")
Back to Journals » Journal of Asthma and Allergy » Volume 16
Impact of Guideline-Based Asthma Treatment on Health Services Use in Singapore Before and During COVID-19 Outbreak
Authors Lim LHM, Lim HF, Liew MF, Chen W
Received 10 June 2023
Accepted for publication 29 September 2023
Published 31 October 2023 Volume 2023:16 Pages 1207—1216
DOI https://doi.org/10.2147/JAA.S425342
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Luis Garcia-Marcos
Laura Huey Mien Lim,1 Hui Fang Lim,2,3 Mei Fong Liew,2– 4 Wenjia Chen1
1Saw Swee Hock School of Public Health, National University of Singapore, Singapore, Singapore; 2Division of Respiratory and Critical Care Medicine, Department of Medicine, National University Hospital, National University Health System, Singapore, Singapore; 3Department of Medicine, Yong Loo Lin School of Medicine, National University of Singapore, Singapore Singapore; 4FAST and Chronic Programmes, Alexandra Hospital, National University Health System, Singapore, Singapore
Correspondence: Laura Huey Mien Lim, PhD Candidate in Health Economics and Outcomes Research, Saw Swee Hock School of Public Health, National University of Singapore, Tahir Foundation Building/ MD1, 12 Science Drive 2, #10-01, Singapore, 117549, Singapore, Tel +65 88527276, Email [email protected]
Introduction: To date, the role of standard asthma care in reducing asthma-related health services use (HSU) during the COVID-19 pandemic remains unclear. This study examined the impact of guideline-based asthma treatment on the use of asthma-related emergency department (ED) visits, polyclinic visits (total visits and urgent visits characterized by nebuliser use) before and during the pandemic.
Methods: Data from April 2017 to October 2020 was obtained from the National University Health System, one of the three healthcare clusters in Singapore. Using generalized linear models, we estimated the joint effects of the ratio of preventer to reliever dispensations (PRR) and COVID-19 on asthma-related ED visits per hospital per month, total asthma-related polyclinic visits and asthma-related urgent polyclinic visits per clinic per month.
Results: Findings show that before the onset of COVID-19, for every 0.5 unit increase in PRR, the number of asthma-related ED visits and urgent polyclinic visits decreased by 12.9% (95% CI: − 13.0% to − 12.9%) and 6.8% (95% CI: − 6.9% to – 6.7%), respectively, whereas total asthma-related polyclinic visits increased by 1.0% (95% CI: 0.9% to 1.0%). During the pandemic, a 0.5 unit increase of PRR decreased the number of asthma-related ED visits, urgent and total polyclinic visits by 16.9% (95% CI: − 17.0% to – 16.9%), 9.3% (95% CI: − 9.5% to − 9.2%) and 0.7% (95% CI: − 0.8% to − 0.7%), respectively.
Discussion: These findings suggest that regardless of the COVID-19 pandemic, an increase in PRR consistently reduced the frequency of asthma-related urgent and emergent care, although it barely influenced routine asthma follow-up visits.
Plain Language Summary: In order to understand how guideline-based asthma management affects asthma-related health services use during the COVID-19 pandemic, in this study, we examined the pattern and impact of asthma medication utilisation (ie, the ratio of preventer to reliever dispensations) on asthma-related total polyclinic visits, urgent polyclinic visits and emergency department visits, and compared such effects before and during COVID-19 outbreak.
We found a significant reduction in reliever medication dispensations and asthma-related total polyclinic visits, urgent polyclinic visits and emergency department visits in Singapore during the COVID-19 pandemic, as compared to the pre-pandemic period. We also observed a rapid increase in the ratio of preventer to reliever dispensations in Singapore since early 2019 which accelerated during the COVID-19 pandemic. Our finding suggests that this increase could be associated with a significant reduction in asthma-related urgent and emergent care. This effect persisted both before and during the COVID-19 pandemic.
These current findings suggest that guideline-based asthma management, which can be delivered through primary care and self-care, is able to reduce asthma-related urgent care even in a global pandemic with restrained healthcare resources.
Keywords: asthma management guidelines, COVID-19, health services use
Introduction
In 2019, asthma affected 252 million people worldwide, and it is the most prevalent chronic disease among children,1 with 11.6% of 6–7-year-old children and 13.7% of 13–14-year-old children suffering from wheezes between 2001 and 2003.2 Over the years, there has been a global increase in the burden of asthma with respect to prevalence, morbidity and costs.3 In Singapore, 20% of children and 5% of adults suffer from asthma.4 Asthma is the second largest contributor to the chronic respiratory disease burden in Singapore,5 incurring SGD$2.09 billion (US$1.50 billion) of economic burden annually.6
The cornerstone of asthma management is to achieve symptom control.7 Asthma can be controlled with the use of preventer medication, ie, inhaled corticosteroids (ICS) alone or in combination with long-acting beta-agonist (LABA), while reliever medications such as the short-acting beta-agonists (SABA) are used on an as-needed basis.7 In April 2019, GINA undertook a fundamental change in its asthma guidelines stipulating that all adults and adolescents with asthma should no longer be treated with SABA alone; rather, they should receive either symptom-driven treatment with ICS-formoterol (in mild asthma) or daily ICS-containing treatment.8 In Singapore, patients presenting to primary care clinics (ie, polyclinics) and emergency departments (ED) with an acute asthma exacerbation are commonly treated with nebulisations.9 The use of nebulisations during asthma attendance is indicative of urgent care, as it serves to deliver high-dose reliever medication quickly and efficiently10 typically to patients experiencing severe asthma attacks.
In recent years, there has been a paradigm shift in asthma management from a severity-based classification system to a control-based approach as reflected in the Global Initiative for Asthma (GINA) guidelines, with increasing focus on reducing patient reliance on relievers and encouraging regular use of controllers such as inhaled corticosteroids (ICS).7 Control-based asthma management in Finland had led to a reduction in morbidity and healthcare and economic burden of asthma.11 In Canada, regular use of ICS was also found to be associated with a lower risk of asthma-related mortality12 and hospitalisation.13
When it comes to managing asthma, COVID-19 is an important factor of consideration as COVID-19 in asthma patients may be associated with prolonged asthma symptoms and worsening asthma control.14,15 Also, we will be living in a COVID-19 era and experiencing recurrent COVID-19 outbreaks,16 and hence a clearer understanding of the impact of guideline-based asthma management in the presence of COVID-19 may better prepare us for a future in which COVID-19 is constantly present. Global literature has shown that the COVID-19 pandemic has caused disruptions to asthma care delivery, resulting in hindered access and adherence to drugs, interrupted contact with healthcare providers, and barriers to physical and mental health due to COVID-19 restrictions.17 Since its onset, a reduction in asthma-related urgent care has been observed globally in primary and tertiary care, such as in the US18 and the UK,19,20 and previous works attributed such reductions to reduced exposure to environmental exposure and respiratory virus.21 While improved asthma self-management has been observed during the COVID-19 pandemic22,23 and several studies had suggested the inverse effect of guideline-based asthma treatment on asthma-related health services use (HSU),24,25 to date, the extent of guideline-based asthma management and its impact on reducing asthma-related HSU during the COVID-19 pandemic has not been clearly established.
Using population-level electronic health records from one of the three healthcare clusters in Singapore, we aim to estimate the impact of guideline-based use of asthma medications on asthma-related HSU including total polyclinic visits, urgent polyclinic visits and ED visits, and compare such effects before and during COVID-19 outbreak.
Materials and Methods
Data Source
The National University Health System (NUHS) is one of the three regional health clusters in Singapore and caters mainly to communities in the western region of the city-state. NUHS data thus cover an estimated 1.5 million residents26 which makes up one-third of Singapore’s resident population, including three public acute hospitals,27 three EDs and seven polyclinics (collectively known as National University Polyclinics or NUP) which provide primary care treatment for acute conditions and management of chronic illnesses. We accessed data from the electronic health records of NUHS. Hospital-level data were available from April 1, 2017, to October 31, 2020, while polyclinic-level data were available from January 1, 2019, to October 31, 2020.
The hospital-level data include hospital-specific total ED attendances and asthma-related ED attendances measured per month in all three public acute hospitals under NUHS.
The clinic-level data include polyclinic-specific monthly information on the number of asthma visits (including both planned and unscheduled visits), the number of asthma visits with any nebuliser dispensation, the dispensation frequencies of preventers (eg, inhaled corticosteroids or ICS) as well as relievers (eg, short-acting beta-agonists or SABA) from six out of the seven total NUPs. However, as data on Queenstown Polyclinic is mostly missing, we excluded all observations made on this polyclinic from our analysis.
Study Sample and Variables
This was a longitudinal retrospective study of patients with asthma who ever visited an NUHS polyclinic or ED during the study period. We measured asthma-related HSU in two settings: ED and polyclinic, respectively, defined as an episode of visit to an ED or a polyclinic with asthma being the primary diagnosis (International Classification of Diseases (ICD) 9: 493 or ICD 10: J45-J46). Respectively, we used the hospital- and clinic-level data obtained to study patterns of asthma-related ED and polyclinic visits.
The primary outcomes of this study include asthma-related polyclinic visits, asthma-related urgent polyclinic visits (characterised by the dispensation of a nebuliser), and asthma-related ED visits, on a monthly basis. Asthma-related ED visits were tracked at the hospital level from April 2017 to October 2020, while overall and urgent asthma-related polyclinic visits were tracked at the clinic level from January 2019 to October 2020.
This study considered two exposure variables: COVID-19, and guideline-based asthma medication use. To measure the impact of COVID-19, we denoted the ordinal variable COVID-19 Stage, which represents the phase of COVID-19 that Singapore underwent at a given time during the study period. To account for both the immediate and longer-term effects of COVID-19, observations were segmented into 3 COVID-19 stages based on two cut-off timepoints: January 2020 which marks the onset of COVID-19 in Singapore,28 and June 2020 which marks the end of the 8-week circuit breaker measures and the beginning of Singapore’s reopening,29 which signifies a change in the control level and length of COVID-19 in Singapore. As such, the variable COVID-19 Stage was assigned a value of 0 for observations made between April 2017 and December 2019, ie, pre-COVID observations, a value of 1 for observations made between January 2020 and May 2020, ie, Phase 1 observations, and a value of 2 for observations made between June 2020-October 2020, ie, Phase 2 observations.
To examine the impact of guideline-based asthma medication use, we derived the ratio of preventer to reliever dispensations (PRR) as an indicator for following GINA-recommended asthma treatment. Clinic-level PRR was calculated for each month throughout the study period by dividing the total number of preventer dispensations by total reliever dispensations, for each polyclinic. As hospital-level PRR component data were not available, aggregate monthly PRR across the polyclinics were used to explain outcomes in the ED setting.
Statistical Analysis
All statistical analyses were performed in R (version 4.1.1). We first described the current trends of asthma-related ED visits, polyclinic visits and urgent polyclinic visits, and PRR in NUHS during the study period. Next, we developed generalized linear models (GLM) with Poisson distribution and log link to estimate the impact of COVID-19 Stage and PRR on asthma-related ED visits and polyclinic visits between April 2017-October 2020 and January 2019-October 2020, respectively. A separate GLM with a logit link and binomial family was used to estimate the impact of COVID-19 and PRR on urgent asthma-related polyclinic visits. The unit of analysis was monthly episodes of HSU at hospital level or clinic level. The dependent variables were, respectively, the numbers of asthma-related ED visits and polyclinic visits and the proportion of asthma-related polyclinic visits which required nebuliser dispensation (indicating urgent polyclinic visits). The independent variables included COVID-19 Stage, PRR, and their first-order interaction. Generalized estimating equations were used to obtain inference by considering the clustering of time-series outcome data within a polyclinic or hospital.
Finally, we estimated the marginal mean estimates of asthma-related ED visits, polyclinic visits and urgent polyclinic visits across different COVID-19 stages and PRR levels. Further, we derived the marginal effects of (1) COVID-19 on asthma-related polyclinic visits, urgent polyclinic visits and ED visits; (2) PRR on the change in expected asthma-related polyclinic visits, urgent polyclinic visits and ED visits; and (3) PRR on the expected asthma-related polyclinic visits, urgent polyclinic visits and ED visits under different stages of the COVID-19 pandemic. Here, the marginal effect is defined as the change in the expected outcome led by a change in the level of the exposure variable, keeping other covariates constant. Marginal effects carry causal interpretations assuming no unmeasured exposure-outcome confounding.30 We performed bootstrapping (10,000 iterations) for the joint distribution of the regression coefficients and for the marginal mean estimates and adjusted mean estimates to obtain robust standard errors.
Results
The NUHS health cluster serves approximately 1.5 million residents in Singapore, ie, a third of the resident population. Between Aril 2017 and October 2020, there was a total of 8170 asthma-related ED episodes incurred, corresponding to an average of 190 asthma-related ED episodes per month which accounts for 1.01% of the total ED visits. Meanwhile, there were a total of 31,326 asthma-related polyclinic visits between January 2019 and October 2020, corresponding to 1424 asthma-related polyclinic visits per month. Supplementary Table 1 presents a summary of asthma-related polyclinic visits. In 2018, 12.94%, 7.46% and 0.86% of the polyclinic visits were associated with any risk, high risk and super high risk of asthma, as suggested by the need for any nebulisation, at least two nebulisations and at least six ventolin canister, respectively.
Figure 1 presents the trends of asthma-related ED visits, total and urgent polyclinic visits and PRR between January 2019-October 2020. While overall asthma-related polyclinic visits did not display a clear trend, the volume of severe asthma healthcare utilisation (ie, asthma-related urgent polyclinic visits and ED visits) more than halved during the COVID-19 outbreak in Singapore. During the pre-pandemic period (January 2019-December 2019), we observed that the number of asthma-related urgent polyclinic visits and ED visits had, respectively, hovered above 150 and 200 episodes per month, but which consistently declined throughout Phase 1 by approximately 70% and remained low in Phase 2.
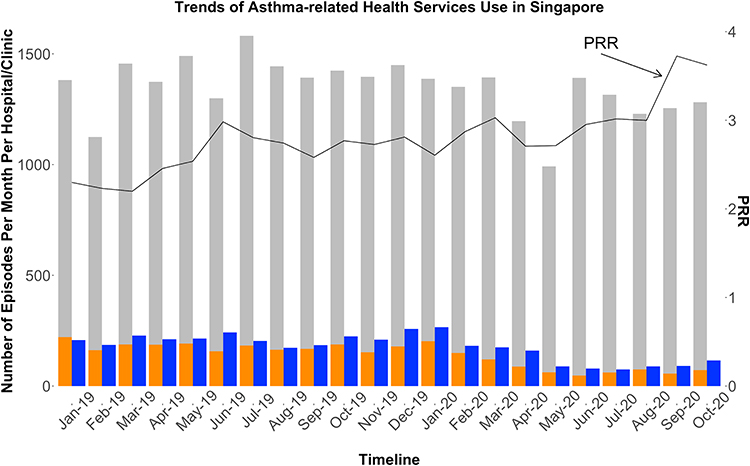 |
Figure 1 Presents the trends of per-hospital asthma-related ED visits (the blue bars), per-clinic asthma-related non-urgent polyclinic visits (the grey bars), per-clinic asthma-related urgent polyclinic visits (the orange bars) and the PRR (the solid black line) between January 2019 and October 2020. |
Figure 2 presents the trends of preventer and reliever dispensations and the PRR between January 2019-October 2020. A constant increase in PRR had been observed since January 2019, and this increase in PRR accelerated during the pandemic. Before the COVID-19 outbreak, PRR increased from 2.298 to 2.605 in 12 months. During Phase 1 of the pandemic, PRR increased from 2.61 to 2.95 in 5 months, and during Phase 2, the increase was even faster (from 2.95 to 3.62 in 5 months). In addition, the total number of reliever medication dispensations decreased significantly from 693 dispensations per month during the pre-COVID-19 period to 604 dispensations per month during the pandemic (Change = −12.77%, 95% CI: −18.55% to −5.74%).
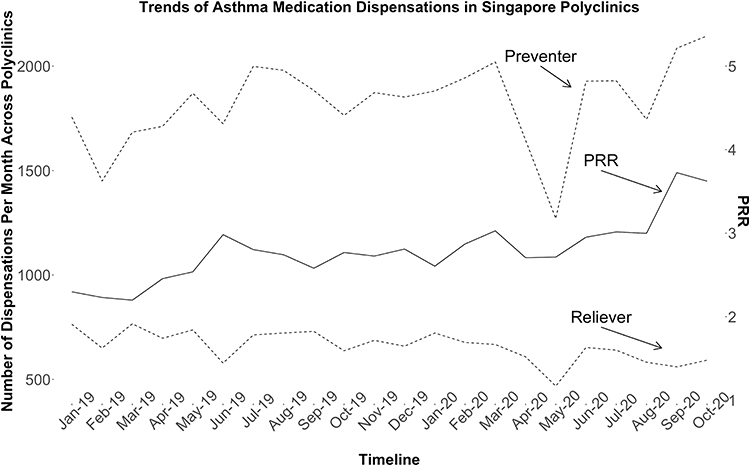 |
Figure 2 Presents the trends of per-clinic preventer and reliever dispensations (the dashed lines) and the PRR (the solid line) between January 2019 and October 2020. |
Figure 3 shows the marginal mean estimates of total asthma-related polyclinic visits, urgent polyclinic visits and ED visits across different phases of the COVID-19 pandemic and PRR levels. Over the whole observation period, COVID-19 had reduced total asthma-related polyclinic visits from 315 to 267 (corresponding to a 15.13% average reduction, 95% CI: −15.26% to −14.99%) episodes per month, urgent polyclinic visits from 35 to 15 (corresponding to a 57.61% average reduction, 95% CI: −57.87% to −57.351%) episodes per month, and ED visits from 76 to 40 (corresponding to a 41.09% average reduction, 95% CI: −41.31% to −40.87%) episode per month.
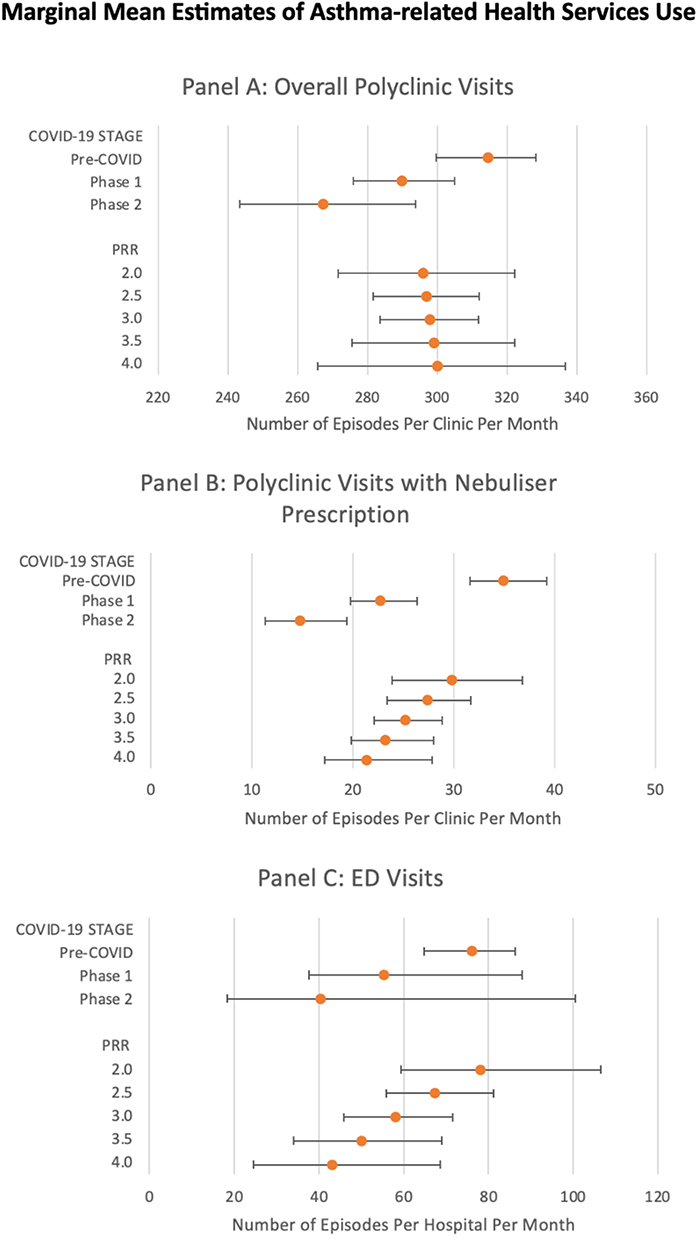 |
Figure 3 Presents the marginal mean estimates of overall asthma-related polyclinic visits (number of episodes per clinic per month), asthma-related urgent polyclinic visits (number of episodes per clinic per month), and asthma-related ED visits (number of episodes per hospital per month) across different COVID-19 stages and PRR levels. |
Figure 4 shows the marginal effects of RR on asthma-related health services use. An Increase of 0.5 units in PRR 5 has led to a consistent reduction in asthma-related urgent polyclinic visits (7.57% average reduction, 95% CI: −7.68% to −7.47%) and ED visits (13.11% average reduction, 95% CI: −13.17% to −13.05%), but it barely affected the frequency of overall asthma-related polyclinic visits (0.38% average increase, 95% CI: 0.35% to 0.42%).
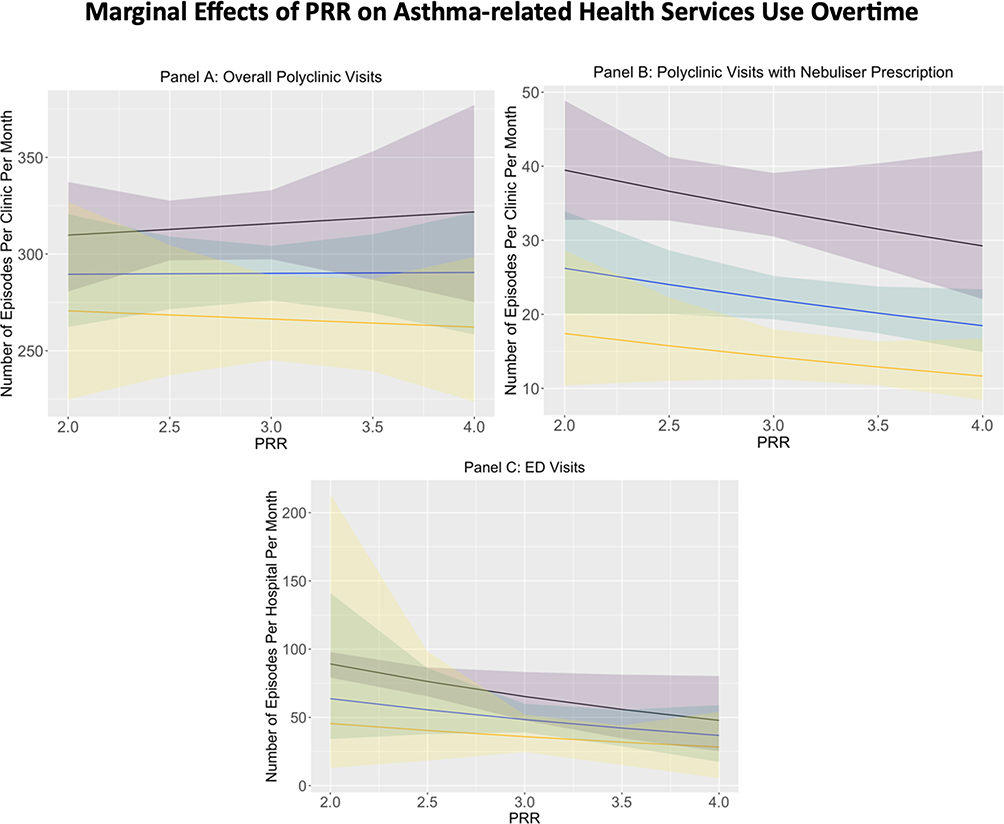 |
Figure 4 Presents the marginal effects of the ratio of PRR on overall asthma-related polyclinic visits (number of episodes per clinic per month), asthma-related urgent polyclinic visits (number of episodes per clinic per month) and asthma-related ED visits (number of episodes per hospital per month) by COVID-19 Stage. For each panel, the black line with purple confidence band, the blue line with blue confidence band, and the yellow line with yellow confidence band each represent the adjusted mean estimates and the 95% confidence interval during Pre-COVID, Phase 1 and Phase 2 respectively. |
Although overall asthma-related polyclinic visits appeared to decrease throughout the COVID-19 outbreak (−15.13%, 95% CI: −15.26% to −14.99%), the visit frequency was not notably affected by changes in PRR. For every 0.5 units increase in PRR, overall asthma-related polyclinic visits increased by 0.96% (95% CI: 0.92% to 0.99%) during pre-COVID times and decreased 0.73% (95% CI: -0.77% to - 0.69%) in the first 10 months of the pandemic.
On the other hand, the increase of PRR consistently reduced asthma-related ED visits and urgent polyclinic visits. These patterns were not affected by the outbreak of COVID-19. For every 0.5 units increase in PRR, asthma-related ED visits decreased by 12.94% (95% CI: −12.99% to −12.88%) and 16.95% (95% CI: −17.01% to −16.88%) before and during the pandemic, respectively, whereas asthma-related urgent polyclinic visits decreased by 6.77% (95% CI: -6.86% to -6.67%) and 9.34% (95% CI: −9.47% to −9.21%) before and during the pandemic, respectively.
Discussion
We obtained a presentable sample of data on patients who incurred any asthma-related polyclinic visit or ED visit in one of the three healthcare clusters in Singapore over the past five years. Supplementary Table 2 summarises the demographic characteristics of asthma patients by care setting based on findings from relevant studies. Of asthma patients presented at the ED, the mean age was an estimated 43 years and 49% were females.31 Of asthma patients presented at polyclinic settings, the mean age of patients is 48.3 and about 71.9% are females.32 Using the data obtained, we estimated the joint effects of PRR and COVID-19 on three HSU outcomes: total asthma-related ED visits per hospital per month, total asthma-related physician visits and urgent care visits per polyclinic per month. We observed a rapid increase in PRR since early 2019, and a sharp decline in asthma-related HSU since the onset of COVID-19. Importantly, our study showed that both before and during different phases of the COVID-19 pandemic, an increase in PRR consistently led to a significant reduction in asthma-related urgent and emergent care, whereas it barely influenced routine asthma follow-up visits. These findings provide critical real-world evidence supporting the effectiveness of guideline-based asthma management in helping individuals cope with asthma through primary care and self-care, particularly in a global pandemic during which healthcare resources are likely to be scarce.
Our findings regarding the lower volumes of asthma-related urgent care use during the COVID-19 pandemic are consistent with findings from studies conducted in other countries. Asthma-related ED visits in the US had declined by 30.7% in 2020 compared to pre-pandemic times.18 In the UK, the national lockdown implemented as a COVID-19 safety measure was associated with a 36% pooled reduction in emergency admissions for asthma in Scotland and Wales.19 Urgent episodes of asthma-related primary care visits also decreased significantly in England by approximately 20 episodes per 100 patients per year, comparing post-lockdown to pre-lockdown times.20
Between 2019 and 2020, a persistent increase in PRR was observed among asthma patients receiving primary care at polyclinics in Singapore, which further accelerated during the COVID-19 pandemic. This may be attributed to a change in GINA guideline in 2019, which emphasised the importance of switching to controllers even in STEP 1 GINA asthma management as compared to the prior recommendation of as-needed usage of relievers.8 In response to this change, physicians in Singapore began prescribing controllers to all asthma patients. The COVID-19 pandemic further expedited this shift, as physicians strived to minimise in-person clinic visits while ensuring patients had sufficient medications at home. As such, home delivery services for medications were rolled out. In addition, the accelerated increase in PRR observed during the COIVD-19 pandemic was accompanied by a significant decrease in reliever medication dispensations. A contributing factor to this change could be the reduction in asthma exacerbations, which have been observed globally during the COVID-19 pandemic,18 which in turn may be due to the reduction in respiratory viral infections led by COVID-19 measures.18
Previous studies have shown that increased adherence to ICS is associated with reduced asthma-related ED visits,33 while high use of SABA is associated with an increased risk of exacerbations and asthma-related primary care consultations.34 Our current study further demonstrated that a combination of higher controller use and lower reliever use can reduce the frequency of asthma-related urgent and emergent care, with this effect persisting across different phases of the COVID-19 pandemic. This finding suggests that reinforcing guideline-based asthma management effectively reduces the need for asthma urgent care, independent of external factors such as reduced social interaction and environmental exposure caused by COVID-19. With the support of guideline-based treatment, asthma patients can achieve better symptom control even during a global pandemic with restricted healthcare access, reducing the risk of functional impairment which potentially requires urgent care. Remote interventions can be used to deliver guideline-based asthma management and support self-management, which has been shown to be clinically effective.35
Healthier SG is a nationwide initiative in Singapore aimed at transforming the healthcare system by promoting preventive care and right-siting patients with certain chronic diseases, such as asthma, in primary care settings.36 Our results support the current focus in Singapore on improving asthma management in primary care and shifting it away from secondary care.37 This shift is especially relevant for the majority of asthma patients who have mild or moderate asthma, who can be effectively managed in primary care clinics. Specialist outpatient clinics can then focus on treating only the difficult-to-treat and severe asthma patients.
Our study has several key strengths. First, to the best of our knowledge, our study is the first to investigate the association between asthma management and reduced HSU during the COVID-19 pandemic. Second, the availability of linked data on asthma medication use and urgent care episodes in the NUHS data system allowed the joint assessment of PRR and asthma-related urgent HSU. Third, this study is population-based and covers 1.5 million residents in Singapore, accounting for one-third of the total resident population.
There are three main limitations in this study. First, without individual-level data, we were unable to adopt a quasi-experimental study design which involves propensity score matching or difference-in-difference approaches to establish causality between guideline-based asthma treatment and reduced asthma HSU. In our future study, we will analyse patient-level polyclinic and ED data to examine the impact of asthma management on the healthcare burden of asthma in Singapore. Second, our study outcomes were limited to urgent primary care and emergent care and did not include inpatient care or specialist outpatient care for asthma nor HSU for asthma-related comorbidities. Future study should holistically evaluate the impact of guideline-based asthma treatment on the HSU of asthma patients during the COVID-19 pandemic. Third, as the current dataset lacked severity categorization, we were unable to assess the impact of PRR on the HSU of patients with the most severe form of asthma who were exposed to high oral corticosteroid use.
Conclusions
Following the change in GINA recommendations to encourage the use of controllers in patients with mild asthma in 2019, Singapore experienced a rapid and sustained increase in the ratio of asthma controller dispensations to relievers, which was accompanied by a significant decrease in reliever medication dispensations during the COVID-19 pandemic. We found that the increase in the ratio of preventer to reliever dispensations could be associated with a significant reduction in asthma-related urgent and emergent care, both before and during different phases of the COVID-19 pandemic. Guideline-based asthma treatment can be delivered in primary care settings, which is crucial as Singapore is currently focused on transforming its healthcare landscape and shifting patients with (mild) asthma from secondary to primary care. Reinforcing guideline-based asthma management in primary care could lead to a more efficient healthcare paradigm. Future studies should project the impact of guideline-based asthma treatment on the future economic burden of asthma in Singapore under different PRR scenarios, to determine the optimal PRR levels and inform best practices for asthma management in Singapore.
Ethics Approval
This study was approved by the National University of Singapore Institutional Review Board (Reference number: NUS-IRB-2021-967).
The data accessed complied with relevant data protection and privacy regulations.
Consent for Publication
The details of this manuscript submission can be published and the persons providing consent have been shown the article contents to be published.
Authors' Contribution
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the National University of Singapore (NUS) Start-up Grant.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Asthma. Available from: https://www.who.int/news-room/fact-sheets/detail/asthma.
2. Pearce N, Aït-Khaled N, Beasley R, et al. Worldwide trends in the prevalence of asthma symptoms: phase III of the International Study of Asthma and Allergies in Childhood (ISAAC). Thorax. 2007;62(9):758–766. doi:10.1136/thx.2006.070169
3. Beasley R. The burden of asthma with specific reference to the United States. J Allergy Clin Immunol. 2002;109(5, Supplement):S482–9. doi:10.1067/mai.2002.122716
4. National Health Survey 2010: epidemiology & Disease Control Division, Ministry of Health, Singapore. Available from: https://www.moh.gov.sg/resources-statistics/reports/national-health-survey-2010.
5. MOH | news Highlights. Available from: https://www.moh.gov.sg/news-highlights/details/speech-by-a-prof-benjamin-ong-director-of-medical-services-ministry-of-health-at-the-opening-of-the-2nd-international-symposium-on-respiratory-research-and-launch-of-the-academic-respiratory-initiative-on-pulmonary-health-%28tariph%29-19-march-2018.
6. Finkelstein EA, Lau E, Doble B, Ong B, Koh MS. Economic burden of asthma in Singapore. BMJ Open Respir Res. 2021;8(1):e000654. doi:10.1136/bmjresp-2020-000654
7. Global Initiative for Asthma: Global strategy for asthma management and prevention, updated 2022. Available from: https://ginasthma.org.
8. Global Initiative for Asthma: Global strategy for asthma management and prevention, updated 2019. Available from: https://ginasthma.org.
9. Quek JS, Tang WE, Chen E, Smith HE. Understanding the journeys of patients with an asthma exacerbation requiring urgent therapy at a primary care clinic. BMC Pulm Med. 2022;22(1):231. doi:10.1186/s12890-022-02024-9
10. Nebulisers | asthma UK. Asthma + Lung UK. Available from: https://www.asthma.org.uk/advice/nhs-care/emergency-asthma-care/nebulisers/.
11. Haahtela T, Tuomisto LE, Pietinalho A, et al. A 10 year asthma programme in Finland: major change for the better. Thorax. 2006;61(8):663–670. doi:10.1136/thx.2005.055699
12. Suissa S, Ernst P, Benayoun S, Baltzan M, Cai B. Low-Dose Inhaled Corticosteroids and the Prevention of Death from Asthma. N Engl J Med. 2000;343(5):332–336. doi:10.1056/NEJM200008033430504
13. Suissa S, Ernst P, Kezouh A. Regular use of inhaled corticosteroids and the long term prevention of hospitalisation for asthma. Thorax. 2002;57(10):880–884. doi:10.1136/thorax.57.10.880
14. Philip KEJ, Buttery S, Williams P, et al. Impact of COVID-19 on people with asthma: a mixed methods analysis from a UK wide survey. BMJ Open Respir Res. 2022;9(1):e001056. doi:10.1136/bmjresp-2021-001056
15. Agondi RC, Menechino N, Marinho AKBB, Kalil J, Giavina-Bianchi P. Worsening of asthma control after COVID-19. Front Med. 2022;9. doi:10.3389/fmed.2022.882665
16. Torjesen I. Covid-19 will become endemic but with decreased potency over time, scientists believe. BMJ. 2021;372:n494. doi:10.1136/bmj.n494
17. Hartmann-Boyce J, Gunnell J, Drake J, et al. Asthma and COVID-19: review of evidence on risks and management considerations. BMJ Evid-Based Med. 2021;26(4):195. doi:10.1136/bmjebm-2020-111506
18. Ye D, Gates A, Radhakrishnan L, Mirabelli MC, Flanders WD, Sircar K. Changes in asthma emergency department visits in the United States during the COVID-19 pandemic. J Asthma. 2023;1(1):1–7.
19. Davies GA, Alsallakh MA, Sivakumaran S, et al. Impact of COVID-19 lockdown on emergency asthma admissions and deaths: national interrupted time series analyses for Scotland and Wales. Thorax. 2021;76(9):867–873. doi:10.1136/thoraxjnl-2020-216380
20. Shah SA, Quint JK, Nwaru BI, Sheikh A. Impact of COVID-19 national lockdown on asthma exacerbations: interrupted time-series analysis of English primary care data. Thorax. 2021;76(9):860–866. doi:10.1136/thoraxjnl-2020-216512
21. Tan JY, Conceicao EP, Sim XYJ, Wee LEI, Aung MK, Venkatachalam I. Public health measures during COVID-19 pandemic reduced hospital admissions for community respiratory viral infections. J Hosp Infect. 2020;106(2):387–389. doi:10.1016/j.jhin.2020.07.023
22. Kaye L, Theye B, Smeenk I, Gondalia R, Barrett MA, Stempel DA. Changes in medication adherence among patients with asthma and COPD during the COVID-19 pandemic. J Allergy Clin Immunol Pract. 2020;8(7):2384–2385. doi:10.1016/j.jaip.2020.04.053
23. Skene IP, Pfeffer PE. Improved asthma control during the COVID-19 pandemic: are there lessons to be learnt? Thorax. 2021;76(9):852–853. doi:10.1136/thoraxjnl-2021-216930
24. Lee TA, Chang CL, Stephenson JJ, et al. Impact of asthma controller medications on medical and economic resource utilization in adult asthma patients. Curr Med Res Opin. 2010;26(12):2851–2860. doi:10.1185/03007995.2010.531255
25. Choi NK, Shantakumar S, Kim MS, et al. Real-world treatment patterns, outcomes, and healthcare resource utilization in newly treated Korean patients with asthma: a retrospective cohort study. Allergy Asthma Immunol Res. 2022;14(2):220–232. doi:10.4168/aair.2022.14.2.220
26. Available from: https://www.healthiersg.gov.sg/resources/white-paper/
27. A Member of NUHS | National University Hospital (NUH), Singapore’s Leading Tertiary Hospital. Available from: https://www.nuh.com.sg/About-NUH/Pages/A-Member-of-NUHS.aspx.
28. MOH | news Highlights. Available from: https:/www.moh.gov.sg/news-highlights/details/confirmed-imported-case-of-novel-coronavirus-infection-in-singapore-multi-ministry-taskforce-ramps-up-precautionary-measures.
29. MOH | news Highlights. Available from: https://www.moh.gov.sg/news-highlights/details/end-of-circuit-breaker-phased-approach-to-resuming-activities-safely.
30. Austin PC, Urbach DR. Using G-computation to estimate the effect of regionalization of surgical services on the absolute reduction in the occurrence of adverse patient outcomes. Med Care. 2013;51(9):797–805. doi:10.1097/MLR.0b013e31829a4fb4
31. Aizhen J Adherence to and efficacy of an evidence based management algorithm for acute asthma in the emergency department. Available from: https://core.ac.uk/download/pdf/48625358.pdf.
32. Wang H, Djajalaksana S, Sharma L, et al. Evaluation of short-acting β2-agonist prescriptions and associated clinical outcomes: findings from the SABA use IN Asthma (SABINA) study in Asia. Jurnal Respirol Indonesia. 2022;42(2):121
33. Williams LK, Pladevall M, Xi H, et al. Relationship between adherence to inhaled corticosteroids and poor outcomes among adults with asthma. J Allergy Clin Immunol. 2004;114(6):1288–1293. doi:10.1016/j.jaci.2004.09.028
34. Bloom CI, Cabrera C, Arnetorp S, et al. Asthma-related health outcomes associated with short-acting β2-agonist inhaler use: an observational UK study as part of the SABINA Global Program. Adv Ther. 2020;37(10):4190–4208. doi:10.1007/s12325-020-01444-5
35. Kinley E, Skene I, Steed E, Pinnock H, McClatchey K. Delivery of supported self‐management in remote asthma reviews: a systematic rapid realist review. Health Expect Int J Public Particip Health Care Health Policy. 2022;25(4):1200–1214.
36. Healthier SG: white Paper on Healthier SG. Available from: https://www.healthiersg.gov.sg/resources/white-paper/.
37. Singapore National Asthma Programme (SNAP). Available from: https://www.primarycarepages.sg/patient-care/chronic-disease-management/singapore-national-asthma-programme-(snap).
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.