")
Back to Journals » Infection and Drug Resistance » Volume 17
Infectious Diarrhea Caused by Nocardia farcinica in a 19-Month-Old Child
Authors Yang J, Hu D, Yin K, Li F, Shi D
Received 2 November 2023
Accepted for publication 12 March 2024
Published 20 March 2024 Volume 2024:17 Pages 1131—1134
DOI https://doi.org/10.2147/IDR.S446032
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Jing Yang,1,* Dixia Hu,2,* Kaige Yin,3 Fang Li,4 Dongyan Shi5
1Hebei Provincial Center for Clinical Laboratories, The Second Hospital of Hebei Medical University, Shijiazhuang, People’s Republic of China; 2Department of Clinical Lab, Zhangjiakou First Hospital, Zhangjiakou, People’s Republic of China; 3Department of Gastroenterology, The Second Hospital of Hebei Medical University, Shijiazhuang, People’s Republic of China; 4Department of Pediatrics, The Second Hospital of Hebei Medical University, Shijiazhuang, People’s Republic of China; 5Department of Clinical Lab, The Second Hospital of Hebei Medical University, Shijiazhuang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Dongyan Shi, Email [email protected]
Background: Nocardia farcinica, a pathogen known for its strong pathogenicity, is frequently implicated in skin, central nervous system, and lung infections among immunosuppressed hosts, while intestinal nocardiosis is rare. We report the case of infectious diarrhea caused by N. farcinica in a child.
Case Presentation: A 19-month-old female child was admitted to the hospital with fever and diarrhea after the consumption of oranges. The etiological agent responsible for the diarrhea was identified through the examination of fecal smears using weak acid-fast staining and conducting fecal cultures. Whole-genome sequencing was employed to analyze the causative gene. Subsequent to a 5-day treatment regimen with amoxicillin-clavulanate at a dosage of 30 mg/kg every 12 hours, the child’s condition improved significantly, leading to an uncomplicated discharge.
Conclusion: This case illustrates the presence of intestine virulence factors in N. farcinica capable of causing diarrhea. The utilization of weak acid-fast staining in the examination of fecal smears is crucial for the accurate diagnosis of infectious diarrhea caused by Nocardia spp.
Keywords: Nocardia farcinica, diarrhea, virulence factors
Introduction
Nocardia are filamentous, aerobic, gram-positive bacteria that commonly cause pulmonary infections in immunosuppressed individuals and skin nocardiosis in those that are immunocompetent.1 N. farcinica, known for its pronounced pathogenicity, is frequently associated with infections affecting central nervous system, blood,2,3 as well as causing pleurisy4 and peritonitis.5 However, isolated abdominal or retroperitoneal nocardiosis has been reported, and liver abscesses6 and kidney abscesses7 are the most common infection site in intra-abdominal nocardiosis, and intestinal nocardiosis is rare. The route of Nocardia acquisition leading to abdominal remains unclear in most case reports.8 Hematologic dissemination after pulmonary or percutaneous inoculation and direct abdominal inoculation have been suggested to occur.9 The occurrence of direct intestinal infection has not been reported at present. We report the case of infectious diarrhea caused by N. farcinica in a child.
Case Report
A previously healthy 19-month-old female child was hospitalized due to fever and diarrhea, which manifested a day after eating oranges. The child’s maximum recorded body temperature was 39.0°C. She presented with green watery stools devoid of mucus or pus (Figure 1a) and experienced moderate stool volumes exceeding 10 times a day. No symptoms of chills, convulsions or vomiting were observed. Physical examination revealed that the child had a body temperature of 37.8°C, a heart rate of 120 beats per minute, a respiratory rate of 30 breaths per minute, moderate nutritional status, an anemic appearance, an absence of rash and foveal depression, clear bilateral breath sounds, a soft abdomen without tenderness, active bowel sounds, and no other discernible abnormalities. The results of routine blood test indicated a white blood cell count was 14.21×109/L, a neutrophil rate was 62.9% and a lymphocyte rate was 29.6%. A routine stool test indicated 5–6 white cells/HP and 2–3 red blood cells/HP. The erythrocyte sedimentation rate was 32mm/h, and the C-reactive protein count was 22.8mg/L. The levels of IgA, IgE, IgM, IgG, ASO and RF were normal.
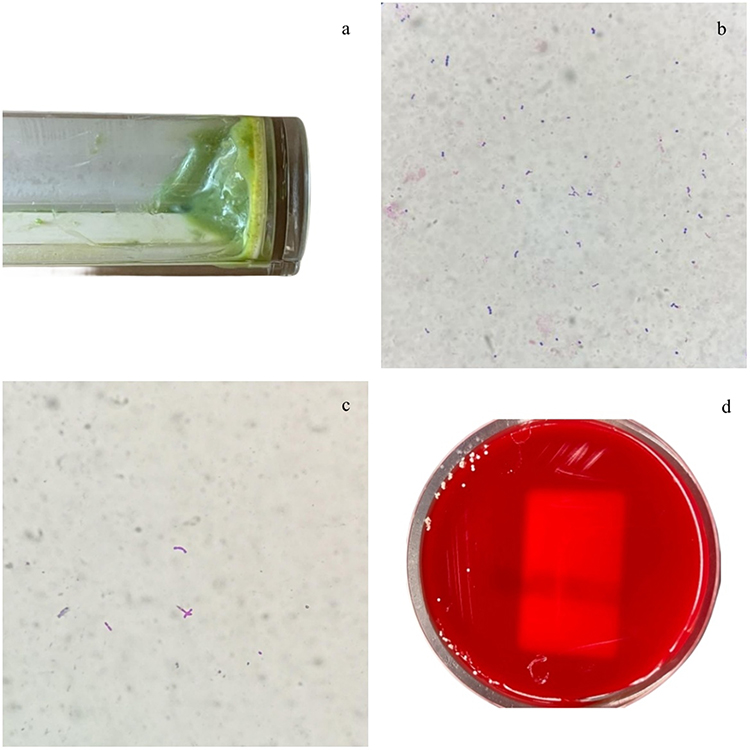 |
Figure 1 (a) Green watery stool specimen from the child; (b) Gram-positive slender bacilli with a non-uniform color fecal smear(Gram staining, 1000×); (c) Acid-fast staining portion weak-positive fecal smear(Weak acid-fast staining, 1000×); (d) Colony morphology after 48h incubation by fecal on Columbia blood plate. |
Gram staining of fecal smear showed gram-positive slender bacilli with non-uniform color (Figure 1b). The acid-fast staining results for the fecal smears were negative, while weak acid-fast staining yielded positive results (Figure 1c). The fecal sample was cultured on Columbia blood, MacConkey and Salmonella-Shigella agar (SS) plates for 48h. After this incubation period, there was no bacterial growth on MacConkey and SS plates; however, small, dry, non-hemolytic colonies were detected on Columbia blood plates (Figure 1d). The bacteria, identified as N. farcinica by MALDI-TOF MS (bioMérieux, Marcy-l’Étoile, France), were gram-positive rod-shaped organisms growing in a branch formation and exhibiting positive weak acid-fast staining. This bacterium was susceptible to linezolid, amikacin, trimethoprim-sulfamethoxazole (TMP-SMX), doxycycline, minocycline, imipenem, amoxicillin-clavulanate, ciprofloxacin, and moxifloxacin and resistant to ceftriaxone, clarithromycin, and tobramycin, as determined by the Sensititre Rapmyco Susceptibility Test (Thermo Fisher Scientific, Waltham, MA, USA).
The treatment regimen consisted of intravenous administration of amoxicillin-clavulanate at a dosage of 30 mg/kg every 12 hours for 5 days. After this treatment period, the child’s fever and diarrhea subsided, and both the blood white cell count and erythrocyte sedimentation rate returned to normal levels. Fecal white cell counts and cultures yielded negative results. Consequently, the child’s condition improved significantly, leading to an uncomplicated discharge.
The pathogenic genes were analyzed through whole genome sequencing which was performed by Personal Biotechnology Company (Shanghai, China) using the Nanopore PromrthION48 platform/Pacific Biosciences platform (Oxford, UK) and the Illumina Novaseq platform 6000 System (San Diego, CA, USA). Within the N. farcinica chromosome, numerous potential virulence-related genes were identified, including the mce operon, and the heat shock protein transcriptional repressor HspR, both recognized as virulence factors of Mycobacterium tuberculosis. Additionally, Catalases (KatG), superoxide dis mutases (SodA), and alkylhydroperoxidase (AhpD) were also identified, likely playing a role in the protection of the bacteria against reactive oxygen species produced by phagocytes. The strain was noted to carry six plasmids, with pNF1 (184,027 bp) and pNF2 (87,093 bp) encoding 160 and 90 kDa proteins, respectively. The remaining four smaller plasmids may have originated from Escherichia coli O157:H7 or Salmonella enterica subsp. However, it is unclear whether these plasmids are related to the observed diarrhea. The accession number of the sequences was CP133580, CP133581, and CP133582.
Discussion
Nocardia are ubiquitously present in soil, water and decomposing vegetation. Nocardia usually infects hosts through inhalation or inoculation through respiratory or dermal routes.10 While opportunistic Nocardia infections are prevalent in immunocompromised individuals, approximately one-third of cases arise in those without discernable underlying conditions.11 In immunocompetent individuals, nocardiosis often remains confined to the site of inoculation. The previous report suggests the occurrence of direct intestinal inoculation.9 In this case, the patient was a 19-month-old child who exhibited no immunodeficiency but had a history of consuming spoiled food. Therefore, we suspected that the diarrhea was caused by food contamination.
The patient presented with characteristic symptoms of diarrhea and was supported by laboratory markers. Our diagnosis is supported by the positive weak acid-fast staining of the fecal smear and positive fecal cultures for N. farcinica, while ruling out other pathogens. This is a unique case of diarrhea caused by Nocardia. The weak acid-fast staining of the fecal smear raised suspicion of Nocardia, which was subsequently cultured and identified as N. farcinica. This finding suggests a potential association between N. farcinica and acute diarrhea. However, it is important to recognize the limitations exist in accurately identifying Nocardia as the causative agent of diarrhea, which could lead to the oversight of certain pathogens. In the future, application of metagenomics next generation sequencing may facilitate the discovery of additional pathogens, leading to more definitive diagnoses.
Common antibiotics for Nocardia infections include TMP-SMX, linezolid, and amikacin.12 In this case, the decision to use amoxicillin-clavulanate for treatment was based on the patient’s young age, with the goal of minimizing potential side effects. After prompt treatment, the child rapidly recovered without any sequelae, indicating the diarrhea caused by food-derived Nocardia is responsive to antibiotic treatment and may even be self-limiting.
To confirm the identity of the virulence gene carried by this strain, we conducted an analysis of the causative gene using whole-genome sequencing. N. farcinica harbors several virulence genes, including the mce operons commonly found in actinomycetes, contributing to the pathogenicity of this bacterial group.13 Notably, M. tuberculosis antigen 85 family proteins, recognized as fibronectin-binding proteins, have been characterized, with N. farcinica containing 12 such protein.13
Typically, the published genomes of N. farcinica demonstrate the presence of at least two plasmids. Interestingly, the strain isolated from the child carried six plasmids, with four potentially originating from Escherichia coli O157:H7 or Salmonella enterica subsp. The potential correlation may arise from their presence in the gastrointestinal tract and the transmission of plasmids facilitated by Enterobacteriaceae. While no virulence genes were detected on these plasmids, it remains unclear whether their presence is associated with diarrhea. Therefore, it is crucial to focus on the potential dissemination of virulence and resistance genes through plasmid transmission.
In summary, Nocardia could be a potential cause of acute diarrhea. Conventional antibiotic treatment has proven to be effective against diarrhea caused by N. farcinica. Weak acid-fast staining of fecal smears is required for the diagnosis of infectious diarrhea. Additionally, the utilization of whole-genome sequencing greatly aids in the investigation of potential virulence factors.
Ethical Approval Statement and Informed Consent
This study was approved by the Ethics Committee of the Second Hospital of Hebei Medical University, with approval number 2022-C022. Written informed consent for publication of case details was obtained from the patient’s parent.
Acknowledgments
We thank the Zhangjiakou First Hospital for their effort in medical records management. We thank International Science Editing for editing this manuscript.
Funding
This study was supported by Natural Science Foundation of Hebei Province (H2022206277).
Disclosure
The authors declare no potential conflicts of interest.
References
1. Brown-Elliott BA, Brown JM, Conville PS, et al. Clinical and laboratory features of the Nocardia spp. based on current molecular taxonomy. Clin Microbiol Rev. 2006;19(2):259–282. doi:10.1128/CMR.19.2.259-282.2006
2. Williams E, Jenney AW, Spelman DW. Nocardia bacteremia: a single-center retrospective review and a systematic review of the literature. Int J Infect Dis. 2020;92:197–207. doi:10.1016/j.ijid.2020.01.011
3. Averbuch D, De Greef J, Duréault A, et al. Nocardia Infections in Hematopoietic Cell Transplant Recipients: a Multicenter International Retrospective Study of the Infectious Diseases Working Party of the European Society for Blood and Marrow Transplantation. Clin Infect Dis. 2022;75(1):88–97. doi:10.1093/cid/ciab866
4. Canouï E, Blanc K, Loubinoux J, et al. The value of molecular techniques to diagnose Ureaplasma urealyticum and Nocardia farcinica pleuropneumonia in a patient with diffuse large B-cell lymphoma. Int J Infect Dis. 2017;64:93–95. doi:10.1016/j.ijid.2017.09.015
5. Adapa S, Naramala S, Gayam V, et al. An Unusual Presentation From a Sporadic Partially Acid-Fast Aerobic Actinomycete Resistant to Common Antibiotics. J Investig Med High Impact Case Rep. 2020;8:2324709619899598. doi:10.1177/2324709619899598
6. Singh S, Verma Y, Pandey P, et al. Granulomatous hepatitis by Nocardia species: an unusual case. Int J Infect Dis. 2019;81:97–99. doi:10.1016/j.ijid.2019.01.046
7. Xu J, Yachnis AT, Malaty I. An independent elderly woman with rapid onset of coma. JAMA Neurol. 2014;71(8):1043–1047. doi:10.1001/jamaneurol.2014.449
8. Kamyab A, Fakhoury JDJ, Sutkowski R, et al. Fulminant colitis secondary to nocardiosis. Int J Colorectal Dis. 2012;27(6):841–842. doi:10.1007/s00384-011-1327-0
9. Tramèr L, Mertz KD, Huegli R, et al. Intra-Abdominal Nocardiosis-Case Report and Review of the Literature. J Clin Med. 2020;9(7):2141. doi:10.3390/jcm9072141
10. Hamdi AM, Fida M, Deml SM, et al. Retrospective analysis of antimicrobial susceptibility profiles of Nocardia species from a tertiary hospital and reference laboratory, 2011 to 2017. Antimicrob Agents Chemother. 2020;64(3):e01868–19. doi:10.1128/AAC.01868-19
11. Haussaire D, Fournier PE, Djiguiba K, et al. Nocardiosis in the south of France over a 10-years period, 2004-2014. Int J Infect Dis. 2017;57:13–20. doi:10.1016/j.ijid.2017.01.005
12. Jing Y, Hong-Tao R, Jie W, et al. Clinical characteristics, susceptibility profiles, and treatment of nocardiosis: a multicenter retrospective study in 2015-2021. Int J Infect Dis. 2023;130:136–143. doi:10.1016/j.ijid.2023.02.023
13. Ishikawa J, Yamashita A, Mikami Y, et al. The complete genomic sequence of Nocardia farcinica IFM 10152. Proc Natl Acad Sci USA. 2004;101(41):14925–14930. doi:10.1073/pnas.0406410101
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.