")
Back to Journals » The Application of Clinical Genetics » Volume 17
Healthcare Burden in Greenland of Gastrointestinal Symptoms in Adults with Inherited Loss of Sucrase-Isomaltase Function
Authors Andersen K , Hansen T , Jørgensen ME, Senftleber N
Received 6 October 2023
Accepted for publication 19 January 2024
Published 2 February 2024 Volume 2024:17 Pages 15—21
DOI https://doi.org/10.2147/TACG.S437484
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Martin Maurer
Kristine Andersen,1,2 Torben Hansen,3 Marit Eika Jørgensen,2,4,5 Ninna Senftleber2,4
1Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, Denmark; 2Steno Diabetes Center Greenland, Nuuk, Greenland; 3Novo Nordisk Foundation Center for Basic Metabolic Research, Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, Denmark; 4Clinical Research, Copenhagen University Hospital – Steno Diabetes Center Copenhagen, Herlev, Denmark; 5Centre for Public Health in Greenland, National Institute of Public Health, University of Southern Denmark, Odense, Denmark
Correspondence: Kristine Andersen, Tel +45 23 61 74 11, Email [email protected]
Background: Congenital sucrase isomaltase deficiency (CSID) is in general a very rare disease. However, 2– 3% of the Greenlandic population are homozygous (HO) carriers of an Arctic-specific loss-of-function (LoF) variant in the sucrase-isomaltase (SI) encoding gene, causing CSID. The condition is characterized by gastrointestinal symptoms such as stomachache, diarrhea, and weight loss when consuming sucrose, the most common dietary sugar. However, the awareness of the condition in the population and the healthcare system seems to be limited, potentially leading to a higher healthcare burden. Hence, we aimed to investigate whether HO-carriers visit the healthcare system more with gastrointestinal symptoms compared to the control groups by using registry data.
Methods: We performed a case–control study identifying cases and controls using genotype information from the 1999– 2001 and 2005– 2010 Greenlandic health population cohorts. The cases were defined as HO LoF SI-carriers and controls were defined as non-carriers and were matched (1:1) on sex, age, place of residence, and European genetic admixture. We used electronic medical records to assess the number of electronic medical record contacts (EMRc) related to gastrointestinal symptoms and the number of gastrointestinal-related diagnostic procedures.
Results: A total of 80 HO-carriers and 80 non-carriers were included. The HO-carriers had 19% more EMRc related to gastrointestinal symptoms (IRR, 1.19, 95% CI [1.02;1.40], p=0.02) and had a 41% higher incidence of gastrointestinal related diagnostic procedures compared to controls (IRR, 1.41, 95% CI [1.05– 1.92], p=0.02). Only one HO-carrier was aware of the condition according to the electronic medical records.
Conclusion: HO-carriers of the LoF SI-variant had both significantly more gastrointestinal-related EMRc and significantly more diagnostic procedures conducted due to gastrointestinal symptoms. Only one HO-carrier was aware of the condition. Given the high prevalence of HO-carriers in the Greenlandic population, we anticipate that diagnosing more patients with CSID and providing dietary advice could potentially reduce symptom burden and healthcare visits among HO-carriers.
Keywords: Inuit, genetic metabolism, sucrase-isomaltase, Greenland, congenital sucrase-isomaltase deficiency, loss-of-function variant
Introduction
Sucrase-isomaltase (SI) is an enzyme that plays a crucial role in the digestion of sucrose, isomaltose, and starch by breaking down α-glycosidic linkages, which is necessary for absorption in the brush border of the small intestine.1 Congenital sucrase-isomaltase deficiency (CSID) is a condition characterized by a decreased SI activity and thus decreased ability to digest and absorb sucrose.2 When individuals with CSID consume sucrose, they experience gastrointestinal symptoms such as stomachache, diarrhea, and weight loss.3 Various genetic mutations have been identified in the SI gene, resulting in varying degrees of enzyme activity.2 Recently, the artic specific SI c.273_274delAG was discovered,1 which is predicted to result in complete loss of SI function in homozygous (HO) individuals, thus preventing the digestion of sucrose and isomaltose.1 While this loss-of-function (LoF) is rare worldwide, the allele frequency was estimated to 14.1% in the Greenlandic population.4 Enzymatic replacement therapy exists, enabling HO-carriers to cleave and absorb sucrose to a higher degree; however, the recommended treatment in Greenland is avoiding sucrose-containing food.5
Traditionally, the lifestyle in Greenland was centered around hunting and fishing.6,7 The diet primarily consisted of fish, sea mammals, and herbs, with minimal sucrose content.6,7 As a result, the SI c.273_274delAG variant may not have caused significant gastrointestinal symptoms in the past. However, the lifestyle of the Greenlandic population, including their diet, has transitioned towards a more Westernized pattern during the last 100 years, with increased consumption of sucrose and starch8; in the general population, the average consumption of sucrose has been estimated to 16% of the total energy intake.7
Symptomatic diagnosis of CSID among Greenlanders can be challenging due to the difficulty in differentiating CSID symptoms from those of other gastrointestinal diseases including other malabsorption diseases, eg, lactose intolerance and trehalase deficiency which are common in Greenland.9,10 Furthermore, the low global prevalence of CSID and limited awareness about the condition can lead to a prolonged diagnostic process; eg, recent studies have shown that adult CSID is often misdiagnosed as irritable bowel syndrome.11–13
Diagnosing CSID typically involves small intestinal biopsy or less invasive tests such as the sucrose breath test and genetic testing.3 In Greenland, CSID can be diagnosed through a sucrose tolerance test because the SI-variant causes a complete loss of function rather than just a reduction in enzyme activity.4 The prolonged diagnostic process within the healthcare system imposes unnecessary time and cost burdens on both patients and the healthcare system. Though data from the Greenlandic cohorts showed no differences between HO-carriers and other individuals in self-reported digestive issues,4 this was only assessed on a broad level and we anticipate that HO-carriers do experience more digestive problems, thus increasing the need for gastrointestinal-related healthcare. We therefore aimed to assess whether Greenlandic HO-carriers visit the healthcare system more with gastrointestinal symptoms compared to the control groups by using registry data.
Materials and Methods
Study Design and Participants
We conducted a case–control study and identified cases and controls using genotype information from two Greenlandic population cohorts collected during 1999–2001 and 2005–2010,14,15 which identified 99 HO LoF SI c.273_274delAG carriers.4 Participants were not informed about their SI genotype at the time of the current study. Cases were defined as HO-carriers of the LoF SI-variant and living in Greenland (referred to as “HO-carriers” in the remaining paper). For each HO-carrier, we included a non-carrier as control, matched on age (± 10 years), sex, European genetic admixture, and place of residence at the time of participation in the population cohort study. We recorded smoking status since smoking has been associated with various gastrointestinal symptoms which could bias the effect of CSID on gastrointestinal-related health activities.16 We assessed carrier status of rs4988235, causing lactase persistence in homozygous carriers of the minor allele,10 and rs2276064 causing decreased trehalase activity with increasing number of minor alleles.9
Data Sources
Data was obtained for a 30-year period, by reviewing electronic medical records in the system Æskulap, covering 1992–2007, and the current electronic medical record system Cambio COSMIC (Cambio, Sweden) covering 2007–2022. We counted the number of electronic medical records contacts (EMRc) due to gastrointestinal symptoms from both primary and the secondary sector, including epigastric pain, acid reflux, stomach ache, bloating, and diarrhea. Furthermore, we investigated the number of diagnostic tests, including imaging, ultrasound, and biopsies due to gastrointestinal symptoms. We used Microsoft Excel (2021) for data management and R (4.1.2)17 for statistical analyses. Participant characteristics were obtained primo 2022.
Statistical Analyses and Data Management
Categorical variables are presented as numbers and percentages. Continuous variables are presented as means and standard deviation (SD) when they are normally distributed and otherwise as medians and interquartile range (IQR). Differences in participant characteristics were compared with Chi-square test for categorical variables and 2-sided t-test for continuous variables. The level of statistical significance was p <0.05. The number of gastrointestinal-related EMRc and the number of diagnostic tests is presented as incidence rates (IR) per 100 person years. Person years were calculated as the time from the first EMRc to either the date of death or end of follow-up, being 1st March 2022. The groups were compared using incidence rate ratio (IRR) with confidence interval and p-value. We conducted subgroup analyses with sex and age, dividing the age subgroup in two groups based on the median age, ie, ≥59 years and <59 years.
Results
Population Characteristics
We had access to electronic medical records on 91 of the 99 HO-carriers. Ten of the 91 were excluded due to immigration after participation in the health population study. We excluded one HO-carrier, as the person died prior to implementation of electronic medical records, resulting in 80 HO-carriers being included. The population characteristics were similar between the two groups, including smoking status, and the carrier status of the TREH variant rs2276064, linked to reduced trehalase activity.9 However, the minor allele of the variant in the lactase gene linked to lactase persistence (rs4988235) was slightly more prevalent in control individuals; however not statistically significant (Table 1). Only one out of 80 HO-carriers was aware of the condition according to electronic medical records.
 |
Table 1 Population Characteristics of HO-Carriers and Controls |
Number of Electronic Medical Record Contracts and Diagnostic Procedures
The two groups had similar mean follow-up periods (p = 0.11) of 15.0 years (SD = 6.44) for the HO-carriers and 16.6 years (SD = 6.40) for the controls, respectively. The HO-carriers had 19% more EMRc due to gastrointestinal symptoms compared with the controls. Moreover, the HO-carriers had a 41% higher incidence of gastrointestinal-related diagnostic procedures compared to the controls (Figure 1).
 |
Figure 1 Incidence rates of electronic medical record contacts and diagnostic tests. aDiagnostic tests due to gastrointestinal symptoms. Abbreviations: EMRc, electronic medical record contacts; GI, gastrointestinal; IRR, incidence rate ratio; PY, person years. |
Subgroup Analyses
We found that both HO-carriers of female sex and those <59 years had more EMRc compared with controls. Specifically, female HO-carriers had 36% more EMRc compared with female controls, while there was no difference between male HO-carriers and controls. Among individuals <59 years, we found that HO-carriers had 222% more EMRc as compared with controls. Among individuals ≥59 years we found that HO-carriers had 21% fewer EMRc compared to controls. Results of the subgroup analyses are shown in Figure 2.
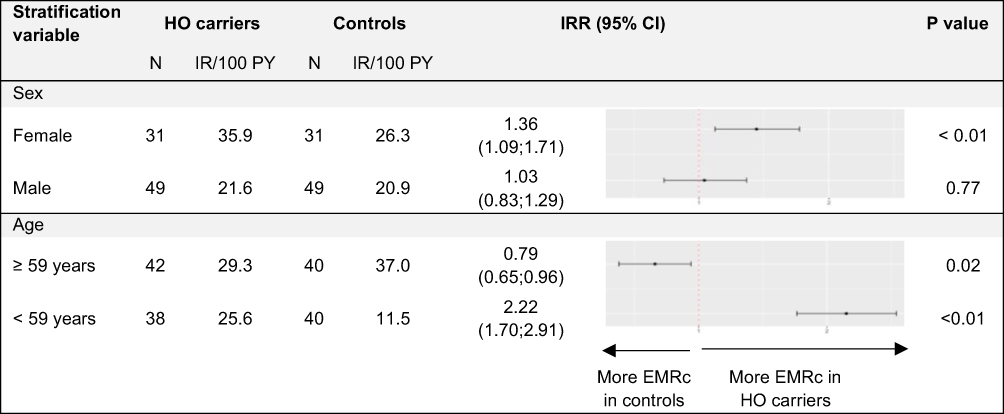 |
Figure 2 Subgroup analyses of incidence rates of electronic medical record contacts. Abbreviations: CI, confidence interval; EMRc, electronic medical record contacts; IR, incidence ratio; IRR, incidence rate ratio. |
Discussion
The main findings of this study showed that Greenlandic HO-carriers of the LoF SI-variant have a higher occurrence of EMRc and diagnostic procedures due to gastrointestinal symptoms compared to the control group. Interestingly, self-reported gastrointestinal symptoms were not found to be higher among HO-carriers compared to others in the previous Greenlandic population survey.4 However, the questions were general and not very specific. Questionnaires have limitations including recall bias whereas quantifying EMRc reduces recall bias. This study is important because it demonstrates that well-known CSID symptoms lead HO-carriers to seek healthcare significantly more than the control group, enhancing our understanding of the broader effects of the HO LoF variant and adding to our existing knowledge.
Globally, CSID is a rare disease, potentially leading to a lack of awareness among physicians. In Greenland, the estimated prevalence of CSID caused by the LoF SI-variant (c.273 274delAG) is 2–3%.4 Notably, our study revealed that only one out of 80 HO-carriers was aware of the condition, as documented in the electronic medical records. The higher incidence rates of EMRc and diagnostic tests are likely attributable to the HO-carrier’s limited awareness of their intolerance, as well as the healthcare system’s limited awareness. Additionally, the current Greenlandic diet, characterized by a high sucrose content, likely induces symptoms among HO-carriers.2,18,19 Examining a broader timeframe, specifically the past 100 years, would be intriguing to evaluate the symptom burden during the transition from a predominantly traditional diet, where no symptoms are expected, to a Western diet. Unfortunately, medical records are only accessible from 1992.
Other malabsorption diseases, such as lactase persistence and trehalase deficiency, present symptoms similar to CSID. However, we observed similar genotype frequencies of the variant affecting trehalase activity in the two groups. Additionally, given the limited presence of trehalose in foods,20 we anticipate minimal impact on our results. The prevalence of lactose intolerance was not significantly different between the groups. However, more HO-carriers were lactose-intolerant, which may have contributed to a potential overestimation of the association between CSID and health-seeking behavior.
Greenlandic HO-carriers have a healthier metabolic profile than the remaining population, with lower BMI, body weight, fat percentage, and fasting triglyceride.4 The health benefits are potentially mediated by reduced sucrose uptake and possibly by higher levels of acetate formed when sucrose passes to and is fermented in the colon.21 If the HO-carriers were aware of the condition, they could adjust their diet more effectively, thereby still obtaining the health benefits and avoiding gastrointestinal symptoms. Hence, we would expect improvements in health-related quality of life of the HO-carriers and a decreased burden of the healthcare system. However, achieving this would require increased awareness among physicians in Greenland and the ability to perform diagnostic testing for CSID, including whole-genome sequencing. Whole-genome sequencing has become easier and cheaper to perform22 and also enables the detection of other known Inuit specific gene variants, eg, the common low-density lipoprotein receptor variant.23
Our subgroup analyses revealed that younger and female HO-carriers had significantly more EMRc compared to their counterparts in the control group. The higher overall rate of EMRc in the younger group may be influenced by multiple factors. Firstly, older individuals, who traditionally consumed less sugar, may experience fewer symptoms due to dietary differences between generations.24 Secondly, the implementation of the electronic medical record system varied across Greenland from 1992 to 2007, making healthcare system data before the implementation unavailable.
Interestingly, we observed that HO-carrier status was associated with more EMRc in women, but not in men. This might be explained by women being more likely to consume Western foods compared to men, who tend to adhere to traditional Greenlandic diets.24 Moreover, women in other populations have been found to be more likely to seek healthcare, while men tend to accept and endure their symptoms.25
This study has several limitations. First, the study design depends on the subjective experience of gastrointestinal symptoms, and health-seeking behavior is affected by, eg, sex, age, culture, and the access to medical attention.26 We have attempted to minimize the effect of these factors by matching HO-carriers with controls on sex, age, the degree of genetic admixture, and place of residence. However, the HO-carriers have experienced gastrointestinal symptoms throughout life, and it is possible that they have become accustomed to their symptoms, and therefore are less likely to visit the healthcare system because of this.
Secondly, the electronic medical record system was not implemented in the same year throughout Greenland but was implemented across the country from 1992 to 2007. However, this should not result in bias, as controls were matched based on place of residence. Moreover, the majority of the population had long follow-up times, with data spanning from 1992 to 2007 and up to 2022, and the mean inclusion time in the two groups was similar, minimizing the risk of bias due to inclusion time. We were able to follow up on all individuals in health records due to the unique national personal identification number, thereby avoiding recall bias which is a major strength of this study. Furthermore, the matching on age, sex, location, and European genetic admixture is a strength, ensuring that the controls closely resemble the genetic profile of the HO-carriers.
Conclusion
The prevalence of CSID caused by the LoF SI-variant (c.273 274delAG) was previously found to be high in the Greenlandic population. Although results from the Greenland population surveys indicated that the HO-carriers do not experience more gastrointestinal-related symptoms than others,4 our results show that HO-carriers not only exhibit significantly more health care visits but also undergo more diagnostic procedures due to gastrointestinal symptoms compared to wildtype individuals. Only one out of 80 HO-carriers was aware of the condition. Therefore, we recommend raising awareness of CSID as an Arctic disease among healthcare professionals in Greenland and in the general population. We anticipate that diagnosing more patients with CSID and providing accurate dietary advice could potentially reduce the symptom burden and healthcare visits among CSID patients.
Ethics Approval and Informed Consent
Approvals were obtained from the Greenlandic scientific ethics committee (KVUG 2017-5582) and the patients have consented to connect data from the population study to electronic medical records. Review of the electronic medical records was granted by the National Health Authorities in Greenland. All data will be handled in accordance with The Act on Processing of Personal Data.
Acknowledgments
We would like to acknowledge the staff and the participants of the Greenlandic health surveys.
Funding
NS received funding from The Greenland Institute of Natural Resources (postdoctoral grant number 80.045) and The Greenlandic Research Council. MEJ is employed at Steno Diabetes Center Greenland, partly funded by the Novo Nordisk Foundation (NNF20SA0064190).
Disclosure
NS held shares in Novo Nordisk AS, but sold in 2022. MEJ has received research grants from Astra Zeneca, Boehringer Ingelheim, Sanofi Aventis. MEJ holds shares in Novo Nordisk AS. The authors report no other conflicts of interest in this work.
References
1. Marcadier JL, Boland M, Scott CR, et al. Congenital sucrase-isomaltase deficiency: identification of a common Inuit founder mutation. CMAJ. 2015;187(2):102–107. doi:10.1503/CMAJ.140657/-/DC1
2. Cohen SA. The clinical consequences of sucrase-isomaltase deficiency. Mol Cell Pediatr. 2016;3(1):1–4. doi:10.1186/S40348-015-0028-0
3. Tuck CJ, Biesiekierski JR, Schmid-Grendelmeier P, Pohl D. Food intolerances. Nutrients. 2019;11(7):1684. doi:10.3390/NU11071684
4. Andersen MK, Skotte L, Jørsboe E, et al. Loss of sucrase-isomaltase function increases acetate levels and improves metabolic health in Greenlandic cohorts. Gastroenterology. 2021:1–12. doi:10.1053/j.gastro.2021.12.236
5. Sakkarose_intolerans_final_DK_net. Available from: https://paarisa.gl/materialer/bestil-materialer?sc_lang=da.
6. Linder M, Belhaj N, Sautot P, Arab Tehrany E. From krill to whale: an overview of marine fatty acids and lipid compositions. Ol Corps Gras Lipides. 2010;17(4):194–204. doi:10.1051/OCL.2010.0328
7. Jeppesen C, Bjerregaard P. Consumption of traditional food and adherence to nutrition recommendations in Greenland. Scand J Public Health. 2012;40(5):475–481. doi:10.1177/1403494812454467
8. Senftleber NK, Overvad M, Dahl-Petersen IK, Bjerregaard P, Jørgensen ME. Diet and physical activity in Greenland: genetic interactions and associations with obesity and diabetes. Appl Physiol Nutr Metab. 2021;46(8):849–855. doi:10.1139/apnm-2021-0020
9. Kozlov A, Vershubskaya G, Gorin I, Petrushenko V, Lavryashina M, Balanovska E. Prevalence of genetically determined trehalase deficiency in populations of Siberia and Russian Far East. Int J Circumpolar Health. 2023;82(1). doi:10.1080/22423982.2023.2183931
10. Niclasen S, Andersen S, Albertsen N, Krarup HB. The influence of Scandinavian presence on Greenlandic lactase persistence. Scand J Gastroenterol. 2023;58(4):349–353. doi:10.1080/00365521.2022.2139155
11. Garcia-Etxebarria K, Zheng T, Bonfiglio F, et al. Increased prevalence of rare sucrase-isomaltase pathogenic variants in irritable bowel syndrome patients. Clin Gastroenterol Hepatol. 2018;16(10):1673–1676. doi:10.1016/J.CGH.2018.01.047
12. Foley A, Halmos EP, Husein DM, et al. Adult sucrase-isomaltase deficiency masquerading as IBS. Gut. 2021:gutjnl-2021–326153. doi:10.1136/GUTJNL-2021-326153
13. Lenhart A, Chey WD, Eswaran S. Sucrase-isomaltase deficiency: hiding in plain sight? Curr Treat Options Gastroenterol. 2021;19(3):500–508. doi:10.1007/S11938-021-00357-8
14. Bjerregaard P, Curtis T, Borch-Johnsen K, et al. Inuit health in Greenland: a population survey of life style and disease in Greenland and among Inuit living in Denmark. Int J Circumpolar Health. 2003;62(Suppl 1):3–79. doi:10.3402/IJCH.V62I0.18212
15. Bjerregaard P. Inuit health in transition Greenland survey 2005–2010. Population sample and survey methods. 2nd ed; 2011. Available from: https://www.sdu.dk/da/sif/rapporter/2011/inuit_health_in_transition.
16. Lundström O, Manjer J, Ohlsson B. Smoking is associated with several functional gastrointestinal symptoms. Scand J Gastroenterol. 2016;51(8):914–922. doi:10.1080/00365521.2016.1174878
17. R Core Team. R: A language and environment for statistical computing; 2021. Available from: https://www.r-project.org/.
18. Chiruvella V, Cheema A, Arshad HMS, Chan JT, Yap JEL. Sucrase-isomaltase deficiency causing persistent bloating and diarrhea in an adult female. Cureus. 2021;13(4). doi:10.7759/CUREUS.14349
19. Smith H, Romero B, Flood E, Boney A. The patient journey to diagnosis and treatment of congenital sucrase-isomaltase deficiency. Qual Life Res. 2021;30(8):2329. doi:10.1007/S11136-021-02819-Z
20. Chen A, Gibney PA. Dietary trehalose as a bioactive nutrient. Nutrients. 2023;15(6). doi:10.3390/nu15061393
21. Senftleber NK, Ramne S, Moltke I, et al. Genetic loss of sucrase-isomaltase function: mechanisms, implications, and future perspectives. Appl Clin Genet. 2023;16:31–39. doi:10.2147/TACG.S401712
22. Prokop JW, May T, Strong K, et al. Genome sequencing in the clinic: the past, present, and future of genomic medicine. Physiol Genomics. 2018;50(8):563–579. doi:10.1152/PHYSIOLGENOMICS.00046.2018
23. Jørsboe E, Andersen MK, Skotte L, et al. An LDLR missense variant poses high risk of familial hypercholesterolemia in 30% of Greenlanders and offers potential of early cardiovascular disease intervention. Hum Genet Genom Adv. 2022;3(4):100118. doi:10.1016/j.xhgg.2022.100118
24. Bjerregaard P, Jeppesen C. Inuit dietary patterns in modern Greenland. Int J Circumpolar Health. 2010;69(1):13–24. doi:10.3402/IJCH.V69I1.17387
25. Powell W, Adams LB, Cole-Lewis Y, Agyemang A, Upton RD. Masculinity and race-related factors as barriers to health help-seeking barriers among African-American men. Behav Med. 2016;42(3):150. doi:10.1080/08964289.2016.1165174
26. Mackian S. A review of health seeking behaviour: problems and prospects; 2003
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.