")
Back to Journals » Journal of Healthcare Leadership » Volume 16
Implementing Clinical Guidelines for the Treatment of Psychosis: The Frontline Leaders’ Point of View. A Qualitative Study
Authors Nordin HMA , Mathisen GE, Rørtveit K, Joa I, Johannessen JO, Ruud T, Hartveit M
Received 6 October 2023
Accepted for publication 24 January 2024
Published 29 February 2024 Volume 2024:16 Pages 93—104
DOI https://doi.org/10.2147/JHL.S430285
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pavani Rangachari
Håkan MA Nordin,1,2 Gro Ellen Mathisen,3 Kristine Rørtveit,1,2 Inge Joa,1,4 Jan O Johannessen,1,4 Torleif Ruud,5,6 Miriam Hartveit7,8
1Department of Psychiatry, Stavanger University Hospital, Stavanger, Norway; 2Department of Caring and Ethics, University of Stavanger, Stavanger, Norway; 3Norwegian School of Hotel Management, University of Stavanger, Stavanger, Norway; 4Department of Public Health, University of Stavanger, Stavanger, Norway; 5Division of Mental Health Services, Akershus University Hospital, Lørenskog, Norway; 6Institute of Clinical Medicine, University of Oslo, Oslo, Norway; 7Department for Research and Innovation, Helse Fonna Health Trust, Valen, Norway; 8Department of Global Public Health and Primary Care, University of Bergen, Bergen, Norway
Correspondence: Kristine Rørtveit
University of Stavanger, Faculty of Health Sciences, Postbox 8600, Stavanger, 4036, Norway
, Tel +4790521114
, Email [email protected]; [email protected]
Background: Despite the large amount of leadership and implementation theories and recommendations, healthcare services continue to struggle with efficiently incorporating new knowledge. The questioning of conventional leadership approaches in healthcare organizations prompted us to investigate how frontline leaders comprehend their own implementation intentions and actions, and how these intentions and actions may impact the implementation of clinical guidelines in mental healthcare in Norway.
Methods: Employing a theory-driven qualitative design, we conducted nine semi-structured interviews with frontline leaders who had recently led implementation of clinical guidelines for the treatment of psychosis in mental health. We employed Systematic Text Condensation, informed by Normalization Process Theory, to structure and analyze the data and used fidelity scales to measure the degree of implementation and distinguish between leaders’ levels of success in implementation.
Results: Frontline leaders in units that achieved high success in implementation described their intentions and actions differently, from those with less success. The former group’s actions aligned more closely with the constructs of the Normalization Process Theory compared to the latter group when describing their actions. Frontline leaders leading units with a high degree of implementation success describe relation-orientation, trust, and providing adaptive space for staff members to take initiative. In contrast, those leading units with less implementation success describe more control and guidance of co-operators and place more emphasize on information and knowledge.
Conclusion: Differences in how frontline leaders describe their actions and intentions to achieve clinical guideline implementation suggest that the leadership approach of these frontline leaders is an important factor to consider when planning and conducting implementation. To better understand the implementation process, it is important to pay attention to how frontline leaders customize their leadership approaches to the dynamics of complex organizations, and how they interact with their team and superiors.
Plain Language Summary: Despite the large amount of available implementation theories and recommendations, healthcare services continue to struggle with efficiently incorporating new and better practice. The clinicians’ closest leader, the Frontline leader, is considered to be in a unique position to manage and enable implementation in the complex healthcare system. The current study’s aim was to improve our understanding of what these leaders do, and how they operate, to enable the implementation of clinical guidelines. We interviewed nine mental health service leaders in Norway with experience of leading implementation of clinical guideline during the last 3 years. We found a variety of leaders’ intentions and actions regarding their involvement in the process and how they relate to their staff and superiors. Frontline leaders that lead units with high degree of implementation success described actions according to all four constructs of the Normalization Process Theory (Coherence, Cognitive participation, Collective action and Reflexive monitoring), while frontline leaders with less implementation success had more fragmented descriptions. Successful leaders appear to be more relation-oriented compared to those in less successful units. This suggests that leaders should focus on inter-personal dynamics, in addition to more concrete implementation interventions, to succeed.
We recommend to take the leadership actions and intentions identified in this study into consideration when planning and evaluating implementation projects and leadership programs, as well as when recruiting frontline leaders.
Keywords: complexity leadership theory, frontline leaders’ implementation of clinical guidelines, normalization process theory, implementation fidelity
Introduction
Healthcare is commonly characterized as a Complex Adaptive System (CAS) recognized by a large set of interacting interdependent actors at the same or different organization levels or other organizations, which foster dynamic processes and complex working processes.1,2 CAS evolves over time and in response to different stakeholders, system inputs and local contexts, highlighting an unpredictability when trying to implement new practices.3 This constant evolution and instability may hinder standardization of working processes as intended by quality improvement and the translation of research findings into clinical practice.4,5 On the other hand, the complexity and instability of the system can present opportunities for innovation and the implementation of new practices in healthcare. Therefore, we should embrace complexity, and engage and empower individuals and teams to constantly improve healthcare.6
Due to their organizational first in line position, managing and supervising clinicians, frontline leaders (FLs) are often recognized as being in a unique position to manage complex systems when implementing new knowledge into clinical practice.7–9
Leadership in Complex Adaptive Systems
Traditional leadership strategies, which include change management, are not well suited for CAS.10,11 In a previous study exploring leadership strategies, we identified a broad range of leadership approaches that are currently used in implementation contexts, transcending traditional leadership strategies.12 In light of CAS, leaders should embrace uncertainty, maintain a minimum of specifications, and adopt a constructive approach to variation.13 Complexity Leadership Theory (CLT), which focuses on leaders promoting learning, creativity, and adaptively within the CAS organization, is highlighted by Uhl-Bien and Arena.14,15 The CLT framework describes operational leadership as formal leadership for executing orders, entrepreneurial leadership as the source of new ideas, innovation, learning and growth for the organization and enabling leadership as promoting conditions that effectively support and sustain adaptive space.14 Enabling leadership interacting with operational and entrepreneurial leadership approaches helps organizations to function as complex adaptive systems.10,14
Frameworks for Implementation in Complex Organizations
The Normalization Process Theory (NPT) describes the implementation of new practices in complex organizations through actions and the inter-subjectivity between agents.16 In accordance with the Context-Mechanism-Outcome (CMO) configuration,17,18 May et al18 defined four constructs inherent the theory of NPT as generative mechanisms: Coherence, which assigns meaning and to make sense of interventions; Cognitive participation, which justifies and engages in interventions; Collective action, which assembles competency and resources to carry out interventions; and Reflexive monitoring, which evaluates the effects of the interventions and potentially restructures organization and social relations. The NPT theory defines these mechanisms as “a process that brings about or prevents some change in a concrete system”.18
Evidence-based clinical guidelines are broadly recognized as a tool, to improve care and treatment outcome,19 and contain healthcare costs and, not at least, reducing variation in clinical practice.20 Guidelines are an important tool helping leaders and providers to make complex healthcare decisions.21
Despite the existence of numerous implementation theories and recommendations on how to lead such processes, healthcare services still struggle to adopt new knowledge rapidly enough.7,22 The questioning of traditional leadership approaches in healthcare organizations, and particularly the operationalization of these theoretical constructs into actions among FL, lead us to explore how FL comprehends their own implementation intentions and actions, and how these intentions and actions may influence implementation of clinical treatment guidelines in mental healthcare in Norway. Knowledge about how FL perceive their own intentions and action in implementation processes can help customize measures of planning implementation projects.
Materials and Methods
Study Design
Employing a theory-driven qualitative design, we conducted interviews with a sample of frontline leaders (FL) who had experiences with implementing clinical guidelines in specialized mental healthcare settings during the last three years. The Context-Mechanism-Outcome (CMO) model, as outlined by May et al,18 was employed to investigate the FL’s perceived actions and intentions through the four mechanisms of Normalization Process Theory (NPT) and how they related to their employees and immediate superior (context), leading to varying degrees of implementation success (outcome). Systematic Text Condensation (STC)23 was used to analyze the interviews. NPT18 was employed as a framework for structuring the results of the analyses and for highlighting the intersubjective elements of the implementation processes. To differentiate between varying degrees of implementation success among FLs, we used validated fidelity scales.24 Additionally, socio-demographic data were collected through a survey completed by each FL.
Context
The present study was undertaken as a part of the Norwegian implementation study entitled “A pairwise randomized study on implementation of guidelines and evidence based treatments of psychosis”.25 The study included 39 mental health clinics from six healthcare trusts and was conducted between 2016 and 2019. The participating units were given the option to choose from four evidence-based practices for psychosis treatment to be implemented. Clinicians and leaders from the attending units were offered training and workshops regarding the practice, measurement, and feedback on implementation outcomes, which were structured and regularly supported by trained facilitators, and access to a toolkit available on a website.
Sample
Purposive sampling was utilized to recruit FLs from nine out of the 39 clinics. All clinics provide specialized psychiatric services to adults with psychosis, at three geographically spread locations in Norway, both rural and urban. Recruitment was finished when the sample was considered to have sufficient information power, ensuring specificity and relevance.26,27
With few exceptions, the clinical units were fully staffed with interdisciplinary teams including nurses, doctors, psychologists, and social workers throughout the implementation project.
The sample consisted of six women and three men, representing the nine clinics. Six FLs were experienced nurses and three had other professions. Four FLs were between the ages of 41 and 50; three were between 51 and 60; one was over 60 and one was under 40. In terms of leadership experiences, two had more than ten years, four had nine years and three had seven years of experience. Seven FLs had experience from leadership improvement programs. Support from colleagues was the most common reported source of support, and some had additional support from mentors.
According to Norwegian legislation, leaders in healthcare have comprehensive responsibility for their unit and the interdisciplinary team.28
Ethical Approval
The study was approved by the hospitals’ Data Protection Officer and the south-east Norwegian Regional Ethics Committee (REK no 2015/2169). All data were anonymized and stored on a secure research server.
Each participant was provided with written and verbal information about the present study and signed an informed consent, including the publication of anonymized responses, prior to the interview.
Data Sharing Statement
Anonymized transcripts, in Norwegian, can be provided, on reasonable request, from the corresponding author for one year after publication.
Data collection
Socio-Demographic Data
The participants completed a demographic questionnaire providing information on their gender, age, profession, years of leadership experience, type of unit they managed, any education or systematic leadership training they had received, and access to leadership support. Owing to the small sample size and confidentiality concerns, profession is not individually reported for the participants.
Semi-Structured Interviews
Semi-structured individual face-to-face interviews were conducted between December 2018 and March 2019 at a location chosen by the participant. The interviews were conducted by the first author with only the interviewee present and lasted between 50 and 100 minutes. All interviews were recorded and transcribed verbatim.
The interview guide was developed by the research group based on experience, research, literature, and input from an informal group of six experienced FL in mental health services by using Nominal Group Technique.29 The guide consisted of open-ended questions designed according to phenomenological theory,30 piloted twice and covering three topics, example questions included:
- General experience as a leader from the implementation project.
What are your experiences as a leader with this particular project?
- Experience and impression from the process.
How would you describe the process for the current implementation, based on your point of view as a leader?
- Relationship to close and important co-operators.
Describe your relationship with your immediate superior and subordinates based on your role as a leader?
Each interview concluded with a question about any remaining topic to cover. The guide was prepared with prompts to deepen the answers, if necessary.
Measured Level of Implementation Success by Fidelity Score
Measures developed for measuring fidelity to the evidence-based practices in treatments for psychoses were employed, providing data on whether a clinical team or program had embedded the key components of a specific evidence-based model.24 Psychometric properties for the four fidelity scales are reported elsewhere.31–34
Each unit achieved an average implementation score between 1 and 5. In the present study, scores 4.0 or higher indicated high fidelity, scores between 3.0 and 3.9 indicated moderate fidelity and scores 2.9 or lesser indicated low fidelity. The scoring definitions were based on McHugo et al.35
Analyses
Systematic Text Condensation (STC) was conducted in the following steps: First, transcripts were thoroughly read and reread by HN, MH, GEM and KR, and a total impression was formed, and preliminary themes were identified for each participant. Next, to ensure consistency of coding and reliability throughout the coding process, emerging preliminary meaning units that were considered relevant to the study’s purpose were coded into operationalized code groups by HN supported by the three other researchers. Then, the content of the meaning units for each FL and each code group are condensed into subgroups and reduced to condensates. Further, the condensates for each FL were interpreted in accordance with the NPT construct model, and finally, the condensates inherent each NPT construct were cross-case synthesized for each group of fidelity level.
Meaning units that deviated from the NPT model but were considered relevant to the purpose of the study, such as relations with the immediate superior and their own staff, were noted for each participant and analyzed for each fidelity group according to the steps of the STC model. The synthesized results of leader actions, intentions and relations for each fidelity group are the unit of analysis for describing the leaders’ expressed leadership approach in the implementation process.
Results
FL reported a diverse range of intentions and actions that they deemed relevant for implementing new practices. Through the process of synthesizing condensates according to NPT constructs within the three fidelity groups, a variation of salient implementation leadership actions and intentions were identified. FL in units with high fidelity scores exhibited more relation-orientation, trust and provided for adaptive space for staff member initiative, while being less controlling compared to those with moderate and low fidelity scores.
In the following, we will describe the results pertaining to the NPT mechanisms for high, moderate, and low fidelity levels, respectively. We will further elaborate on how the FL describes their intentions and actions, and how they interacted and related to their staff and their immediate superior through illustrative quotes.
Description of the Sample According to Level of Fidelity
As shown in Table 1, three of the FL were leaders at a unit that achieved a high fidelity score, four leaders achieved a moderate fidelity, and two leaders achieved a low fidelity. Furthermore, the high implementation success group differs from the other two groups regarding the choice of intervention practice and the number of leaders having experience from leadership training programs.
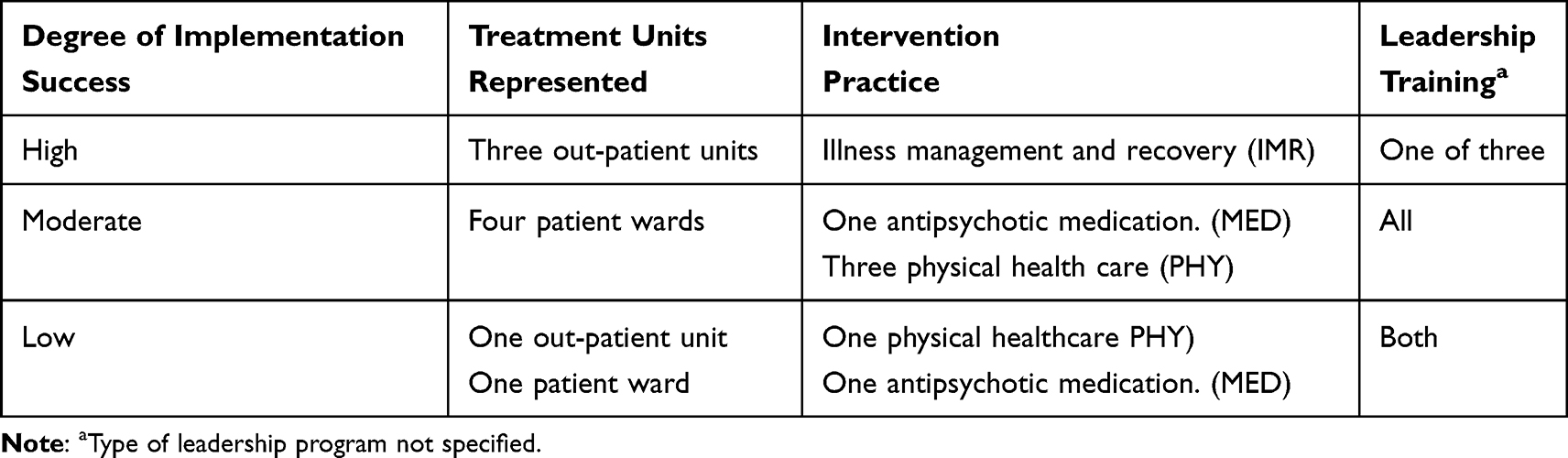 |
Table 1 Implementation Success Measured by Fidelity Level Score, Distributed Across Treatment Unit, Clinical Practice and Experience from Leadership Development Programs |
FLs’ intentions and actions
The result for the three fidelity level groups is presented for each group separately, with text and a summing-up table, illustrating leaders intentions and actions across the four steps of the NPT construct model, respectively (Tables 2–4). Finally, Table 5 summarizes the synthetized leadership approaches for FL of each fidelity level group across leadership features, NPT constructs’, relations to immediate superior and own staff.
The High Fidelity Level Group
FL in units that achieved high level of implementation described actions and intention that indicated reflexivity, taking time and efforts to understand individual staff members’ positions, reactions, and questions in the implementation process. This approach showed potential for preventing conflicts and resistance. FL1:
I have reflected on it beforehand. Tried to understand it. Uhm, understand their starting point. What is it that makes the resistance so strong? What makes them feel personally attacked? What can be done to avoid triggering it?
They expressed a generally positive attitude to new ideas and innovations, which they aimed to instill in the clinicians. In order to motivate staff, they chose to focus on the advantages of the new practice for the staff, patients, and department. FL2:
So, it’s a bit about that attitude towards it. What can be made of it? It’s kind of the core of what I think makes my job interesting. How can you put this to good use? Instead of in a way being hesitant and thinking that this is unsafe.
These leaders emphasized the importance of having competent and engaged employees and reflected on their efforts to build individual identity, improve competence, and foster talent among their cooperators.
They also placed a strong emphasis on strategic recruitment of dedicated implementation team members and change agent(s), seeing it as an opportunity for personal development for their employees. FL3:
I actually feel like an amateur in [the clinical practice to be implemented] compared to her. She’s the one who knows this (…) I see her artistic creativity together with the professional, then she has really blossomed.
FL participated in the implementation group for evaluation of the process. They were conscious regarding their role as a leader. FL1:
I am not involved in the management of that group, but I participate in the start-up and evaluation to see how we can provide good conditions for those who will run it, in relation to everything else that needs to happen. And look at everything from such organizational things as time off, etc., to others who will participate and how to solve it. So now I actually own it as a leader.
These leaders also described actions to foster an appropriate relationship with their immediate superiors. The relationships were characterized by mutual respect and trust. In cases where different priorities caused obstacles, they engaged in discussions and negotiations to reach an agreement. They emphasized the importance of maintaining a respectful, open, direct and constructive dialogue, and being flexible rather than rigid in their approach. Table 2 illustrates a rich protocol for the high fidelity level group interpreted according to the four constructs of NPT. This group considered all four constructs.
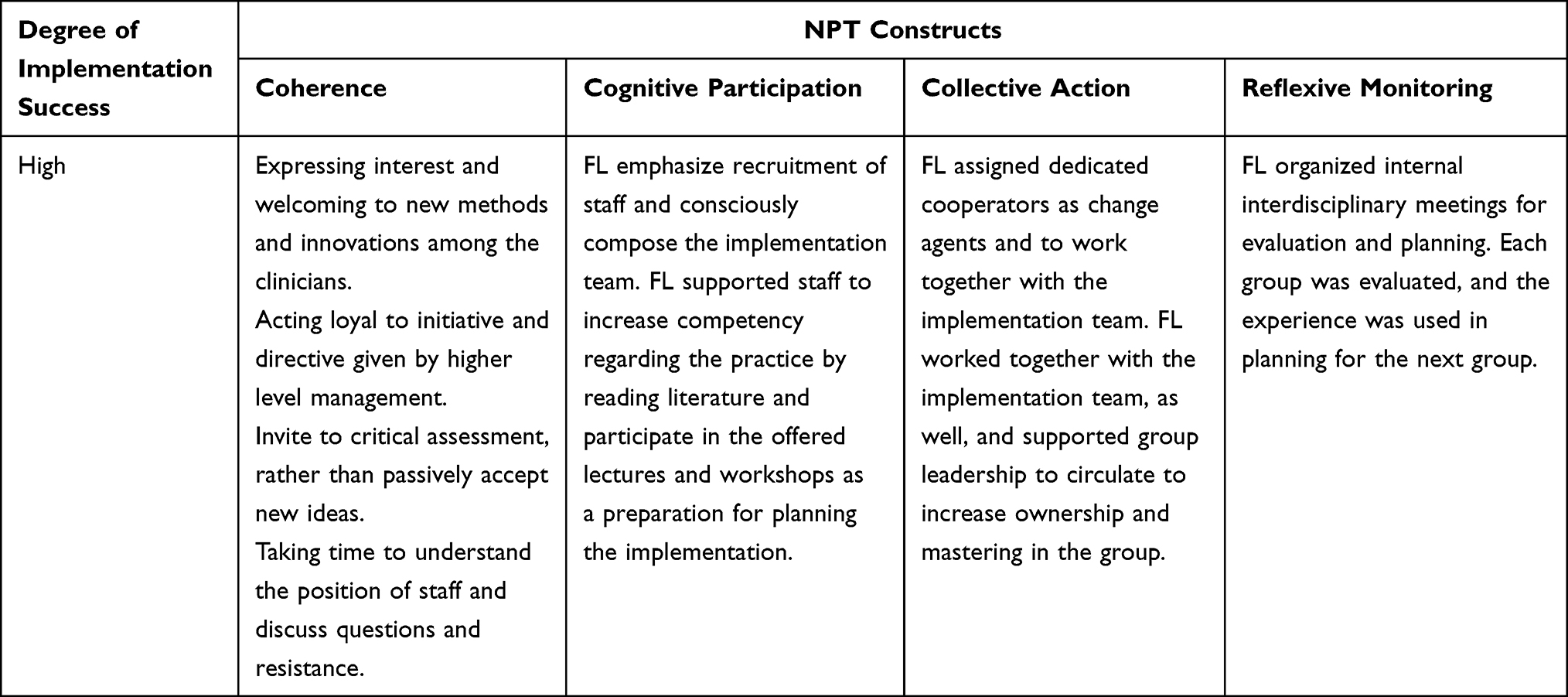 |
Table 2 The Synthesized Result of FL Approach of the High Fidelity Group Across the Four Steps of the NPT Construct Model |
The Moderate Fidelity Group
The FL who led units with moderate implementation success described how they supported the implementation process by expressing their positive attitude towards the new practice to the staff. They emphasized the importance of convincing the staff to actively participate the implementation process. FL4:
When you know that there are changes underway and there is something that you want to have introduced, you also have a small discussion, not necessarily a discussion but inform that from then and there we will start with such and such and then you will get those comments weeded out. If we can talk a little about it, we will also agree that it will be like that.
The FLs were active in the implementation process and followed the process carefully. FL5:
Then I get to take the overall view. So, I was pretty involved from start to finish.
Three out of four FLs mentioned the importance of carefully selecting motivated staff to form implementation teams. FL6:
I established a project group and I had one person who had a bit more authority than the other members of that group.
FLs emphasize the importance of leaders being honest in order to motivate cooperators to engage in the project. FL7:
Yes, I definitely think so [about the manager’s honest commitment], yes, yes, I do believe that, so we have to keep going, we have to keep going. If I just hadn’t cared so much but said that we should start with this, it probably wouldn’t have been the same.
FLs in this fidelity group did not report about planned and purposeful reflexive evaluation meetings.
These FLs generally considered their immediate superiors as supportive and trustworthy. The guidance and confirmation from their immediate superior were seen as important in carrying out the implementation efforts.
The FLs showed ambivalence in their approach to their own staff. They highlighted both their confidence in their staff competency and the need for guidance, control and follow-up.
Table 3 illustrates the protocol for the medium fidelity level group interpreted according to the four constructs of NPT. This group considered three of the four constructs.
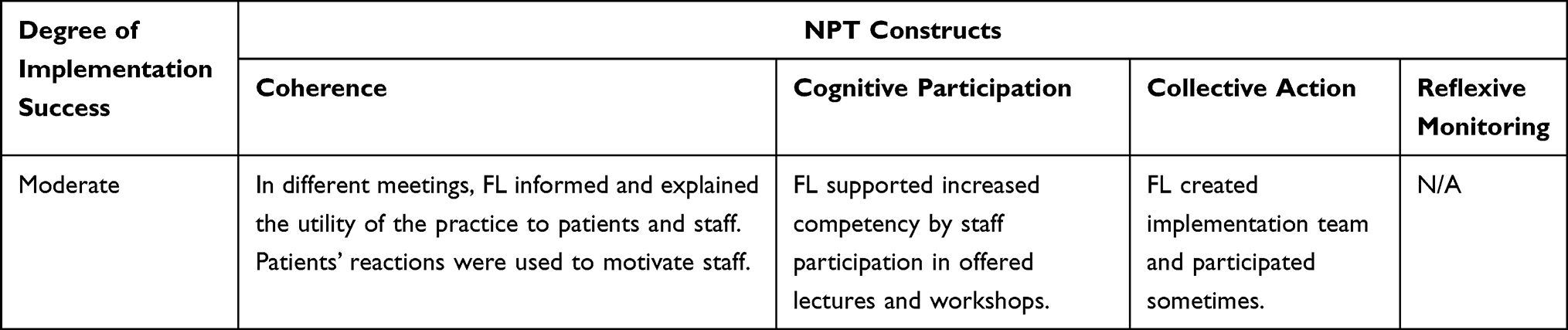 |
Table 3 The Synthesized Result of FL Approach of the Moderate Fidelity Group Across the Four Steps of the NPT Construct Model |
The Low Fidelity Group
The two FLs who represented units with limited implementation success described their lesser involvement. One of them described his/her role as limited to administration and giving instructions to clinicians for this implementation task. FL8:
Yes, it was us managers who made sure that it was done, who reminded them to do it, introduced and presented forms, showing where and how they should fill it out.
FL9 described taking on an active and central role but involving few others initially. The leader emphasized his/her own engagement and activity as key factors in achieving any result. FL9:
Yes, yes. I was the leader, implementer, teacher and I was basically everywhere.
This FL emphasized importance of providing information and education during the implementation process.
Yes, information and training simply. That’s what it’s all about. That people need to gain knowledge.
The leader utilized various meetings to inform and encourage staff participation in the project. However, there were no reported activities related to the NPT construct of Cognitive participation.
The FLs generally expressed a critical attitude towards their immediate superior and perceived a lack of interest in the project.
Interviews about their own staff revealed limited substance. In general, the importance of providing information and disseminating knowledge regarding the practice was emphasized. Knowledge, training and information to staff were deemed necessary.
Table 4 illustrates the protocol for the low fidelity level group interpreted according to the four constructs of NPT. This group considered three of the four constructs.
 |
Table 4 The Synthesized Result of FL Approach of the Low Fidelity Group Across the Four Steps of the NPT Construct Model |
Summary of Findings
The three sets of leadership approaches and their related factors in the implementation process are summarized in Table 5.
Table 5 shows the essence of FL leadership approaches and how leaders in different fidelity groups express salient factors that are of importance for implementation.
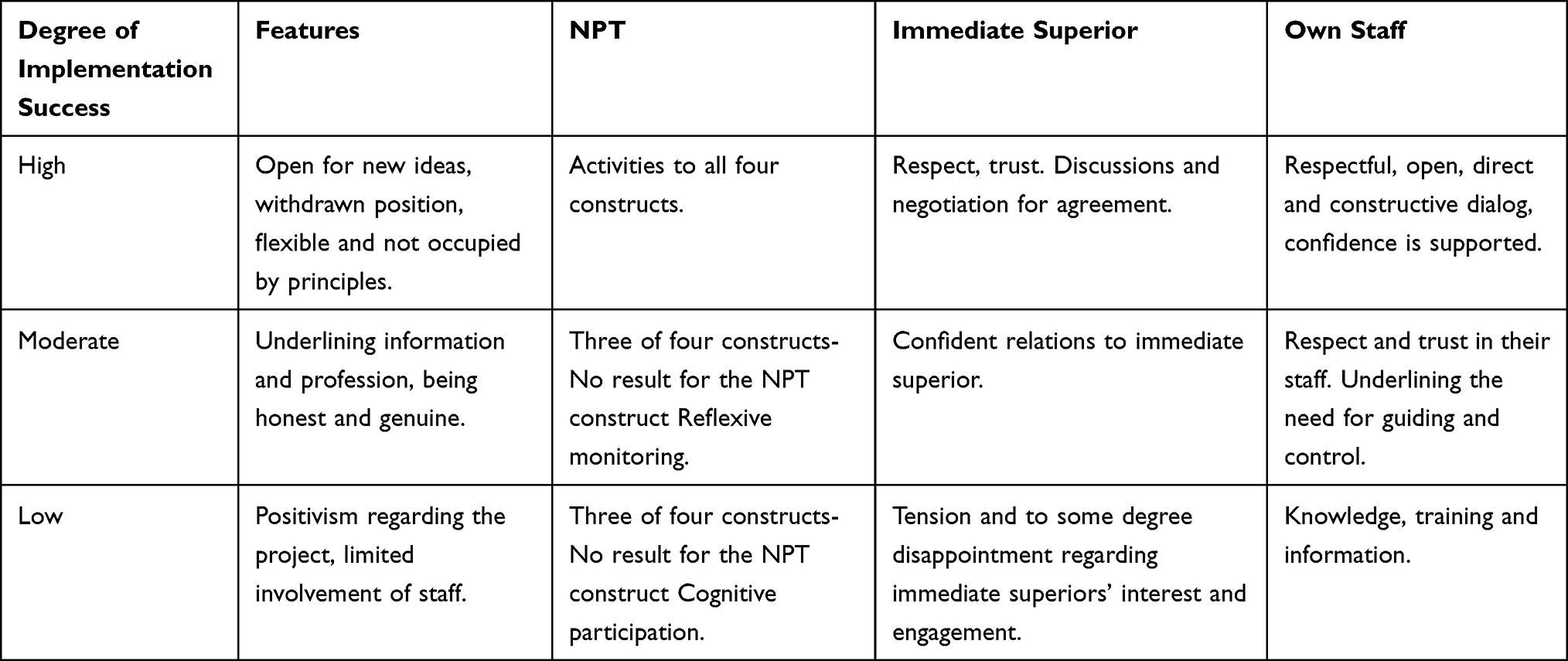 |
Table 5 Synthetized Leadership Approaches Across Implementation Success Level Groups and According to Peak Features, NPT Constructs, Relations to Immediate Superior and Own Staff |
Discussion
Our study details a wide range of actions taken by FL to facilitate the implementation of new clinical practices among their employees. The FL’s approaches to engaging employees in the changing environment varied across the three groups with differing levels of fidelity. The high fidelity group described leadership actions aligned with all four NPT constructs. In contrast, the FLs achieving moderate fidelity did not emphasize actions in line with the construct of Reflexive monitoring, and those who had low fidelity score did not highlight the construct of Cognitive participation. The lack of information on Cognitive participation may suggest insufficient processes related to initiation, enrollment, legitimation and activation, while the limited narrative on the construct of Reflexive monitoring may indicate inadequate actions related to the processes of interactional workability, relational integration, skill set workability and contextual integration,36,37 potentially impeding successful implementation. Our findings support May et al,’s18 definition of the four NPT constructs as mechanisms within the CMO configuration for implementing changes in complex organizations.
Using the Complexity Leadership Theory (CLT) lens15 to analyze and structure leadership actions and intentions, we perceived differences between the three groups of FL in how they approached the changing context, including the practice to be implemented, the mixture of professionals and individual resistance, structural changes in the team or unit, and lack of information and support from superiors. FLs leading units with a high degree of implementation success described a relation-oriented approach with an intention to pro-actively understand individual resistance, and with trust and providing adaptive space for staff member initiatives. FLs leading units with moderate or low fidelity score described a more control-oriented and guidance-oriented approach to co-operators, with a focus on providing information and knowledge to co-operators in the implementation process of implementation. The results regarding leadership approach underlined the importance of an entrepreneurial leadership approach, as defined by the CLT.15
Our results imply the importance of considering the coherence between the contexts, NPT constructs, and leadership approaches when planning for implementation in complex organizations.
Our findings also suggest that superiors who are planning for implementation in healthcare should consider the key characteristics of the FL who achieved high fidelity score such as encouraging creativity, providing space for experimentation, tolerating diversity, and embracing complexity to motivate FL to implement new knowledge.
The results highlight the importance of recognizing the complexity of the healthcare system when implementing new knowledge and embracing dynamic system processes as opportunities for implementation and improvement, in line with Khan et al,’s1 perspective.
Furthermore, it is noteworthy that the only two participants reporting to have no formal leadership training were in the high fidelity group. We have no information about the content and comprehensiveness of the training programs reported by the others, but the findings gave the impression that traditional leadership program may not cover the skills needed to lead implementation processes. Due to the magnitude of different leadership styles and the challenge to evaluate leadership in complex organizations, the result is in line with disparate and limited evidence for leadership training outcome, Njah et al.38
Limitations
Interview data from a Norwegian sample of FL within the mental health system form the basis for this study. The representativeness of the sample to a larger population or the findings as evidence of any phenomena cannot be determined. The findings are accounts of phenomena. However, the interviews facilitated the collection of rich data and enhanced the participants’ reflections.26 The sample consisted of nine participants, of which six were women. The findings may have been different if a greater number of men and a diversity of professions were included in the sample.39
The findings are limited by the organization, culture and legislation of Norwegian mental health. Although the participants were reasonably similar, which is desirable in explorative, interpretative studies,40,41 this homogeneity could also be a limitation that could result in different findings with a broader professional profile.
The study did not consider leadership approaches on multiple organizational levels, broader characteristics of treatment units, professional profile of the staff, and competency improvement programs, which may provide important complementary information.
The first author, who conducted the interviews, had previous employment as a clinical psychologist and director in one of the participating clinics. To minimize interviewer bias, two members of the research team focused on the interaction between the interviewer and the interviewee.42 No evidence of bias was observed. Moreover, the diversity of the research group increased the chances of detecting other types of biases.
The study followed the COREQ checklist where appropriate.43
Conclusion
This study describes facets of frontline leadership to facilitate the implementation of new practices, reported by the FLs themselves. It exemplifies actions and intentions in line with the four main NPT mechanisms and contemporaneously various leadership approaches that range from relation-oriented to profession-oriented to knowledge-oriented. The relation-oriented approach seems to be more beneficial for implementation than the others. The success of the high fidelity leaders is, accordingly, based on some key activities: Pro-actively and individually approach the team members by listening to the concerns and thoughts of their clinicians, give room for creativity and ensure that the four constructs in NPT are respected. The findings shed light on how FLs can exploit the instability in complex dynamic organizations, by facilitating interdisciplinary and inter-subjectively relationships to succeed implementation.
The differences in what the FLs emphasize in their leadership, even though all leaders in the low and moderate fidelity groups had attained leadership training, suggest further investigations in how FLs should be trained to succeed in implementation. However, in line with the leadership approach of the high fidelity group, it seems logical for employers to consider complexity leadership theory when designing leadership training and programs.
It seems to be an important mission for superiors to ensure that the FLs have the necessary skills to lead complex implementation, as exemplified by the skills of the high fidelity group. The result suggests the crucial meaning for employers is to find out the level of implementation process competency when recruiting new FL and their superiors.
Abbreviations
CAS, Complex Adaptive System; CLT, Complexity Leadership Theory; CMO, Context-Mechanism-Outcome; FL, Frontline leaders; NPT, Normalization Process Theory; STC, Systematic Text Condensation.
Acknowledgments
The authors would like to thank the FLs for their participation in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, analyses and interpretation, or in all these areas; took part in drafting, critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by South-Eastern Norway Regional Health Authority (Helse Sør-Øst HF) (grant number 2015106) and Stavanger University Hospital, Trial registration: ClinicalTrials.gov Identifier: NCT03271242.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Khan S, Vandermorris A, Sheperd J, et al. Embracing uncertainty, managing complexity: applying complexity thinking principles to transformation efforts in healthcare systems. BMC Health Serv Res. 2018;18(192). doi:10.1186/s12913-018-2994-0
2. Thompson DS, Fazio X, Kustra E, Patric L, Stanley D. Scoping review of complexity theory in health services research. BMC Health Serv Res. 2016;16(87). doi:10.1186/s12913-016-1343-4
3. Braithwaite J, Churruca K, Long JC, Ellis LA, Herkes J. When complexity science meets implementation science: a theoretical and empirical analysis of systems change. BMC Med. 2018;1663. doi:10.1186/s12916-018-1057-z
4. Greenhalgh T, Papoutsi C. Studying complexity in health services research: desperately seeking an overdue paradigm shift. BMC Med. 2018;16(95). doi:10.1186/s12916-018-1089-4
5. Wensing M, Grol R (2020). Theories on Implementation of Change in Healthcare. In: Wensing M, Grol R Grimshaw JM (editors), Improving Patient Care. The Implementation of Change in Healt Care (
6. Reed JE, Green S, Howe C. Translating evidence in complex systems: a comparative review of implementation and improvement frameworks. Int J Qual Health Care. 2019;31(3):173–182. doi:10.1093/intqhc/mzy158
7. Meza RD, Triplett NS, Woodward GS, et al. The relationship between first-level leadership and inner-context and implementation outcomes in behavioral health: a scoping review. Implement Sci. 2021;16(1). doi:10.1186/s13012-021-01104-4
8. Birken SA, Clary A, Tabriz AA, et al. Middle managers’ role in implementing evidence-based practices in healthcare: a systematic review. Implement Sci. 2018;13(149). doi:10.1186/s13012-018-0843-5
9. McSherry R, Pearce P. What are the effective ways to translate clinical leadership into health care quality improvement? J Healthc Leadersh. 2016;8:11–17. doi:10.2147/JHL.S46170
10. Uhl-Bien M, Marion R, McKelvey B. Complexity leadership theory: shifting leadership from the industrial age to the knowledge era. Leadersh Q. 2007;18:298–318. doi:10.1016/j.leaqua.2007.04.002
11. Daly J, Jackson D, Mannix J, Davidson PM, Hutchinson M. The importance of clinical leadership in the hospital setting. J Healthc Leadersh. 2014;6:75–83. doi:10.2147/JHL.S46161
12. Nordin H, Rørtveit K, Mathisen GE, et al. Frontline leadership for implementing clinical guidelines in Norwegian mental health services: a qualitative study. J Health Organiz Manage. 2022;36(5):617–632. doi:10.1108/JHOM-08-2021-0286
13. Plsek P, Wilson T. Complexity, leadership, and management in healthcare organisations. BMJ. 2001;323(7315):746–749. doi:10.1136/bmj.323.7315.746
14. Uhl-Bien M, Arena M. Complexity leadership: enabling people and organizations for adaptability. Org Dyn. 2017;46(1):9–20. doi:10.1016/j.orgdyn.2016.12.001
15. Uhl-Bien M, Arena M. Leadership for organizational adaptability: a theoretical synthesis and integrative framework. Leadersh Q. 2018;29(1):89–104. doi:10.1016/j.leaqua.2017.12.009
16. May C, Mair R, Finch F, et al. Development of a theory of implementation and integration: normalization process theory. Implement Sci. 2009;4(29). doi:10.1186/1748-5908-4-29
17. Flynn R, Rotter T, Hartfeild D, Newton AS, Scott SD. A realist evaluation to identify contexts and mechanisms that enabled and hindered implementation and had an effect on sustainability of a lean intervention in pediatric healthcare. BMC Health Serv Res. 2019;19(1). doi:10.1186/s12913-019-4744-3
18. May C, Albers B, Bracher M, et al. Translational framework for implementation evaluation and research: a normalisation process theory coding manual for qualitative research and instrument development. Implement Sci. 2022;17(1). doi:10.1186/s13012-022-01191-x
19. Pereira VC, Silva SN, Carvalho VKS, Zanghelini F, Barreto JOM. Strategies for the implementation of clinical practice guidelines in public health: an overview of systematic reviews. Health Res Policy Syst. 2022;20(13). doi:10.1186/s12961-022-00815-4
20. De Leo A, Bloxsome D, Bayes S. Approaches to clinical guideline development in healthcare: a scoping review and document analysis. BMC Health Serv Res. 2023;23(37). doi:10.1186/s12913-022-08975-3
21. Kueny A, Shever LL, Mackin ML, Titler MG. Facilitating the implementation of evidence-based practice through contextual support and nursing leadership. J Healthc Leadersh. 2015;29–39. doi:10.2147/JHL.S45077
22. Girlanda F, Fiedler I, Becker T, Barbui C, Koesters M. The evidence-practice gap in specialist mental healthcare: systematic review and meta-analysis of guideline implementation studies. Br J Psychiatry. 2017;210(1):24–30. doi:10.1192/bjp.bp.115.179093
23. Malterud K. Systematic text condensation: a strategy for qualitative analysis. Scand J Public Health. 2012;40(8):795–805. doi:10.1177/1403494812465030
24. Ruud T, Drake RE, Benth JS, et al. The effect of intensive implementation support on fidelity for four evidence-based psychosis treatments: a cluster randomized trial. Adm Policy Ment Health Ment Health Serv Res. 2021;48:909–920. doi:10.1007/s10488-021-01136-4
25. Ruud T. Implementation of guidelines for treatment of psychosis (NCT03271242) U.S. National Library of Medicine ClinicalTrials.gov. 2017.
26. Malterud K, Siersma VD, Guassora AD. Sample size in qualitative interview studies: guided by information power. Qual Health Res. 2016;26(13):1753–1760. doi:10.1177/1049732315617444
27. Braun V, Clarke V. To saturate or not to saturate? Questioning data saturation as a useful concept for thematic analysis and sample-size rationales. Qual Res Sport Exerc Health. 2019;1–16. doi:10.1080/2159676x.2019.1704846
28. Lederansvaret i sykehus (Det Kongelige Helse- og Omsorgsdepartementet) [managerial responsibility in hospitals]; 2013.
29. McMillan SS, King M, Tully MP. How to use the nominal group and Delphi techniques. Int J Clin Pharm. 2016;38(3):655–662. doi:10.1007/s11096-016-0257-x
30. Bevan MT. A method of phenomenological interviewing. Qual Health Res. 2014;24(1):136–144. doi:10.1177/1049732313519710
31. Egeland KM, Heiervang KS, Landers M, Ruud T, Drake RE, Bond GR. Psychometric properties of a fidelity scale for illness management and recovery. Adm Policy Ment Health Ment Health Serv Res. 2020;47(6):885–893. doi:10.1007/s10488-019-00992-5
32. Joa I, Johannessen JO, Heiervang KS, et al. The family psychoeducation fidelity scale: psychometric properties. Adm Policy Ment Health Ment Health Serv Res. 2020;47(6):894–900. doi:10.1007/s10488-020-01040-3
33. Ruud T, Drivenes K, Drake RE, et al. The antipsychotic medication management fidelity scale: psychometric properties. Adm Policy Ment Health Ment Health Serv Res. 2020;47(6):911–919. doi:10.1007/s10488-020-01018-1
34. Ruud T, Høifødt TS, Hendrick DC, et al. The physical health care fidelity scale: psychometric properties. Adm Policy Ment Health Ment Health Serv Res. 2020;47(6):901–910. doi:10.1007/s10488-020-01019-0
35. McHugo GJ, Drake RE, Whitley R, et al. Fidelity outcomes in the national implementing evidence-based practices project. Psychiatric Serv. 2007;58(10):1279–1284. doi:10.1176/ps.2007.58.10.1279
36. McNaughton RJ, Steven A, Shucksmith J. Using normalization process theory as a practical tool across the life course of a qualitative research project. Qual Health Res. 2020;30(2):217–227. doi:10.1177/1049732319863420
37. May C, Finch T. Implementing, embedding, and integrating practices: an outline of normalization process theory. Sociology. 2009;43(3):535–554. doi:10.1177/0038038509103208
38. Njah J, Hansoti B, Adeyemi A, et al. Measuring for success: evaluating leadership training programs for sustainable impact. Ann Glob Health. 2021;87(1):1–10. doi:10.5334/aogh.3221
39. Shen W, Joseph DL. Gender and leadership: a criterion-focused review and research agenda. Hum Resour Manag Rev. 2021;31(2). doi:10.1016/j.hrmr.2020.100765
40. Smith J, Flowers A, Larkin P. Planning an IPA research study. In: Interpretative Phenomenological Analysis Theory, Method and Research. Sage Publications Ltd.; 2012:40–55.
41. Robinson OC. Sampling in interview-based qualitative research: a theoretical and practical guide. Qual Res Psychol. 2013;11(1):25–41. doi:10.1080/14780887.2013.801543
42. Pannucci CJ, Wilkins EG. Identifying and avoiding bias in research. Plast Reconst Surg. 2010;126(2):619–625. doi:10.1097/PRS.0b013e3181de24bc
43. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.