")
Back to Journals » Infection and Drug Resistance » Volume 17
Incidence and Risk Factors of Active Tuberculosis Among Hospitalized Patients with Latent Tuberculosis Infection in China: A Cohort Study
Authors Liu Y, Zhang L, Chen Y, Ruan G , Liu Y, Chen S, Xie L, Wu F, Shi X, Liu X
Received 6 November 2023
Accepted for publication 5 March 2024
Published 11 March 2024 Volume 2024:17 Pages 953—960
DOI https://doi.org/10.2147/IDR.S447245
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Sandip Patil
Ye Liu,1,* Lifan Zhang,1– 4,* Yan Chen,1,* Guiren Ruan,1– 3 Yuchen Liu,1 Shi Chen,1 Lantian Xie,1 Fengying Wu,1 Xiaochun Shi,1– 3 Xiaoqing Liu1– 4
1Division of Infectious Diseases, Department of Internal Medicine, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China; 2State Key Laboratory of Complex Severe and Rare Disease, Peking Union Medical College Hospital, Beijing, People’s Republic of China; 3Center for Tuberculosis Research, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China; 4Clinical Epidemiology Unit, Peking Union Medical College, International Clinical Epidemiology Network, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaochun Shi; Xiaoqing Liu, Division of Infectious Diseases, Department of Internal Medicine, State Key Laboratory of Complex Severe and Rare Disease, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Shuaifuyuan No. 1, Beijing, 100005, People’s Republic of China, Email [email protected]; [email protected]
Background: The population with latent tuberculosis infection (LTBI) represents a potential pool of patients with active tuberculosis (ATB). T-SPOT.TB is an important test tool for screening LTBI. Owing to the large population of LTBI patients in China, it is necessary to identify a high-risk group for LTBI and enlarge tuberculosis preventive treatment (TPT) to reduce the incidence of ATB.
Methods: Hospitalized patients with positive T-SPOT.TB results were recruited from January 2013 to December 2016. Patients with ATB were excluded. Basic information was collected and the development of ATBs was examined during follow-up. The life-table method was used to calculate cumulative incidence rates. Potential risk factors were analyzed through Cox regression analysis.
Results: A total of 1680 patients with LTBI were recruited in the follow-up cohort, and 377 (22.44%) patients dropped out. With a median follow-up time of 81 months [interquartile range (IQR):61– 93], 19 of 1303 patients with LTBI developed ATB. The 1-year incidence of ATB was 614 per 100,000 individuals [95%confidence interval (95% CI):584– 644]. Over 5-year period, the cumulative incidence of ATB was 1496 per 100,000 [95% CI:1430– 1570], and the incidence density was 240 per 100,000 person-years[95% CI:144– 375]. In the Cox regression model, exposure of pulmonary tuberculosis (PTB) [adjusted hazard ratio (aHR)=10.557, 95% CI:2.273– 49.031], maximum daily dosage of glucocorticoids (GCs)≥ 50 mg/d (aHR=2.948, 95% CI:1.122– 7.748), leflunomide (LEF) treatment (aHR=8.572, 95% CI:2.222 − 33.070), anemia (aHR=2.565, 95% CI:1.015– 6.479) and T-SPOT.TB level≥ 300SFCs/106 PBMCs (aHR=4.195, 95% CI:1.365– 12.892) were independent risk factors for ATB development in LTBI patients.
Conclusion: The incidence of ATB is significantly higher in hospitalized patients with LTBI than in the general population. The exposure history of PTB, maximum daily dosage of GCs≥ 50 mg/day, LEF treatment, anemia, and T-SPOT.TB level≥ 300SFCs/106PBMCs, were the risk factors of tuberculosis reactivation. Hospitalized LTBI patients with the above factors may need TPT.
Keywords: latent tuberculosis infection, active tuberculosis, incidence, risk factors
Introduction
Tuberculosis (TB) is an important infectious disease caused by Mycobacterium tuberculosis (MTB) that threatens human health. The Global TB Report 2022 noted that 10.6 million new TB cases were diagnosed in 2021, increasing of 3.6% over the previous year. China is one of the 30 high-burden countries. The WHO Health Organization estimated that China has 780,000 new TB patients, with an incidence of 55 per 100,000 in 2021.1 The cumulative incidence of TB has reduced by only 11% from 2015 to 2021, far from the target of the Global End TB Strategy, which states that the incidence of TB should be reduced by 20% in 2020.2,3
Latent tuberculosis infection (LTBI) is defined as a persistent immune response to stimulation by MTB antigens without active tuberculosis (ATB). LTBI has a 5% to 10% lifetime risk of progressing to ATB, mostly within 5 years of the initial infection.4 There are two methods recommended by WHO for screening LTBI: tuberculin skin test (TST) and Interferon-γ release assays (IGRAs), including T-SPOT.TB.5 The prevalence was estimated to be 20.3%, with nearly 300 million cases in China.6 Selecting at-risk populations for LTBI management and carrying out preventive interventions among high-risk groups will significantly reduce the incidence of ATB.
A systematic review showed that the risk of ATB could be reduced by tuberculosis preventive treatment (TPT) from 70 to 90%.7 In 2015, the WHO Guidelines for the management of LTBI noted that the risk of ATB will increase in people exposed to pulmonary tuberculosis (PTB), people living with human immunodeficiency virus (HIV) infection, patients receiving dialysis, patients initiating anti-tumor necrosis factor (TNF) therapy, patients preparing for organ or hematologic transplantation, patients with silicosis, patients with diabetes, illicit drug users, health workers and students, immigrants from high TB burden countries, prisoners, homeless persons, patients with harmful alcohol use, smokers, and underweight people.5 However, the selection of at-risk populations for LTBI management should be adapted to the national epidemiology of TB and other local determinants. To date, there have been only a few studies on the clinical characteristics and related risk factors of ATB development in the LTBI population in China; one study was conducted in a rural general population, and the other in patients with rheumatic disease.8,9
This study was conducted on hospitalized patients with LTBI who tested positive for T-SPOT.TB results to investigate the incidence of ATB and to explore the risk factors for ATB development in this patient population, which would provide evidence for the stratified management of LTBI.
Methods
Participants
This cohort study was conducted at the Peking Union Medical College Hospital. All hospitalized patients with positive T-SPOT.TB results and those aged 18 years or older between January 2013 and December 2016 were recruited. Patients with ATB, HIV/AIDS, and expected survival of less than one year were excluded. (Figure 1)
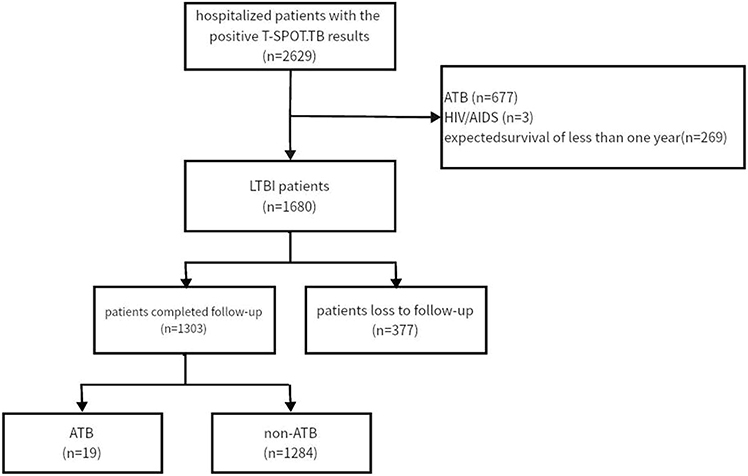 |
Figure 1 Study flow diagram of hospitalized patients with LTBI enrollment. |
The study was approved by the Ethics Committee of the Peking Union Medical College Hospital (S-K 2048).
T-SPOT.TB Test
T-SPOT.TB was tested by the T-SPOT®.TB kit (Oxford Immunotec Ltd, UK). Each well of the enzyme-linked immunosorbent spot assay plate precoated with interferon-γ was seeded with 2.5×105 peripheral blood mononuclear cells (PBMCs). AIM-V medium liquid, phytohemagglutinin (PHA), peptide antigens derived from Early secreting antigen target-6 (EAST-6), and Culture filtrate protein-10 (CFP-10) were added into the negative control, positive control, panel A and panel B, respectively and the plate was incubated at 5% CO2 and 37°C for 24h. If pane A or B had more than six spots and the spots were more than twice the negative control per well, the result was considered positive.
Procedures
Data were collected using a unified questionnaire between 2022 and 2023.
Baseline information was collected in detail, including (1) demographic information incorporated sex and age; (2) comorbidities incorporated rheumatic disease, diabetes, chronic kidney disease (CKD), inflammatory bowel disease (IBD), and malignancy); (3) use of medications included glucocorticoids (GCs) and immunosuppressant agents (ISAs) (such as cyclophosphamide (CTX), methotrexate (MTX), mycophenolate (MMF), azathioprine (AZA), leflunomide (LEF), cyclosporine (CsA), tacrolimus (FK506)), and biologics (TNF-αinhibitors); (4) history of chemoradiotherapy;(5) history of tuberculosis and the exposure history of PTB;(6) laboratory results incorporated routine blood tests and T-SPOT.TB results.
Follow-up information was obtained via questionnaire as directly as possible, but if patients cannot get to the hospital, it is acceptable to phone them. The follow-up evaluation included diagnosis of ATB (including diagnosis date, site, and diagnostic basis) and anti-tuberculosis medication. The history of PTB exposure, emerging comorbidities, and medication use were also collected during the follow-up period. If a patient was suspected or confirmed to have ATB, the relevant medical records must be reviewed and discussed by an expert panel before confirmation.
Diagnosis Criteria of ATB
The diagnosis of ATB was based on the Chinese diagnostic criteria for tuberculosis (WS 288—2017) and classification of tuberculosis (WS 196-2017).10,11 Briefly, the diagnosis criteria of ATB were as follows: (1) any of the bacteriological evidence: including acid-fast bacillus microscopy, culture, GeneXpert MTB/RIF assay, and tuberculosis nucleic acid determination. (2) histological evidence: pathological changes of the tissue specimens show histological evidence of caseous necrosis and epithelioid granulomas. (3) Clinically diagnosed ATB cases were based on clinical manifestations, laboratory findings compatible with ATB, and effective response to anti-tuberculosis treatment. Meanwhile, other analogous diseases were excluded.
Statistical Analysis
All statistical results were obtained using SPSS25 (IBM Corp., SPSS Inc., NY, USA) software. The median and interquartile range [IQR] were used to describe continuous variables following a non-normal distribution, and the rank-sum test was used for comparisons between groups. Categorical variables were described as frequency and percentage, and the Fisher’s exact test was used for comparisons between groups. The life table method was used to calculate the cumulative incidence and the corresponding confidence intervals. A Cox proportional hazards regression model was used to analyze the risk factors for ATB development in the population after the proportional assumption satisfied. Variables significantly related to ATB infection in the univariate Cox regression analysis (P<0.05) were included in the multivariate COX regression analysis. P<0.05 was considered statistically significant.
Results
General Characteristics
A total of 1680 eligible patients were recruited in the study, of which 377 were lost to follow-up, with a dropout rate of 22.4%. Baseline data of patients lost and who responded to treatment are shown in Supplementary Table 1. Until the end of observation, 19 out of 1303 LTBI patients who completed follow-up developed ATB (Figure 1). The baseline information is shown in Table 1 and Figure 2.
 |
Table 1 General Characteristics of 1303 Enrolled Patients |
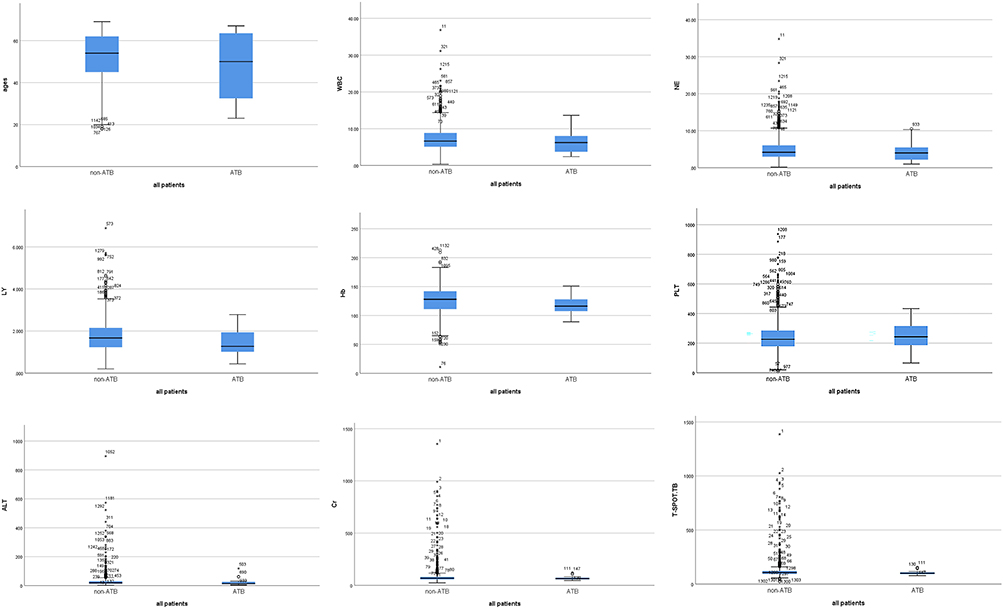 |
Figure 2 The box plots of variables in all enrolled patients (n=1303). Abbreviations: WBC, White Blood Cell; NE, Neutrophil; LY, Lymphocyte; Hb, Hemoglobin; PLT, Platelet count; ALT, alanine aminotransferase; Cr, Creatinine. |
ATB Incidence in LTBI Patients
During the median follow-up period of 81 months [IQR:61–93], 19 patients developed ATB among 1303 LTBI patients. Among the 19 ATB cases, 9 (47.37%) cases were confirmed by microbiology, 1 (5.26%) case was confirmed by histopathology, and the remaining 9 (47.37%) cases were clinically diagnosed. Among the 9 cases with microbiologic diagnosis, 4 cases and 2 cases were only positive for acid-fast staining and MTB nucleic acid detection, respectively. 2 cases were positive for both acid-fast staining and culture and 1case was positive for both acid-fast staining and MTB nucleic acid detection. According to the disease site, 12 cases (63.16%) had lung involvement, including 10 cases of PTB and two cases of PTB combined with tuberculous meningitis. The others were two cases of osteoarticular TB one case of urogenital TB, one case of tuberculous meningitis, 1case of intestinal TB, and two cases diagnosed with effective anti-TB therapy who presented with fever of unknown origin.
The 1-year incidence of ATB in this cohort was 614 per 100,000 [95% confidence interval (95% CI):584–644], and the 5-year cumulative incidence of ATB was 1496 per 100,000 (95% CI:1430–1570) (Table 2). The incidence density of ATB in patients with LTBI was 240 per 100,000 person-years (95% CI:144–375).
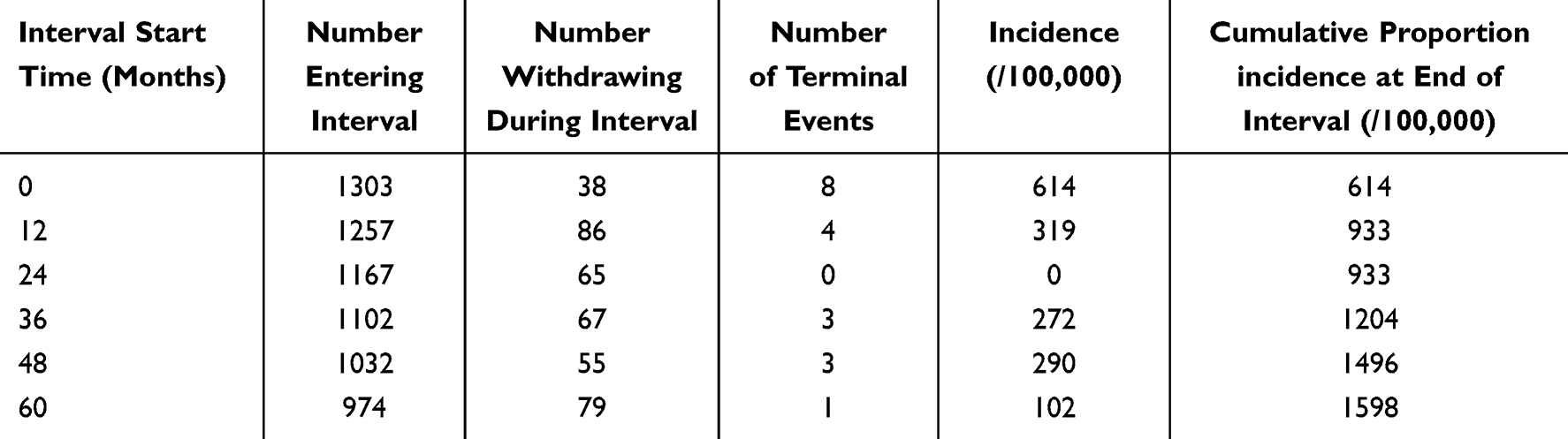 |
Table 2 Incidence of ATB in LTBI Patients |
Risk Factors for ATB in LTBI Patients
The risk factors for ATB in the 1303 enrolled patients with LTBI were analyzed. Univariate Cox regression analysis was conducted on sex, age, comorbidities, maximum daily dosage of GCs, use of ISAs, use of TNF-α inhibitors, chemoradiotherapy, and laboratory results, including white blood cell (WBC) count, hemoglobin (Hb), platelet count (PLT), alanine aminotransferase (ALT), albumin (ALB), total bilirubin (TBIL), creatinine (Cr), and T-SPOT.TB (Supplementary Table 2). The results of the multivariate Cox regression analysis are shown in Table 3. Exposure to PTB [adjusted hazard ratio (aHR)= 10.557, 95% CI:2.273–49.031], maximum daily dosage of GCs ≥ 50 mg/d (aHR= 2.948, 95% CI:1.122–7.748), LEF treatment (aHR= 8.572, 95% CI:2.222–33.070), anemia (aHR= 2.565, 95% CI:1.015–6.479) and T-SPOT.TB level ≥300 SFCs/106PBMCs (aHR= 4.195, 95% CI: 1.365–12.892) were independent risk factors for ATB development in LTBI patients.
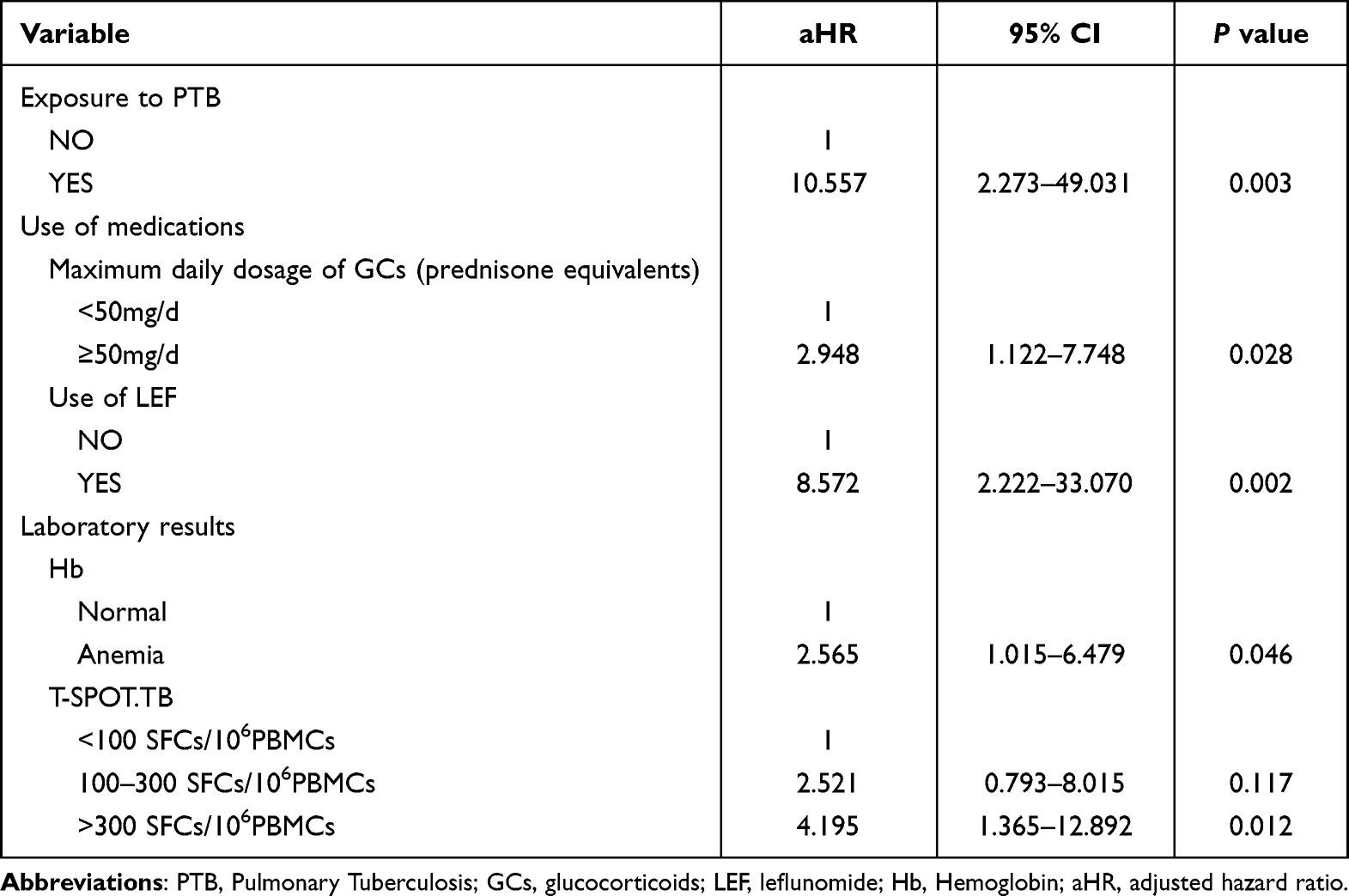 |
Table 3 Multivariable COX Regression Analysis of ATB in Cohort |
Discussion
According to the 2022 Global Tuberculosis Report, the incidence of ATB in China was 55 per 100,000 in China.1 We reported an ATB incidence of 614 per 100,000 in patients with LTBI at 1 year, which was 11-fold higher than that in the general population. Therefore, patients with LTBI are a high-risk population for ATB, which is consistent with some previous studies. A systematic review assessed the absolute risk of ATB among untreated populations with a positive tuberculin skin test (TST) or IGRA results and found that the incidence of ATB among patients with a TST induration of ≥10 mm was 30 per 100,000 person-years (95% CI 10–110), significantly higher than that in the local general population (5.3 per 100,000 in Canada; 2.6 per 100,000 in the USA). The incidence of ATB in LTBI patients was also higher than that in TST/IGRA negative patients among different high-risk patient groups (incidence rate ratios 1.7–48.1).12 Another cohort study on rheumatic disease showed that 5.16% of patients with positive IGRA results, but only 0.35% of patients with negative IGRA results developed ATB (P <0.05).8
In our study, history of PTB exposure was an independent risk factor for ATB (aHR= 10.557). Previous studies have reached similar conclusion.13,14 Patients with LTBI had an increased risk of ATB within the first two years after exposed, about 15-fold.15 Patients with LTBI with an exposure history of PTB may have an increased risk of ATB and should receive sufficient attention in clinical practice. In this study, none of the 30 patients who underwent TPT developed ATB and none of the 19 ATB patients received TPT.
Several medications, such as GCs, ISAs, and TNF-α inhibitors, may affect specific immune responses to MTB, thereby increasing the risk of ATB development. In our study, a maximum daily dosage of GCs ≥ 50 mg/day (aHR= 2.948) and LEF treatment (aHR= 8.572) were risk factors for ATB development in patients with LTBI.
Owing to their anti-inflammatory and immunosuppressive actions, GCs have been widely used to treat inflammatory diseases. However, it is worth noting that long-term exposure to GCs may lead to serious complications such as an increased risk of ATB. The underlying mechanism may disturb macrophage function and inhibit cellular immunity.16,17 In patients with SLE, a maximum daily dose of GCs ≥ 30 mg/day is an independent risk factor for ATB development.18 Another prospective cohort study also found that a high dosage of GCs (>15 mg daily) for > 4 weeks was an independent risk factor for ATB.8 Studies have confirmed that GCs increase the risk of ATB development in patients with LTBI, and patients with high and medium doses are at a higher risk than those with low doses.14 Moreover, one study showed that a low dose of GCs (< 10 mg/day) did not increase the risk of MTB reactivation.19 We found that in patients with LTBI, the maximum daily dosage of GCs ≥ 50 mg/day, but not a history of GCs use, significantly increased the risk of developing ATB (approximately 3-fold). These findings may be valuable in the management of TPT.
ISAs are widely used for the treatment of immune-associated diseases. The overwhelming variety of ISAs, mechanisms of action, and immunosuppression intensity complicate the effect of ISAs on MTB reactivation. LEF, MTX, CsA, and AZA are presumed to be associated with ATB development. This study showed that LEF was associated with a nearly 8-fold risk of MTB reactivation. A review showed that RA patients using LEF had a 4 to 11 times risk of ATB development.20 The proposed mechanisms are possibly mediated via the suppression of T lymphocyte and B lymphocyte activation and inhibition of the TNF-α signaling pathway.21,22 LEF significantly increases the risk of MTB reactivation, leading to a call for systematic screening in these populations to allow the timely initiation of TPT.
TNF-α inhibitor treatment is similarly associated with an increased risk of tuberculosis infection, and a consensus has emerged that screening and treatment for LTBI are essential before starting TNF-α inhibitor therapy. However, this study found no significant correlation between TNF-α inhibitor treatment and ATB development. This difference may be due to the small sample size; only 35 patients (2.7%) were treated with TNF-α inhibitors in our study. Of the 35 patients, only 12 completed TPT and none developed ATB; one of the 23 patients without TPT developed ATB during follow-up.
One study found that the level of Hb was significantly lower in the ATB group than in the LTBI group.23 Hb is a proxy for nutritional status and condition. Malnutrition is a recognized risk factor for ATB. A genomic study found significantly increased expression of RISK4 and PREDICT29 progression signatures in malnourished individuals with LTBI, consistent with the known association between inflammatory pathway activation and progression to ATB.24 The increase in serum iron levels in individuals with anemia of chronic disease provides a favorable environment for MTB.25 We found that anemia was a significant risk factor for ATB development (aHR= 2.565).
Although the IGRA test cannot distinguish ATB from LTBI, IGRA levels can indirectly reflect the load of MTB in non-immunocompromised populations indirectly.26,27 Higher IGRA levels in the LTBI population suggest a higher risk of developing ATB. A systematic review and meta-regression quantified the dose-response relationship between interferon-gamma levels and the risk of progression to ATB, they found that compared to 0 IU/mL, the relative risk of progression to ATB among those with IFN-γ levels of 5 IU/mL was 11.38 (95% CI 6.64–16.38).28 Our study found that patients with LTBI underwent the T-SPOT.TB≥ 300 SFC/106PBMCs are at increased risk of developing ATB. T-SPOT.TB level stratification will help identify patients with LTBI at a high risk of developing ATB.
This study has several limitations. First, it was a single-center study conducted at a large 3A grade hospital in China. In addition, the recruited subjects were hospitalized patients with severe diseases, which may have overestimated the incidence of ATB in the LTBI population owing to a selection bias. Second, the study used T-SPOT.TB to screen LTBI without TST for the BCG vaccine is generally inoculated in our country. Thus, some LTBI patients may be missed. Third, the dropout rate at the follow-up was 22.44%. We found no significant difference in the general characteristics between patients with follow-up and dropout; thus, dropout was unlikely to have affected our results. Finally, owing to the small number of outcome events, the estimated incidences had wide confidence intervals, which would require further verification.
Conclusions
In summary, the incidence was significantly higher in patients with LTBI than in the general population. These factors (history of PTB exposure, maximum daily dosage of GCs, LEF treatment, and levels of Hb and T-SPOT.TB) should be considered when evaluating the risk of LTBI patients developing ATB. Thus, LTBI patients with an exposure history of PTB, maximum daily dosage of GCs ≥ 50 mg/day, LEF treatment, anemia, or T-SPOT.TB levels ≥ 300 SFCs/106PBMCs may be considered for TPT.
Ethical Approval
The study involving human participants was reviewed and approved by the Ethics Committee of PUMCH (K-S 2048). The study conducted a retrospective analysis of hospitalized patients records, without patient samples obtained and without intervention during the diagnosis and treatment of patients. All clinical data of the recruited patients were anonymous. Therefore, the ethics committee agreed that all patients were exempt from informed consent. The study was conducted in accordance with the Helsinki principles.
Funding
This study was supported by National High Level Hospital Clinical Research Funding (2022-PUMCH-C-013 and 2022-PUMCH-A-043).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Bagcchi S. WHO’s Global Tuberculosis Report 2022. Lancet Microbe. 2023;4(1):e20. doi:10.1016/S2666-5247(22)00359-7
2. World Health organization. Implementing the end TB strategy: the essentials, 2022 update. World Health Organization; 2022. Available from: https://www.who.int/publications/i/item/9789240065093.
3. World Health organization. The end TB strategy. World Health organization; 2015. Available from: https://www.who.int/publications/i/item/WHO-HTM-TB-2015.19.
4. Comstock GW, Livesay VT, Woolpert SF. The prognosis of a positive tuberculin reaction in childhood and adolescence. Am J Epidemiol. 1974;99(2):131–138. doi:10.1093/oxfordjournals.aje.a121593
5. World Health organization. Guidelines on the Management of Latent Tuberculosis Infection. World Health organization; 2015. Available from: https://www.who.int/publications/i/item/9789241548908.
6. Gao L, Zhang H. Expert consensus on the estimation of the national burden on latent tuberculosis infection. Chin J Antituberculosis. 2022;44(1):4–8. doi:10.19982/j.issn.1000-6621.20210662
7. Getahun H, Matteelli A, Chaisson RE, et al. Latent Mycobacterium tuberculosis infection. N Engl J Med. 2015;372(22):2127–2135. doi:10.1056/NEJMra1405427
8. Long W, Cai F, Wang X, et al. High risk of activation of latent tuberculosis infection in rheumatic disease patients. Infect Dis. 2020;52(2):80–86. doi:10.1080/23744235.2019.1682187
9. Gao L, Li X, Liu J, et al. Incidence of active tuberculosis in individuals with latent tuberculosis infection in rural China: follow-up results of a population-based, multicentre, prospective cohort study. Lancet Infect Dis. 2017;17(10):1053–1061. doi:10.1016/S1473-3099(17)30402-4
10. People’s Republic of China state health and Family Planning Commission. Diagnostic criteria for tuberculosis (WS 288—2017). Electr J Emerg Infect Dis. 2018;3(01):59–61. doi:10.19871/j.cnki.xfcrbzz.2018.01.017
11. People’s Republic of China state health and Family Planning Commission. Tuberculosis classification (WS196—2017). Electr J Emerg Infect Dis. 2018;3(3):191–192. doi:10.19871/j.cnki.xfcrbzz.2018.03.018
12. Campbell JR, Winters N, Menzies D. Absolute risk of tuberculosis among untreated populations with a positive tuberculin skin test or interferon-gamma release assay result: systematic review and meta-analysis. BMJ. 2020;368:m549. doi:10.1136/bmj.m549
13. Shah M, Dorman SE, Solomon CG. Latent Tuberculosis Infection. N Engl J Med. 2021;385(24):2271–2280. doi:10.1056/NEJMcp2108501
14. Ai JW, Ruan QL, Liu QH, et al. Updates on the risk factors for latent tuberculosis reactivation and their managements. Emerg Microbes Infect. 2016;5(2):e10. doi:10.1038/emi.2016.10
15. Landry J, Menzies D. Preventive chemotherapy. Where has it got us? Where to go next? Int J Tuberc Lung Dis. 2008;12(12):1352–1364.
16. Cain DW, Cidlowski JA. Immune regulation by glucocorticoids. Nat Rev Immunol. 2017;17(4):233–247. doi:10.1038/nri.2017.1
17. Xie Y, Xie J, Meijer AH, et al. Glucocorticoid-Induced Exacerbation of Mycobacterial Infection Is Associated with a Reduced Phagocytic Capacity of Macrophages. Front Immunol. 2021;12:618569. doi:10.3389/fimmu.2021.618569
18. Zhang L, Zou X, Jiang N, et al. Incidence and risk factors of tuberculosis in systemic lupus erythematosus patients: a multi-center prospective cohort study. Front Immunol. 2023;14:1157157. doi:10.3389/fimmu.2023.1157157
19. Brode SK, Jamieson FB, Ng R, et al. Increased risk of mycobacterial infections associated with anti-rheumatic medications. Thorax. 2015;70(7):677–682. doi:10.1136/thoraxjnl-2014-206470
20. Cantini F, Niccoli L, Capone A, et al. Risk of tuberculosis reactivation associated with traditional disease modifying anti-rheumatic drugs and non-anti-tumor necrosis factor biologics in patients with rheumatic disorders and suggestion for clinical practice. Expert Opin Drug Saf. 2019;18(5):415–425. doi:10.1080/14740338.2019.1612872
21. Breedveld F, Dayer J. Leflunomide: mode of action in the treatment of rheumatoid arthritis. Ann Rheum Dis. 2000;59(11):841–849. doi:10.1136/ard.59.11.841
22. Miceli-Richard C, Dougados M. Leflunomide for the treatment of rheumatoid arthritis. Expert Opin Pharmacother. 2003;4(6):987–997. doi:10.1517/14656566.4.6.987
23. Kang Y-J, Park H, Park S-B, et al. Combined analysis of whole blood interferon gamma release assay and complete blood count analysis for rapid discrimination of active tuberculosis and latent tuberculosis infection. J Clin Tuberc Other Mycobact Dis. 2021;24:100253. doi:10.1016/j.jctube.2021.100253
24. VanValkenburg A, Kaipilyawar V, Sarkar S, et al. Malnutrition leads to increased inflammation and expression of tuberculosis risk signatures in recently exposed household contacts of pulmonary tuberculosis. Front Immunol. 2022;13:1011166. doi:10.3389/fimmu.2022.1011166
25. Lee SW, Kang YA, Yoon YS, et al. The prevalence and evolution of anemia associated with tuberculosis. J Korean Med Sci. 2006;21(6):1028–1032. doi:10.3346/jkms.2006.21.6.1028
26. Kang WL, Wang GR, Wu MY, et al. Interferon-gamma release assay is not appropriate for the diagnosis of active tuberculosis in high-burden tuberculosis settings: a retrospective multicenter investigation. Chin Med J. 2018;131(3):268–275. doi:10.4103/0366-6999.223860
27. Herrmann JL, Belloy M, Porcher R, et al. Temporal dynamics of interferon gamma responses in children evaluated for tuberculosis. PLoS One. 2009;4(1):e4130. doi:10.1371/journal.pone.0004130
28. Ledesma JR, Ma J, Zheng P, et al. Interferon-gamma release assay levels and risk of progression to active tuberculosis: a systematic review and dose-response meta-regression analysis. BMC Infect Dis. 2021;21(1):467. doi:10.1186/s12879-021-06141-4
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.