")
Back to Journals » Patient Preference and Adherence » Volume 18
Impact of COVID-19 Pandemic on Routine Childhood Immunization Programs in Indonesia: Taking Rural and Urban Area into Account
Authors Rahayuningsih N, Sinuraya RK , Fatinah Y, Diantini A , Suwantika AA
Received 8 November 2023
Accepted for publication 1 March 2024
Published 13 March 2024 Volume 2024:18 Pages 667—675
DOI https://doi.org/10.2147/PPA.S448901
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Nur Rahayuningsih,1,2 Rano K Sinuraya,1,3,4 Yasmin Fatinah,1 Ajeng Diantini,1,4 Auliya A Suwantika1,4,5
1Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Sumedang, Indonesia; 2Faculty of Pharmacy, Universitas Bakti Tunas Husada, Tasikmalaya, Indonesia; 3Unit of Global Health, Department of Health Sciences, University of Groningen, University Medical Center Groningen, Groningen, the Netherlands; 4Center of Excellence for Pharmaceutical Care Innovation, Universitas Padjadjaran, Sumedang, Indonesia; 5Center for Health Technology Assessment, Universitas Padjadjaran, Sumedang, Indonesia
Correspondence: Rano K Sinuraya, Email [email protected]; [email protected]
Background: To date, the primary global concern has revolved around addressing the COVID-19 pandemic. However, there is a growing awareness of the pandemic’s secondary impacts on critical aspects of healthcare, such as childhood immunization programs.
Objective: This study aims to assess the impact of the COVID-19 pandemic on childhood immunization programs in Indonesia, with a specific focus on performance disparities between rural and urban areas. It considers factors like access, utilization, and program workload.
Methods: Data were collected from primary health cares (PHCs) in two regions in West Java Province, Indonesia, representing rural and urban areas. A descriptive analysis was conducted to compare vaccination coverage, drop-out rates, and the ratio of vaccinators per dose from 2019 to 2021 in 40 and 22 PHCs for rural and urban areas, respectively. A general linear model was employed to evaluate the differences in these parameters over the three consecutive years.
Results: The results indicate fluctuations in vaccine coverage over the three years, with the most significant impact observed in 2020, particularly in rural areas. Statistical analysis revealed a significant difference in routine immunization coverage, drop-out rates, and vaccinator ratios between rural and urban areas from 2019 to 2021 (p< 0.05). In 2021, both rural and urban areas displayed significant differences in performance parameters for routine immunization and COVID-19 vaccination (p< 0.05), except in terms of coverage for IPV and COVID-19 vaccination.
Conclusion: The study highlights a reduction in routine immunization coverage during the pandemic, a concerning issue that increases the risk of vaccine-preventable diseases, particularly in rural areas.
Keywords: immunization coverage, dropout rate, workload, primary healthcare centers
Introduction
The SARS-CoV-2 virus, which causes COVID-19, is primarily transmitted through airborne particles and droplets released from an infected person’s mouth or nose during activities like coughing, sneezing, speaking, singing, or breathing.1 These particles can carry the virus and infect others, particularly in confined spaces with poor ventilation.1,2 The virus primarily spreads through close contact, and there is a risk of airborne transmission when infectious droplets are inhaled or come into contact with the eyes, nose, or mouth.1–3 To mitigate this risk, it is crucial to enhance indoor air quality and ventilation. Recommended preventive measures include vaccination, social distancing, and maintaining high personal hygiene standards.2
However, to date, extensive research and development efforts have been undertaken to combat COVID-19. This includes the application of artificial intelligence, which has the potential to revolutionize travel medicine by providing accurate, tailored, and up-to-date health information to both travelers and healthcare providers.4 Furthermore, continuous advancements in the development of COVID-19 vaccines, utilizing mRNA, heterologous prime-boost vaccine regimens, and nanovaccines, aim to improve the stability of vaccine components, enhance the immune response, and enable precise delivery to specific cells.5–8
The global impact of the COVID-19 pandemic has had profound consequences for healthcare systems and public health programs worldwide.9 While the primary focus understandably revolves around addressing the unique challenges posed by the coronavirus, there is an increasing recognition of the pandemic’s secondary impacts on critical aspects of healthcare, including routine childhood immunization programs.10 In March 2020, Indonesia reported its first case of COVID-19, and the pandemic has significantly disrupted routine immunization programs.10,11 Most healthcare facilities have experienced interruptions in their regular services as resources were redirected to prioritize COVID-19 treatment and prevention efforts.12 Data reveals a concerning trend: vaccination coverage for measles, rubella, diphtheria, pertussis, and tetanus has dropped by up to 35% in Indonesia compared to the previous year.13
Traditionally, immunization programs have been the cornerstone of public health, substantially reducing the burden of vaccine-preventable diseases among children.14 However, the disruptions these programs have encountered could potentially reverse decades of progress, raising concerns about the resurgence of preventable diseases and the health risks faced by millions of Indonesian children.10,15
Despite the decline in routine immunization due to the pandemic, the availability of both routine and COVID-19 vaccines in healthcare services, especially in primary healthcare, could become a significant issue due to the lack of cold storage.16 Additionally, the availability of vaccinators may present a challenge in various healthcare settings, both in urban and rural areas.17,18 This study aims to shed light on the repercussions of the COVID-19 pandemic on Indonesia’s childhood immunization programs, with a particular emphasis on performance disparities in rural and urban locales, taking into account factors such as access, utilization, and the workload of the vaccination program. This research could contribute to exploring disparities and evaluating implications for public health policy and planning in the post-pandemic era.
Methods
This study focuses on West Java, Indonesia’s most populous province, and employs two districts to represent both urban and rural areas. These districts are equipped with 33 and 47 primary healthcare units (PHCs) for urban and rural regions, adhering to the standard ratio of one PHC for every 1000 individuals. Our data collection involved gathering information from 22 PHCs in urban areas and 40 PHCs in rural areas. This data includes details such as the target population of infants under one year old, the doses of administered vaccines, which encompass Bacillus Calmette-Guérin (BCG), Hepatitis B (Hep-B), Pentavalent (Diphtheria, Pertussis, Tetanus, Hepatitis B, and Hib), Polio (OPV/Oral Poliovirus Vaccines), Measles-Rubella (MR), Inactivated Polio Vaccine (IPV), and COVID-19 vaccines. We also collected data on the number of vaccinators and the hours of vaccination services provided at each public health center.
To assess the impact of the COVID-19 pandemic on routine childhood immunization programs, we conducted an assessment spanning from 2019 to 2021, taking into account the introduction of the COVID-19 vaccination program in 2021. Our evaluation focused on three key parameters: access, utilization, and workload within the vaccination program. These parameters were evaluated through immunization coverage, drop-out rates, and the ratio of administered doses per vaccinator. Immunization coverage assessed access, drop-out rates measured utilization, and the ratio of administered doses per vaccination determined workload.
Immunization coverage was calculated by considering the number of administered doses in relation to the target population. Drop-out rates were derived by comparing the number of infants who began the immunization schedule with those who successfully completed it. The ratio of administered doses per vaccinator was established by dividing the number of doses administered daily by the count of trained vaccinators.
We conducted a descriptive analysis to compare three key parameters: coverage, drop-out rates, and the ratio of vaccinators. To assess the differences in these parameters in 2021 and their association with the COVID-19 vaccination program, we conducted an ANOVA test. Furthermore, a general linear model was employed to investigate variations in these parameters over the course of three consecutive years. The significance threshold for all analyses was set at p < 0.05.
Furthermore, we conducted a descriptive gap analysis to understand the disparities in access, utilization, and workload both before and during the COVID-19 pandemic. We categorized these parameters based on specific thresholds in line with WHO guidelines.19 For access and utilization, we considered an immunization coverage of 70% as the threshold, where less than 70% denoted poor access and over 70% signified good access. Similarly, a drop-out rate of 10% served as the threshold, with over 10% indicating poor utilization and less than 10% indicating good utilization.
Regarding workload, a ratio of administered doses per vaccinator at 30:1 was the threshold, with over 30:1 indicating poor workload and below 30:1 indicating good workload. However, for the COVID-19 vaccination program, we applied a different threshold for the ratio of administered doses per vaccinator, setting it at 70:1, with over 70:1 indicating poor workload and below 70:1 indicating good workload. All statistical analyses were carried out using the Statistical Package for Social Sciences (SPSS) 27 software provided by SPSS Inc. in Chicago, IL, United States.
Results
The selected areas have populations of 716,155 and 1,865,203 for the rural and urban areas, respectively. Each area covers immunization for a range of 100–1500 and 200–1000 infants in the rural and urban areas, respectively. In terms of COVID-19 cases, the rural area reported 6663 cases, while the urban area reported 11,937 cases.
The analysis of vaccine data across various vaccine types in rural and urban regions for the years 2019, 2020, and 2021 reveals some noteworthy trends (see Table 1). Notably, the BCG vaccine experienced a decrease in rural coverage, dropping from 95.46% in 2019 to 88.59% in 2021, alongside a significant rise in dropout rates. In contrast, urban areas saw a modest increase in BCG vaccine coverage, but the rate of individuals discontinuing immunization remained relatively stable The ratios of vaccinators to doses remained consistent in both rural and urban settings. Similarly, the polio vaccine displayed a consistent pattern of immunization coverage and dropout rates across both rural and urban areas over the specified timeframe.
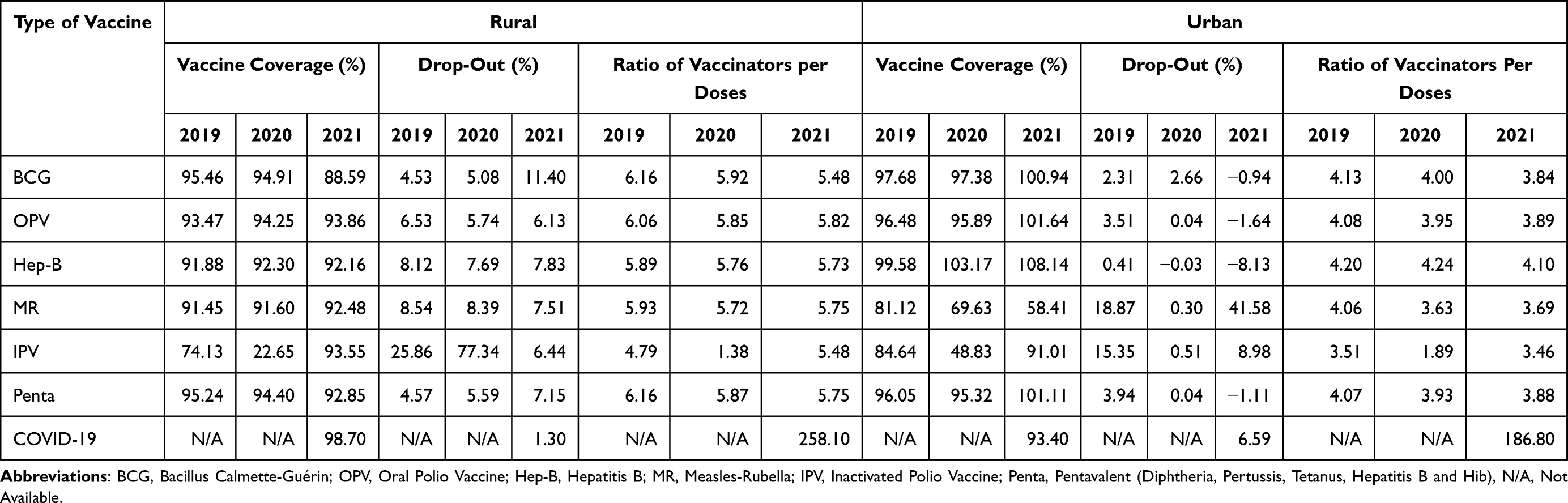 |
Table 1 Mean Comparison of the Routine Vaccination Program |
Shifting to MR vaccination, rural coverage exhibited a slight increase, rising from 91.45% in 2019 to 92.48% in 2021. In contrast, urban regions experienced a notable decline, falling from 81.12% to 58.41%, accompanied by a significant rise in dropout rates. The IPV vaccine coverage demonstrated significant fluctuations, dropping to 22.65% in rural areas in 2020, followed by a subsequent increase to 93.55% in 2021. Urban areas showed a similar trend, with a decline to 48.83% in 2020, followed by a recovery to 91.01% in 2021. The pentavalent vaccine consistently maintained its coverage and dropout rates in both rural and urban contexts. In 2021, the analysis of COVID-19 vaccination data highlighted a significant urban coverage rate of 98.70% with a ratio of vaccinators per dose of 258.10.
A comparative analysis conducted in 2021 aimed to examine routine immunization and COVID-19 vaccination, specifically focusing on vaccine type, coverage, drop-out rates, and the ratio of vaccinators to doses in both rural and urban settings (Table 2). The findings revealed that urban regions consistently exhibited significantly higher coverage and lower drop-out rates for BCG, Polio, Hepatitis B, MR, IPV, and Penta vaccinations. Furthermore, urban areas displayed a significantly higher ratio of vaccinators to doses for these vaccines.
 |
Table 2 Average Differences Between Routine Vaccination Programs and COVID-19 Vaccination Initiatives in Rural and Urban Regions |
Conversely, in the case of the COVID-19 vaccination in 2021, higher coverage was observed in urban regions, although this disparity did not yield statistically significant results. Notably, there was no substantial difference in the drop-out rates for COVID-19 vaccination between rural and urban areas. However, a significant variation was observed in the ratio of vaccinators to doses for COVID-19 vaccination between rural and urban areas.
A repeated measurement was performed to analyze the differences in coverage, drop-out rates, and the ratio of vaccinators in routine immunization from 2019 to 2021 using a general linear model. The results showed significant differences in these three variables with p<0.05 between urban and rural areas (Figure 1).
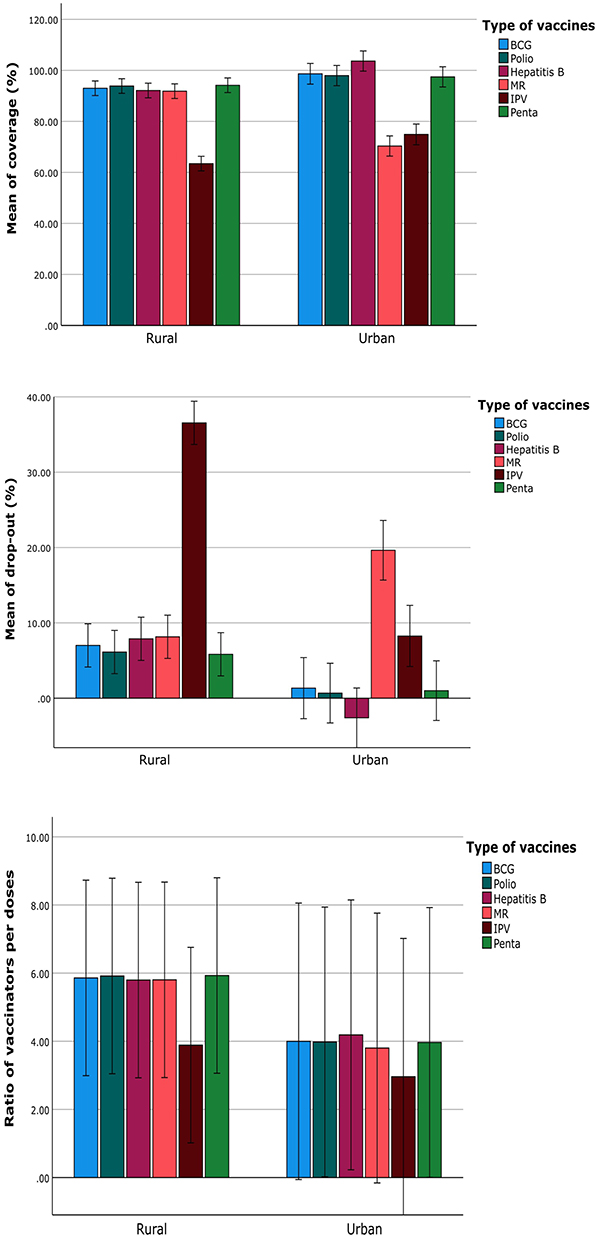 |
Figure 1 Significant mean differences in repeated measurements between rural and urban areas from 2019 to 2021 (p < 0.05). |
Then, we converted the vaccination coverage, drop-out rates, and ratio of vaccinators per dose into accessibility, utilization, and workload based on the Ministry of Health guidelines (Figure 2). The results indicated that, in terms of accessibility, COVID-19 immunization demonstrated nearly universal reach in rural regions, achieving a 100% coverage rate. In contrast, urban areas maintained relatively stable accessibility levels, consistently hovering around 86–87%. Conversely, routine immunization consistently exhibited better accessibility in rural areas.
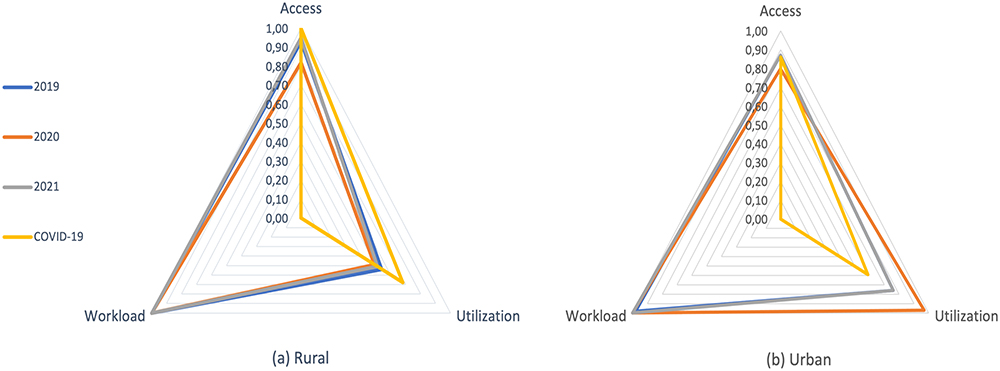 |
Figure 2 Access, utilization, and workload score of PHCs between (a) rural and (b) urban area. |
Utilization rates for COVID-19 vaccination were found to be higher in rural areas compared to urban areas, with respective rates of 0.68 and 0.59. However, routine immunization consistently favored urban areas in terms of utilization. Both rural and urban areas displayed consistent patterns regarding the workload associated with routine vaccination for both programs. Nevertheless, COVID-19 immunization efforts in both regions showed a significant deficiency in terms of workload management.
Discussion
This study focuses on the performance of routine vaccination before and during the COVID-19 pandemic. The results indicate fluctuations in vaccination coverage and drop-out rates from 2019 to 2021. However, there was an improvement in 2021 when the COVID-19 vaccine was introduced. One significant challenge for the COVID-19 vaccine is the ratio of vaccinators per dose administered, as this vaccine targets a broader population spanning all age groups.
The COVID-19 pandemic has drawn attention to concerns about the accessibility of routine immunization services.20 According to a previous study, at least 80 million children under the age of one are at risk of diseases like diphtheria, measles, and polio due to disruptions in routine vaccination caused by COVID-19.21 Vaccine coverage declined in all regions, with the East Asia and Pacific region experiencing the most significant drop in DTP3 coverage, decreasing by nine percentage points in just two years.22 Additionally, a study conducted in India found that immunization coverage was lower in COVID-affected children compared to unaffected children, ranging from a 2% decrease for BCG and hepB0 to a 9% decrease for the measles-containing vaccine 1 (MCV1).23
Our study findings indeed show a decrease in coverage, which is correlated with an increase in drop-out rates in routine immunization, with a significant difference over three consecutive years between rural and urban areas. The challenges in rural areas are particularly evident due to limited healthcare infrastructure.24 Individuals living in geographically isolated areas face difficulties accessing vaccination centers, primarily due to the reduced availability of public transportation services and the significant distances separating them from healthcare facilities.24,25 On the other hand, urban regions derive advantages from enhanced accessibility to immunization services, owing to the presence of more concentrated healthcare facilities and improved transportation systems.24 The increased availability of vaccination locations in urban areas has the potential to positively impact vaccine coverage rates.
Moreover, the shortage of vaccinators has disrupted immunization services, leading to clinic closures and the suspension of outreach services.26 This has made it challenging for people to access immunization services, resulting in a decline in immunization rates.26,27 Our study reveals a higher ratio of vaccinators per dose in rural areas compared to urban areas for COVID-19 vaccination. This is primarily because there are fewer healthcare workers available to administer vaccines, especially considering that COVID-19 vaccines are administered to people of all age groups. Similar to a previous study in Colombia,28 the pandemic’s impact on the shortage of human resources, including vaccinators, has affected routine immunization coverage, with rural populations being the most affected.
Several factors must be considered as determinants for the declining performance of routine vaccination programs during the pandemic.29 These factors include disruptions in the supply chain, lockdown measures, and reduced availability of medical staff, which led to the temporary suspension of vaccination services at the peak of the COVID-19 pandemic.20,29 Consequently, this suspension has contributed to the recent decline in routine immunization coverage.
Furthermore, Indonesia’s healthcare system encountered difficulties such as strained resources, limited healthcare infrastructure, and disparities across different regions, influencing the country’s COVID-19 response.30 The integration of COVID-19 and routine childhood vaccination resulted in more children receiving routine immunizations, but it was not without challenges, as reports of vaccine refusals surfaced.31 In addition, a study analyzed the declining coverage of the co-production system in Posyandu health services during the COVID-19 pandemic, potentially affecting routine childhood immunization programs.32
Moreover, vaccine hesitancy can also be identified as a significant reason for the low uptake of vaccinations.33 While a previous study indicated that parents had good knowledge, attitude, and practice during the COVID-19 pandemic,34 according to the Ministry of Health, half of the parents and caregivers surveyed expressed hesitancy in bringing their children to healthcare facilities due to concerns about COVID-19 transmission and a lack of proper safety precautions.35 The complex and unpredictable nature of the COVID-19 infection may have contributed to negative perceptions and reluctance toward other essential healthcare services, including immunization services.
The Indonesian Ministry of Health has implemented three strategies to enhance routine immunization coverage, underpinned by collaborative efforts across ministries, agencies, and sectors to reach children who may have missed immunization in previous years.36 These collective endeavors are crucial for surmounting barriers to immunization services in rural areas and ensuring the continuity of routine immunization programs, even amid a pandemic. Therefore, it remains essential for countries to continually monitor immunization program coverage and disease outbreaks at both the national and subnational levels. Alongside this, conducting catch-up vaccination activities is paramount to reducing the risk of vaccine-preventable disease outbreaks, all while ensuring an adequate supply of vaccines and healthcare personnel to maintain routine immunization programs in rural regions.
This study has several limitations. One significant constraint is that our data collection was confined to primary healthcare facilities, excluding information from private healthcare services. This limitation could potentially introduce bias into our findings. Therefore, our study might only offer a partial perspective on the ever-evolving impact of the pandemic on vaccination efforts without delving deeply into the unique challenges encountered in both urban and rural areas. Additionally, we narrowed the focus of this study to vaccination coverage, dropout rates, and workload. Despite this, these variables remain essential when conducting a gap analysis between the standard immunization program and the COVID-19 vaccination program.
However, our study also boasts notable strengths. For example, it is the first of its kind in the nation, and its results will swiftly illustrate to relevant stakeholders the pandemic’s effects on the immunization program in both urban and rural areas. These results can serve as a valuable baseline for monitoring the impact of future public health crises or vaccination campaigns on routine childhood immunization in Indonesia. Furthermore, the utilization of data from public health facilities mirrors real-world healthcare settings, providing valuable insights into the actual experiences and challenges faced by healthcare providers and recipients during the pandemic. These strengths enhance the credibility and practical relevance of our study.
Conclusion
There are disruptions to the routine immunization program during the COVID-19 pandemic, with greater impact in rural areas. Monitoring immunization program coverage and disease outbreaks at both the national and subnational levels is of utmost importance for countries to mitigate the potential occurrence of vaccine-preventable disease outbreaks.
Data Sharing Statement
The raw data supporting the conclusions of this article can be accessed through the corresponding author upon reasonable request.
Ethical Approval
The study obtained ethical clearance from the Health Research Ethics Committee of Universitas Padjadjaran, Indonesia (registration number: 1140/UN6.KEP/EC/2023).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was funded by Universitas Padjadjaran through AAS, under grant number 2203/UN6.3.1/PT.00/2023.
Disclosure
The authors declare that they have no competing interest in this work.
References
1. Zhao X, Liu S, Yin Y, Zhang TT, Chen Q. Airborne transmission of COVID-19 virus in enclosed spaces: an overview of research methods. Indoor Air. 2022;32(6):e13056. doi:10.1111/ina.13056
2. World Health Organization. Coronavirus disease (COVID-19): how is it transmitted?; 2021. Available from: https://www.who.int/news-room/questions-and-answers/item/coronavirus-disease-covid-19-how-is-it-transmitted.
3. Priyanka Choudhary OP, Singh I, Patra G, Patra G. Aerosol transmission of SARS-CoV-2: the unresolved paradox. Travel Med Infect Dis. 2020;37:101869. doi:10.1016/j.tmaid.2020.101869
4. Choudhary OP. ChatGPT in travel medicine: a friend or foe? Travel Med Infect Dis. 2023;54:102615. doi:10.1016/j.tmaid.2023.102615
5. Priyanka Chopra H, Choudhary OP, Choudhary OP. mRNA vaccines as an armor to combat the infectious diseases. Travel Med Infect Dis. 2023;52:102550. doi:10.1016/j.tmaid.2023.102550
6. Ahmed JQ, Maulud SQ, Dhawan M, et al. MicroRNAs in the development of potential therapeutic targets against COVID-19: a narrative review. J Infect Public Health. 2022;15(7):788–799. doi:10.1016/j.jiph.2022.06.012
7. Choudhary OP, Priyanka Ahmed JQ, Mohammed TA, Singh I, Rodriguez-Morales AJ, Rodriguez-Morales AJ. Heterologous prime-boost vaccination against COVID-19: is it safe and reliable? Hum Vaccin Immunother. 2021;17(12):5135–5138. doi:10.1080/21645515.2021.2007015
8. Priyanka Abusalah MAH, Chopra H. Nanovaccines: a game changing approach in the fight against infectious diseases. Biomed Pharmacother. 2023;167:115597.
9. Haileamlak A. The impact of COVID-19 on health and health systems. Ethiop J Health Sci. 2021;31(6):1073–1074. doi:10.4314/ejhs.v31i6.1
10. World Health Organization. COVID-19 pandemic leads to major backsliding on childhood vaccinations, new WHO, UNICEF data shows; 2021. Available from: https://www.who.int/news/item/15-07-2021-covid-19-pandemic-leads-to-major-backsliding-on-childhood-vaccinations-new-who-unicef-data-shows.
11. Portal Informasi Indonesia. Kasus COVID-19 pertama, masyarakat jangan panik; 2020. Available from: https://indonesia.go.id/narasi/indonesia-dalam-angka/ekonomi/kasus-covid-19-pertama-masyarakat-jangan-panik.
12. Núñez A, Sreeganga SD, Ramaprasad A. Access to Healthcare during COVID-19. Int J Environ Res Public Health. 2021;18(6):2980. doi:10.3390/ijerph18062980
13. Suwantika AA, Boersma C, Postma MJ. The potential impact of COVID-19 pandemic on the immunization performance in Indonesia. Expert Rev Vaccines. 2020;19(8):687–690. doi:10.1080/14760584.2020.1800461
14. Rémy V, Zöllner Y, Heckmann U. Vaccination: the cornerstone of an efficient healthcare system. J Mark Access Health Pol. 2015;2:3.
15. Bigouette JP, Callaghan AW, Donadel M, et al. Effects of COVID-19 on vaccine-preventable disease surveillance systems in the World Health Organization African Region, 2020. Emerg Infect Dis. 2022;28(13):S203–S207. doi:10.3201/eid2813.220088
16. Alam ST, Ahmed S, Ali SM, Sarker S, Kabir G, Ul-Islam A. Challenges to COVID-19 vaccine supply chain: implications for sustainable development goals. Int J Prod Econ. 2021;239:108193. doi:10.1016/j.ijpe.2021.108193
17. Gibson E, Zameer M, Alban R, Kouwanou LM. Community Health Workers as Vaccinators: a Rapid Review of the Global Landscape, 2000–2021. Glob Health Sci Pract. 2023;11(1):e2200307. doi:10.9745/GHSP-D-22-00307
18. Kuehn M, LaMori J, DeMartino JK, et al. Assessing barriers to access and equity for COVID-19 vaccination in the US. BMC Public Health. 2022;22(1):2263. doi:10.1186/s12889-022-14636-1
19. World Health Organization. Microplanning for immunization service delivery using the Reaching Every District (RED) strategy; 2009. Available from: https://www.who.int/publications/i/item/microplanning-for-immunization-service-delivery-using-the-reaching-every-district-(-red)-strategy.
20. Lassi ZS, Naseem R, Salam RA, Siddiqui F, Das JK. The impact of the COVID-19 pandemic on immunization campaigns and programs: a systematic review. Int J Environ Res Public Health. 2021;18(3):988. doi:10.3390/ijerph18030988
21. Shet A, Carr K, Danovaro-Holliday MC, et al. Impact of the SARS-CoV-2 pandemic on routine immunisation services: evidence of disruption and recovery from 170 countries and territories. Lancet Glob Health. 2022;10(2):e186–e194. doi:10.1016/S2214-109X(21)00512-X
22. World Health Organization. COVID-19 Pandemic Fuels Largest Continued Backslide in Vaccinations in Three Decades. World Health Organization; 2022.
23. Summan A, Nandi A, Shet A, Laxminarayan R. The effect of the COVID-19 pandemic on routine childhood immunization coverage and timeliness in India: retrospective analysis of the National Family Health Survey of 2019–2021 data. Lancet Reg Health Southeast Asia. 2023;8:100099. doi:10.1016/j.lansea.2022.100099
24. Albers AN, Thaker J, Newcomer SR. Barriers to and facilitators of early childhood immunization in rural areas of the United States: a systematic review of the literature. Prev Med Rep. 2022;27:101804. doi:10.1016/j.pmedr.2022.101804
25. Rosen B, Waitzberg R, Israeli A, Hartal M, Davidovitch N. Addressing vaccine hesitancy and access barriers to achieve persistent progress in Israel’s COVID-19 vaccination program. Israel J Health Policy Res. 2021;10(1):43. doi:10.1186/s13584-021-00481-x
26. Fiorillo S. Has the COVID-19 pandemic disrupted routine immunization services?; 2022.
27. Cardoso Pinto AM, Ranasinghe L, Dodd PJ, Budhathoki SS, Seddon JA, Whittaker E. Disruptions to routine childhood vaccinations in low- and middle-income countries during the COVID-19 pandemic: a systematic review. Front Pediatr. 2022;10:979769. doi:10.3389/fped.2022.979769
28. Moreno-Montoya J, Ballesteros SM, Sotelo JCR, Cervera CLB, Barrera-López P, Hoz-Valle J. Impact of the COVID-19 pandemic on routine childhood immunisation in Colombia. Arch Dischildhood. 2022;107(3):e4–e4. doi:10.1136/archdischild-2021-321792
29. Cardoso Pinto AM, Shariq S, Ranasinghe L, et al. Reasons for reductions in routine childhood immunisation uptake during the COVID-19 pandemic in low- and middle-income countries: a systematic review. PLOS Global Public Health. 2023;3(1):e0001415. doi:10.1371/journal.pgph.0001415
30. Harapan BN, Harapan T, Theodora L, Anantama NA. From archipelago to pandemic battleground: unveiling Indonesia’s COVID-19 Crisis. J Epidemiol Glob Health. 2023;13(4):591–603. doi:10.1007/s44197-023-00148-7
31. Mokaya EN, Atem NA, Awzenio G, et al. Lessons From the COVID-19 pandemic response implementation: a case study of South Sudan and Sierra Leone. Global Health. 2023;2:1.
32. Al Farizi S, Harmawan BN. Decreasing coverage of co-production based on maternal and child health services (Posyandu) during the COVID-19 pandemic in Indonesia. Cogent Soc Sci. 2023;9(2):2267743. doi:10.1080/23311886.2023.2267743
33. Kumar D, Chandra R, Mathur M, Samdariya S, Kapoor N. Vaccine hesitancy: understanding better to address better. Israel J Health Policy Res. 2016;5(1):2. doi:10.1186/s13584-016-0062-y
34. Sinuraya RK, Kusuma ASW, Pardoel ZE, Postma MJ, Suwantika AA. Parents’ Knowledge, Attitude, and practice on childhood vaccination during the COVID-19 pandemic in Indonesia. Patient Prefer Adherence. 2022;16:105–112. doi:10.2147/PPA.S339876
35. Ministry of Health of Indonesia, NITAG, UNICEF, WHO. COVID-19 Vaccine Acceptance Survey in Indonesia; 2020. Available from: https://www.unicef.org/indonesia/media/7631/file/COVID-19%20Vaccine%20Acceptance%20Survey%20in%20Indonesia.pdf.
36. World Health Organization. Indonesia Targets Low Vaccination Areas to Tackle Decline in Childhood Immunization. World Health Organization; 2023.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.