")
Back to Journals » Blood and Lymphatic Cancer: Targets and Therapy » Volume 9
IDH1-mutated relapsed or refractory AML: current challenges and future prospects
Authors Megías-Vericat JE , Ballesta-López O , Barragán E, Montesinos P
Received 29 January 2019
Accepted for publication 7 May 2019
Published 27 June 2019 Volume 2019:9 Pages 19—32
DOI https://doi.org/10.2147/BLCTT.S177913
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor David Dingli
Juan Eduardo Megías-Vericat,1 Octavio Ballesta-López,1 Eva Barragán,2,3 Pau Montesinos2,3
1Servicio de Farmacia, Área del Medicamento, Hospital Universitari i Politècnic La Fe, Valencia, Spain; 2Servicio de Hematología y Hemoterapia, Hospital Universitari i Politècnic La Fe, Valencia, Spain; 3CIBERONC, Instituto Carlos III, Madrid, Spain
Abstract: The prognosis of patients with relapsed or refractory acute myeloid leukemia (R/R AML) is discouraging with salvage standard approaches. Mutations of isocitrate dehydrogenase 1 (IDH1mut,), present in 7–14% of AML patients, have been discovered recently, opening the door to targeted agents aiming to improve the outcomes in this setting. Several oral selective IDH1mut, inhibitors are under investigation, ivosidenib being the first approved for R/R AML. We performed a systematic review to analyze the clinical outcomes and safety reported with IDH1mut, inhibitors and other agents in adult patients with IDH1mut, R/R AML. Ivosidenib in monotherapy achieved complete remission (CR) of 24%, overall response of 42%, and median overall survival of 9 months in R/R AML, and promising outcomes were reported with IDH305 and FT-2102. IDH1mut, inhibitors were generally well tolerated, but some therapy-related toxicities should be monitored, including IDH-differentiation syndrome, prolongation of the QT interval, and leukocytosis, all manageable and reversible. Also, venetoclax, CB-839, PARP inhibitors, and IDH1 peptide vaccine are being studied in IDH1mut, AML. The results of the ongoing and upcoming clinical trials will bring new evidence to establish the role of IDH1mut, inhibitors in therapeutic strategies of AML.
Keywords: isocitrate dehydrogenase 1, acute myeloid leukemia, relapsed/refractory, ivosidenib, FT-2102, venetoclax
Introduction
Despite improvements in chemotherapy over the last years, the majority of adult patients with acute myeloid leukemia (AML) will show primary refractory disease or relapse after achieving complete remission (CR).1 The prognosis of relapsed/refractory (R/R) AML patients is particularly poor, but in a subset of patients salvage therapy followed by allogeneic hematopoietic stem cell transplantation (alloHSCT) was shown to be possibly curative.2
Whole-genome sequencing of AML has revealed some acquired mutations in such genes as isocitrate dehydrogenase 1 (IDH1) or 2 (IDH2) genes, encoding for two enzymes that catalyze the conversion of isocitrate to α-ketoglutarate (αKG) and reduce nicotinamide adenine dinucleotide phosphate (NADP+) to NADPH. In mutated IDH1 (IDH1mut) and IDH2 (IDH2mut), NADPH is oxidized to NADP+ and αKG transformed into the oncometabolite D-2-hydroxyglutarate (2HG). When levels of 2HG are increased, they interfere with cellular metabolism and epigenetic regulation and hence contribute to leukemogenesis. Somatic mutations of IDH1 and IDH2 genes are found in 7–14% and 8–19% of AML cases, respectively.3,4
The recent discovery of new mutations in AML has opened the door to targeted agents that are actually in use or under investigation. This is the case for IDH1mut and IDH2mut inhibitors for patients with IDH mutations. Enasidenib was the first inhibitor of IDH2 to be approved by the US Food and Drug Administration (FDA) in August 2017 for R/R AML that carries IDH2mut. More recently, in July 2018, ivosidenib which inhibits mutated cytosolic IDH1 was also approved for R/R AML. Following this path, there are other IDH1mut and IDH2mut inhibitors and their combinations with other therapies under investigation (ie, intensive chemotherapy and hypomethylating agents).5 Our aim was to perform a systematic review of the literature and to analyze the clinical outcomes reported with IDH1mut inhibitors and other agents in adult patients with IDH1mut R/R AML.
Materials and methods
Search strategy and selection of studies
In accordance with the PRISMA guidelines, two independent reviewers (JMV and PM) conducted this systematic review.6 The following databases were searched without restrictions: Pubmed, EMBASE, the Cochrane Central Register, the ProQuest Medical Library, the EBSCOhost Online Research Databases, the Web of Science, and the Database of Abstracts of Reviews of Effects (DARE). In addition, the reference lists of important studies and reviews were hand-searched. Available abstracts and oral communications from conferences of the American Society of Hematology, the American Society of Clinical Oncology, and the European Hematology Association were also reviewed. Reference lists of relevant reviews and studies were searched manually. The last literature search was on November 12, 2018.
Similar keywords were used in different databases: “isocitrate dehydrogenase inhibitor 1” or “inhibitor of mutant isocitrate dehydrogenase 1” or “IDH1 mutated” and “acute myeloid leukemia” [Mesh] and relapse or refractory or resistance or recurrence or recrudescence or “salvage therapy” or “salvage treatment”.
The study selection was conducted by both authors independently. In cases of disagreement, a third reviewer (EB) adjudicated. Inclusion criteria were studies using IDH1mut inhibitors in IDH1mut adult AML patients, especially in the subset of R/R AML, studies evaluating effectiveness and/or safety of IDH1mut inhibitors in IDH1mut R/R AML, with at least CR rate or overall survival (OS), studies analyzing combinations of IDH1mut inhibitors with other agents in R/R AML, and studies analyzing untargeted therapies that might be employed in the treatment of IDH1mut R/R AML.
Our systematic search obtained 59 citations from databases and journals, and 19 records were identified through other sources (Figure 1). Of the 78 citations selected for full reading, 46 fulfilled the inclusion criteria and 22 were included. Agreement on study selection among the reviewers was excellent (kappa =0.97).
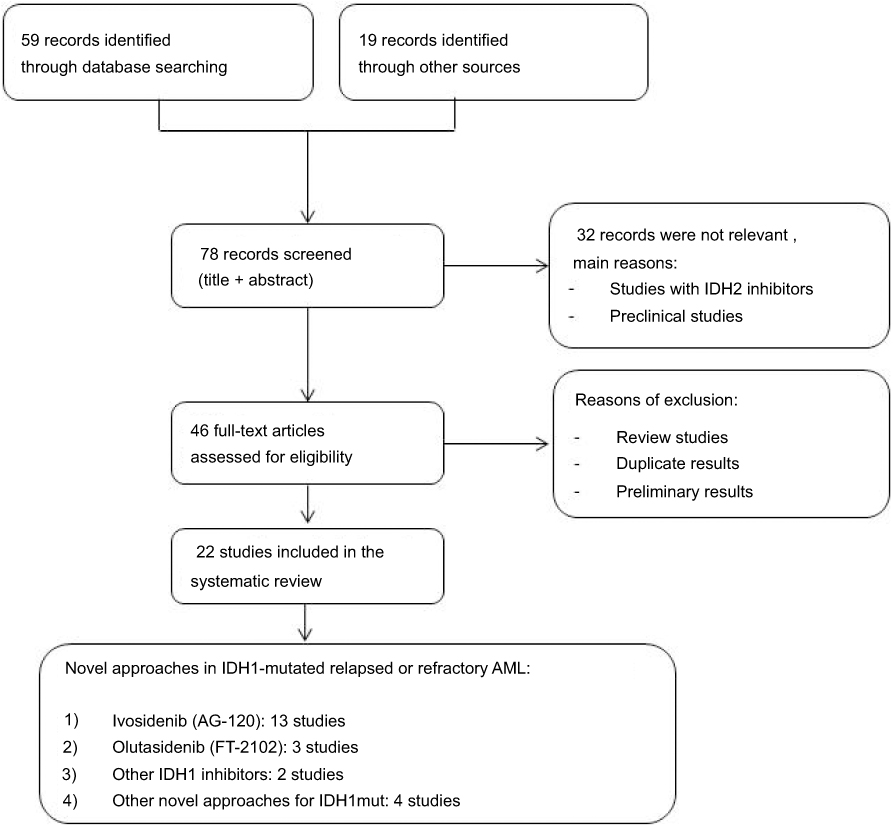 |
Figure 1 Summary of evidence search and selection. Abbreviations: AML, acute myeloid leukemia; IDH1, isocitrate dehydrogenase 1; IDH2, isocitrate dehydrogenase 2; IDH1mut, isocitrate dehydrogenase 1 mutated. |
Data extraction
From the selected studies, we extracted data on study design, chemotherapy scheme, AML status, median age, CR, OS, and safety data. Different CR rates were reported in the included studies, including CR with incomplete blood count recovery (CRi), CR without platelet recovery (CRp), and CR with partial hematological recovery (CRh). Median CR duration (mCRD) is reported when data were available.
Diagnosis and epidemiology of IDH1mut AML
IDH1 mutation
The IDH1 enzyme is encoded by the IDH1 gene on chromosome 2q33.3 and localized in the cytoplasm and peroxisomes.3,7,8 The IDH1 gene normally encodes NADPH-dependent enzyme that catalyze the conversion of isocitrate to αKG. IDH1mut reduces αKG to the oncometabolite D2HG, causing its accumulation.3,9,10 Biochemical studies have shown that D2HG production can potentially affect epigenetic regulation and cell differentiation through inhibition of both histone and DNA demethylation.11
In AML, the most frequently detected IDH1mut is located in the Arg132 residue (R132), modifying the substrate-binding arginine of the enzyme catalytic domain for R132H, R132C, R132G, R132L, or R132S residues. The results of R132 IDH1mut are hypermethylation of DNA and histones and a block in differentiation that implies the presence of leukemogenic myeloid progenitor cells.7 Despite these effects, IDHmut enzymes alone do not cause leukemic transformation in mice. Several studies have demonstrated that IDH mutations tend to occur in combination with other mutations, suggesting cooperation to drive leukemogenesis in human AMLs.12 Mutations in IDH1 and IDH2 are thought to be mutually exclusive, although occasionally in rare AML, patients have concurrent mutations in both IDH1 and IDH2.8,13
IDH1 epidemiology
Several studies have demonstrated that IDH1mut and IDH2mut are associated with older age and confer an adverse prognosis, especially IDH1mut in AML with a cytogenetically normal karyotype (CN-AML).8,14 Other covariants are associated with IDH1mut, including intermediate-risk cytogenetics, a higher platelet count, increased bone marrow–blast percentage at diagnosis, FLT3-ITD and NPM1 mutations,3,8,14,15 and rarely related to therapy-related AML, TET2, and WT1 mutations.3,16,17
IDH1 comutations
A meta-analysis performed by Patel et al found that NPM1 is the most frequent concurrent mutation (87/144; 60.4%), followed by FLT3-ITD (37/146; 25.3%) and CEBPA (14/155; 9.0%).18 In several studies, it has been shown that a heterogeneous pattern of certain gene mutations is associated with different prognostics. In CN-AML, a favorable genotype is defined by the association of NPM1 or CEBPA mutation without either FLT3-ITD nor IDH1 mutations.16 Furthermore, IDH1 mutations confer adverse prognoses in CN-AML with NPM1 mutation without FLT3-ITD.8,14,19
IDH1mut diagnosis
IDHmut testing is essential in the clinical setting to identify AML patients who may benefit from targeted IDH treatments. Several methods are used to test IDH mutations from patients with hematologic malignancies, including Sanger sequencing, PCR-based methods, and next-generation sequencing (NGS).3,20–25 Sanger sequencing has been the classical way to detect IDHmut. However, this procedure is low sensitive and produces slow turnaround, and thus might be less suitable as a molecular diagnostic tool.
PCR-based methods are rapid and not expensive methods to detect known mutations. Because IDH1mut are recurrently located at codon 132 in exon 4 of the IDH1 gene, several PCR-based methods have been developed to detect them.3,20,21 Recently, new digital PCR technology (BEAMing) enabled IDH1mut detection up to 5 different mutations (R132S, R132G, R132C, R132H, and R132L) from a single sample with higher sensitivity than NGS (lower limit of detection 0.02–0.04%).24 NGS is used as a substitute for PCR and Sanger sequencing in many academic medical centers, and gene panels are used for diagnostic and prognostic purposes. It allows quantification of variant allele frequency (VAF) and the detection of co-occurring mutations.25 Serial monitoring by NGS has been employed in clinical trials to detect minimal residual disease (MRD) after therapy with IDHmut inhibitors.26
Prognostic impact of IDH1 mutations in AML patients receiving standard chemotherapy
The prognostic impact of IDH1mut has been widely studied in newly diagnosed AML with contradictory results, suggesting adverse outcomes,7,14,19 no influence,3,8,27–33 or a favorable outcome in one study.15 A meta-analysis of 8 studies found a lower event-free survival (EFS) in patients with IDH1mut, but there were no differences in OS.17 However, two meta-analyses including 15 studies34 and 24 studies35 obtained significant associations between IDH1mut and lower OS, as well as a lower event-free survival and CR rate in the last meta-analysis.35 These associations were reproduced in the subset of CN-AML IDH1mut patients.34,35 Furthermore, the IDH1 single-nucleotide polymorphism rs11554137 was also related to a poor OS.35
The influence of these mutations in R/R AML remains scarcely reported. Mutation of IDH1 was an unfavorable factor for survival in a large cohort of 761 R/R AML treated with intensive salvage therapy.36 The main schemes employed were based on a high dose of Ara-C (HiDAC), used in 71.2% of the patients. Unfortunately, specific data regarding the outcomes of IDH1mut with each salvage scheme were not provided. The next large study analyzing the clinical outcomes of IDH mutations did not find any differences in the CR/CRi and the median OS (mOS) among IDH1mut, IDH2mut, and wild-type IDH (wtIDH) for AML induction or the first salvage therapy (S1) and the second or beyond salvage therapy (S2). This study employed at S1 and S2 schemes based on HiDAC (36% and 41%), hypomethylating agents (HMA) (32% and 27%), and low-dose Ara-C (24% and 3%). Specifically, IDH1mut showed a CR/CRi of 40% vs 41% and 36% vs 27% at S1 and S2 against wtIDH, respectively, and a mOS of 5.9 and 7.7 months at S1 and 4.0 and 4.8 months at S2, respectively.3 Lower survival rates were reported in a French cohort of 185 R/R AML patients treated with standard salvage therapies (intensive chemotherapy in 68%, azacitidine in 18%, and other therapies in 14%) comparing IDH1mut versus wtIDH and IDH2mut (mOS 5.9, 7.6, and 11 months; 3-year OS 8%, 19%, and 23%), whereas no differences were reported in CR (50%, 43%, and 52%, respectively).4 Recently, the outcomes of R/R AML with IDH1mut from the UK NCRI AML trials treated with nontargeted therapy were analysed, showing mOS of 4.4 months, 1-year OS of 32%, 2-year OS of 17%. and remission rate of 23%. Age and AML subtypes (refractory, relapsed post-HSCT, second relapse, and relapsed within 1 year of remission) were not associated with differences in survival rates.37
Novel approaches in IDH1-mutated relapsed or refractory AML
Several targeted therapy agents are currently under development for IDH1mut R/R AML patients, andare showing promising results.
Ivosidenib (AG-120)
Drug development and pharmacokinetics
Ivosidenib (AG-120) is the first oral selective small molecule inhibitor of the IDH1-R132mut, resulting in inhibition of mutant IDH1 enzyme and decreased D2HG levels. The efficacy, safety, and pharmacokinetics of ivosidenib were evaluated in Phase I/II clinical trial in patients with IDH1mut advanced hematologic malignancies, including R/R AML [NCT02074839].38,39 Besides, this agent is being tested for advanced cholangiocarcinoma [NCT02989857], glioma [NCT03343197], and advanced solid tumors [NCT02073994]. In July of 2018, the FDA approved ivosidenib for the treatment of R/R AML patients with IDH1mut.40
The selected oral dose was 500 mg/24 hrs (maximum tolerated dose was not reached). It was rapidly absorbed (median 3 hrs to peak plasma concentration) and a steady state reached at 14 days. The steady-state mean apparent volume of distribution was 234 L and the protein bound was near 92–96%. CYP3A4 was the main way of metabolism, although 77% was excreted unchanged in the feces and 17% in the urine (10% unchanged), obtaining a clearance of 4.3 L/hr and a terminal elimination half-life of 93 hrs.38,41 A population pharmacokinetic model of ivosidenib has been recently performed, suggesting that no dose adjustments were needed according to the patient and disease conditions, and only the concomitant use of azoles (moderate/strong CYP3A4 inhibitors) was able to reduce ivosidenib clearance.42
Efficacy
The Phase I dose-escalation and dose-expansion clinical trial included 179 AML R/R IDH1mut patients treated with 500 mg of ivosidenib every 24 hrs in a 28-day cycle (cutoff date May 12, 2017;38 second cutoff date November, 201739) (Table 1). The primary endpoint of this study, CR or CRh, was achieved in 30.2% for an mCRD of 6.5 months (31.8% and 8.2 months at the second cutoff). In addition, the CR rate was 21.8% with an mCRD of 9.3 months (24.0% and 10.1 months at second cut-off) and overall response (OR) of 39.1% and mCRD of 6.5 months (41.9% and 6.5 months at second cutoff). The mOS in the first primary efficacy cohort of 125 patients treated with 500 mg/24 hrs was 8.8 and 9.0 months after a median follow-up of 14.8 and 15.3 months. Transfusion independence ≥56 days was achieved in 35% of patients with previous transfusion dependence and maintained in 56% of the patients who were transfusion-independent at baseline.
 |
Table 1 Studies using IDH1 inhibitors in IDH1-mutated relapsed or refractory AML |
After ivosidenib therapy, 21% IDH1mut clearance was detected using digital PCR among the 34 patients who had CR or CRh38 (23%, 11 of 47 at the second cutoff).39 This subset of patients showed longer CRD (11.1 vs 6.5 months) and mOS (14.5 vs 10.2 months) than those without IDH1mut clearance. The role of the baseline comutated genes was also evaluated, and a significant association between CR or CRh and a lower comutational burden was found (P=0.02). However, no specific preexisting mutations were identified as predictors of CR or resistance, although mutations in receptor tyrosine–kinase pathway genes were enriched in patients without response.38
Safety
Ivosidenib monotherapy of 500 mg/24 hrs in R/R AML had acceptable tolerance and was not related to any dose-limiting toxic effects, although adverse events (AEs) were reported in 99% of the patients enrolled in Phase I clinical trial and the dose-expansion study [NCT02074839].38,39 Table 1 summarizes the AEs reported in >20% patients in all the grades, as well as AE grades ≥3. Treatment-related AEs from ivosidenib were IDH differentiation syndrome (IDH-DS), prolongation of the QT interval, and leukocytosis. All these AEs are manageable and reversible, without needing permanent discontinuation of treatment. There were no deaths related to ivosidenib dose of 500 mg/24 hrs, whereas at 800 mg/24 hrs one AE-related death (cardiac tamponade) was reported as possibly associated with ivosidenib.
IDH-DS is a potentially fatal AE that produces a rapid increase in the differentiation of neutrophils after the removal of the differentiation block in the malignant myeloid clone. It was initially described in acute promyelocytic leukemia and it is a common AE of IDHmut inhibitors.43,44 IDH-DS showed similar incidence with enasidenib (ivosidenib, total: 19 [10.6%], grade ≥3: 9 [5.0%];38 enasidenib, total: 33 [11.7%]; grade ≥3: 15 [6.3%]),45 an IDH2 inhibitor, and in more than a third of the cases it could be accompanied with leukocytosis. A recent systematic analysis performed by the FDA46 obtained a higher incidence of 19% of IDH-DS in clinical trials of ivosidenib and enasidenib in R/R AML using the diagnosed criteria of Montesinos et al.47 IDH-DS could be managed by discontinuation and treatment with glucocorticoids and/or hydroxyurea, and these patients had clinical responses.38,42
Future directions
After the FDA approval of ivosidenib monotherapy in R/R AML with IDH1mut, an expanded-access program has been promoted by manufacturing company including adult patients and children ≥12 years of age who weigh at least approximately 100 lb [NCT03245424]. Combinations of ivosidenib with HMAs or intensive chemotherapy in R/R AML IDH1mut patients have not been evaluated yet. However, the addition of venetoclax to ivosidenib is under investigation in this subset of patients in a Phase I/II trial [NCT03471260].
The use of ivosidenib as a front-line therapy as a single agent38,48 has been analyzed in a Phase Ib clinical trial [NCT02074839] (Table 2), and it has shown a promising 42.4% CR/CRh rate among the 33 subjects. Ongoing clinical trials are testing in IDH1mut-untreated AML patients, the safety and efficacy of different combinations of ivosidenib with azacitidine [NCT03173248; NCT02677922]49–51 or intensive chemotherapy [NCT02632708]52 (Table 2). It is worth noting that a new international Phase III randomized clinical trial aiming to enroll a large number of patients will compare AZA+IVO vs AZA in newly diagnosed IDH1mut patients unfit for intensive chemotherapy [NCT03173248]. Moreover, ivosidenib is being tested as maintenance therapy after allo-HSCT in IDH1mut myeloid malignancies in a Phase I dose-escalation trial [NCT03564821].
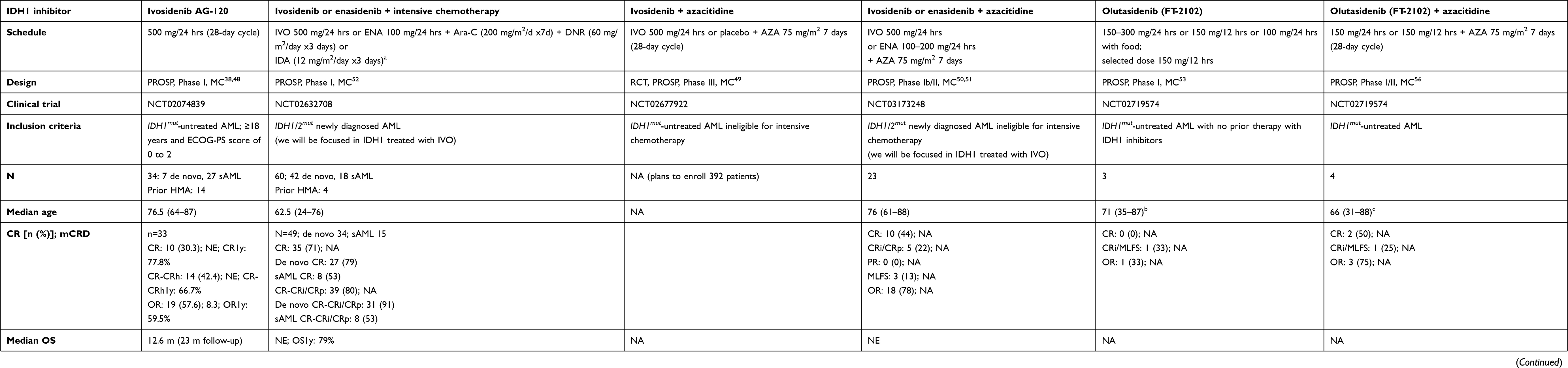 |
Table 2 Studies using IDH1 inhibitors in IDH1-mutated untreated AML |
Olutasidenib (FT-2102)
Drug development and pharmacokinetics
Olutasidenib (FT-2102) is a new IDH1mut inhibitor that is being tested in an ongoing Phase I/II clinical trial in patients with IDH1mut AML (R/R or untreated) and MDS [NCT02719574] in monotherapy and combined with azacitidine. Preclinical studies in rats and human tissue showed a major excretion route through the hepatic metabolism by CYP enzymes (CPY3A4, 2C9 and 1A1). Pharmacokinetic, pharmacodynamic, and safety data have supported the selection of a 150 mg/12 hr dose, reaching a durable steady state at 2 weeks without a low threshold for QTc-prolongation risk and achieving prompt and durable 2-HG reductions.53 FT-2102 is also being tested in advanced solid tumors and gliomas with IDH1mut [NCT03684811].
Efficacy
The first set of data of the Phase I/II clinical trial was recently presented, including 31 patients treated with FT-2102 as a single agent with a median of 3 months (range 0.2–20 months), 22 of them with R/R AML with no prior therapy with IDH1mut inhibitors (Table 1).53 Preliminary endpoints reported were CR rate of 14%, a CRi and morphologic leukemia-free state (MLFS) of 19%, and OR of 33%.
Safety
Regarding the safety of olutasidenib, severe AEs occurring in >5% of patients of the entire cohort are included in Table 1. IDH-DS was reported in 3 patients and resolved after temporary discontinuation and treatment with dexamethasone, hydroxyurea, and supportive care. There were no deaths related to FT-2102 therapy.53
Future directions
Combinations of HMA and IDHmut inhibitors are being evaluated in several clinical trials because this combination increases hemoglobinization and the expression of erythroid differentiation markers, reduces leukemic stem cell populations, and potentiates apoptosis.54,55 The addition of azacitidine had no impact on FT-2102 pharmacokinetics.
At data cutoff (April 7, 2018), 26 patients had beentreated with FT-2102 (150 mg/24 hrs or 150 mg/12 hrs) plus azacitidine (75 mg/m2 for 7 days) for a median of 3 months (range 0.2–12 months), 20 of them with R/R AML56 (Table 1). Preliminary end points reported were CR rate of 0%, CRi + MLFS of 32%, and OR of 32%. AEs with a grade ≥3 occurring in >5% of patients of the entire cohort are summarized in Table 1. IDH-DS developed in 3 patients, all of which remitted after temporary interruption and treatment (glucocorticoids, hydroxyurea, and supportive care). No deaths related to FT-2102 were reported.
Untreated AML patients were also included in a Phase I/II clinical trial, with scarce reported data [NCT02719574] (Table 2): 3 patients were treated with FT-2102 monotherapy53 and 4 patients had it in combination with azacytidine.56 At the first cutoff, these schemes had obtained CR of 0% and 50%, CRi/MLFS of 33% and 25%, and OR of 33% and 75%, respectively. Safety profiles were analyzed together with the subsets of R/R AML and MDS.
FT-2102 monotherapy at 150 mg/12 hrs will be analyzed in an ongoing Phase II study with three cohorts [NCT02719574]: R/R AML, AML/MDS with CR/CRi (ie, with MRD), and R/R MDS/AML with a prior exposure to an IDH1m inhibitor. Moreover, three Phase 2 combination-therapy (FT-2102 150 mg/12 hrs plus azacitidine 75 mg/m2 7 days) cohorts are currently open [NCT02719574]: patients <60 years with R/R AML or MDS naïve to HMA and IDH1m inhibitors; R/R AML or MDS with inadequate response/PD on HMA; and R/R AML or MDS who have progressed on a prior IDH1m inhibitor.
Other IDH1mut inhibitors
IDH305
IDH305 is an oral small-molecule IDH1mut inhibitor active against the IDH1R132 mutation and assayed in a Phase I dose-finding clinical trial [NCT02381886] in AML/MDS (including R/R AML; Table 1), gliomas, and other/noncentral nervous system (CNS) solid tumors. Preliminary results in 21 AML patients were reported at cutoff on March 30, 2016, showing promising antitumoral activity:57 a CR of 9.5%, a CRi of 4.8%, and partial remission (PR) of 19%. Hepatotoxicity was detected in the 3 malignancies (Table 1), although in AML/MDS the incidence was lower. Unfortunately, 3 subsequent clinical trials [NCT02987010, NCT02977689, NCT02826642] were withdrawn before enrolling the first participant, and no new clinical data about this drug have been reported.
Vorasidenib (AG881)
Vorasidenib (AG-881) is an oral inhibitor of IDH1mut and IDH2mut which is being evaluated in a Phase I trial in solid tumors, including gliomas, as it penetrates the blood–brain barrier [NCT02481154], with the first report of the safety profile in 93 of the patients.58 Furthermore, AG-881 is being tested in advanced hematologic malignancies after progression with a prior IDHmut-inhibitor treatment [NCT02492737].
BAY1436032
BAY1436032 is an oral pan-mutant IDH1 inhibitor, active against IDH1R132H, IDH1R132C, IDH1R132G, IDH1R132L, and IDH1R132S, which has demonstrated, in preclinical in vitro and in vivo studies strong antileukemic activity in IDH1mut patient-derived xenograft (PDX) models.59 BAY1436032 is being tested in Phase I trials as a single agent in R/R AML [NCT03127735] and advanced solid tumors [NCT02746081], but the clinical reports have not been presented yet. Also, synergistic activity has been detected in PDX IDH1mut models with a combination of BAY-1436032 and azacitidine through inhibition of the cell cycle by dysregulating EGR, GFI1, and NFkB signaling.60
DS-1001
DS-1001 is a new oral IDH1mut inhibitor being studied in patients with recurring or progressing gliomas [NCT03030066]. Potentially, DS-1001 could be active in R/R AML IDH1mut patients.
Non-targeted therapies tested in IDH1mut AML
Venetoclax
Venetoclax is an oral selective inhibitor of the antiapoptotic B-cell lymphoma-2 (BCL-2) that is being tested in R/R AML. Preclinical studies have obtained activity against IDHmut cells mediated by the intracellular accumulation of the oncometabolite D2HG.61 This finding was reproduced in clinical trials of venetoclax monotherapy in R/R or untreated AML62 and combined with HMA or low-dose cytarabine in R/R myeloid malignancies,63 achieving a CR/CRi of 33% and a 27% response rate in IDHmut patients, respectively. This study revealed that venetoclax could be an alternative treatment after IDH-inhibitor failure (7 of 11 patients were pretreated with IDHmut inhibitors).63 In elderly untreated AML patients who are unfit for intensive therapies, combinations of HMA and venetoclax obtained in an IDHmut subgroup a CR/CRi rate of 71% and a median OS of 24.4 months.64 Combinations of venetoclax and ivosidenib will be tested in this subset of patients in a Phase I/II trial [NCT03471260].
CB839
CB-839 is an oral glutaminase inhibitor under investigation. Glutaminase is an enzyme which generates glutamine, the main source of α-KG in IDH1mut cells. Preclinical and in vivo studies demonstrated that CB839 reduced the growth of IDH1/2mut AML cells.65–67 In R/R AML IDHmut patients, CB-839 is being tested in monotherapy and in combinations with azacitidine [NCT02071927].68
PARP inhibitors: olaparib and talazoparib
The D2HG produced by IDH1/2mut enzymes is associated with increased DNA damage and improved responses to poly (ADP-ribose) polymerases (PARP) inhibitors in solid tumor cells. In an in vitro study, AML IDH1/2mut cells were sensitive to monotherapy with PARP inhibitors (olaparib and talazoparib). This activity was potentiated in combination with daunorubicin, a DNA-damaging agent. However, the combination of PARP and IDH1/2mut inhibitors decreased and antagonized their efficacy.69 Monotherapy with olaparib is being studied in glioma, cholangiocarcinoma, and other solid tumors with IDH1mut or IDH2mut [NCT03212274], and BGB-290 (PARP inhibitor) combined with temozolomide in glioma, but these agents have not been tested in R/R AML yet.
IDH1-peptide vaccine
The mutation-specific vaccination of IDH1 (R132H) has been tested as a novel target for immunotherapy in glioma, as this neoantigen shows high uniform expression and penetrance in glioma cells. Preclinical studies in mice with IDH1-peptide vaccination obtained an effective mutation-specific antitumour immune response against IDH1R132H-expressing tumor cells and reduced the growth of gliomas.70,71 Three different clinical trials are evaluating the safety and efficacy of IDH1-peptide vaccine in different grades of glioma alone [NCT02454634, NCT02771301] or combined with temozolamide [NCT02193347].
Conclusion
R/R is the subset of AML with worse long-term outcomes with standard salvage therapies. The investigation of new targeted therapies (IDH and FLT3) has shown promising results, achieving a better antileukemic efficacy and safety profile in comparison with salvage regimens. In this review, we have analyzed the impact of IDH1mut inhibitors, a new targeted therapy with positive results in R/R AML.
Two IDHmut inhibitors (ivosidenib and enasidenib) have achieved fast approval with Phase I/II clinical trial results in the subgroup of IDH1/2mut R/R AML, pending further studies to demonstrate a significant improvement in survival and/or other long-term outcomes. Nevertheless, with the advent of new targeted therapies, the diagnostic workup of R/R AML will now include a systematic screening for IDH1 mutations, in order to personalize treatments. Ongoing clinical trials are testing the use of IDHmut inhibitors as single agent or in combination with HMAs or intensive chemotherapy as frontline therapy and the role of these inhibitors in post-transplant maintenance.
Acknowledgments
This study was supported in part by a grant from the “Instituto Carlos III” (PI16/00665).
Disclosure
Dr Pau Montesinos reports grants from Celgene and Daiichi Sankyo during the conduct of the study and is on the advisory board for AGIOS, Celgene and Daiichi Sankyo. The authors report no other conflicts of interest in this work.
References
1. Döhner H, Estey E, Grimwade D, et al. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood. 2017;129(4):424–427. doi:10.1182/blood-2016-08-733196
2. Megias-Vericat JE, Martinez-Cuadron D, Sanz MA, Montesinos P. Salvage regimens using conventional chemotherapy agents for relapsed/refractory adult AML patients: a systematic literature review. Ann Hematol. 2018;97(7):1115–1153. doi:10.1007/s00277-018-3304-y
3. DiNardo CD, Ravandi F, Agresta S, et al. Characteristics, clinical outcome, and prognostic significance of IDH mutations in AML. Am J Hematol. 2015;90(8):732–736. doi:10.1002/ajh.24072
4. Bertoli S, Tavitian S, Delabesse E, Sarry A, Huguet F, Récher C. Outcome of AML patients with IDH1 or IDH2 mutations from diagnosis and refractory/relapse phase of the disease in routine practice. Blood. 2016;128(22):1718. doi:10.1182/blood-2016-06-724161
5. Dhillon S. Ivosidenib: first Global Approval. Drugs. 2018;78(14):1509–1516. doi:10.1007/s40265-018-0978-3
6. Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;339:b2700. doi:10.1136/bmj.b2651
7. Kaushansky K, Lichtman MA, Prchal JT, et al. Williams Hematology.
8. Paschka P, Schlenk RF, Gaidzik VI, et al. IDH1 and IDH2 mutations are frequent genetic alterations in acute myeloid leukemia and confer adverse prognosis in cytogenetically normal acute myeloid leukemia with NPM1 mutation without FLT3 internal tandem duplication. J Clin Oncol. 2010;28(22):3636–3643. doi:10.1200/JCO.2010.28.3762
9. Schnittger S, Haferlach C, Ulke M, Alpermann T, Kern W, Haferlach T. IDH1 mutations are detected in 6.6% of 1414 AML patients and are associated with intermediate risk karyotype and unfavorable prognosis in adults younger than 60 years and unmutated NPM1 status. Blood. 2010;116(25):5486–5496. doi:10.1182/blood-2010-02-267955
10. Nassereddine S, Lap CJ, Haroun F, Tabbara I. The role of mutant IDH1 and IDH2 inhibitors in the treatment of acute myeloid leukemia. Ann Hematol. 2017;96(12):1983–1991. doi:10.1007/s00277-017-3116-5
11. Garrett-Bakelman FE, Melnick AM, Mutant IDH. a targetable driver of leukemic phenotypes linking metabolism, epigenetics and transcriptional regulation. Epigenomics. 2016;8(7):945–957. doi:10.2217/epi-2016-0008
12. Dang L, Jin S, Su SM. IDH mutations in glioma and acute myeloid leukemia. Trends Mol Med. 2010;16(9):387–397. doi:10.1016/j.molmed.2010.07.002
13. Platt MY, Fathi AT, Borger DR, et al. Detection of dual IDH1 and IDH2 mutations by targeted next-generation sequencing in acute myeloid leukemia and myelodysplastic syndromes. J Mol Diagn. 2015;17(6):661–668. doi:10.1016/j.jmoldx.2015.06.004
14. Marcucci G, Maharry K, Wu YZ, et al. IDH1 and IDH2 gene mutations identify novel molecular subsets within de novo cytogenetically normal acute myeloid leukemia: a Cancer and Leukemia Group B study. J Clin Oncol. 2010;28(14):2348–2355. doi:10.1200/JCO.2009.27.3730
15. Patel JP, Gonen M, Figueroa ME, et al. Prognostic relevance of integrated genetic profiling in acute myeloid leukemia. N Engl J Med. 2012;366(12):1079–1089. doi:10.1056/NEJMoa1114705
16. Rampal R, Alkalin A, Madzo J, et al. DNA hydroxymethylation profiling reveals that WT1 mutations result in loss of TET2 function in acute myeloid leukemia. Cell Rep. 2014;9(5):1841–1855. doi:10.1016/j.celrep.2014.11.004
17. Zhou KG, Jiang LJ, Shang Z, et al. Potential application of IDH1 and IDH2 mutations as prognostic indicators in non-promyelocytic acute myeloid leukemia: A meta-analysis. Leuk Lymphoma. 2012;53(12):2423–2429. doi:10.3109/10428194.2012.695359
18. Patel KP, Ravandi F, Ma D, et al. Acute myeloid leukemia with IDH1 or IDH2 mutation. Am J Clin Pathol. 2011;135(1):35–45. doi:10.1309/AJCPD7NR2RMNQDVF
19. Boissel N, Nibourel O, Renneville A, et al. Prognostic impact of isocitrate dehydrogenase enzyme isoforms 1 and 2 mutations in acute myeloid leukemia: a study by the Acute Leukemia French Association group. J Clin Oncol. 2010;28(23):3717–3723. doi:10.1200/JCO.2010.28.2285
20. Patel KP, Barkoh BA, Chen Z, et al. Diagnostic testing for IDH1 and IDH2 variants in acute myeloid leukemia an algorithmic approach using high resolution melting curve analysis. J Mol Diagn. 2011;13(6):678–686. doi:10.1016/j.jmoldx.2011.06.004
21. Mahdieh N, Rabbani B. An overview of mutation detection methods in genetic disorders. Iran J Pediatr. 2013;23(4):375–388.
22. Horbinski C, Kelly L, Nikiforov YE, Durso MB, Nikiforova MN. Detection of IDH1 and IDH2 mutations by fluorescence melting curve analysis as a diagnostic tool for brain biopsies. J Mol Diagn. 2010;12(4):487–492. doi:10.2353/jmoldx.2010.090228
23. Gorniak P, Ejduk A, Borg K, et al. Comparison of high-resolution melting analysis with direct sequencing for the detection of recurrent mutations in DNA methyltransferase 3A and isocitrate dehydrogenase 1 and 2 genes in acute myeloid leukemia patients. Eur J Haematol. 2016;96(2):181–187. doi:10.1111/ejh.12566
24. Dressman D, Yan H, Traverso G, Kinzler KW, Vogelstein B. Transforming single DNA molecules into fluorescent magnetic particles for detection and enumeration of genetic variations. Proc Natl Acad Sci U S A. 2003;100(15):8817–8822. doi:10.1073/pnas.1133470100
25. Alonso CM, Llop M, Sargas C, et al. Clinical utility of a next-generation sequencing panel for acute myeloid leukemia diagnostics. J Mol Diagn. 2019;21(2):228-240. doi:10.1016/j.jmoldx.2018.09.009 .
26. Yang H, Ye D, Guan KL, Xiong Y. IDH1 and IDH2 mutations in tumorigenesis: mechanistic insights and clinical perspectives. Clin Cancer Res. 2012;18(20):5562–5571. doi:10.1158/1078-0432.CCR-12-1773
27. Chou WC, Hou HA, Chen CY, et al. Distinct clinical and biologic characteristics in adult acute myeloid leukemia bearing the isocitrate dehydrogenase 1 mutation. Blood. 2010;115(14):2749–2754. doi:10.1182/blood-2009-11-253070
28. Abbas S, Lugthart S, Kavelaars FG, et al. Acquired mutations in the genes encoding IDH1 and IDH2 both are recurrent aberrations in acute myeloid leukemia: prevalence and prognostic value. Blood. 2010;116(12):2122–2126. doi:10.1182/blood-2009-11-250878
29. Wagner K, Damm F, Gohring G, et al. Impact of IDH1 R132 mutations and an IDH1 single nucleotide polymorphism in cytogenetically normal acute myeloid leukemia: SNP rs11554137 is an adverse prognostic factor. J Clin Oncol. 2010;28(14):2356–2364. doi:10.1200/JCO.2009.27.6899
30. Green CL, Evans CM, Zhao L, et al. The prognostic significance of IDH2 mutations in AML depends on the location of the mutation. Blood. 2011;118(2):409–412. doi:10.1182/blood-2010-12-322479
31. Chotirat S, Thongnoppakhun W, Promsuwicha O, Boonthimat C, Auewarakul CU. Molecular alterations of isocitrate dehydrogenase 1 and 2 (IDH1 and IDH2) metabolic genes and additional genetic mutations in newly diagnosed acute myeloid leukemia patients. J Hematol Oncol. 2012;5(1):5. doi:10.1186/1756-8722-5-5
32. Ravandi F, Patel K, Luthra R, et al. Prognostic significance of alterations in IDH enzyme isoforms in patients with AML treated with high-dose cytarabine and idarubicin. Cancer. 2012;118(10):2665–2673. doi:10.1002/cncr.26580
33. Willander K, Falk IJ, Chaireti R, et al. Mutations in the isocitrate dehydrogenase 2 gene and IDH1 SNP 105C > T have a prognostic value in acute myeloid leukemia. Biomark Res. 2014;2(1):18. doi:10.1186/2050-7771-2-18
34. Feng JH, Guo XP, Chen YY, Wang ZJ, Cheng YP, Tang YM. Prognostic significance of IDH1 mutations in acute myeloid leukemia: a meta-analysis. Am J Blood Res. 2012;2(4):254–264.
35. Xu Q, Li Y, Lv N, et al. Correlation between isocitrate dehydrogenase gene aberrations and prognosis of patients with acute myeloid leukemia: a systematic review and meta-analysis. Clin Cancer Res. 2017;23(15):4511–4522. doi:10.1158/1078-0432.CCR-16-2628
36. Wattad M, Weber D, Döhner K, et al. Impact of salvage regimens on response and overall survival in acute myeloid leukemia with induction failure. Leukemia. 2017;31(6):1306–1313. doi:10.1038/leu.2017.23
37. Hills RK, Gale R, Linch DC, et al. Outcomes of relapsed/refractory patients with IDH1/2 mutated AML treated with non-targeted therapy: results from the NCRI AML trials [abstract]. Blood. 2018;132(Suppl 1):664.
38. DiNardo CD, Stein EM, de Botton S, et al. Durable remissions with ivosidenib in IDH1-mutated relapsed or refractory AML. N Engl J Med. 2018;378(25):2386–2398. doi:10.1056/NEJMc1711583
39. Pollyea DA, Dinardo CD, de Botton S, et al. Ivosidenib (IVO; AG-120) in mutant IDH1 relapsed/refractory acute myeloid leukemia (R/R AML): results of a phase 1 study [abstract plus oral communication]. J Clin Oncol. 2018;36(Suppl 15):7000. doi:10.1200/JCO.2018.36.15_suppl.7000
40. US Food & Drug Administration. FDA approves first targeted treatment for patients with relapsed or refractory acute myeloid leukemia who have a certain genetic mutation [home page on the Internet]. 2018. Available from: https://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm614115.htm.
41. Agios Pharmaceuticals. TIBSOVO ® (Ivosidenib): US prescribing Information [home page on the internet]. 2018. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/211192s000lbl.pdf.
42. Le K, Wada R, Dai D, et al. Population pharmacokinetics of ivosidenib (AG-120) in patients with IDH1-mutant advanced hematologic malignancies [abstract]. Blood. 2018;132(Suppl 1):1394.
43. Birendra KC, DiNardo CD. Evidence for clinical differentiation and differentiation syndrome in patients with acute myeloid leukemia and IDH1 mutations treated with the targeted mutan IDH1 inhibitor, AG-120. Clin Lymphoma Myeloma Leuk. 2016;16(8):460–465. doi:10.1016/j.clml.2016.04.006
44. Fathi AT, DiNardo CD, Kline I, et al. Differentiation syndrome associated with enasidenib, a selective inhibitor of mutant isocitrate dehydrogenase 2: analysis of a phase 1/2 study. JAMA Oncol. 2018;4(8):1106–1110. doi:10.1001/jamaoncol.2017.4695
45. Stein EM, DiNardo CD, Pollyea DA, et al. Enasidenib in mutant IDH2 relapsed or refractory acute myeloid leukemia. Blood. 2017;130(6):722–731. doi:10.1182/blood-2017-04-779405
46. Norsworthy KJ, Mulkey F, Ward AF, et al. Incidence of differentiation syndrome with ivosidenib (IVO) and enasidenib (ENA) for treatment of patients with relapsed or refractory (R/R) isocitrate dehydrogenase (IDH)1- or IDH2-mutated acute myeloid leukemia (AML): a systematic analysis by the U.S. Food and Drug Administration (FDA) [abstract]. Blood. 2018;132(Suppl 1):288.
47. Montesinos P, Bergua JM, Vellenga E, et al. Differentiation syndrome in patients with acute promyelocytic leukemia treated with all-trans retinoic acid and anthracycline chemotherapy: characteristics, outcome, and prognostic factors. Blood. 2009;113(4):775–783. doi:10.1182/blood-2008-07-168617
48. Roboz GJ, DiNardo CD, Stein EM, et al. Ivosidenib (AG-120) induced durable remissions and transfusion independence in patients with IDH1-mutant untreated AML: results from a phase 1 dose escalation and expansion study [abstract plus oral communication]. Blood. 2018;132(Suppl 1):561.
49. Stein E, Dinardo CD, Jang JH, et al. AGILE: A phase 3, multicenter, randomized, placebo-controlled study of ivosidenib in combination with azacitidine in adult patients with previously untreated acute myeloid leukemia with an IDH1 mutation. J Clin Oncol. 2018;36(Suppl15):TPS7074. doi:10.1200/JCO.2018.36.15_suppl.TPS7074
50. DiNardo CD, Stein AS, Fathi AT, et al. Mutant isocitrate dehydrogenase (mIDH) inhibitors, enasidenib or ivosidenib, in combination with azacitidine (AZA): preliminary results of a phase 1b/2 study in patients with newly diagnosed acute myeloid leukemia (AML) [abstract plus oral communication]. Blood. 2017;130(Suppl 1):639.
51. Dinardo CD, Stein AS, Stein EM, et al. Mutant IDH (mIDH) inhibitors, ivosidenib or enasidenib, with azacitidine (AZA) in patients with acute myeloid leukemia (AML) [abstract plus poster]. J Clin Oncol. 2018;36(Suppl 15):7042. doi:10.1200/JCO.2018.36.15_suppl.7042
52. Stein EM, DiNardo CD, Fathi AT, et al. Ivosidenib or enasidenib combined with induction and consolidation chemotherapy in patients with newly diagnosed AML with an IDH1 or IDH2 mutation is safe, effective, and leads to MRD-negative complete remissions [abstract plus oral communication]. Blood. 2018;132(Suppl 1):560. doi:10.1182/blood-2018-99-110449.
53. Watts J, Baer MR, Yang J, et al. Phase 1 study of the IDH1m inhibitor FT-2102 as a single agent in patients with IDH1m acute myeloid leukemia (AML) or myelodysplastic syndrome (MDS) [abstract]. Blood. 2018;132 (Suppl 1):1453. doi: 10.1182/blood-2018-99-114263.
54. Chopra VS, Avanzino B, Mavrommatis K, Olshen A, DiMartino J, MacBeth KJ. Functional characterization of combining epigenetic modifiers azacitidine and AG-221 in the TF-1: IDH2R140QAML model [abstract]. Cancer Res. 2016;76(Suppl 14):2280. doi:10.1158/0008-5472.CAN-16-0584
55. Yen K, Chopra VS, Tobin E, et al. Functional characterization of the ivosidenib (AG-120) and azacitidine combination in a mutant IDH1 AML cell model [abstract]. Cancer Res. 2018;8(Suppl 1):4956. doi:10.1158/1538-7445.AM2018-4956
56. Cortes JE, Watts J, Prebet T, et al. FT-2102, an IDH1m inhibitor, in combination with azacitidine in patients with acute myeloid leukemia (AML) or myelodysplastic syndrome (MDS): results from a phase 1 study [abstract]. Blood. 2018;132 (Suppl 1):1452; doi: 10.1182/blood-2018-99-114126.
57. DiNardo CD, Schimmer AD, Yee KWL, et al. A phase I study of IDH305 in patients with advanced malignancies including relapsed/refractory AML and MDS that harbor IDH1R132 mutations. Blood. 2016;128(22):1073. doi:10.1182/blood-2016-06-724161
58. Mellinghoff IK, Penas-Prado M, Peters KB, et al. Phase 1 study of AG-881, an inhibitor of mutant IDH1/IDH2, in patients with advanced IDH-mutant solid tumors, including glioma [abstract]. J Clin Oncol. 2018;36(Suppl 15):2002. doi:10.1200/JCO.2018.36.15_suppl.2002
59. Chaturvedi A, Herbst L, Pusch S, et al. Pan-mutant-IDH1 inhibitor BAY1436032 is highly effective against human IDH1 mutant acute myeloid leukemia in vivo. Leukemia. 2017;31(10):2020–2028. doi:10.1038/leu.2017.46
60. Chaturvedi A, Gupta C, Goparaju R, et al. Synergistic activity of IDH1 inhibitor bay-1436032 with azacitidine in IDH1 mutant acute myeloid leukemia [abstract]. Blood. 2017;130(Suppl 1):1352.
61. Chan SM, Thomas D, Corces-Zimmerman MR, et al. Isocitrate dehydrogenase 1 and 2 mutations induce BCL-2 dependence in acute myeloid leukemia. Nat Med. 2015;21(2):178–184. doi:10.1038/nm.3788
62. Konopleva M, Pollyea DA, Potluri J, et al. Efficacy and biological correlates of response in a phase II study of venetoclax monotherapy in patients with acute myelogenous leukemia. Cancer Discov. 2016;6(10):1106–1117. doi:10.1158/2159-8290.CD-16-0313
63. DiNardo CD, Rausch CR, Benton C, et al. Clinical experience with the BCL2-inhibitor venetoclax in combination therapy for relapsed and refractory acute myeloid leukemia and related myeloid malignancies. Am J Hematol. 2018;93(3):401–407. doi:10.1002/ajh.25000
64. DiNardo CD, Pratz K, Pullarkat V, et al. Venetoclax combined with decitabine or azacitidine in treatment-naive, elderly patients with acute myeloid leukemia. Blood. 2019;133(1):7–17. doi:10.1182/blood-2018-08-868752
65. Emadi A, Jun SA, Tsukamoto T, Fathi AT, Minden MD, Dang CV. Inhibition of glutaminase selectively suppresses the growth of primary acute myeloid leukemia cells with IDH mutations. Exp Hematol. 2014;42(4):247–251. doi:10.1016/j.exphem.2013.12.001
66. Fathi AT, Wander SA, Faramand R, Emadi A. Biochemical, epigenetic, and metabolic approaches to target IDH mutations in acute myeloid leukemia. Semin Hematol. 2015;52(3):165–171. doi:10.1053/j.seminhematol.2015.03.002
67. Matre P, Velez J, Jacamo R, et al. Inhibiting glutaminase in acute myeloid leukemia: metabolic dependency of selected AML subtypes. Oncotarget. 2016;7(48):79722–79735. doi:10.18632/oncotarget.12944
68. Wang ES, Frankfurt O, Orford KW, et al. Phase 1 study of CB-839, a first-in-class, orally administered small molecule inhibitor of glutaminase in patients with relapsed/refractory leukemia [abstract]. Blood. 2015;126(23):2566.
69. Molenaar RJ, Radivoyevitch T, Nagata Y, et al. IDH1/2 mutations sensitize acute myeloid leukemia to PARP inhibition and this is reversed by IDH1/2-mutant inhibitors. Clin Cancer Res. 2018;24(7):1705–1715. doi:10.1158/1078-0432.CCR-17-2796
70. Schumacher T, Bunse L, Pusch S, et al. A vaccine targeting mutant IDH1 induces antitumour immunity. Nature. 2014;512(7514):324–327. doi:10.1038/nature13387
71. Pellegatta S, Valletta L, Corbetta C, et al. Effective immuno-targeting of the IDH1 mutation R132H in a murine model of intracranial glioma. Acta Neuropathol Commun. 2015;3:4. doi:10.1186/s40478-014-0180-0
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.