")
Back to Journals » Journal of Healthcare Leadership » Volume 15
Important Leadership Skills and Benefits of Shared Leadership Training for Chief Residents: A Delphi Analysis
Authors Levy KL , Sheffield V, Sturza J, Heidemann LA
Received 23 March 2023
Accepted for publication 4 September 2023
Published 19 September 2023 Volume 2023:15 Pages 221—230
DOI https://doi.org/10.2147/JHL.S413799
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Russell Taichman
Kathryn L Levy,1,2 Virginia Sheffield,1 Julie Sturza,2 Lauren A Heidemann1
1Department of Internal Medicine, University of Michigan, Ann Arbor, MI, USA; 2Department of Pediatrics, University of Michigan, Ann Arbor, MI, USA
Correspondence: Kathryn L Levy, Internal Medicine and Pediatrics Department, University of Michigan, 1500 East Medical Center Drive, Ann Arbor, MI, 48109, USA, Tel +1 585 732 0597, Email [email protected]
Background: Chief residents (CRs) have pivotal educational and leadership roles in residency programs. The necessary CR leadership skills that transcend specialties have not been defined and most training on these skills occurs in silo.
Objective: The primary goal was to define leadership skills important for the general CR role. The secondary aim was to determine which skills should be included in cross-specialty CR training and identify benefits of such training.
Methods: Sixty-three CRs and 25 program directors (PDs) from 25 residency programs at a single institution were surveyed via a modified Delphi approach in 2022 as part of a needs assessment on CR leadership training. First, respondents answered three open-ended questions about skills needed for the CR role and the potential benefits of cross-specialty CR training. Respondents then rated categorized responses on the importance of the skill, agreement that skills should be included in cross-specialty training, and agreement on benefit of cross-specialty training using a 5-point Likert scale. Positive consensus was defined as 80% agreement.
Results: Fifty respondents (53%) participated in round one and 28 (32%) in round two. Positive consensus was reached on 38 skills (63%). Nine skills reached consensus on inclusion in cross-specialty training including communication skills and certain management skills. Consensus on benefits of training include learning from and collaborating with other residency programs.
Conclusion: The authors defined important skills for the CR role that reached consensus across a broad range of specialties and identified the perceived benefits of shared leadership training. Residency programs should consider cross-specialty leadership training for CRs with a focus on communication and management skills.
Keywords: chief residents, leadership skills, leadership training, cross-specialty training
Introduction
The Chief Resident (CR) position has long been recognized as an important role in graduate medical education (GME) and is critical to the success of residency programs.1 The specifics of the role for an individual residency program or specialty may differ, but many aspects of the role are similar across programs. CRs hold a unique “middle manager” position2 where they promote the residency program’s vision, respond to program and departmental leadership, educate and mentor junior residents and students, and serve as assessors and coaches of residents in the program.1,3–7 CRs are also often involved in administrative tasks such as schedule-building and coordination of educational conferences or other program activities.8,9 Through many of these responsibilities, they interact with CRs from different departments. While existing literature describes current CR training practices, there is no literature to our knowledge that focuses on both CR and program director (PD) input as to what topics are most valuable to include in modern training, and sparse information about which skills have universal importance for CRs across specialties.10–12
Targeted CR leadership training courses exist both at institutional and national levels,13–24 however, many are siloed within specialties or departments, with few crossing departmental lines.13–15,17,20,22,24 In one study, chief residents from a shared geographic region who participated in shared leadership training identified developing an active community of practice as a major advantage of shared training.13 The COVID19 pandemic has further highlighted the importance of interprofessional collaboration for responding to crises big and small. The rapidly changing challenges of healthcare from global pandemics, artificial intelligence, shift to virtual care and virtual recruitment, and financial constraints within healthcare demand skillful and dynamic leadership which can be accomplished best through collaboration and diverse teams.25
Driven by the recognition of the importance of providing leadership training for CRs and cross-specialty collaboration, we organize shared leadership trainings for CRs from all specialties at our institution. As part of our needs assessment as we expanded and deepened this curriculum, we sought to study CR leadership skills and benefits of cross-specialty training for CRs. The primary goal of our study was to define the key leadership skills necessary for success in the role of CR regardless of specialty. Secondarily, we aimed to define which of these skills should be included in cross-specialty CR training, and the potential benefits of cross-specialty training opportunities. Ultimately, we aimed to provide a practical list of skills that could be taught through shared leadership training at any institution.
Methods
Setting and Study Participants
We invited all CRs (n = 63) and PDs (n = 25) from the 25 Accreditation Council for Graduate Medical Education (ACGME) accredited residency training programs with designated CRs at our Midwest academic institution to participate in a survey-based Delphi study in the spring of 2022. This study was embedded in a larger needs assessment at our institution about leadership training for CRs and readiness for their role. We recruited participants via email invitations from one author (KL) and GME leadership. Targeted follow-up emails were sent to specialties not initially represented in responses. All current CRs and PDs were invited to participate given their broad and varied specialty backgrounds and either their personal experience in the chief resident role (CRs and some PDs) and/or experience overseeing residency training and specifically their chief residents (PDs). Individuals from all specialties were invited to gain a comprehensive insight into the CR role. Our goal was to obtain at least 20 responses, because a panel of 15 to 30 participants is recommended to effectively perform the Delphi technique.26 A $15 gift card incentive was offered to CRs who completed both rounds of surveys.
Delphi Study
We used a modified Delphi approach26 consisting of two sequential anonymous surveys designed to define consensus. The round 1 survey captured free-text responses to the questions outlined below. These responses were then analyzed and consolidated. The round 2 survey questions asked participants to rate responses which were then analyzed for consensus.
The surveys were created in Qualtrics (Qualtrics LLC, Provo, UT). This electronic survey software allows for easy distribution over email with an anonymous link for accessing and for capture of both multiple choice and free-text responses.
Round 1 Survey Questions
CRs were asked the following questions:
- What leadership skills are important for the chief resident role? (List as many as you can think of)
- What are potential benefits to YOU INDIVIDUALLY of participating in leadership training with chief residents from different specialties? (List as many as you can think of)
- What are broader potential benefits of chief residents participating in leadership training with chief residents from different specialties? (ie beyond those you listed in individual benefits above)
PDs were asked the same three questions with this slightly different wordings of question two: What are potential benefits to the INDIVIDUAL chief residents of participating in leadership training with chief residents from different specialties? (List as many as you can think of).
Round 1 survey ended with giving participants the option to opt in to Round 2 by entering their information in a separate unlinked survey.
Review of Round 1 Responses
Three of the authors (KL, VS, LH) independently reviewed the free-text responses and consolidated them. This consolidation consisted of reviewing the responses and grouping similar responses together into categories. For some, it was similar words such as “approachability” and “being approachable” which were grouped together under “approachability”. For others, it was taking longer statements and grouping them together under one category. An example of this would be “ability to recognize and maintain confidentiality” or “able to handle sensitive resident issues discretely” fell into the category of “integrity”. We reviewed the categorized responses as a group, discussed differences or responses that were hard to interpret and came to a joint agreement on the consolidation of the response. We then collectively identified key themes and grouped the categorized responses under those themes. Vague responses that were overly broad or difficult to interpret were excluded.
Of note, we elected to ask about benefits in two different ways via questions 2 and 3 to increase the type and depth of responses. As expected, there was substantial overlap in answers across these 2 questions. The answers to these two questions were consolidated into one list for review and categorizing prior to round 2.
Round 2 Survey Questions
Respondents from round 1 who elected to participate in round 2 were then given a second survey about the categorized responses. First, respondents were asked to rate how important each skill was for the CR role on a 5-point Likert scale (1-not at all important, 2-slightly important, 3-moderately important, 4-important, 5-very important). Next, respondents were shown the list of the potential benefits of shared leadership training and asked to rate how strongly they agreed with the statement “this is a benefit of shared leadership training with chief residents from different specialties” on a 5-point Likert scale of agreement (1-strongly disagree, 2-disagree, 3-neither agree nor disagree, 4-agree, 5-strongly agree). For the skills, respondents were asked to rate how strongly they agreed with the statement “this topic should be included in chief resident leadership training with chiefs from different specialties” on a 5-point Likert scale of agreement (1-strongly disagree, 2-disagree, 3-neither agree nor disagree, 4-agree, 5-strongly agree). The latter question was included to guide in the creation of shared leadership training for CRs.
Statistical Analysis
Univariate statistics were used to determine both the mean and standard deviation of the Likert scale responses as well as the percent agreement for each item. The study was not powered to detect differences in CR vs PD responses. All analyses were completed using SAS 9.4 (SAS Institute, Cary, NC).
Defining Consensus
Agreement was defined as positive or negative. Positive agreement was defined as the majority of respondents choosing either a 4 or 5 on the Likert scale. Negative agreement was defined as the majority of respondents choosing “1-not at all important” for question one. For questions two and three, negative agreement meant that the majority chose either “1-strongly disagree” or “2-disagree”. High consensus was defined as 80% agreement among the respondents, approaching consensus was defined as 51% to 79% agreement, and no consensus was defined as 50% or less agreement.
The study was determined to be exempt by the University of Michigan Institutional Review Board (HUM00210501) since it is research involving surveys in which any disclosure of responses would not place subjects at risk.
Results
Demographic Information
In round one, 50 physicians participated (response rate 53%) including 35 CRs (56%) and 15 PDs (60%). Forty-three of the round one participants (32 CRs and 11 PDs) opted to participate in Round 2. Response rate of round two was 56% of those who elected to participate during round one (22 CRs and 6 PDs). This represents 35% of the CR population and 24% of the PD population initially invited to participate. Further demographic information is included in Figure 1.
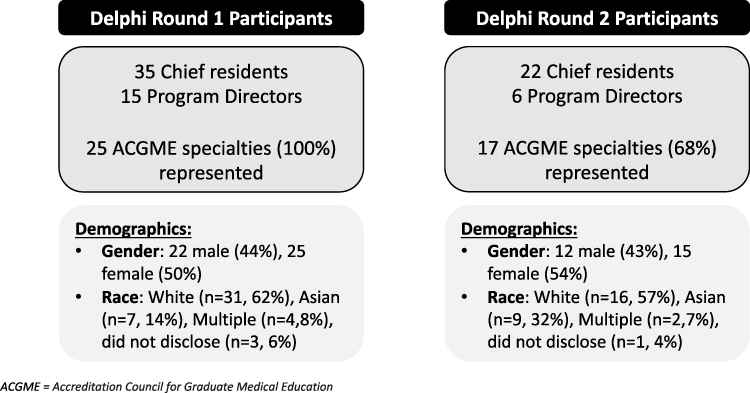 |
Figure 1 Participant overview and demographics. |
Delphi Survey Round One
Categorization of free-text responses identified 60 leadership skills in six distinct categories. Thirty-five benefits of shared training were cited and were categorized into five distinct categories. Twelve free-text responses (11 skills and 1 benefit) were excluded.
Delphi Survey Round Two
Regarding the importance of leadership skills, positive consensus was reached on 38 skills (63%, Table 1). Seventeen skills (28%) approached consensus and five (8%) did not reach consensus (Table 2). No skills achieved negative consensus. The most important skills (mean + SD) were cited as organization (4.9 + 0.4), professionalism (4.9 + 0.4), integrity (4.9 + 0.4), and teamwork (4.8 + 0.4).
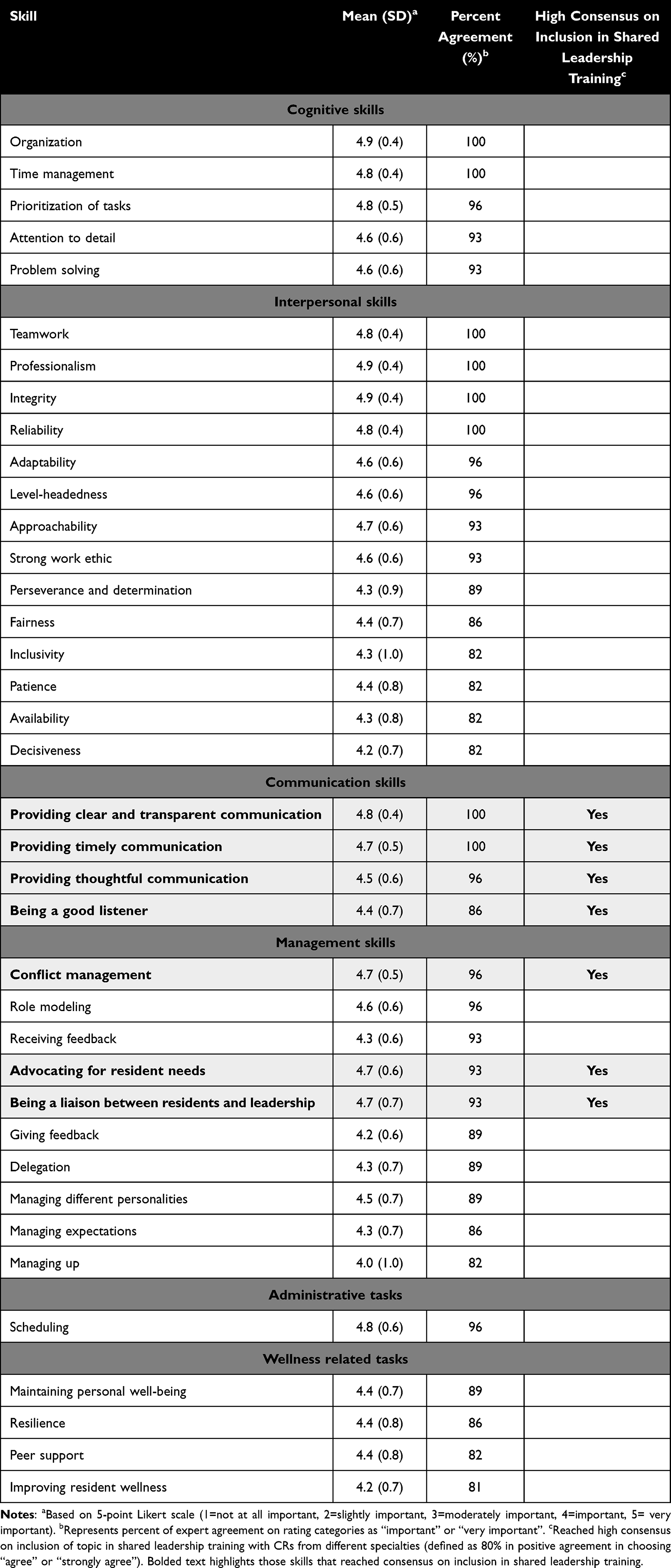 |
Table 1 High Consensus Regarding Important or Very Important Skills for the Chief Resident Role, N = 38 |
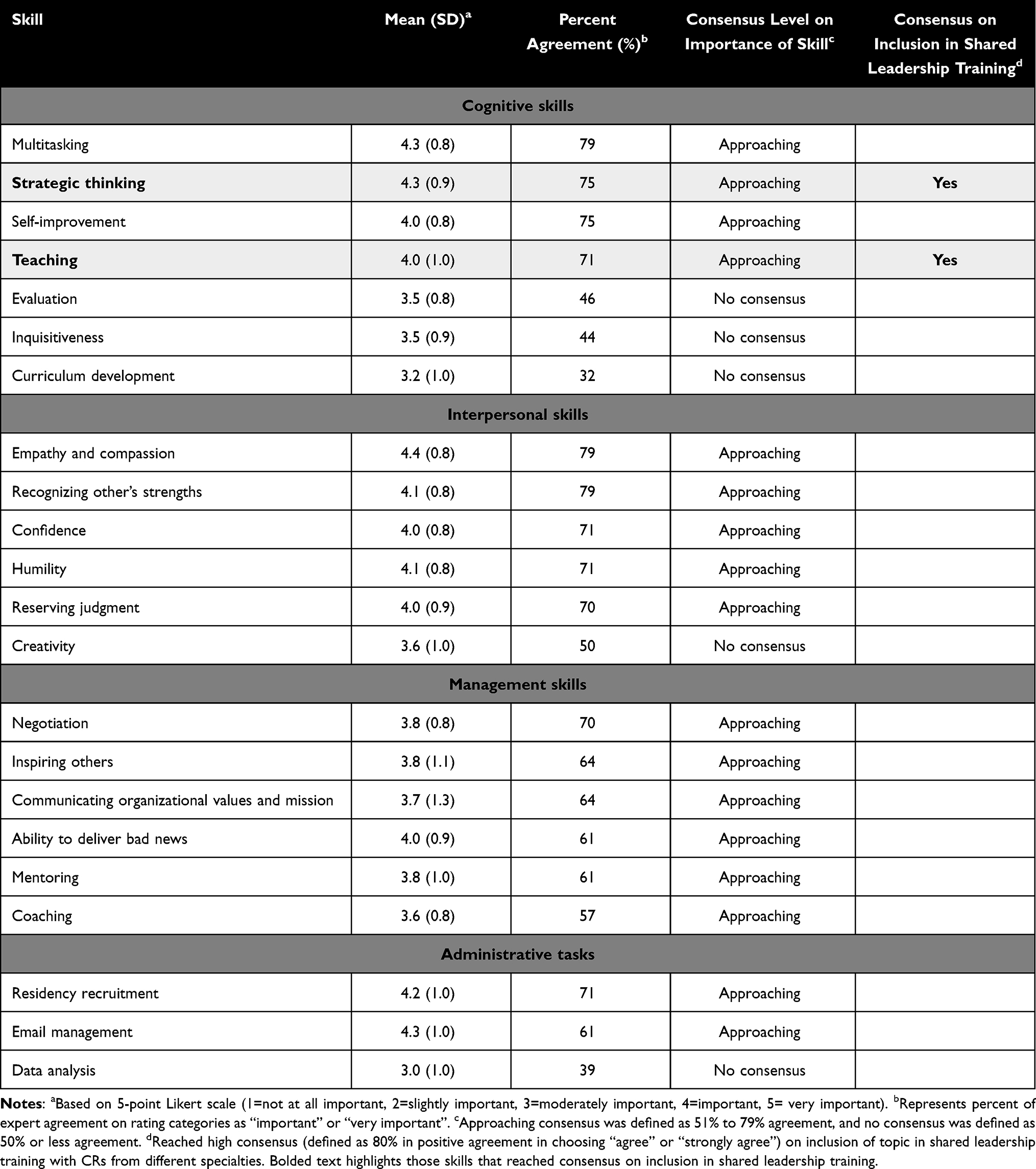 |
Table 2 Approaching Consensus or No Consensus Regarding Important Skills for the Chief Resident Role, N = 22 |
Benefits of shared leadership training achieved positive consensus in six areas (17%), approached consensus in 28 areas (80%) and did not reach consensus in one area (3%) (Table 3). No benefits achieved negative consensus.
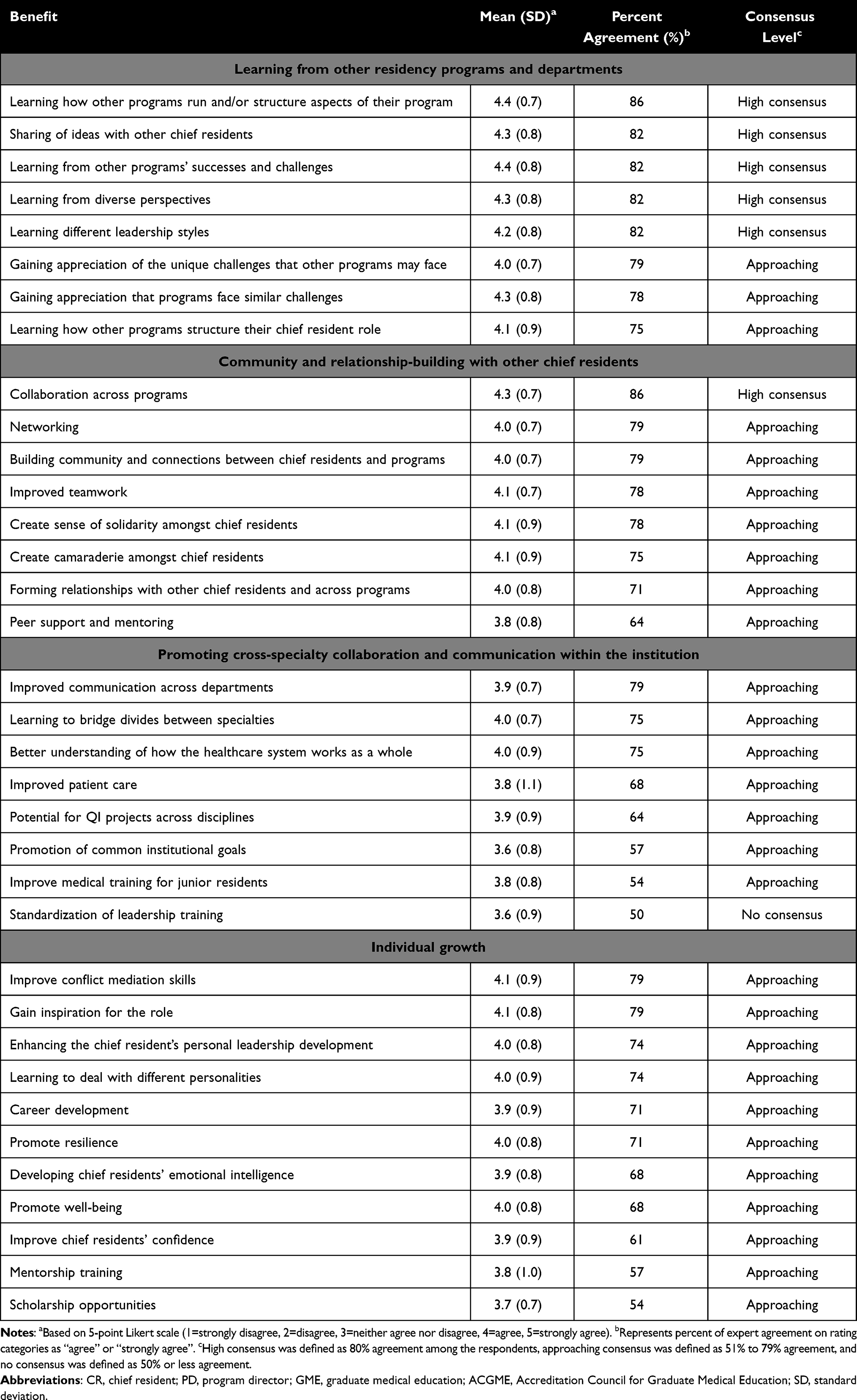 |
Table 3 Consensus on Benefits of Shared Leadership Training with CRs from Different Specialties, N = 35 |
Regarding whether a skill should be included in shared leadership training, positive consensus was reached on nine skills (15%) including communication skills and certain management skills (Table 1 and Table 2). Forty-two skills (70%) approached consensus and nine (15%) did not reach consensus (Table 1 and Table 2). No skills achieved negative consensus.
Discussion
In this study, we defined the common leadership skills deemed important for the CR role at our institution across a broad range of specialties using a Delphi approach. The perceived key benefits from shared leadership training with CRs from different departments included learning from and collaborating with CRs from other residency programs. Topics that met high consensus to include in cross-specialty CR leadership training were communication skills, certain management skills, teaching, and strategic thinking.
Our study adds to the current literature by revealing which topics are valuable to include in CR training from the perspective of both CRs and PDs. Many skills that met inclusion for CR training in our study are included in the curricula of other published CR training programs, however some skills are not explicitly mentioned. For example, existing CR training programs include conflict resolution and tools for effective communication,13–16,24 however there is no overt mention of certain management skills such as advocating for resident needs and serving as an effective liaison between residents and program leadership. These latter skills are crucial to the CR role as “middle manager”2 and may be worthwhile to explicitly address in CR training. Other GME leadership training programs include topics, such as time management and delegation,24 that our respondents agreed are important skills however did not feel should be included in CR training. It is possible that these skills are felt to be less “teachable” than other skills or that CRs may already possess such skills given that these are attributes that are generally considered for CR selection.12
Notably, the main area of perceived benefit of shared leadership training was learning from and collaborating with other residency programs and departments. We speculate that CRs desire to learn new approaches to common problems they are asked to address. Likewise, there are ample opportunities for collaboration to enhance education, quality improvement, and/or research endeavors. For example, at our own institution collaboration between CRs through encounters in shared leadership training led to programs sharing policies around supporting lactating mothers and influencing the institutional policy around social media accounts. From a practical standpoint, we urge current CR training programs to consider incorporating CRs from other programs into a shared training experience. This may also be beneficial in that it is less resource- and labor-intensive than numerous individual trainings for each specialty’s CRs and allows programs to leverage expertise and knowledge from leaders in different specialties.
Our study has several limitations. This is a single-center study which limits generalizability. Response rate was moderate leading to potential selection bias. The survey participants included a small number of PDs compared to CRs, therefore differences between the two were not able to be assessed, and there was attrition between the first and second Delphi rounds. We did not examine differences across specialties, so it is possible that certain skills or benefits are not applicable to all specialties. Lastly, it is important to note that our surveys were distributed in the spring of 2022 and the ongoing COVID-19 pandemic which may have influenced responses to this survey. Future directions in this area would be to quantify the benefits of shared leadership training more tangibly, for example tracking interdepartmental educational, quality improvement, or research interventions. It would also be helpful to objectively evaluate CRs’ skills or overall leadership abilities over time which may help inform areas of future training.
Conclusions
CRs from all specialties hold a unique leadership position within GME and share a common skillset that requires specialized training. Based on our needs assessment, we recommend that training programs incorporate sessions dedicated to conflict management, effective communication techniques, as well as “middle manager” skills such as strategies for how to advocate for resident needs and serve as a liaison between residents. We recommend consideration of shared CR training programs across specialties as this may enhance learning, relationship-building, and cross-departmental collaboration.
Acknowledgments
The authors would like to thank Dr. Sybil Biermann, DIO, and the GME office for their support of this work and leadership training for our chief residents and Dr. Sarah Hartley for her mentorship in the early phases of this work.
Disclosure
Lauren A Heidemann receives an honorarium for being a participant on a Transition to Residency Editorial board which is sponsored by the non-profit Macy Faculty Scholars Program as well as the non-profit Zell Family Foundation. Lauren Heidemann receives institutional grant funding from the University of Michigan Graduate Medical Education Innovations fund to research cross-cover medicine. Neither disclosure is related to this work. The other authors have no disclosures to report for this work.
References
1. Grant I, Dorus W, McGlashan T, Perry S, Sherman R. The Chief Resident in Psychiatry. Arch Gen Psychiatry. 1974;30(4):503–507. doi:10.1001/archpsyc.1974.01760100069011
2. Berg DN, Huot SJ. Middle Manager Role of the Chief Medical Resident: an Organizational Psychologist’s Perspective. J Gen Intern Med. 2007;22(12):1771–1774. doi:10.1007/s11606-007-0425-8
3. Anderson ML, Hartley SE, Huang GC. Essential Mediators of the Competency Process: chief Residents as Assessors and Coaches. J Grad Med Educ. 2020;12(4):394–398. doi:10.4300/JGME-D-19-00801.1
4. Young MA, Stiens SA, Hsu P. Chief residency in PM&R. A balance of education and administration. Am J Phys Med Rehabil. 1996;75(4):257–262. doi:10.1097/00002060-199607000-00003
5. Lim RF, Schwartz E, Servis M, Cox PD, Lai A, Hales RE. The Chief Resident in Psychiatry: roles and Responsibilities. Acad Psychiatry. 2009;33(1):56–59. doi:10.1176/appi.ap.33.1.56
6. Hafner JW, Gardner JC, Boston WS, Aldag JC. The Chief Resident Role in Emergency Medicine Residency Programs. West J Emerg Med. 2010;11(2):120–125.
7. Nelson CS, Brown IE, Rao TK. A study of the responsibilities of chief residents in anesthesiology with a suggested job description. Anesthesiol Rev. 1994;21(6):199–202.
8. Wortmann RL, Costrini NV, Adams ND. The chief medical residency: a description and recommendations. J Med Educ. 1982;57(4):288–293. doi:10.1097/00001888-198204000-00003
9. Dabrow SM, Harris EJ, Maldonado LA, Gereige RS. Two Perspectives on the Educational and Administrative Roles of the Pediatric Chief Resident. J Grad Med Educ. 2011;3(1):17–20. doi:10.4300/JGME-D-10-00039.1
10. VanOrder T, Wisniewski SJ. Chief Resident Skills: a Study on Resident Perceptions of Skill Importance and Confidence. Spartan Med Res J. 2018;3(1):6466. doi:10.51894/001c.6466
11. Saxena A, Garg A, Desanghere L. Common pitfalls in the chief resident role: impact on effective leadership practices. Int J Leadership Educ. 2015;18(3):386–393. doi:10.1080/13603124.2014.962102
12. Turner J, Litzau M, Mugele J, Pettit K, Sarmiento EJ, Humbert A. Qualities Important in the Selection of Chief Residents. Cureus. 2020;12(4):e7580. doi:10.7759/cureus.7580
13. Luciano G, Blanchard R, Hinchey K. Building chief residents’ leadership skills. Med Edu. 2013;47(5):524. doi:10.1111/medu.12194
14. Farver CF, Smalling S, Stoller JK. Developing leadership competencies among medical trainees: five-year experience at the Cleveland Clinic with a chief residents’ training course. Australas Psychiatry. 2016;24(5):499–505. doi:10.1177/1039856216632396
15. Mustafa S, Stoller JK, Bierer SB, Farver CF. Effectiveness of a Leadership Development Course for Chief Residents: a Longitudinal Evaluation. J Grad Med Educ. 2020;12(2):193–202. doi:10.4300/JGME-D-19-00542.1
16. Doughty RA, Williams PD, Brigham TP, Seashore C. Experiential Leadership Training for Pediatric Chief Residents: impact on Individuals and Organizations. J Grad Med Educ. 2010;2(2):300–305. doi:10.4300/JGME-02-02-30
17. Frich JC, Brewster AL, Cherlin EJ, Bradley EH. Leadership development programs for physicians: a systematic review. J Gen Intern Med. 2015;30(5):656–674. doi:10.1007/s11606-014-3141-1
18. Deane K, Ringdahl E. The family medicine chief resident: a national survey of leadership development. Fam Med. 2012;44(2):117–120.
19. Gisondi MA, Bavishi A, Burns J, Adler MD, Wayne DB, Goldstein JL. Use of a Chief Resident Retreat to Develop Key Leadership Skills. MedSciEduc. 2017;27(2):173–176. doi:10.1007/s40670-017-0381-9
20. Pettit JE, Wilson MC. Leadership certificate program for chief residents. Med Educ Dev. 2014;4(1). doi:10.4081/med.2014.5089
21. American Academy of Family Physicians. Chief Resident Leadership Development Program. Available from: https://www.aafp.org/students-residents/residency-program-directors/chief-resident-leadership-development-program.html.
22. University at Buffalo. Chief Resident Leadership Conference. Available from: https://medicine.buffalo.edu/offices/gme/residents/educational-activities/leadership-conference.html.
23. Bandstra BS, Katz M, Huang RW. A Curriculum to Address Issues and Challenges of the Professional Developmental Stage of Chief Residency. Acad Psychiatry. 2013;37(1):18–22. doi:10.1176/appi.ap.10080123
24. Sadowski B, Cantrell S, Barelski A, O’Malley PG, Hartzell JD. Leadership Training in Graduate Medical Education: a Systematic Review. J Grad Med Educ. 2018;10(2):134–148. doi:10.4300/JGME-D-17-00194.1
25. Page S. The Diversity Bonus: How Great Teams Pay off in the Knowledge Economy. Princeton University Press; 2017.
26. de Villiers MR, de Villiers PJT, Kent AP. The Delphi technique in health sciences education research. Med Teach. 2005;27(7):639–643. doi:10.1080/13611260500069947
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.