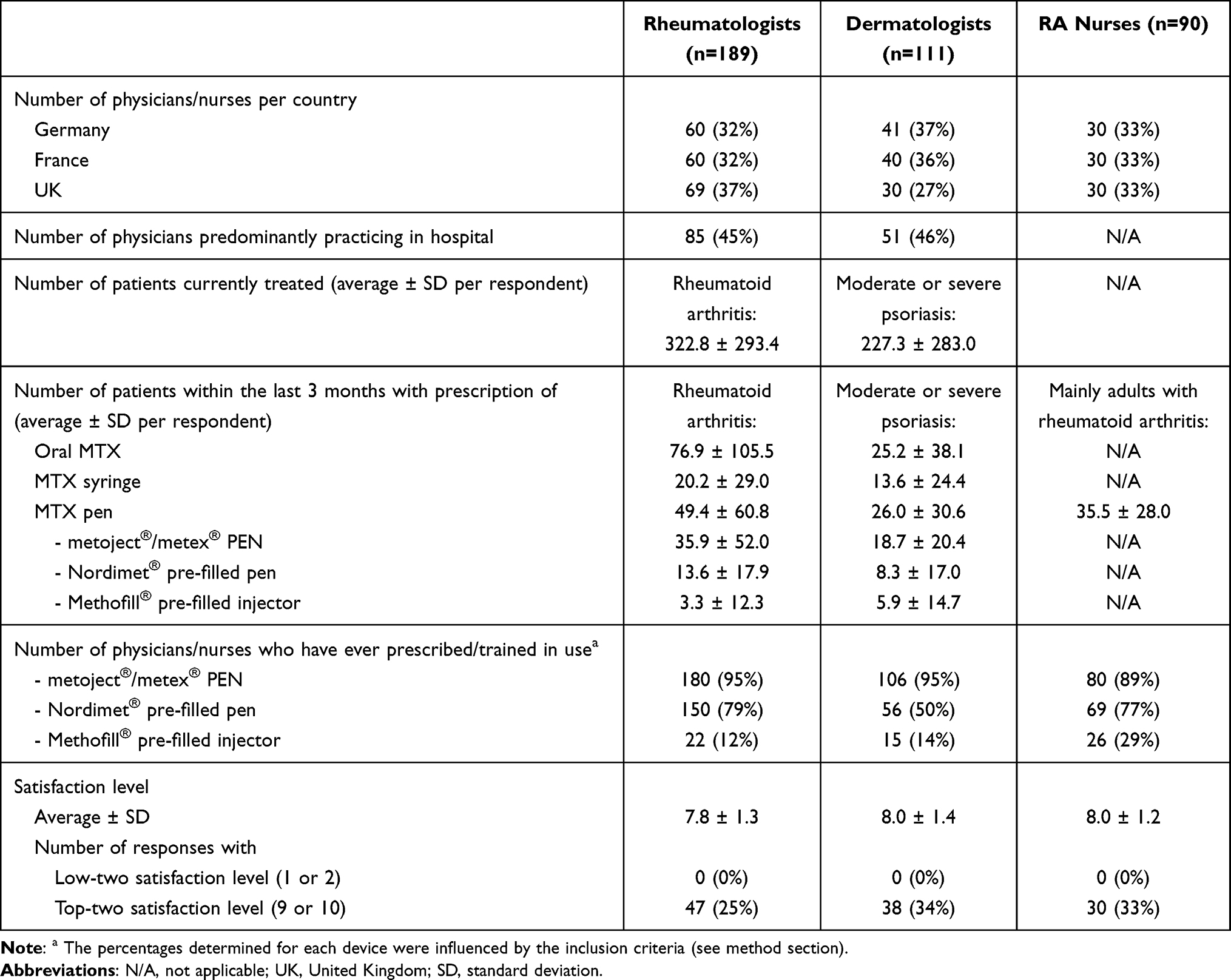 |
Table 2 Characteristics of Physicians and Nurses Participating in the Survey and Satisfaction Levels with MTX Pens Currently Available on the Market |
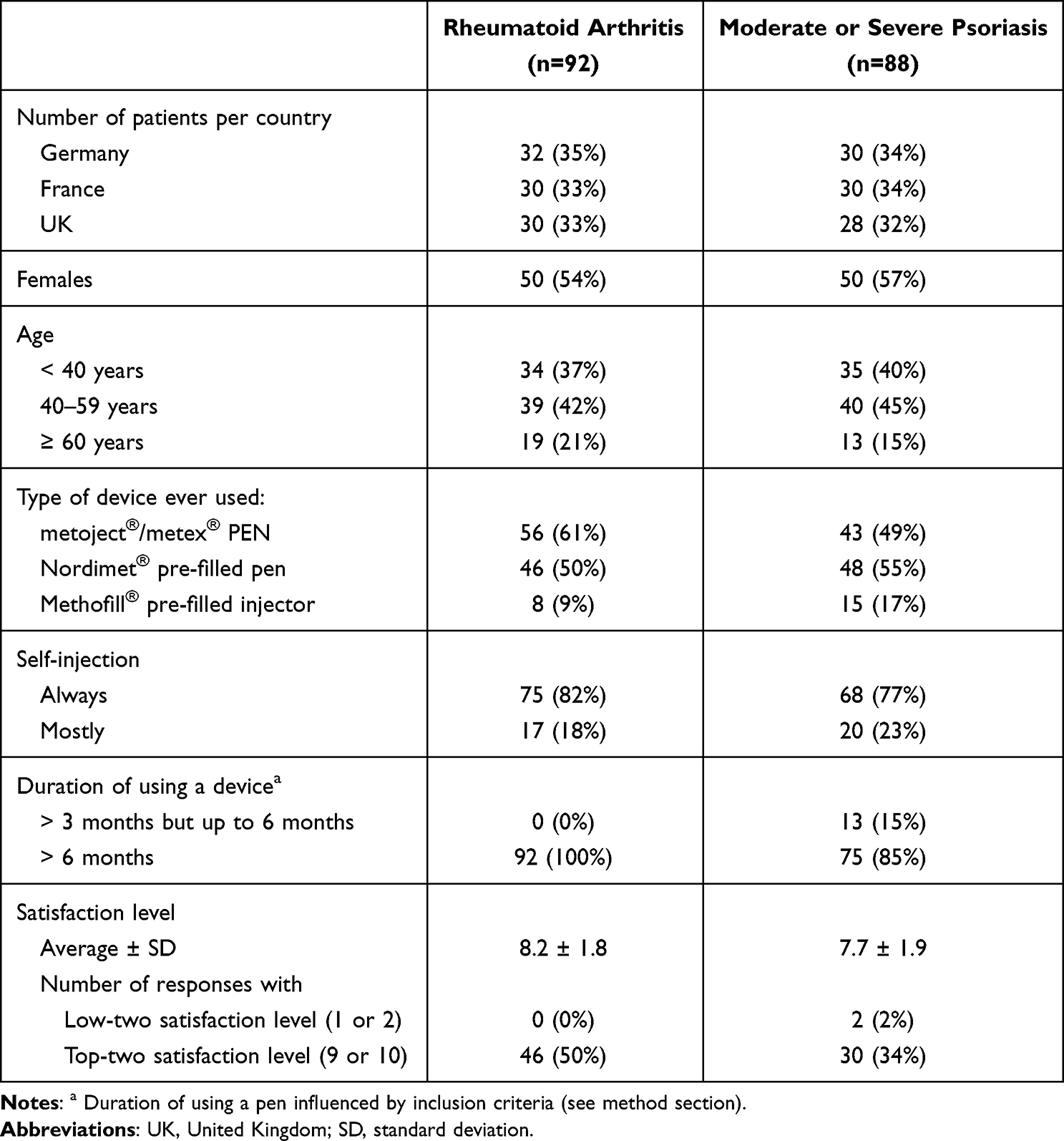 |
Table 3 Characteristics of Patients Participating in the Survey and Satisfaction Level with MTX Pens Currently Available on the Market |
There were some differences between countries regarding baseline characteristics (Table S2, Table S3). In Germany, only 3 physicians (5%) were practicing predominantly in a hospital versus the majorities of physicians in France and the UK. In general, physicians had more patients with prescriptions of a pen versus syringes (Table 2). Only in the UK, the majority of patients received oral MTX (Table S2). There were no experiences with the Methofill® injector in Germany (Table S2, Table S3). Physicians, nurses, and patients are generally satisfied with the MTX pens currently available on the market as shown by mean satisfaction levels between 7.7 and 8.2 and top-two satisfaction levels (9 or 10) assigned by 25% to 50% of respondents (Tables 2 and 3).
Specific arguments which might favor the use of a MTX pen as opposed to a PFS could predominantly be assigned to the two categories “dosing/administration” and “ease of use” in all three subgroups of respondents (Table 4). Within the remaining five categories the highest percentages of respondents listed arguments referring to safety/side effects, especially 47% of respondents in the subgroup of nurses (Table 4).
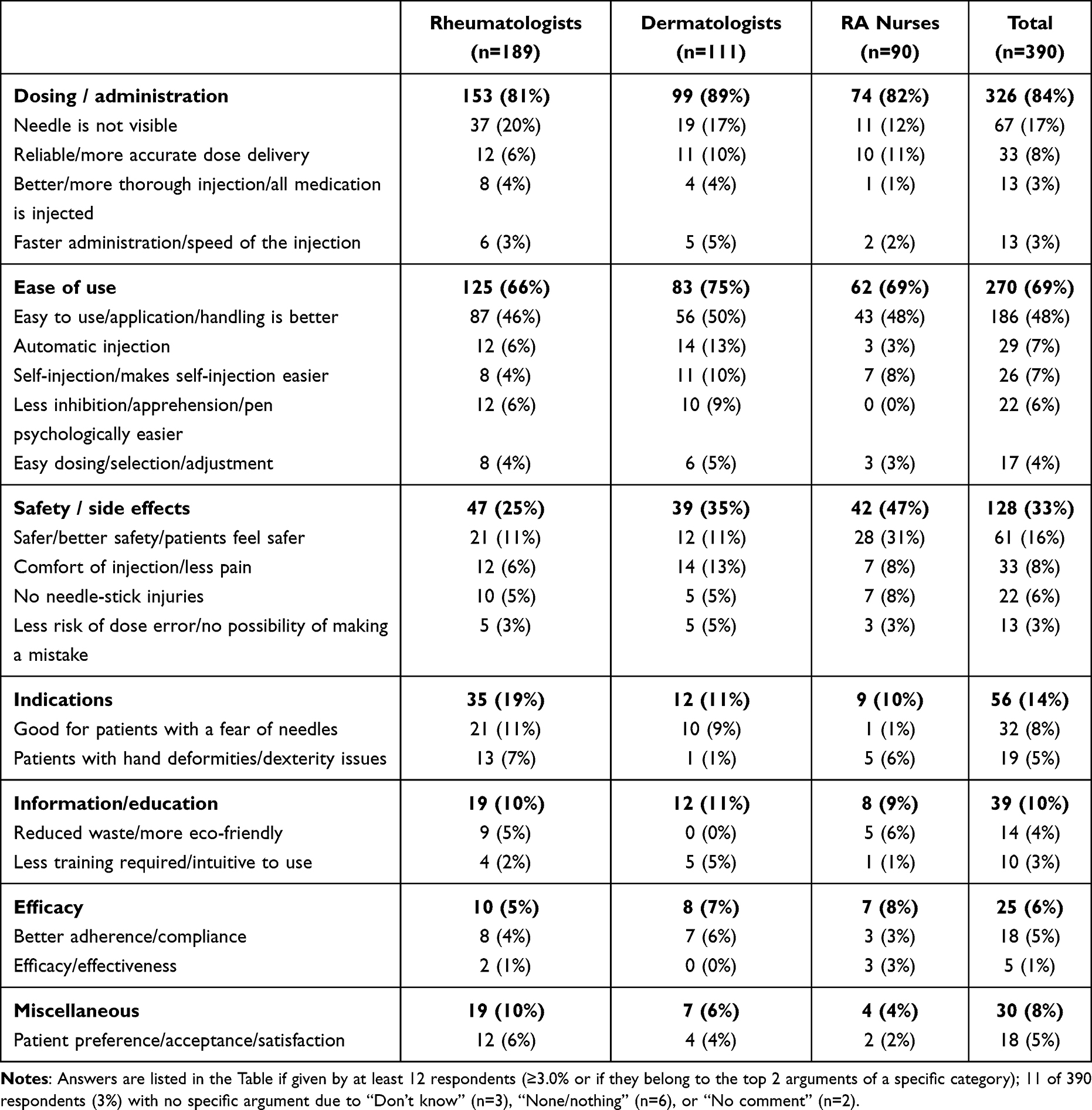 |
Table 4 Medical Arguments Which Might Advocate the Use of a MTX Pen as Opposed to a PFS |
The first impression of the new MTX autoinjector was positive in 245 of 300 physicians (82%), 78 of 90 nurses (87%), and 136 of 180 patients (76%). The others were mostly ambivalent (13%, 12%, 16%) or did not know, yet (5%, 1%, 8%). The most important features of the new MTX autoinjector were the 2-step autoinjector mechanism, the small injection volume, and the dose flexibility (Table 1). Patients also rated injection time below 5 seconds highly (11.1 of 100 chips in average).
The ease of use/administer was selected by 51% of physicians, 47% of nurses, and 48% of patients as one of up to three major benefits to be specified regarding the feature “2-step application” of the new MTX autoinjector (Figure 2A). Each of the other seven potential benefits were chosen by 23% to 33% of physicians, 20% to 39% of nurses, and 19% to 32% of patients. With respect to the feature “10 doses from 7.5 mg to 30 mg” the four potential benefits were selected by 43% or 47% of physicians, 46% to 59% of nurses, and 32% to 44% of patients as one of up to three major benefits (Figure 2B). Regarding the feature “short injection time” the first four of seven potential benefits listed in Figure 2C were chosen by at least 30% of respondents. The main benefit in terms of the feature “Small injection volume” was “Less/no pain”, selected by 57% of physicians, 59% of nurses, and 46% of patients (Figure 2D). However, the other three potential benefits of the feature “Small injection volume” listed in the questionnaire were chosen by 38% to 52% of respondents.
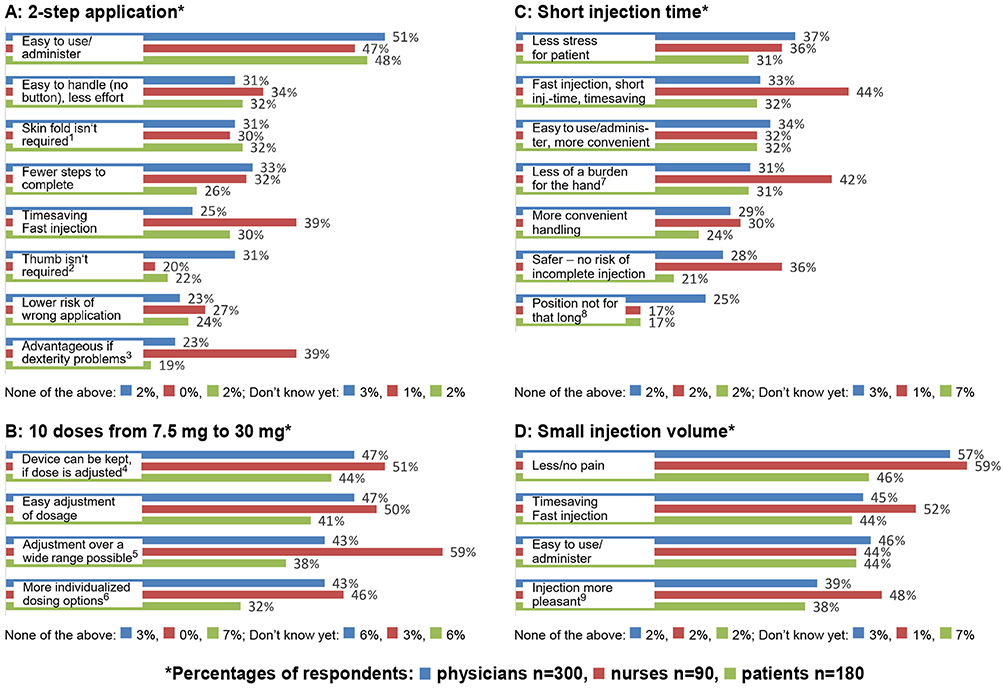 |
Figure 2 Ratings of potential benefits by respondents regarding the four most important features of the new MTX autoinjector according to ranking in Table 1. Notes: For each feature, up to three main benefits could be selected. The benefits have been identified during a preceding qualitative research resulting in different numbers of benefits per feature. With respect to footnote numbers 1 to 9 exact wording in the questionnaire was follows: 1 Building a skin fold for the injection is not required. The injection can be applied according to the patient’s preference: either one or two hands can be used. 2 Thumb is not required; you can trigger it with the whole hand. 3 Advantage in the case of hand deformities / dexterity problems, arthritic diseases / joint problems. 4 Even if the dose is adjusted, you can keep the same device. 5 The physician can adjust the dosage over a wide range, and in smaller steps; highly individualized treatment possible. 6 More individualized dosing options, depending on patients’ requirements. 7 Very short injection time, less of a burden for the hand. 8 You do not have to hold the pen in the same position for that long. 9 Due to the highest concentration possible for MTX, the injection volume is as small as possible and the injection itself is more comfortable and more pleasant. |
About 90% of physicians (88%), nurses (94%), and patients (89%) would likely or very likely use the new MTX autoinjector. The major concerns about switching to the new MTX autoinjector are costs/pricing (selected by 51% of physicians, 60% of nurses, and 31% of patients), the need for re-education of the patient (49%, 47%, 18%), and availability in pharmacies/logistics (39%, 51%, 32%).
Discussion
Most patients treated with MTX or biologic drugs prefer autoinjectors over prefilled syringes (PFS).19,21–25,30–32 Considering responses given by physicians and nurses listed in Table 4 this may primarily be due to the ease of use and an improved handling. In addition, several patients treated with the former MTX autoinjector highlighted the relatively pain free injection.33 This international online survey confirms that the MTX pens currently available on the market are quite satisfactory as also shown by clinical studies and other surveys.19,21,33,34 The mean satisfaction level reaching 8.2 ± 1.8 points in 92 patients with RA fits well to 8.3 ± 2.4 points determined in RA patients treated with an etanercept pen in a randomized controlled study showing a higher satisfaction level versus etanercept PFS (7.2 ± 2.6 points).35 However, mean satisfaction levels between 7.7 and 8.0 points in the other subgroups of this international online survey show that there is room for improvement.
In this international online survey, the general impression concerning the new MTX autoinjector was positive across all target groups. The most important advantages identified were its simplicity due to the 2-step autoinjector mechanism versus 3 steps with the former MTX autoinjector, as well as the features small injection volume, dose flexibility, and short injection time below 5 seconds. The rapid injection reduces the risk that the patient removes the device prematurely with the consequence of underdosing.27 Maximum injection time of 5 seconds was already possible with the former MTX autoinjector and is linked to small injection volumes between 0.15 and 0.60 mL. The small injection volume is one factor which may decrease the pain in conjunction with subcutaneous injection,36 may improve the comfort of injection and is potentially associated with a psychological benefit to the patient.37 In the international online survey 57% of physicians, 59% of nurses, and 46% of patients selected “Less/no pain” as one benefit of the small volume. The somewhat lower percentage in the patient subgroup may be biased by individual experience whereas physicians and nurses were able to respond on the basis of expertise and guidance of many patients.
Concerning dose flexibility, the new MTX autoinjector as well as the former MTX autoinjector allow for the prescription of 10 different doses ranging from 7.5 mg MTX (0.15 mL) up to 30 mg MTX (0.60 mL) whereas maximum dose of another MTX autoinjector is 25 mg MTX (1.0 mL).38 According to the international online survey this may be advantageous for dose adjustments as the device can be kept even if the MTX dose is adjusted to 27.5 mg or 30 mg.
The major benefit of the most important feature “2-step application” was “Easy to use / administer”. Other benefits listed in the questionnaire described details of the easiness to use the new MTX autoinjector, for example “Building a skin fold for injection isn’t required. The injection can be applied according to the patient’s preference: either one or two hands can be used”, and “Thumb isn’t required; you can trigger it with the whole hand”. A skin fold is foreseen for subcutaneous injection with the former button-activated MTX autoinjector as well as with the button-free MTX autoinjector already available on the market.34
In accordance with the results of our international online survey there are several investigations spelling out favorable features and benefits of button-free autoinjectors on the basis of physicians’, nurses’, and/or patients’ feedback.39–45 Even patients with RA and severe hand disability were able to properly perform self-injection with a button-free autoinjector as shown by an electromagnetic motion analysis system during simulated subcutaneous self-injection using a foam pad.46 In addition, patients using a button-free autoinjector highlighted the easiness to determine injection completion.43 As shown in Table 1 “Audible signals at the beginning and end of injection” was ranked fifth among 13 features of the new MTX autoinjector. “Ease of grip” is another important feature for autoinjectors.39,40 This feature was not evaluated for the new MTX autoinjector as the participants of the international online survey could not hold the device in their hands.
The international online survey showed that replacing the former MTX autoinjector with the new MTX autoinjector does not seem to raise any new or specific concern. Issues refer to costs/pricing, availability in pharmacies/logistics, and need for re-education. Sufficient instructions on how to use the pen before switching are of major importance. For example, after only 18.2% of patients received instructions concerning a button-free autoinjector for adalimumab biosimilar treatment, almost half (46.6%) evaluated the use of this pen more difficult and only 12.5% easier versus a button-activated autoinjector which was explained to 90.5% of the patients.47 Besides supporting the use of the new MTX autoinjector, the guidance may be an occasion to improve patient education which is a strong predictor of adherence.48,49 In general, the availability of various devices is advantageous to meet the individual needs of different patients.17,42,50 However, switching back and forth should be avoided.51
Finally, improvement of tolerance to MTX treatment is an important target. For example, in patients with psoriasis safety reasons for stopping MTX treatment were more frequent with oral (16%) versus subcutaneous (4%) MTX.52 MTX intolerance may in parts be explained by the psychological adverse effect of anticipatory nausea reported in 41% of adolescents and 30% of adults with inflammatoryarthritis.53 Anticipatory nausea may lead to non-adherence and treatment discontinuation.54 Besides using modern MTX autoinjectors, measures to prevent nausea during MTX treatment are folic acid supplementation, antiemetics, and behavioral therapies.54
Limitations
One limitation of the international online survey, although reflecting the clinical routine when switching to another device for injection, is that the new MTX autoinjector was presented by illustrations and description of the features, only. Therefore, the respondents could not hold the new device in their hands or gain clinical experiences prior to first real injection. In addition, respondents may also have gained experiences with pens used for other drugs, or they differed with respect to their experiences with different types of MTX pens. For example, respondents who are familiar with button-free autoinjector pens may have different views if compared to respondents not experienced in such pens. No question concerning general preference of MTX pens over PFS was included in the questionnaire as physicians and nurses cannot give one universal answer due to individual needs of the patients, and as inclusion of patients in this survey was possible without any experience in the use of PFS. As in similar surveys, the wordings and closed questions used in the questionnaire may have influenced responses. Important criteria and features had to be given in advance to reach categories for evaluation.
Conclusion
In conclusion, arguments for the use of MTX pens as opposed to PFS predominantly refer to the categories dosing/administration, ease of use, and safety/side effects. MTX pens currently available are quite satisfactory. However, the new button-free MTX autoinjector combines four main advantageous features identified by the international online survey, that is simplicity due to the 2-step button-free autoinjector mechanism, the small injection volume, 10 different doses for dose flexibility, and the short injection time below 5 seconds.
Abbreviations
DMARDs, disease-modifying antirheumatic drugs; MTX, Methotrexate; PFS, prefilled syringes; RA, rheumatoid arthritis.
Data Sharing Statement
The datasets generated and analyzed during this international online survey are available from Aurum Research GmbH, Lauf a.d. Pegnitz, Germany on reasonable request.
Ethics Approval and Informed Consent
This study was an online market research and conducted according to the binding rules of quality and professional conduct set down by the EPhMRA (European Pharmaceutical Market Research Association) code of conduct, ESOMAR (European Society for Opinion and Market Research), the German association ADM (Arbeitskreis Deutscher Markt- und Sozialforschungsinstitute e.V.), and the legal obligations for data protection. It was also conducted in accordance to the ADM standards for interviewing physicians for the purposes of market and social research. An ethics committee approval was therefore not required. All participants provided informed consent before participating in the online survey due to their individual registration and access to the online panel site which includes their agreement to the terms and conditions of the M3 Global Research community such as anonymized reporting of the data.29
Acknowledgments
The authors thank physicians, nurses and patients for participation in the online survey, Alexander Rummel (Aurum Research GmbH, Lauf a.d. Pegnitz, Germany) for his contribution to the design and the realization of this study, and Detlev Janssen (Med-i-Scene Concept GmbH, Weisendorf, Germany) for the medical writing assistance to prepare this manuscript which was funded by medac GmbH, Wedel, Germany.
Funding
The international online survey was funded by medac GmbH, Wedel, Germany.
Disclosure
Ulf Müller-Ladner served as a speaker/advisor for medac GmbH, Wedel, Germany. Andreas Erkens served as senior partner Aurum Research and advisor for medac GmbH, Wedel, Germany. The authors report no other conflicts of interest in this work.
References
1. Bedoui Y, Guillot X, Sélambarom J, et al. Methotrexate an old drug with new tricks. Int J Mol Sci. 2019;20:5023. doi:10.3390/ijms20205023
2. Tanaka Y, Okuda K, Takeuchi Y, et al. Efficacy and tolerability of subcutaneously administered methotrexate including dose escalation in long-term treatment of rheumatoid arthritis in a Japanese population. Mod Rheumatol. 2023;33(4):680–689. doi:10.1093/mr/roac103
3. Warren RB, Mrowietz U, von Kiedrowski R, et al. An intensified dosing schedule of subcutaneous methotrexate in patients with moderate to severe plaque-type psoriasis (METOP): a 52 week, multicentre, randomised, double-blind, placebo-controlled, Phase 3 trial. Lancet. 2017;389(10068):528–537. doi:10.1016/S0140-6736(16)32127-4
4. Bujor AM, Janjua S, LaValley MP, Duran J, Braun J, Felson DT. Comparison of oral versus parenteral methotrexate in the treatment of rheumatoid arthritis: a meta-analysis. PLoS One. 2019;14(9):e0221823. doi:10.1371/journal.pone.0221823
5. Pichlmeier U, Heuer K-U. Subcutaneous administration of methotrexate with a prefilled syringe autoinjector pen results in a higher relative bioavailability compared with oral administration of methotrexate. Clin Exp Rheumatol. 2014;32(4):563–571.
6. Li D, Yang Z, Kang P, Xie X. Subcutaneous administration of methotrexate at high doses makes a better performance in the treatment of rheumatoid arthritis compared with oral administration of methotrexate: a systematic review and meta-analysis. Sem Arthritis Rheum. 2016;45(6):656–662. doi:10.1016/j.semarthrit.2015.11.004
7. Otón T, Carmona L, Loza E, Rosario MP, Andreu JL. Use of parenteral methotrexate in rheumatic disease: a systematic review. Reumatol Clin. 2022;18:207–226. doi:10.1016/j.reuma.2020.11.006
8. Tanaka Y. Subcutaneous injection of methotrexate: advantages in the treatment of rheumatoid arthritis. Mod Rheumatol. 2022;33(4):633–639. doi:10.1093/mr/roac156
9. Bello AE, Perkins EL, Jay R, Efthimiou P. Recommendations for optimizing methotrexate treatment for patients with rheumatoid arthritis. Open Access Rheumatol. 2017;9:67–79. doi:10.2147/OARRR.S131668
10. Pasma A, Schenk CV, Timman R, et al. Non-adherence to disease-modifying antirheumatic drugs is associated with higher disease activity in early arthritis patients in the first year of the disease. Arthritis Res Ther. 2015;17:218. doi:10.1186/s13075-015-0801-4
11. Hope HF, Bluett J, Barton A, Hyrich KL, Cordingley L, Verstappen SMM. Psychological factors predict adherence to methotrexate in rheumatoid arthritis; findings from a systematic review of rates, predictors and associations with patient-reported and clinical outcomes. RMD Open. 2016;2(1):e000171. doi:10.1136/rmdopen-2015-000171
12. Maniadakis N, Toth E, Schiff M, et al. A targeted literature review examining biologic therapy compliance and persistence in chronic inflammatory diseases to identify the associated unmet needs, driving factors, and consequences. Adv Ther. 2018;35(9):1333–1355. doi:10.1007/s12325-018-0759-0
13. Kang J-H, Choi S-E, Xu H, Park D-J, Lee J-K, Lee S-S. Non-adherence to methotrexate was associated with high disease activity and poor health-related outcomes during 4-year follow-up of rheumatoid arthritis patients. Clin Exp Rheumatol. 2022;40(9):1744–1753. doi:10.55563/clinexprheumatol/ir6yds
14. Curtis JR, Bykerk VP, Aassi M, Schiff M. Adherence and persistence with methotrexate in rheumatoid arthritis: a systematic review. J Rheumatol. 2016;43(11):1997–2009. doi:10.3899/jrheum.151212
15. Müller S, Wilke T, Fuchs A, et al. Non-persistence and non-adherence to MTX therapy in patients with rheumatoid arthritis: a retrospective cohort study based on German RA patients. Patient Prefer Adherence. 2017;11:1253–1264. doi:10.2147/PPA.S134924
16. Generali E, Carrara G, Bortoluzzi A, et al. Non-adherence and discontinuation rate for oral and parenteral methotrexate: a retrospective-cohort study in 8,952 patients with psoriatic arthritis. J Trans Autoimmun. 2021;4:100113. doi:10.1016/j.jtauto.2021.100113
17. Van den Bemt BJF, Gettings L, Domanska B, Bruggraber R, Mountain I, Kristensen LE. A portfolio of biologic self-injection devices in rheumatology: how patient involvement in device design can improve treatment experience. Drug Deliv. 2019;26(1):384–392. doi:10.1080/10717544.2019.1587043
18. Senbel E, Tropé S, Herman-Demars H, et al. Benefits of switch from oral to subcutaneous route on adherence to methotrexate in patients with rheumatoid arthritis in real life setting. Patient Prefer Adherence. 2021;15:751–760. doi:10.2147/PPA.S301010
19. Saraux A, Hudry C, Zinovieva E, Herman-Demars H. Self-I Investigators group. Use of autoinjectors for methotrexate subcutaneous self-injections: high satisfaction level and good compliance in SELF-I study, a randomized, open-label, parallel group study. Rheumatol Ther. 2019;6(1):47–60. doi:10.1007/s40744-018-0134-2
20. Liu Y, Söderberg J, Chao J. Adherence to and persistence with adalimumab therapy among Swedish patients with Crohn’s disease. Pharmacy. 2022;10(4):87. doi:10.3390/pharmacy10040087
21. Roszkiewicz J, Swacha Z, Smolewska E. Prefilled pen versus prefilled syringe: a pilot study evaluating two different methods of methotrexate subcutaneous injection in patients with JIA. Pediatr Rheumatol. 2020;18(1):64. doi:10.1186/s12969-020-00455-4
22. Kivitz A, Cohen S, Dowd JE, et al. Clinical assessment of pain, tolerability, and preference of an autoinjection pen versus a prefilled syringe for patient self-administration of the fully human, monoclonal antibody adalimumab: the TOUCH trial. Clin Ther. 2006;28(10):1619–1629. doi:10.1016/j.clinthera.2006.10.006
23. Borrás-Blasco J, Gracia-Pérez A, Rosique-Robles JD, Castéra MDE, Abad FJ. Acceptability of switching adalimumab from a prefilled syringe to an autoinjection pen. Expert Opin Biol Ther. 2010;10(3):301–307. doi:10.1517/14712590903530633
24. Borrás-Blasco J, Gracia-Pérez A, Castéra MDE, Rosique-Robles, D, Abad, J . Educational session as a tool to increase patients satisfaction of switching etanercept from the prefilled syringe to the autoinjection pen. Expert Opin Biol Ther. 2013;13(8):1103–1108. doi:10.1517/14712598.2013.795942
25. Ghil J, Zielinska A, Lee Y. Usability and safety of SB5 (an adalimumab biosimilar) prefilled syringe and autoinjector in patients with rheumatoid arthritis. Curr Med Res Opin. 2019;35(3):497–502. doi:10.1080/03007995.2018.1560211
26. Tornero Molina J, López Robledillo JC, Ruiz NC. Potential benefits of the self-administration of subcutaneous methotrexate with autoinjector devices for patients. A review. Drug Healthc Patient Saf. 2021;13:81–94. doi:10.2147/DHPS.S290771
27. Schiff M, Jaffe J, Freundlich B, Madsen P. New autoinjector technology for the delivery of subcutaneous methotrexate in the treatment of rheumatoid arthritis. Expert Rev Med Devices. 2014;11(5):447–455. doi:10.1586/17434440.2014.929492
28. Andre AD, Brand-Schieber E, Ramirez M, Munjal S, Kumar R. Subcutaneous sumatriptan delivery devices: comparative ease of use and preference among migraineurs. Patient Prefer Adherence. 2017;11:121–129. doi:10.2147/PPA.S125137
29. M3 Global Research. Frequently Asked Questions. Available from: https://m3globalresearch.com/faq.
30. Demary W, Schwenke H, Rockwitz K, et al. Subcutaneously administered methotrexate for rheumatoid arthritis, by prefilled syringes versus prefilled pens: patient preference and comparison of the self-injection experience. Patient Prefer Adherence. 2014;8:1061–1071. doi:10.2147/PPA.S64111
31. Fleischmann RM, Bock AE, Zhang W, et al. Usability study of PF-06410293, an adalimumab biosimilar, by prefilled pen: open-label, single-arm, sub-study of a phase 3 trial in patients with rheumatoid arthritis. Rheumatol Ther. 2022;9(3):839–850. doi:10.1007/s40744-022-00439-8
32. Vermeire S, D’heyghere F, Nakad A, et al. Preference for a prefilled syringe or an auto-injection device for delivering golimumab in patients with moderate-to-severe ulcerative colitis: a randomized crossover study. Patient Prefer Adherence. 2018;12:1193–1202. doi:10.2147/PPA.S154181
33. Pachon JA, Kivitz AJ, Heuer K-U, Pichlmeier U. Assessing usability, label comprehension, pen robustness and pharmacokinetics of a self-administered prefilled autoinjector pen of methotrexate in patients with rheumatoid arthritis. SAGE Open Med. 2014;2:2050312114564241. doi:10.1177/2050312114564241
34. Hudry C, Lebrun A, Moura B, Zinovieva E, Backers O, Herman-Demars H. Evaluation of usability and acceptance of a new autoinjector intended for methotrexate subcutaneous self-administration in the management of rheumatoid arthritis. Rheumatol Ther. 2017;4:183–194. doi:10.1007/s40744-017-0057-3
35. Müller-Ladner U, Flipo RM, Vincendron P, Brault Y, Kielar D. Comparison of patient satisfaction with two different etanercept delivery systems. A randomised controlled study in patients with rheumatoid arthritis. Z Rheumatol. 2012;71(10):890–899. doi:10.1007/s00393-012-1034-4
36. Usach I, Martinez R, Festini T, Peris J-E. Subcutaneous injection of drugs: literature review of factors influencing pain sensation at the injection site. Adv Ther. 2019;36(11):2986–2996. doi:10.1007/s12325-019-01101-6
37. Müller-Ladner U, Rockwitz K, Brandt-Jürgens J, et al. Tolerability and patient/physician satisfaction with subcutaneously administered methotrexate provided in two formulations of different drug concentrations in patients with rheumatoid arthritis. Open Rheumatol J. 2010;4:15–22. doi:10.2174/1874312901004010015
38. McKeage K, Lyseng-Williamson KA. Methotrexate pre-filled autoinjector pen (Nordimet®) for subcutaneous injection: a profile of its use in the EU. Drugs Ther Perspect. 2018;34:197–202. doi:10.1007/s40267-018-0505-3
39. Tischer B, Mehl A. Patients’ and nurses’ preferences for autoinjectors for rheumatoid arthritis: results of a European survey. Patient Prefer Adherence. 2018;12:1413–1424. doi:10.2147/PPA.S169339
40. Fenwick S, Thakur K, Munro D. Nurse and patient perceptions and preferences for subcutaneous autoinjectors for inflammatory joint or bowel disease: findings from a European survey. Rheumatol Ther. 2019;6(2):195–206. doi:10.1007/s40744-019-0144-8
41. Egeth M, Soosaar J, Nash P, et al. Patient and healthcare professionals preference for Brenzys vs. Enbrel autoinjector for rheumatoid arthritis: a randomized crossover simulated-use study. Adv Ther. 2017;34(5):1157–1172. doi:10.1007/s12325-017-0523-x
42. Zeitoun J-D, Morvan Y. Patients’ perceptions and preferences regarding two different forms of methotrexate autoinjectors for moderate to severe rheumatoid arthritis: a European crossover survey. Patient Prefer Adherence. 2020;14:2177–2185. doi:10.2147/PPA.S269575
43. Domanska B, VanLunen B, Peterson L, Mountian I, Schiff M. Comparative usability study for a certolizumab pegol autoinjection device in patients with rheumatoid arthritis. Expert Opin Drug Deliv. 2017;14(1):15–22. doi:10.1080/17425247.2016.1256283
44. Thakur K, Biberger A, Handrich A, Rezk MF. Patient perceptions and preferences of two etanercept autoinjectors for rheumatoid arthritis: findings from a patient survey in Europe. Rheumatol Ther. 2016;3(2):245–256. doi:10.1007/s40744-016-0048-9
45. Thakur K, Biberger A, Handrich A, Rezk MF. Perceptions and preferences of two etanercept autoinjectors for rheumatoid arthritis: a new European Union-approved etanercept biosimilar (Benepali®) versus etanercept (Enbrel®) – findings from a nurse survey in Europe. Rheumatol Ther. 2016;3(1):77–89. doi:10.1007/s40744-016-0035-1
46. Xiao X, Li W, Clawson C, et al. Evaluation of performance, acceptance, and compliance of an auto-injector in healthy and rheumatoid arthritic subjects measured by a motion capture system. Patient Prefer Adherence. 2018;12:515–526. doi:10.2147/PPA.S160394
47. Karlsdottir K, Gunnarsdottir AI, Grondal G, et al. A patients’ perspective towards the injection devices for Humira® and Imraldi® in a nationwide switching program. Front Med. 2022;9:799494. doi:10.3389/fmed.2022.799494
48. Arshad N, Ahmad NM, Saeed MA, Khan S, Batool S, Farman S. Adherence to methotrexate therapy in rheumatoid arthritis. Pak J Med Sci. 2016;32(2):413–417. doi:10.12669/pjms.322.9566
49. Coyne M, Rinaldi A, Brigham K, et al. Impact of routines and rituals on burden of treatment, patient training, cognitive load, and anxiety in self-injected biologic therapy. Patient Prefer Adherence. 2022;16:2593–2607. doi:10.2147/PPA.S375037
50. Schiff M, Saunderson S, Mountian I, Hartley P. Chronic disease and self-injection: ethnographic investigations into the patient experience during treatment. Rheumatol Ther. 2017;4(2):445–463. doi:10.1007/s40744-017-0080-4
51. Feagan BG, Marabani M, Wu JJ, Faccin F, Spronk C, Castaneda-Hernández G. The challenges of switching therapies in an evolving multiple biosimilar landscape: a narrative review of current evidence. Adv Ther. 2020;37(11):4491–4518. doi:10.1007/s12325-020-01472-1
52. Reich K, Sorbe C, Griese L, Reich JLK, Augustin M. The value of subcutaneous vs. oral methotrexate: real-world data from the German psoriasis registry PsoBest. Br J Dermatol. 2021;184(4):765–767. doi:10.1111/bjd.19690
53. Patil P, Parker RA, Rawcliffe C, et al. Methotrexate-induced nausea and vomiting in adolescent and young adult patients. Clin Rheumatol. 2014;33(3):403–407. doi:10.1007/s10067-013-2389-x
54. Falvey S, Shipman L, Ilowite N, Beukelman T. Methotrexate-induced nausea in the treatment of juvenile idiopathic arthritis. Pediatr Rheumatol Online J. 2017;15(1):52. doi:10.1186/s12969-017-0180-2
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.