")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Increasing Risk of Dementia Among Patients with Subsequent Epilepsy Within 2 Years Post-Traumatic Brain Injury: A Population‐Based Case-Control Study
Authors Chu SF, Liao KH, Wei L
Received 28 November 2023
Accepted for publication 13 March 2024
Published 30 March 2024 Volume 2024:17 Pages 1447—1457
DOI https://doi.org/10.2147/JMDH.S452086
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pavani Rangachari
Shu-Fen Chu,1 Kuo-Hsing Liao,2– 5 Li Wei2,6
1College of Nursing and Health Management, Shanghai University of Medicine and Health Sciences, Shanghai, People’s Republic of China; 2Division of Neurosurgery, Department of Surgery, Wan Fang Hospital, Taipei Medical University, Taipei, Taiwan; 3Division of Critical Medicine, Department of Emergency and Critical Medicine, Wan Fang Hospital, Taipei Medical University, Taipei, Taiwan; 4Department of Neurotraumatology and Intensive Care, Taipei Neuroscience Institute, Taipei Medical University, Taipei, Taiwan; 5Division of Neurosurgery, Department of Surgery, School of Medicine, College of Medicine, Taipei Medical University, Taipei, Taiwan; 6Graduate Institute of Injury Prevention and Control, Taipei Medical University, Taipei, Taiwan
Correspondence: Li Wei, Graduate Institute of Injury Prevention and Control, Taipei Medical University, 250 Wu-Hsing Street, Taipei City, Taiwan 110, Taiwan, Email [email protected]
Background: Although the association between neurodegenerative diseases, such as dementia, and traumatic brain injury (TBI) has long been known, the association between dementia and TBI with epilepsy has been controversial.
Aim: This data-driven population-based study is designed to investigate the association between dementia and epilepsy after TBI within a 2-year period.
Methods: This case-control cohort study was conducted using the Longitudinal Health Insurance Database 2000 (LHID2000). We included 784 individuals ambulatory or hospitalized for TBI with epilepsy from 2001 to 2011, compared with 2992 patients with TBI without epilepsy who were matched for characteristics including sex, age, and healthcare resource use index date. Every participant was followed up for 5 years to ascertain any dementia development. Data were stratified and analyzed using the Cox proportional hazards regression.
Results: Through the 5-year follow-up period, 39 patients (5.21%) with TBI with epilepsy and 55 (1.53%) with TBI without epilepsy developed dementia. TBI with epilepsy was independently associated with a > 3.03 times risk of dementia after correcting for age, sex, and comorbidities.
Conclusion: These findings suggest an increased risk of dementia in patients with TBI with epilepsy. Our research recommends that individuals with TBI and epilepsy be monitored more intensively.
Keywords: neurodegenerative diseases, dementia, epilepsy, traumatic brain injury, data-driven, population-based study
Introduction
Dementia in the aging population is a significant public health issue. A study estimated that there were 24.3 million patients with dementia globally in 2005, predicted to reach 81.1 million in 2040.1 This number is expected to treble by 2050.2 Dementia is diagnosed ordinarily when developed cognition impairment becomes more severe to disturb social and/or occupational function, using standard criteria such as the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition.3 Memory loss is caused by a variety of cognitive capacities or a general cognition deterioration, not just memory.4–6 To our knowledge, the mechanisms could be β-amyloid deposits, hippocampal damage, or chronic infections.7 The causes of dementia are numerous and include original neurologic, neuropsychiatric, and medical conditions. In older adults, neurodegenerative dementias are the most common, such as Alzheimer disease and dementia with Lewy bodies. The incidence of dementia rises gradually until age 85 or 90 years and is greater in women. Annual age-specific rates varied from 0.1% at age 60–64 years to 8.6% at age 95 years.8 The global annual cost of dementia is estimated to be >800 billion United States (US) dollars for individuals, their families, and health and social care systems.9 Notably, dementia is not amenable to modification through current interventions. Consequently, dementia has become a major contributor to significant rise in disease burden.
Epilepsy is characterized by a long-term predisposition to epileptic seizures. A clinical manifestation of epileptic seizures involves abnormal and excessive neuronal discharge (International League Against Epilepsy Commission Report) with sudden, varied, and temporary onset. It includes various events affecting consciousness, motor function, sensory perceptions, and psychiatric states.10 Several studies have shown that the estimated incidence of epilepsy is 43 per 100,000 people in developed countries and is approximately twice that in the developing world.11,12 Epilepsy affects approximately 50 million people worldwide.13 Posttraumatic epilepsy is the most common trigger of new-onset epilepsy in young adults, with an incidence of up to 30,000 per year in the US, and it has been linked to the location, type, and severity of the injury.14 Surina F. et al provided valuable insights into the occurrence and meaning of dissociative seizures after mild traumatic brain injury (TBI) and the impact of types of intracranial hemorrhage on the risk of later epilepsy, along with risk factors causal to the risk of posttraumatic epilepsy.15 The incidence is about 5% and the prevalence is nearly 20% in the epilepsy population, may be because of previous TBI.14,16 Patients with posttraumatic epilepsy have a higher risk of posttraumatic epilepsy after TBI, and lesion site, size, and type are predictors of posttraumatic epilepsy.14 Many studies demonstrated the accumulation of β -amyloid (Aβ) peptide in animal models of Alzheimer disease, leading to recurrent seizure activity. Similar mechanisms have been suggested in the disease. Lesion epilepsy is fitted with subgroups of focal epilepsy that are attributable to fundamental etiologies, including hippocampal sclerosis, TBI, cerebrovascular disease, brain tumors, and central nervous system infections.17,18 Dementia increases the risk of subsequent epilepsy, particularly in patients with young-onset Alzheimer disease.19,20 Increased morbidity and mortality of epilepsy can severely impact the quality of life.21,22
TBI is a major cause of morbidity and mortality worldwide owing to its high prevalence, comprehensive risk factors, and considerable long-term familial and societal impact. The Department of Defense’s Clinical Practice Guideline for Management of Concussion/Minor Traumatic Brain Injury in the US (version 1.0, April 2009) states that TBI is induced structural injury traumatically and/or brain function, which physiologically disrupts the result of an external force that is indicated by new onset or worsening of at least one of the following clinical signs immediately following the event.23 In TBI, all insults to the brain result in primary and secondary damage to the brain parenchyma. Secondary damage is often related to molecular mechanisms that occur after TBI. Secondary damage may result in the prominent mechanisms underlying neuroinflammation and cytokine damage. Due to its high incidence rate and often enduring sequelae, in addition to the pathophysiology of TBI, focusing on Alzheimer disease, epilepsy, and chronic traumatic encephalopathy would contribute significantly to increasing healthcare expenditures annually.24–26 The prevalence of dementia is similar in veteran and civilian populations, and the risk of dementia is likely to be increased by TBI.27 Additionally, evidence has shown that the Hazard Ratio for dementia is higher in patients with repeat TBI than in patients with TBI.7,28 Several studies have shown that long-term brain changes and pathological biomarker accumulation (eg, amyloid and tau proteins) are associated with a prior history of moderate-to-severe TBI and have also validated that individuals with moderate-to-severe injuries develop a higher risk of dementia.29–32 Many processes following TBI may cause circuit changes that result in subsequent epilepsy, especially inflammation, oxidative stress, and the later phases of neurodegeneration and regeneration.15 Factors related to postinjury damage and age-related brain changes in cognitive decline and dementia.33 One of the most common presentations of seizures is TBI, which has different effects at various points after injury. The incidence of early seizures was 4.5% in 1000 patients with TBI and was related to skull fractures or intracranial hemorrhage.34 Therefore, the risk of dementia-associated epilepsy between patients with and without TBI is controversial. Studies have suggested that epilepsy impairs cognitive function, which is a common symptom of dementia. However, associations between dementia and epilepsy have not been studied among patients with a higher risk of a prior history of TBI within 2 years. This case-control study aimed to investigate the association between dementia and subsequent epilepsy within 2 years after TBI using a data-driven population-based dataset.
Materials and Methods
Database
In this population-based case-control study, sample patients were retrieved from the Taiwan “Longitudinal Health Insurance Database 2000” (LHID2000) were retrieved). This dataset provides a tremendous opportunity to track enrollees’ healthcare utilization since 1995, the year of the Administration of Health Insurance operations in Taiwan. The Health and Welfare Data Science Center, Ministry of Health and Welfare, collects the LHID2000, which attributes the fundamental medical claims dataset of 2,000,000 patient registration files to a random sample retrieved from over 23,000,000 enrollees of the Administration Health Insurance Research Claim Dataset in Taiwan. The Department of National Health Insurance stated no suggestive differences in sex, age, or measurement of typical payroll-linked insurance expenditures among the LHID2000 fundamental participants. As the LHID2000 was collected from de-identified data for research, this research was reviewed comprehensively by the institutional review board. The Health and Welfare Data Science Center and other researchers validated the LHID2000 dataset. Researchers can approach the data for research purposes and employ the LHID2000 for publication in peer-reviewed journals.35,36
Study Sample
The Health and Welfare Data Science Center, Ministry of Health and Welfare, provided a dataset from 2000 to 2018. This case-control cohort study included patients with a first-time diagnosis of TBI (ICD-9-CM codes: 800. XX~804.XX, 850.XX~854.XX) patients at clinics and hospital departments from January 1, 2001, to December 31, 2011, followed by follow-up epilepsy (ICD-9-CM code 345) occurring or non-onset within 2 years. To certify a clinically homogeneous sample, we checked our sample of an adult population aged >18 years. We also excluded those diagnosed with epilepsy and/or dementia within one year before their first diagnosis of epilepsy. In total, 748 patients were included in the case group.
A control group was extracted from the dataset of the LHID2000 remaining patients. First, we excluded participants who had prior Administration Health Insurance dataset claim records specifying the diagnosis of those with epilepsy and/or dementia within one year before their first diagnosis of epilepsy and those aged <18 years (n=4065). We randomly chose 2992 beneficiaries (four comparison subjects for each TBI patient without epilepsy) between January 1, 2001, and December 31, 2011. We identified the first outpatient care visit in the index date healthcare resource using year; then, we matched sex and age from January 1, 2001, to December 31, 2011.
Every individual (n=3740) was followed up until they developed dementia over the following 5 years. Furthermore, all patients were diagnosed with dementia using the International Classification of Diseases (ICD) system ([ICD]-9-CM 290, 330–331 code and [ICD]-10-CM F00, F01, F02, F03, G30 – G31 code [because of the NHI switch to ICD-9 and −10 codes in 2016]). As dementia is considered a disability by degree under the Administration Health Insurance guidelines of long-term care payments, disability severity would allow these patients to use any medical resource without copayments at any institution of medical access. This concern may increase patients’ financial access to medical institutions when needed. It could be noticed that to diminish abuse, the appropriate diagnosis of dementia is sensibly supervised and audited as needed by Administration Health Insurance. Thus, dementia diagnostic validity, clinical error, or diagnostic upcoding in the Administration Health Insurance claims dataset is considered vigorous. This study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Taipei Medical University (approval number: TMU-JIRB NO. N202109070).
Statistical Analysis
The principal endpoint of our study was an individual who had access to medical care visits or endured hospitalization for dementia. All statistical analyses were performed using the SAS statistical package (SAS System for Windows, version 9.2; SAS Institute Inc.). The Pearson Chi-square test was used to analyze the variations between the case group patients and the control group patients in terms of monthly income and residence urbanization level from the highest (level I) to least level (level IV) and selected baseline of comorbid diseases (including stroke, diabetes, hyperlipidemia, hypertension, coronary heart disease, heart failure, and atrial fibrillation). These specific medical comorbidities are possible risk factors for dementia; if diagnosed before the index date, they were included. Stratified Cox proportional hazard regression was used to appraise the relationship between dementia and Subsequent Epilepsy within 2 years after Traumatic Brain Injury and subsequent dementia until the development of dementia 5 years after their index medical utilization date. We calculated Hazard ratios (HRs) and 95% confidence intervals (CI) and used a significance level of 0.05. We also investigated the association between epilepsy and dementia in diverse sex groups. We analyzed the incidence of dementia between two groups of patients with TBI with or without subsequent epilepsy within a 2-year period after TBI. The Kaplan–Meier method was used to calculate the 5-year survival rates of dementia patients using the Log rank test to assess differences between the two groups.
Results
Our study aimed to evaluate the association between dementia and epilepsy, which is a key contributor to a history of TBI within a 2-year period. In this study of 3740 sampled individuals, a case group comprising 748 TBI individuals with subsequent epilepsy within a 2-year period and 2992 TBI individuals without epilepsy were included as the control group.
Table 1 shows the demographic features of patients with TBI stratified by the occurrence of epilepsy. Of the 3740 sample patients, two-thirds were male (69.79%) and were stratified into age groups: 18–64, 65–74 and >75 years. The mean age was 47.8 years (standard deviation [SD]:19.2). Chi-squared tests showed no differences in age and sex among patients with TBI who had epilepsy and those who did not (p = 1.0000). Among the 3740 subjects, the incidence rates of dementia in a 5-year follow-up period were 5.21% (n=39) and 1.84% (n=55), respectively, for patients with TBI and epilepsy and those who did not have epilepsy. After matching for age and sex, stroke was more prevalent (p<0.0001) in individuals with TBI and epilepsy than those without epilepsy. No significant differences were observed in the selected comorbidities between the two groups.
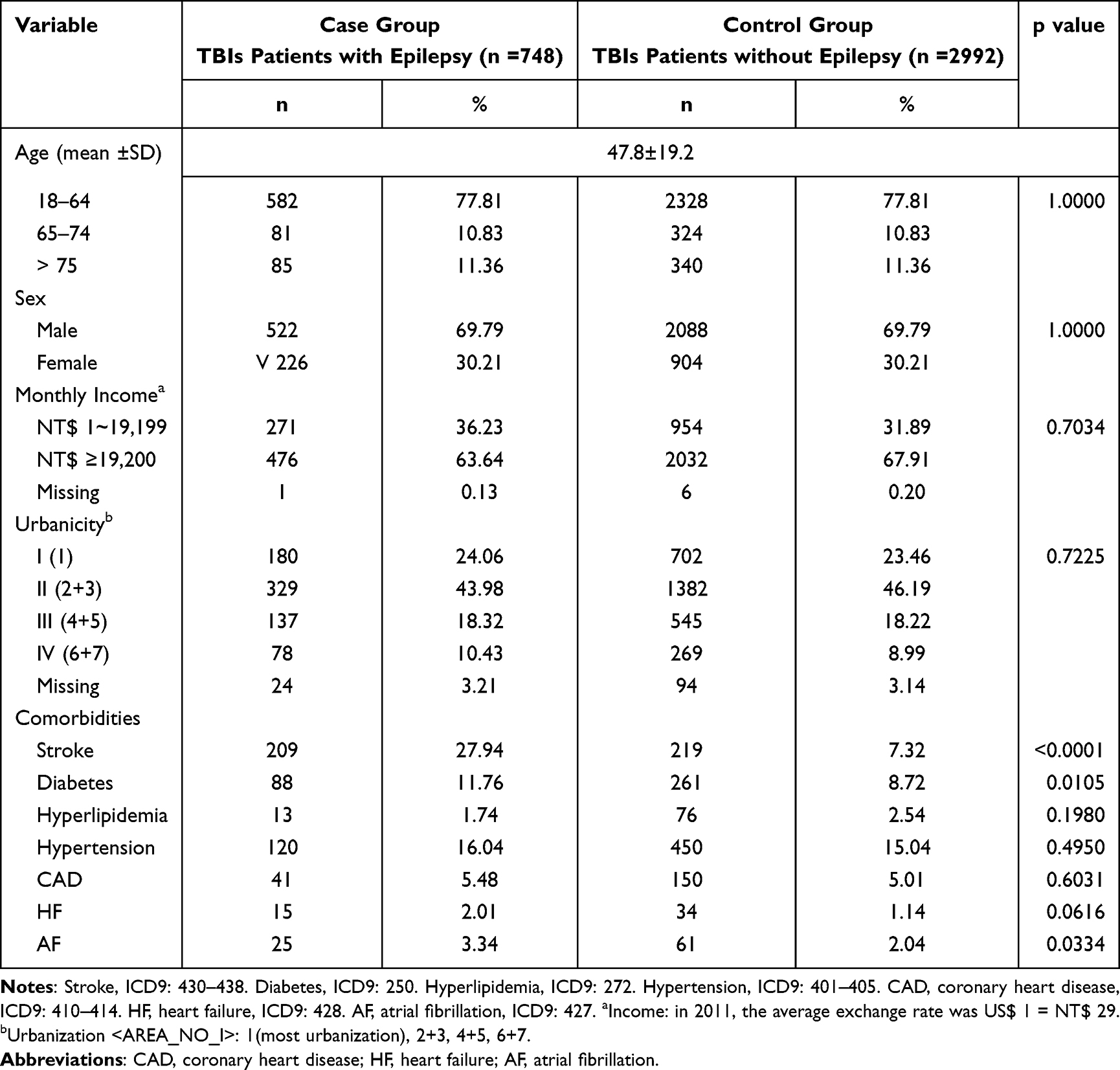 |
Table 1 TBI Demographic Features with and without Epilepsy (n = 3740) |
Table 2 shows the HRs, including crude and adjusted by stratified Cox proportional hazard regressions. In the study of 3740 patients, 5.21% suffered from dementia beneath the 5-year follow-up; the average dementia onset period was 1.32 years for patients with TBI with subsequent epilepsy of the study cohort and 2.59 years for patients with TBI without subsequent epilepsy of the comparison cohort. Compared with control group individuals, study group individuals were more likely to develop dementia than follow-up over the 5-year (HR: 3.16, 95% CI: 2.10–4.76, p<0.05). Next to adjusting patient age, sex, monthly revenue, geographic location and co-morbidities, the HR of dementia for patients with TBI with epilepsy was 3.03 (95% CI: 1.96–4.69, p<0.05) compared with patients with TBI without epilepsy. Figure 1 shows the free survival curves of patients with dementia using the Kaplan–Meier method. Among males, the adjusted hazard of dementia for the study group was 5.32 times (95% CI: 3.06–9.26) that of the control group. No increased risk of dementia was observed among female patients with TBI with epilepsy.
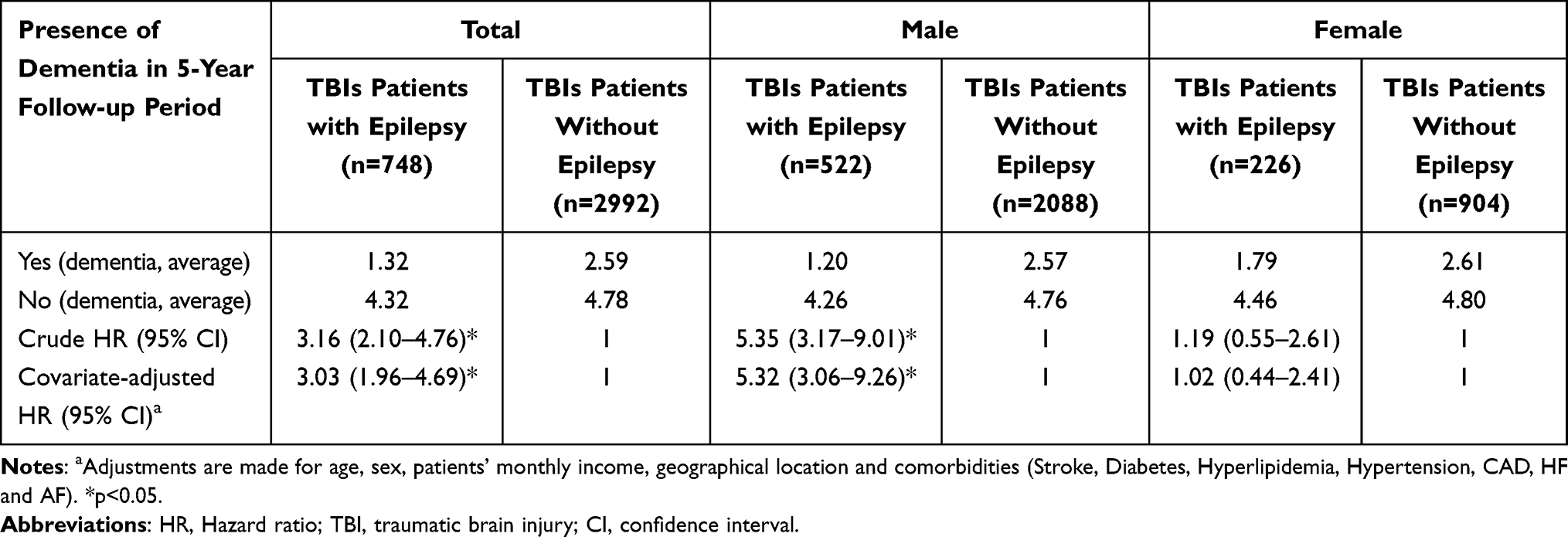 |
Table 2 Dementia Incidence Over 5-Year Follow-Up, HRs Next to Crude and Covariate-Adjusted, Indexed by Medical Utilization Initiation |
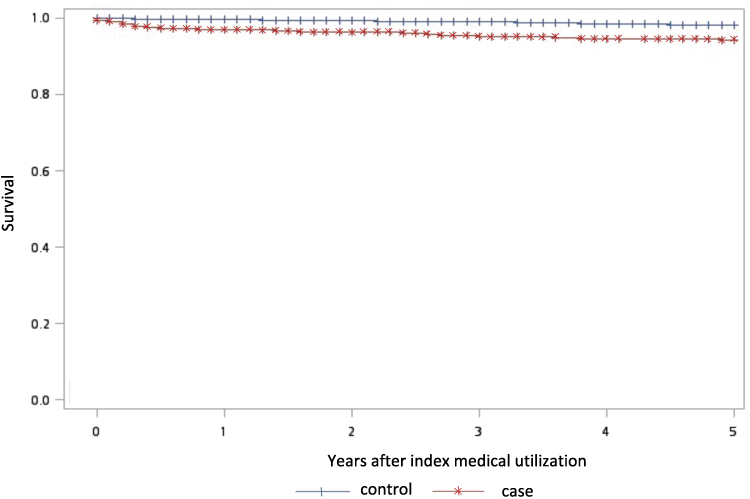 |
Figure 1 Presents the dementia-free survival curves using the Kaplan–Meier method. TBI Patients with epilepsy had significantly lower 5-year dementia-free survival rates than patients without epilepsy (Log rank test: 33.6462, p=<0.0001). |
Table 3 shows the dementia HR among the different age groups corresponding to the development of epilepsy in patients with a prior history of TBI within a 2-year period during the 5-year follow-up. In comparison with patients with TBI without epilepsy, we used Stratified Cox proportional hazard regressions to generate the effects for over 5 years. The HR for TBI with patients with epilepsy was 21.14 (95% CI: 7.22–61.86; p<0.05) in the 18–64 years group; and the HR was 3.69 (95% CI: 1.71–7.96; p<0.05) in the 65–74 years age group. Moreover, this study found that the HR after adjusting of dementia aged 18–64 years group in patients with TBI with epilepsy for 5 years follow-up was 14.37 (95% CI: 4.64–44.51; p<0.05); the adjusted HR of aged 65–74 years group in patients with TBI with epilepsy was 3.41 (95% CI 1.44–8.08; p<0.05). But no significant differences among groups were detected for HR (1.23, 95% CI: 0.57–2.66) and adjusted HR (0.98, 95% CI: 0.43–2.26) for the group aged >75 years. After adjusted HR of dementia for the 18–64 years age bracket for males in the study group was 18.19 times (95% CI: 5.09–64.93; p<0.05); the study group was 6.00 times (95% CI: 1.92–18.70; p<0.05) in the age group 65–74 years that of the comparison group. However, no meaningful differences were detected between groups for HR (1.51, 95% CI: 0.50–4.56) and adjusted HR (2.00, 95% CI: 0.62–6.42) for the >75 years age group. Increased HR for dementia was absent in female patients with TBI or epilepsy.
 |
Table 3 Crude and Adjusted HR for Dementia in Sampled Individuals of Atypical Age Groups Over a 5-Year Follow-Up Periods from the Index Date of Healthcare Utilization (n = 3740) |
Discussion
This data-driven population-based case-control cohort study revealed an association between dementia and epilepsy after TBI. We found that dementia was more often diagnosed in patients with TBI with epilepsy than those without epilepsy. The 3740 individuals in this study were more likely to be diagnosed with TBI without epilepsy than those in the case group. During the 5-year follow-up, epilepsy with a history of TBI within a 2-year period associated with the risk of subsequent dementia was more than tripled after adjusting for age, sex, patient income, geographical location, and comorbid diseases.
Furthermore, our research results are in accordance with those of prior studies that showed an association between dementia and epilepsy with a prior history of TBI and complicated their work by supporting the results of a data-driven population-based study on dementia and epilepsy.37 Many studies have shown an advanced risk of dementia, especially in individuals with a genetic predisposition. The cumulative incidence of dementia in individuals with TBI and epilepsy greatly exceeds this opportunity. The 10-year cumulative incidence of dementia was 22.20%, and dementia identification time was 5.4±3.9 years.38 More recently, a growing amount of research data consistently matching our results has validated that epilepsy among patients with a history of TBIs may increase the risk of dementia and has been suggested to increase the risk of dementia among patients with TBI with subsequent epilepsy.7,28
Several studies have explored the association between TBI and dementia.39–41 One study indicated that moderate TBI may have a two-fold increased risk of AD or other forms of dementia, and severe TBI may have a four-fold increased risk.42 Chu et al showed that dementia patients with TBI had an adjusted HR (HR = 3.21) for developing dementia compared with the control cohort. The advancing adjusted HR for dementia patients with repeated TBI was 3.62.28 Little et al reported that a positive TBI history is related to an increased incidence of neurological diseases and psychiatric comorbid conditions such as chronic traumatic encephalopathy, Alzheimer disease, Parkinson’s disease, and amyotrophic lateral sclerosis.43,44
However, the strength of the estimates of the associations between dementia TBIs and epilepsy varied. Injury mechanisms might explain the association between dementia, TBI, and epilepsy, and the risk of TBI in patients increases with age. The mechanisms thought to affect the incidence of dementia include amyloid accumulation, hippocampal injury, or chronic infection. Traumatic mechanisms that trigger neurodegeneration have been widely recognized. For instance, diffuse axonal injury with disrupted microtubule roles is important for providing a latent context for developing tau and amyloid pathology. However, the clinical diagnosis of subsequent traumatic dementia is difficult, and it is often problematic to distinguish the direct effects of TBI from those formed by progressive neurodegeneration or other subsequent traumatic sequelae, such as psychiatric disorders. Subsequent neuropathological dementia is gradually well characterized, with recent work focusing on chronic traumatic encephalopathy. Chronic traumatic encephalopathy can simply be recognized under dissection, and patients are often confused and concerned, most likely because of their subsequent traumatic problems.30 Clinically, chronic traumatic encephalopathy results in behavioral changes, decision-making dysfunction, memory loss, and cognitive damage that begin to progress continuously and slowly over the decades. Pathologically, chronic trauma encephalopathy leads to the atrophy of the frontal and temporal lobes, thalamus, and hypothalamus, septal defects, and abnormal bonds of hyperphosphorylated tau, such as neurofibrillary tangles and disordered neurites, throughout the brain.45 Survivors of TBI may harmfully disturb their psychological systems, rush the development of neurodegenerative diseases, and develop chronic disabilities due to their damage. Epilepsy is a chronic brain disease categorized by recurrent episodic onset, epileptic seizures, and somatic and psychiatric symptoms. The prevalence of active epilepsy was 6.4 per 1000, and the lifelong prevalence was 7.6 per 1000. The incidence of epilepsy was 61.4/per 100,000 person-years. Martin et al found that both neurological (dementia and traumatic brain injury) and psychiatric (depression and posttraumatic stress disorder (PTSD) factors meaningfully projected new-onset epilepsy in a population-based study of older adults.46 Hommet et al reported that epilepsy in patients with dementia substantially affects the diagnosis of underlying dementia.39 The prevalence of dementia ranged from 8.1 to 17.5 per 100 individuals with epilepsy. The prevalence of epilepsy in the pooled period of persons with dementia is 5 per 100 persons in a population-based study and 4 per 100 persons in a clinical setting.47 Chronic epilepsy, especially mesial temporal lobe epilepsy with hippocampal sclerosis, is related to cognitive impairment, which can be uncontrolled, secondary to underlying biological abnormalities. Although the prevalence of epilepsy varies, upper brain dysfunction is known to manifest as epilepsy.48 Our findings match those of studies on the association between TBI with epilepsy and dementia and consist of reports that TBI with epilepsy is associated with an increased prevalence of dementia.
Age is an important factor in the relationship between epilepsy and dementia. We found that age differentiation in the relationship between TBI with epilepsy and dementia was prominent and consistent with other reports. This study revealed that the HRs after crude and adjusted for dementia related to TBI with epilepsy were greater in younger patients. After considering confounding factors in our study, there was a higher proportion of cases in younger older adults with dementia (HR: 3.41; 95% CI: 1.44–8.08) compared with controls. In addition, the adjusted HR for dementia among the case group with TBI with epilepsy in the age groups of 18–64 and 65–74 years were 14.37 and 3.41, respectively; however, no statistical significance was observed in the group aged >75 years. Additionally, the association between TBI and epilepsy is significant in males. The development of epilepsy correlates with age not only because of age but also because aging progression could be a hazard factor for epilepsy.19,49,50 One of them would be occupied with clarifying the connection between aging and epilepsy, as the production of free radicals is a characteristic of neurodegenerative diseases such as Parkinson’s disease, stroke, and dementia.51–53 Most studies have reported a relationship between epilepsy and dementia, particularly in elderly populations.38,48,54,55 Japan is facing an increase in the number of patients with dementia, and the incidence rate of epilepsy is increasing in older adults. Ishigaki et al surveyed 279 patients with epilepsy admitted to a hospital between 2007 and 2012 and found that new-onset epilepsy occurred more frequently in elderly patients. Of 153 patients aged ≥65 with epilepsy, 20.2% had dementia as an underlying disease.48 Sen, A. et al evaluated the underlying initiation of epilepsy in the elderly population and showed cognitive, mental, and psychosocial comorbid conditions and the effect that epilepsy may have on the elderly broader social or care network in developed versus developing countries.55 One study showed that prevalence boosted with a cumulative level of intelligence disability, decreasing to 10.3% (95% CI 8.4–12.6) focusing on older people.56 In Europe, the prevalence of dementia is assessed to be nearly 6–8% after age 65 years and may increase to 20–30% in individuals aged >85 years. Some studies have reported that the lifetime prevalence is 7.6 per 1000 people, increasing with age. The progressive aging of the world ‘s population would be associated with an increase in the frequency of epilepsy. Friedman et al showed that evidence has renowned boosted seizure risk increases with increasing dementia severity or with a younger age of Alzheimer disease onset. Recent studies have shown that elderly people with epilepsy are more likely to experience cognitive dysfunction, which may indicate a vital bidirectional association between epilepsy and dementia.57 Epilepsy has a bimodal distribution matching age, with the highest peaks in young individuals and older people.58
Consistent with previous studies, our observed age and sex differences in the relationship between TBI, epilepsy and dementia were substantial among the younger male population. Compared with female patients, younger male patients were more likely to develop dementia during the 5-year follow-up (adjusted HR: 18.19, 95% CI: 5.09–64.93 and adjusted HR: 6.00, 95% CI: 1.92–18.70 in the subgroup of patients aged 18–64 and 65–74 years, with no significant difference in the group of those aged >75). Moreover, sex was correlated with the clinical outcomes of dementia. The mechanisms underlying age and gender in the association among dementia, TBI, and epilepsy remain unclear, and further research is essential to clarify this correlation.
In this study, we provided an enormous sample size and appropriate statistical power to assess the association between dementia, TBI, and epilepsy. Nationally, sampling can reduce the selection bias of a single clinic or hospital sample. However, some limitations of our research will be discussed. First, data that might be linked to both TBI with epilepsy and dementia, such as diet patterns, alcohol use, obesity, and tobacco use, were inaccessible in this study. These confounding factors may have affected the association between epilepsy and dementia. Second, the diagnoses of TBI with epilepsy and dementia affording diagnosis codes from governmental claims data might be less accurate than those of TBI with epilepsy and dementia clarified by diagnostic tests. However, routine validations implemented by administrative health insurance may avoid unfitting coding or incorrect medical claims; this procedure involves multiciliary measures for such differences. Third, the study population primarily consisted of Chinese individuals; therefore, the generalizability to other ethnic populations may be limited. Fourth, we did not include participants with dementia or controls who had TBI without epilepsy or dementia prior to the year 2000 because the Administration Health Insurance operation claims data only provided medical records for samples from 1996 onwards. Finally, the Administration Health Insurance operation secondary data does not contain sufficient information about patient status to determine the severity of TBI with epilepsy or dementia. Furthermore, the subtypes of TBI with epilepsy or dementia were not considered in our study and should be explored in future research. These limitations may impact the research findings, and further research is required to address these factors. This data-driven population-based study has highlighted a higher percentage of patients with dementia were diagnosed with TBI and epilepsy than controls without epilepsy. A relationship between dementia, TBI, and epilepsy was established in this study. Subsequent studies are crucial for validating our findings and for advancing the quantitative assessment of the relationship between dementia, TBI, and epilepsy.
Conclusions
In this study, we recommend the superior monitoring of patients with TBI and epilepsy for long-standing neuropsychiatric sequelae in clinical and community settings. Psychiatric indicators should be assessed following epilepsy to identify possible secondary problems. Patients with TBI and epilepsy should be informed about potential cognitive and behavioral deficits. Timely psychiatric care can improve prognosis. Our findings suggest a potential association between patients with TBI with epilepsy within 2 years and dementia, offering significant evidence from a population to a selection of surveys in Asia. Our results support the need for further research to explore various potential pathways and gene–environment interfaces involved in the development of dementia and TBI in patients with epilepsy. This study highlights the importance of genetic markers and genetic predisposition to specific outcomes, as well as potential strategies for patients with TBI exhibiting epilepsy-related symptoms. Therefore, further studies in this area are crucial to address these issues and determine the effectiveness of appropriate TBI management in reducing the risk of dementia.
Abbreviations
CI, Confidence Interval; HR, Hazard ratio; ICD, International Classification of Diseases; LHID, Longitudinal Health Insurance Database; PTSD, Posttraumatic stress disorder; TBI, Traumatic brain injury.
Data Sharing Statement
In this population-based case-control study, sample patients were retrieved from the Taiwan “Longitudinal Health Insurance Database 2000” (LHID2000) were retrieved). This dataset provides a tremendous opportunity to track enrollees’ healthcare utilization since 1995, the year of the Administration of Health Insurance operations in Taiwan. The Health and Welfare Data Science Center, Ministry of Health and Welfare, collects the LHID2000, which attributes the fundamental medical claims dataset of 2,000,000 patient registration files to a random sample retrieved from over 23,000,000 enrollees of the Administration Health Insurance Research Claim Dataset in Taiwan. The Health and Welfare Data Science Center and other researchers validated the LHID2000 dataset. Researchers can approach the data for research purposes and employ the LHID2000 for publication in peer-reviewed journals.
Ethics Approval and Informed Consent
This study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Taipei Medical University (approval number: TMU-JIRB NO. N202109070).
Consent for Publication
There has no external images, videos, recordings, etc can be published in this research.
Acknowledgments
This is a short text to acknowledge the contributions of specific colleagues Mr. Van-We Lee, Taipei Medical University that aided the efforts of the authors.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Ferri CP, Prince M, Brayne C., et al. Global prevalence of dementia: a Delphi consensus study. Lancet. 2005;366(9503):2112–2117. doi:10.1016/S0140-6736(05)67889-0
2. Mohanannair Geethadevi G, Quinn TJ, George J, et al. Multi‐domain prognostic models used in middle‐aged adults without known cognitive impairment for predicting subsequent dementia. Cochrane Database Syst Rev. 2023;3:6.
3. Regier DA, Kuhl EA, Kupfer DJ. The DSM-5: classification and criteria changes. World Psychiatry. 2013;12(2):92–98. doi:10.1002/wps.20050
4. Sicras A, Rejas J, Arco S, et al. Prevalence, resource utilization and costs of vascular dementia compared to Alzheimer’s dementia in a population setting. Dement Geriatr Cognit Disord. 2005;19(5–6):305–315. doi:10.1159/000084556
5. Biedermann F, Fleischhacker WW. Psychotic disorders in DSM-5 and ICD-11. CNS Spectr. 2016;21(4):349–354. doi:10.1017/S1092852916000316
6. National Collaborating Centre for Mental H. National Institute for Health and Care Excellence: guidelines. In: Dementia: A NICE-SCIE Guideline on Supporting People with Dementia and Their Carers in Health and Social Care. Leicester (UK): British Psychological Society (UK) Copyright © 2007, The British Psychological Society & The Royal College of Psychiatrists; 2007.
7. Wang HK, Lin SH, Sung PS, et al. Population based study on patients with traumatic brain injury suggests increased risk of dementia. J Neurol Neurosurg Psychiatry. 2012;83(11):1080–1085. doi:10.1136/jnnp-2012-302633
8. Hugo J, Ganguli M. Dementia and cognitive impairment: epidemiology, diagnosis, and treatment. Clin Geriatr Med. 2014;30(3):421–442. doi:10.1016/j.cger.2014.04.001
9. Prince MJ, Wimo A, Guerchet MM, Ali GC, Wu Y-T, Prina M. World Alzheimer Report 2015 - the Global Impact of Dementia. London: Alzheimer’s Disease International; 2015.
10. Fisher RS, Acevedo C, Arzimanoglou A, et al. ILAE Official Report: a practical clinical definition of epilepsy. Epilepsia. 2014;55(4):475–482. doi:10.1111/epi.12550
11. McHugh JC, Delanty N. Epidemiology and classification of epilepsy: gender comparisons. Int Rev Neurobiol. 2008;83:11–26.
12. Neligan A, Hauser WA, Sander JW. The epidemiology of the epilepsies. Handb Clin Neurol. 2012;107:113–133.
13. Wu FJ, Sheu SY, Lin HC. Osteoporosis is associated with antiepileptic drugs: a population-based study. Epileptic Disord. 2014;16(3):333–342. doi:10.1684/epd.2014.0673
14. Raymont V, Salazar AM, Lipsky R, Goldman D, Tasick G, Grafman J. Correlates of posttraumatic epilepsy 35 years following combat brain injury. Neurology. 2010;75(3):224–229. doi:10.1212/WNL.0b013e3181e8e6d0
15. Fordington S, Manford M. A review of seizures and epilepsy following traumatic brain injury. J Neurol. 2020;267(10):3105–3111. doi:10.1007/s00415-020-09926-w
16. Yeh CC, Chen TL, Hu CJ, Chiu WT, Liao CC. Risk of epilepsy after traumatic brain injury: a retrospective population-based cohort study. J Neurol Neurosurg Psychiatry. 2013;84(4):441–445. doi:10.1136/jnnp-2012-302547
17. Scheffer IE, Berkovic S, Capovilla G, et al. ILAE classification of the epilepsies: position paper of the ILAE commission for classification and terminology. Epilepsia. 2017;58(4):512–521. doi:10.1111/epi.13709
18. Martorana A, Di Lorenzo F, Belli L, et al. Cerebrospinal fluid Aβ42 levels: when physiological become pathological state. CNS Neurosci Ther. 2015;21(12):921–925. doi:10.1111/cns.12476
19. Zelano J, Brigo F, Garcia-Patek S. Increased risk of epilepsy in patients registered in the Swedish Dementia Registry. Eur J Neurol. 2020;27(1):129–135. doi:10.1111/ene.14043
20. Schnier C, Duncan S, Wilkinson T, Mbizvo GK, Chin RFM. A nationwide, retrospective, data-linkage, cohort study of epilepsy and incident dementia. Neurology. 2020;95(12):e1686–e1693. doi:10.1212/WNL.0000000000010358
21. Quintas R, Alvarez AS, Koutsogeorgou E, et al. The relationship between health-related quality-of-life and disability in patients with controlled epilepsy: a cross-sectional observational study. Am J Phys Med Rehabil. 2012;91(13 Suppl 1):S31–38. doi:10.1097/PHM.0b013e31823d4db9
22. Thurman DJ, Faught E, Helmers S, Kim H, Kalilani L. New-onset lesional and nonlesional epilepsy in the US population: patient characteristics and patterns of antiepileptic drug use. Epilepsy Res. 2019;157:106210. doi:10.1016/j.eplepsyres.2019.106210
23. McKee AC, Daneshvar DH. The neuropathology of traumatic brain injury. Handb Clin Neurol. 2015;127:45–66.
24. Najem D, Rennie K, Ribecco-Lutkiewicz M, et al. Traumatic brain injury: classification, models, and markers. Biochem Cell Biol. 2018;96(4):391–406. doi:10.1139/bcb-2016-0160
25. Khellaf A, Khan DZ, Helmy A. Recent advances in traumatic brain injury. J Neurol. 2019;266(11):2878–2889. doi:10.1007/s00415-019-09541-4
26. Ladak AA, Enam SA, Ibrahim MT. A review of the molecular mechanisms of traumatic brain injury. World Neurosurg. 2019;131:126–132. doi:10.1016/j.wneu.2019.07.039
27. Peterson K, Veazie S, Bourne D, Anderson J. Association between traumatic brain injury and dementia in veterans: a rapid systematic review. J Head Trauma Rehabil. 2020;35(3):198–208. doi:10.1097/HTR.0000000000000549
28. Chu SF, Chiu WT, Lin HW, Chiang YH, Liou TH. Hazard ratio and repeat injury for dementia in patients with and without a history of traumatic brain injury: a population-based secondary data analysis in Taiwan. Asia Pac J Public Health. 2016;28(6):519–527. doi:10.1177/1010539516662956
29. LoBue C, Munro C, Schaffert J, et al. Traumatic brain injury and risk of long-term brain changes, accumulation of pathological markers, and developing dementia: a review. J Alzheimers Dis. 2019;70(3):629–654. doi:10.3233/JAD-190028
30. Graham NS, Sharp DJ. Understanding neurodegeneration after traumatic brain injury: from mechanisms to clinical trials in dementia. J Neurol Neurosurg Psychiatry. 2019;90(11):1221–1233. doi:10.1136/jnnp-2017-317557
31. Bray MJC, Richey LN, Bryant BR, et al. Traumatic brain injury alters neuropsychiatric symptomatology in all-cause dementia. Alzheimers Dement. 2021;17(4):686–691. doi:10.1002/alz.12225
32. Antonioni A, Raho EM, Di Lorenzo F. Is blood pTau a reliable indicator of the CSF status? A narrative review. Neurol Sci. 2023. doi:10.1007/s10072-023-07258-x
33. Plassman BL, Grafman J. Traumatic brain injury and late-life dementia. Handb Clin Neurol. 2015;128:711–722.
34. Jennett WB. Late epilepsy after blunt head injuries: a clinical study based on 282 cases of traumatic epilepsy. Ann R Coll Surg Engl. 1961;29(6):370–384.
35. Chung SD, Chen YK, Wu FJ, Lin HC. Hormone therapy for prostate cancer and the risk of stroke: a 5-year follow-up study. BJU Int. 2012;109(7):1001–1005. doi:10.1111/j.1464-410X.2011.10459.x
36. Kang JH, Keller JJ, Lin HC. Bisphosphonates reduced the risk of acute myocardial infarction: a 2-year follow-up study. Osteoporos Int. 2013;24(1):271–277. doi:10.1007/s00198-012-2213-5
37. Feigin VL, Vos T, Alahdab F, et al. Burden of neurological disorders across the us from 1990–2017: a global burden of disease study. JAMA Neurol. 2021;78(2):165–176. doi:10.1001/jamaneurol.2020.4152
38. Ophir K, Ran B, Felix B, Amir G. Ten year cumulative incidence of dementia after late onset epilepsy of unknown etiology. J Clin Neurosci. 2021;86:247–251. doi:10.1016/j.jocn.2021.01.030
39. Caramelli P, Castro LH. Dementia associated with epilepsy. Int Psychogeriatr. 2005;17(Suppl 1):S195–206. doi:10.1017/S1041610205002024
40. Hommet C, Mondon K, Camus V, De Toffol B, Constans T. Epilepsy and dementia in the elderly. Dement Geriatr Cognit Disord. 2008;25(4):293–300. doi:10.1159/000119103
41. Friedman D, Honig LS, Scarmeas N. Seizures and epilepsy in Alzheimer’s disease. CNS Neurosci Ther. 2012;18(4):285–294. doi:10.1111/j.1755-5949.2011.00251.x
42. Mendez MF. What is the relationship of traumatic brain injury to dementia? J Alzheimers Dis. 2017;57(3):667–681. doi:10.3233/JAD-161002
43. Little DM, Geary EK, Moynihan M, et al. Imaging chronic traumatic brain injury as a risk factor for neurodegeneration. Alzheimers Dement. 2014;10(3 Suppl):2.
44. Antonioni A, Raho EM, Lopriore P, et al. Frontotemporal dementia, where do we stand? A narrative review. Int J Mol Sci. 2023;24(14). doi:10.3390/ijms241411732
45. McKee AC, Robinson ME. Military-related traumatic brain injury and neurodegeneration. Alzheimers Dement. 2014;10(3 Suppl):S242–253. doi:10.1016/j.jalz.2014.04.003
46. Martin RC, Faught E, Richman J, et al. Psychiatric and neurologic risk factors for incident cases of new-onset epilepsy in older adults: data from U.S. Medicare beneficiaries. Epilepsia. 2014;55(7):1120–1127. doi:10.1111/epi.12649
47. Subota A, Pham T, Jetté N, Sauro K, Lorenzetti D, Holroyd-Leduc J. The association between dementia and epilepsy: a systematic review and meta-analysis. Epilepsia. 2017;58(6):962–972. doi:10.1111/epi.13744
48. Ishigaki S, Sugimoto A, Kawamura M. Epilepsy and dementia. Nihon Rinsho. 2014;72(5):926–930.
49. Chin RF, Neville BG, Scott RC. A systematic review of the epidemiology of status epilepticus. Eur J Neurol. 2004;11(12):800–810. doi:10.1111/j.1468-1331.2004.00943.x
50. Lu M, Faure M, Bergamasco A, et al. Epidemiology of status epilepticus in the United States: a systematic review. Epilepsy Behav. 2020;112:107459. doi:10.1016/j.yebeh.2020.107459
51. Costello DJ, Delanty N. Oxidative injury in epilepsy: potential for antioxidant therapy? Expert Rev Neurother. 2004;4(3):541–553. doi:10.1586/14737175.4.3.541
52. Aguiar CC, Almeida AB, Araújo PV, et al. Oxidative stress and epilepsy: literature review. Oxid Med Cell Longev. 2012;2012:795259. doi:10.1155/2012/795259
53. de Lores Arnaiz GR, Ordieres MG. Brain Na(+), K(+)-ATPase activity in aging and disease. Int J Biomed Sci. 2014;10(2):85–102. doi:10.59566/IJBS.2014.10085
54. Ishigaki S, Kawamura M, Ono K. Characteristics of geriatric epilepsy can include dementia. Brain Nerve. 2017;69(10):1125–1130. doi:10.11477/mf.1416200880
55. Sen A, Jette N, Husain M, Sander JW. Epilepsy in older people. Lancet. 2020;395(10225):735–748. doi:10.1016/S0140-6736(19)33064-8
56. Robertson J, Hatton C, Emerson E, Baines S. Prevalence of epilepsy among people with intellectual disabilities: a systematic review. Seizure. 2015;29:46–62. doi:10.1016/j.seizure.2015.03.016
57. Sen A, Capelli V, Husain M. Cognition and dementia in older patients with epilepsy. Brain. 2018;141(6):1592–1608. doi:10.1093/brain/awy022
58. Beghi E, Giussani G. Aging and the Epidemiology of Epilepsy. Neuroepidemiology. 2018;51(3–4):216–223. doi:10.1159/000493484
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.