")
Back to Journals » Journal of Asthma and Allergy » Volume 16
Identifying Chili as a Risk Factor for the Geographic Tongue: A Case Report
Authors Novianti Y , Nur’aeny N
Received 4 September 2023
Accepted for publication 10 November 2023
Published 23 November 2023 Volume 2023:16 Pages 1279—1285
DOI https://doi.org/10.2147/JAA.S434177
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Luis Garcia-Marcos
Yessy Novianti,1 Nanan Nur’aeny2
1Oral Medicine Residency Program, Faculty of Dentistry, Universitas Padjadjaran, Bandung, Indonesia; 2Oral Medicine Department, Faculty of Dentistry, Universitas Padjadjaran, Bandung, Indonesia
Correspondence: Yessy Novianti, Faculty of Dentistry, Universitas Padjadjaran, Jalan Sekeloa Selatan I, Bandung, 40132, Indonesia, Tel +6281368429045, Email [email protected]
Introduction: Geographic tongue (GT) is a chronic tongue condition triggered by various factors such as immune reactions, allergies, stress, hereditary factors, and nutritional deficiencies. The prevalence of GT in the population ranges from 1% to 3%, and its symptoms can cause discomfort to patients. Spicy foods are popular among Indonesians. Chili is one such food that can cause allergies and trigger GT.
Objective: This report highlights the significance of identifying the risk factors associated with symptomatic GT.
Case: A 19-year-old female patient complained of a rough and sore dorsal tongue for a year, particularly after consuming spicy food. Extra-oral examination revealed dry lips. Intra-oral examination showed red patches with white borders on the dorsal tongue. A complete blood count and allergy test were performed. The eosinophil count was 4%, the total IgE level was 698 IU/mL, and the skin prick test for chili was positive. The diagnosis of chili-induced GT was made.
Case Management: The patient was advised to avoid chilies, and benzydamine hydrochloride mouthwash was administered. One week after treatment, clinical improvement was observed. Severity decreased on the Geographic Tongue Area and Severity Index (GTASI) from 12 (moderate) to 0.4 (mild). Pain decreased from 6 to 0 on the numerical rating scale (NRS).
Conclusion: Management of symptomatic GT includes the avoidance of allergens such as chilies and appropriate pharmacological therapy. The identification of risk factors is required for effective management.
Keywords: allergy, GTASI, IgE, prick test, spicy food
Introduction
The oral cavity is a complex anatomical structure designed to facilitate pivotal physiological functions, including speech, breathing, chewing, swallowing, and deglutition.1–3 Among these functions is the tongue, which ultimately contributes to the oral cavity’s and oropharynx’s essential functions.2 The muscular structure of the tongue and its position on the floor of the mouth, as well as its muscular attachment, allow it to perform these functions. Anatomical changes may alter these functions.1
The tongue has protrusions on its dorsal surface called papillae, consisting of four types: filiform, fungiform, circumvallate, and foliate papillae. Apart from the filiform papillae, lingual papillae have taste buds responsible for transmitting taste’s sensory function.1,4,5 If the sensitivity of smell and taste is disturbed, it can reduce appetite because the food becomes tasteless.6 Changes in the papillae can affect individual nutrition and thus impact general health.7
Spicy food is a fundamental part of various culinary traditions in Indonesia.8 Indonesians have been used to eating spicy food for generations, as most traditional Indonesian food tastes spicy.9 Although capsicum allergies seem rare, allergic reactions have been observed after consuming chili.10 Spicy foods or chili can affect the taste buds, cause allergies, and trigger GT.11,12
GT is a pattern of reaction on the tongue due to an underlying condition. Characteristically, it presents as red patches with raised white edges, resembling islands and exhibiting a benign migration pattern.1,4,11,13,14 It may be asymptomatic or symptomatic, feeling uncomfortable, hot, itchy, soreness on the tongue, and intermittent.1,15,16 The etiology of GT is still unknown. Predisposing factors associated with GT include genetic factors, immune reactions, allergies, hormonal disorders, pregnancy, emotional stress, nutritional deficiencies, and drugs.1,17,18
The appearance of the surface of the dorsal tongue is clinically important because it may reflect the health of an individual.1,5,16 A comprehensive oral cavity examination is required to assess the presence or absence of pathological conditions. The diagnosis of GT can be challenging due to various predisposing factors. This case report highlights the significance of identifying the risk factors for symptomatic GT meticulously.
Case Report
A 19-year-old female came to the Department of Oral Medicine at Universitas Padjadjaran Dental Hospital with a complaint of a rough, painful, and intermittent tongue that had persisted for a year. The patient reported that the condition occurred after the consumption of spicy foods. The condition solely affected her tongue, with no involvement of the skin or other parts of the oral mucosa. The patient identified spicy food as an aggravating factor, but there were no limiting factors. The patient was prescribed topical corticosteroids following a visit to the dentist. The complaint showed improvement after three days of medication. Without medication, issues usually resolve within a week. There were no preceding symptoms of fever or illness.
The patient has an oral health check-up with the dentist every six months, and the recent visit entailed scaling. A history of drug and food allergies has been denied. The patient reported a lifelong history of asthma but has never had a relapse. The patient has never been hospitalized in the last year. The patient’s mother confirmed complete immunization. The social profile reveals that the patient is an unmarried student with no pets. The patient seldom consumes fruits and vegetables, drinks 2 liters of water per day, refrains from smoking and alcohol, and has routine menstrual cycles.
The Depression Anxiety Stress Scale (DASS)-21 test indicated normal levels of depression (2), anxiety (3), and stress (0) in the assessment of a negative emotional state. The physical examination revealed a good general status and compos mentis level of awareness. The patient has a weight of 50 kg and a height of 155 cm. The obtained vital signs were blood pressure 110/70 mmHg, pulse 80 times/minute, respiration 20 times/minute, and temperature 36.5 oC.
The extra-oral examination showed a symmetrical face, non-anemic conjunctiva, non-icteric sclera, and dry lips (Figure 1A). Additionally, palpable and painless lymph nodes were observed, along with a normal jaw joint. The intra-oral examination revealed red patches (depapillation) with a white border on the anterior two-thirds of the dorsal tongue extending to the right lateral of the tongue (Figure 1B–E). The OHI-S (Oral Hygiene Index Simplified) score indicated a good oral hygiene status with a score of 1. The GTASI score was 12 (moderate), and the NRS score was 6 (moderate pain) on the first visit.
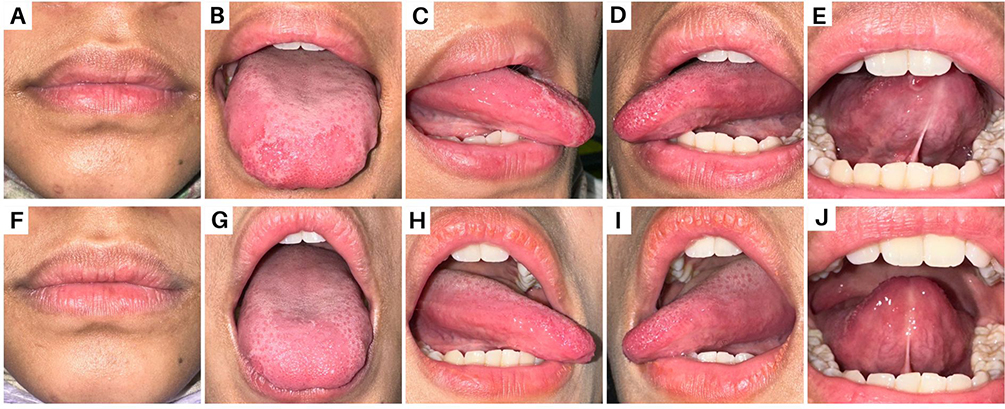 |
Figure 1 (A) shows dry lips; (B–E) intra-oral examination of the dorsal tongue, right lateral tongue, left lateral tongue, and ventral tongue at the first visit; (F–J) shows that the lesion improved clinically at the follow-up visit. |
Physical examinations and routine hematological tests were conducted during the first visit. The blood test results revealed an elevated platelet count, indicating inflammation, and an increase in eosinophil count, signifying an allergic response. Therefore, the patient should conduct additional tests, such as total IgE and skin prick tests. The complete results of the blood test may be seen in Table 1.
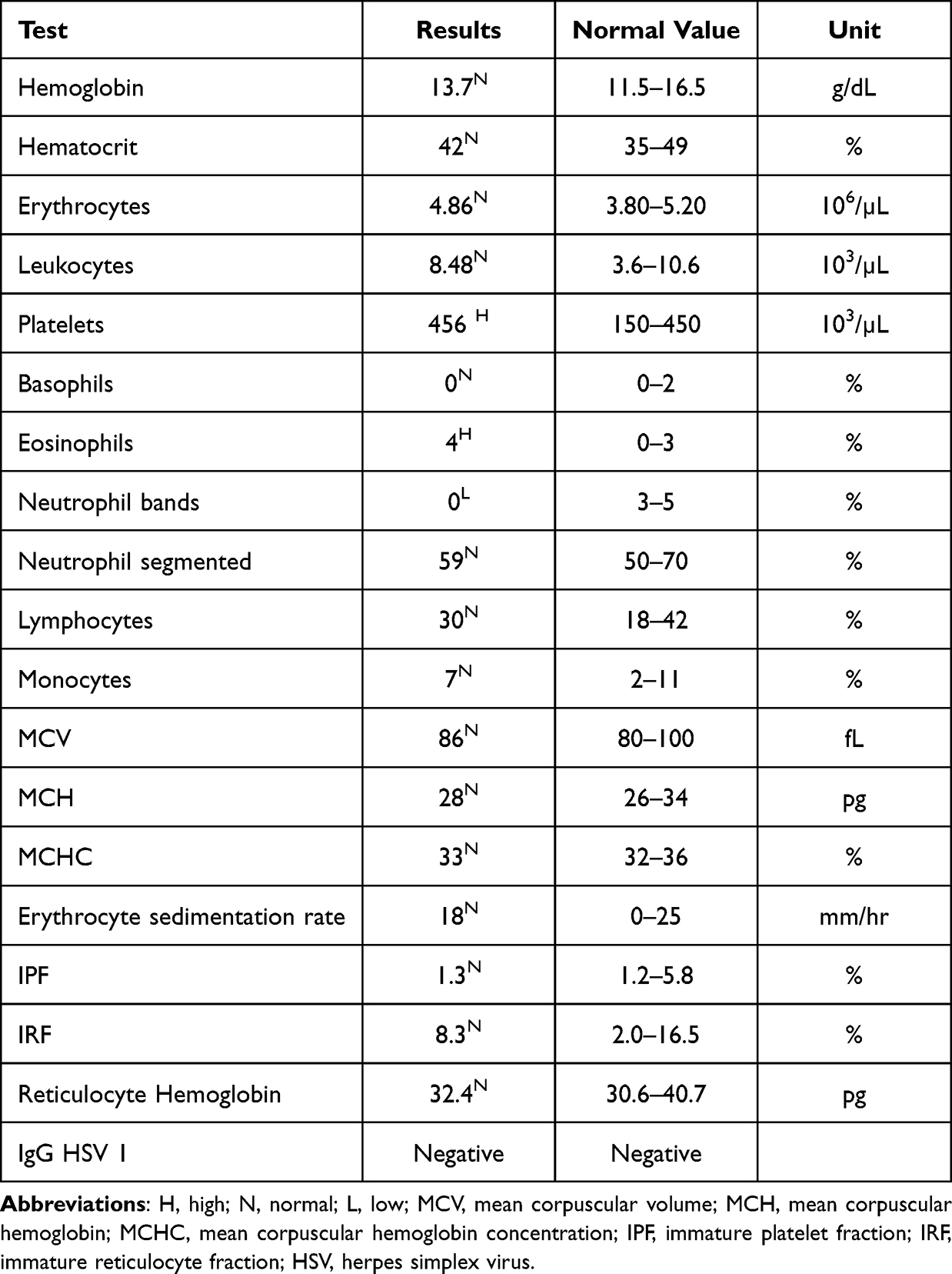 |
Table 1 Blood Test Results |
The working diagnosis was geographic tongue due to an allergic reaction. The non-pharmacological management of the patient included an explanation that the tongue condition was benign. The patient was advised to avoid consuming spicy foods and to brush her teeth and tongue twice daily using a soft-bristled toothbrush, once in the morning after breakfast and once in the evening before bed. Furthermore, the patient was recommended to maintain a healthy lifestyle by consuming nutritious foods and ensuring sufficient sleep. We prescribed a mouthwash containing benzydamine hydrochloride to alleviate the sensation of burning on the tongue, with a recommended dosage of 10 mL three times daily. A follow-up appointment was set for the patient one week later.
One week later, the patient attended a follow-up appointment with the results of additional tests. The total IgE examination value was 698 IU/mL (standard value <100 IU/mL), and there was a positive skin prick test result for chili (Figure 2). The patient was also found to be allergic to house dust, cottonwood, animal fur, crabs, chicken meat, and tomatoes, according to the skin prick test results, along with chili.
 |
Figure 2 Skin prick test. |
A diagnosis of chili-induced GT was confirmed after further investigation. Following both subjective and objective examinations, the patient reported no complaints. The NRS score was 0 (no pain), and the GTASI score was 0.4 (mild). Supplementary extra-oral and intra-oral photos taken during the follow-up visit are presented in Figure 1F–J. The patient was currently advised to avoid consuming spicy foods, including chili, and other known allergens, while also refraining from mouthwashes containing benzydamine hydrochloride.
Discussion
GT was originally described by Reiter in 1831 to denote persistent inflammatory oral lesions of unknown etiology that are immunologically mediated.19–22 GT is also referred to as erythema migrans, stomatitis migrans, annulus migratory, benign migratory glossitis, wandering tongue rash, and glossitis areata exfoliativa.14–16,23–25 It is a recurrent condition characterized by loss of epithelium, particularly of the filiform papillae on the dorsum of the tongue. The lesions present as multiple circular, irregular erythematous patches bounded by a slightly elevated, white, or cream-colored keratotic band or line. The central erythematous patch indicates the atrophy of the filiform papillae. The white border comprises regenerating filiform papillae and a mixture of keratin and neutrophils.26–30
GT affects approximately 1–3% of the population and appears to occur in both males and females,1 although some literature suggests a slightly higher female predilection (2:1).31 This may be because GT is associated with female hormones.32 GT is most common in adolescents and adults aged 5 to 84 years. In adults, changes in the tongue due to GT are more noticeable than in children.1,11,14,15,17,18
The etiology of GT is still unknown. Several related etiological factors have been proposed, including heredity, psoriasis, allergies, diabetes mellitus, hormonal disorders, nutritional disorders, psychological disorders such as stress, drugs such as oral contraceptives, lichen planus, Down syndrome, and Reiter’s syndrome.1,5,11,14,15,17,22,27,28,33 Heredity is associated with GT due to the observation that many parents and siblings of individuals with GT experience similar conditions, which is supported by findings of human leukocyte antigen (HLA)-DR5, HLA-DRW6, and HLA-Cw6.15,22,24,34 In this case, it is known that other family members do not exhibit a similar condition of the tongue (GT). However, her mother and siblings have a history of allergies.
Emotional stress is also associated with the occurrence and severity of GT.15 However, in this case, the GT condition was not related to stress, as supported by the negative emotional state scores on the DASS-21, which remained within normal limits. There is a significant relationship between Cw6 and psoriasis in GT.15 In this case, the GT condition was not related to psoriasis, as the results of the extraoral examination did not show psoriatic lesions on other parts of the body, such as the scalp and arms.
Allergies or atopy may be conditions underlying the occurrence of GT,22,32 as in this patient. Previous studies have shown that GT is frequently found in patients with allergies.26 Allergic conditions can be identified by the presence of abnormalities such as asthma, eczema, or allergic rhinitis, an elevated eosinophil count, elevated serum immunoglobulin E (IgE) levels, the presence of IgE to specific antigens, and a positive patch test or prick test. The patient’s history, serum levels of total IgE, and prick testing have indicated an association between GT and allergies.24,26,32,33 GT is directly related to high serum IgE levels (> 200 IU/mL).32
Predisposing factors for GT are associated with allergies triggered by the consumption of certain foods, including hot, spicy, salty, and cheese.33 Approximately 56% of GT patients have a history of related allergies.28,33 In this case, GT was triggered by allergies, supported by blood test results showing an elevated eosinophil count of 4%, a total IgE of 698 IU/mL (six times the standard value), and a positive prick test for chili. During the anamnesis, the patient recognized that after consuming spicy food (chili), the GT appeared.
Chili allergy is rare,10 which is the uniqueness of this case. It presents with tongue lesions and a persistent burning sensation. Based on the results of the anamnesis, physical examination, and supporting investigations, the diagnosis of chili-induced GT was established. Symptomatic GT may interfere with quality of life,22,35 as the patient needs to be constantly vigilant about the foods she consumes. Therefore, identifying risk factors is required to improve the quality of life for GT patients.
To investigate the presence of a food allergy, it’s essential to begin with a medical history, and a skin prick test may confirm symptoms. The skin prick test is an important test for evaluating allergic predisposing factors in GT patients.26,36 It is used to measure the incidence of type 1 allergic reactions, atopy, and IgE.26 This test is the preferred method for identifying the specific allergen responsible for an allergic reaction because it is simple, accurate, affordable, and has minimal side effects.37 The test involves marking the patient’s forearms, usually about 2 cm apart (Figure 2). Small amounts of potential allergens are applied to these marked areas and then pricked with a lancet. After 20 minutes, evaluate if a skin induration of 3 mm or more is considered a positive reaction.26
The pathogenesis of GT is related to epithelial turnover through desquamation and keratinization processes.38 The rate of desquamation of epithelial cells is typically the same as that of the basal layer of the epithelial lining of the oral mucosa. GT occurs due to the faster rate of desquamation of epithelial cells, resulting in a decrease in mature keratin and developing into ulcers.38 GT is generally asymptomatic, but some patients with GT may experience symptoms such as pain, burning, or itching of the tongue.16
The diagnosis of GT is based on history, clinical examination, and lesion characteristics and is rarely confirmed by histopathological examination.19 The clinical diagnosis criteria for GT include lesion-shaped islands like a map, migration, mild pain, and remissions and relapses within a short time.27,38 GT histopathological findings showed hyperkeratosis, acanthosis, elongated rete pegs, and migration of neutrophils.4,15,28
Therapy was evaluated by assessing the severity of GT using GTASI and NRS. GTASI is a clinical tool used to categorize the severity of GT, with scores ranging from 0 to 54. Categories include 1–7 for mild GT, 7–12 for moderate GT, and >12 for severe GT.27,39 NRS is an instrument used to measure pain intensity, with scores ranging from 0 to 10. Categories include 0 for no pain, 1–3 for mild pain, 4–6 for moderate pain, and 7–10 for severe pain. Clinical improvement was observed after one week, marked by a decrease in severity as measured by the GTASI from a score of 12 (moderate GT) to 0.4 (mild GT) and a decrease in NRS from 6 (moderate pain) to 0 (no pain). Unfortunately, we did not test the total IgE count after the lesion improved to check for a decreased value, which is a limitation of this case report.
GT is a typically harmless condition11,15 that is often asymptomatic and does not require any specific treatment.20 GT patients are advised to maintain optimal oral hygiene.27 GT patients also should avoid trigger factors (allergens) or certain foods such as chili, dried salted nuts, kiwi, tomatoes, pineapples, spicy, sour, hot foods, cigarettes or tobacco, and alcohol.11,18,20,36
There are no specific pharmacological interventions for the treatment of symptomatic GT.30 However, by understanding the pathogenesis of GT, the basis for the use of steroids as the first line of treatment aims to reduce symptoms.22 Symptomatic GT patients should receive palliative therapy with topical or systemic antihistamines that have proven beneficial. Benzydamine hydrochloride mouthwash can be used to alleviate the burning sensation.16 Some research has shown zinc supplementation is effective for GT management.15
Conclusion
Identifying risk factors, such as chili as an allergen, plays an important role in making a diagnosis and providing appropriate therapy for symptomatic geographic tongue patients.
Acknowledgments
The authors would like to express our sincere gratitude to the patient for granting her consent and to all those who kindly assisted us at the Universitas Padjadjaran Dental Hospital. The authors also gratefully acknowledge funding support from the directorate of research and community service at Universitas Padjadjaran.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Farah C, Balasubramaniam R, Mccullough MJ. Contemporary Oral Medicine. Springer Nature; 2019. doi:10.1007/978-3-319-72303-7
2. Dotiwala AK, Samra NS. Anatomy Head and Neck, Tongue. StatPearls; 2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507782/.
3. Sawczuk A, Mosier KM. Neural control of tongue movement with respect to respiration and swallowing. Crit Rev Oral Biol Med. 2001;12(1):18–37. doi:10.1177/10454411010120010101
4. Malamos D, Scully C. Clinical Guide to Oral Diseases. John Wiley & Sons, Inc; 2021.
5. Erriu M, Pili FMG, Cadoni S, Garau V. Diagnosis of lingual atrophic conditions: associations with local and systemic factors: a descriptive review. Open Dent J. 2016;10(1):619–635. doi:10.2174/1874210601610010619
6. Walliczek-Dworschak U, Schöps F, Feron G, Brignot H, Hähner A, Hummel T. Differences in the density of fungiform papillae and composition of saliva in patients with taste disorders compared to healthy controls. Chem Senses. 2017;42(8):699–708. doi:10.1093/chemse/bjx054
7. Correa M, Hutchinson I, Laing DG, Jinks AL. Changes in fungiform papillae density during development in humans. Chem Senses. 2013;38(6):519–527. doi:10.1093/chemse/bjt022
8. Zhou Y, Liu Y, Yang C, Chen H. Reactivity to food cues in spicy food cravers: physiological and behavioral responses. Physiol Behav. 2023;265. doi:10.1016/j.physbeh.2023.114157
9. Surya R, Tedjakusuma F. Diversity of sambals, traditional Indonesian chili pastes. J Ethn Foods. 2022;9(1):1–19. doi:10.1186/s42779-022-00142-7
10. Takei M, Nin C, Iizuka T, et al. Capsicum allergy: involvement of cap a 7, a new clinically relevant gibberellin-regulated protein cross-reactive with Cry j 7, the gibberellin-regulated protein from Japanese cedar pollen. Allergy Asthma Immunol Res. 2022;14(3):328–338. doi:10.4168/AAIR.2022.14.3.328
11. Glick M, Greenberg M, Lockhart P, et al. Burket’s Oral Medicine. Vol. 4.
12. Khanduri N, Rohatgi S, Kurup D, Mitra M. Asymptomatic benign migratory glossitis: a rare case report. Int J Pedod Rehabil. 2019;4(2):88. doi:10.4103/ijpr.ijpr_21_18
13. Neville BW, Damm DD, Allen CM, Chi AC. Color Atlas of Oral and Maxillofacial Diseases. Elsevier Inc; 2019.
14. Ghom AG, Ghom SA. Textbook of Oral Medicine.
15. Ongole R, P BN. Textbook of Oral Medicine, Oral Diagnosis and Oral Radiology.
16. Terezhalmy GT, Huber MA, Garcia LT, Or L. Physical Evaluation and Treatment Planning in Dental Practice. John Wiley & Sons; 2021.
17. Scully C. Oral and maxillofacial medicine. Elsevier; 2013. doi:10.1111/j.1601-0825.2008.01461.x
18. Bröcker Eva-Bettina PE. Diseases of the Oral Mucosa. Springer; 2021.
19. Picciani B, Santos VDC, Teixeira-souza T, et al. Investigation of the clinical features of geographic tongue: unveiling its relationship with oral psoriasis. Int J Dermatol. 2017:1–7. doi:10.1111/ijd.13460
20. Fernando H, Gonzaga DS, Gripp AC. Geographic tongue and psoriasis: clinical, histopathological, immunohistochemical and genetic correlation-A literature review. Ana Brasil De Dermatol. 2016;91(4):410–421. doi:10.1590/abd1806-4841.20164288
21. Liang J, Huang P, Li H, Zhang J, Ni C. Mutations in IL36RN are associated with geographic tongue. Hum Genet. 2017;136(2):241–252. doi:10.1007/s00439-016-1750-y
22. Oyetola EO, Oluwande A, Agho ET, Dentistry C, Ife I. Geographic tongue: pattern of presentation in a south western Nigerian teaching hospital. Ann Ibad Postgrad Med. 2018;16:2
23. van der Waal I. Burning Mouth Disease. Springer; 2021.
24. Ogueta IC, Ramírez MP, Jiménez CO, Cifuentes MM. Geographic tongue: what a dermatologist should know. Actas Dermo-Sifiliográficas. 2019;110(5):341–346. doi:10.1016/j.adengl.2019.05.001
25. Onda T, Hayashi K, Katakura A, Takano M, Report C. Geographic tongue: a tongue that changes appearance. Int J Case Rep Images. 2022;13(2):134–136. doi:10.5348/101344Z01TO2022CI
26. Goregen M, Melikoglu M, Miloglu O. Predisposition of allergy in patients with benign migratory glossitis. YMOE. 2010;110(4):470–474. doi:10.1016/j.tripleo.2010.04.036
27. Picciani BL, Santos LR, Amin TN, et al. Applicability of the geographic tongue area and severity index among healthcare professionals: a cross-sectional clinical validation of a newly developed geographic tongue scoring system. J Clin Med. 2021;10(23):5493. doi:10.3390/jcm10235493
28. Gonz L, Garc J, Garc M. Geographic tongue: predisposing factors, diagnosis and treatment: a systematic review. Rev Clíínica Española. 2018. doi:10.1016/j.rceng.2018.05.009
29. Matić-Petrović S, Đorđević M, Radunović M, et al. Geographic tongue - does candida play a role in its pathogenesis. Balkan J Dent Med. 2019;23(3):152–156. doi:10.2478/bjdm-2019-0027
30. De Campos WG, Esteves CV, Domaneschi C, Domaneschi C, Júnior CAL. Treatment of symptomatic benign migratory glossitis: a systematic review. Clin Oral Invest. 2018;22(7):2487–2493. doi:10.1007/s00784-018-2553-4
31. Scully C, Bagan J, Pedro Diz Dios AM. Oral Medicine and Pathology at a Glance.
32. Teixeira-souza T, Carneiro S, Moore D, et al. Geographic tongue and atopy: is there an association? Brazilian J Dent. 2018:1–7. doi:10.18363/rbo.v75.2018.e1186
33. Rezaei F, Safarzadeh M, Mozafari H, Tavakoli P. Prevalence of geographic tongue and related predisposing factors in 7–18 Year-old students in Kermanshah, Iran 2014. Glob J Health Sci. 2015;7(5):91–95. doi:10.5539/gjhs.v7n5p91
34. Picciani BL, Souza TT, Santos VDCB, et al. Geographic tongue and fissured tongue in 348 patients with psoriasis: correlation with disease severity. Sci World J. 2015;2015:1. doi:10.1155/2015/564326
35. Ferreira AO, Marinho RT, Velosa J, Costa JB. Geographic tongue and tenofovir. Case Rep. 2013;2013. doi:10.1136/bcr-2013-008774
36. Bajaj P, Kapoor C, Garg D, et al. Geographic tongue in A 6 year old child. Dent J Adv Stud. 2013;3:112–117.
37. Bignardi D, Comite P, Mori I, Ferrero F, Fontana V, Bruzzone M. Allergen-specific IgE: comparison between skin prick test and serum assay in real life. Allergol Sel. 2019;3(3):9–14. doi:10.5414/ALX01891E
38. Dafar A, Çevik-Aras H, Robledo-Sierra J, Mattsson U, Jontell M. Factors associated with geographic tongue. Acta Odontol Scand. 2016;74(3):210–216. doi:10.3109/00016357.2015.1087046
39. Lavinas B, Picciani S, Teixeira-Souza T. Geographic tongue severity index: a new and clinical scoring system. Oral Surg Oral Med Oral Pathol Oral Radiol. 2020;129(4):330–338. doi:10.1016/j.oooo.2019.12.007
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.